Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Electroacupuncture Reduces Waistline in Patients with Abdominal Obesity: A Randomized Controlled Trial with Mechanistic Analysis of Lipidomic and Intestinal Microbiota
Authors Chen X ![]() , Zhang Y, Fu C, Huang M, Wei D, Zhou W, Liu Y, Huang B, Rao Y, Zhang Y, Xia H, Hu Y, Li H, Huang W
, Zhang Y, Fu C, Huang M, Wei D, Zhou W, Liu Y, Huang B, Rao Y, Zhang Y, Xia H, Hu Y, Li H, Huang W ![]() , Zhou Z
, Zhou Z
Received 8 July 2025
Accepted for publication 14 September 2025
Published 30 September 2025 Volume 2025:18 Pages 3649—3669
DOI https://doi.org/10.2147/DMSO.S551806
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Donald McClain
Xia Chen,1– 4 Yanji Zhang,1– 4 Chengwei Fu,1– 4 Mengyuan Huang,5 Dan Wei,1– 4 Wei Zhou,1– 4 Yiran Liu,1– 4 Bei Huang,1– 4 Yingyue Rao,5 Yingrong Zhang,5 Hongjie Xia,5 Yaxin Hu,5 Hui Li,6 Wei Huang,1– 4 Zhongyu Zhou1– 4
1Department of Acupuncture, Hubei Provincial Hospital of Traditional Chinese Medicine, Wuhan, People’s Republic of China; 2Hubei Shizhen Laboratory, Wuhan, People’s Republic of China; 3Department of Acupuncture, Affiliated Hospital of Hubei University of Chinese Medicine, Wuhan, People’s Republic of China; 4Hubei Provincial Clinical Research Center for Acupuncture and Moxibustion in Obesity Treatment, Wuhan, People’s Republic of China; 5College of Acupuncture and Orthopedics, Hubei University of Chinese Medicine, Wuhan, People’s Republic of China; 6Medical Department, Taixing People’s Hospital, Taixing, People’s Republic of China
Correspondence: Zhongyu Zhou, Department of Acupuncture, Hubei Provincial Hospital of Traditional Chinese Medicine, No. 4, Huayanshan, Wuhan, People’s Republic of China, Email [email protected] Wei Huang, Department of Acupuncture, Hubei Provincial Hospital of Traditional Chinese Medicine, No. 4, Huayanshan, Wuhan, People’s Republic of China, Email [email protected]
Background: Abdominal obesity is a major risk factor for metabolic diseases and certain cancers. Although lifestyle intervention is the cornerstone of treatment, maintaining weight reduction is challenging. Electroacupuncture (EA) has shown potential in improving abdominal obesity, but its underlying mechanisms remain unclear.
Objective: This randomized controlled trial evaluates the efficacy of electroacupuncture combined with lifestyle intervention for reducing waist circumference in adults with abdominal obesity, and explores potential mechanisms through lipidomics and intestinal microbiota analyses.
Methods: The studies were performed in Hubei Provincial Hospital of Traditional Chinese Medicine between July 2020 and March 2023. Sixty-eight patients with abdominal obesity and 34 matched – healthy controls (HC) were recruited. After randomization, patients with abdominal obesity received an 8-week EA treatment or sham electroacupuncture (SA) treatment followed by 24-week follow-up. The change of waistline was to evaluate the efficacy of EA. Serum and stool specimen of EA group (pre- and post-treatment) and HC were collected for lipid metabolism markers and intestinal microbiota analysis.
Results: Compared with baseline, the difference of waistline between EA and SA was 7.38 (95% CI, 2.88 to 11.87; P = 0.002) cm at the end of treatment (week 8) and 8.99 (95% CI, 4.48 to 13.50; P < 0.001) cm at the end of follow-up (week 32), respectively. Lipidomic analysis indicated that some lipid species previously found to differ between patients with abdominal obesity and healthy controls showed a trend toward reversal after EA treatment. Microbiota analysis showed that EA did not significantly alter overall richness, but the abundance of certain taxa changed, particularly Akkermansia muciniphila.
Trial Registration: ClinicalTrials, NCT04957134. Registered 30 June 2021, https://clinicaltrials.gov/study/NCT04957134?term=NCT04957134&rank=1.
Conclusion: Our findings suggest that electroacupuncture is effective and safe in reducing waistline in patients with abdominal obesity. These results provide preliminary evidence that its benefits may be related to changes in lipid metabolism and intestinal microbiota, although further studies are warranted.
Keywords: electroacupuncture, abdominal obesity, intestinal microbiota, lipidomics, randomized controlled trail
Introduction
Abdominal obesity, characterized by excessive fat around the organs in the abdomen, is a significant risk factor for various metabolic and chronic diseases.1 Evidence has shown that the abdominal obesity plays a more crucial role in the pathogenesis of other metabolic diseases and certain chronic diseases.2–4 Research, including meta-analyses, has highlighted its association with increased risks of colorectal and gastroesophageal cancers.5,6 Moreover, each 10 cm increase in waistline has been linked to an 11% higher risk of all-cause mortality.7 In response to these findings, the International Atherosclerosis Society and the International Chair on Cardiometabolic Risk Working Group have recommended that waist circumference be regarded as a ‘vital sign’ for assessing obesity-related health risks in routine clinical practice.8 Therefore, implementing effective strategies to reduce abdominal obesity is essential for improving overall health outcomes.
The European, American, and Chinese Endocrine Societies all emphasize that lifestyle interventions, including behavioral therapy, dietary modifications and physical exercise, remain the cornerstone of weight management.9–11 However, it demands high self-discipline and sustained efforts over at least six months to achieve significant improvements in body weight control.12,13 Moreover, studies on lifestyle intervention have shown that maintaining weight stability can be challenging, particularly when obesity is accompanied by metabolic changes.14
Preliminary studies have shown encouraging results regarding the efficacy of electroacupuncture (EA) in addressing abdominal obesity.15,16 A recent randomized controlled trial found that twice-weekly EA effectively reduced waist circumference in individuals with abdominal obesity, however, objective assessments such as lipid metabolism markers were not evaluated.17 Furthermore, a 2022 meta-analysis summarized the existing evidence on acupuncture for abdominal obesity, indicating potential benefits in reducing waist circumference and body weight, with only mild adverse events reported; however, the overall certainty of the evidence was very low due to methodological limitations and suboptimal study design.18 These findings highlight the need for well-designed, high-quality randomized controlled trials incorporating objective measures to rigorously evaluate the clinical efficacy of EA.
Obesity is associated with dyslipidemia and intestinal microbiota dysbiosis. Dyslipidemia is highly prevalent among individuals with obesity, affecting approximately 60–70% of patients.19 Lipids are a diverse class of hydrophobic organic compounds, encompassing cholesterol, fats and oils, and phospholipids.20 They serve essential functions in biological systems, such as energy storage and supply, constituting the structural framework of cellular membranes, and participating in signal transduction and various physiological regulatory processes.19,20 Prolonged energy surplus increases the synthesis of fatty acids and triglycerides, forming cytosolic lipid droplets stored in adipose tissue, leading to adipocyte hypertrophy and hyperplasia, and ultimately resulting in obesity.20
The intestinal microbiota is often conceptualized as a “virtual organ”, and its dysbiosis is closely associated with the development of metabolic diseases. Patients with obesity typically exhibit decreased microbial diversity, altered proportions of dominant taxa, and significant correlations between specific bacterial groups and clinical metabolic parameters.21–23 Under pathological conditions, microbiota-derived metabolites such as lipopolysaccharides (LPS) may translocate into the circulation through a compromised intestinal barrier, triggering inflammatory responses that disrupt lipid metabolism and contribute to lipid metabolism–related disorders. In contrast, short-chain fatty acids (SCFAs) can promote the secretion of glucagon-like peptide-1 (GLP-1), thereby enhancing satiety and improving insulin sensitivity.22 Moreover, other microbial metabolites, including secondary bile acids, act as signaling molecules that regulate glucose and lipid metabolism through receptors such as FXR and TGR5, ultimately influencing the development of metabolic diseases such as obesity.23
Especially, recent studies have highlighted that changes in the composition of intestinal microbiota can contribute to metabolic disorders, such as disturbances in lipid metabolism, which are implicated in obesity.24–27 Obese individuals often exhibit significant metabolic alterations compared to lean individuals, potentially influenced by specific intestinal microbial species associated with obesity and its metabolic complications.28 This underscores the synergistic role of intestinal microbiota and lipid metabolism in the pathophysiological process of obesity.
Experimental studies have demonstrated that EA can reserve disordered intestinal microbiota in obese models, thereby ameliorating obesity. This effect is characterized by an increase in beneficial bacteria such as Bacteroidota and Actinobacteria, and a reduction in harmful bacteria such as Firmicutes, shifting the microbial composition toward that of normal mice.29–31 To date, no studies have combined microbiota analysis and lipidomics to investigate the effectiveness of EA and elucidate its potential underlying mechanism by which it regulates lipid metabolism. However, whether EA alleviates abdominal obesity by modulating intestinal microbiota and lipid metabolism remains unclear. To address this gap, we conducted a randomized controlled trial to evaluate the efficacy of EA compared with sham EA. In addition, we analyzed serum lipid metabolism markers and intestinal microbiota from EA-treated patients (pre- and post-treatment) and healthy controls, aiming to explore the potential mechanisms underlying the effects of EA on abdominal obesity.
Methods
Study Design
This study was performed at Hubei Provincial Hospital of Traditional Chinese Medicine, from July 22, 2021 to March 15, 2023 and adhered to rigorous ethical standards. The protocol received approval from the Hubei Provincial Hospital of Traditional Chinese Medical Ethics Committee (HBZY2021-C12-01). The study was performed abiding by the Declaration of Helsinki. Additionally, the study was registered on ClinicalTrials.gov with identifier NCT04957134. Detailed protocols and the statistical analysis plan can be found in Supplemental Study Protocol. Informed consents were obtained from each participant (patients with abdominal obesity and HC). The study followed the guidelines set forth by the Consolidated Standards of Reporting Trials (CONSORT) and the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA).32,33 Participants were recruited through advertisements to ensure transparency and clarity in the enrollment process.
Participant
Patients with Abdominal Obesity
The inclusion criteria of patients with abdominal obesity were as follows: (1) men or women aged 18 to 55 years. (2) diagnosis of abdominal obesity, defined as waistline ≥ 85cm in men or ≥ 80cm in women.9 (3) voluntarily signed informed consent accepting EA intervention. The exclusion criteria were as follows: (1) Endocrine diseases that can cause obesity, such as polycystic ovary syndrome, Cushing syndrome, or hypothyroidism. (2) Using medications known to interfere with glycometabolism or lipid metabolism. (3) Diabetes mellitus or poorly managed hypertension (systolic blood pressure ≥ 160 mmHg and/or diastolic blood pressure ≥ 100 mmHg).34 (4) Severe internal diseases such as serious lung, heart, liver, or kidney disease; nervous system diseases or mental disorders. (5) Women who were pregnant, lactating, or planning to become pregnant within the next 32 weeks. (6) Clinical diagnosis of an eating disorder such as bulimia nervosa or anorexia nervosa. (7) Weight changes greater than 5 kg in the previous 3 months or use of drugs known to influence weight or appetite within the same period (eg, diet pills, corticosteroids, antidepressants, diazepam, non-selective antihistamines, nicotine replacements, or hypoglycemic drugs). (8) Plans to quit smoking or drinking. (9) Participation in other clinical research on obesity within the previous 3 months. (10) Received acupuncture within 6 months before enrollment.
HC
Age- and sex-matched HC were recruited. All of them provided the medical report confirming the absence of organic diseases (within 6 months) as well as drug use history that may affect intestinal microbiota (within 3 months). The inclusion criteria of patients with abdominal obesity were as follows: (1) No organic or functional diseases in the past; (2) No cold or other abnormalities in the near future; (3) Males and females aged between 18 and 55 years old; (4) Males’ waist circumference < 85cm or females’ waist circumference < 80cm; (5) Patients without mental illness; who has not participated in other clinical studies recently; who sign the informed consent and voluntarily accept the project. Exclusion criteria for the HC group were the same as those applied to abdominally obese participants.35
Randomization and Blinding
In this study, an independent programmer who did not contact with participants generated the randomization sequence using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). The sequence was securely kept in sequentially numbered, opaque, sealed envelopes (SNOSE),36 which were prepared in advance by a researcher not involved in participant enrollment or outcome evaluation. Following baseline assessments, eligible patients were randomized in a 1:1 ratio into two groups: the EA group, receiving real electroacupuncture treatment, and the SA group, receiving sham electroacupuncture treatment, according to the randomization sequence within the envelopes. Throughout the study, patients remained blinded to their assigned group. The envelopes were opened sequentially and only after the participant had been fully enrolled and completed baseline data collection, by a study coordinator who was not involved in outcome assessments and was blinded to the treatment codes. This procedure ensured strict allocation concealment and prevented prediction of future assignments. After allocation, experienced acupuncturists, who were not involved in outcome assessment or data analysis, conducted the respective interventions. Each treatment session occurred in a private setting with patients wearing eye masks and no communication among them to prevent unblinding. At the end of the 8-week intervention, patients were asked to guess their group assignment to assess blinding efficacy.37 Clinical assessments of participants were performed by independent assessors who were blinded to the group allocations. Apart from the acupuncturists, all other researchers and participants remained blinded throughout the study. This approach ensured rigorous blinding procedures and minimized bias in outcome assessment.
Interventions
The study spanned 32 weeks, comprising an 8-week intervention phase followed by a 24-week follow-up period. All participants were instructed to keep healthy lifestyle habits such as regular exercise and healthy diet. Based on body weight, participants were instructed to follow a calorie-restricted diet: those weighing less than 250 pounds were advised to consume 1200–1499 kcal/day, while those over 250 pounds were recommended 1500–1800 kcal/day. The diet consisted of traditional foods, with approximately 15–20% of total calories from protein, 20–35% from fat, and the remainder from carbohydrates. Participants were also instructed to track their daily food and calorie intake. Regarding physical activity, they were encouraged to engage in at least 180 minutes per week of low-to-moderate intensity exercise (such as walking), preferably reaching 225 minutes or more across at least five days each week.38 To objectively assess adherence, all participants were provided with diet and physical activity diaries and asked to record their dietary intake and physical activity each week. Participants whose mean daily caloric intake and cumulative weekly physical activity duration met the recommended standards were classified as having good dietary and exercise adherence, respectively.
EA and SA interventions were administered by 2 acupuncturists, each with over 5 years of experience in acupuncture techniques. To maintain trial quality, both research assistants and acupuncturists underwent a training session conducted by the principal investigator prior to the commencement of the study. Both patients in the EA group and SA group received a total of 24 treatment sessions, with each session lasting 30 minutes. These sessions were administered over 8 consecutive weeks, amounting to 3 sessions per week, typically every other day. Disposable needles from Hwato (Suzhou, China) and the SDZ-V electro-stimulator from Suzhou Medical Appliance Co., Ltd. were utilized for acupuncture procedures.
Patients in the EA group received treatment at the bilateral acupoints of Zusanli (ST36), Sanyinjiao (SP6), Zhongwan (CV12), Tianshu (ST25), Shuifen (CV9), Daheng (SP15), Daimai (GB26), Shuidao (ST28), Huaroumen (ST24), Fujie (SP14) and Shuifen (CV9). The selection of these acupoints and electroacupuncture parameters was based on our previous research findings and the extensive clinical experience of our team.39 The location of all acupoints were set according to the World Health Organization standard. During treatment, patients were positioned supine, and acupuncture needles measuring 0.30 × 50 mm or 0.35 × 75 mm were inserted slowly and vertically into the selected acupoints, typically to a depth of 10 to 30 mm. The needles were manipulated by techniques such as twirling, lifting, and thrusting to achieve deqi, characterized by sensations of soreness, heaviness, and distension. After deqi was achieved, paired electrodes from an electroacupuncture stimulator were connected transversely to the needle handles at bilateral ST25 (anode) and SP15 (cathode). A disperse-dense wave with alternating frequencies of 10 and 50 Hz was delivered for 30 minutes. The intensity of the current was adjusted according to the participant’s tolerance and subjective sensation (eg, aching, tingling), typically ranging from 0.1 to 1 mA, but always kept below the pain threshold. If a participant experienced pain or discomfort, the intensity was immediately reduced to ensure both safety and comfort.
For the SA group, disposable sterile acupuncture needles (0.30 × 50 mm or 0.35 × 75 mm) will be inserted superficially (approximately 2–3 mm in depth) at “placebo acupoints”, which are located approximately 1 cun (≈20 mm) lateral to the corresponding real acupoints used in the EA group. No manual stimulation will be performed, and the procedure will not elicit the Deqi sensation.40 Similar to the EA group, paired electrodes were attached from a specially constructed electro-stimulator to the needle holders placed at sham acupoints ST25 and SP15. When activated, the electro-stimulator in the SA group displayed the same working power indicator as in the EA group. However, internally, the output power cord of the EA stimulation instrument was interrupted to ensure no actual electrical stimulation was delivered. For visual reference and clarity regarding the location of acupoints and electrode placement, please refer to Supplemental Study Protocol.
Measurements and Outcomes
Throughout the study, patients with abdominal obesity participated in clinical assessments, specimen collection, and recording any adverse events that occurred during the procedure. In contrast, HC only underwent clinical assessments and specimen collection at baseline.
Clinical Assessment
Outcomes were measured by blinded assessors. Measurements of waistline, weight, BMI, hipline, and Waist-Hip Ratio (WHR) were conducted at several time points: baseline, week 4, week 8 (primary endpoint), week 20, and week 32. Additionally, participants completed the IWQOL-Lite and Kessler 10 scales at specific intervals: baseline, week 8, week 20, and week 32. In this study, we set the primary outcome as the change of waistline from baseline to week 8.
Adverse Events
Adverse events were monitored throughout the trial and recorded at all assessment time points. Safety evaluation related to EA includes needle breakage, needle loss, needle fainting, unbearable acupuncture pain (VAS ≥ 8 points), local hematoma, infection, and abscess. Furthermore, we also recorded the duration and intensity of other adverse events may related to acupuncture. We formed a specific record form and ask whether the above situation occurs after each acupuncture session.
Specimen Collection
Participants in the EA group (pre- and post-treatment) and HC provided stool and blood samples under fasting conditions in the morning. Approximately 3–5 g of fresh stool was collected and, along with the aliquoted serum obtained from blood samples (collected in heparinized tubes, kept at 4°C for 1 hour, and centrifuged at 2000 rpm for 10 minutes), was stored at −80°C for long-term preservation and subsequent analyses. Assessment of gut microbiome and metabolic parameters analysis will be performed by Wuhan Metware Biotechnology Co., Ltd.
Analysis of Untargeted Lipidomics
The serum lipidomics analysis in the study involved the following detailed methodology:
Lipids Extraction
Serum samples were thawed and mixed with MTBE:MeOH (3:1, v/v), followed by vortexing for 15 minutes to extract total lipids. Subsequently, 200 μL of water was added, and the mixture was vortexed for an additional 1 minute. Samples were centrifuged at 12,000 rpm for 10 minutes. After centrifugation, 200 μL of the upper organic layer was transferred to a new tube and evaporated to dryness using a vacuum concentrator to remove the solvent. The dried lipid extract was reconstituted in 200 μL ACN:IPA (1:1, v/v) for subsequent LC-MS/MS analysis.
Chromatography and Mass Spectrometry Conditions
Lipidomics analysis was performed using an LC-ESI-MS/MS system. Chromatography was carried out on a Thermo Accucore™ C30 column, with mobile phase A consisting of acetonitrile/water (60:40, v/v) and mobile phase B consisting of acetonitrile/isopropanol (10:90, v/v), using a gradient elution. The flow rate was 0.35 mL/min, the column temperature was maintained at 45°C, and the injection volume was 2 μL. The column effluent was introduced into a QTRAP® triple quadrupole-linear ion trap mass spectrometer equipped with an ESI Turbo Ion-Spray interface, operating in both positive and negative ion modes. Key parameters included GS1 = 45 psi, GS2 = 55 psi, curtain gas (CUR) = 35 psi, collision gas at medium strength, source temperature 500°C, and ion spray voltage +5500 V (positive)/−4500 V (negative). Instrument tuning and mass calibration were performed using 10 and 100 μmol/L polypropylene glycol solutions, respectively. In QQQ mode, metabolites were monitored using MRM experiments with optimized declustering potential (DP) and collision energy (CE). Lipidomics analysis was performed using a local metabolite database to qualitatively and quantitatively analyze the lipids in the samples.
Quality Control
To ensure the stability and reliability of the lipidomics analysis, quality control (QC) samples were prepared by thoroughly mixing equal volumes (10 μL each) of multiple serum samples. The QC samples were processed using the same extraction and analytical procedures as the test samples to ensure consistency across all steps. During the continuous analysis sequence, after every 10 test samples, a mixed QC sample and a solvent blank (pure acetonitrile) were automatically injected to monitor the consistency of sample preparation and the stability of the instrument.
Lipidomic Analysis
Lipid analysis was carried out by using Analyst 1.6.1 software (AB SCIEX, Toronto, Ontario, Canada). Differentially expressed lipid species were identified based on a variable importance in projection (VIP) score >1 from the orthogonal partial least-squares discriminant analysis (OPLS-DA) model and a fold change (FC) threshold of ≥ 1.2 or ≤ 0.83.41
Analysis of Intestinal Microbiota
This study employed 16S rRNA sequencing to analyze the intestinal microbiota. The methodology was as follows:
DNA Sequencing and PCR Amplification
Genomic DNA was extracted from stool samples using the CTAB method. The V3-V4 hypervariable regions of the bacterial 16S rRNA gene were amplified using barcoded specific primers and a high-fidelity polymerase, following the manufacturer’s instructions, to ensure accurate amplification.
Quality Control
PCR products were first assessed by electrophoresis on a 2% agarose gel to confirm specificity and expected band size. Qualified products were then purified using magnetic beads or a gel extraction kit, quantified, and pooled in equimolar amounts to prepare samples for subsequent sequencing.
16S rRNA Sequencing
The sequencing libraries were prepared using the TruSeq® DNA PCR-Free Sample Preparation Kit. The constructed libraries were quantified and quality-checked using Qubit and qPCR to ensure they met the required standards. Qualified libraries were then sequenced on the NovaSeq 6000 platform to generate raw sequence data. Sequencing data quality was assessed by evaluating Q30 scores, read length, and GC content, and low-quality reads or adapter contamination were removed. Finally, DNA fragments shorter than twice the read length were merged using FLASH software to improve sequence accuracy and effective length.
Operational Taxonomic Units Construction
Raw sequencing data were subjected to quality control and merging to obtain high-quality sequences (Clean Data). Based on these data, Operational Taxonomic Unit (OTU) clustering was performed, grouping sequences with ≥97% similarity into the same OTU. Representative sequences from each OTU were then selected for taxonomic annotation, yielding corresponding species information and abundance distributions at the taxonomic level.
Microbial Analysis
Microbial diversity was assessed using α-diversity indices to evaluate species richness and diversity, thereby exploring community structure differences among groups. Statistical methods including T-test, and LEfSe analysis were applied to test the significance of differences in species composition and community structure between groups.
Sample Size
It was designed as a superiority study with a 1:1 ratio. Based on a previous EA study and related literature,42 the decline in waistline was 4.8 ± 1.2 cm in the EA group and 2.5 ± 1.1 cm in the SA group. To detect the superiority of difference between the two groups to 1.3 cm as the minimal clinically important difference, a total of 58 subjects is required to obtain at least 90% power and control alpha level at 0.025 (one-sided). A drop-out rate of 15% was assumed, the final sample size was determined to be 68 subjects with 34 subjects in each group.
Statistical Analysis
The final analysis was performed based on the intention to treat principle. We performed statistical descriptions for the two groups, categorical variables were described using frequencies and percentages, and continuous variables were expressed as mean with standard deviation or median with interquartile ranges (IQRs) based on normality test. For primary and secondary endpoints using changes from baseline as outcomes, analysis of covariance (ANOCOVA) was performed to estimate the adjusted difference in changes between the two groups and corresponding 95% confidence interval, meanwhile, baseline group variable of interest, sex and age were included as covariant variables. Missing data were handled using the last observation carried forward (LOCF) method for continuous outcomes. The incidence of adverse (AEs) effects in each group was reported along with an exact (Clopper-Pearson) two-sided 95% CI for percentage. James Blinding Index was used to assess the success of blinding.43 We compared the proportions of participants who guessed that they had received EA between groups. All analyses were done with SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA).
Results
Patient Characteristics
A total of 224 participants underwent screening, from which 68 patients were initially enrolled for baseline assessment. Two participants from the SA group discontinued the study due to relocation to another city (Figure 1). The demographic and clinical characteristics of the patients and HC were summarized and presented in Table 1. According to the table, apart from height and sex, all other demographic information and baseline characteristics were found to be well-balanced between the EA and SA groups.
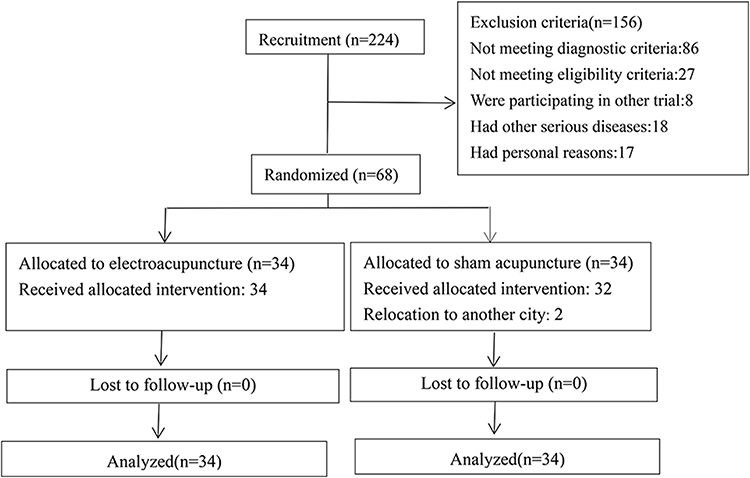 |
Figure 1 Study Flowchart. Notes: CONSORT figure was adapted from Schulz KF, Altman DG, Moher D, Group C. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. Mar 23 2010;340:c332. doi:10.1136/bmj.c332. Creative Commons.32 |
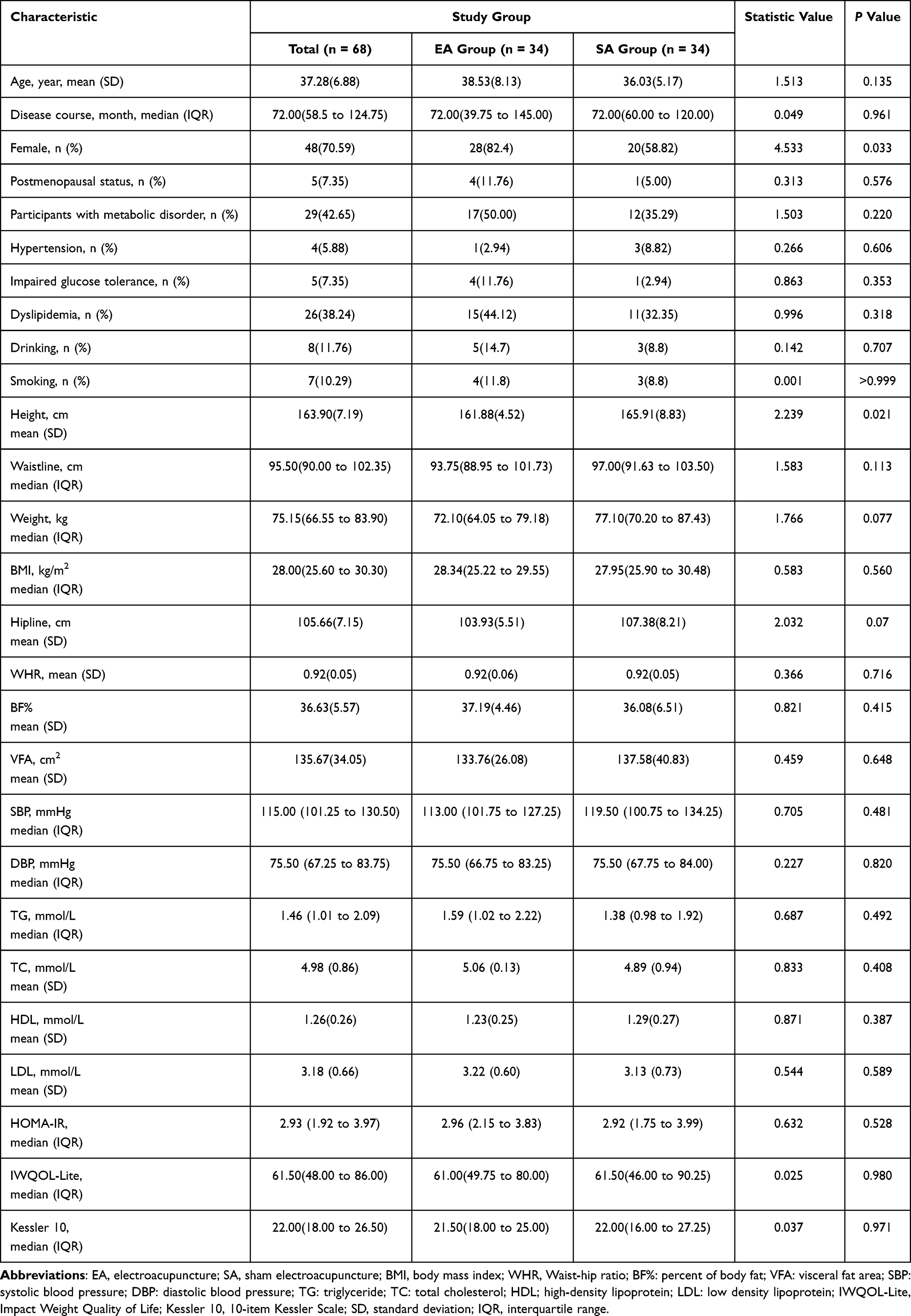 |
Table 1 Baseline Characteristics of the Intention-to-Treat Population |
Efficacy
Primary Outcomes
In Table 2, the changes in waistline between the EA and SA groups over the 8-week intervention and 24-week follow up are summarized. Figure 2 illustrates the trends of waistline changes in both groups. After 8 weeks of treatment, the EA group exhibited a significant reduction in waist circumference, which continued to improve during the follow-up period. In contrast, the SA group showed only a slight decrease during the intervention phase, with waist circumference gradually returning to baseline after discontinuation. Compared with the control group, the EA group demonstrated significantly greater reductions in waist circumference at all measured time points (weeks 4, 8, 20, and 32), with between-group differences reaching statistical significance (all P < 0.05).
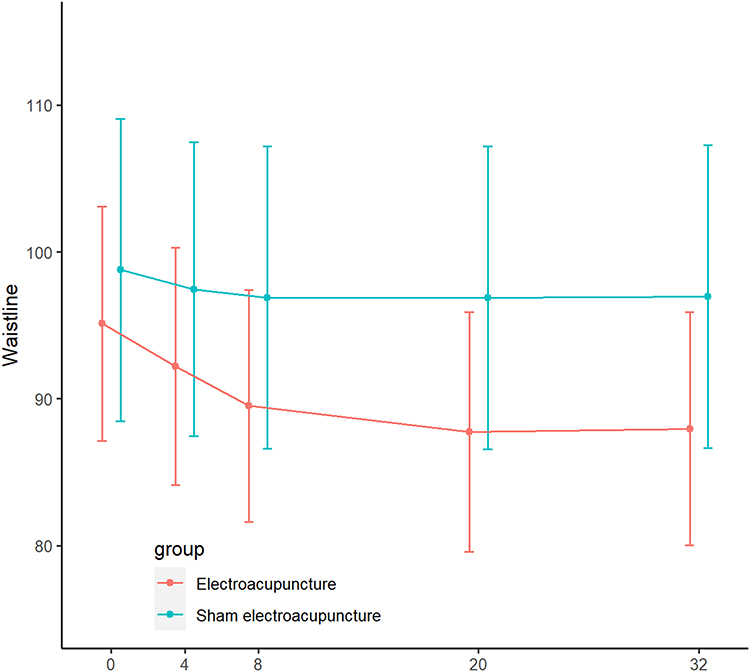 |
Figure 2 Changes in Waistline in the Two Groups Over Time. |
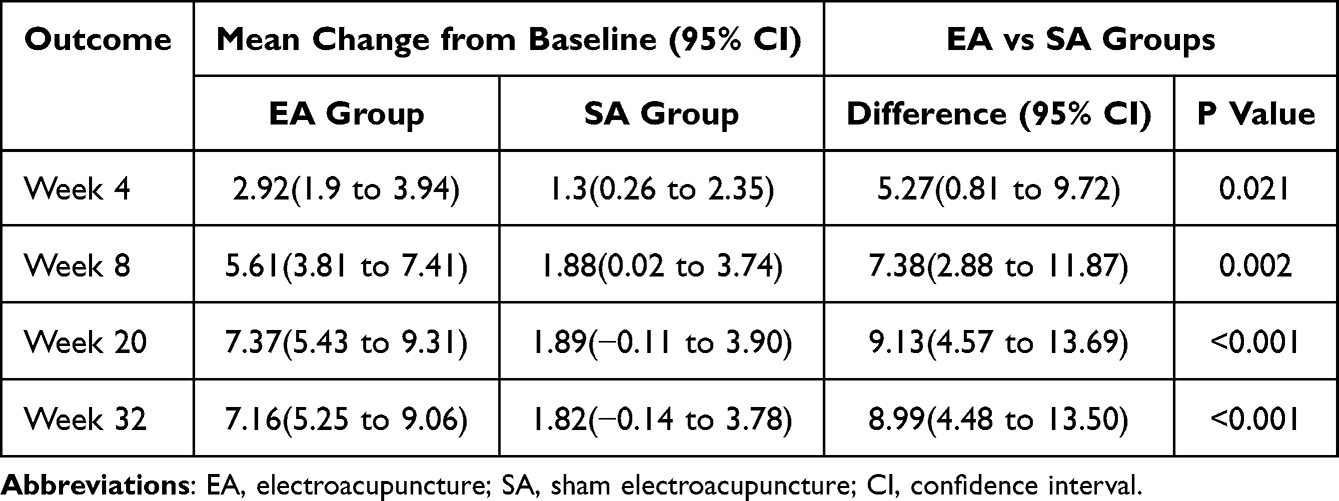 |
Table 2 Waistline Changes Between Study Groups |
Secondary Outcomes
Table 3 summarizes the results of secondary outcomes at the end of intervention and the follow-up.
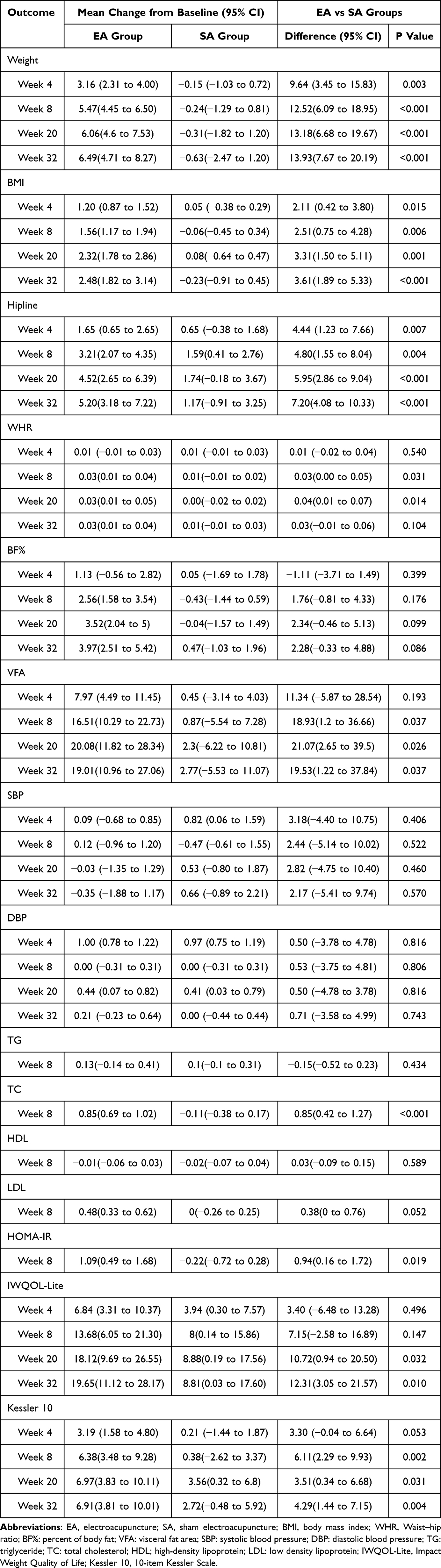 |
Table 3 Secondary Outcomes Between Study Groups |
Within-group comparisons indicated that participants in the EA group experienced significant and sustained improvements in multiple secondary outcomes over the 32-week period. Notably, reductions in body weight, BMI, hipline, and visceral fat area were observed at all follow-up time points (weeks 8, 20, and 32). Although body fat percentage showed a downward trend, the change was not statistically significant. Measures of psychological well-being and obesity-related quality of life also improved over time, as reflected by increasing IWQOL-Lite scores and decreasing Kessler-10 scores. In contrast, the SA group exhibited no significant changes in these variables throughout the study. A transient decrease in TC, LDL, and HOMA-IR was observed in the EA group at week 8, suggesting a possible short-term metabolic adjustment during the intervention.
Between-group comparisons at week 32 further confirmed the superior efficacy of electroacupuncture. The EA group demonstrated significantly greater reductions in body weight, BMI, hipline, and visceral fat area compared to the SA group. However, changes in body fat percentage, blood pressure, and most lipid parameters did not differ significantly between groups. Importantly, improvements in quality of life and psychological distress were more pronounced in the EA group, indicating that electroacupuncture may provide additional psychosocial benefits beyond body composition regulation.
Safety and Blinded
Acupuncture-related adverse events occurred in 3 patients (8.82%) in the EA group and 2 patients (5.88%) in the SA group. No significant difference was found among groups for the proportion of patients with adverse events (P = 1.00). The most reported acupuncture-related adverse events were hematoma around the site of needling and local pain, all of which were mild and resolved spontaneously without any intervention. No patients had severe adverse events in the trial. (Table S1). No statistical difference was found between groups in the proportion of participants who guessed that they received EA at week 8 with a JBI of 0.471 (95% CI 0.380–0.561) (Table S2).
Adherence
Participants in both the EA and SA groups showed high adherence to the prescribed diet and exercise regimens, with no significant differences observed between groups in overall or weekly adherence (Table S3).
Lipidomic Analysis
Screening of Serum Biomarkers
As shown in the principal component analysis (PCA) score plot, separation between the HC group and pre-EA group could be observed (Figure S1A). To explore the high level of group separation, two multivariate models were obtained to understand the lipid alteration by OPLS-DA analysis with validation parameters of fitness (R2X = 0.492 and R2Y = 0.987) and predictability (Q2= 0.787) between HC group and pre-EA group (Figure S1B), suggesting that lipid metabolic disorders were induced in pre-EA group. Furthermore, there was obvious separation among pre-EA group and post-EA group based on the PCA analysis and OPLS-DA analysis (Figures S1C and 1D). The results indicated that the plasma metabolic profile of the post-EA group was significantly altered compared with the pre-EA group.
Lipid Composition Analysis
We used the UPLC-MS/MS platform in negative or positive mode to analyze the differences in lipid composition. A total of 1607 lipid species were detected in the serum of HC group, pre-EA and post-EA group, including 769 GPs, 454 GLs, 234 SPs, 99 FAs, 49 STs, and 2 Prenol Lipids (PRs), shown in Table S4. As shown in the volcano plot analysis (Figure 3), distinct lipid biomarker candidates were screened out. Using the criteria of VIP >1 and FC ≥ 1.2 or ≤ 0.83, 480 significant lipid changes between the HC and pre-EA groups and 106 between the pre-EA and post-EA groups. To further investigate which lipid biomarkers were regulated, we identified 32 differential lipids that appeared in both comparisons including 1 GL, 23 GPs, 7 SPs, and 1 ST. Among them, compared with HC, 29 lipids of abdominal obese patients in pre-EA group were upregulated, while 3 downregulated. Interestingly, the trends of them were ameliorated after EA treatment (Table 4).
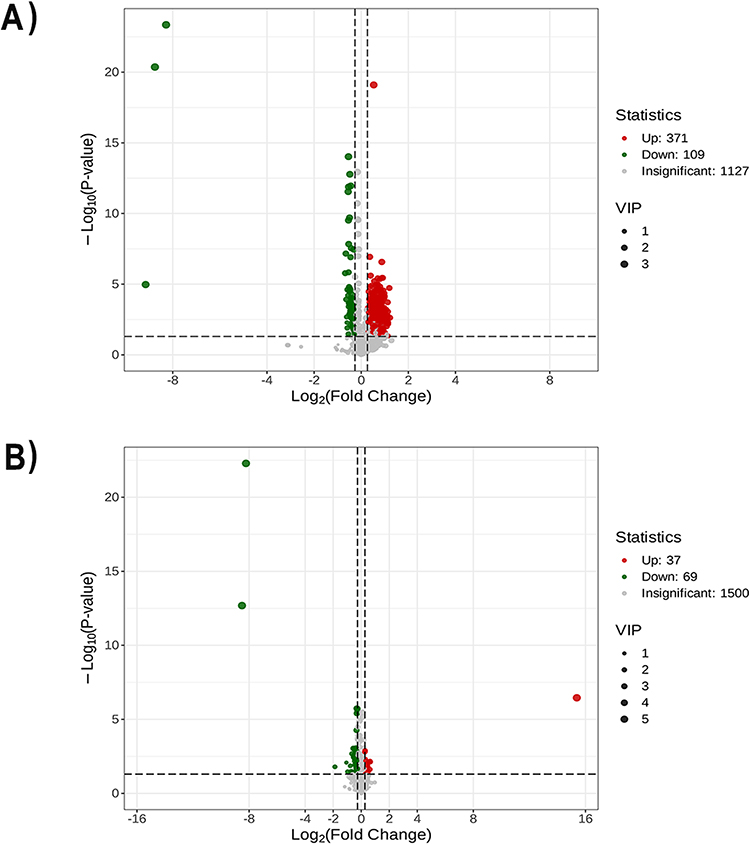 |
Figure 3 Volcano plots of differential lipids with VIP >1. and FC ≥ 1.2 or ≤ 0.83. (A) Volcano plots of differential lipids between HC and pre-EA group. (B) Volcano plots of differential lipids between post-EA and pre-EA group. |
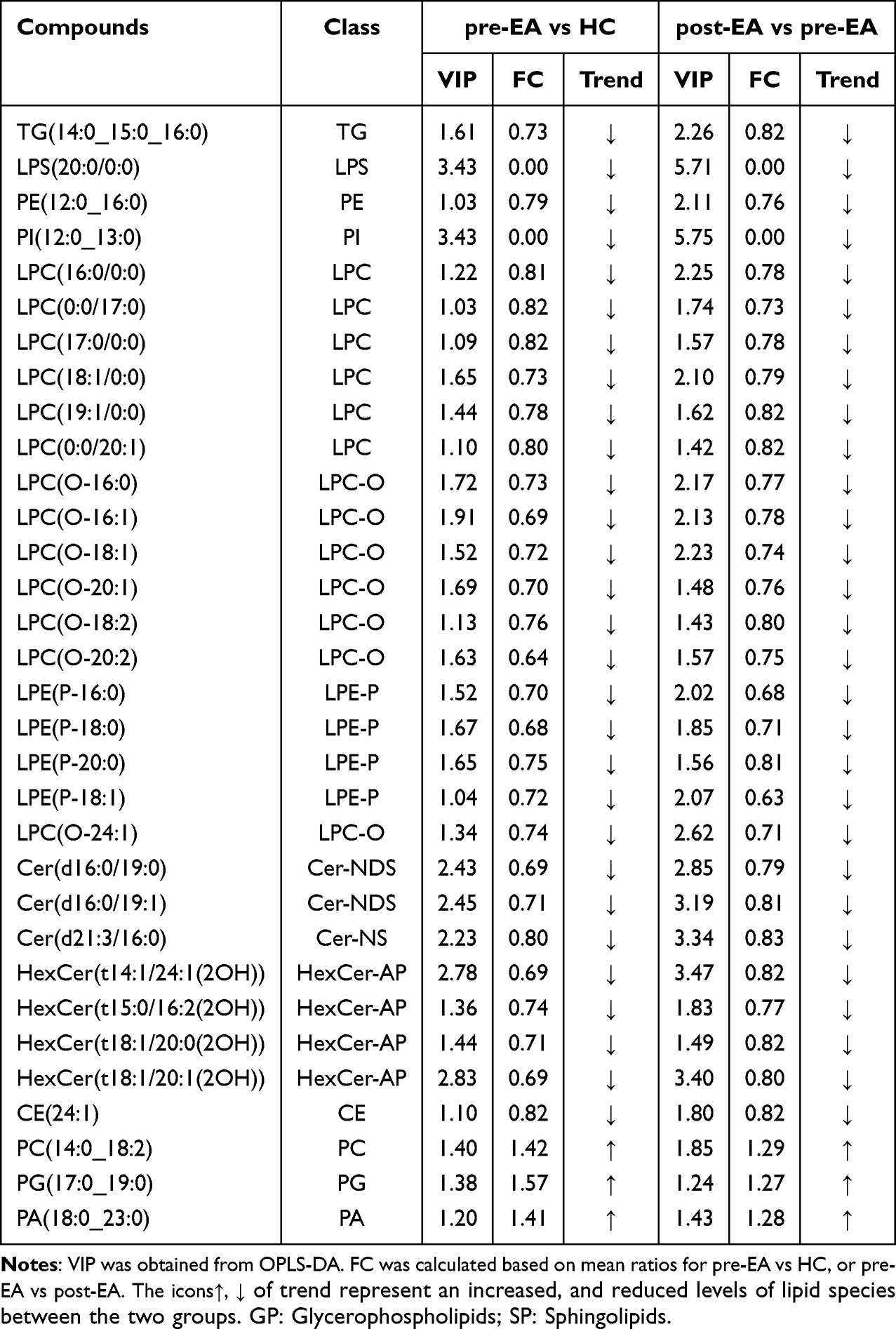 |
Table 4 Identification of Potential Lipid Biomarkers Based on the Criteria of an FC ≥ 1.2 or ≤ 0.83 and VIP ≥ 1 |
Pathway Analysis
Pathway enrichment analysis provided clues for biochemical and signal transduction pathways involved in lipid species differences. The results showed that 117 metabolic pathways were concentrated between the HC group and pre-EA group, which could be attributed to five items: organismal systems (number of pathways 49), metabolism (16), human diseases (32), environmental information processing (15) and cellular processes (5) (Figure S2A). Compared with the HC group, the pre-EA group clearly had significantly different expression of the glycerolipid metabolism, regulation of lipolysis in adipocytes, lipid and atherosclerosis, vitamin digestion and absorption, cholesterol metabolism, thermogenesis, insulin resistance, long-term depression, fat digestion and absorption, inositol phosphate metabolism, metabolic pathways, sphingolipid metabolism, carbohydrate digestion and absorption, apelin signaling pathway, adrenergic signaling in cardiomyocytes, and et al (Figure S2C). Whereas EA ameliorated these symptoms. A total of 116 metabolic pathways were concentrated between the post-EA group and pre-EA group (Figure S2B). Figure S2D shows the enriched functions via the classification of differentiated pathways in the post-EA group compared with the pre-EA group, including glycerophospholipid metabolism, aldosterone synthesis and secretion, insulin secretion, inflammatory mediator regulation of TRP channels, choline metabolism in cancer, apelin signaling pathway, and et al.
Fecal Microbiota Analysis
OTU Analysis
The numbers of OTUs unique to the HC group, the pre-EA group and post-EA groups were 2048, 381 and 602, respectively (Figure S3A). After treatment, the number of unique OTUs in acupuncture group increased by 1506 (559 to 2065), and the number of OTUs coinciding with the HC group increased by 1285 (Figure S3B–3D). This suggests that abdominal obesity caused a decrease in species diversity in the intestinal microbiota, while EA improved it.
α-Diversity Index Analysis
With regard to microbial communities, the species richness, diversity and evenness were quantified by the alpha diversity. The Chao1 indexes to represent diversity. The larger the Chao1 index is, the more abundant the community. Similarly, the higher the ACE indexes are, the greater the diversity of the community. Compared with the HC group, the Chao1, ACE indices markedly decreased in the pre-EA group, which suggests a low intestinal bacterial community richness in abdominal obesity patients. However, there was no significant difference between the pre-EA and post-EA groups (Figure 4A and B). The results indicated that EA did not improve the richness and diversity of intestinal microbes in abdominal obesity people.
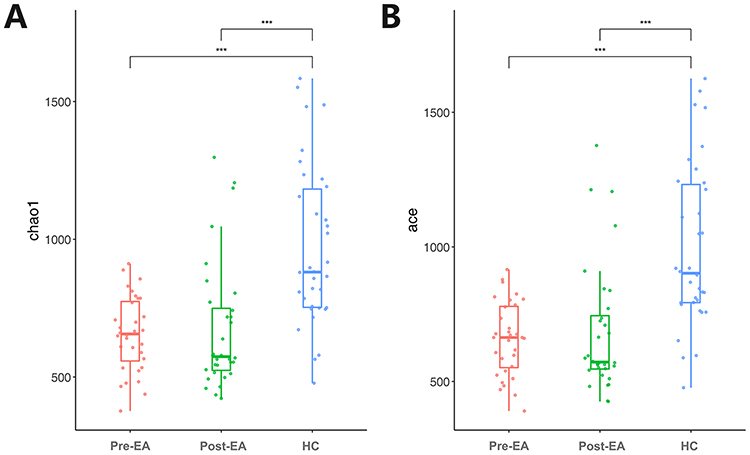 |
Figure 4 The alpha-diversity index between pre-EA group, post-EA group and HC group. (A) Chao1; (B) ACE. |
Microbial Structure Analysis
As shown in Figure S4A, Firmicutes (accounting for an average of 55.35%) was the most prominent phylum in the pre-EA group, while Bacteroidota (accounting for an average of 28.84%) and Firmicutes (accounting for an average of 37.36%) both were the dominated phylum in post-EA group. Compared with the HC group, the abundances of Akkermansia-muciniphila, Cutibacterium-acnes, and Staphylococcus-epidermidis were significantly lower in the pre-EA group, whereas Bacteroides-uniformis, Parabacteroides-distasonis, Phascolarctobacterium-faecium, and Bacteroides-clarus were significantly higher (Figure S4B). Compared with the pre-EA group, the abundances of Faecalibacterium-prausnitzii, and Bacteroides-uniformis were significantly lower in the post-EA group, whereas Akkermansia-muciniphila, Bacteroides-ovatus, and Bacteroides-fragilisBacteroides-clarus were significantly higher (Figure S4C). Compared with the post-EA group, the abundances of Akkermansia-muciniphila, Bacteroides-ovatus and Parabacteroides-distasonis were significantly lower in the HC group, whereas Faecalibacterium-prausnitzii was significantly higher (Figure S4D).
Lefse Analysis
LEfSe analysis was conducted to further clarify the gut flora features and taxonomic differences, with significance defined as LDA score > 4 and p < 0.05. The LDA histogram plot revealed 43 differential features among the three groups (Figure 5A). Specifically, 5 bacterial species, including unidentified-Prevotellaceae, Faecalibacterium, unidentified-Enterobacteriaceae, Agathobacter, Roseburia, and Klebsiella, along with their high taxonomic classifications, were significantly enriched in the HC group. Meanwhile, Megamonas, unidentified-Lachnospiraceae, unidentified-Oscillospiraceae, Lachnoclostridium and Lachnospiraceae were more abundant in the pre-EA group. The abundance of 2 bacterial species, including Sutterella, Akkermansia, and their high taxa were significantly higher in the post-EA group. The cladogram depicts the phylogenetic relationships of the differentially enriched taxa among the three groups (Figure 5B).
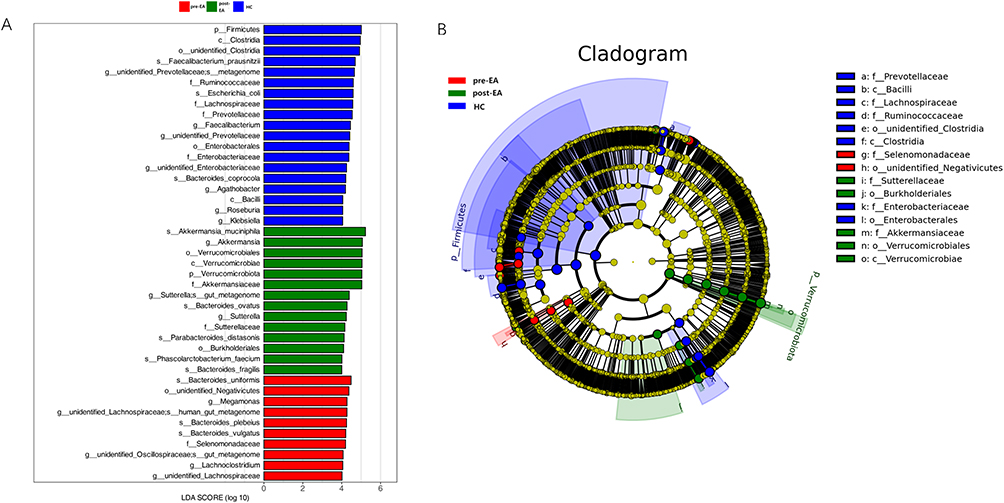 |
Figure 5 Microbiomics analysis. (A) Histogram of the LDA score of microbes that showed a significant impact in the pre-EA group, post-EA group and HC group. (B) Cladogram of the linear discriminant analysis (LDA) effect size (Lefse) analysis of significant difference of microbial population. |
Discussion
Our study showed that, compared with SA group, 8-week EA intervention could significantly reduce the waistline, weight, BMI, hipline and Kessler 10, with these improvements persisting throughout the 24-week observational follow-up. Additionally, we observed significant changes in 187 lipid products after EA treatment, with a predominance of down-regulation. Microbiota analysis revealed that, compared with the pre-treatment condition, intestinal microbial richness in patients with abdominal obesity showed no evident changes after treatment; however, the abundance of certain taxa was significantly altered.
Though in routine clinical practice, the risk of abdominal obesity historically relied on BMI, waistline is increasingly advocated which is highly accessible anthropometric proxy for abdominal obesity.44 Waistline is used to assess visceral fat, which is strongly associated with metabolic syndrome, type 2 diabetes and cardiovascular disease.45 Therefore, interventions effectively targeting abdominal obesity hold promise for improving health-care outcomes. EA has gained popularity as a complementary and alternative therapy with growing clinical evidence supporting its efficacy in treating obesity. Previous systematic reviews have indicated that EA can reduce waistline by 2.39 cm compared to SA in patients with obesity.46 In our study, we observed an effect size more than twice as large as reported in the literature, with the difference in waistline between EA and SA groups widening to three times during the follow-up period. Other studies assessed the efficacy of EA with or without dietary change generated a therapeutic effect on abdominal obesity.15,16 Our study rigorously controlled eligibility criteria, extended the follow-up period, and increased the sample size, further confirming the clinical efficacy of EA for abdominal obesity. In addition, compared with calorie restrict, the present study demonstrates that EA exhibits superior efficacy without the necessity for caloric control. In terms of safety and acceptability, EA was generally well-tolerated by participants. No serious adverse events were reported, and minor events such as hematoma or sharp pain resolved spontaneously without intervention. Moreover, participants demonstrated good adherence to the treatment regimen, completing all scheduled sessions over the 8-week intervention period. These observations suggest that EA is not only effective but also safe and acceptable, supporting its potential as a viable complementary therapy for abdominal obesity.
Previous studies have demonstrated significant changes in lipidomics among patients with obesity, which can be corrected through interventions such as exercise, bariatric surgery, and fasting.47–49 To our knowledge, this is the first to investigate lipidomics changes in patients with abdominal obesity undergoing EA treatment. The results revealed EA regulated the aberrant lipidomic metabolism in patients with abdominal obesity. In addition, among the 32 lipid species that differed between patients with abdominal obesity and healthy controls, 29 were down-regulated and 3 were up-regulated, these lipids, belonging to GPs and SPs, exhibited changes between pre- and post-treatment measurements. Though GPs and SPs are account for only 3% of total lipids, they play important roles in the development and prognosis of metabolic diseases.47 Furthermore, enrichment analysis revealed that these differential lipid products were enriched in the Apelin signaling pathway, which is implicated in glucose and lipid metabolism and linked with obesity.50 Weight loss often accompanies muscle mass reduction, increasing cardiovascular disease and osteoporosis risks.51,52 Interestingly, studies have shown that EA can improve skeletal muscle morphology and function in sarcopenia-model animals.53,54 These findings suggest a potential role for EA in modulating lipid metabolism, providing a basis for further investigation into its possible application in obesity management.
Recently, a growing number of studies have revealed the change of intestinal microbiota can cause obesity, including the loss of beneficial bacteria, the excessive growth of potentially pathogenic bacteria, and the reduction in the microbial diversity.55 Yan et al specifically identified a strong association between visceral fat area and intestinal microbiota.56 Since visceral fat accumulation contributes to abdominal obesity, in our study, the Chao1 and ACE indices were markedly reduced in the pre-EA group compared with HC, which is in partial agreement with the observations reported by Yan et al. However, compared with pre-EA, the diversity of the intestinal microbiota in post-EA did not show a significant increase. Similarly, preclinical studies have demonstrated that EA can modulate intestinal microbiota in obese mice induced by high-fat diets.29,57 These findings suggest a plausible mechanism wherein EA may mitigate abdominal obesity by restoring intestinal microbiota balance. This hypothesis underscores the potential therapeutic role of EA in influencing intestinal microbiota as part of its treatment strategy for abdominal obesity.
Further analysis suggested that compared with pre-EA group, an increase in the relative abundance of Akkermansia muciniphila in post-EA group. Akkermansia-muciniphila, a Gram-negative obligatory anaerobe predominantly found in the intestinal mucus layer, has been noted to decrease in abundance with obesity.58 Interventions such as calorie restriction or bariatric surgery have shown to influence Akkermansia muciniphila levels, potentially mitigating obesity and related pathological conditions.59,60 Moreover, insulin resistance is the crucial pathological feature induced abdominal obesity to metabolic syndrome. Recent exploratory studies have indicated that supplementation with Akkermansia muciniphila for three months can reduce insulin resistance and weight in overweight or obese individuals.61 The underlying mechanisms involve Akkermansia muciniphila inhibiting phospho-JNK and activating IKBA expression.62 The results underscore the importance of understanding the Akkermansia-muciniphila’s specific role in lower insulin resistance and weight loss in humans as well as its potential as a therapeutic target.58
Limitations
The study has several limitations that warrant consideration. First, the baseline differences in waist circumference and weight showed a trend toward imbalance. Although adjusted in analysis, this may still affect results interpretation. Second, the small sample size limited our ability to conduct subgroup analyses by age or gender, which may affect lipid metabolism and microbiota composition. Third, although samples were collected from all participants, microbiota and lipidomics analyses were only performed in the EA group and HC group due to funding constraints, limiting interpretation of non-specific effects in the SA group. Fourth, while standardized lifestyle recommendations were provided, adherence to diet and exercise was not rigorously monitored, which may have introduced confounding influences. Finally, the study population consisted primarily of adults recruited from a single hospital in China, which may limit the generalizability of the findings to other demographic or clinical populations. Despite these limitations, the study provides preliminary mechanistic insights into electroacupuncture for abdominal obesity and lays the groundwork for future large-scale, multicenter research.
Conclusions
EA could effectively reduce waistline in patients with abdominal obesity, with long-term effectiveness maintained over 24 weeks. Parallel changes in lipid metabolism and Akkermansia muciniphila abundance suggest potential correlations, though causality cannot be confirmed due to the lack of sham EA data. Further studies with appropriate control groups are needed to clarify the underlying mechanisms and establish the broader implications for clinical practice.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
Xia Chen, Yanji Zhang, and Chengwei Fu contributed equally to this work. Conceptualization: Xia Chen, Yanji Zhang, Wei Huang, Zhongyu Zhou. Data curation: Mengyuan Huang, Dan Wei, Wei Zhou, Yiran Liu, Bei Huang, Yinyue Rao, Yingrong Zhang, Hongjie Xia, Yaxin Hu. Formal analysis: Chengwei Fu, Hui Li. Funding acquisition: Zhongyu Zhou. Investigation: Mengyuan Huang, Dan Wei, Wei Zhou, Yiran Liu, Bei Huang, Yinyue Rao, Yingrong Zhang, Hongjie Xia, Yaxin Hu. Methodology: Xia Chen, Yanji Zhang, Chengwei Fu. Project administration: Dan Wei, Wei Huang, Zhongyu Zhou. Resources: Dan Wei, Wei Zhou, Yiran Liu, Wei Huang, Zhongyu Zhou. Software: Chengwei Fu, Wei Huang, Zhongyu Zhou. Supervision: Xia Chen, Yanji Zhang, Wei Huang, Zhongyu Zhou. Validation: Wei Huang, Zhongyu Zhou. Visualization: Xia Chen, Yanji Zhang, Chengwei Fu. Writing-original draft: Xia Chen, Yanji Zhang, Chengwei Fu. Writing-review & editing: Wei Huang, Zhongyu Zhou. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Scientific Research Project of Traditional Chinese Medicine of Hubei Provincial Health Commission (ZY2021Z004, ZY2025L284), the Scientific Research Project of Hubei Provincial Health Commission (WJ2025Q086), the Hubei Provincial Natural Science Foundation (2022CFD160, 2025AFD536), the High-level Key Discipline Construction Project of the National Administration of Traditional Chinese Medicine (Advanced Education Letters of National Administration of Traditional Chinese Medicine [2023]85), the Knowledge Innovation Project of Wuhan Science and Technology Department (2023020201010172), the Hubei Provincial Science and Technology Program Project (2025BCB024), and the National Natural Science Foundation of China (82505746).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the paper; and decision to submit the paper for publication.
References
1. Gupta RD, Tamanna N, Siddika N, Haider SS, Apu EH, Haider MR. Obesity and abdominal obesity in Indian population: findings from a nationally representative study of 698,286 participants. Epidemiologia. 2023;4(2):163–172. doi:10.3390/epidemiologia4020017
2. Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. 2012;13(3):275–286. doi:10.1111/j.1467-789X.2011.00952.x
3. Manolopoulos KN, Karpe F, Frayn KN. Gluteofemoral body fat as a determinant of metabolic health. Int J Obes. 2010;34(6):949–959. doi:10.1038/ijo.2009.286
4. Decoda Study G, Nyamdorj R, Qiao Q, et al. BMI compared with central obesity indicators in relation to diabetes and hypertension in Asians. Obesity. 2008;16(7):1622–1635. doi:10.1038/oby.2008.73
5. Dong Y, Zhou J, Zhu Y, et al. Abdominal obesity and colorectal cancer risk: systematic review and meta-analysis of prospective studies. Biosci Rep. 2017;37(6). doi:10.1042/BSR20170945
6. Du X, Hidayat K, Shi BM. Abdominal obesity and gastroesophageal cancer risk: systematic review and meta-analysis of prospective studies. Biosci Rep. 2017;37(3). doi:10.1042/BSR20160474
7. Jayedi A, Soltani S, Zargar MS, Khan TA, Shab-Bidar S. Central fatness and risk of all cause mortality: systematic review and dose-response meta-analysis of 72 prospective cohort studies. BMJ. 2020;370:m3324. doi:10.1136/bmj.m3324
8. Ross R, Neeland IJ, Yamashita S, et al. Waist circumference as a vital sign in clinical practice: a consensus statement from the IAS and ICCR working group on visceral obesity. Nat Rev Endocrinol. 2020;16(3):177–189. doi:10.1038/s41574-019-0310-7
9. Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocrine Pract. 2016;22 Suppl 3:1–203. doi:10.4158/EP161365.GL
10. Apovian CM, Aronne LJ, Bessesen DH, et al. Pharmacological management of obesity: an endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2015;100(2):342–362. doi:10.1210/jc.2014-3415
11. Department of Medical Administration NHCotPsRoC. Chinese guidelines for the clinical management of obesity (2024 Edition). Med J of Peking Union Med Coll Hosp. 2025;16(1):90–108. doi:10.12290/xhyxzz.2024-0918.
12. Sumithran P, Prendergast LA, Delbridge E, et al. Long-term persistence of hormonal adaptations to weight loss. N Engl J Med. 2011;365(17):1597–1604. doi:10.1056/NEJMoa1105816
13. Kesztyus D, Erhardt J, Kesztyus T, Schonsteiner D. Therapeutic treatment for abdominal obesity in adults. Deutsches Arzteblatt International. 2018;115(29–30):487–493. doi:10.3238/arztebl.2018.0487
14. Du F, Virtue A, Wang H, Yang XF. Metabolomic analyses for atherosclerosis, diabetes, and obesity. Biomarker Res. 2013;1(1):17. doi:10.1186/2050-7771-1-17
15. Sheng J, Yang G, Jin X, et al. Electroacupuncture combined with diet treatment has a therapeutic effect on perimenopausal patients with abdominal obesity by improving the community structure of intestinal flora. Front Physiol. 2021;12:708588. doi:10.3389/fphys.2021.708588
16. Lei H, Chen X, Liu S, Chen Z. Effect of electroacupuncture on visceral and hepatic fat in women with abdominal obesity: a randomized controlled study based on magnetic resonance imaging. J Alternative Complementary Med. 2017;23(4):285–294. doi:10.1089/acm.2016.0361
17. Lam TF, Lyu Z, Wu X, et al. Electro-acupuncture for central obesity: a patient-assessor blinded, randomized sham-controlled clinical trial. BMC Complement Med Ther. 2024;24(1):62. doi:10.1186/s12906-024-04340-5
18. Wujie YE, Jingyu X, Zekai YU, Xingang HU, Yan Z. Systematic review and meta-analysis of acupuncture and acupoint catgut embedding for the treatment of abdominal obesity. J Tradit Chin Med. 2022;42(6):848–857. doi:10.19852/j.cnki.jtcm.2022.06.002
19. Feingold KR. Obesity and Dyslipidemia. In: Feingold KR, Ahmed SF, Anawalt B, editors. Endotext. MDText.com, Inc; 2000.
20. Bays HE, Kirkpatrick CF, Maki KC, et al. Obesity, dyslipidemia, and cardiovascular disease: a joint expert review from the obesity medicine association and the national lipid association 2024. J Clin Lipidol. 2024;18(3):e320–e350. doi:10.1016/j.jacl.2024.04.001
21. Gao Y, Liu W, Ma X, et al. The role of intestinal microbiota and its metabolites in the occurrence and intervention of obesity. Front Microbiol. 2025;16:1559178. doi:10.3389/fmicb.2025.1559178
22. Baek KR, Singh S, Hwang HS, Seo SO. Using gut microbiota modulation as a precision strategy against obesity. Int J Mol Sci. 2025;26(13):6282. doi:10.3390/ijms26136282
23. Augustynowicz G, Lasocka M, Szyller HP, et al. The role of gut microbiota in the development and treatment of obesity and overweight: a literature review. J Clin Med. 2025;14(14):4933. doi:10.3390/jcm14144933
24. Cox AJ, West NP, Cripps AW. Obesity, inflammation, and the gut microbiota. Lancet Diab Endocrinol. 2015;3(3):207–215. doi:10.1016/S2213-8587(14)70134-2
25. Ridaura VK, Faith JJ, Rey FE, et al. Gut microbiota from twins discordant for obesity modulate metabolism in mice. Science. 2013;341(6150):1241214. doi:10.1126/science.1241214
26. Fan Y, Pedersen O. Gut microbiota in human metabolic health and disease. Nat Rev Microbiol. 2021;19(1):55–71. doi:10.1038/s41579-020-0433-9
27. Janssen AW, Kersten S. The role of the gut microbiota in metabolic health. FASEB J. 2015;29(8):3111–3123. doi:10.1096/fj.14-269514
28. Liu R, Hong J, Xu X, et al. Gut microbiome and serum metabolome alterations in obesity and after weight-loss intervention. Nature Med. 2017;23(7):859–868. doi:10.1038/nm.4358
29. Si YC, Ren CC, Zhang EW, et al. Integrative analysis of the gut microbiota and metabolome in obese mice with electroacupuncture by 16S rRNA gene sequencing and HPLC-MS-based metabolic profiling. Am J Chin Med. 2022;50(3):673–690. doi:10.1142/S0192415X22500276
30. Xia X, Xie Y, Gong Y, et al. Electroacupuncture promoted intestinal defensins and rescued the dysbiotic cecal microbiota of high-fat diet-induced obese mice. Life Sci. 2022;309:120961. doi:10.1016/j.lfs.2022.120961
31. Liu X, She C, Li X, et al. Electroacupuncture improves lipid metabolism via proteome and gut microbiota profiling in obese rats. Am J Transl Res. 2025;17(5):4008–4022. doi:10.62347/ZQZS9458
32. Schulz KF, Altman DG, Moher D, Group C. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. doi:10.1136/bmj.c332
33. MacPherson H, Altman DG, Hammerschlag R, et al. Revised standards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. J Alternative Complementary Med. 2010;16(10):ST1–14. doi:10.1089/acm.2010.1610
34. Hunt K, Wyke S, Gray CM, et al. A gender-sensitised weight loss and healthy living programme for overweight and obese men delivered by Scottish premier league football clubs (FFIT): a pragmatic randomised controlled trial. Lancet. 2014;383(9924):1211–1221. doi:10.1016/S0140-6736(13)62420-4
35. Ribeiro G, Fernandes AB, Oliveira FPM, et al. Postingestive reward acts through behavioral reinforcement and is conserved in obesity and after bariatric surgery. PLoS Biol. 2024;22(12):e3002936. doi:10.1371/journal.pbio.3002936
36. Doig GS, Simpson F. Randomization and allocation concealment: a practical guide for researchers. J Crit Care. 2005;20(2):187–91;discussion191–3. doi:10.1016/j.jcrc.2005.04.005
37. Bang H, Ni L, Davis CE. Assessment of blinding in clinical trials. Control Clin Trials. 2004;25(2):143–156. doi:10.1016/j.cct.2003.10.016
38. Tronieri JS, Wadden TA, Walsh OA, et al. Effects of liraglutide plus phentermine in adults with obesity following 1 year of treatment by liraglutide alone: a randomized placebo-controlled pilot trial. Metabolism. 2019;96:83–91. doi:10.1016/j.metabol.2019.03.005
39. Chen X, Huang W, Jin Y, et al. Prescription analysis of electroacupuncture for simple obesity based on complex network technique. Zhongguo Zhen Jiu. 2018;38(3):331–336. doi:10.13703/j.0255-2930.2018.03.028
40. Liu Z, Liu Y, Xu H, et al. Effect of electroacupuncture on urinary leakage among women with stress urinary incontinence: a randomized clinical trial. JAMA. 2017;317(24):2493–2501. doi:10.1001/jama.2017.7220
41. Chen J, Wu F, Wang H, et al. Identification of key taste components in Baccaurea ramiflora Lour. fruit using non-targeted metabolomics. Food Sci Human Wellness. 2023;12(1):94–101. doi:10.1016/j.fshw.2022.07.027
42. Zhou W, Zhou ZY, Hu F, et al. Clinical comparative study on electroacupuncture and acupoint catgut embedding therapy for treatment of obesity. Liaoning J Trad Chin Med. 2020;47:156–159.
43. James KE, Bloch DA, Lee KK, Kraemer HC, Fuller RK. An index for assessing blindness in a multi-centre clinical trial: disulfiram for alcohol cessation--a VA cooperative study. Stat Med. 1996;15(13):1421–1434. doi:10.1002/(SICI)1097-0258(19960715)15:13<1421::AID-SIM266>3.0.CO;2-H
44. Armstrong A, Jungbluth Rodriguez K, Sabag A, et al. Effect of aerobic exercise on waist circumference in adults with overweight or obesity: a systematic review and meta-analysis. Obes Rev. 2022;23(8):e13446. doi:10.1111/obr.13446
45. Siu PM, Yu AP, Chin EC, et al. Effects of Tai Chi or conventional exercise on central obesity in middle-aged and older adults: a three-group randomized controlled trial. Ann Internal Med. 2021;174(8):1050–1057. doi:10.7326/M20-7014
46. Gao Y, Wang Y, Zhou J, Hu Z, Shi Y. Effectiveness of electroacupuncture for simple obesity: a systematic review and meta-analysis of randomized controlled trials. Evidence-Based Complementary Alternative Med. 2020;2020:2367610. doi:10.1155/2020/2367610
47. Cho YK, Lee S, Lee J, et al. Lipid remodeling of adipose tissue in metabolic health and disease. Exp Mol Med. 2023;55(9):1955–1973. doi:10.1038/s12276-023-01071-4
48. Duft RG, Bonfante ILP, Palma-Duran SA, Chacon-Mikahil MPT, Griffin JL, Cavaglieri CR. Moderate-intensity combined training induces lipidomic changes in individuals with obesity and type 2 diabetes. J Clin Endocrinol Metab. 2024;109:2182–2198. doi:10.1210/clinem/dgae177
49. Angelidi AM, Kokkinos A, Sanoudou D, et al. Early metabolomic, lipid and lipoprotein changes in response to medical and surgical therapeutic approaches to obesity. Metabolism. 2023;138:155346. doi:10.1016/j.metabol.2022.155346
50. Li C, Cheng H, Adhikari BK, et al. The role of Apelin-APJ system in diabetes and obesity. Front Endocrinol. 2022;13:820002. doi:10.3389/fendo.2022.820002
51. Volpe S, Lisco G, Fanelli M, et al. Oral semaglutide improves body composition and preserves lean mass in patients with type 2 diabetes: a 26-week prospective real-life study. Front Endocrinol. 2023;14:1240263. doi:10.3389/fendo.2023.1240263
52. Boccardi V. Sarcopenia: a dive into metabolism to promote a multimodal, preventive, and regenerative approach. Mech Ageing Dev. 2024;219:111941. doi:10.1016/j.mad.2024.111941
53. Guo F, Fu L, Lu Z. Effect of electroacupuncture combined with sulforaphane in the treatment of sarcopenia in SAMP8 mice. Iran J Basic Med Sci. 2024;27(5):560–566. doi:10.22038/IJBMS.2024.71345.15509
54. Jin J, Yang Z, Liu H, et al. Effects of acupuncture on the miR-146a-mediated IRAK1/TRAF6/NF-kappaB signaling pathway in rats with sarcopenia induced by D-galactose. Ann Transl Med. 2023;11(2):47. doi:10.21037/atm-22-6082
55. Su Z, Tian C, Wang G, Guo J, Yang X. Study of the effect of intestinal microbes on obesity: a bibliometric analysis. Nutrients. 2023;15(14). doi:10.3390/nu15143255
56. Yan H, Qin Q, Chen J, et al. Gut microbiome alterations in patients with visceral obesity based on quantitative computed tomography. Front Cell Infect Microbiol. 2021;11:823262. doi:10.3389/fcimb.2021.823262
57. Dou D, Chen QQ, Zhong ZQ, Xia XW, Ding WJ. Regulating the enteric nervous system against obesity in mice by electroacupuncture. Neuroimmunomodulation. 2020;27(1):48–57. doi:10.1159/000506483
58. Mruk-Mazurkiewicz H, Kulaszynska M, Czarnecka W, et al. Insights into the mechanisms of action of akkermansia muciniphila in the treatment of non-communicable diseases. Nutrients. 2024;16(11):1695. doi:10.3390/nu16111695
59. Dao MC, Everard A, Aron-Wisnewsky J, et al. Akkermansia muciniphila and improved metabolic health during a dietary intervention in obesity: relationship with gut microbiome richness and ecology. Gut. 2016;65(3):426–436. doi:10.1136/gutjnl-2014-308778
60. Niu H, Zhou M, Zogona D, et al. Akkermansia muciniphila: a potential candidate for ameliorating metabolic diseases. Front Immunol. 2024;15:1370658. doi:10.3389/fimmu.2024.1370658
61. Depommier C, Everard A, Druart C, et al. Supplementation with Akkermansia muciniphila in overweight and obese human volunteers: a proof-of-concept exploratory study. Nat Med. 2019;25(7):1096–1103. doi:10.1038/s41591-019-0495-2
62. Zhao S, Liu W, Wang J, et al. Akkermansia muciniphila improves metabolic profiles by reducing inflammation in chow diet-fed mice. J Mol Endocrinol. 2017;58(1):1–14. doi:10.1530/JME-16-0054
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.