Back to Journals » Infection and Drug Resistance » Volume 19
Emergence of a CTX-M-14- ESBL-Producing Multidrug-Resistant Pasteurella multocida from Human Bacteremia in China: A Case Report and Literature Review
Authors Meng H ![]() , Deng S, Chen X, Li C
, Deng S, Chen X, Li C ![]() , Li Y
, Li Y ![]()
Received 6 November 2025
Accepted for publication 30 January 2026
Published 4 March 2026 Volume 2026:19 576581
DOI https://doi.org/10.2147/IDR.S576581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Huixia Meng,1 Shumin Deng,1 Xingchun Chen,2 Chunhong Li,1 Yuan Li1
1Department of Microbiology, Guangxi KingMed Diagnostics, Nanning, People’s Republic of China; 2Department of Laboratory Medicine, The People’s Hospital of Guangxi Zhuang Autonomous Region, Guangxi Academy of Medical Sciences, Nanning, People’s Republic of China
Correspondence: Yuan Li, Email [email protected]
Abstract: Pasteurella multocida (P. multocida) bloodstream infections in humans without a history of animal bites are commonly associated with immunocompromise. Empirical therapy typically involves a β-lactam/β-lactamase inhibitor combination (eg, amoxicillin-clavulanate), but a small number of amoxicillin-clavulanate–resistant strains have been reported. Herein, we report a rare case of human P. multocida bacteremia in a patient with no history of animal bites. Antibacterial susceptibility testing showed the strain was sensitive to trimethoprim-sulfamethoxazole; resistant to erythromycin; and non-susceptible to azithromycin, levofloxacin, tetracycline, penicillin, ampicillin, amoxicillin-clavulanate and ceftriaxone. Whole-genome sequencing (WGS) confirmed the presence of CTX-M-14-type extended-spectrum β-lactamases (ESBLs). The potential emergence of multidrug-resistant (MDR) P. multocida may challenge the empirical treatment of the strain. This case highlights the necessity of studying the antibiotic susceptibility patterns of P. multocida in humans and animals, as well as the need for a One Health approach.
Keywords: Pasteurella multocida, extended-spectrum β-lactamases, ESBLs, multidrug-resistant, whole-genome sequencing, one health
Introduction
P. multocida is a small, gram-negative, facultative anaerobic coccobacillus that is highly prevalent in the digestive tract and oral cavity of many animal species.1,2 The bacterium harbors various potential virulence factors, such as toxins, lipopolysaccharides, fimbriae, adhesins, iron-regulated acquisition proteins, hyaluronidase, and sialic acid metabolism pathways.3 These factors can cause infections in diverse hosts, including livestock, wildlife, and humans.4 Of the reported human cases of P. multocida infection, approximately 43% had no history of animal bites. Although many infections associated with animal bites are limited to soft tissues, the isolation of P. multocida from respiratory tract and bloodstream is more often associated with no animal bite.5–7
Most P. multocida infections can be traced to cat and dog bites. As previously documented, infections unrelated to animal bites are typically associated with bacteremia, severe comorbidities, advanced age, or immunocompromised states.5 Most P. multocida isolates from humans are susceptible to penicillin and other antibiotics such as macrolides fluoroquinolones and tetracyclines.2,6,8 Approximately 13% of strains are β-lactamase–positive, but the specific types of enzyme have been little studied.5 Resistance to amoxicillin/clavulanate is extremely rare in human infections caused by P. multocida.9,10 MDR P. multocida isolated from animals has been reported, but primarily involving resistance to ampicillin, macrolides, aminoglycosides, fluoroquinolones, and/or tetracyclines.11–13 Here, we present a case of human bacteremia caused by P. multocida whose isolate was resistant or non-susceptible to penicillin, ampicillin, amoxicillin/clavulanate, and ceftriaxone. WGS revealed a chromosomally located blaCTX-M-14. The strain was also resistant or non-susceptible to macrolides, quinolones, and tetracyclines.
Case Presentation
An 88-year-old woman was admitted to a local hospital on October 25, 2024, following 7 days of dizziness, blurred vision, facial drooping, generalized weakness, and persistent abdominal distension and pain. Her medical history included hypertension, heart disease, cerebral infarction, and rheumatic diseases. On admission, a physical examination revealed bilateral crackles in the lungs. She had no cough, sputum, or fever (36.5°C), and no evidence of scratches or bite marks. The patient’s cranial CT showed multiple lacunar infarcts in the bilateral basal ganglia, the left corona radiata, and the brainstem (some lesions are considered old). Laboratory tests showed leukocytosis (35.40 × 109/L), markedly elevated C-reactive protein (CRP; 315.2 mg/L; normal < 5 mg/L), anemia (hemoglobin 92 g/L; normal 110–150 g/L), and an increased erythrocyte sedimentation rate (116 mm/h; normal 0–15 mm/h). One set of blood cultures (aerobic and anaerobic) was obtained. An empirical treatment with intravenous cefoperazone-sulbactam was initiated. On the third day of hospitalization, small gram-negative coccobacilli were detected in both the aerobic and anaerobic blood culture bottles. The isolate was subcultured on blood and chocolate agar plates at 37°C and 5% CO2. Small, non-hemolytic, gray colonies grew on both media. The bacterial strain was identified as P. multocida by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS1000, Antu). By the sixth day of hospitalization, the patient’s leukocyte was 8.52 × 109/L and CRP level was 81.76 mg/L, indicating a favorable response to treatment, which was continued for 2 weeks. On the 14th day, her leukocyte count of 5.47 × 109/L and CRP < 5.0 mg/L. She was conscious with no other discomfort and was discharged.
Antibiotic Sensitivity Testing
Following the CLSI M45-Ed3 protocol,14 broth microdilution and disk diffusion methods were used for antimicrobial susceptibility testing. Blood Mueller–Hinton agar plates supplemented with 5% sheep blood were used for disk diffusion, whereas a commercial susceptibility testing kit (Bio-Mérieux, France) was used for the broth microdilution method. All the plates were incubated at 35°C in ambient air. Each antibiotic susceptibility test was performed in duplicate. Streptococcus pneumoniae (ATCC 49619), Escherichia coli (ATCC 35218), and Staphylococcus aureus (ATCC 25923) were used as the quality control strains. Inhibition zones were measured after 18 hours. Inhibition zones of the strain were showed in Figure 1A–C. The results showed that the isolate was sensitive to trimethoprim–sulfamethoxazole (SXT), resistant to erythromycin (E), and non-susceptible to azithromycin (AZM), levofloxacin (LEV), tetracycline (TE), amoxicillin, amoxicillin/clavulanate (AMC), ceftriaxone (CRO), penicillin (P), and ampicillin (AMP; Table 1). Presently, no CLSI breakpoints are available for ceftazidime (CAZ), cefepime, piperacillin/tazobactam, Cefoperazone-sulbactam, meropenem (MEM), and imipenem (IPM); however, their MIC values are markedly low, suggesting good in vitro activity against the isolates.
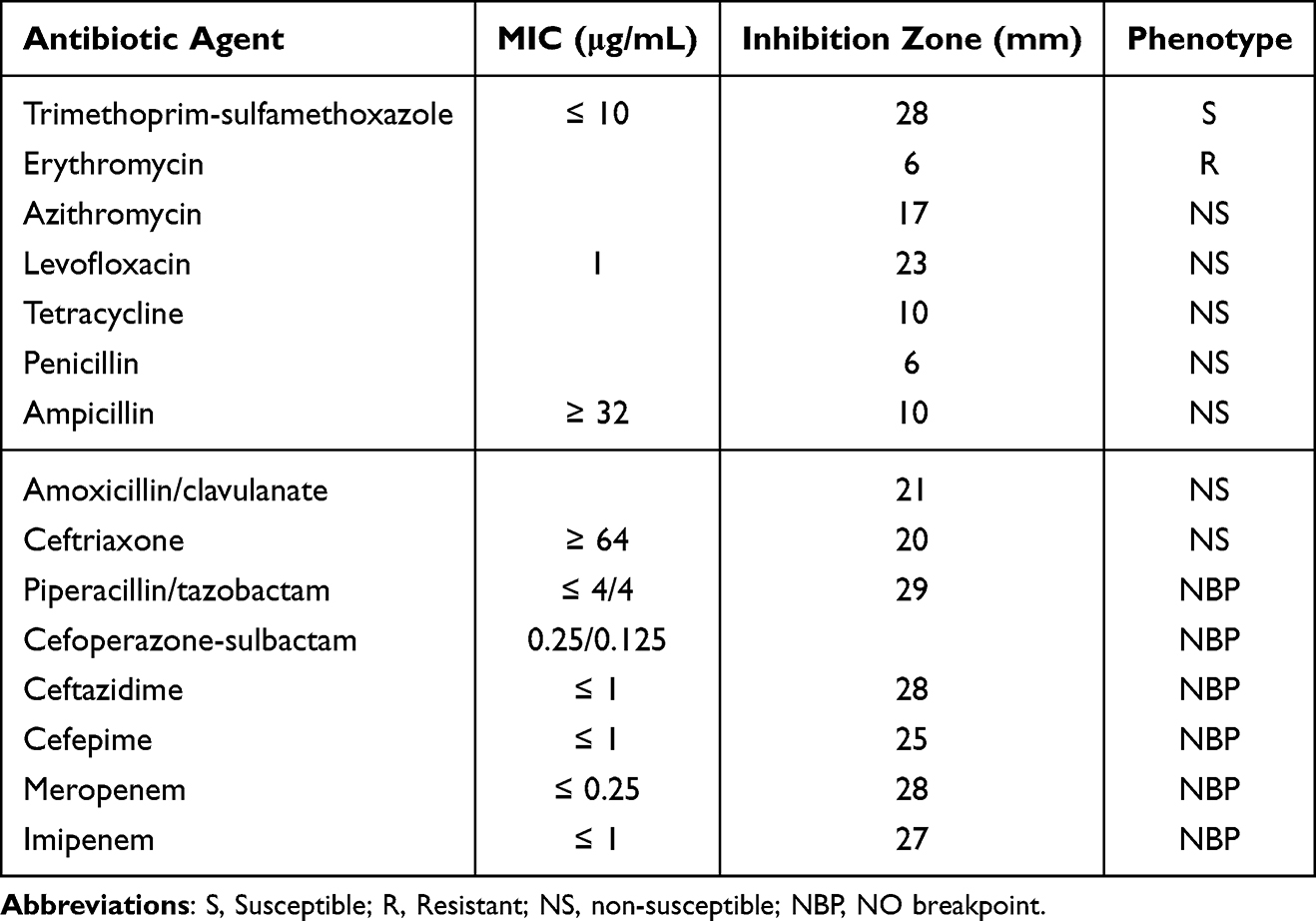 |
Table 1 Drug Susceptibility of P. Multocida Determined by Broth Microdilution and Disk Diffusion Methods |
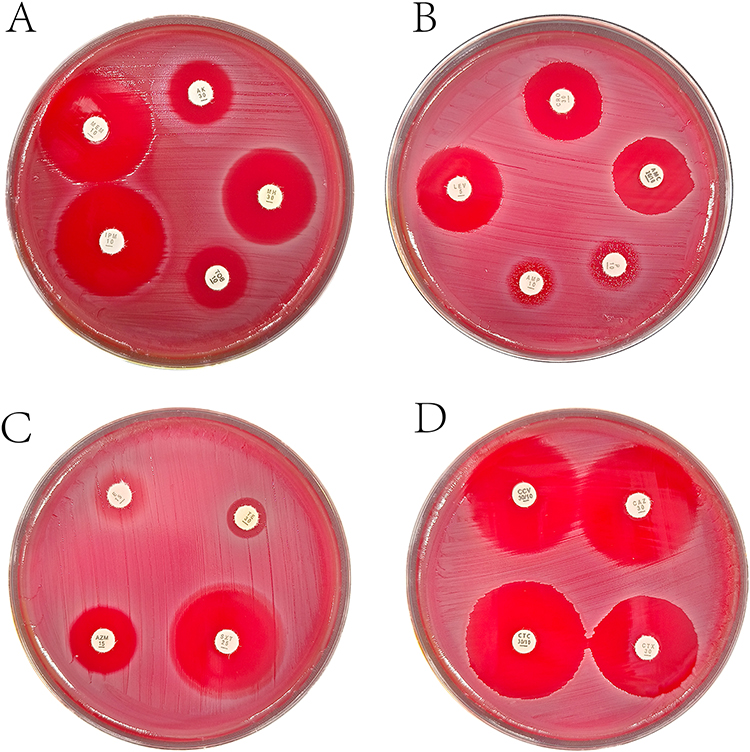 |
Figure 1 (A–C) Inhibition zones of P. multocida after incubating at 35°C for 24 hours. (D) Test for ESBL production. |
ESBL Test
The ESBL test was performed in accordance with the CLSI M100.15 The ceftazidime (CAZ) zone measured 29 mm, and the ceftazidime–clavulanate (CCV) zone measured 29 mm. The cefotaxime (CTX) zone measured 24 mm, while the cefotaxime–clavulanate (CTC) zone measured 31 mm. The 7 mm increase in the CTC zone in combination with CTC (Figure 1D) indicated that the strain was a CTX-M-type ESBL producer.14
Genome Sequencing and Analysis
Whole genome sequencing (WGS) was performed using the Illumina HiSeq 2500 and PacBio platforms. Raw reads were filtered using Skewer and Porechop (https://github.com/rrwick/Porechop) to remove low-quality sequences and adaptors, respectively. De novo assembly was performed using the SPAdes Genome Assembler v3.13.1 and Unicycler. Antimicrobial resistance genes were identified using the CGE server (https://cge.food.dtu.dk/services/) and Comprehensive Antibiotic Resistance Database (CARD).
The strain carried 13 antibiotic resistance genes (ARGs), including those conferring resistance to β-lactam drugs such as Haemophilus influenzae (H. influenzae) PBP3, blaCTX-M-14 (located at positions 2,166,705–2,167,580; Figure 2), and blaOXA-1. Additional resistance genes included catP (chloramphenicol acetyltransferase), tetB, tetR, FosA3 (fosfomycin thiol transferase), ermT (erm 23S rRNA methyltransferase), and aminoglycoside antibiotic inactivation genes, such as APH(3ʹ)-Ia, APH(3ʹʹ)-Ib, APH(6)-Id, and aadA15. Mutations were also detected in E. coli EF-Tu (elfamycin-resistant EF-Tu). Notably, this region harbors the ESBL gene, blaCTX-M-14.
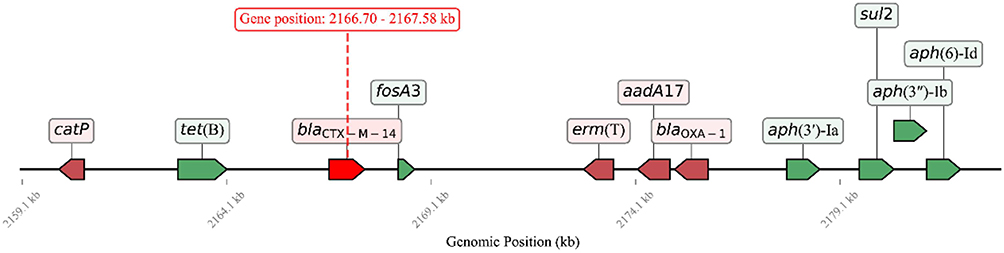 |
Figure 2 Linear alignment of blaCTX-M-14 and its genomic context. |
Discussion
P. multocida is commonly found in the oropharynx and gastrointestinal tract of many animals, particularly cats and dogs, with carriage rates ranging from 70% to 90%.5 Human infections are closely associated with exposure to animals. Rarely, P. multocida bacteremia may develop in patients with underlying liver dysfunction or immunodeficiency following its spread from a localized bite wound, pneumonia, or arthritis.6,16 In the present case, the patient had no history of an animal bite and the definitive route of infection remained obscure. Frequent exposure to domestic animals, however, increases the potential for indirect transmission. Given her advanced age (88 years) and multiple comorbidities (hypertension, cardiovascular disease, cerebral infarction, rheumatism, and anemia), she was likely in a immunologically vulnerable state. Based on these factors and prior reports, we speculate that the patient’s immune status may have predisposed her to P. multocida bloodstream infection. Regrettably, only one set of blood cultures was obtained; nevertheless, considering the clinical presentation, laboratory findings, and the patient’s favorable response to antibiotic therapy, P. multocida was considered the most likely pathogen.
Most P. multocida isolated from animals and humans are generally susceptible to commonly used antibiotics.5 However, P. multocida strains resistant to penicillin, ampicillin, and amoxicillin–clavulanic acid have been reported, albeit infrequently.9,10,17,18 Some resistance phenotypes have been attributed to plasmid-mediated ROB-1 and TEM-1 β-lactamases in P. multocida isolates, theβ-lactamases may originate from drug-resistant strains in animals or human-infected H. influenzae or H. parainfluenzae strains.17,18 In our case, the isolate was non-susceptible to penicillin, ampicillin, amoxicillin–clavulanic acid, and ceftriaxone. ESBL testing indicated a CTX-type ESBL, and WGS confirmed the presence of chromosomally located blaCTX-M-14, which can encode a CTX-M-14 β-lactamase. β-lactam antibiotics remain the most widely used antimicrobial class globally, and β-lactamases are a major resistance mechanism among Gram-negative bacilli.19 CTX-M-type ESBLs are highly prevalent globally, and blaCTX-M-14 is particularly widespread in China.20 CTX-M-type enzymes typically exhibit strong cefotaximase activity—preferentially hydrolyzing cefotaxime/ceftriaxone and some penicillins and narrow-spectrum cephalosporins—but generally have lower activity against the bulkier molecule ceftazidime.21 Consistent with this activity profile, the P. multocida isolate in this report was non-susceptible to ceftriaxone and showed a low MIC for ceftazidime. Although CTX-M enzymes are most often reported in Klebsiella pneumoniae and Escherichia coli, they can also be transferred to other Enterobacterales species, and non-fermenting bacteria.19
The MDR P. multocida isolate in this case was also resistant or non-susceptible to macrolides, fluoroquinolones, and tetracyclines. WGS identified several ARGs, including catP, tetB, tetR, ermT; the tet and erm genes likely explain reduced susceptibility to tetracyclines and macrolides, respectively, whereas catP is associated with chloramphenicol resistance. MDR P. multocida isolates from animals—showing phenotypic resistance to ampicillin, macrolides, aminoglycosides, fluoroquinolones, and/or tetracyclines—have been reported and are thought to result, at least in part, from the routine use of antibiotics in animal feed.11–13,22,23 The increase in MDR microorganisms triggering infections is growing worldwide and becoming more serious in developing countries.24,25 The emergence and dissemination of antibiotic resistance have been driven by inappropriate antibiotic use in humans, animals, and the environment. Although cross-species transmission of antibiotic resistance is relatively uncommon, it is difficult to distinguish whether a zoonotic infectious organism originated from foodborne sources or directly from humans and animals. Antibiotic resistance is therefore a key One Health issue.26
Human P. multocida infections are typically treated with penicillin; for β-lactamase–producing isolates, second- and third-generation cephalosporins, tetracyclines, and fluoroquinolones are commonly recommended.5 Therefore, the isolation of a multidrug-resistant P. multocida in this case poses a significant challenge to existing empirical antimicrobial regimens and underscores the need for routine antimicrobial susceptibility surveillance of P. multocida. Moreover, clinical outcome from one case cannot establish treatment recommendations.
In conclusion, we report a case of P. multocida bacteremia in a patient without a history of animal bites. To the best of our knowledge, based on a comprehensive search of the literature and sequence databases (PubMed, Embase, Medline, Scopus, CNKI, and Wanfang) up to 13 January 2026, this is an infrequent case of a human clinical isolate of P. multocida in which a CTX-M-14 ESBL was identified and confirmed by WGS. The patient was successfully treated with cefoperazone-sulbactam. The limitations of this report include the use of a single set of blood cultures, the lack of source tracking for the resistant isolate, and the interpretive limitations of antimicrobial susceptibility testing for ESBLs in non-Enterobacterales organisms. Although the route of infection and the origin of the resistance gene remain unclear, this case highlights the necessity of routine antibiotic susceptibility testing of P. multocida isolates from humans and livestock. Because animal and human health, food/feed production systems, and the agricultural environment are all directly linked to antibiotic resistance, a multidimensional One Health approach is urgently needed to mitigate this global threat.
Data Sharing Statement
Data supporting the conclusions of this study are included in this published article.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Guangzhou KingMed Diagnostics (the headquarter of Guangxi KingMed Diagnostics) (Approval No. 2025131). Institutional approval for conducting and publishing this case report was obtained from the Guangzhou KingMed Diagnostics (Approval No.KCLWFBSQ-20251020-0006), confirming that the clinical information and patient data could be disclosed in accordance with ethical standards. The studies were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the patient for the publication of any potentially identifiable images or data included in this article.
Acknowledgments
We thank the team of the Infection Diagnosis Center in Guangxi King Med Diagnostics for their contribution.
Funding
This study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors have no competing interests to declare in this work.
References
1. Xiao J, Li Y, Hu Z, et al. Characterization of Pasteurella multocida isolated from ducks in China from 2017 to 2019. Microb Pathog. 2021;160:105196. doi:10.1016/j.micpath.2021.105196
2. Mu H, Yang M, Zhang Y, et al. Pet-related Pasteurella multocida induced peritonitis in peritoneal dialysis: a case report and review of the literatures. BMC Nephrol. 2020;21(1). doi:10.1186/s12882-020-01765-1
3. El-Demerdash AS, Mowafy RE, Fahmy HA, Matter AA, Samir M. Pathognomonic features of Pasteurella multocida isolates among various avian species in Sharkia Governorate, Egypt. World J Microbiol Biotechnol. 2023;39(12):335. doi:10.1007/s11274-023-03774-2
4. Li Y, Xiao J, Cai Q, et al. Whole genome characterization of a multidrug-resistant hypervirulent Pasteurella multocida with a new drug-resistant plasmid. Poult Sci. 2023;102(5):102583. doi:10.1016/j.psj.2023.102583
5. Giordano A, Dincman T, Clyburn BE, Steed LL, Rockey DC. Clinical Features and Outcomes of Pasteurella multocida Infection. Medicine. 2015;94(36):e1285. doi:10.1097/md.0000000000001285
6. Lu B, Feng X, Ye T, et al. Bloodstream infection, peritonitis, and pneumonia caused by Pasteurella multocida in a patient with liver cirrhosis despite no animal contact: case report and literature review. Front Cell Infect Microbiol. 2023;13:1267941. doi:10.3389/fcimb.2023.1267941
7. Ali E, Tytgat N, Vergote L, Devue K, Nonneman B. Elderly and their companion animals, cause for pleasure or for harm, a case report of a non-bite Pasteurella multocida bacteremia in an 85-year-old woman with a fatal outcome. BMC Geriatr. 2023;23(1). doi:10.1186/s12877-023-04224-2
8. Hanson J, Etemady-Deylamy A, Frisby J, et al. Femoral artery aneurysm with large hematoma from Pasteurella: case report and literature review. BMC Infect Dis. 2022;22(1):170. doi:10.1186/s12879-022-07136-5
9. Wei A, Dhaduk N, Taha B. Wrist abscess due to drug-resistant Pasteurella multocida. IDCases. 2021;26:e01277. doi:10.1016/j.idcr.2021.e01277
10. Maritati M, Liverani L, Gigante A, Zanoli GA, De Rito G. The first case of a drug-resistant Pasteurella multocida prosthetic knee infection successfully treated with debridement, antibiotics, and implant retention. Cureus. 2023. doi:10.7759/cureus.38389
11. Saha O, Islam MR, Rahman MS, Hoque MN, Hossain MA, Sultana M. First report from Bangladesh on genetic diversity of multidrug-resistant Pasteurella multocida type B:2 in fowl cholera. Vet World. 2021:2527–7. doi:10.14202/vetworld.2021.2527-2542
12. Serna C, Calderón Bernal JM, Torre-Fuentes L, et al. Integrative and conjugative elements associated with antimicrobial resistance in multidrug resistant Pasteurella multocida isolates from bovine respiratory disease (BRD)-affected animals in Spanish feedlots. Vet Q. 2025;45(1):1–15. doi:10.1080/01652176.2025.2474220
13. Monteiro HF, Hoyos-Jaramillo A, Garzon A, et al. Antibiogram use on dairy cattle for bovine respiratory disease: multidrug resistance in Pasteurella multocida and Mannheimia haemolytica in California dairies. J Dairy Sci. 2025;108(9):10060–10072. doi:10.3168/jds.2025-26708
14. Clinical and Laboratory Standards Institute. Methods for antimicrobial dilution and disk susceptibility testing of infrequently isolated or fastidious bacteria: M45. 2016. Available from: http://www.clsi.org.
15. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing CLSI M100. 2024. Available from: http://www.clsi.org.
16. Al-Ouqaili MTS, Hussein RA, Kanaan BA, Al-Neda ATS. Investigation of carbapenemase-encoding genes in Burkholderia cepacia and Aeromonas sobria isolates from nosocomial infections in Iraqi patients. PLoS One. 2025;20(8):e0315490. doi:10.1371/journal.pone.0315490
17. Rosenau A, Labigne A, Escande F, Courcoux P, Philippon A. Plasmid-mediated ROB-1 beta-lactamase in Pasteurella multocida from a human specimen. Antimicrob Agents Chemother. 1991;35(11):2419–2422. doi:10.1128/AAC.35.11.2419
18. Naas T, Benaoudia F, Lebrun L, Nordmann P. Molecular identification of TEM-1 β-lactamase in a Pasteurella multocida isolate of human origin. Eur J Clin Microbiol Infect Dis. 2001;20(3):210–213. doi:10.1007/PL00011254
19. Cantón R, González-Alba JM, Galán JC, McKay RML, Wilhelm SW. CTX-M enzymes: origin and diffusion. Front Microbiol. 2012;3:3. doi:10.3389/fmicb.2012.00110
20. Yu K, Huang Z, Liu X, et al. The spread of CTX-M-type extended-spectrum beta-lactamases in China: epidemiology and evolutionary analyses. J Infect. 2025;90(4):106457. doi:10.1016/j.jinf.2025.106457
21. Rossolini GM, D’Andrea MM, Mugnaioli C. The spread of CTX-M-type extended-spectrum beta-lactamases. Clin Microbiol Infect off Publ Eur Soc Clin Microbiol Infect Dis. 2008;14 (Suppl 1):33–41. doi:10.1111/j.1469-0691.2007.01867.x
22. Nüesch-Inderbinen M, Treier A, Zurfluh K, Stephan R. Raw meat-based diets for companion animals: a potential source of transmission of pathogenic and antimicrobial-resistant Enterobacteriaceae. R Soc Open Sci. 2019;6(10):191170. doi:10.1098/rsos.191170
23. Bourély C, Cazeau G, Jouy E, et al. Antimicrobial resistance of Pasteurella multocida isolated from diseased food-producing animals and pets. Vet Microbiol. 2019;235:280–284. doi:10.1016/j.vetmic.2019.07.017
24. Hussein RA, AL-Kubaisy SH, Al-Ouqaili MTS. The influence of efflux pump, outer membrane permeability and β-lactamase production on the resistance profile of multi, extensively and pandrug resistant Klebsiella pneumoniae. J Infect Public Health. 2024;17(11):102544. doi:10.1016/j.jiph.2024.102544
25. Al-Ouqaili MTS, Jameel N, Sabri M. The occurrence of CRISPR-encoding genes in extensively drug-resistant Escherichia coli causing urinary tract infection. Al- Anbar Med J. 2025;21(4):223–229. doi:10.33091/amj.2025.158299.2162
26. Aslam B, Khurshid M, Arshad MI, et al. Antibiotic resistance: one health one world outlook. Front Cell Infect Microbiol. 2021;11:771510. doi:10.3389/fcimb.2021.771510
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Molecular and Clinical Characteristics of Carbapenem-Resistant Klebsiella pneumoniae Isolates at a Tertiary Hospital in Wuhan, China
Hu F, Lin ML, Mou JL, Feng JH, Huang K, Lao YJ, Cheng J, Lin J
Infection and Drug Resistance 2023, 16:65-76
Published Date: 5 January 2023
Genomic and Phylogenetic Analysis of a Multidrug-Resistant blaNDM-carrying Klebsiella michiganensis in China
Jiang T, Li G, Huang L, Ding D, Ruan Z, Yan J
Infection and Drug Resistance 2023, 16:3109-3116
Published Date: 18 May 2023