Back to Journals » International Journal of Women's Health » Volume 17
Electroacupuncture for Refractory Chronic Pelvic Pain: A Case Report with 24-Month Follow-Up
Received 28 May 2025
Accepted for publication 10 November 2025
Published 20 November 2025 Volume 2025:17 Pages 4671—4679
DOI https://doi.org/10.2147/IJWH.S541559
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Shuai Gao, Yuanjie Sun, Zhishun Liu
Department of Acupuncture, Guang’ anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China
Correspondence: Zhishun Liu, Department of Acupuncture, Guang’ anmen Hospital, China Academy of Chinese Medical Sciences, No. 5 Beixian’ge Street, Xicheng District, Beijing, 10010, People’s Republic of China, Tel +86 1088001196, Email [email protected]
Introduction: Chronic pelvic pain (CPP) is a common condition involving multiple systems, characterized by complex manifestations and diverse clinical symptoms. The current treatment options for CPP are limited and may be only effective for some patients with identifiable etiologies. This paper aims to report a woman with refractory CPP who experienced significant improvement in pain and quality of life following electroacupuncture (EA) treatment.
Case Summary: A 28-year-old woman experienced abdominal pain (Numeric Rating Scale [NRS] score of 6– 7) after a medical abortion and intense exercise. Despite treatment with leuprolide acetate and pregabalin, her pain persisted (NRS score of 7– 8). In January 2022, she was diagnosed with CPP and underwent superior hypogastric plexus neurolysis. Postoperatively, she experienced severe pain exacerbation (NRS score of 10). Traditional Chinese medicine and acupuncture provided little relief. After 40 sessions of EA treatment, the patient experienced significant relief in pain (from 10 to 2 in the worst NRS score and from 8 to 1 in the average NRS score), and there was also notable improvements in her quality of life and overall health status (from 0.331 to 0.942 in five-level EuroQol five-dimensional questionnaire [EQ-5D-5L] index and from 20 to 80 in the EQ visual analogue scale [EQ VAS]).
Conclusion: EA may be a complementary and alternative therapy for CPP women, particularly when other treatments failed. Additionally, EA may offer potential long-term relief for CPP patients.
Keywords: case report, electroacupuncture, long-term effects, female chronic pelvic pain
Introduction
Chronic pelvic pain (CPP) is defined as pain located within the pelvic region involving the anatomical pelvic cavity, abdomen below the umbilicus, perineum, lumbosacral back, and buttocks, and typically persists over six months.1,2 In addition to pain, CPP is often accompanied by various symptoms, including dyspareunia, anxiety and depression, bowel dysfunction, and urinary frequency and urgency.2,3 These symptoms significantly impact patients’ work productivity, quality of life, and daily social interactions, resulting in a substantial psychological burden as well as healthcare costs for them. It is estimated that CPP affects 2–26% of women worldwide and CPP is the most common symptom presenting in gynecological outpatient clinics, making it a major contributor to healthcare expenditures.4–7
The etiology of CPP is multifactorial and not yet fully understood. It may relate to central sensitization (CS), which includes alterations in sensory processing in the brain, malfunctioning of descending pain inhibitory mechanisms, and cross-sensitization among pelvic structures.8 Additionally, gynecological conditions (such as dysmenorrhea, adenomyosis, and endometriosis, pelvic floor myofascial dysfunction and inflammation) and specific psychological factors may also contribute to CPP.9,10 Current guidelines suggest a multimodal non-surgical management strategy, involving pain neuroscience education, psychotherapy, cognitive-behavioral therapy, complementary and alternative medicine, physical therapy, and pharmacological interventions.9,11 Analgesics, hormonal therapies, neuromodulators, anticonvulsants, and antidepressants are commonly selected for CPP management.10,12 However, these medications primarily target pelvic pain with identifiable etiologies, such as neuropathic or gynecological conditions and offer only temporary alleviation of the symptoms. For the majority of patients, it is difficult to recognize clear etiologies. Moreover, the side effects associated with these medicines, including psychiatric disorders, gastrointestinal discomfort, dizziness and visual disturbances, and the recurrence of symptoms upon discontinuation, significantly limit their clinical application.13 Because of the gradual onset, complex etiology, chronic duration, and recurring nature of CPP, along with the absence of effective treatment options, there is an urgent need to explore a suitable therapeutic approach.
Acupuncture is commonly adopted for CPP patients, which exerts therapeutic effects by inserting needles at specific points on the body.14 Previous studies have shown that the analgesic mechanism of acupuncture may be multifaceted, involving the regulation of the nervous system, anti-inflammatory effects, and modulation of the immune response.15–17 In 2024, the European Association of Urology guideline provided a strong recommendation for the use of acupuncture for chronic prostatitis/chronic pelvic pain (CP/CPPS).18 Systematic reviews showed that acupuncture combined with conventional treatment may offer better potential short-term outcomes for women with CPP compared to conventional treatment alone.19,20 However, the evidence remains insufficient and lacks assessment of long-term efficacy. There is currently little knowledge regarding the efficacy and safety of electroacupuncture (EA) as a standalone treatment for women with CPP. In this paper, we report a case of a woman with refractory CPP who accepted EA and was followed up for 24 months post-treatment.
Case Presentation
In April 2022, a 29-year-old woman presented to Guang’anmen Hospital, China Academy of Chinese Medical Sciences with a 10-month history of recurrent lower abdominal pain. In July 2021, she had undergone a medical abortion and subsequently engaged in intense exercise, which leads to diffuse abdominal pain characterizing a stabbing and burning sensation and with a score of 6–7 on Numeric Rating Scale (NRS). The pain was persistent throughout the day, and was exacerbated by fatigue and emotional fluctuations. In October 2021, due to the persistence of pain without relief, she consulted Peking Union Medical College Hospital, where ultrasound examination showed that the echo of the uterine myometrium was uneven. MRI demonstrated a slight patchy abnormal signal in the left uterine wall, with adenomyosis not excluded. Culture of the discharge showed no gonorrheal, chlamydial, mycoplasmal, and trichomonal infections. Based on her history of dysmenorrhea and imaging findings, she was diagnosed with adenomyosis and treated with injections of leuprolide acetate 3.75 mg monthly for three months, during which she experienced amenorrhea. However, there was no significant pain relief, with a NRS score of 7–8. Subsequently, she discontinued leuprolide acetate and pregabalin 75 mg twice a day was prescribed. This initially provided a 20% reduction in pain. However, with continued use of pregabalin, the pain relief became less noticeable, which prompted the patient to discontinue it herself.
In January 2022, seeking further evaluation and treatment, she visited Peking University People’s Hospital. Physical examination identified trigger points (tender areas that reproduced the pain symptoms) in the bilateral coccygeus, obturator, levator ani muscles and sciatic spines. Considering the duration of pelvic pain lasting more than six months and in conjunction with the laboratory and imaging reports, she was diagnosed with CPP and received C-arm-guided chemical neurolysis of the superior hypogastric plexus with 15 mL of 95% ethanol. Postoperatively, duloxetine 20 mg twice a day was prescribed for one week. On the third postoperative day, she experienced acute exacerbation of severe pain radiating to her back, recurring 3–4 days a week, with a NRS score of 10. She was preoccupied with thoughts of her pain throughout the day, even experiencing suicidal ideation. Pregabalin 75 mg twice a day was prescribed again. In the following two months, she attempted traditional Chinese medicine, including Chinese herbal medicine and acupuncture, but with poor response (shown in Figure 1).
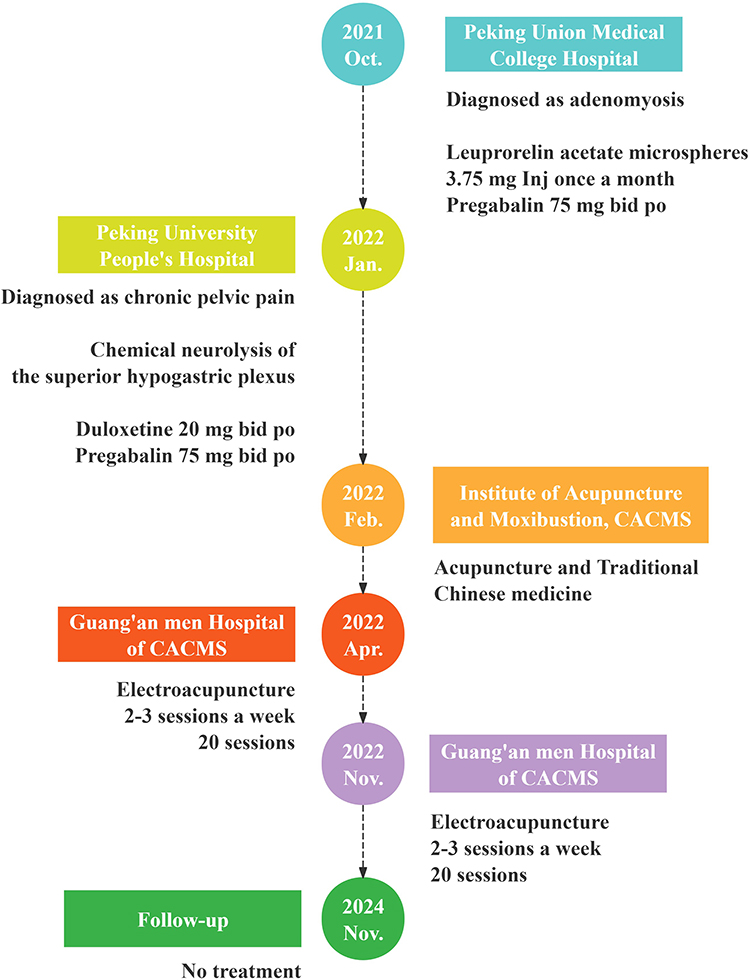 |
Figure 1 The timeline of the patient’s treatment. Abbreviations: CACMS, China Academy of Chinese Medical Sciences. |
Current symptoms: The patient presented with severe lower abdominal pain that impaired ambulation, accompanied by lumbar discomfort and lassitude. Bowel movements were hard and infrequent. Her tongue was purple with a thin white coating and her pulse was thread and string-like.
Electroacupuncture Treatment
After providing informed consent, the patient underwent EA treatment administered by an acupuncturist with 30 years of clinical experience. After routine disinfection of the skin, stainless steel needles (Hwato, 0.30×40 mm or 0.30×75 mm, Suzhou Medical Appliance Factory) were inserted into following acupoints: Shangyintang (On the head, 1 B-cun superior to Yintang), Zhongwan (CV12), Tianshu (ST25), Guanyuan (CV4), Zhongji (CV3), Zigong (EX-CA1), Shenshu (BL23), Ciliao (BL32), Zhongliao (BL33), Huiyang (BL35) and Sanyinjiao (SP6). BL32, BL33 and BL35 were inserted by needles of 0.30×75 mm size with a depth of 60–70 mm. Other acupoints were vertically inserted by needles of 0.30×40 mm size with a depth of 25–35 mm. BL32, BL33, BL35 and SP6 were transversally connected by EA therapeutic apparatus (Hwato, Suzhou Medical Appliance Factory). EA stimulation lasted for 30 minutes with a continuous wave of 5 Hz and current intensity of 0.5–2.0 mA for SP6 and 1–5 mA BL32, BL33 and BL35 based on the patient’s tolerance. The patient received a total of 4-month EA treatment, consisting of two 2-month courses. Each course involved three sessions per week for the first four weeks, followed by two sessions per week for the next four weeks, totaling 40 sessions (a minimum 24 hours interval between any two consecutive sessions). Two predefined prescriptions of acupoints were used. Prescription A: Shangyintang, CV12, CV4, CV3, bilateral ST25 and EX-CA1. Prescription B: bilateral BL23, BL32, BL33, BL35 and SP6. For the first course, both prescriptions A and B were used on the same day, with a 30-minute needle retention for each prescription, totaling 60 minutes per session. The second course involved treatment in either a prescription A or B on alternating treatment days, with a 30-minute retention per session.
Follow-Up and Outcomes
The patient’s pain intensity and health status were evaluated using the NRS, the five-level EuroQol five-dimensional questionnaire (EQ-5D-5L, including the EQ-5D-5L index and EQ visual analogue scale [EQ VAS]), and Patient Global Impression of Change (PGIC) during both treatment and follow-up period. The NRS was used to assess the severity of pain which consists of 11 numbers, ranging from 0 (no pain) to 10 (the most severe pain imaginable).21,22 Health-related quality of life was assessed using the EQ-5D-5L questionnaire, with higher scores indicating better quality of life.23,24 It comprises two parts: a health state description based on five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and VAS estimating overall health status ranging from 0 (worst) to 100 (best).
After one month of EA, the patient reported pain relief, with the worst NRS score decreasing by 40% (from 10 to 6) and the average NRS score dropping by 37.5% (from 8 to 5, Figure 2). The EQ-5D-5L index improved from 0.331 to 0.782, and EQ VAS values increased from 20 to 50 (Figure 3). The PGIC rating was “much improved” and the patient discontinued pregabalin. The patient reported normal bowel movements and stable mental status. In the second month of EA treatment, further improvements were noted, with both the worst and the average NRS scores decreasing to 2 (reducing by 80% and 75%, respectively). The EQ-5D-5L index rose to 0.942, and EQ VAS values increased to 80 (Figure 3), with the PGIC rating “very much improved”. Feeling that the pain had nearly resolved, the patient chose to discontinue treatment and return to work. Nevertheless, two months later, the pain recurred, with the worst NRS pain score of 5, average NRS score of 4, EQ-5D-5L index value of 0.564, and EQ VAS scores of 60, prompting the patient to resume EA (Figures 2 and 3). After another two months of EA treatment, pain levels significantly decreased again, with the worst NRS score dropping to 2 and the average NRS score to 1 (Figure 2). The patient reported occasional mild lower-abdominal pain that did not interfere with daily activities and denied lumbar discomfort, resulting in her decision to stop treatment. Her tongue was pale red with a thin whit coating, and her pulse was thread. EQ-5D-5L health-related subscale assessments revealed that the most significantly affected aspects for this patient were mobility, pain/discomfort, and emotional disorders. Correspondingly, improvements in these three domains were also the most pronounced following EA treatment (Figure 4). Over the 24 months follow-up period, the patient reported no recurrence of pain, indicating the long-term efficacy of EA. No adverse events were observed during the treatment and follow-up period.
 |
Figure 2 The assessment of worst and average numerical rating scale pain scores. Abbreviations: NRS, numerical rating scale score; EA, electroacupuncture. |
 |
Figure 3 The assessment of the five-level EuroQol five-dimensional questionnaire scores. Abbreviations: EA, electroacupuncture; EQ, EuroQol five-dimensional questionnaire; EQ VAS, EQ visual analogue scale. |
 |
Figure 4 The assessment of the five-level EuroQol five-dimensional questionnaire subscales. (A) The assessment of the EQ mobility subscale scores; (B) The assessment of the EQ personal care subscale scores; (C) The assessment of the EQ daily activities subscale scores; (D) The assessment of the EQ pain subscale scores; (E) The assessment of the EQ anxiety/depression subscale scores; (F) The assessment of the EQ VAS scores. Abbreviations: EA, electroacupuncture; EQ, EuroQol five-dimensional questionnaire; EQ VAS, EQ visual analogue scale. |
Discussion
In this case report, we present a woman with refractory CPP who, after an unsuccessful response to various medical and surgical interventions, experienced significant symptom alleviation treated by EA. Notably, the benefits of EA were sustained for at least 24 months post-treatment, suggesting that EA could be a viable option for the management of CPP.
CPP is the most common symptom in gynecological consultations, affecting around one-quarter of women globally, with a prevalence as frequent as that of asthma and migraines.4,25 Due to the complex, multifactorial nature of CPP, treatment methods remain controversial. Current consensus suggest that pain relief should not be the sole objective, rather, it is important to interdisciplinary management addressing key concerns based on each patient’s specific circumstances (including sleep, mood, work, social and sexual activities), with the goal of enhancing overall quality of life.9,26
Modern medical treatments for CPP typically include pharmacological, conservative and surgical interventions. Leuprolide acetate, a gonadotropin-releasing hormone agonist, has been proven to alleviate dysmenorrhea, anemia, and reduce uterine volume in patients with adenomyosis.27–29 However, there was no significant relief of pelvic pain, indicating that adenomyosis was not the only cause of her CPP. Neuropathic components are increasingly recognized in CPP, with approximately one-third of patients exhibiting neurological symptoms.30 Neuromodulators, like pregabalin and gabapentin, are commonly used for neuropathic pain. The patient initially experienced pain relief after starting pregabalin, yet the analgesic effect waned as treatment duration extended. This is consistent with findings from other studies, which did not demonstrate that these medicines were more effective than placebo in treating pelvic pain.13,31
Following the ineffective pharmacological therapies, the patient was referred for surgical intervention. The superior hypogastric plexus receives nociceptive stimuli from pelvic visceral pain, and transmits signals to the central nervous system, thereby generating pain. This pathway can be interrupted by nerve block with alcohol or phenol.32 Neuro-destructive procedures have demonstrated efficacy in various pelvic pain conditions, including cancer pain and secondary dysmenorrhea, with significant reductions in pain levels and decreased medication usage.33–35 In this research, the patient experienced sudden pain postoperatively, which was severe and intolerable. Previous studies have identified the risk of transient back pain, nerve injury, hypotension and other mild adverse effects associated with the surgery, but an exacerbation of pain has never been reported.32,36
In concern of chronic pain, CS is a pivotal mechanism, especially in patients with CPP of unknown etiology, where symptoms of CS (such as generalized pain, sleep disturbances, and mood disorders) should be identified as key feature.10 In this case, the patient had no definitive etiology and presented with significant emotional disturbances. Despite trying various medical approaches, the patient experienced limited symptom relief. Given the potential presence of CS, thus EA was chosen as the treatment method. EA is a therapeutic modality that combines acupuncture with electrical stimulation, providing a more consistent and controllable level of stimulation through adjustable electric currents. This method is particularly useful for conditions that may require more intensive stimulation, such as chronic pain, muscle spasms, and some neurological disorders.37,38 The potential mechanisms underlying the efficacy of EA in alleviating CPP are multifaceted, encompassing modulation of various neurotransmitters and neuromodulators, regulation of inflammatory pathways, normalization of neural plasticity, stimulation of descending inhibitory pathways, improve emotional disorders, and enhance overall physical condition, thereby improving quality of life.14,15,39 Therefore, for CPP, a disease characterized by diverse symptoms and unclear etiology, EA may be a suitable option due to its broad and multifaceted therapeutic effects.
In Traditional Chinese medicine theory, medical abortion is held to injure the uterus and exhaust qi and blood. Vigorous exercise after the procedure further consumes the blood and qi, resulting in static blood. The core pattern is therefore dual qi deficiency with blood stasis, for which the treatment principle is to tonify qi and blood, activate blood and resolve stasis. Because the Ren, Spleen and Stomach meridians all pass the lower abdomen, points (CV12, CV4, CV3, SP6 and ST25) along these three meridians were selected. Following the anterior-posterior point combination principle, lumbosacral acupoints belonging to bladder meridian (BL23, BL32, BL33 and BL35) were adopted. The two groups of points acted synergistically to regulate qi–blood and relieve pain. Anatomically, the sacral nerves distribute to BL32 and BL33, the tibial nerve (a branch of the sacral plexus) courses near SP6, and BL35 lies close to the pudendal nerve.40,41 The nerves distribution of EX-CA1, CV4, CV3, and ST25 overlaps with the spinal segments that innervate the ovaries and uterus.42 Stimulating these acupoints may therefore produce analgesia by direct inhibition at the spinal level.
For patients with chronic pain lasting a year or more, a few months of relief, while welcome, raises the crucial question of whether the intervention offers long-term benefits. The principal clinical significance of our findings is that we could reassure women with CPP refractory to various measures that EA may not only improve symptoms and quality of life but also maintain the therapeutic benefits for 24 months post-treatment. This result is consistent with findings from a previous study, which demonstrated that, compared to no acupuncture, the effects of acupuncture on chronic pain did not significantly decline within 12 months after therapy cessation.43
Strengths and Limitations
The strength of this study lies in its status as the first to describe the effects of EA on CPP in women, with a 24-month follow-up to assess the long-term efficacy of EA. However, this report also has several limitations. First, as a single-case study, it lacks a control arm; consequently, we cannot rule out placebo effects attributable to either the EA intervention itself or the additional attention and expectation. Second, the findings may not be generalisable to the broader CPP population, given the variability in pain etiology and psychosomatic factors among individual patients. Third, the data may be insufficient to formulate a standardized, optimized acupuncture regimen for future clinical use. Finally, although pain and quality-of-life scores improved markedly compared with baseline, mild pain persisted at follow-up, indicating that complete symptom resolution was not achieved.
Conclusions
Although this report is confined to a single case, it offers preliminary evidence that EA may serve as a potential alternative for women with CPP who are refractory to conventional therapy, and demonstrates a sustained effect lasting 24 months. To advance the clinical application of EA and facilitate its integration into multidisciplinary pain management strategies, future research should focus on large-scale, randomized controlled trials to validate our findings and develop standardized, evidence-based protocols.
Abbreviations
CPP, chronic pelvic pain; CS, central sensitization; CP/CPPS, chronic prostatitis/chronic pelvic pain; EA, electroacupuncture; NRS, Numeric Rating Scale; EQ-5D-5L, five-level EuroQol five-dimensional questionnaire; VAS, visual analogue scale; ST25, Tianshu; CV4, Guanyuan; CV3, Zhongji; EX-CA1, Zigong; BL23, Shenshu; BL32, Ciliao; BL33, Zhongliao; BL35, Huiyang; SP6, Sanyinjiao; PGIC, Patient Global Impression of Change.
Data Sharing Statement
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent for Publication
This case report has been approved by the Ethics Committee of Guang’ anmen Hospital, China Academy of Chinese Medical Sciences [Approval number: 2024-043-KY], which explicitly authorized publication of anonymized case details. The research procedure was explained to the patient, and written informed consent was obtained for the publication of this case report and any related images.
Acknowledgments
The authors thank the patient for consenting to the publication of this report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the High Level Chinese Medical Hospital Promotion Project (grant no. HLCMHPP2023089) and the China Academy of Chinese Medical Sciences Innovation Fund (grant no. CI2021A03518).
Disclosure
The authors declare that they have no commercial or financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Gynaecologists RCoOa. Chronic pelvic pain, initial management (Green-top Guideline no. 41). 2017.
2. Pain CP. Chronic Pelvic Pain: ACOG Practice Bulletin, Number 218. Obstet Gynecol. 2020;135(3):e98–e109. doi:10.1097/AOG.0000000000003716
3. Shoskes DA, Nickel JC, Dolinga R, Prots D. Clinical phenotyping of patients with chronic prostatitis/chronic pelvic pain syndrome and correlation with symptom severity. Urology. 2009;73(3):538–542. discussion 542-533. doi:10.1016/j.urology.2008.09.074
4. Ahangari A. Prevalence of chronic pelvic pain among women: an updated review. Pain Physician. 2014;17(2):E141–147. doi:10.36076/ppj.2014/17/E141
5. Maturen KE, Akin EA, Dassel M, et al. ACR appropriateness criteria(®) postmenopausal subacute or chronic pelvic pain. J Am Coll Radiol. 2018;15(11s):S365–s372. doi:10.1016/j.jacr.2018.09.023
6. Huang G, Le AL, Goddard Y, et al. A systematic review of the cost of chronic pelvic pain in women. J Obstet Gynaecol Can. 2022;44(3):286–293.e283. doi:10.1016/j.jogc.2021.08.011
7. Latthe P, Latthe M, Say L, Gülmezoglu M, Khan KS. WHO systematic review of prevalence of chronic pelvic pain: a neglected reproductive health morbidity. BMC Public Health. 2006;6(1):177. doi:10.1186/1471-2458-6-177
8. Kaya S, Hermans L, Willems T, Roussel N, Meeus M. Central sensitization in urogynecological chronic pelvic pain: a systematic literature review. Pain Physician. 2013;16(4):291–308. doi:10.36076/ppj.2013/16/291
9. Allaire C, Yong PJ, Bajzak K, et al. Guideline No. 445: management of chronic pelvic pain. J Obstet Gynaecol Can. 2024;46(1):102283. doi:10.1016/j.jogc.2023.102283
10. Lamvu G, Carrillo J, Ouyang C, Rapkin A. Chronic pelvic pain in women: a review. JAMA. 2021;325(23):2381–2391. doi:10.1001/jama.2021.2631
11. Starzec-Proserpio M, Frawley H, Bø K, Morin M. Effectiveness of nonpharmacological conservative therapies for chronic pelvic pain in women: a systematic review and meta-analysis. Am J Obstet Gynecol. 2024;232(1):42–71. doi:10.1016/j.ajog.2024.08.006
12. Speer LM, Mushkbar S, Erbele T. Chronic pelvic pain in women. Am Fam Physician. 2016;93(5):380–387.
13. Horne AW, Vincent K, Hewitt CA, et al. Gabapentin for chronic pelvic pain in women (GaPP2): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet. 2020;396(10255):909–917. doi:10.1016/S0140-6736(20)31693-7
14. Lin KY, Chang YC, Lu WC, Kotha P, Chen YH, Tu CH. Analgesic efficacy of acupuncture on chronic pelvic pain: a systemic review and meta-analysis study. Healthcare. 2023;11(6). doi:10.3390/healthcare11060830
15. Wang H, Zhang J, Ma D, Zhao Z. The role of acupuncture and its related mechanism in treating chronic prostatitis/chronic pelvic pain syndrome. Int J Gen Med. 2023;16:4039–4050. doi:10.2147/IJGM.S417066
16. Lee IS, Cheon S, Park JY. Central and peripheral mechanism of acupuncture analgesia on visceral pain: a systematic review. Evid Based Complement Alternat Med. 2019;2019:1304152. doi:10.1155/2019/1304152
17. Qin P, Cao X, Ni H, et al. Efficacy of different acupuncture therapies for chronic prostatitis/chronic pelvic pain syndrome: a network meta-analysis. J Pain Res. 2025;18:3653–3673. doi:10.2147/JPR.S530646
18. (EAU) EAoU. Guidelines on chronic pelvic pain. 2022.
19. Zheng J, Lai X, Zhu W, Huang Y, Chen C, Chen J. Effects of acupuncture combined with rehabilitation on chronic pelvic pain syndrome in females: a meta-analysis running head-acupuncture combined with rehabilitation on chronic pelvic pain. J Healthc Eng. 2022;2022:8770510. doi:10.1155/2022/8770510
20. Sung SH, Sung AD, Sung HK, An TE, Kim KH, Park JK. Acupuncture treatment for chronic pelvic pain in women: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2018;2018(1):9415897. doi:10.1155/2018/9415897
21. de Arruda GT, Driusso P, Rodrigues JC, de Godoy AG, Avila MA. Numerical rating scale for dysmenorrhea-related pain: a clinimetric study. Gynecol Endocrinol. 2022;38(8):661–665. doi:10.1080/09513590.2022.2099831
22. Goudman L, Pilitsis JG, Billet B, et al. The level of agreement between the numerical rating scale and visual analogue scale for assessing pain intensity in adults with chronic pain. Anaesthesia. 2024;79(2):128–138. doi:10.1111/anae.16151
23. Luo N, Liu G, Li M, Guan H, Jin X, Rand-Hendriksen K. Estimating an EQ-5D-5L value set for China. Value Health. 2017;20(4):662–669. doi:10.1016/j.jval.2016.11.016
24. Foundation ER. EQ-5D-5L User Guide, Version 3.0, 2019.
25. Zondervan K, Barlow DH. Epidemiology of chronic pelvic pain. Baillieres Best Pract Res Clin Obstet Gynaecol. 2000;14(3):403–414. doi:10.1053/beog.1999.0083
26. Turk DC, Dworkin RH, Revicki D, et al. Identifying important outcome domains for chronic pain clinical trials: an IMMPACT survey of people with pain. Pain. 2008;137(2):276–285. doi:10.1016/j.pain.2007.09.002
27. Donnez J, Tomaszewski J, Vázquez F, et al. Ulipristal acetate versus leuprolide acetate for uterine fibroids. N Engl J Med. 2012;366(5):421–432. doi:10.1056/NEJMoa1103180
28. Ji M, Yuan M, Jiao X, et al. A cohort study of the efficacy of the dienogest and the gonadotropin-releasing hormone agonist in women with adenomyosis and dysmenorrhea. Gynecol Endocrinol. 2022;38(2):164–169. doi:10.1080/09513590.2021.2000961
29. Kashiwabara S, Yabe S, Samejima K, et al. A study on the efficacy and safety of long-term adjusted low-dose gonadotropin-releasing hormone agonist therapy for uterine fibroids and adenomyosis. J Obstet Gynaecol Res. 2024;50(12):2319–2326. doi:10.1111/jog.16128
30. George AK, Sadek MA, Saluja SS, Fariello JY, Whitmore KE, Moldwin RM. The impact of neuropathic pain in the chronic pelvic pain population. J Urol. 2012;188(5):1783–1787. doi:10.1016/j.juro.2012.07.034
31. Aboumarzouk OM, Nelson RL. Pregabalin for chronic prostatitis. Cochrane Database Syst Rev. 2012;2012(8):Cd009063. doi:10.1002/14651858.CD009063.pub2
32. Hou S, Novy D, Felice F, Koyyalagunta D. Efficacy of superior hypogastric plexus neurolysis for the treatment of cancer-related pelvic pain. Pain Med. 2020;21(6):1255–1262. doi:10.1093/pm/pnz151
33. Urits I, Jones MR, Orhurhu V, et al. A comprehensive review of the celiac plexus block for the management of chronic abdominal pain. Curr Pain Headache Rep. 2020;24(8):42. doi:10.1007/s11916-020-00878-4
34. Abdelghaffar NA, Farahat TE. Fluoroscopic anterior approach versus ultrasound guided superior hypogastric plexus neurolysis in cancer pelvic pain: a randomized controlled study. BMC Anesthesiol. 2022;22(1):403. doi:10.1186/s12871-022-01948-3
35. Yang X, You J, Tao S, Zheng X, Xie K, Huang B. Computed tomography-guided superior hypogastric plexus block for secondary dysmenorrhea in perimenopausal women. Med Sci Monit. 2018;24:5132–5138. doi:10.12659/MSM.906970
36. Abdelghafar EM, Othman AH, Soliman MS, Kilany A, Shaaban MH, Shaker EH. The role of double modality ultrasonographic and fluoroscopic guided superior hypogastric plexus neurolysis in treating intractable pelvic cancer pain: a comparative study. J Pain Res. 2021;14:1465–1473. doi:10.2147/JPR.S308743
37. Kong JT, Puetz C, Tian L, et al. Effect of electroacupuncture vs sham treatment on change in pain severity among adults with chronic low back pain: a randomized clinical trial. JAMA Network Open. 2020;3(10):e2022787. doi:10.1001/jamanetworkopen.2020.22787
38. Hu R, Xu Z, Dang M, et al. Comprehensive electroacupuncture treatments reduce serum inflammatory factors and relieve pain symptoms in patients with lumbar disc herniation-a systematic review and network meta-analysis. Int J Surg. 2024;111(1):1526–1530.
39. Wu Z, Shen Z, Xu Y, et al. A neural circuit associated with anxiety-like behaviors induced by chronic inflammatory pain and the anxiolytic effects of electroacupuncture. CNS Neurosci Ther. 2024;30(4):e14520. doi:10.1111/cns.14520
40. Sahin S, Bicer M, Eren GA, et al. Acupuncture relieves symptoms in chronic prostatitis/chronic pelvic pain syndrome: a randomized, sham-controlled trial. Prostate Cancer Prostatic Dis. 2015;18(3):249–254. doi:10.1038/pcan.2015.13
41. Sun Y, Liu Y, Chen H, Yan Y, Liu Z. Electroacupuncture for stress-predominant mixed urinary incontinence: a protocol for a three-armed randomised controlled trial. BMJ Open. 2021;11(1):e038452. doi:10.1136/bmjopen-2020-038452
42. Qu F, Li R, Sun W, et al. Use of electroacupuncture and transcutaneous electrical acupoint stimulation in reproductive medicine: a group consensus. J Zhejiang Univ Sci B. 2017;18(3):186–193. doi:10.1631/jzus.B1600437
43. MacPherson H, Vertosick EA, Foster NE, et al. The persistence of the effects of acupuncture after a course of treatment: a meta-analysis of patients with chronic pain. Pain. 2017;158(5):784–793. doi:10.1097/j.pain.0000000000000747
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.