Back to Journals » Journal of Pain Research » Volume 14
Electromyography and Therapeutic Response to Lumbosacral Epidural Steroid Injections: A Systematic Review
Authors Meiling JB, Moman R ![]() , Pagan-Rosado R
, Pagan-Rosado R ![]() , Kinzelman-Vesely E, Hunt C, Hooten WM
, Kinzelman-Vesely E, Hunt C, Hooten WM ![]()
Received 1 July 2021
Accepted for publication 21 August 2021
Published 11 September 2021 Volume 2021:14 Pages 2851—2858
DOI https://doi.org/10.2147/JPR.S327504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishnan Chakravarthy
James B Meiling,1 Rajat Moman,2 Robert Pagan-Rosado,1 Elissa Kinzelman-Vesely,3 Christine Hunt,2,4 W Michael Hooten2,4
1Department of Physical Medicine and Rehabilitation, Mayo Clinic, Rochester, MN, USA; 2Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN, USA; 3Mayo Clinic Libraries, Rochester, MN, USA; 4Division of Pain Medicine, Mayo Clinic, Rochester, MN, USA
Correspondence: W Michael Hooten
Department of Anesthesiology and Perioperative Medicine, Division of Pain Medicine, Mayo Clinic, 200 First St SW, Rochester, MN, 55902, USA
Tel +1 507-266-9670
Email [email protected]
Abstract: The association between electromyography (EMG)-confirmed lumbosacral (LS) radiculopathy and pain outcomes following epidural steroid injection (ESI) has not been systematically summarized. The primary objective of this systematic review was to summarize the effects of EMG-confirmed LS radiculopathy on pain intensity following ESI. A secondary objective was to summarize the effects of EMG-confirmed LS radiculopathy on physical functioning following ESI. An a priori protocol was registered and a database search conducted by a reference librarian from January 2000 through December 2020. The search was date-limited to ensure the results of the systematic review represented contemporary clinical practice. Study-inclusion criteria included randomized trials, prospective and retrospective studies, cross-sectional studies, case series, and case reports, age ≥ 18 years, and use of EMG as a prognostic tool prior to an ESI. Two independent reviewers screened all titles, abstracts, and full texts. Data were extracted using a templated electronic database. The risk of bias was assessed using the Risk of Bias in Nonrandomized Studies of Interventions tool and certainty in evidence assessed using the Grading of Recommendations, Assessment, Development, and Evaluation approach. Due to clinical heterogeneity in study characteristics, a meta-analysis was not performed. A total of 454 studies were screened, and eight nonrandomized studies met the inclusion criteria. Five studies had a moderate risk of bias, two serious risks, and one a critical risk. The key findings included four of eight nonrandomized studies reporting a significant association between EMG-confirmed radiculopathy and ESI response and four of eight nonrandomized studies reporting no significant association. Important sources of bias limited interpretation of individual study findings, and multiple sources of clinical heterogeneity limited between-study comparisons. The findings of this systematic review demonstrate that associations existed between EMG-confirmed LS radiculopathy and pain outcomes after ESI in some, but not all studies. These results should be carefully interpreted with full understanding of the risk of bias and very low certainty in evidence that characterize the nonrandomized studies comprising this systematic review.
Keywords: electromyography, lumbosacral epidural steroid injection, systematic review
Plain-Language Summary
Positive electromyographic findings of radiculopathy were associated with greater levels of pain relief in some, but not all studies.
Introduction
Lumbosacral (LS) radiculopathy is a spinal condition characterized by impingement or damage to the lumbar spine nerve roots. Clinically, LS radiculopathy presents with a constellation of symptoms, including low-back and leg pain with or without lower-extremity paresthesia, numbness, or weakness.1 Electromyography (EMG) can play an important role in the diagnosis of LS radiculopathy when discordance exists between physical exam findings and the results of advanced imaging.1,2 EMG can also provide important information about the chronicity of nerve dysfunction and the presence or absence of active denervation.2 Because EMG is a widely available diagnostic test, a better understanding of its use to guide treatment could potentially improve the clinical outcomes of patients with LS radiculopathy.
Although use of electrodiagnostic studies to predict the clinical response to epidural steroid injections (ESIs) has been narratively reviewed,3 the association between EMG findings and pain outcomes following ESI have not been systematically summarized. The primary objective of this systematic review was to summarize the effects of EMG-confirmed LS radiculopathy on pain intensity following ESI. A secondary objective was to summarize the effects of EMG-confirmed LS radiculopathy on measures of physical functioning following ESI.
Methods
Study Protocol
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines were followed.4 An a priori protocol was followed and registered in the International Prospective Register for Systematic Reviews database (CRD42021227244).5
Search Strategy
A comprehensive database search was conducted for the dates of January 2000 through December 2020. The database search was date limited to ensure the results of the systematic review represent contemporary clinical practice. The databases included Ovid Medline Epub ahead of print, in process, and other nonindexed citations, daily and versions, Ovid Embase, Ovid Cochrane Central Register of Controlled Trials, Ovid Cochrane Database of Systematic Reviews, ACP Journal Club, Database of Abstracts of Reviews of Effects, Cochrane Clinical Answers, Cochrane Methodology Register, Health Technology Assessment, NHS Economic Evaluation Database, Scopus, and Web of Science. The search was designed and conducted by a reference librarian with input from the principal investigator. The search strategy and all search terms are presented in the supplemental materials document.
Study-Selection Process
Study-inclusion criteria were randomized trials, prospective and retrospective studies, cross-sectional studies, case series, studies involving adults aged ≥18 years,) use of EMG to identify LS radiculopathy prior to performing an ESI, and pain assessment following ESI. Exclusion criteria were conference abstracts and studies that did not include ESI or assessment of pain following ESI.
In the first review phase, two independent reviewers screened all titles and abstracts identified by the search strategy. In the second phase, two independent reviewers screened the full texts of all studies generated in the first review phase. Any disputes were resolved by consensus or involvement of a third party.
Data Extraction
Data were extracted by two independent reviewers in duplicate using a templated electronic database. Based on the a priori protocol, extracted data comprised authorship, publication year, study design, sample size, patient demographics, imaging results, ESI procedure, EMG results, follow-up, method used to assess post-ESI pain outcomes, and post-ESI pain scores. EMG results were categorized into three groups: EMG-confirmed positive for radiculopathy (Pos-EMG), EMG-confirmed negative for radiculopathy (Neg-EMG), and EMG-confirmed equivocal (Eqv-EMG) for radiculopathy.
Risk of Bias
Risk of bias was assessed using the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) tool.6 The ROBINS-I tool was developed to evaluate the risk of bias in the results of nonrandomized clinical studies that compare the effects of two or more interventions.
Certainty in Evidence
Certainty in evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach, adapted for use with quantitative data that are not combinable in meta-analysis.7,8
Evidence Synthesis
Due to clinical heterogeneity in study characteristics, a meta-analysis was not performed. As a result, the summary of findings is presented using a narrative approach. A narrative approach is indicated when a content area has been studied using disparate methods.9,10 This approach is useful when key clinical factors vary among studies. Narrative methods for evidence synthesis have been used to study various populations of patients with pain.11–16
Results
Characteristics of Included Studies
A flow diagram of the study-selection process is depicted in Figure 1. Eight studies met inclusion and exclusion criteria: four retrospective cohort studies,17–20 three prospective cohort studies,21–23 and one mixed prospective and retrospective cohort study24 (Table 1).
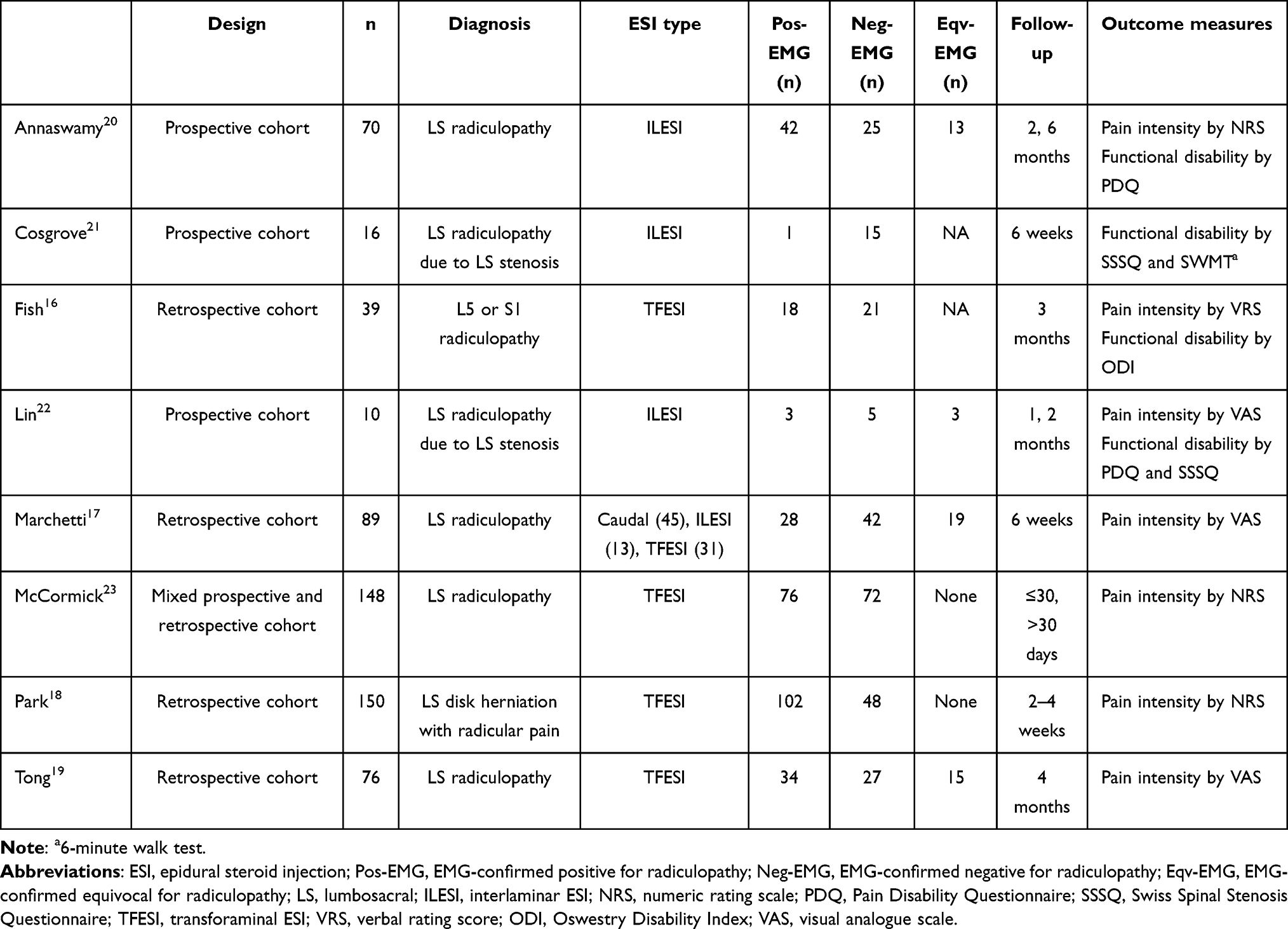 |
Table 1 Study characteristics |
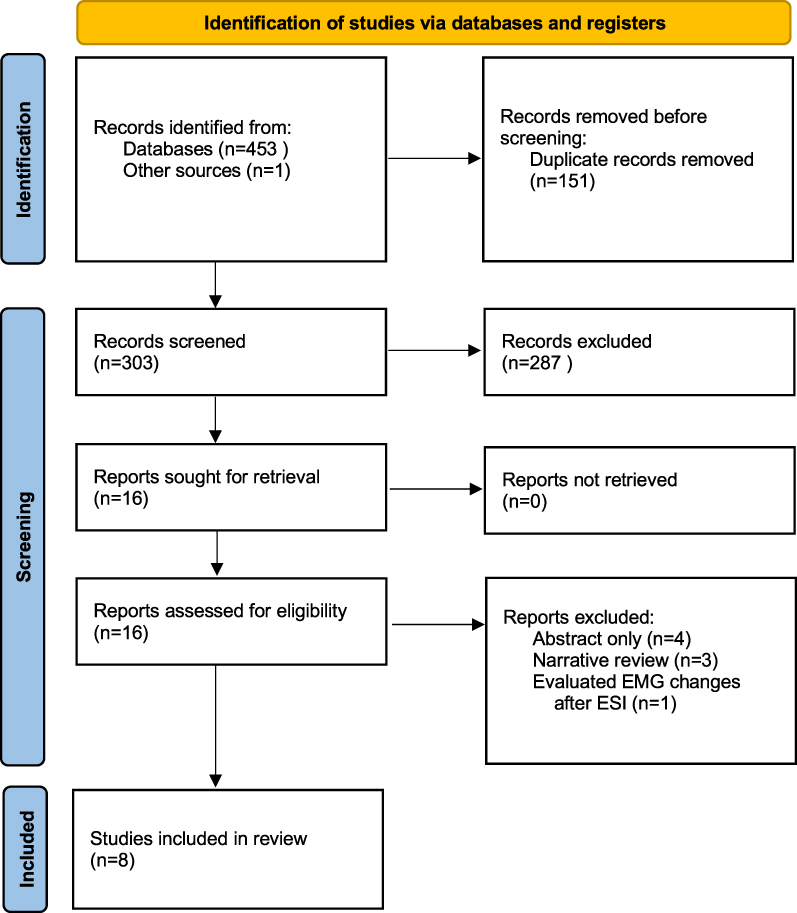 |
Figure 1 Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart of the study selection process. Notes: Adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.4. |
EMG and Radiculopathy
In three studies, the EMG tecnicians were certified by the American Board of Electrodiagnostic Medicine (ABEM),21–23 but the ABEM board–certified status of those in the remaining five studies had not been specified.17–19, 24 In seven studies,17–22, 24 five to six paravertebral and lower-extremity muscles had been screened. Criteria for Pos-EMG included evidence of denervation characterized by positive sharp waves or fibrillations in two or more muscles innervated by the same nerve root, but different peripheral nerves. Criteria for Neg-EMG included the absence of Pos-EMG radicular findings or definitive findings of an alternative diagnosis, such as peripheral neuropathy. In four studies,18,20,21,23 criteria for Eqv-EMG included denervation in a single muscle instead of two, limb-musculature denervation with the absence of paraspinal musculature findings, or if another peripheral process could not be reliably excluded as an alternative diagnosis.
Significant Associations Between Pos-EMG and ESI Outcomes
The statistical test results of each study are presented in the supplemental materials document. Fish et al17 performed a retrospective cohort study of 39 patients with L5 or S1 radiculopathies who received unilateral transforaminal ESI at L4/5, L5/S1, or both. At month 3 follow-up, no significant difference in mean verbal pain-rating scores was observed between the Pos-EMG and Neg-EMG groups. Mean month 3 Oswestry Disability Index score was significantly greater in the Pos-EMG than the Neg-EMG group.
Annaswamy et al21 conducted a prospective cohort study of 70 patients with a history of LS radiculopathy who received interlaminar ESIs. The initial cohort comprised 89 adults, but 19 were excluded, due to EMG not being performed (n=7), incomplete EMG data (n=2), interlaminar ESI not performed (n=2), and (4) months 2 and 6 follow-up assessments not completed (n=8). EMG was not used to designate the level of ESI. Individuals in the Pos-EMG group reported significantly greater improvement in pain on a numeric rating scale (NRS) from baseline to months 2 and 6 follow-up than the Neg-EMG group. A total of 43 (55%) of 78 individuals, including the 70 from the final cohort and the eight who did not complete the follow-up assessments, received a second interlaminar ESI, although the proportion of Pos- versus Neg-EMG individuals was not reported. Individuals in the Pos-EMG group also reported significantly greater improvement in total Pain Disability Questionnaire (PDQ) scores and functional subscores from baseline to months 2 and 6 follow-up than the Neg-EMG group. A nonsignificant change in PDQ psychosocial subscores from baseline to month 2 follow-up was observed. Finally, individuals in the Neg-EMG group demonstrated significant improvements in pain-drawing scores, specifically less-lower extremity pain, from baseline to months 2 and 6 follow-up compared to the Pos-EMG group.
McCormick et al24 conducted a mixed prospective and retrospective cohort study of 148 individuals with LS radiculopathy who had received a transforaminal ESI. EMG was used to clarify or confirm the diagnosis of radiculopathy, but it was uncertain whether EMG was used to designate the level of the ESI. In sum, 22 individuals had cervical radiculopathy, and these data were omitted from this systematic review. A significantly greater proportion of individuals in the Pos-EMG group experienced >50% reduction in baseline NRS pain scores at >30-day follow up compared to the Neg-EMG group. At follow-up of ≤30 days, no significant group differences in change in pain scores was observed. Myotomal spontaneous activity results were not reported separately for the LS and cervical radiculopathy groups, and thus the LS data could not be independently evaluated.
Lin et al23 performed a prospective cohort study of eleven adults with LS radiculopathy due to lumbar spinal stenosis who received an interlaminar ESI. The Eqv-EMG and Pos-EMG groups were combined, and one individual in the Eqv-EMG group did not receive an ESI or complete all follow-up assessments. Individuals in the combined Pos-EMG group reported statistically greater improvement in PDQ and visual analogue scale (VAS) pain scores at month 1 follow-up than the Neg-EMG group.
No Significant Associations Between Pos-EMG and ESI Outcomes
Tong et al20 conducted a retrospective cohort study of 76 individuals with LS radiculopathy who had received a transforaminal ESI. On univariate analysis, Pos-EMG was significantly associated with greater reductions in VAS pain scores (R=−0.25, P=0.04); however, this was not significant on multivariate regression analysis when the two factors of litigation and workers’ compensation were controlled for.
Marchetti et al18 conducted a retrospective cohort study of 89 individuals with LS radiculopathy who had received caudal (n=45), transforaminal (n=31), or interlaminar (n=13) ESIs. ESI level was determined by a combination of MRI results, clinical symptoms, and EMG results. Follow-up was 11–128 days after ESI. The proportion of individuals reporting >50% reduction in VAS low-back and leg pain scores was similar across all three EMG groups.
Cosgrove et al22 conducted a prospective cohort study of 16 patients with LS radicular symptoms due to lumbar spinal stenosis who received interlaminar ESIs. The ESI could be repeated at 2-week intervals so that individuals received one to three injections, with an average of 2.4. The number of individuals receiving more than one ESI was not reported. Only one of 16 patients had a Pos-EMG result, which limited interpretation of the study findings. Improvement in walking ability and functional status was seen post-ESI, regardless of EMG results.
Park et al19 conducted a retrospective cohort study of 150 patients with MRI-confirmed LS disk herniations resulting in radiculopathy who had received transforaminal ESIs. The primary outcome was >50% reduction in NRS pain scores from baseline to follow-up at 2–4 months. EMG was not used to designate the level of ESI. No significant difference in the proportion of patients who experienced >50% reduction in pain scores was observed between the Pos-EMG and Neg-EMG groups. Similarly, no significant difference in the presence of motor-unit action-potential changes was observed between patients who experienced >50% pain reduction compared to those who experienced <50% pain reduction. On univariate analysis, Pos-EMG patients with positive sharp waves and fibrillations were more likely to experience >50% pain reduction than Pos-EMG patients without these EMG changes. A significant association between positive sharp waves, fibrillations, and the likelihood of experiencing >50% pain reduction was retained on multivariate logistic regression analysis.
Risk of Bias
The risk-of-bias assessment demonstrated that five studies had a moderate risk of bias,17–20,24 two serious risks,21,23 and one a critical risk of bias22 (Table 2). Three studies were judged as having moderate risk of bias for confounding because of poor reporting,24 planned use of multiple interventions,18 or planned use of interventions due to aspecific treatment effects.21 One study was judged to have a critical risk of bias for selection due to a very small Pos-EMG sample22 and one to have a moderate risk of bias for using nonuniform data from multiple institutions.24 Two studies were judged as having a serious risk of bias for protocol deviations related to performing multiple ESIs.21,22 One study was found to have a serious risk of bias for including results from a patient that did not complete the study.23 Three studies were judged as having a serious risk of bias for outcome measurements, due to reinjection data being intermixed with single-intervention data17,21 or combining the data of two groups in the reported results.23 Another three studies in this domain were judged to have a moderate risk of bias due to insufficient or highly variable follow-up18,19 or intermixed data that were difficult to interpret.24 Three studies were judged as having a moderate risk of bias for selection of reported results because the statistical significance of the study findings had been inaccurately reported17,21 or the actual data incompletely reported.20 One study in this same domain was judged to have a serious risk of bias for reporting correlations without supporting data.23
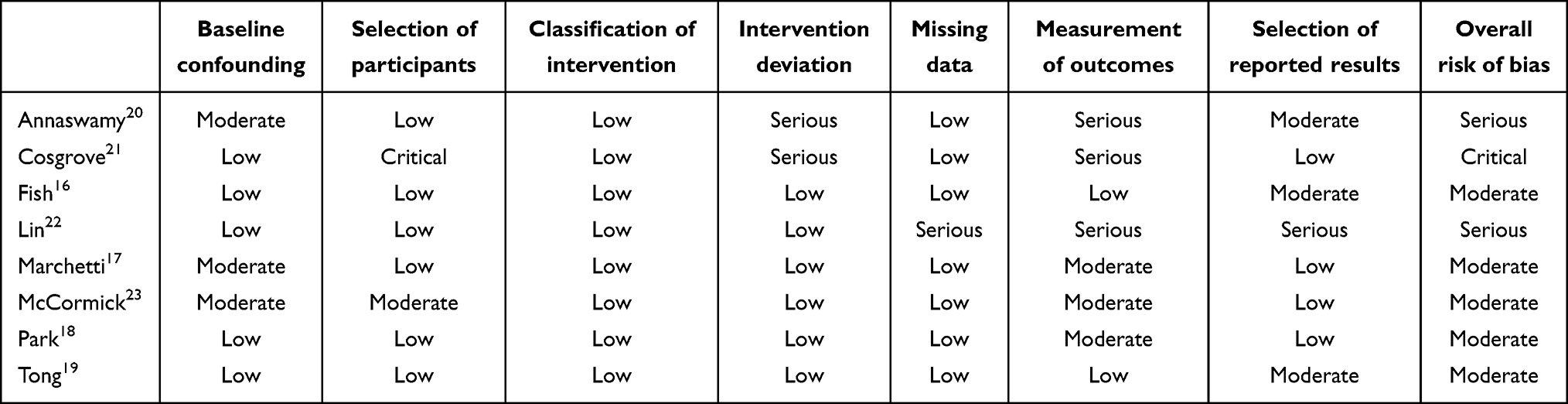 |
Table 2 Risk of bias using the Risk of Bias in Nonrandomized Studies of Interventions tool |
Certainty of Evidence
The GRADE assessment indicated that certainty in the evidence was very low due to nonrandomized study designs, small samples, heterogeneity of interventions used, heterogeneity in outcome assessment, and risk of bias.
Discussion
The key findings of this systematic review include four of eight nonrandomized studies reporting a significant association between Pos-EMG and ESI response and four of eight reporting no significant association between Pos-EMG and ESI response. Important sources of bias limited interpretation of individual study findings, and multiple sources of clinical heterogeneity limited the comparison of study findings.
The lack of a consistent association between EMG changes in radiculopathy and pain-intensity outcomes of ESIs warrants further consideration. While a majority of the studies assessed EMG evidence of denervation, only two assessed EMG evidence of reinnervation.17,19 EMG changes in denervation, such as increased insertional activity, positive sharp waves, and fibrillations, are first seen at the paraspinal level within 10–14 days after injury.25,26 Similar changes gradually involve the proximal and distal musculature during the 3 weeks after injury. Acute radiculopathy exhibits changes in denervation, but reinnervation is associated with polyphasia and large-amplitude motor-unit action potentials.26 Over several months, changes in denervation subside and EMG findings indicating reinnervation can be detected.27 A diagnosis of radiculopathy on reinnervation changes alone may indicate identification of a chronic radiculopathy that is symptomatic.25,26 The inclusion criteria of two studies specified temporal parameters for the duration of radicular symptoms.22,24 The minimum duration of radicular symptoms in the Cosgrove et al22 study was ≥1 month, but approximately 50% of patients reported intermittent symptoms extending beyond 1 year. In the McCormick et al24 study, EMG was required within 6 months prior to the ESI, but no other information about the timing of EMG was reported. Based on the temporal course of EMG evidence indicating radiculopathy and the absence of information about the temporal parameters of radicular symptoms and EMG being conducted, it is posited that a proportion of patients classified as Eqv-EMG or Neg-EMG due to the absence of denervating changes may have had EMG evidence of reinnervation indicating the presence of symptomatic chronic radiculopathy. This may explain in part why some patients with Eqv-EMG or Neg-EMG findings experienced improvements in pain after the ESI, despite the lack of reported EMG evidence of radiculopathy.
The findings of this systematic review have important implications for future research. First, randomized controlled trials are needed to determine the effects of ESIs on EMG-confirmed radiculopathy. Although the feasibility of completing a fully powered, sham-controlled ESI trial is low, a randomized trial using a wait-list control design may be a pragmatic alternative. This design enhances feasibility by ensuring all subjects have access to the study intervention. Second, the findings of this systematic review demonstrate the importance of carefully delineating the duration of radicular symptoms and timing of EMG. Third, the study findings demonstrate the importance of reporting EMG evidence of both denervation and reinnervation. Fourth, in a prospective study involving 46 patients with unilateral L5 radiculopathy published after the specified search dates of this systematic review, the L5 paraspinal mapping score was significantly lower in patients experiencing >80% improvement in pain intensity compared to those who reported <80% pain improvement at 3-month follow up.28 These data suggest that paraspinal mapping should be considered for inclusion in future clinical trials. Fifth, the level of the ESI should be consistently reported and performed using a standardized approach. Finally, the reported pain outcomes identified in this systematic review provide an estimate of the ESI-treatment effect that can be used in sample-size calculations of future studies.
This review has limitations. Although a comprehensive search strategy of the contemporary medical literature identified 454 records, only eight nonrandomized studies met the criteria for inclusion, and thus randomized trials are needed. Most identified studies had significant sources of clinical heterogeneity and bias, which limited the opportunity to perform a meta-analysis of the study findings. More specifically, important sources of clinical heterogeneity included use of an interlaminar versus a transforaminal approach to the epidural space, variations in determining the spinal level targeted for an ESI, and the potential impact of inaccurate needle placement on the reported EMG results.29,30
In conclusion, the findings of this systematic review suggest associations exist between Pos-EMG–confirmed LS radiculopathy and pain outcomes following ESI in some, but not all studies. These results should be carefully interpreted with the full understanding of the risk of bias and very low certainty in evidence that characterize the nonrandomized studies comprising this systematic review. Our results provide important information that can be used to develop future randomized trials designed to further investigate the associations between EMG-confirmed LS radiculopathy and pain outcomes following ESI. From a pragmatic clinical perspective, this systematic review provides the basis for using EMG in clinical practice to aid in determining the spinal level for an ESI and identifying patients who may be more likely to respond to an ESI.
Funding
No funds were used to produce this work.
Disclosure
Dr Christine Hunt reports grants from Abbott and Nevro outside the submitted work. The authors have no other conflicts of interest to report.
References
1. Hooten WM, Cohen SP. Evaluation and treatment of low back pain: a clinically focused review for primary care specialists. Mayo Clin Proc. 2015;90(12):1699–1718. doi:10.1016/j.mayocp.2015.10.009
2. Sandoval AE. Electrodiagnostics for low back pain. Phys Med Rehabil Clin N Am. 2010;21(4):767–776. doi:10.1016/j.pmr.2010.06.007
3. Barrette K, Levin J, Miles D, Kennedy DJ. The value of electrodiagnostic studies in predicting treatment outcomes for patients with spine pathologies. Phys Med Rehabil Clin N Am. 2018;29(4):681–687. doi:10.1016/j.pmr.2018.06.004
4. Page MJ, McKenzie JE, Bossuyt PM, et al. The prisma 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
5. Meiling J, Rosando RP, Hunt C. The prognostic benefit of needle electromyography in predicting therapeutic response to lumbosacral epidural steroid injection. Prospero: International prospective register of systematic reviews; 2021:CRD42021227244. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=227244.
6. Sterne JA, Hernan MA, Reeves BC, et al. Robins-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi:10.1136/bmj.i4919
7. Murad MH, Mustafa RA, Schunemann HJ, Sultan S, Santesso N. Rating the certainty in evidence in the absence of a single estimate of effect. Evid Based Med. 2017;22(3):85–87. doi:10.1136/ebmed-2017-110668
8. Murad MH. Clinical practice guidelines: a primer on development and dissemination. Mayo Clin Proc. 2017;92(3):423–433. doi:10.1016/j.mayocp.2017.01.001
9. Wong G, Greenhalgh T, Westhort G, Pawson R. Development of methodological guidance, publication standards and training materials for realist and meta-narrative reviews: the RAMESES (realist and meta-narrative evidence syntheses - evolving standards) project. Health Serv Deliv Res. 2014;2(30):1–278. doi:10.3310/hsdr02300
10. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O, Peacock R. Storylines of research in diffusion of innovation: a meta-narrative approach to systematic review. Soc Sci Med. 2005;61(2):417–430. doi:10.1016/j.socscimed.2004.12.001
11. Hooten WM, Dvorkin J, Warner NS, Pearson AC, Murad MH, Warner DO. Characteristics of physicians who prescribe opioids for chronic pain: a meta-narrative systematic review. J Pain Res. 2019;12:2261–2289. doi:10.2147/JPR.S202376
12. MacNeela P, Doyle C, O’Gorman D, Ruane N, McGuire BE. Experiences of chronic low back pain: a meta-ethnography of qualitative research. Health Psychol Rev. 2015;9(1):63–82. doi:10.1080/17437199.2013.840951
13. Sim J, Madden S. Illness experience in fibromyalgia syndrome: a metasynthesis of qualitative studies. Soc Sci Med. 2008;67(1):57–67. doi:10.1016/j.socscimed.2008.03.003
14. Toye F, Seers K, Allcock N, et al. Patients’ experiences of chronic non-malignant musculoskeletal pain: a qualitative systematic review. Br J Gen Pract. 2013;63(617):e829–841. doi:10.3399/bjgp13X675412
15. Wong AYL, Forss KS, Jakobsson J, Schoeb V, Kumlien C, Borglin G. Older adult’s experience of chronic low back pain and its implications on their daily life: study protocol of a systematic review of qualitative research. Syst Rev. 2018;7(1):81. doi:10.1186/s13643-018-0742-5
16. Snelgrove S, Liossi C. Living with chronic low back pain: a metasynthesis of qualitative research. Chronic Illn. 2013;9(4):283–301. doi:10.1177/1742395313476901
17. Fish DE, Shirazi EP, Pham Q. The use of electromyography to predict functional outcome following transforaminal epidural spinal injections for lumbar radiculopathy. J Pain. 2008;9(1):64–70. doi:10.1016/j.jpain.2007.08.011
18. Marchetti J, Verma-Kurvari S, Patel N, Ohnmeiss DD. Are electrodiagnostic study findings related to a patient’s response to epidural steroid injection? PM R. 2010;2(11):1016–1020. doi:10.1016/j.pmrj.2010.07.002
19. Park DY, Kang S, Park JH. Factors predicting favorable short-term response to transforaminal epidural steroid injections for lumbosacral radiculopathy. Medicina (Kaunas. 2019;55(5):162.
20. Tong HC, Williams JC, Haig AJ, Geisser ME, Chiodo A. Predicting outcomes of transforaminal epidural injections for sciatica. Spine J. 2003;3(6):430–434. doi:10.1016/S1529-9430(03)00179-7
21. Annaswamy TM, Bierner SM, Chouteau W, Elliott AC. Needle electromyography predicts outcome after lumbar epidural steroid injection. Muscle Nerve. 2012;45(3):346–355. doi:10.1002/mus.22320
22. Cosgrove JL, Bertolet M, Chase SL, Cosgrove GK. Epidural steroid injections in the treatment of lumbar spinal stenosis efficacy and predictability of successful response. Am J Phys Med Rehabil. 2011;90(12):1050–1055. doi:10.1097/PHM.0b013e31822dea76
23. Lin CK, Borresen A, Kroll M, Annaswamy TM. Predicting response to epidural steroid injections for lumbar spinal stenosis with biomarkers and electromyography. PM R. 2020;12(7):663–670. doi:10.1002/pmrj.12272
24. McCormick Z, Cushman D, Caldwell M, et al. Does electrodiagnostic confirmation of radiculopathy predict pain reduction after transforaminal epidural steroid injection? A multicenter study. J Nat Sci. 2015;1(8):e140.
25. Dillingham TR. Evaluating the patient with suspected radiculopathy. PM R. 2013;5(5 Suppl):S41–S49. doi:10.1016/j.pmrj.2013.03.015
26. Wilbourn AJ, Aminoff MJ. Aaee minimonograph #32: the electrophysiologic examination in patients with radiculopathies. Muscle Nerve. 1988;11(11):1099–1114. doi:10.1002/mus.880111102
27. Barr K. Electrodiagnosis of lumbar radiculopathy. Phys Med Rehabil Clin N Am. 2013;24(1):79–91. doi:10.1016/j.pmr.2012.08.011
28. Leblebicier MA, Gunduz OH, Kaplan BM, Ercalik T. Role of paraspinal mapping before transforaminal epidural injections for lumbar radiculopathy. Turk J Phys Med Rehab. 2021;67(2):196–202. doi:10.5606/tftrd.2021.5042
29. Goodmurphy C, Chiodo A, Haig A. The accuracy of needle placement in extremity muscles: a blinded study. J Clin Neurophysiol. 2007;24(4):366–378. doi:10.1097/WNP.0b013e3180ca9724
30. Haig AJ, Goodmurphy CW, Harris AR, Ruiz AP, Etemad J. The accuracy of needle placement in lower-limb muscles: a blinded study. Arch Phys Med Rehabil. 2003;84(6):877–882. doi:10.1016/S0003-9993(03)00014-5
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.