Back to Journals » Vascular Health and Risk Management » Volume 22
Elevated Hydrocarbon Exposure Escalates Coronary and Cerebrovascular Disease Risks: A Comprehensive Systematic Review
Authors Sulthana H ![]() , Kasoj M, Kumar S, Jan A
, Kasoj M, Kumar S, Jan A ![]() , Dubwa D
, Dubwa D
Received 8 March 2026
Accepted for publication 5 July 2026
Published 10 July 2026 Volume 2026:22 607849
DOI https://doi.org/10.2147/VHRM.S607849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Akash Batta
Huma Sulthana,1 Manasa Kasoj,2 Shubham Kumar,3,4 Asif Jan,5– 7 Daniel Dubwa8
1Department of Pharmaceutical Chemistry, Faculty of Pharmacy, MS Ramaiah University of Applied Sciences, Bangalore, India; 2Kalam Institute of Health Technology, Visakhapatnam, Andhra Pradesh, India; 3Dental Research Cell, Dr. D. Y. Patil Dental College & Hospital, Dr. D. Y. Patil Vidyapeeth (Deemed to be University), Pune, India; 4Global Research Cell, Dr. D. Y. Patil Medical College Hospital and Research Centre, Dr. D. Y. Patil Vidyapeeth, (Deemed to be University), Pune, India; 5Department of Pharmacy, University of Peshawar, Peshawar, Khyber Pakhtunkhwa, Pakistan; 6Saidu Group of Teaching Hospitals, Saidu Sharif Swat, Khyber Pakhtunkhwa, Pakistan; 7District Headquarter Hospital Charsadda, Charsadda, Khyber Pakhtunkhwa, Pakistan; 8Department of Pharmacy Practice, Makerere University, Kampala, Uganda
Correspondence: Asif Jan, Department of Pharmacy, University of Peshawar, Peshawar, Khyber Pakhtunkhwa, Pakistan, Tel +92-3015940602, Email [email protected] Daniel Dubwa, Department of Pharmacy, Makerere University, P.O. Box 7072, Kampala, Uganda, Email [email protected]
Abstract: Exposure to hydrocarbons, including polycyclic aromatic hydrocarbons (PAHs) and volatile organic compounds (VOCs), represents an escalating public health concern. These compounds induce systemic inflammation, oxidative stress, and endothelial dysfunction, driving cardiovascular disease (CVD) pathogenesis. This systematic review evaluates the association between hydrocarbon exposure and CVD risk, focusing on specific metabolite biomarkers. A comprehensive search of PubMed, Embase, and Web of Science was conducted up to June 10, 2025. Observational studies evaluating correlations between hydrocarbon exposure and CVD outcomes—including coronary heart disease (CHD), stroke, and myocardial infarction (MI)—were selected for narrative synthesis. Eleven studies met the inclusion criteria. Included studies were of moderate to high quality with a low overall risk of bias. The PAH metabolites 1-hydroxynaphthalene (6 studies), 2-hydroxynaphthalene (7 studies), 2-hydroxyfluorene (6 studies), 3-hydroxyfluorene (5 studies), and 1-hydroxypyrene (5 studies) were consistently associated with elevated risks of CHD, stroke, and MI. Similarly, exposure to BTEX components (benzene, toluene, ethylbenzene, and xylene) evaluated in one study significantly correlated with heightened CVD incidence. These associations appeared more pronounced in highly exposed populations, particularly occupational cohorts, although effect sizes varied across studies because of study design differences and residual confounding factors such as smoking. Overall, the available evidence suggests an association between hydrocarbon exposure and increased CVD risk. Further prospective longitudinal studies are needed to confirm these findings and clarify the underlying toxicological mechanisms.
Keywords: cardiovascular diseases, polycyclic aromatic hydrocarbons, volatile organic compounds, oxidative stress
Introduction
Cardiovascular diseases (CVDs) represent the leading cause of global mortality, claiming an estimated 17.9 to 19.8 million lives annually, which accounts for approximately 32% of all deaths worldwide. These conditions include coronary artery disease, stroke, angina, myocardial infarction, and heart failure. The vast majority of these fatalities—nearly 85%—are caused by myocardial infarctions and strokes driven by systemic atherosclerosis. While preventable through the mitigation of behavioral risks such as tobacco use, poor diet, and physical inactivity, CVDs inflict a disproportionate burden on low- and middle-income countries, where over 75% of these deaths occur due to limited healthcare infrastructure and delayed clinical interventions,1,2 significantly impacting quality of life while placing an estimated economic burden of over $1 trillion annually on healthcare systems.3 CVDs arise from a combination of genetic, behavioral, and environmental factors.4,5 While traditional risk factors like smoking, hypertension, hyperlipidemia, diabetes, and sedentary lifestyles are well established,6,7 emerging evidence suggests that environmental exposures, such as air pollution and occupational hazards, may also play a critical role in cardiovascular health.8,9
Hydrocarbons, a diverse group of organic compounds composed of hydrogen and carbon, are widespread environmental pollutants primarily derived from fossil fuels such as petroleum, coal, and natural gas.10 They are broadly categorized into aromatic and aliphatic groups, with polycyclic aromatic hydrocarbons (PAHs) being a particularly concerning subclass of aromatic hydrocarbons.11 PAHs are generated during the incomplete combustion of organic materials, including vehicle exhaust, industrial emissions, tobacco smoke, and residential heating.12 These compounds, along with volatile organic compounds (VOCs), are pervasive in the environment and accounts for significant risks to human health. Hydrocarbons are commonly encountered through occupational exposure in industries such as petrochemicals and through ambient air pollution, making them a critical area of focus in environmental and public health research due to their widespread presence and potential to disrupt vital biological functions.13–16
In recent years, research has increasingly highlighted the potential cardiovascular effects of hydrocarbons. Evidence suggests that exposure to hydrocarbons, such as PAHs and volatile organic compounds, may elevate cardiovascular risks through mechanisms like systemic inflammation, oxidative stress, and endothelial dysfunction.17 PAHs and VOCs can penetrate the respiratory system and enter systemic circulation, where they stimulate the generation of reactive oxygen species (ROS), leading to oxidative stress and cellular injury. Excessive ROS production damages lipids, proteins, and DNA, promotes lipid peroxidation, and impairs antioxidant defense systems.18,19 In addition, hydrocarbons activate inflammatory signaling pathways, including nuclear factor-kappa B (NF-κB) and pro-inflammatory cytokines such as interleukin-6 and tumor necrosis factor-alpha, resulting in chronic low-grade systemic inflammation.20 These inflammatory and oxidative processes contribute to endothelial dysfunction by reducing nitric oxide bioavailability, impairing vascular relaxation, increasing vascular permeability, and promoting leukocyte adhesion to vascular walls. Persistent endothelial injury further accelerates atherosclerotic plaque formation, thrombogenesis, vascular stiffness, and dysregulation of lipid metabolism, thereby increasing the risk of coronary artery disease, myocardial infarction, stroke, and other cardiovascular complications.
Studies have reported a higher prevalence of cardiovascular conditions, including myocardial infarction, arrhythmias, and cardiovascular mortality, in populations exposed to hydrocarbons through occupational settings and environmental pollution.21,22 However, the specific role of hydrocarbon exposure in cardiovascular diseases remains inconclusive due to inconsistent and limited findings across studies.
Several mechanisms have been proposed to explain the link between hydrocarbon exposure and CVDs. Hydrocarbons, particularly PAHs, induce oxidative stress by generating reactive oxygen species (ROS), which damage DNA, proteins, and lipids.23 This oxidative stress, combined with inflammation, contributes to endothelial dysfunction, a critical factor in atherosclerosis the buildup of fatty plaques in arteries that underlies coronary artery disease and stroke.24 Hydrocarbons can also disrupt lipid metabolism, leading to dyslipidemia, enhance thrombogenesis, and impair vascular homeostasis by reducing nitric oxide production, essential for vascular health.21 Chronic exposure, whether through occupational environments or ambient air pollution, exacerbates these effects, increasing the risk of cardiovascular conditions over time.
Studies exploring the link between hydrocarbon exposure and CVD have shown mixed results. Some research reports a strong connection, with increased risks of conditions like coronary artery disease, stroke, and heart failure, particularly among people exposed to air pollution with hydrocarbons or those in petrochemical industries.15,25,26 Prolonged or high-level exposure is often linked to higher rates of heart attacks and markers of inflammation and oxidative stress. However, other studies report weaker or no significant associations,27,28 possibly due to differences in study design, populations, and exposure measurement methods. Confounding factors like smoking or other pollutants and reliance on indirect measures such as air quality data or proximity to industrial sites may also influence findings. These inconsistencies call for a systematic review to clarify the relationship, identify at-risk groups, and guide strategies to reduce CVD risks from hydrocarbon exposure.
Although previous reviews have broadly examined the cardiovascular effects of environmental pollutants and air pollution, limited attention has been given specifically to individual hydrocarbon metabolites and their differential associations with cardiovascular outcomes. To our knowledge, this is among the first systematic reviews to comprehensively evaluate specific PAH metabolites, including hydroxynaphthalene, hydroxyfluorene, hydroxyphenanthrene, and hydroxypyrene, as well as BTEX compounds, in relation to coronary heart disease, stroke, myocardial infarction, and ASCVD risk. By focusing on metabolite-specific cardiovascular associations, this review provides a more detailed understanding of the potential toxicological and clinical significance of hydrocarbon exposure.
This systematic review aimed to evaluate the association between hydrocarbon exposure and cardiovascular diseases, clarifying the relationship and identifying at risk populations. By synthesizing existing evidence, it seeks to inform public health strategies and support policies to reduce exposure to harmful pollutants, contributing to a better understanding of environmental impacts on cardiovascular health. With the prevalence of CVDs continuing to rise, particularly in low- and middle-income countries where 75% of cases occur,29 there is an urgent need to explore these lesser-known contributors to better address this growing public health challenge.8,9
Methods
Study Design
This systematic review was designed to gather and evaluate existing research on the relationship between hydrocarbon exposure and the risk of CVDs. The review process was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines30 (Table S1).
Data Sources and Search Strategy
A thorough search was carried out using several electronic databases, including Embase, Web of Science, and PubMed, to locate studies published up to June 10, 2025, that were relevant to the topic. The search process involved a combination of free text keywords such as (“polycyclic aromatic hydrocarbons” OR “PAHs” OR “polynuclear aromatic hydrocarbons” OR “aromatic hydrocarbons” OR “polycyclic hydrocarbons” OR “mono-hydroxylated PAHs” OR “1-hydroxynaphthalene” OR “1-hydroxypyrene”) AND (“cardiovascular risk” OR “cardiovascular disease” OR “myocardial infarction” OR “coronary artery disease” OR “stroke” OR “heart failure” OR “atherosclerosis” OR “arrhythmia”). Boolean operators (AND, OR) were used to combine the search terms to ensure a comprehensive and systematic approach. No limitations were applied regarding language or type of publication to include a broad spectrum of studies. The entire search approach is detailed in Table S2.
Eligibility Criteria
The selection of studies was based on specific inclusion and exclusion criteria. Included studies were: (1) observational research (such as cohort, case-control, or cross-sectional studies) that explored the relationship between exposure to hydrocarbons (including PAHs, VOCSs, or other forms of hydrocarbons) and CVDs including heart failure, coronary heart disease, angina, heart attack, and stroke; (2) studies that provided quantitative measures of risk, such as odds ratios (OR), risk ratios (RR), hazard ratios (HR), or sufficient data to calculate these values; (3) peer-reviewed articles. The primary focus was on hydrocarbon exposure, while the outcome of interest was the occurrence of cardiovascular diseases, including but not limited to heart attack, coronary artery disease, stroke, heart failure, and arrhythmias. Both occupational and environmental exposure types were considered. No restrictions were placed on language or article type. Eligible studies included those assessing any form of hydrocarbon exposure, whether through occupational settings (eg, industries involving petrochemicals) or through environmental pollutants (eg, air quality). Excluded studies consisted of case reports, conference proceedings, opinion articles, and review papers.
Study Selection
The titles and abstracts of all studies identified through the search strategy were independently reviewed by two researchers to determine their eligibility based on the predefined criteria. Full-text articles of studies deemed potentially relevant were then retrieved and evaluated by the same two reviewers to make a final decision on inclusion. Conflicts between the reviewers were settled by discussion when they occurred, and a third reviewer was approached for arbitration if an agreement could not be reached.
To improve the efficiency and accuracy of the study selection process, semi-automated software (eg, Nested-Knowledge, MN, USA) was employed to eliminate duplicate records and facilitate the initial screening phase. This approach ensured a systematic and thorough review of all relevant studies.
Data Extraction and Quality Assessment
To ensure accuracy and consistency throughout the process, two reviewers separately retrieved the data from the relevant studies using a standardized form. Study parameters including the country of origin, publication year, first author, study location, total sample size, and study design type were among the important data that was retrieved. Population details focused on the age distribution. The exposure data covered the classification and specifics of hydrocarbon exposure, while the outcomes related to CVDs were recorded. Together with their matching 95% CIs and adjusted variables, statistical metrics such as OR, HR, or RR were also retrieved. Any disputes that arose throughout the data extraction process were settled by discussion, and if required, a third reviewer was engaged. Effective data extraction was made possible via the Nested-Knowledge platform’s “tagging” capability.
Two reviewers independently assessed the included studies’ methodological quality using the Newcastle-Ottawa Scale (NOS) (Table S3). The selection of participants, the comparability of research groups, and the calculation of exposure and results were the criteria used to evaluate each study. For cohort studies, NOS scores of 7–9 were considered high quality, 4–6 moderate quality, and ≤3 low quality. For cross-sectional studies adapted from the NOS, scores of 5–6 were considered high quality, 3–4 moderate quality, and ≤2 low quality.
Data Synthesis and Statistical Analysis
The data synthesis for this systematic review was primarily quantitative, focusing on summarizing OR and other effect estimates across studies. Although pooling of OR for a meta-analysis was not feasible due to variations in study designs, exposure classifications, and outcome measures, the review aimed to identify significant patterns and trends in the relationship between hydrocarbon exposure and CVDs. The synthesis process involved comparing the OR and associated CI across studies, highlighting variations in effect estimates, and identifying common factors influencing these associations. Key quantitative data, such as OR were tabulated to facilitate direct comparisons between studies and to emphasize overarching trends in the literature regarding the cardiovascular risks associated with hydrocarbon exposure. As a quantitative meta-analysis was not performed because of substantial heterogeneity in study designs, exposure assessments, and outcome measures, formal assessment of publication bias was not feasible.
Results
Literature Search
Database searches turned up 2240 entries in all, including 1041 from Embase, 411 from PubMed, and 788 from Web of Science. There were 1366 distinct records left for screening after 874 duplicate entries were eliminated. Of these, 1298 were excluded based on their titles and abstracts as they did not meet the inclusion criteria, leaving 68 full-text articles for detailed evaluation. After thorough assessment, 59 publications were excluded due to reasons such as case reports,4 review articles,7 irrelevant studies,21 and failure to address the outcomes of interest.15 Additionally, 2 records identified through other sources were reviewed but excluded. Ultimately, 11 studies31–40 were included in the systematic review, focusing on the association between and cardiovascular diseases (Figure 1) and hydrocarbon exposure.
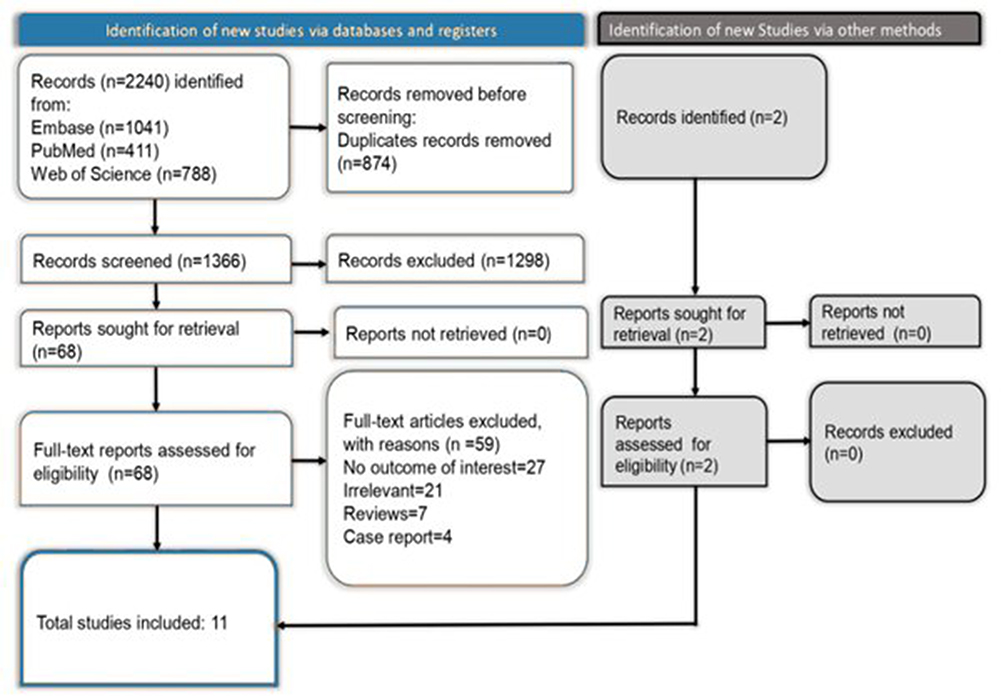 |
Figure 1 PRISMA flowchart depicting article selection and screening process. |
Characteristics of Included Studies
The included studies comprised 8 cross-sectional and 3 prospective cohort studies (Table 1). Sample sizes ranged from 1100 to 17,007 participants, with ages spanning from 6 years to over 60 years. Among the 11 included studies, eight were conducted in the United States and three were conducted in China. The US-based studies primarily utilized data from the National Health and Nutrition Examination Survey (NHANES) and focused on environmental hydrocarbon exposure in the general population, whereas the Chinese studies largely involved prospective cohort designs and occupationally exposed populations, including coke oven workers and urban residents. Hydrocarbon exposure was primarily assessed through measurements of urinary PAH metabolites (eg, 1-hydroxynaphthalene, 2-hydroxyfluorene, 1-hydroxypyrene) and BTEX (Benzene, Toluene, Ethylbenzene, Xylene) levels in blood. Cardiovascular outcomes assessed included coronary heart disease, stroke, angina, myocardial infarction, self-reported CVD, and atherosclerotic cardiovascular disease (ASCVD). Hydrocarbon analysis techniques, such as gas chromatography coupled with mass spectrometry and high-resolution mass spectrometry, were employed to quantify exposure Effect sizes, reported as OR with 95% CI, demonstrated strong associations between hydrocarbon exposure and increased CVD and ASCVD risks. Key adjusted factors included age, gender, BMI, smoking, alcohol consumption, physical activity, and serum cotinine levels, with mediators like inflammation, obesity, and diabetes influencing the associations. These findings emphasize the consistent link between hydrocarbon exposure and heightened cardiovascular risks, as summarized in Tables 1 and S4.
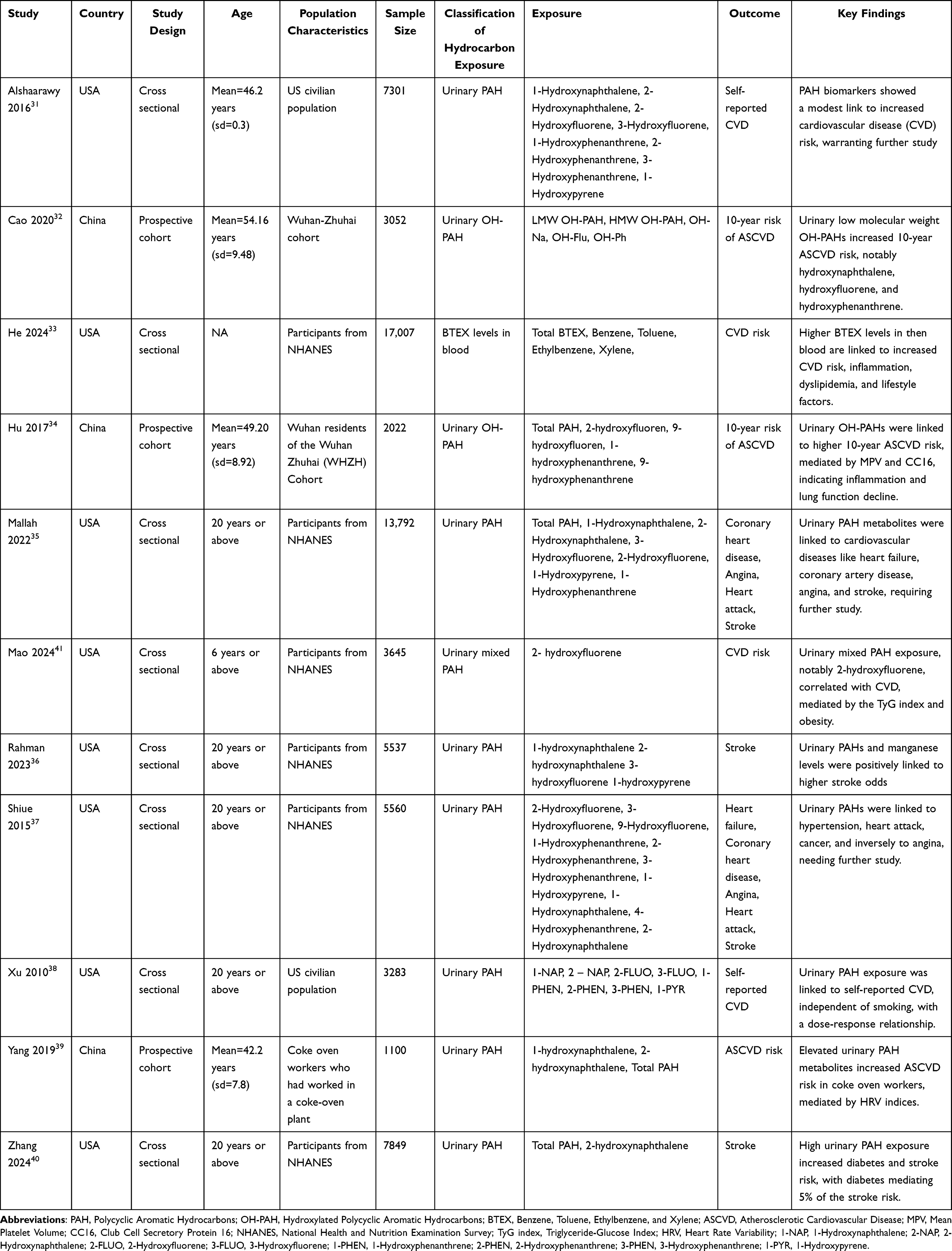 |
Table 1 Characteristics of Included Studies |
Quality of Studies
Quality assessment using the NOS demonstrated that the included studies were generally of moderate to high methodological quality. Among the 11 included studies, the cross-sectional studies achieved the maximum adapted NOS score of 6/6, indicating adequate participant selection, exposure ascertainment, comparability, and outcome assessment. The prospective cohort studies scored between 8 and 9 out of 9, reflecting strong methodological rigor, sufficient follow-up duration, and adequate follow-up assessment. Overall, the findings suggest a relatively low risk of bias across the included studies, supporting the reliability of the synthesized evidence.
Association of Hydrocarbons and Their Metabolites with CVD
Hydroxy Naphthalene Metabolites
1-Hydroxy Naphthalene
1-Hydroxy Naphthalene was consistently associated with increased cardiovascular risks across multiple studies. Alshaarawy et al31 reported an OR of 1.11 (95% CI: 1.04–1.18) for self-reported CVD, while Cao et al32 observed an OR of 1.158 (95% CI: 1.019–1.317) for increased 10-year ASCVD risk. Rahman et al36 found an OR of 2.33 (95% CI: 0.96–5.63) for stroke. Mallah et al35 demonstrated significant associations, reporting an OR of 2.21 (95% CI: 1.89–2.58) for coronary heart disease, 2.75 (95% CI: 2.33–3.25) for angina, 2.00 (95% CI: 1.74–2.32) for heart attack, and 1.89 (95% CI: 1.62–2.20) for stroke. Shiue et al37 reported an OR of 1.00 (95% CI: 0.64–1.57) for heart failure, 0.71 (95% CI: 0.47–1.07) for coronary heart disease, 0.92 (95% CI: 0.70–1.20) for angina, 1.01 (95% CI: 0.67–1.51) for heart attack, and 1.21 (95% CI: 0.95–1.56) for stroke. Yang et al39 noted elevated ASCVD risk among coke oven workers, reporting an OR of 2.36 (95% CI: 1.47–3.78). Additionally, Xu et al38 observed an OR of 1.32 (95% CI: 0.85–2.07) for self-reported CVD, further supporting the link between 1-OH-NA exposure and increased cardiovascular risks.
2-Hydroxy Naphthalene
2-Hydroxy Naphthalene was strongly associated with cardiovascular risks across multiple studies. Alshaarawy et al31 reported an OR of 1.22 (95% CI: 1.08–1.38) for self-reported CVD. Rahman et al36 observed an OR of 2.449 (95% CI: 1.067–5.622) for stroke. Mallah et al35 demonstrated significant associations, reporting an OR of 1.75 (95% CI: 1.51–2.03) for coronary heart disease, 1.83 (95% CI: 1.56–2.14) for angina, 1.39 (95% CI: 1.21–1.61) for heart attack, and 1.48 (95% CI: 1.28–1.72) for stroke. Yang et al39 noted elevated ASCVD risk among coke oven workers, with an OR of 6.58 (95% CI: 3.90–11.09). Xu et al38 found an OR of 1.27 (95% CI: 0.94–1.72) for self-reported CVD, while Zhang et al40 reported an OR of 2.23 (95% CI: 1.17–4.25) for stroke.
Total Hydroxy Naphthalene
In Cao et al,32 Total Hydroxy Naphthalene was found to have a significant association with an increased 10-year ASCVD risk. Specifically, individuals with higher urinary concentrations of Total OH-Na had an OR of 1.158 (95% CI: 1.019–1.317), indicating a 15.8% higher risk of developing ASCVD for each unit increase in exposure.
Hydroxy Fluorene Metabolites
2-Hydroxy Fluorene
2-Hydroxy Fluorene showed significant associations with cardiovascular risks across multiple studies. Alshaarawy et al31 reported an OR of 1.27 (95% CI: 1.12–1.43) for self-reported CVD. Mallah et al35 demonstrated associations with coronary heart disease (OR: 1.99, 95% CI: 1.71–2.31), angina (OR: 2.10, 95% CI: 1.78–2.48), heart attack (OR: 1.61, 95% CI: 1.39–1.87), and stroke (OR: 1.94, 95% CI: 1.66–2.26). Hu et al34 observed an OR of 1.71 (95% CI: 1.19–2.44) for ASCVD risk, with inflammatory and lung function markers as mediators. Xu et al38 reported an OR of 1.31 (95% CI: 0.97–1.76) for self-reported CVD. Mao et al41 found a striking association, reporting an OR of 115.80 (95% CI: 5.05–2654.32) for CVD risk. Shiue et al37 observed modest associations, reporting an OR of 1.13 (95% CI: 0.68–1.88) for heart failure, 0.83 (95% CI: 0.56–1.23) for coronary heart disease, 0.85 (95% CI: 0.61–1.18) for angina, 1.27 (95% CI: 0.73–2.22) for heart attack, and 0.96 (95% CI: 0.63–1.47) for stroke.
3-Hydroxy Fluorene
3-Hydroxy Fluorene was moderately associated with cardiovascular risks across multiple studies. Alshaarawy et al31 reported an OR of 1.18 (95% CI: 1.06–1.32) for self-reported CVD. Rahman et al36 observed an OR of 2.201 (95% CI: 1.115–4.346) for stroke. Mallah et al35 demonstrated associations with coronary heart disease (OR: 1.78, 95% CI: 1.53–2.08), angina (OR: 1.77, 95% CI: 1.51–2.09), heart attack (OR: 1.47, 95% CI: 1.27–1.69), and stroke (OR: 1.68, 95% CI: 1.44–1.95). Xu et al38 found an OR of 1.12 (95% CI: 0.78–1.62) for self-reported CVD. Shiue et al37 observed modest associations, reporting an OR of 1.07 (95% CI: 0.62–1.87) for heart failure, 0.82 (95% CI: 0.55–1.22) for coronary heart disease, 0.92 (95% CI: 0.63–1.34) for angina, 1.18 (95% CI: 0.69–2.04) for heart attack, and 1.00 (95% CI: 0.71–1.41) for stroke.
9-Hydroxy Fluorene
9-Hydroxy Fluorene demonstrated mixed associations with cardiovascular risks across studies. Hu et al34 reported an OR of 1.40 (95% CI: 1.01–1.77) for ASCVD risk. Shiue et al37 observed minimal associations, reporting an OR of 0.87 (95% CI: 0.65–1.17) for coronary heart disease, 0.97 (95% CI: 0.71–1.34) for angina, 1.05 (95% CI: 0.68–1.62) for heart attack, and 1.03 (95% CI: 0.63–1.68) for stroke.
Total Hydroxy Fluorene
In Cao et al,32 Total Hydroxy Fluorene exhibited a strong association with increased 10-year ASCVD risk. The study reported an OR of 1.246 (95% CI: 1.115–1.392), indicating a 24.6% higher likelihood of developing ASCVD for individuals with elevated urinary levels of Total OH-Flu.
Hydroxy Phenanthrene Metabolites
1-Hydroxy Phenanthrene
1-Hydroxy Phenanthrene was associated with cardiovascular risks across multiple studies. Alshaarawy et al31 reported an OR of 1.07 (95% CI: 0.94–1.21) for self-reported CVD. Mallah et al35 demonstrated significant associations, reporting an OR of 1.68 (95% CI: 1.45–1.94) for coronary heart disease, 1.85 (95% CI: 1.58–2.18) for angina, 1.56 (95% CI: 1.35–1.81) for heart attack, and 1.88 (95% CI: 1.61–2.19) for stroke. Xu et al38 observed an OR of 1.28 (95% CI: 0.93–1.76) for self-reported CVD. Hu et al34 reported an OR of 1.50 (95% CI: 1.05–2.14) for ASCVD risk, mediated by inflammatory and lung function markers. Shiue et al37 noted minimal associations, reporting an OR of 0.73 (95% CI: 0.39–1.34) for heart failure, 1.08 (95% CI: 0.75–1.57) for coronary heart disease, 1.02 (95% CI: 0.57–1.83) for angina, 1.14 (95% CI: 0.65–2.00) for heart attack, and 0.93 (95% CI: 0.54–1.60) for stroke.
2-Hydroxy Phenanthrene
2-Hydroxy Phenanthrene demonstrated associations with cardiovascular risks across multiple studies. Alshaarawy et al31 reported an OR of 1.11 (95% CI: 0.98–1.26) for self-reported CVD. Xu et al38 observed an OR of 1.45 (95% CI: 1.01–2.07) for self-reported CVD. Shiue et al37 noted associations across various cardiovascular outcomes, reporting an OR of 1.06 (95% CI: 0.56–2.01) for heart failure, 1.11 (95% CI: 0.73–1.69) for coronary heart disease, 1.10 (95% CI: 0.55–2.20) for angina, 1.32 (95% CI: 0.80–2.17) for heart attack, and 0.81 (95% CI: 0.45–1.47) for stroke.
3-Hydroxy Phenanthrene
3-Hydroxy Phenanthrene demonstrated weak or minimal associations with cardiovascular risks across studies. Alshaarawy et al31 reported an OR of 1.10 (95% CI: 0.96–1.25) for self-reported CVD. Xu et al38 observed an OR of 1.34 (95% CI: 0.92–1.96) for self-reported CVD. Shiue et al37 noted associations across several outcomes, reporting an OR of 0.76 (95% CI: 0.42–1.40) for heart failure, 0.83 (95% CI: 0.60–1.14) for coronary heart disease, 0.95 (95% CI: 0.57–1.58) for angina, 1.10 (95% CI: 0.67–1.81) for heart attack, and 0.91 (95% CI: 0.57–1.45) for stroke.
4-Hydroxy Phenanthrene
4-Hydroxy Phenanthrene demonstrated limited or weak associations with cardiovascular risks in the available studies. Shiue et al37 observed minimal associations, reporting an OR of 0.70 (95% CI: 0.39–1.29) for heart failure, 0.76 (95% CI: 0.48–1.18) for coronary heart disease, 1.08 (95% CI: 0.61–1.91) for angina, 1.02 (95% CI: 0.56–1.85) for heart attack, and 0.73 (95% CI: 0.42–1.28) for stroke. These findings suggest limited evidence for a strong relationship between 4-Hydroxy Phenanthrene exposure and cardiovascular risks.
9-Hydroxy Phenanthrene
9-Hydroxy Phenanthrene demonstrated notable associations with cardiovascular risks in certain studies. Hu et al34 reported an OR of 1.45 (95% CI: 1.04–2.02) for ASCVD risk, highlighting inflammation and lung function as mediators of the relationship. No other studies specifically reported findings for 9-Hydroxy Phenanthrene in relation to cardiovascular risks.
Total Hydroxy Phenanthrene
In Cao et al,32 Total Hydroxy Phenanthrene demonstrated a weaker association with 10-year ASCVD risk compared to other hydroxy PAH metabolites. The reported OR of 1.079 (95% CI: 0.943–1.234) suggests only a modest 7.9% increase in the likelihood of developing ASCVD for individuals with higher urinary concentrations of total hydroxy phenanthrene.
Hydroxy Pyrene Metabolites
1-Hydroxy Pyrene
1-Hydroxy Pyrene demonstrated consistent associations with cardiovascular risks across studies. Alshaarawy et al31 reported an OR of 1.12 (95% CI: 1.00–1.26) for self-reported CVD. Rahman et al36 observed an OR of 2.07 (95% CI: 1.04–4.11) for stroke, indicating a strong association. Mallah et al35 showed significant associations with coronary heart disease (OR: 1.38, 95% CI: 1.21–1.61), angina (OR: 1.44, 95% CI: 1.24–1.69), heart attack (OR: 1.19, 95% CI: 1.03–1.37), and stroke (OR: 1.41, 95% CI: 1.22–1.64). Shiue et al37 noted weaker associations, reporting ORs of 0.99 (95% CI: 0.59–1.66) for heart failure, 1.10 (95% CI: 0.83–1.47) for coronary heart disease, 1.21 (95% CI: 0.71–2.05) for heart attack, and 1.47 (95% CI: 1.05–2.06) for stroke. Xu et al38 found an OR of 0.96 (95% CI: 0.59–1.56) for self-reported CVD.
BTEX
BTEX exposures were consistently associated with increased cardiovascular risks across studies. He et al33 reported an OR of 1.64 (95% CI: 1.23–2.19) for CVD associated with total BTEX exposure in blood. For individual components, benzene showed an OR of 1.63 (95% CI: 1.25–2.12), toluene had an OR of 1.58 (95% CI: 1.20–2.07), ethylbenzene demonstrated an OR of 1.35 (95% CI: 1.09–1.66), and xylene presented an OR of 1.29 (95% CI: 1.04–1.59). These findings highlight the significant risks posed by BTEX exposure, suggesting that these volatile organic compounds may exacerbate cardiovascular risks through mechanisms such as inflammation and dyslipidemia.
Total PAH
Total PAH exposure demonstrated consistent associations with increased cardiovascular risks across studies. Mallah et al35 reported significant associations, with an OR of 1.24 (95% CI: 1.09–1.42) for coronary heart disease, 1.30 (95% CI: 1.13–1.49) for angina, 1.28 (95% CI: 1.12–1.47) for heart attack, and 1.17 (95% CI: 1.02–1.33) for stroke. Hu et al34 observed an OR of 1.63 (95% CI: 1.13–2.34) for ASCVD risk, mediated by markers of inflammation and lung function decline. Yang et al39 found strong associations among coke oven workers, with an OR of 1.60 (95% CI: 1.03–2.49) for ASCVD risk. Zhang et al40 noted an OR of 1.97 (95% CI: 1.11–3.52) for stroke, further reinforcing the cardiovascular risks linked to total PAH exposure. These findings highlight the pervasive cardiovascular risks associated with total PAH exposure, emphasizing the need for mitigation efforts, especially among high-risk populations. Additionally, Cao et al32 reported significant associations between low molecular weight (LMW) and high molecular weight (HMW) OH-PAHs and cardiovascular risks. For LMW OH-PAHs, an OR of 1.22 (95% CI: 1.065–1.402) was observed for a 10-year ASCVD risk. Meanwhile, HMW OH-PAHs showed a weaker association, with an OR of 1.018 (95% CI: 0.898–1.155). These findings indicate that LMW OH-PAHs may pose a more substantial cardiovascular risk compared to their HMW counterparts, suggesting the importance of molecular weight in determining the toxicity of PAH metabolites.
Discussion
This systematic review evaluates the current evidence on the association between hydrocarbon exposure, particularly PAH and VOC, and the risk of CVD. The findings pointed to a consistent link between hydrocarbon metabolites, such as hydroxy PAHs and BTEX components, and increased risks of coronary heart disease, stroke, heart attack, and ASCVD. However, variations in the magnitude of associations across studies highlight the need for further investigation into exposure mechanisms, population differences, and confounding factors.
The findings from this review consistently indicate that PAH metabolites, such as hydroxy naphthalene and hydroxy fluorene derivatives, are strongly associated with cardiovascular risks. For instance, 1-hydroxy naphthalene was significantly linked to increased odds of coronary heart disease and stroke, as reported by Mallah et al,35 while Cao et al32 identified an elevated 10-year ASCVD risk. Similarly, OH-FLUO metabolites like 2-hydroxy fluorene and 3-hydroxy fluorene demonstrated strong associations with coronary heart disease, angina, and stroke, further emphasizing their role as biomarkers of hydrocarbon exposure. The cumulative evidence points to a dose-response relationship, wherein higher urinary concentrations of these metabolites correspond to a greater likelihood of adverse cardiovascular outcomes. These findings align with the broader understanding of hydrocarbon toxicity, including their ability to induce oxidative stress, systemic inflammation, and endothelial dysfunction key drivers of atherosclerosis and CVD progression.
Notably, while hydroxy naphthalene and hydroxy fluorene metabolites consistently showed significant associations, hydroxy phenanthrene and hydroxy pyrene derivatives exhibited more variable results. For example, 1-hydroxy phenanthrene demonstrated significant links to coronary heart disease and stroke in studies by Mallah et al35 and Xu et al,38 while weaker associations were observed for 3-hydroxy phenanthrene and 4-hydroxy phenanthrene. These discrepancies might be explained by variances in research populations, exposure levels, or analytical techniques. Additionally, BTEX components were consistently associated with increased CVD risks, as demonstrated by He et al,33 emphasizing the cardiovascular burden posed by VOCs in occupational and environmental settings.
A significant strength of this review is its focus on specific hydrocarbon metabolites, such as total hydroxy naphthalene, total hydroxy fluorene, and total hydroxy phenanthrene groups, which provide a more nuanced understanding of the cardiovascular impacts of hydrocarbon exposure. For instance, Cao et al32 reported strong associations for total hydroxy fluorene (OR: 1.246, 95% CI: 1.115–1.392) and total OH-Na (OR: 1.158, 95% CI: 1.019–1.317), while total hydroxy phenanthrene showed a weaker association. This pattern suggests that molecular weight and chemical properties of PAH metabolites may influence their cardiovascular toxicity, with low molecular weight (LMW) PAHs posing greater risks compared to high molecular weight (HMW) PAHs. The implications of these findings extend to public health and occupational safety, emphasizing the need for targeted interventions to reduce exposure to high-risk hydrocarbons.
Despite the consistency of these associations, the variability in effect sizes across studies warrants attention. Factors such as baseline exposure levels, differences in population characteristics, and variations in exposure duration and measurement techniques may contribute to these discrepancies. For instance, studies like Hu et al34 and Yang et al39 highlighted the role of occupational exposures, such as those among coke oven workers, in amplifying cardiovascular risks. Conversely, environmental exposures in the general population, as examined by Shiue et al,37 demonstrated weaker associations, potentially due to lower exposure levels or differences in confounding factors like smoking and air pollution.
The findings of this systematic review align with previous research highlighting the adverse cardiovascular effects of hydrocarbons, including PAHs and VOCs.42,43 Our study advances this understanding by demonstrating specific associations between hydrocarbon metabolites, such as 1-hydroxy naphthalene and 2-hydroxy fluorene, and distinct CVD outcomes, including coronary heart disease, stroke, and myocardial infarction. This focus on individual metabolites provides a nuanced perspective, building on earlier studies and emphasizing the need for targeted research on metabolite-specific cardiovascular risks.
The findings from this review have significant implications for public health and policy. Efforts to mitigate hydrocarbon exposure, such as stricter industrial regulations, improved air quality standards, and enhanced occupational safety measures, could reduce the cardiovascular burden associated with these pollutants. Public awareness campaigns emphasizing the health risks of hydrocarbons and promoting protective behaviors, such as avoiding high-pollution areas and using personal protective equipment, are also crucial.
The overall certainty of evidence was considered moderate. Although most included studies were of moderate-to-high methodological quality, the predominance of cross-sectional designs, heterogeneity in exposure and outcome assessment, and potential residual confounding reduced confidence in establishing causal associations between hydrocarbon exposure and cardiovascular disease risk.
When evaluating the results of this review, it is important to take into account a number of limitations. The included studies varied in design, population characteristics, and exposure assessment methods, which may have influenced the reported associations. Cross-sectional designs, which predominated in this review, limit the ability to establish causality between hydrocarbon exposure and CVD outcomes. Confounding factors such as smoking, air pollution, and occupational co-exposures to metals or other toxins may amplify or obscure observed associations, with serum cotinine frequently adjusted for as a key confounder.
Formal assessment of publication bias using funnel plots or Egger’s test was not feasible. Reliance on urinary biomarkers of PAHs and VOCs, while advantageous for quantifying internal exposure, may introduce variability due to differences in metabolic rates, collection timing, or laboratory techniques, and may not fully capture long-term exposure patterns or differentiate between occupational and environmental sources. Additionally, the generalizability of findings is constrained by the geographical concentration of studies, predominantly conducted in the USA and China, potentially overlooking exposure dynamics in other regions. Future research should prioritize prospective cohort studies with larger, more diverse populations and standardized exposure assessment methods that encompass both environmental and occupational settings. Mechanistic research exploring the specific pathways through which hydrocarbon metabolites influence cardiovascular health is also critical to inform targeted interventions and advance policies to protect public health.
Conclusion
This systematic review evidence indicates or suggests an association between hydrocarbon metabolites, such as 1-hydroxy naphthalene and 2-hydroxy fluorene, and cardiovascular outcomes like coronary heart disease, stroke, and myocardial infarction. Variability across studies emphasizes the need for prospective research with standardized methods to confirm these these associations, clarify mechanisms, and assess long-term impacts and mitigation strategies to reduce associated health risks.
Funding
No funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hussain MM, Rafi U, Imran A, Rehman MU, Abbas SK. Risk factors associated with cardiovascular disorders: risk factors associated with cardiovascular disorders. Pakistan BioMed J. 2024;03–14. doi:10.54393/pbmj.v7i02.1034
2. Czinege M, Ruța F, Nyulas V, Halațiu V-B, Nyulas T, Benedek T. Serum albumin concentration and the risk of cardiovascular disease and acute coronary syndrome—a narrative review. J Cardiovasc Emerg. 2024;11(1):11–19.
3. Fuster V, Frazer J, Snair M, Vedanthan R, Dzau V. The future role of the United States in global health: emphasis on cardiovascular disease. J Am College Cardiol. 2017;70(25):3140–3156. doi:10.1016/j.jacc.2017.11.009
4. Karunarathna I, De Alvis K, Gunasena P, Jayawardana A. The role of alcohol in cardiovascular and neurological disorders: current perspectives. Charlottesville: Uva Clinical Psychiatry; 2024.
5. Shabil M, Kumar VU, Dhingra S, et al. Current scenario and strategies to tackle cardiovascular disease risk in HIV geriatrics. Curr Pharmacol Rep. 2023;9(6):523–539. doi:10.1007/s40495-023-00332-0
6. Adhikary D, Barman S, Ranjan R, Stone H. A systematic review of major cardiovascular risk factors: a growing global health concern. Cureus. 2022;14(10):e30119. doi:10.7759/cureus.30119
7. Shabil M, Murti K, Kumar VU, et al. Older PLHIV are at higher cardiovascular risk with poor quality of life. Curr HIV Res. 2023;21(6):354–360. doi:10.2174/011570162X277586231218104922
8. Krismanuel H. Air pollution and cardiovascular diseases: mechanisms, evidence, and mitigation strategies. J Med Life. 2025;18(5):411–427. doi:10.25122/jml-2025-0018
9. Makar A, Al-Hemoud A, Khraishah H, Berry J, Alahmad B. A review of the links between work and heart disease in the 21st century. Methodist Debakey Cardiovasc J. 2024;20(5):71–80. doi:10.14797/mdcvj.1478
10. Binhazzaa Z. Hydrocarbons are the backbone of sustainable civilization. 2024.
11. Liu Q, Peng Y, Liao J, et al. Broad-spectrum hydrocarbon-degrading microbes in the global ocean metagenomes. Sci Total Environ. 2024;926:171746. doi:10.1016/j.scitotenv.2024.171746
12. Sawyer WE, Amabie T, Sylva L, Nwodo MU, Etim NG. Polycyclic Aromatic Hydrocarbons as Ambient Air Pollutants. Springer; 2024.
13. Lin XY, Liu YX, Zhang YJ, Shen HM, Guo Y. Polycyclic aromatic hydrocarbon exposure and DNA oxidative damage of workers in workshops of a petrochemical group. Chemosphere. 2022;303(Pt 2):135076. doi:10.1016/j.chemosphere.2022.135076
14. Manisalidis I, Stavropoulou E, Stavropoulos A, Bezirtzoglou E. Environmental and health impacts of air pollution: a review. Front Public Health. 2020;8:14. doi:10.3389/fpubh.2020.00014
15. Marris CR, Kompella SN, Miller MR, et al. Polyaromatic hydrocarbons in pollution: a heart-breaking matter. J Physiol. 2020;598(2):227–247. doi:10.1113/JP278885
16. Sun Y, Kan Z, Zhang ZF, et al. Association of occupational exposure to polycyclic aromatic hydrocarbons in workers with hypertension from a northeastern Chinese petrochemical industrial area. Environ Pollut. 2023;323:121266. doi:10.1016/j.envpol.2023.121266
17. Cao Q, Song Y, Huan C, et al. Biological aging mediates the association between volatile organic compounds and cardiovascular disease. BMC Public Health. 2024;24(1):2928. doi:10.1186/s12889-024-20349-4
18. Ju S, Lim L, Ki YJ, Choi DH, Song H. Oxidative stress generated by polycyclic aromatic hydrocarbons from ambient particulate matter enhance vascular smooth muscle cell migration through MMP upregulation and actin reorganization. Part Fibre Toxicol. 2022;19(1):29. doi:10.1186/s12989-022-00472-z
19. Verma A, Naidu SV, Sulthana H, et al. Musculoskeletal manifestations in post-acute sequelae of SARS-CoV-2 infection: a systematic review and meta-analysis. Front Public Health. 2025;13:1662953. doi:10.3389/fpubh.2025.1662953
20. Bahman F, Choudhry K, Al-Rashed F, Al-Mulla F, Sindhu S, Ahmad R. Aryl hydrocarbon receptor: current perspectives on key signaling partners and immunoregulatory role in inflammatory diseases. Front Immunol. 2024;15:1421346.
21. Asiwe JN, Oritsemuelebi B. Environmental toxicant-mediated cardiovascular diseases: an insight into the mechanism and possible preventive strategy. Toxicol Environ Health Sci. 2024;16(1):1–19. doi:10.1007/s13530-023-00196-3
22. Habeeb E, Aldosari S, Saghir SA, et al. Role of environmental toxicants in the development of hypertensive and cardiovascular diseases. Toxicol Rep. 2022;9:521–533. doi:10.1016/j.toxrep.2022.03.019
23. Ferreira Azevedo L, de Souza Rocha CC, Souza MCO, et al. High molecular weight polycyclic aromatic hydrocarbon (HMW-PAH) isomers: unveiling distinct toxic effects from cytotoxicity to oxidative stress-induced DNA damage. Arch Toxicol. 2024;1–9.
24. Vogel CF, Van Winkle LS, Esser C, Haarmann-Stemmann T. The aryl hydrocarbon receptor as a target of environmental stressors–Implications for pollution mediated stress and inflammatory responses. Redox Biol. 2020;34:101530. doi:10.1016/j.redox.2020.101530
25. Anakwue R, Anakwue A. Cardiovascular disease risk profiling in Africa: environmental pollutants are not on the agenda. Cardiovasc Toxicol. 2014;14(3):193–207. doi:10.1007/s12012-013-9242-y
26. Essiet AG, Gordon AA, Inyang IB, Mkpan SB. The hidden impact of hydrocarbon pollution on cardio-metabolic health in Akwa Ibom State. Faculty Nat Appl Sci J Appl Chem Sci Res. 2024;2(1):58–68.
27. Alhamdow A, Lindh C, Albin M, Gustavsson P, Tinnerberg H, Broberg K. Early markers of cardiovascular disease are associated with occupational exposure to polycyclic aromatic hydrocarbons. Sci Rep. 2017;7(1):9426. doi:10.1038/s41598-017-09956-x
28. Clark III JD, Serdar B, Lee DJ, Arheart K, Wilkinson JD, Fleming LE. Exposure to polycyclic aromatic hydrocarbons and serum inflammatory markers of cardiovascular disease. Environ Res. 2012;117:132–137. doi:10.1016/j.envres.2012.04.012
29. Lu W-L, Yuan J-H, Liu Z-Y, et al. Worldwide trends in mortality for hypertensive heart disease from 1990 to 2019 with projection to 2034: data from the global burden of disease 2019 study. European J Preventive Cardiol. 2024;31(1):23–37. doi:10.1093/eurjpc/zwad262
30. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–341. doi:10.1016/j.ijsu.2010.02.007
31. Alshaarawy O, Elbaz HA, Andrew ME. The association of urinary polycyclic aromatic hydrocarbon biomarkers and cardiovascular disease in the US population. Environ Int. 2016;89:174–178. doi:10.1016/j.envint.2016.02.006
32. Cao L, Wang D, Zhu C, et al. Polycyclic aromatic hydrocarbon exposure and atherosclerotic cardiovascular disease risk in urban adults: the mediating role of oxidatively damaged DNA. Environ Pollut. 2020;265:114860. doi:10.1016/j.envpol.2020.114860
33. He Y, Qiu H, Wang W, Lin Y, Ho KF. Exposure to BTEX is associated with cardiovascular disease, dyslipidemia and leukocytosis in national US population. Sci Total Environ. 2024;919:170639. doi:10.1016/j.scitotenv.2024.170639
34. Hu C, Hou J, Zhou Y, et al. Association of polycyclic aromatic hydrocarbons exposure with atherosclerotic cardiovascular disease risk: a role of mean platelet volume or club cell secretory protein. Environ Pollut. 2018;233:45–53. doi:10.1016/j.envpol.2017.10.042
35. Mallah MA, Changxing L, Mallah MA, et al. Association of urinary polycyclic aromatic hydrocarbon metabolites and cardiovascular disease among US population: a cross-sectional study. Environ Res. 2022;209:112775. doi:10.1016/j.envres.2022.112775
36. Rahman HH, Sheikh SP, Munson-McGee SH. Arsenic, polycyclic aromatic hydrocarbons, and metal exposure and risk assessment of stroke. Environ Sci Pollut Res. 2023;30(37):86973–86986. doi:10.1007/s11356-023-28593-8
37. Shiue I. Are urinary polyaromatic hydrocarbons associated with adult hypertension, heart attack, and cancer? USA NHANES, 2011–2012. Environ Sci Pollut Res. 2015;22(21):16962–16968. doi:10.1007/s11356-015-4922-8
38. Xu X, Cook RL, Ilacqua VA, Kan H, Talbott EO, Kearney G. Studying associations between urinary metabolites of polycyclic aromatic hydrocarbons (PAHs) and cardiovascular diseases in the United States. Sci Total Environ. 2010;408(21):4943–4948. doi:10.1016/j.scitotenv.2010.07.034
39. Yang L, Guo W, Zeng D, et al. Heart rate variability mediates the association between polycyclic aromatic hydrocarbons exposure and atherosclerotic cardiovascular disease risk in coke oven workers. Chemosphere. 2019;228:166–173. doi:10.1016/j.chemosphere.2019.04.101
40. Zhang A, Zhang H, Mi L, et al. Diabetes: a potential mediator of associations between polycyclic aromatic hydrocarbon exposure and stroke. Environ Sci Pollut Res. 2024;1–11.
41. Mao Q, Zhu X, Zhang X, Kong Y. Triglyceride-glucose index and its combination with obesity indicators mediating the association between 2-hydroxyfluorene and the prevalence of cardiovascular disease: evidence from the NHANES (2005–2018). Ecotoxicol Environ Saf. 2024;287:117283. doi:10.1016/j.ecoenv.2024.117283
42. Leachi HFL, Marziale MHP, Martins JT, Aroni P, Galdino MJQ, Ribeiro RP. Polycyclic aromatic hydrocarbons and development of respiratory and cardiovascular diseases in workers. Revista Brasileira de Enfermagem. 2020;73(3):e20180965. doi:10.1590/0034-7167-2018-0965
43. Wu P. Association between polycyclic aromatic hydrocarbons exposure with red cell width distribution and ischemic heart disease: insights from a population-based study. Sci Rep. 2024;14(1):196. doi:10.1038/s41598-023-50794-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.