Back to Journals » International Journal of General Medicine » Volume 19
Elevated CA19-9 in IgG4-Related Autoimmune Pancreatitis: A Single-Center Retrospective Cohort Study
Authors Han DG, Li SY, Zhou RT, Tong QY, Liu W ![]()
Received 15 January 2026
Accepted for publication 11 March 2026
Published 16 March 2026 Volume 2026:19 596352
DOI https://doi.org/10.2147/IJGM.S596352
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Dong-Ge Han,1– 3,* Su-Yu Li,4,* Rui-Ting Zhou,1– 3 Qiao-Yun Tong,1– 3 Wei Liu1– 3
1The First College of Clinical Medical Science, China Three Gorges University, Yichang, People’s Republic of China; 2Institute of Digestive Disease, China Three Gorges University, Yichang, People’s Republic of China; 3Department of Gastroenterology, Yichang Central People’s Hospital, Yichang, People’s Republic of China; 4Department of Gastroenterology, Affiliated Renhe Hospital of China Three Gorges University, Yichang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Liu, Institute of Digestive Disease, China Three Gorges University, 8 Daxue Road, Yichang, 443000, People’s Republic of China, Email [email protected] Qiao-Yun Tong, Institute of Digestive Institute of Digestive Disease, China Three Gorges University, 8 Daxue Road, Yichang, 443000, People’s Republic of China, Email [email protected]
Background: IgG4-related autoimmune pancreatitis (IgG4-AIP) is a rare autoimmune pancreatic disorder, with elevated carbohydrate antigen 19– 9 (CA19-9) observed in some patients.
Objective: This study aims to compare the clinical features of IgG4-AIP patients with elevated versus normal CA19-9 levels to clarify the clinical significance of CA19-9 in this condition.
Methods: This study conducted a retrospective analysis of the clinical data of 41 patients with IgG4-AIP who underwent CA19-9 testing at Yichang Central People’s Hospital from January 2019 to April 2025. In this study, the normal reference range for CA19-9 levels was defined as 0 to 39 U/mL.
Results: Among the 41 patients with IgG4-AIP, 23 patients (56.10%) had normal CA19-9 levels, while 18 patients (43.90%) exhibited elevated CA19-9 levels. Patients with elevated CA19-9 levels were more likely to be misdiagnosed as having pancreatic tumors (55.56% vs. 13.04%) and had a higher incidence of bile duct involvement (88.89% vs. 26.09%), whereas the incidence of lymph node involvement (22.22% vs. 56.52%) was lower (P< 0.05). Compared to the normal CA19-9 group, patients in the elevated CA19-9 group had significantly higher levels of total bilirubin (TBIL), direct bilirubin (DBIL), alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP), and complement C3 (C3) (P< 0.05). Additionally, CA19-9 levels demonstrated a moderate positive correlation with TBIL, DBIL, ALT, AST, GGT, and ALP (P< 0.05). However, no significant correlation was found between CA19-9 levels and C3 or serum immunoglobulin G4 (IgG4) levels (P> 0.05).
Conclusion: Patients with elevated CA19-9 levels in IgG4-AIP exhibit more complex clinical features. Clinicians should consider CA19-9 level differences when evaluating and managing IgG4-AIP patients to guide personalized diagnostic and therapeutic strategies.
Keywords: IgG4-related autoimmune pancreatitis, IgG4-related disease, carbohydrate antigen 19-9
Introduction
Immunoglobulin G4-related disease (IgG4-RD) is a chronic, systemic fibroinflammatory disorder of immune-mediated origin that can involve multiple organs throughout the body.1–6 IgG4-related autoimmune pancreatitis (IgG4-AIP) is a prominent and commonly encountered subtype of IgG4-RD, characterized by diffuse or focal enlargement of the pancreas and significantly elevated serum immunoglobulin G4 (IgG4) levels in the majority of patients.7–11 In clinical practice, the early and accurate diagnosis of IgG4-AIP poses several challenges, primarily due to its imaging features, which often closely resemble those of pancreatic cancer. Moreover, carbohydrate antigen 19–9 (CA19-9) is a significant tumor marker for pancreatic malignancies. Studies have shown that some patients with IgG4-AIP exhibit elevated levels of CA19-9,12–14 further increasing the likelihood of misdiagnosis as pancreatic cancer. Such misdiagnosis can lead not only to delays in appropriate treatment but also to unnecessary surgical interventions. However, there is currently a lack of systematic research in the medical community regarding whether elevated CA19-9 levels are associated with unique clinical features in patients with IgG4-AIP.
Therefore, the aim of the study was to conduct a retrospective analysis of the clinical data of 41 IgG4-AIP patients who underwent CA19-9 testing at Yichang Central People’s Hospital from January 2019 to April 2025, systematically comparing the clinical characteristics between those with elevated CA19-9 levels and those with normal levels. We hope that this study will summarize and elucidate the unique clinical features of IgG4-AIP patients with elevated CA19-9 levels, providing new insights for a deeper understanding of the disease and offering a solid evidence-based foundation for optimizing the differential diagnosis process.
Patients and Methods
Patients
This study included a total of 41 IgG4-AIP patients who underwent CA19-9 testing at Yichang Central People’s Hospital from January 2019 to April 2025. The research was conducted in strict accordance with the ethical guidelines established by the Declaration of Helsinki. Given that this study employed a retrospective design and analyzed anonymized patient data, it was reviewed by the hospital’s Medical Ethics Committee (Approval No: 2024–361-01) and deemed exempt from full ethical review, as well as from obtaining informed consent from the subjects. This decision ensured compliance with ethical standards while effectively safeguarding patient privacy rights.
Inclusion Criteria
All patients in this study met the 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD.15 During the diagnostic process, each patient underwent a collaborative assessment involving two rheumatology experts, two gastroenterology specialists, and two radiology experts. This multidisciplinary collaboration and rigorous review ensured the scientific validity and accuracy of the diagnostic process, thereby enhancing the reliability of the research findings. We implemented a standardized patient baseline data collection form to systematically gather information on age, sex, smoking and alcohol consumption history, and prior medical conditions. This approach ensures that the baseline data is comprehensive and traceable.
Exclusion Criteria
The exclusion criteria were as follows: 1. IgG4-AIP patients who did not undergo CA19-9 laboratory testing; 2. Patients already diagnosed with type 2 autoimmune pancreatitis or other similar conditions; 3. Patients with incomplete medical records or lacking essential clinical information.
Laboratory Tests and Imaging
In this study, all patients underwent laboratory tests including complete blood count, liver function tests, lipase levels, serum amylase concentrations, pancreatic amylase activity, serum immunoglobulin G (IgG), complement C3 (C3), complement C4 (C4), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Additionally, a total of 36 patients had their IgG4 levels measured.
In this study, all samples from the research subjects were collected from peripheral venous blood. Blood was drawn from the antecubital vein in the early morning, after admission and prior to the administration of hormonal or other therapies, ensuring a fasting state. All serum samples were free from hemolysis, clots, and turbidity, and the collection and storage procedures adhered to laboratory operating standards. Samples were excluded if they had received any relevant therapeutic interventions prior to collection, exhibited significant physicochemical abnormalities, or underwent freeze-thaw cycles or contamination during storage. Laboratory tests were performed using standard automated analyzers: complete blood count was measured using a Sysmex XN series hematology analyzer; liver function tests, lipase, amylase, and pancreatic amylase were measured using a Roche Cobas 8000 chemistry analyzer; serum IgG, C3, C4, and CRP were measured by immunoturbidimetry on a Beckman Coulter AU5800 or Siemens BN ProSpec system; ESR was determined using an Alifax Test 1 automated analyzer. Serum CA19-9 levels were measured by electrochemiluminescence immunoassay on a Roche Cobas 8000. Serum IgG4 levels were measured by nephelometry on a Siemens BN ProSpec.
All patients also underwent imaging studies, which included computed tomography (CT), magnetic resonance imaging (MRI), magnetic resonance cholangiopancreatography (MRCP), or ultrasound examinations.
Imaging studies were performed using 64-slice CT (Siemens SOMATOM Definition AS) or 3.0T MRI (GE Signa Pioneer), and ultrasound examinations were performed using a Philips EPIQ 7 system. The imaging results were independently interpreted by two radiology experts, two rheumatology and immunology specialists, and two gastroenterology experts, who collectively reached a consensus through a blinded evaluation process. This approach ensured the accurate identification of organ involvement in patients with IgG4-AIP and enhanced the reliability and consistency of the findings. All imaging data were assessed according to standardized evaluation criteria to minimize subjective bias.
Definitions
In this study, the normal reference range for CA19-9 levels was defined as 0 to 39 U/mL. Based on this criterion, patients with CA19-9 levels less than or equal to 39 U/mL were classified into the normal CA19-9 group, while those with CA19-9 levels greater than 39 U/mL were categorized into the elevated CA19-9 group.
Statistics
This study assessed the normal distribution of continuous variables using the Shapiro–Wilk test. Data that followed a normal distribution were presented as mean ± standard deviation (SD), while non-normally distributed data were described using median and interquartile range (IQR). Categorical variables were summarized and analyzed using frequency counts and relative percentages. When comparing continuous variables between different groups, the t-test was used if the data met the normality assumption; for non-normally distributed data, the Mann–Whitney U-test was employed. Prior to conducting the t-test, Levene’s test was used to check for homogeneity of variances; if the variances were unequal, Welch’s t-test was applied as an alternative. For categorical variables, the chi-square test was used for analysis if the expected frequency conditions were met; in cases where any cells had low frequencies, Fisher’s exact test was utilized. To explore correlations between variables, Pearson correlation coefficients were calculated for normally distributed data, while Spearman rank correlation analysis was used for non-normally distributed or ordinal data. To ensure the reliability of statistical analysis results, all observations were assumed to be independent, and measures were taken during data collection to avoid interference between variables. The treatment of missing data depended on the missing data mechanism: if data were missing completely at random (MCAR), listwise deletion was used; if missing at random (MAR), multiple imputation was employed. All statistical analyses were conducted using SPSS Statistics 27.0 software (IBM Corp., Armonk, NY, USA). All hypothesis tests were two-tailed, with a significance level set at P<0.05.
Results
Baseline Characteristics
A total of 41 diagnosed IgG4-AIP patients were included in this study, and their baseline characteristics are detailed in Table 1. The average age at diagnosis in this cohort was 61.76 ± 10.04 years (range: 35 to 87 years). Among the patients, 36 were male (87.80%) and 5 were female (12.20%), resulting in a male-to-female ratio of 7.2:1. Among all patients, 23 (56.10%) had serum CA19-9 levels within the normal range, while 18 (43.90%) exhibited elevated CA19-9 levels. It is noteworthy that in this cohort, 13 patients (31.71%) with IgG4-AIP were misdiagnosed as having pancreatic tumors at the time of their initial consultation. Further analysis revealed that the misdiagnosis rate was significantly higher in the elevated CA19-9 group compared to the normal CA19-9 group (55.56% vs. 13.04%, P<0.05) (Table 1).
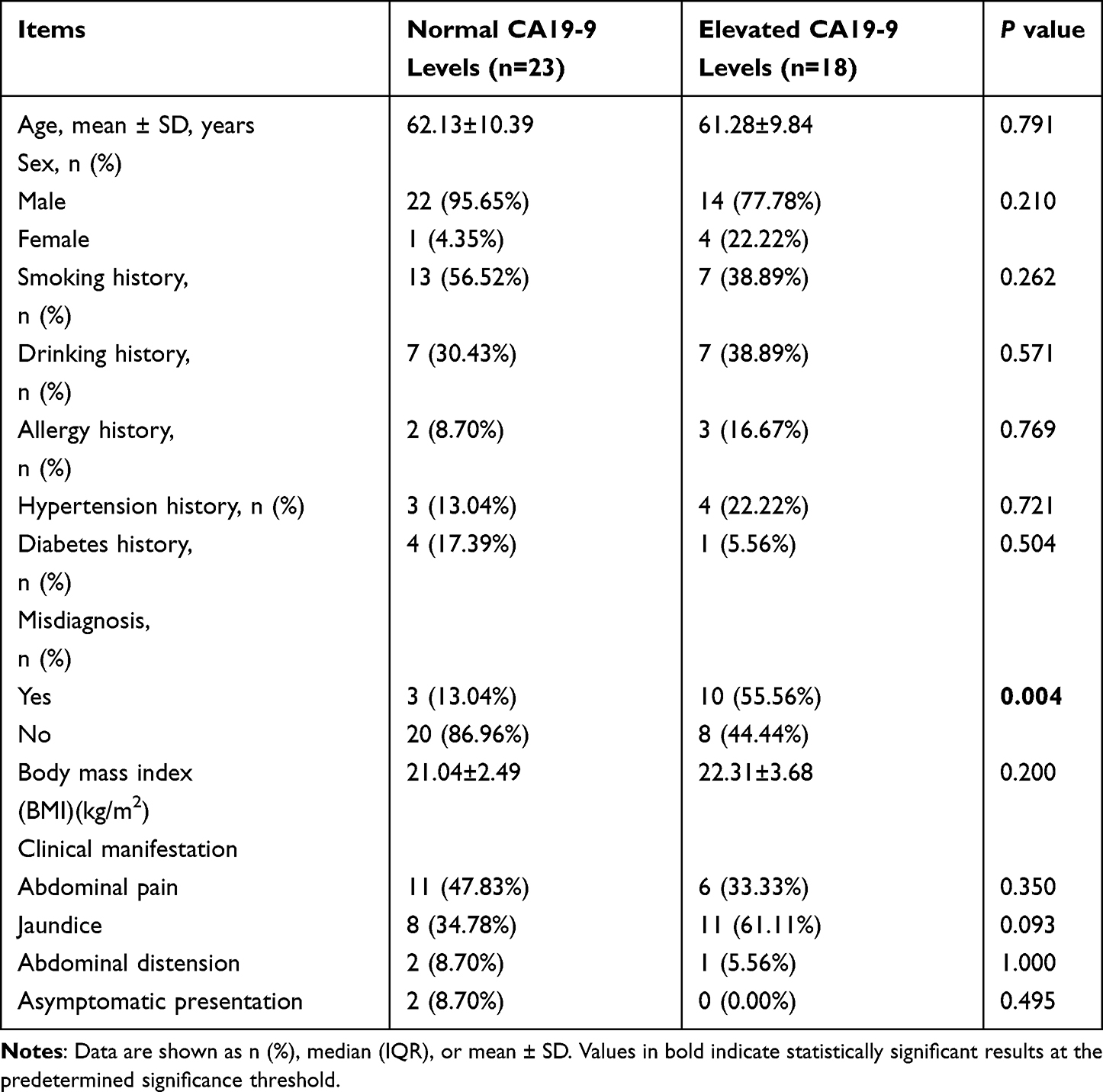 |
Table 1 Comparison of Baseline Characteristics Between IgG4-AIP Patients with Normal and Elevated CA19-9 Levels |
Comparison of Affected Organs in Patients with IgG4-AIP in the Normal CA19-9 Level Group and the Elevated CA19-9 Level Group
The comparison of organ involvement in IgG4-AIP patients between those with normal and elevated CA19-9 levels is summarized in Table 2. Among the 41 IgG4-AIP patients, 11 (26.83%) presented with isolated pancreatic involvement, while the remaining 30 (73.17%) exhibited extra-pancreatic organ involvement. Notably, the incidence of concomitant bile duct involvement in IgG4-AIP patients with elevated CA19-9 levels was significantly higher than that in the normal CA19-9 group (88.89% vs. 26.09%, P<0.05). Conversely, the incidence of concomitant lymph node involvement was significantly lower in the elevated CA19-9 group compared to the normal CA19-9 group (22.22% vs. 56.52%, P<0.05).
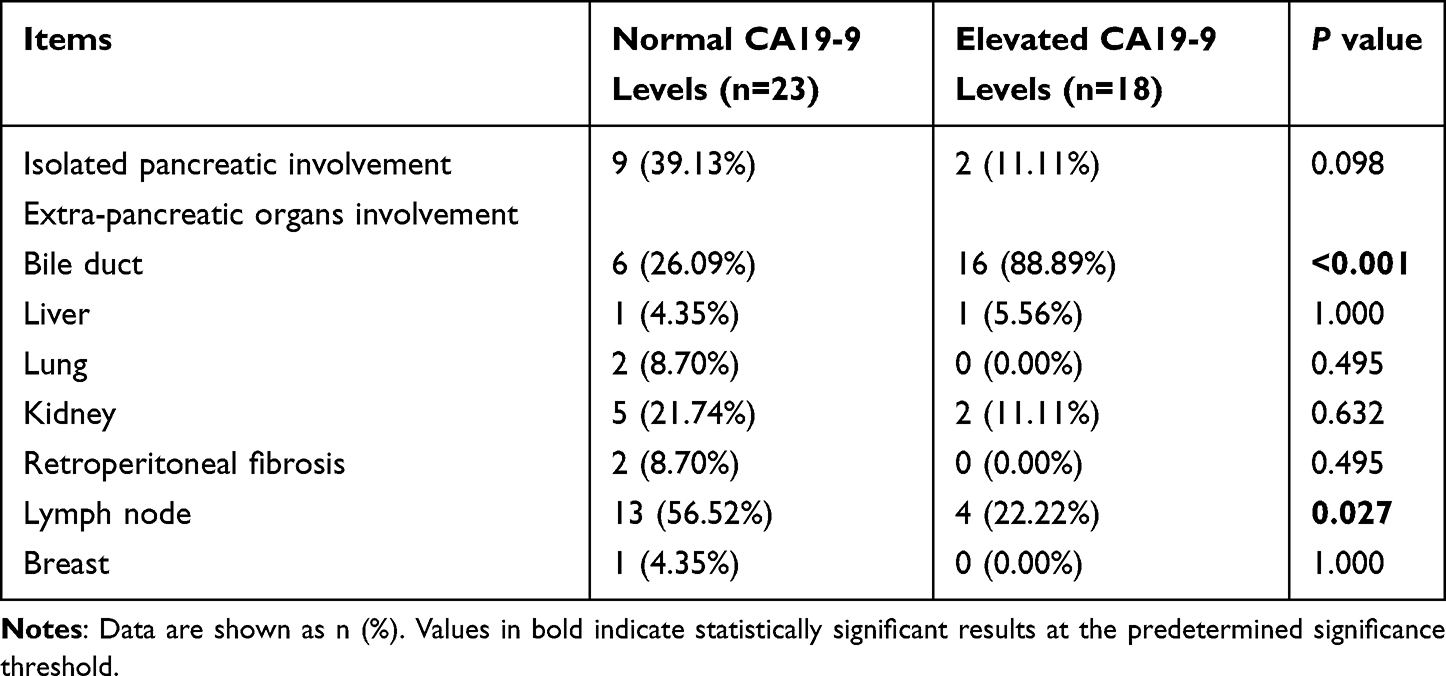 |
Table 2 Comparison of Affected Organs Between IgG4-AIP Patients with Normal and Elevated CA19-9 Levels |
Comparison of Laboratory Tests Between the Normal CA19-9 Level Group and the Elevated CA19-9 Level Group of Patients with IgG4-AIP
The results of the comparison of laboratory indicators between IgG4-AIP patients with normal and elevated CA19-9 levels are presented in Table 3. In this study, liver function tests were performed in all 41 patients with IgG4-AIP at the time of hospital admission. The results indicated that among the 41 IgG4-AIP patients, the median total bilirubin (TBIL) level was 32.55 (IQR: 9.60–102.84) µmol/L, the median direct bilirubin (DBIL) level was 17.30 (IQR: 2.83–64.20) µmol/L, the median alanine aminotransferase (ALT) level was 106.00 (IQR: 22.00–256.50) U/L, the median aspartate aminotransferase (AST) level was 69.00 (IQR: 27.50–198.00) U/L, the median gamma-glutamyl transferase (GGT) level was 350.00 (IQR: 117.00–632.00) U/L, and the median alkaline phosphatase (ALP) level was 267.00 (IQR: 99.00–471.00) U/L. We observed that the median levels of TBIL [69.75 (IQR: 39.99–168.93) µmol/L vs. 11.10 (IQR: 6.64–37.48) µmol/L, P<0.05], DBIL [55.19 (IQR: 23.27–108.22) µmol/L vs. 3.40 (IQR: 2.70–22.78) µmol/L, P<0.05], ALT [232.50 (IQR: 126.50–397.25) U/L vs. 31.00 (IQR: 13.00–115.00) U/L, P<0.05], AST [183.00 (IQR: 118.25–245.25) U/L vs. 38.00 (IQR: 19.00–69.00) U/L, P<0.05], GGT [441.00 (IQR: 160.50–860.50) U/L vs. 132.65 (IQR: 23.50–467.48) U/L, P<0.05], and ALP [411.00 (IQR: 255.50–678.00) U/L vs. 102.50 (IQR: 63.00–293.00) U/L, P<0.05] in the elevated CA19-9 group were significantly higher than those in the normal CA19-9 group.
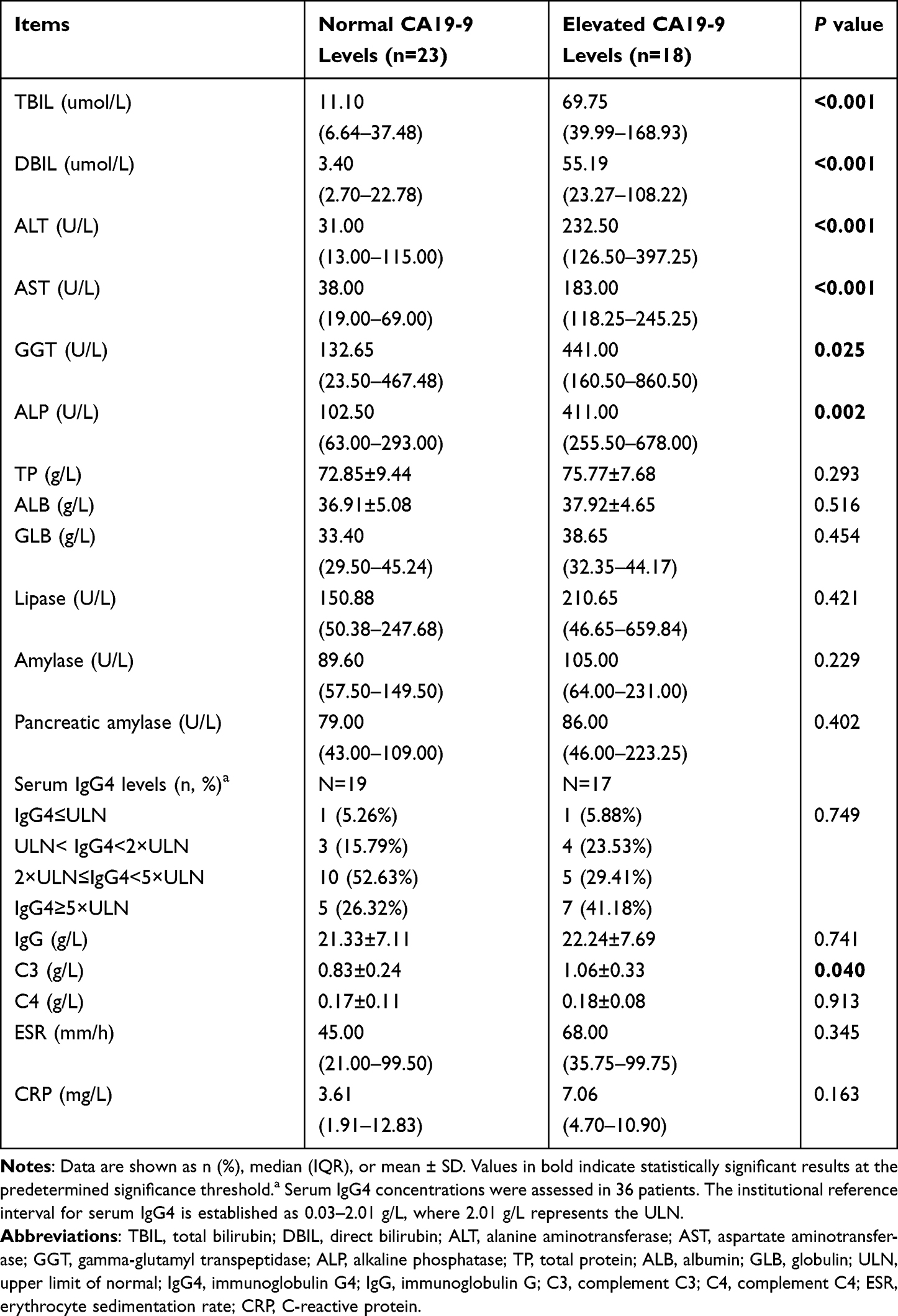 |
Table 3 Comparison of Laboratory Indicators Between IgG4-AIP Patients with Normal and Elevated CA19-9 Levels |
Additionally, in this study, C3 levels were measured in all 41 IgG4-AIP patients. The results showed that the mean C3 level was 0.94 ± 0.31 g/L. We found that the mean C3 level in the normal CA19-9 group was significantly lower than that in the elevated CA19-9 group (0.83 ± 0.24 g/L vs. 1.06 ± 0.33 g/L, P<0.05).
It is noteworthy that in this study, 36 IgG4-AIP patients underwent serum IgG4 level testing. In the normal CA19-9 group, the serum IgG4 levels were primarily concentrated in the range of 2×upper limit of normal (ULN) ≤IgG4<5×ULN (10 patients, 52.63%), while in the elevated CA19-9 group, the majority were in the range of IgG4≥5×ULN (7 patients, 41.18%). However, further statistical analysis revealed that there was no significant statistical difference in serum IgG4 levels between the normal and elevated CA19-9 groups (P>0.05).
Correlation Analysis Between CA19-9 Levels and Laboratory Indicators
We conducted a Spearman correlation analysis of CA19-9 levels with various laboratory parameters in the 41 IgG4-AIP patients (Table 4). The results indicated a moderate positive correlation between CA19-9 levels and TBIL (r=0.622, P<0.001), DBIL (r=0.635, P<0.001), ALT (r=0.642, P<0.001), AST (r=0.673, P<0.001), GGT (r=0.562, P<0.001), and ALP (r=0.655, P<0.001). Additionally, CA19-9 levels showed a weak positive correlation with total protein (TP) (r=0.418, P=0.007) and ESR (r=0.377, P=0.026).
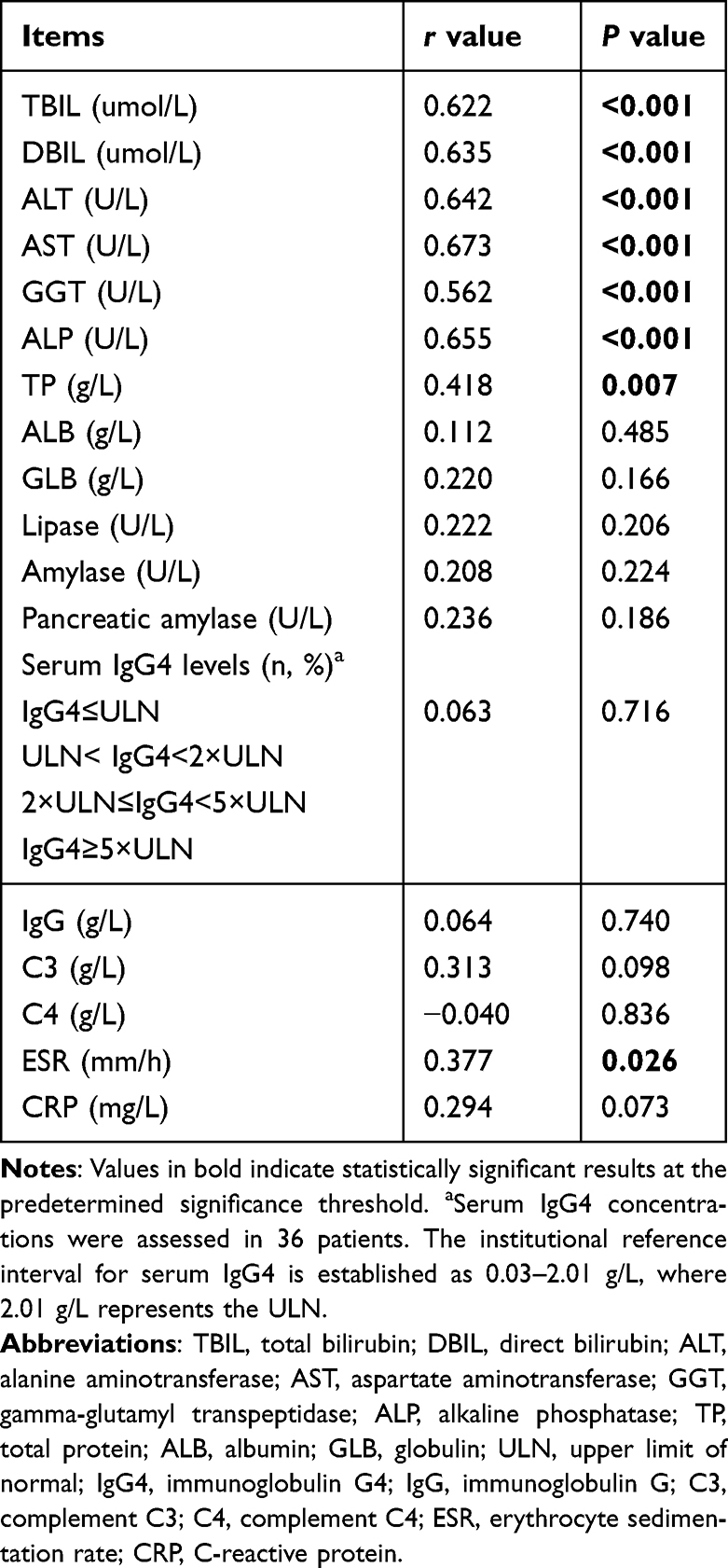 |
Table 4 Correlation Analysis Between CA19-9 Levels and Laboratory Indicators |
Imaging Features
In this study, all 41 IgG4-AIP patients underwent CT, MRI, or MRCP. Among the 23 patients with normal CA19-9 levels, 14 patients (60.87%) exhibited diffuse pancreatic enlargement, while 9 patients (39.13%) showed enlargement of the pancreatic head. In the 18 patients with elevated CA19-9 levels, 9 patients (50.00%) presented with diffuse pancreatic enlargement, and the other 9 patients (50.00%) displayed enlargement of the pancreatic head. Further statistical analysis revealed no significant differences in the pancreatic imaging findings between the normal and elevated CA19-9 groups (P>0.05).
Discussion
Elevated levels of CA19-9 are observed in some patients with IgG4-AIP, which may result in misdiagnosis as pancreatic tumors.16–20 This study compared and analyzed the clinical characteristics of IgG4-AIP patients with elevated versus normal CA19-9 levels, to improve clinicians’ understanding of the clinical value of CA19-9 in this disease.
Numerous cases of misdiagnosis of IgG4-AIP patients as pancreatic tumors have been reported in the literature.21–24 Our study further demonstrated that IgG4-AIP patients with elevated CA19-9 levels were more likely to be misdiagnosed as having pancreatic tumors compared to those with normal CA19-9 levels. This is primarily due to CA19-9 being the most commonly used tumor marker for the clinical diagnosis of pancreatic ductal adenocarcinoma (PDAC).25 Although IgG4-AIP is a benign autoimmune pancreatitis, some patients may still exhibit elevated CA19-9 levels. This phenomenon, where both benign and malignant conditions share the same elevated marker, is a major contributor to misdiagnosis. These findings suggest that clinicians should not automatically attribute elevated CA19-9 levels to malignancy; instead, they should consider other potential causes, particularly IgG4-AIP. We recommend conducting serum IgG4 testing when appropriate and considering endoscopic ultrasound-guided fine-needle aspiration biopsy to obtain a definitive pathological diagnosis, thereby avoiding unnecessary treatment interventions.
As a subtype of IgG4-RD,26,27 IgG4-AIP frequently involves extra-pancreatic organs.28–32 We further observed that IgG4-AIP patients with elevated CA19-9 levels were more prone to bile duct involvement, whereas those with normal CA19-9 levels were more commonly associated with lymph node involvement. This phenomenon may be related to the biological characteristics of CA19-9, which is primarily secreted by cholangiocytes and pancreatic ductal epithelial cells. We hypothesize that when IgG4-AIP affects the bile ducts, the inflammatory response in the biliary epithelial cells may enhance their secretory function, leading to elevated levels of CA19-9. In contrast, lymph node involvement in IgG4-AIP typically manifests as follicular hyperplasia and infiltration of IgG4-positive plasma cells, processes that do not directly engage the CA19-9 secreting cells and thus are less likely to cause fluctuations in CA19-9 levels. This finding suggests that CA19-9 levels may serve as a useful biomarker for predicting extra-pancreatic organ involvement in IgG4-AIP patients, aiding in the identification of those at greater risk for concurrent organ complications. Future studies should conduct larger-scale mechanistic investigations to further validate the role of CA19-9 in the organ-specific pathology of IgG4-AIP and its clinical significance.
We conducted a comparative analysis of laboratory parameters between IgG4-AIP patients with normal CA19-9 levels and those with elevated levels. The results indicated that patients in the elevated CA19-9 group had significantly higher levels of TBIL, DBIL, ALT, AST, GGT, and ALP compared to those in the normal CA19-9 group. Additionally, we observed a moderate positive correlation between CA19-9 levels and these biochemical markers. These findings further support the association between elevated CA19-9 levels and bile duct involvement in patients with IgG4-AIP. We hypothesize that inflammation and damage to the biliary system may trigger the release of CA19-9 into the bloodstream, accompanied by impaired bile flow, which in turn leads to elevated levels of bilirubin and hepatic enzymes. This pathophysiological mechanism may provide a plausible explanation for our observations. However, our findings are inconsistent with those reported by Chong et al regarding CA19-9 levels in IgG4-RD.12 Chong et al indicated that in IgG4-RD, patients with elevated CA19-9 levels did not show significantly higher bilirubin levels compared to those with normal CA19-9 levels. We believe this discrepancy may be attributed to differences in the study populations. Our research primarily focused on IgG4-AIP patients, whereas Chong et al’s study included all patients with IgG4-RD. Furthermore, the sample sizes for the normal and elevated CA19-9 groups in our statistical analysis were significantly larger than those in Chong et al’s study. These differences may have a substantial impact on the comparison of results. Importantly, despite the differences between our study and that of Chong et al, both studies found no statistically significant differences or correlations in serum IgG4 levels between the normal and elevated CA19-9 groups. This suggests that while elevated CA19-9 levels may be associated with bile duct involvement, changes in IgG4 levels in IgG4-AIP patients may not be directly influenced by CA19-9 levels, offering new avenues for further research. Future studies should continue to explore the variations of CA19-9 and related biochemical markers in different subtypes of IgG4-RD patients to gain a more comprehensive understanding of their clinical significance.
C3 is recognized as a significant biomarker in IgG4-RD.33–35 In this study, we observed that patients with IgG4-AIP who had normal CA19-9 levels exhibited significantly lower C3 levels compared to those with elevated CA19-9 levels. We speculate that elevated CA19-9 levels often indicate a higher disease activity in IgG4-AIP. At this stage, the immune system is highly activated, leading to a compensatory increase in the synthesis of C3 by the liver to counteract the intense immune inflammatory response. In contrast, patients in the normal CA19-9 group have relatively lower disease activity and weaker immune stimulation, resulting in a more stable state of C3 synthesis and consumption, which leads to lower levels of complement C3. However, it is important to note that our findings did not establish a significant correlation between C3 levels and CA19-9 concentrations. This suggests that the activation of the complement system may serve as an independent inflammatory marker, distinct from CA19-9. Therefore, clinicians should consider both CA19-9 and C3 levels concurrently when assessing the immune inflammatory status to achieve a more comprehensive clinical evaluation.
This study has certain limitations. First, due to its retrospective, single-center design and the relatively small number of included cases, there may be biases introduced in subgroup analyses. To enhance the scientific validity and applicability of the findings, future research will be conducted as multi-center, large-scale studies to more effectively reduce selection bias, thereby increasing the reliability and generalizability of the conclusions. Second, this study did not thoroughly investigate the prognostic differences between IgG4-AIP patients in the normal CA19-9 level group and those with elevated levels. Future studies will incorporate more comprehensive follow-up data to systematically assess the impact of CA19-9 levels on the prognosis of IgG4-AIP patients, providing a more solid foundation for individualized clinical treatment.
Conclusion
Therefore, the clinical characteristics of patients with elevated CA19-9 levels in IgG4-AIP are more complex. Clinicians should take into account the variations in CA19-9 levels when assessing and managing patients with IgG4-AIP, in order to develop individualized diagnostic and therapeutic strategies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Yichang Medical and Health Research Project (A24-2-008).
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Han D-G, Ying C-L, Cai Z-P, Tong Q-Y, Liu W. Comparative analysis of clinical characteristics in multi-organ and single-organ involvement of igg4-related disease: a single-center retrospective study. Arch Iran Med. 2025;28(5):303–10. doi:10.34172/aim.34027
2. Liu W, Wei DH, Tong QY. The bull’s-eye sign in liver: are they liver metastases? Gastroenterology. 2023;164(7):1056–1058. doi:10.1053/j.gastro.2022.12.020
3. Liu W, Dao-Hui W, Tong QY. Localized gastric wall thickening: it’s not what you think. Gastroenterology. 2023;165(1):e1–e2. doi:10.1053/j.gastro.2022.12.028
4. Han DG, Hou SR, Liu L, Liu W. Abdominal pain and vomiting by isolated retroperitoneal IgG4 lymphadenopathy. Dig Liver Dis. 2025;57(10):2021–2023. doi:10.1016/j.dld.2025.07.033
5. Han DG, Ying CL, Zhao TQ, Tong QY, Liu W. Clinical characteristics of IgG4-related lung disease: a single-center based experience. Clin Rheumatol. 2025;44(10):4159–4168. doi:10.1007/s10067-025-07678-4
6. Tan L, Guan X, Zeng T, et al. The significance of serum IgG(4) and CA19-9, autoantibodies in diagnosis and differential diagnosis of IgG(4)-related sclerosing cholangitis. Scand J Gastroenterol. 2018;53(2):206–211. doi:10.1080/00365521.2017.1416159
7. Okazaki K, Kawa S, Kamisawa T, et al. Amendment of the Japanese consensus guidelines for autoimmune pancreatitis, 2020. J Gastroenterol. 2022;57(4):225–245. doi:10.1007/s00535-022-01857-9
8. Shimosegawa T, Chari ST, Frulloni L, et al. International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the international association of pancreatology. Pancreas. 2011;40(3):352–358. doi:10.1097/MPA.0b013e3182142fd2
9. Han DG, Ying CL, Tian LG, Liu W, He Z. Comparative analysis of clinical features in diffuse and focal enlargement of IgG4-related autoimmune pancreatitis: a single-center retrospective study. Clin Rheumatol. 2025;44(10):4149–4157. doi:10.1007/s10067-025-07663-x
10. Cai Z-P, Fan F-C, Liu W. Vague upper abdominal pain—igg4-related pancreatitis. Indian J Surg. 2022;85(4):987–988. doi:10.1007/s12262-022-03594-y
11. Czakó L, Gyökeres T, Topa L, et al. Autoimmune pancreatitis in Hungary: a multicenter nationwide study. Pancreatology. 2011;11(2):261–267. doi:10.1159/000327092
12. Chong DH, Mattman A, Dou A, et al. Elevated CA19-9 in IgG4-related disease. Ann Clin Biochem. 2025:45632251370803. doi:10.1177/00045632251370803.
13. Farrukh L, Akhtar MF, Waqar HH, Peredo-Wende R. Significant CA 19-9 elevation in IgG4-related autoimmune pancreatitis - A diagnostic dilemma. Am J Med Sci. 2024;367(1):67–71. doi:10.1016/j.amjms.2023.09.016
14. Agarwal KK, Jassal R, Browne A, Hossain M, Akhtar R. Autoimmune pancreatitis masquerading as pancreatic cancer: a case report and literature review. Cureus. 2022;14(2):e21900. doi:10.7759/cureus.21900
15. Umehara H, Okazaki K, Kawa S, et al. The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD. Mod Rheumatol. 2021;31(3):529–533. doi:10.1080/14397595.2020.1859710
16. Karamya ZA, Kovács A, Illés D, et al. Prevalence of autoimmune pancreatitis in pancreatic resection for suspected malignancy: a systematic review and meta-analysis. BMC Gastroenterol. 2024;24(1):278. doi:10.1186/s12876-024-03367-9
17. Xi W, Liao W, Guo T, et al. CA19-9/DBil: a promising indicator to distinguish between CA19-9-elevated pancreatic head-type autoimmune pancreatitis and pancreatic head cancer. BMC Gastroenterol. 2025;25(1):306. doi:10.1186/s12876-025-03925-9
18. De Marchi G, Paiella S, Luchini C, Capelli P, Bassi C, Frulloni L. Very high serum levels of CA 19-9 in autoimmune pancreatitis: report of four cases and brief review of literature. J Dig Dis. 2016;17(10):697–702. doi:10.1111/1751-2980.12403
19. Chang MC, Liang PC, Jan S, et al. Increase diagnostic accuracy in differentiating focal type autoimmune pancreatitis from pancreatic cancer with combined serum IgG4 and CA19-9 levels. Pancreatology. 2014;14(5):366–372. doi:10.1016/j.pan.2014.07.010
20. van Heerde MJ, Buijs J, Hansen BE, et al. Serum level of Ca 19-9 increases ability of IgG4 test to distinguish patients with autoimmune pancreatitis from those with pancreatic carcinoma. Dig Dis Sci. 2014;59(6):1322–1329. doi:10.1007/s10620-013-3004-3
21. Li CR, Wang JC, Lin CH, Hsu JS. Focal IgG4-related autoimmune pancreatitis mimicking pancreatic tumor. Kaohsiung J Med Sci. 2021;37(8):741–742. doi:10.1002/kjm2.12380
22. Mohamed F, Vijayan B, Saraswat L. IgG4-related autoimmune pancreatitis mimicking pancreatic cancer: a report of two cases. Cureus. 2024;16(7):e65289. doi:10.7759/cureus.65289
23. Hsu WL, Chang SM, Wu PY, Chang CC. Localized autoimmune pancreatitis mimicking pancreatic cancer: case report and literature review. J Int Med Res. 2018;46(4):1657–1665. doi:10.1177/0300060517742303
24. Ruiz Rebollo ML, Álvarez-Quiñones-Sanz M, Fuertes Alija JJ, Izquierdo Santervás S. IgG4-related disease mimicking pancreatic tumour. Gastroenterol Hepatol. 2021;44(9):660–661. doi:10.1016/j.gastrohep.2020.07.021
25. Li Y, Cao Y, Zhang Y, et al. Diagnostic Value of Serum D-dimer, CA19-9, and CT imaging features in pancreatic ductal adenocarcinoma and benign pancreatic lesions. J Cancer. 2025;16(9):2812–2821. doi:10.7150/jca.111548
26. Lanzillotta M, Vujasinovic M, Löhr JM, Della Torre E. Update on autoimmune pancreatitis and igg4-related disease. United Eur Gastroenterol J. 2025;13(1):107–115. doi:10.1002/ueg2.12738
27. Maritati F, Peyronel F, Vaglio A. IgG4-related disease: a clinical perspective. Rheumatology. 2020;59(Suppl 3):iii123–iii31. doi:10.1093/rheumatology/kez667
28. Xu B, Cai ZP, Liu W. IgG4-related cholangiopathy, pancreatopathy and lymphadenopathy. Am J Med Sci. 2023;366(4):e60–e1. doi:10.1016/j.amjms.2023.05.009
29. Martín-Nares E, Hernández-Molina G, Baenas DF, et al. Performance of the 2019 American College of Rheumatology/European League Against Rheumatism Classification Criteria for IgG4-Related Disease in a Latin American Cohort. J Clin Rheumatol. 2024;30(2):52–57. doi:10.1097/rhu.0000000000002052
30. Van Moerkercke W, Verhamme M, Doubel P, Meeus G, Oyen R, Van Steenbergen W. Autoimmune pancreatitis and extrapancreatic manifestations of IgG4-related sclerosing disease. Acta Gastroenterol Belg. 2010;73(2):239–246.
31. Nadi A, Benhayoun Y, Cherkaoui R, Delsa H, Rouibaa F. Case series of autoimmune pancreatitis and igg4-related sclerosing cholangitis. Cureus. 2022;14(7):e26657. doi:10.7759/cureus.26657
32. Han DG, Ying CL, Tian LG, Liu W, He Z. A retrospective study on pancreatic and extra-pancreatic characteristics of IgG4-related disease. Clin Rheumatol. 2025;44(12):4975–4984. doi:10.1007/s10067-025-07707-2
33. Zhang N, Peng Y, Li R, et al. Elevated eosinophil-to-lymphocyte ratio (ELR) as a predictor of relapse for IgG4-related disease: a retrospective study across a decade. Clin Exp Med. 2025;25(1):193. doi:10.1007/s10238-025-01741-9
34. Fujita Y, Fukui S, Umeda M, et al. Clinical characteristics of patients with igg4-related disease complicated by hypocomplementemia. Front Immunol. 2022;13:828122. doi:10.3389/fimmu.2022.828122
35. Wang R, He D, Zhao L, et al. Role of complement system in patients with biopsy-proven immunoglobulin G4-related kidney disease. Hum Pathol. 2018;81:220–228. doi:10.1016/j.humpath.2018.07.008
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.