Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Elephantiasis Nostras Verrucosa: A Treated Case With Dietary Intervention and Acitretin
Authors Tsaqilah L ![]() , Octavia N, Hidayah RMN
, Octavia N, Hidayah RMN ![]() , Avriyanti E
, Avriyanti E ![]() , Dharmadji HP
, Dharmadji HP
Received 2 October 2023
Accepted for publication 24 November 2023
Published 11 December 2023 Volume 2023:16 Pages 3535—3539
DOI https://doi.org/10.2147/CCID.S438610
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Laila Tsaqilah, Nadia Octavia, Risa Miliawati Nurul Hidayah, Erda Avriyanti, Hartati Purbo Dharmadji
Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Laila Tsaqilah, Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin General Hospital, Jl. Pasteur No. 38, Bandung, West Java, 40161, Indonesia, Tel +62222032426 Ext 3449, Email [email protected]
Abstract: Elephantiasis nostras verrucosa (ENV) is a rare and extreme complication of chronic non-filarial lymphedema. It can lead to severe disfiguration of body parts, especially the lower extremities, and is characterized by non-pitting edema and papulonodules with a verrucose or cobblestone-like appearance. Obesity is a risk factor of ENV. Various treatments have been reported for ENV. A 52-year-old woman presented to our outpatient dermatology clinic with non-pitting edema, cobblestone-like papulonodules, and erythematous plaques on both legs for 2 years. Her medical history included morbid obesity with a body mass index of 44.8 kg/m2, hypertension, and type II diabetes mellitus. Biopsy specimens obtained from skin lesions showed multiple dilated lymph nodes throughout the papillary and reticular dermis. Doppler ultrasonography and lymphoscintigraphy revealed lymph stasis and lymphedema, respectively. Based on clinical, histopathological, and imaging findings, the final diagnosis was ENV. She was initially treated with conservative approaches such as compression stockings and dietary intervention for a month. She went on a low-calorie diet (1350 kcal/day) consisting protein 50.7 g/day, fat 32.5 g/day, and carbohydrate 202.7 g/day, for a month. Owing to the hyperkeratotic lesions, she was given oral acitretin 0.3 mg/kg/day. The dosage was increased to 0.6 mg/kg/day after one month. The lesions were slightly flattened after 2 months of therapy. Acitretin was ceased. Early identification is crucial for preventing morbidity in patients with ENV. Management of ENV is challenging for physicians because of the lack of definitive treatment and poor prognosis. In the management of ENV, it is crucial to treat underlying causes, such as obesity. Acitretin induces loosening and thinning of the hyperkeratotic stratum corneum. Thus, it can result in improvement of cutaneous ENV lesions.
Keywords: lymphedema, nutrition, obesity
Introduction
Elephantiasis nostras verrucosa (ENV) is a rare and extreme complication of chronic non-filarial lymphedema.1 Robust epidemiologic data on ENV is lacking. Exact data regarding the prevalence of this disorder are limited.2 ENV can lead to severe disfigurement of body parts, particularly the lower extremities, characterized by non-pitting edema and papulonodules with a verrucose or cobblestone-like appearance.1,3 The pathogenesis of ENV remains unclear, but some of the etiologies including genetic, infection, malignancy, trauma, radiation, venous stasis, and obesity.1,3,4 Those conditions caused obstruction and impaired lymphatic drainage. This will result in lymphedema.3,4 Obesity can disrupt lymphatic flow and result in lymphedema.3,4 Furthermore, chronic lymphedema can lead to ENV.1,4 Management of ENV is challenging.1,3 Currently, there is no established treatment guideline for ENV.5 Conservative, mechanical, medical, and surgical procedures are among the treatment options for ENV.3,5 To achieve significant improvement, the underlying cause of lymphatic obstruction, such as obesity, should be treated.1,6 In an obesity-related ENV, weight loss is one of the conservative treatment.7 Thus, nutrition intervention could be an option.7,8 Treatment with oral acitretin may also improve quality of life in ENV patients by causing hyperkeratotic stratum corneum loosening and thinning.9 This case report aimed to present a successful and rare case of ENV in an obesity patient treated with nutrition intervention and acitretin.
Case
A 52-year-old-woman presented to our hospital with bilateral leg swelling (Figure 1A), itchy erythematous (Figure 1B) and verrucous plaques (Figure 1C) on her lower legs that had persisted for 2 years. The skin lesions first appeared two years ago as itchy erythematous papules on her left thigh and bilateral leg swelling. These lesions eventually became erythematous plaques and appeared on both thighs. A year later, cobblestone-like papulonodules formed on the left lower leg. She visited a dermatologist and was diagnosed with common warts, treated with topical treatment, and there was no improvement. She denied having a family history of the same complaints.
 |
Figure 1 Clinical image of skin lesions before treatment. (A) Skin lesions on lower legs. (B) Erythematous plaques on left thigh. (C) Verrucous plaques on left lower leg. |
Clinical examination of the lesions revealed bilateral non-pitting edema, cobblestone-like papulonodules, and plaques on both legs. Her medical history included morbid obesity (body mass index (BMI) 44.8 kg/m2), hypertension, and type 2 diabetes mellitus. Doppler sonography (Figure 2A) and lymphoscintigraphy of the lower legs revealed lymphedema and lymphatic stasis. Histopathological examination revealed extensive fibrous tissue hyperplasia in the dermis, loss of sweat glands, and dilated lymph channels (Figure 2B). On the basis of these findings, a diagnosis of ENV was established.
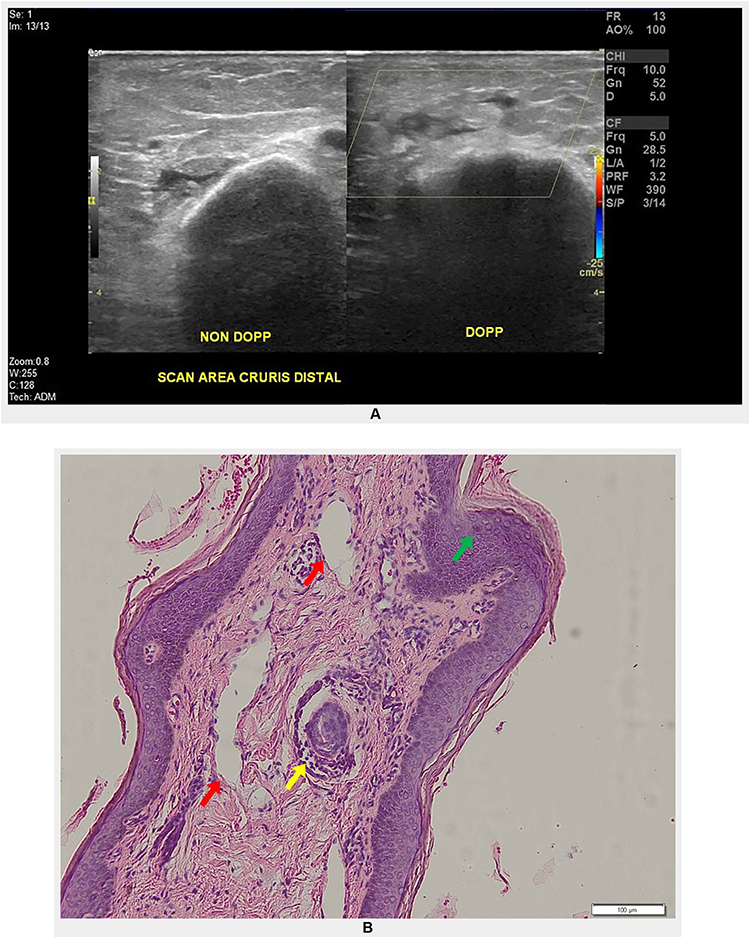 |
Figure 2 Histopathology and imaging. (A) Doppler ultrasonography. Multiple hypoechoic lesions on left leg showing avascularization indicate lymphedema (yellow box). (B) Histopathological results. Hyperkeratosis of the epidermis (green arrow), loss of sweat glands (yellow arrow), and dilated lymph vessels (red arrows) supported diagnosis of ENV. |
Patient received dietary intervention for weight reduction (low-calorie diet 1350 cal/day) and used compression stockings. There was an improvement in skin lesions after she lost 8 kg. She was commenced on oral acitretin that was administered at a dose of 0.3 mg/kg/day. The dosage was increased to 0.6 mg/kg/day after one month. After 2 months, partial resolution of skin lesions on her lower legs (Figure 3A), especially the erythematous plaques on her left thigh (Figure 3B), and verrucous plaques on left lower leg (Figure 3C) were observed.
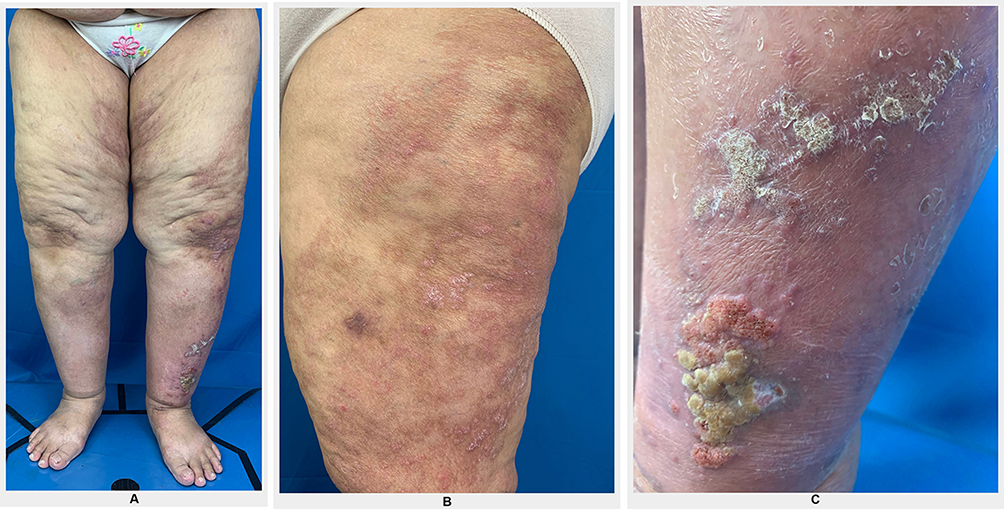 |
Figure 3 Clinical image of skin lesions 2 months after treatment. (A) Skin lesions on lower legs. (B) Erythematous plaques on left thigh. (C) Verrucous plaques on left lower leg. |
Discussion
Elephantiasis nostras verrucosa is a chronic, progressive, and difficult condition to treat.1 It results from impaired lymphatic drainage that subsequently leads to chronic lymphedema.4,6,9 Underlying obstructive causes of ENV include infection and non-infection.3 Infectious etiologies include filarial, staphylococcal, and streptococcal infections, while non-infectious include trauma, malignancy, radiation, venous stasis, and obesity.3,6,9 In obesity patient, excessive adipose tissue can impair lymphatic drainage and lead to the buildup of protein-rich lymphedema and associated fibrosis and inflammation.6 It is also related to increased activity of macrophages, keratinocytes, and adipocytes.10 Our patient’s morbid obesity might be a contributing factor in the development of ENV.
The diagnosis of ENV was established based on history taking, clinical examination, and histopathological results.3,10 Initially, cutaneous changes appeared as erythematous lesions and persistent edema.1 Later on, cutaneous changes of ENV appeared described as hypertrophic, verrucose, cobblestone-like appearance.6,9,11 Sites of predilection are in gravity-dependent parts of the body, particularly the lower extremities.4,5 Additional imaging procedures such as lymphangiography and lymphoscintigraphy can be beneficial to identify lymph obstruction.1 In this case report, cobblestone-like papulonodules, and plaques on lower legs were part of the clinical manifestations, along with bilateral non-pitting edema. We also performed lymphoscintigraphy, which revealed lymphatic stasis in both the lower legs. Histopathological changes of the ENV showed hyperkeratosis of the epidermis, loss of sweat glands, and dilated lymph vessels,3,10 which is similar to our patient.
Currently, there is no established standard of care for the treatment of ENV.1,3 The goal of treating ENV is to correct the underlying cause and prevent further complications.1,6 Lymphedema can be treated conservatively using compression stockings and lymphatic massages.3,5 Weight loss is another conservative treatment for obesity-associated ENV.6,7 Reduction of excessive adipose tissue can restore lymphatic drainage and improve skin lesions.6 After a low-calorie diet (1350 kcal/day) for a month, our patient successfully lost 8 kg (BMI reduced from 44.8 kg/m2 to 41.18 kg/m2). Her diet consisted of protein 50.7 g/day, fat 32.5 g/day, and carbohydrate 202.7 g/day. We also encouraged her to use the compression stockings. The verrucous and erythematous plaques on her lower legs were markedly flattened. Our findings are similar to those reported by Shaw et al12 in 251 lymphedema patients with BMI >26 kg/m2 that advised to reduce their intake to 1000–1200 kcal/day. As a result, the lymphedema improved within 12 weeks.
The use of oral retinoids, such as etretinate and acitretin, has been reported to be beneficial in reducing papillomatous and verrucous lesions.3,9,10 Acitretin is widely used to treat diverse hyperkeratotic disorders.9,11 The mechanism of action is to normalize keratinocyte proliferation and differentiation.9 Acitretin may induce degradation of collagen and reduce fibrosis. Thus, it will result in improvement of ENV lesions.11 Oral acitretin should be given at the initial stage of ENV to maximize the therapeutic effect.9,11 Bock et al9 reported 2 cases successfully treated with acitretin at a dose of 0.3 mg/kg/day then increased to 0.6 mg/kg/day after 1 month. Another patient showed improvement by given acitretin at a dose of 0.15 mg/kg/day and increased to 0.3 mg/kg/day after two months.9 We decided to give oral acitretin at a dose of 0.3 mg/kg/day. The dosage was increased to 0.6 mg/kg/day after 1 month. Soon after, her problems flared again owing to poor compliance and weight gain.
Conclusion
Diagnosis and effective therapy of ENV are challenging for physicians. Management options include conservative, mechanical, medical, and surgical intervention. Therefore, treatment decisions should be made on an individual basis. Early intervention for weight loss is important to prevent further sequelae in obese patients with ENV. Low-calorie diet (1350 kcal/day) for a month successfully induced weight loss in our patient. Oral acitretin is a useful alternative treatment option for ENV. Acitretin at a dose of 0.3 mg/kg/day for a month then increased to 0.6 mg/kg/day produced an ameliorating effect. Combination of both treatments was beneficial in improving skin lesions in her lower legs. Poor patient compliance is a crucial factor contributing to ENV advancement.
Ethic Statement
Publications of images were included in the patient’s consent to publish the case. Institutional approval was obtained for the publication of case details.
Consent Statement
The authors certify that they have obtained all appropriate patient consent forms. The patient signed a consent form for the publication of case details and images.
Acknowledgments
The authors would like to thank the staff of the Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liaw FY, Huang CF, Wu YC, Wu BY. Elephantiasis nostras verrucosa: swelling with verrucose appearance of lower limbs. Can Fam Physician. 2012;58(10):551–553.
2. Dean SM, Zirwas MJ, Horst AV. Elephantiasis nostras verrucosa: an institutional analysis of 21 cases. J Am Acad Dermatol. 2011;64(6):1104–1110. doi:10.1016/j.jaad.2010.04.047
3. Sisto K, Khachemoune A. Elephantiasis nostras verrucosa: a review. Am J Clin Dermatol. 2008;9(3):141–146. doi:10.2165/00128071-200809030-00001
4. Yosipovitch G, DeVore A, Dawn A. Obesity and the skin: skin physiology and skin manifestations of obesity. J Am Acad Dermatol. 2007;56(6):901–916. doi:10.1016/j.jaad.2006.12.004
5. Kar Keong N, Siing Ngi AT, Muniandy P, Voon Fei W. Elephantiasis nostras verrucosa: a rare complication of lower limb lymphoedema. BMJ Case Rep. 2017;28(8):1–3.
6. Baird D, Bode D, Akers T, Deyoung Z. Elephantiasis Nostras Verrucosa (ENV): a complication of congestive heart failure and obesity. J Am Board Fam Med. 2010;23(3):413–417. doi:10.3122/jabfm.2010.03.090139
7. Shimbo K, Okuhara Y, Yokota K. Hybrid treatment combining lymphaticovenous anastomoses and the oriental herbal medicine bofutsushosan for obesity-associated lower leg elephantiasis nostras verrucosa: a case report. Int J Low Extrem Wounds. 2020;20(3):282–284. doi:10.1177/1534734620932802
8. Eda Y, Arita Y, Ogasawara N, Hasegawa S. Tolvaptan for the treatment of elephantiasis nostras verrucosa. Intern Med. 2019;58(22):3347–3348. doi:10.2169/internalmedicine.2815-19
9. Bock VL, Lee S. Taming elephantiasis with Acitretin. Hong Kong J Dermatol Venereol. 2011;19:125–129.
10. Yoho RM, Budny AM, Pea AS. Elephantiasis nostras verrucosa. J Am Podiatr Med Assoc. 2006;96(5):442–444. doi:10.7547/0960442
11. Low DW, Jamil A, Nor NM. Case report Acitretin an additional treatment option for elephantiasis nostras verrucosa: a case report. Malays J Dermatol. 2017;6(38):79–82.
12. Shaw C, Mortimer P, Judd PA. A randomized controlled trial of weight reduction as a treatment for breast cancer-related lymphedema. Cancer. 2007;110(8):1868–1874. doi:10.1002/cncr.22994
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Age-Related Differences in Anthropometric and Lifestyle Factors Linked to Metabolic Syndrome in Women with Overweight and Obesity: A Cross-Sectional Study
Łuszczki E, Zielińska M, Oleksy Ł, Stolarczyk A, Dereń K
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1765-1781
Published Date: 28 May 2025