Back to Journals » Journal of Asthma and Allergy » Volume 17
Elevated Saliva Pepsin Concentration as a Risk Factor for Asthma in Children with Allergic Rhinitis: A Preliminary Study
Authors Sui H, Shen H, Zhang C, Wang M, Zhen Z, Zhang J ![]()
Received 30 October 2023
Accepted for publication 8 April 2024
Published 22 April 2024 Volume 2024:17 Pages 391—397
DOI https://doi.org/10.2147/JAA.S447145
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Haijing Sui,1,* Hong Shen,1,* Chi Zhang,1 Minghui Wang,1 Zhen Zhen,1 Junbo Zhang2
1Department of Otolaryngology, Head and Neck Surgery, Peking University First Hospital, Beijing, People’s Republic of China; 2Department of Otolaryngology, Head and Neck Surgery, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Junbo Zhang, Department of Otolaryngology, Head and Neck Surgery, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, Beijing, People’s Republic of China, Email [email protected] Zhen Zhen, Department of Otolaryngology, Head and Neck Surgery, Peking University First Hospital, Beijing, People’s Republic of China, Email [email protected]
Objective: This study aimed to explore whether saliva pepsin concentration (SPC) could be regarded as a risk factor for the occurrence and unfavorable control of asthma in children with allergic rhinitis.
Methods: A prospective study was conducted on a group of 20 consecutive children newly diagnosed with allergic rhinitis and asthma (referred to as the asthma group). All these children underwent fractional exhaled nitric oxide (FeNO) measurement, lung function tests, and assessment of asthma control using the 7-item Childhood Asthma Control Test (C-ACT) score. Simultaneously, a control group consisting of 20 children with simple allergic rhinitis, matched for baseline characteristics, was included. SPC measurement was performed in the two groups.
Results: The SPC value was significantly higher in the asthma group than that in the control group (165.0 ± 82.8 ng/mL vs 68.4 ± 34.5 ng/mL) (P < 0.001). In the asthma group, SPC was independently associated with FeNO, the ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC), and forced expiratory flow at 50% and 75% of FVC (FEF50 and FEF75) (all P < 0.05). The severity of nasal symptoms evaluated by the visual analogue scale (N-VAS) was independently associated with FEF75, the maximal mid-expiratory flow (MMEF), and C-ACT score (P < 0.05).
Conclusion: Direct pepsin exposure and uncontrolled nasal symptoms may play crucial roles in the pathogenesis and progression of childhood allergic asthma. The SPC value can be considered as a risk factor for asthma in children with allergic rhinitis.
Keywords: saliva pepsin concentration, asthma, allergic rhinitis, gastroesophageal reflux disease
Introduction
Asthma stands as the prevailing chronic respiratory condition among children globally, impacting approximately 14% of youth and adolescents.1 Poor asthma control is associated with a number of negative effects on children and their families, including reduced quality of life, increased economic costs, and even the risk of death caused by severe attacks.
Gastroesophageal reflux disease (GERD) has been considered as a risk factor for asthma and a trigger for asthma attacks in children.1–3 It has been estimated to be present in 40–80% of children with asthma.4 Nevertheless, the precise pathophysiological mechanism by which GERD exacerbates asthma remains elusive. However, certain drugs routinely used for GERD may have the potential to enhance lung volumes in respiratory function tests and alleviate asthma symptoms. This improvement contributes to a more effective subjective control of asthma.3 Notably, pepsin, consistently found in all refluxate, may be a significant contributor, distinguishing itself from other gastric components, such as bile acids. In vitro experiments suggested that pepsin exposure disrupts respiratory epithelium and causes direct contact between submucosal tissue and allergens and pathogens.5 Thus, pepsin concentration in upper respiratory secretions could be theoretically an indicator of asthma risk. To our knowledge, no study has yet assessed the role of pepsin concentration in pediatric asthma risk.
Utilizing the Peptest device, a commercially available immune-serologic test facilitating precise measurement of saliva pepsin concentration (SPC), the present study aimed to assess the involvement of pepsin in the pathogenesis and management of childhood asthma.
Methods
Study Subjects
Between August 2022 and September 2022, data of a total of 20 consecutive children who aged 6–12 years old with newly diagnosed allergic rhinitis and asthma at Peking University First Hospital (Beijing, China) were prospectively analyzed (asthma group). The diagnosis of allergic asthma was performed according to the following criteria: (1) typical clinical symptoms, such as cough, wheezing, shortness of breath, exercise intolerance, and reversibility to bronchodilators and/or positive response to bronchial methacholine challenge;6 (2) detection of positive results for at least one allergen through either allergen skin prick or serum immunoglobulin E (IgE) test; and (3) exposure to specific allergens (mainly dust mites, pollen, mold, and animal fur) could trigger or exacerbate the abovementioned symptoms. Children who had other chronic lung diseases or acute respiratory infections over the past four weeks were excluded. During the same period, another group of 20 children with simple allergic rhinitis matched for sex, age, body mass index (BMI), and the severity of nasal symptoms evaluated by visual analogue scale (N-VAS) were included as control group (Table 1). None of children in the control group had experienced any of the abovementioned asthma-related symptoms even under the exposure to specific allergens.
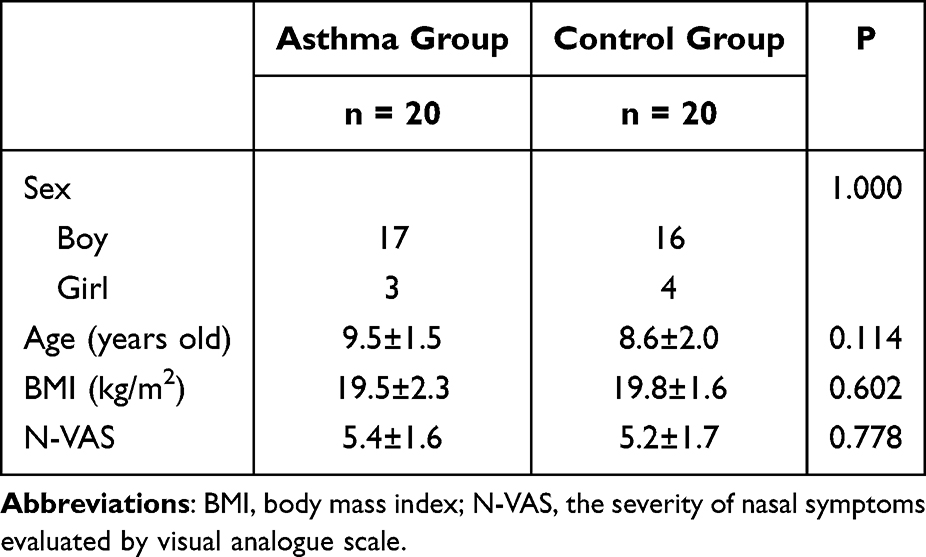 |
Table 1 The Comparison of Baseline Information Between Asthma and Control Groups |
SPC was measured in both groups of children. In addition, fractional exhaled nitric oxide (FeNO) measurement, lung function tests, and subjective assessment of asthma control were performed for all children in the asthma group on the day of saliva collection. This study was performed followed the principle of the Declaration of Helsinki and the study protocol was approved by the Ethics Committee of Peking University First Hospital (Approval No. 2021–250), and all children’s caregivers had signed informed consent forms.
Measurement of SPC
All saliva samples from children were collected in the morning upon waking and standing, prior to having breakfast or brushing their teeth. The children’s caregivers were instructed to collect saliva into a tube containing 0.5 mL of 0.01 M citric acid. The samples were refrigerated at 4 °C, and the SPC was evaluated using the Peptest device (RD Biomed Ltd., London, UK) according to the standardized procedure that has been previously described.7,8 The result was considered to be valid when a blue line appeared under the letter C (control) of the Peptest device at 15 min after applying the sample. The apparition of a blue line under the letter T (test) was indicative of a positive result. The SPC was also accurately measured using the PEP-test Cube, which is an electronic lateral flow device that can detect pepsin down to 16 ng/mL. The test was considered positive when the pepsin level reached ≥16 ng/mL.
FeNO, Lung Function Test, and Assessment of Asthma Control
FeNO measurement (NIOX MINO device, Circassia, Stockholm, Sweden) was conducted according to the ATS guidelines.9 Lung function test was performed using spirometry (Spirolab II, Medical International Research, Rome, Italy) as described previously.10 The ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) (FEV1/FVC), forced expiratory flow at 50% and 75% of FVC (FEF50 and FEF75), and the maximal mid-expiratory flow (MMEF) were recorded and used in the analyses. The subjective asthma control was evaluated by the 7-item Childhood Asthma Control Test (C-ACT).11,12 The Chinese version of this questionnaire has been validated in previous research.13 Asthma was regarded controlled if the C-ACT score was greater than 19 points and classified as uncontrolled if it was 19 points or lower.
Statistical Analysis
The statistical analysis was carried out using SPSS 20.0 software (IBM, Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation. The unpaired Student’s t-test was utilized to compare continuous variables between two groups. The Fisher’s exact test was used to compare categorical data between two groups. The Pearson correlation test was employed to identify significant associations. The linear regression analysis was used to identify independent significant associations. P <0.05 was considered statistically significant.
Results
As illustrated in Figure 1, the overall SPC in the asthma group was 165.0 ± 82.8 (range, 25.0–301.2) ng/mL, which was significantly higher than that in the control group (68.4 ± 34.5 ng/mL; range, 16.5–150.6 ng/mL) (P < 0.001). According to the definition of pathological pepsin level of ≥75 ng/mL,14 the proportion of children with proximal reflux in the asthma group was 90% (18/20), which was also significantly higher than that in the control group (45% (9/20)) (P = 0.006).
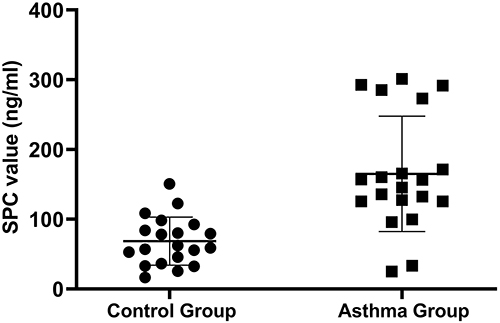 |
Figure 1 The comparison of SPC values between the asthma group and the control group. |
The FeNO values, lung function test results, and the C-ACT scores of 20 children in the asthma group and their correlations with SPC values are presented in Table 2. It was revealed that the SPC was significantly correlated with FeNO, FEV1/FVC, FEF50, FEF75, MMEF, and C-ACT score (all P < 0.05).
 |
Table 2 FeNO Values, Lung Function Test Results, and C-ACT Scores of 20 Children in the Asthma Group and Their Correlations with SPC Values |
Linear regression analysis, involving sex, age, BMI, N-VAS, and SPC to predict the abovementioned parameters, was conducted. The independent factors associated with the outcomes are presented in Table 3, revealing that SPC was the sole parameter independently correlated with FeNO, FEV1/FVC, and FEF50 (all P < 0.05). SPC and N-VAS were both independently associated with FEF75 and MMEF (all P < 0.05), while N-VAS was the only parameter that was independently associated with C-ACT score (P < 0.05).
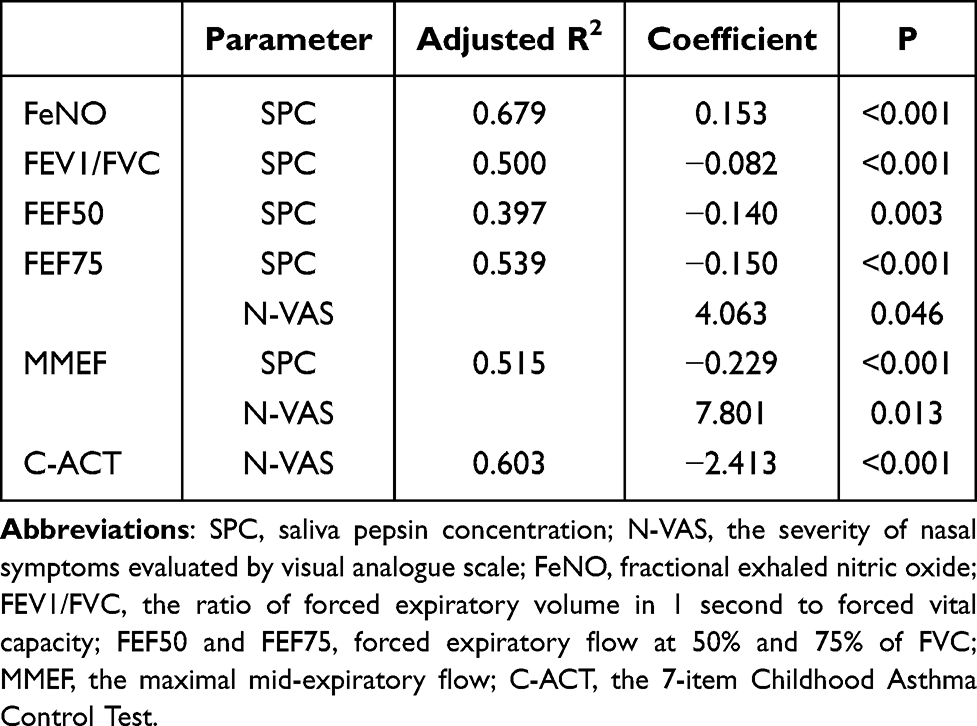 |
Table 3 Factors Independently Associated with FeNO Value, Lung Function Test Results, and C-ACT Score |
Discussion
GERD has been considered as a possible risk factor for childhood asthma.1,2 However, the mechanisms were not fully explored; some attributed it to the direct noxious effects of gastric contents in the tracheobronchial tree, while others demonstrated that reflux into the esophagus might activate a neural reflex arc through the vagus nerve, indirectly leading to asthma-related symptoms. Additionally, a preliminary clinical study has suggested the coexistence of both mechanisms.3 The findings of the present study could provide robust evidence supporting the first mechanism, given that pepsin A is an enzyme exclusively produced by gastric chief cells. Its presence in upper airway secretions may be considered as a marker of reflux.15 This was consistent with the results of an in vitro experiment, which indicated that refluxate exposure could lead to bronchial epithelial damage, barrier leakiness, and/or neutrophil breach of the epithelium, highlighting the crucial role of pepsin in exacerbating asthma.5
The aforementioned results also indicated the significance of proximal reflux, also known as laryngopharyngeal reflux (LPR), in exacerbating asthma. LPR is characterized by the reflux of gastric acid and refluxate (containing pepsin) above the upper esophageal sphincter.16 Despite being considered as an extension of GERD, it frequently manifests without typical GERD symptoms, such as heartburn and regurgitation, posing a challenge for clinicians in making accurate diagnosis and determining an appropriate treatment.17 Therefore, a portable and non-invasive test is essential to confirm the possibility of reflux and provide evidence for further treatment, including SPC measurement.
Another important finding of the current study was that the SPC value was independently associated with FeNO value and all lung function test variables in the asthma group, and it was significantly correlated with C-ACT score. FeNO represents type 2 airway inflammation, which is closely associated with the occurrence and progression of asthma.18 FEV1 and FEV1/FVC mainly reflect large airway function, while FEF50, FEF75, and MMEF are traditional indices used to assess peripheral airway obstruction.19 Therefore, pepsin exposure may exacerbate asthma by inducing airway inflammation and decreasing the patency of both small and large airways.
In the asthma group, a higher N-VAS score was also found to be independently associated with unfavorable pulmonary function and unsatisfactory asthma control. Similarly, Ohta et al reported a close relationship between severe rhinitis and asthma exacerbation.20 Explaining this is not challenging, given the strong correlation between asthma and allergic rhinitis. They share common allergens and inflammatory processes.21,22 The clinical significance of this finding emphasizes the importance of controlling rhinitis symptoms.
This study has certain limitations that should be pointed out. Firstly, the sample size was limited, although meaningful results were still obtained. Secondly, the absence of a normal control group comprising children without allergic rhinitis and asthma could enhance the reliability of the results; however, this is planned for the future research. Thirdly, the results lack additional verification, and a study exploring the impact of anti-reflux therapy on the aforementioned parameters could strengthen the conclusions. Additionally, the detection of SPC alone has limitations in diagnosing GERD, as physiological reflux may also lead to pepsin presence in upper airway secretions. On the other hand, GERD with mainly non-acid reflux may also showed a negative result of SPC test. Combining it with the gold standard method for diagnosing GERD in children, dual-probe esophageal 24-h pH monitoring23 might yield more meaningful results, while this test is invasive and may pose ethical limitations in this study. Lastly, the symptoms of asthma itself, such as cough, may potentially exacerbate GERD, introducing a correlation that cannot be ruled out and acting as a potential confounder.
In conclusion, it was found that the SPC was significantly higher in children with allergic rhinitis and asthma than that in children with simple allergic rhinitis. Moreover, a high SPC value was closely correlated with the increased airway inflammation, unfavorable pulmonary function, and more importantly, poor asthma control. The abovementioned findings indicated a significant role of direct pepsin exposure in the pathogenesis and progression of childhood allergic asthma. Furthermore, it was revealed that the SPC value could be regarded as a potential risk factor for asthma in children with allergic rhinitis.
Abbreviations
GERD, gastroesophageal reflux disease; SPC, saliva pepsin concentration; BMI, body mass index; N-VAS, the severity of nasal symptoms evaluated by visual analogue scale; FeNO, fractional exhaled nitric oxide; FEV1/FVC, the ratio of forced expiratory volume in 1s to forced vital capacity; FEF50 and FEF75, forced expiratory flow at 50% and 75% of FVC; MMEF, the maximal mid-expiratory flow; C-ACT, the 7-item Childhood Asthma Control Test; LPR, laryngopharyngeal reflux.
Data Sharing Statement
The data underlying this article will be shared upon reasonable request to the corresponding author.
Ethics Statement
The study protocol had been proved by the Ethics Committee of Peking University First Hospital with an ID of 2021-250, and all the children’s caregivers had provided signed informed consents. No patient-identifying information was accessible during the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National High Level Hospital Clinical Research Funding (Youth clinical research project of Peking University First Hospital) (No. 2022CR103), the Beijing Municipal Natural Science Foundation (No. 7204315), and the Youth clinical research project of Peking University First Hospital (No. 2019CR30).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest and report no conflicts of interest for this work.
References
1. Martin J, Townshend J, Brodlie M. Diagnosis and management of asthma in children. BMJ Paediatrics Open. 2022;6(1):e001277. doi:10.1136/bmjpo-2021-001277
2. National Asthma E, Prevention P. Expert Panel Report 3 (EPR-3): guidelines for the diagnosis and management of asthma-summary report 2007. J Allergy Clin Immunol. 2007;120(5 Suppl):S94–138.
3. Scaramozzino MU, Festa M, Levi G, Plastina UR, Sapone G Correlation between gastro-oesophageal reflux disease (GERD) lung volumes and exacerbation of bronchial asthma: Italian pilot observational retrospective study GERDAS. Monaldi archives for chest disease = Archivio monaldi per le malattie del torace; 2023.
4. Thakkar K, Boatright RO, Gilger MA, El-Serag HB. Gastroesophageal reflux and asthma in children: a systematic review. Pediatrics. 2010;125(4):e925–930. doi:10.1542/peds.2009-2382
5. Perotin JM, Wheway G, Tariq K, et al. Vulnerability to acid reflux of the airway epithelium in severe asthma. Eur Respir J. 2022;60(2):2101634. doi:10.1183/13993003.01634-2021
6. Bateman ED, Hurd SS, Barnes PJ. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008;31(1):143–178. doi:10.1183/09031936.00138707
7. Bobin F, Journe F, Lechien JR. Saliva pepsin level of laryngopharyngeal reflux patients is not correlated with reflux episodes. Laryngoscope. 2020;130(5):1278–1281. doi:10.1002/lary.28260
8. Hayat JO, Gabieta-Somnez S, Yazaki E, et al. Pepsin in saliva for the diagnosis of gastro-oesophageal reflux disease. Gut. 2015;64(3):373–380. doi:10.1136/gutjnl-2014-307049
9. Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602–615. doi:10.1164/rccm.9120-11ST
10. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338.
11. Leung TF, Ko FW, Sy HY, et al. Identifying uncontrolled asthma in young children: clinical scores or objective variables? J Asthma. 2009;46(2):130–135. doi:10.1080/02770900802468533
12. Liu AH, Zeiger R, Sorkness C, et al. Development and cross-sectional validation of the childhood asthma control test. J Allergy Clin Immunol. 2007;119(4):817–825. doi:10.1016/j.jaci.2006.12.662
13. Zhou X, Ding FM, Lin JT, Yin KS. Validity of asthma control test for asthma control assessment in Chinese primary care settings. Chest. 2009;135(4):904–910. doi:10.1378/chest.08-0967
14. Zhang M, Chia C, Stanley C, Phyland DJ, Paddle PM. Diagnostic utility of salivary pepsin as compared with 24-hour dual pH/impedance probe in laryngopharyngeal reflux. Otolaryngol Head Neck Surg. 2021;164(2):375–380. doi:10.1177/0194599820951183
15. Wang J, Zhao Y, Ren J, Xu Y. Pepsin in saliva as a diagnostic biomarker in laryngopharyngeal reflux: a meta-analysis. Eur Arch Otorhinolaryngol. 2018;275(3):671–678. doi:10.1007/s00405-017-4845-8
16. Xiao S, Li J, Zheng H, et al. An epidemiological survey of laryngopharyngeal reflux disease at the otorhinolaryngology-head and neck surgery clinics in China. Eur Arch Otorhinolaryngol. 2020;277(10):2829–2838. doi:10.1007/s00405-020-06045-0
17. Sidhwa F, Moore A, Alligood E, Fisichella PM. Diagnosis and treatment of the extraesophageal manifestations of gastroesophageal reflux disease. Ann Surg. 2017;265(1):63–67. doi:10.1097/SLA.0000000000001907
18. Rupani H, Kent BD. Using fractional exhaled nitric oxide measurement in clinical asthma management. Chest. 2022;161(4):906–917. doi:10.1016/j.chest.2021.10.015
19. Koefoed HJL, Zwitserloot AM, Vonk JM, Koppelman GH. Asthma, bronchial hyperresponsiveness, allergy and lung function development until early adulthood: a systematic literature review. Pediatric Allergy and Immunology. 2021;32(6):1238–1254. doi:10.1111/pai.13516
20. Ohta K, Tanaka H, Tohda Y, et al. Asthma exacerbations in patients with asthma and rhinitis: factors associated with asthma exacerbation and its effect on QOL in patients with asthma and rhinitis. Allergology. 2019;68(4):470–477. doi:10.1016/j.alit.2019.04.008
21. Greiner AN, Hellings PW, Rotiroti G, Scadding GK. Allergic rhinitis. Lancet. 2011;378(9809):2112–2122. doi:10.1016/S0140-6736(11)60130-X
22. Togias A. Rhinitis and asthma: evidence for respiratory system integration. J Allergy Clin Immunol. 2003;111(6):1171–1183. [quiz 1184]. doi:10.1067/mai.2003.1592
23. Wlodarczyk E, Jetka T, Raj-Koziak D, et al. Diagnosis of laryngopharyngeal reflux in children with voice disorders using 24-hour pharyngeal pH monitoring. Int J Pediatr Otorhinolaryngol. 2019;121:188–196. doi:10.1016/j.ijporl.2019.03.010
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Specific IgE Response and Omalizumab Responsiveness in Severe Allergic Asthma
Tajiri T, Suzuki M, Kutsuna T, Nishiyama H, Ito K, Takeda N, Fukumitsu K, Kanemitsu Y, Fukuda S, Umemura T, Ohkubo H, Maeno K, Ito Y, Oguri T, Takemura M, Yoshikawa K, Niimi A
Journal of Asthma and Allergy 2023, 16:149-157
Published Date: 22 January 2023
Association of Mite Molecular Sensitization Profiles with Respiratory Allergies and Asthma Control in Children from East China
He J, Lin N, Jin T, Lin M, Huang Z, Li S, Liu J, Su L, Ye X, Wu L, Song Z, Xu H, Chen Z
Journal of Asthma and Allergy 2024, 17:965-975
Published Date: 7 October 2024
Knowledge Mapping of COVID-19 and Asthma/Allergic Rhinitis: A Visual and Bibliometric Analysis
Chen Y, Song C, Wang J, Cao Y, Lu Y, Han X
Journal of Asthma and Allergy 2025, 18:705-721
Published Date: 6 May 2025
Dupilumab is Effective in Young Children with Atopic Dermatitis Regardless of Type 2 Comorbidities
Boguniewicz M, Sher LD, Paller AS, Arkwright PD, Yoshihara S, Smith Begolka W, Chen Z, Shah P, Rodríguez Marco A
Journal of Asthma and Allergy 2026, 19:590176
Published Date: 19 May 2026
Allergen Sensitization Profiles and Co-Sensitization Networks in Children with Allergic Rhinitis and Asthma: A Propensity Score-Matched Retrospective Study
Zou P, Fan Y, Xie C, Xia W, Liu Y, Tao P, Huang Y, Wang L, Ai T
Journal of Asthma and Allergy 2026, 19:620785
Published Date: 17 June 2026