Back to Journals » Clinical Interventions in Aging » Volume 15
Elder Abuse Assessment Tools and Interventions for use in the Home Environment: a Scoping Review
Authors Van Royen K ![]() , Van Royen P
, Van Royen P ![]() , De Donder L
, De Donder L ![]() , Gobbens RJ
, Gobbens RJ ![]()
Received 8 May 2020
Accepted for publication 3 July 2020
Published 28 September 2020 Volume 2020:15 Pages 1793—1807
DOI https://doi.org/10.2147/CIA.S261877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Kathleen Van Royen,1,2 Paul Van Royen,1 Liesbeth De Donder,3 Robbert J Gobbens1,4,5
1Department of Primary and Interdisciplinary Care, University of Antwerp, Antwerp, Belgium; 2Department of Communication Studies, University of Antwerp, Antwerp, Belgium; 3Faculty of Psychology and Educational Sciences, Vrije Universiteit Brussel (VUB), Brussels, Belgium; 4Faculty of Health, Sports and Social Work, Inholland University of Applied Sciences, Amsterdam, the Netherlands; 5Zonnehuisgroep Amstelland, Amstelveen, the Netherlands
Correspondence: Kathleen Van Royen
Department of Primary and Interdisciplinary Care, University of Antwerp, Gouverneur Kinsbergencentrum, Doornstraat 331-2610, Doornstraat, Wilrijk, Belgium
Tel +32 32655099
Email [email protected]
Background and Aim: Caregivers in the home environment have an important role in timely detecting and responding to abuse. The aim of this review was to provide insight into both the existing tools for the assessment of and interventions for elder abuse by formal and informal caregivers in the home environment, and to categorize them according to a public health perspective, into primary, secondary, tertiary or quaternary prevention.
Methods: We selected the assessment tools and interventions that can be used by caregivers in the home environment included in previous reviews by Gallione et al (2017) and Fearing et al (2017). To identify published studies after these reviews, a search was performed using PubMed, Cochrane Database, CINAHL and Web of Science.
Results: In total, fifteen assessment tools and twelve interventions were included. The number of assessment tools for elder abuse for use in the home environment is increasing; however, tools must be validated over different cultures and risk groups. In addition, the tools lack attention for the needs of vulnerable older persons such as persons with dementia. Existing interventions for caregivers in the home environment lack evidence for addressing elder abuse and do not address potential adverse effects (quaternary prevention).
Conclusion: Assessment tools for elder abuse need further testing for validity and reliability for use by caregivers in the home environment. For interventions, meaningful outcome measures are needed. Important to note is that quaternary prevention requires more attention. This argues for taking into account perspectives of (abused) older persons and caregivers in the development of assessment tools and interventions protocols.
Keywords: caregivers, elder abuse management, prevention, assessment tools, interventions, review
Introduction
In 2017, globally there were an estimated 962 million people aged 60 or more, comprising 13% of the global population.1 Demographic projections demonstrate that the proportions of old people will continue to grow, so that by 2050 all regions of the world except Africa will have nearly a quarter or more of their populations at ages 60 and above. This rapid ageing of the population leads to an increasing number of people staying at home. Aging-in-place policies have been implemented by many Western governments,2 leading to a shift towards home‐based care and significant roles for care partners and home care services.3,4
Population aging is also expected to result in higher abuse rates of older persons, a worldwide problem urgently requiring attention. A recent systematic review and meta-analysis 5 shows that abuse affects one in six older persons worldwide, which amounts to approximately 141 million people. However, prevalence figures of elder abuse vary widely.5,6 The variance in prevalence rates can be explained by the following factors: the difference in definitions of elder abuse studied or explored, categories of types of elder abuse, measurements and instruments used, time frames examined, populations, age restrictions, income classification of the country, sampling methods and sample sizes and research designs used. All these differences make it extremely difficult, if not virtually impossible, to compare results on the prevalence of elder abuse from the different studies undertaken.5,6 The definition of the World Health Organization (WHO) is frequently used. In their Toronto Declaration the WHO describes elder abuse as
A single or repeated act, or lack of appropriate action, occurring within any relationship where there is an expectation of trust which causes harm or distress to an older person.7
Six different types of elder abuse can be distinguished: physical, psychological, sexual, financial abuse, neglect and violation of personal rights.6
Despite higher abuse rates, elder abuse continues to be a neglected problem, particularly compared to child abuse and domestic violence. In addition, the urgency to tackle older persons’ abuse is all the more important given the adverse outcomes for the victims: physical health problems, including increased hospitalization and mortality; psychological distress; loss of property and security.8–10 Evidence demonstrates that elder abuse has high economic costs, including direct healthcare costs for treatment and rehabilitation as well as provision of protection and care by the legal and social system.11
Previous reviews of Fearing et al12 and Gallione et al13 only focused either on tools for the assessment or on interventions for elder abuse. To manage elder abuse by caregivers in the home environment, it is important we have insight in which validated instruments exist and at the same time can be used in the home environment, both in terms of assessment and intervention. This review also categorized all included elder abuse assessment tools and interventions according to a public health perspective into primary, secondary or tertiary prevention.11
Primary prevention concerns interventions that are designed to avoid the occurrence of elder abuse and focus on eliminating risk factors. These include risk assessment tools, programs to identify and support caregivers who are at “high risk” of abusing or for example programs for older people to prepare for less capability (eg, legal/financial tools).14 Secondary prevention is aimed at preventing further abuse or harm by early detecting abuse with the help of screening instruments intended to detect and measure elder abuse. Other programs include counseling for victims or legal protection. Tertiary prevention includes actions to manage the consequences of elder abuse such as justice system services and medical follow-up11 as well as programs to prevent further re-victimization such as housing, counselling and legal services.14 In addition, we will also look at mechanisms to control negative consequences or side-effects of interventions, also known as quaternary prevention or actions to prevent more harm than good.15 This can be due to, for example, inappropriate risk assessment, a breach of confidentiality, invasion of privacy and failure in safety plan.16
Objectives
With this scoping review, the overall aim is to provide insight in which tools are available for the assessment of and which interventions for elder abuse, specifically for informal caregivers and professionals in the home environment.
Given that cases of elder abuse are often left undetected, it is important for health care providers and social workers who are ideally placed to recognize the abuse of older persons, to equip them with the right tools. Therefore, it is important to identify effective assessment instruments.
Several studies have been conducted to review instruments intended to detect and measure elder abuse.13,17,18 Currently there is no gold standard test for identifying elder abuse,18 due to numerous tools and different methods employed in various studies, coupled with varying definitions of thresholds for age. Gallione et al13 presented eleven measurement instruments for elder abuse. Based on their findings they concluded that several measurements have been tested, but none have been evaluated against measurable violence or health outcomes, premature death and disability or the adverse outcomes of screening and interventions. In addition, no study evaluated the acceptability of the instruments by older people themselves.13
Next to the assessment, it is particularly important to develop and implement effective interventions, both focused on the prevention and management of elder abuse. Systematic reviews and meta-analyses were conducted focused on providing an overview of interventions designed to prevent or stop elder abuse.12,19,20 In the study by Ploeg et al20 the findings suggested insufficient evidence to support any intervention associated with elder abuse addressed to the victims, perpetrators, or healthcare professionals. Ayalon et al19 included 24 studies which were divided into three groups: (i) interventions designed to improve the ability of healthcare professionals to identify and stop elder abuse, (ii) Interventions that target the victims, and (iii) interventions focused on caregivers who maltreat older people. The majority of these studies were carried out in a nursing home and addressed people with dementia. Interventions with the aim to reduce physical restraint in nursing homes proved to have the greatest empirical support.
A Cochrane review was performed by Baker et al.11 This review demonstrates that among the interventions for preventing elder abuse there is inadequate evidence to assess the effects of these interventions on occurrence or recurrence of elder abuse. Some evidence was present that interventions might change depression in combination with anxiety by the caregivers. In addition, it is not certain that educational interventions improve the relevant knowledge of both healthcare professionals and caregivers.
The last systematic review was conducted byFearing et al12 aiming to review the efficacy of community-based interventions for elder abuse. The authors12 identified nine studies of which only two studies with Level-1 evidence. They emphasize the importance of further research in order to elevate knowledge concerning elder abuse and to develop effective interventions on identification and management.
Materials and Methods
Aforementioned studies about instruments for the identification of elder abuse were conducted until May 201513 and interventions on prevention and management of elder abuse until December 2015.12 The aim of the present study is to update the evidence with regard to these tools and interventions, as well as distinguish between the different types of prevention (primary, secondary, tertiary and quaternary prevention). We searched for instruments aimed at secondary (screening tools) and tertiary prevention (interventions to address elder abuse when it has occurred); however, in addition we look whether the included instruments focus on primary or quaternary prevention. In our review, we focus on community-dwelling older people. Since the scope is limited to elder abuse in the home environment, excluding residential settings, we will focus exclusively on tools to be used by healthcare professionals or informal caregivers coming in the home environment of older people.
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR).21
Assessment Tools
For providing insight in which tools are available for the assessment of elder abuse we are building on the content and methods of the systematic review by Gallione et al.13 We used the following inclusion criteria:
- The study includes community-dwelling people aged 60 years and older
- The study describes a measurement tool for the assessment of elder abuse, of which the validity was established
- The tool can be used by caregivers (informal or formal) in the home environment
- No applied restriction to type of instrument (e.g. self-report questionnaire, interview)
- No applied restriction to type of elder abuse
- Articles in English, French, German, and Dutch
The databases PubMed (including MEDLINE), Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Web of Science were consulted by two researchers (RG, KVR), to search for relevant studies that were published in the period after May 2015; after the review by Gallione et al.13 We finished our search on August 31, 2019. We used the following search terms: For Cochrane “elder abuse” and for the other databases: “elder abuse OR elder neglect* OR elder maltreat* AND assess* OR screen* OR diagnosis”. See Figure 1 for our search outcomes.
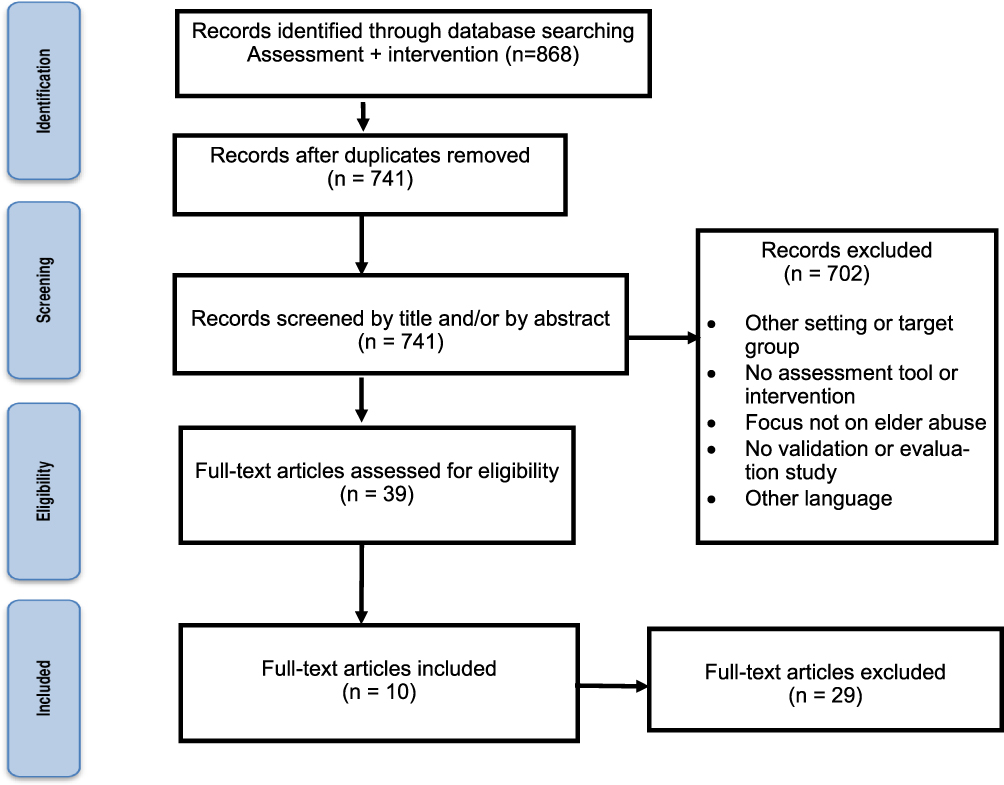 |
Figure 1 Flow chart of search strategy for new tools. |
Interventions
Our starting point for updating the evidence with regard to interventions aiming to prevent or manage elder abuse was the systematic review on community-based interventions conducted by Fearing et al.12 For this part of our scoping review we used the inclusion criteria:
- The study includes community-dwelling people aged 60 years and older
- The study describes an intervention focused on preventing or managing elder abuse and assesses the effect of the intervention
- The intervention can be applied by caregivers (informal or formal)
- No applied restriction to type of intervention (e.g. individual, group)
- No applied restriction to type of elder abuse
- Articles in English, French, German, and Dutch
Following the review by Fearing et al12 we used the keywords “elder abuse* OR elder neglect* OR elder maltreat* AND prevent* OR interven* OR program*” to search within each database. Because the authors12 searched for relevant studies until December 2015, we examined which studies were published thereafter (until June 30, 2019).
Aforementioned databases were consulted by the two researchers (RG, KVR). All titles and abstracts were reviewed by two independent researchers (RG, KVR) based on the inclusion criteria. In case of disagreements, a consensus was established.
Data extraction was conducted independently by the same two researchers. Disagreements were discussed with a third researcher (PVR) until a consensus agreement was reached. Extraction details are presented in Tables 1 and 2.
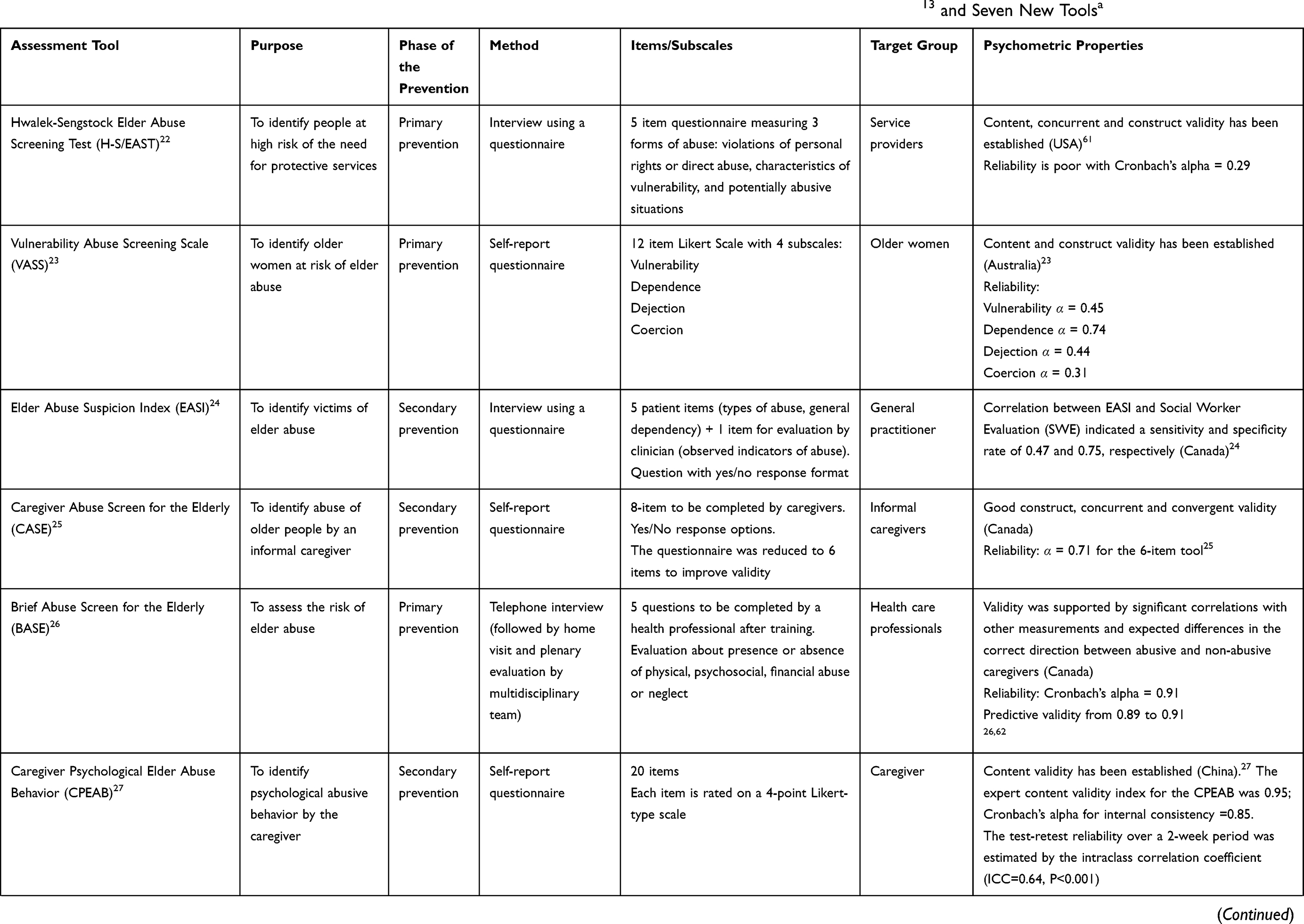 |  | 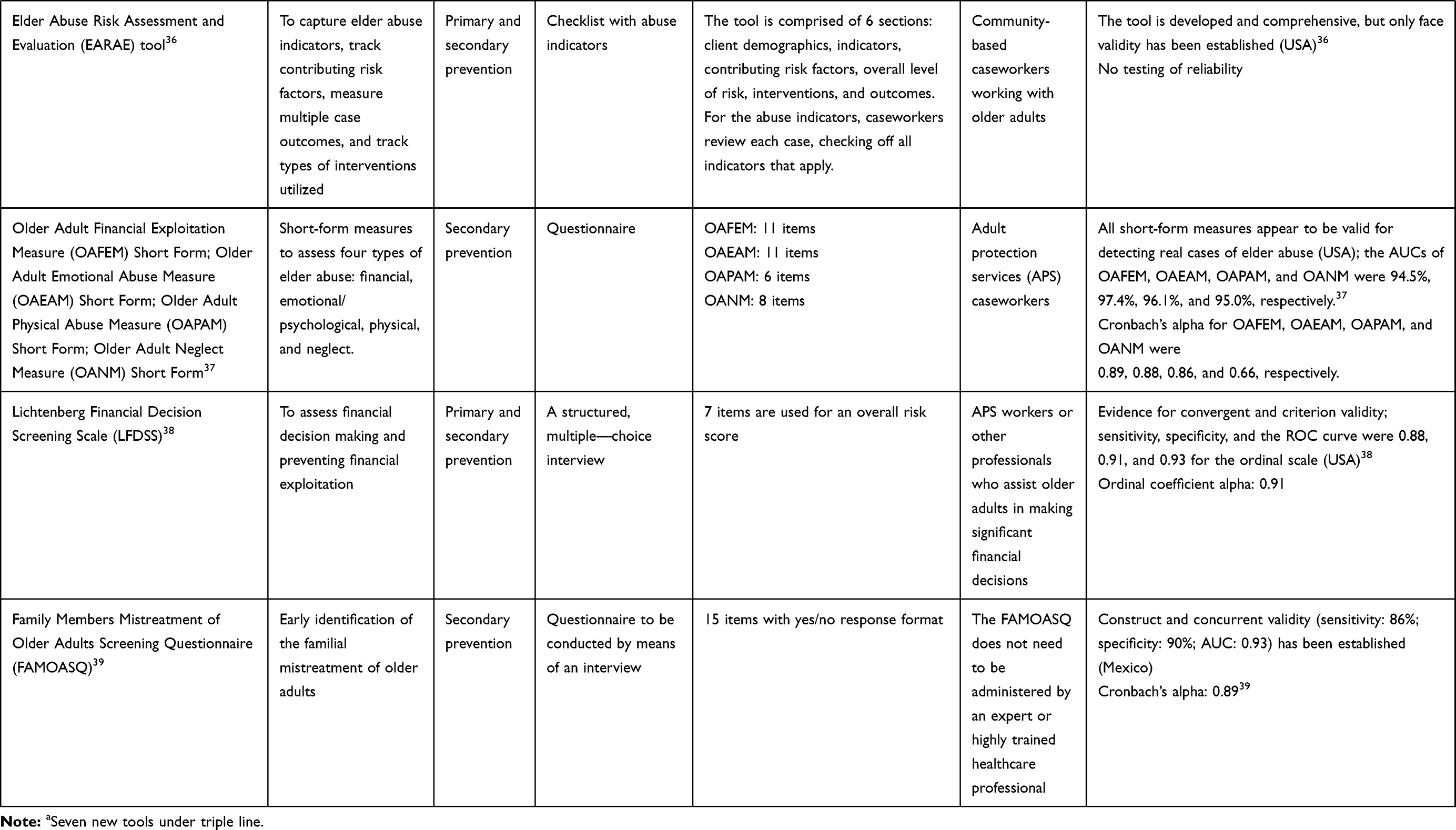 |
Table 1 Assessment Tools for Elder Abuse, Including Eight Tools Based on Gallione, Dal Molin, Cristina, Ferns, Mattioli, Suardi13 and Seven New Toolsa |
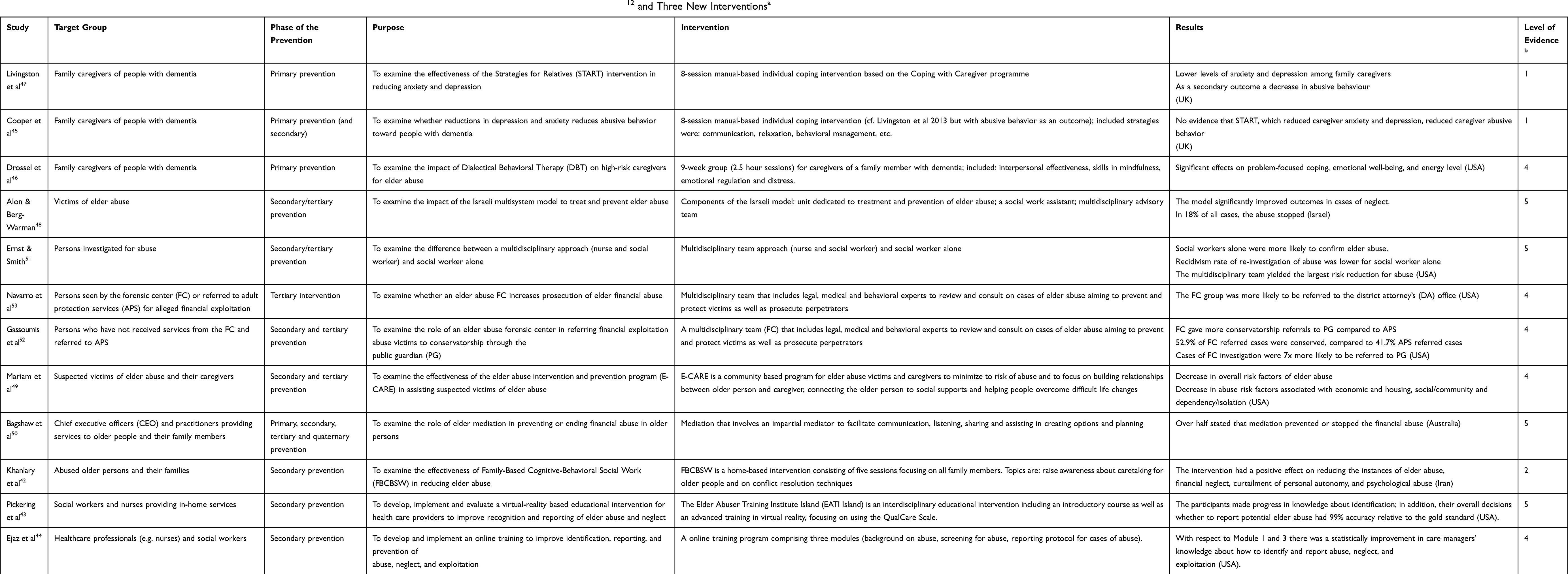 |
Table 2 Community-Based Interventions for Elder Abuse, Including Nine Interventions Based on Fearing, Sheppard, McDonald, Beaulieu, Hitzig12 and Three New Interventionsa |
Results
Assessment Tools
Gallione et al13 found eleven assessment tools for elder abuse in their systematic review. Of these, eight tools were eligible for inclusion in our scoping review: Hwalek-Sengstock Elder Abuse Screening Test (H-S/EAST),22 Vulnerability Abuse Screening Scale (VASS),23 Elder Abuse Suspicion Index (EASI),24 Caregiver Abuse Screen for the Elderly (CASE),25 Brief Abuse Screen for the Elderly (BASE),26 Caregiver Psychological Elder Abuse Behavior (CPEABS),27 Older Adult Abuse Psychological Measure (OAPAM)28 and Older Adult Financial Exploitation Measure (OAFEM).29 The three tools we have excluded are: Elderly Indicators of Abuse (E-IOA),30 Elder Abuse Instrument (EAI)31 and Elder Psychological Abuse Scale (EPAS).32 All three tools have not been validated in a sample of community-dwelling older people. The E-IOA, EAI and the EPAS were validated in patients admitted to a hospital, an emergency department and in long-term care (nursing home), respectively.
Seven new instruments have been published since June 2015: Risk on Elder Abuse and Mistreatment Instrument (REAMI),33 Assessment Tool for Domestic Elder Abuse (ATDEA),34 QualCare Scale,35 Elder Abuse Risk Assessment and Evaluation (EARAE) tool,36 short-form measures of four types of elder abuse (financial, emotional/psychological, physical, neglect),37 the Lichtenberg Financial Decision Screening Scale (LFDSS),38 and the Family Members Mistreatment of Older Adults Screening Questionnaire (FAMOASQ).39
The REAMI, a questionnaire that contains 22 items, was developed and tested using a mixed method design. In total, 1920 older clients of home care were assessed by their Flemish home care professionals with the REAMI. In addition, 24 of these professionals were interviewed about experiences using this assessment tool. The findings demonstrated good internal reliability and internal validity for the REAMI.33
The ATDEA is recently developed in Japan; it is a checklist containing 34 items covering all types of elder abuse that can be used by healthcare professionals, in particular nurses, to detect and prevent elder abuse. Findings of face and content validity testing established the validity of the ATDEA.34
The QualCare Scale is a direct observational scale that was originally developed as a measure of the quality of caregiving provided by family caregivers40 including the dimensions of physical care, psychological care, medical care maintenance, environmental care, human rights violations and financial care. Pickering et al35 decided to use the QualCare Scale for assessing elder abuse among older persons receiving home care. The EARAE tool was developed for community-based caseworkers working with older adults. The tool is used to capture information from elder abuse cases in order to determine changes in the level of risk for primary and secondary types of abuse and abuse outcomes to identify and determine changes in contributing risk factors, and track interventions and outcomes.36 The instrument is comprehensive, especially within the domains of indicators and contributing risk factors for most forms of elder mistreatment, minus self-neglect. However, the tool needs to be validated.
The short-form measures for assessing financial, emotional/psychological, and physical abuse and neglect were developed using data from the Elder Abuse Decision Support System (EADSS). The validity of the four short-form measures was similar to the original long-form measures.37
The LFDSS was introduced in 2016 aiming to prevent financial exploitation.38 This scale is taken orally; because it is a rating scale the interviewer’s judgment is critical.38 However, the LFDSS can be easily taught to professionals of the Adult protection services (APS).38
Finally, the FAMOASQ is also a questionnaire that is answered orally. This instrument is culturally and socially tailored to Mexican older adults.39 It contains eight questions referring to psychological/emotional abuse; nine questions addressed neglect/abandonment and two questions each addressed physical, economic and sexual abuse.
Table 1 presents an overview of the characteristics of the fifteen assessment tools for elder abuse included in our scoping review. Four of the included tools are aiming to identify older people at risk for elder abuse (primary prevention); seven tools aim at secondary prevention, the purpose of which is to early detect elder abuse. Four assessment tools; the ATDEA,34 QualCare Scale,35,40 the EARAE tool36 and the LFDSS38 can be used for both primary and secondary prevention. Moreover, the substantive focus of the tools is different. Ten tools have a wide scope on elder abuse, while CPEABS27 and OAPAM28 focus exclusively on identifying psychological abusive behavior by the caregiver and psychological abuse of an older person. The OAFEM29 and the LFDSS38 only consider the identification of financial abuse.
The data collection differs between the assessment tools. Six out of fifteen tools are questionnaires or a checklist. For six tools, the data will be collected by means of an interview, e.g. BASE26 includes a telephone interview. As described above, the QualCare Scale35,40 is a tool that can be used to collect data by means of observations. The target group also differs according to the tool. For example, the VASS23 has been used and validated among older women. The OAPAM28 also targets older people themselves. In particular, the BASE,26 ATDEA34 and REAMI33 indicate that the tool can be used by a diversity of healthcare professionals. The last column of Table 1 briefly describes the validity of the instrument in question. Seven assessment tools are validated in the USA (H-S/EAST, OAPAM, OAFEM, QualCare Scale, the short-form measures, EARAE, LFDSS) and three in Canada (EASI, CASE, BASE).
Interventions
The systematic review on community-based interventions for elder abuse conducted by Fearing et al12 covers the period from 2009 to 2015; this study continued where the systematic review by Ploeg et al20 ended. Fearing et al12 found nine studies eligible for inclusion. All these studies are presented in Table 2. In the last column, the level of evidence is described for each intervention. The levels of evidence are based on the Modified Sackett Scale.41 Our literature search yielded three new studies that met our inclusion criteria.42–44 The first of these studies was conducted by Khanlary et al.42 This research group carried out a randomized clinical trial with the aim to determine the effectiveness of Family-Based Cognitive Behavioral Social Work (FBCBSW) in reducing older persons’ abuse. This intervention resulted in a significant reduction of emotional neglect, financial neglect, care neglect, curtailment of personal autonomy, financial abuse, and psychological abuse. The second study we added was conducted by Pickering et al.43 They developed, implemented and evaluated the Elder Abuser Training Institute Island (EATI Island), a virtual-reality-based older persons’ abuse educational intervention for social workers and nurses. Finally, we included the study by Ejaz et al44 in our review. The authors44 developed and implemented three online modules focusing on background on abuse, screening for abuse, and reporting protocol for cases of abuse, respectively. Statistically significant improvements in knowledge from pre- to post-training were evident for the participants (healthcare professionals, social workers) in all parts of Module 1 and most parts of Module 3. With respect to Module 3 (screening for abuse), none of the responses on the questions asked showed an improvement in their knowledge.
Five target groups can be distinguished: family caregivers of people with dementia,45–47 victims of elder abuse,48 victims of elder abuse and their caregivers,49 victims of elder abuse and all their family members42 and professionals, whether or not attached to a center (e.g. a forensic center).43,44,50–53
Table 2 also briefly presents the interventions. In the studies by Cooper et al 45 and Livingston et al,47 an individual coping intervention focused on family caregivers of people with dementia has been carried out, including strategies such as behavioral management and relaxation. Drossel et al46 offered a similar intervention for the same target group. Several studies emphasize that the intervention should be carried out in a multidisciplinary team;51–53 in the Israeli multisystem model aiming to treat and prevent older persons’ abuse a multidisciplinary advisory team was involved.48
All twelve studies examined the impact of the intervention; the outcome measures were all different. For example, a lower level of depression by family caregivers of people with dementia,47 stopping the abuse48,50 or progress in knowledge of nurses and social worker about the identification of older persons’ abuse43 and knowledge of background on abuse and reporting abuse.44
Collected data were evaluated in terms of changes in knowledge, changes in practice and user satisfaction. All included studies present positive results (see Table 2). However, as Fearing et al12 described, the level of evidence of most studies is low. Only two studies have Level-1 evidence (the highest level)45,47 and one study has Level-2 evidence42 according to the Modified Sackett Scale;41 the other studies have evidence of Level-4 or Level-5. The intervention studies demonstrate a lack of validated outcome measures to systematically detect change over time. Finally, it should be noted that seven of the twelve intervention studies were carried out in the USA.
As a final note, interventions are focused on primary, secondary or tertiary interventions; however, very few studies addressed quaternary intervention. Only one study50 examined an intervention, the role of elder mediation in preventing or ending financial abuse in older persons, focusing on primary, secondary, tertiary as well as quaternary prevention. In their study the researchers included also the views of older people in order to develop, pilot, and evaluate a model of older-person-centered mediation to prevent the financial abuse of older people by family members.50 Hardly any study included in this review emphasizes the effects for older persons or victims when preventing or responding to elder abuse.
Discussion
In this scoping review, we provide an overview of assessment tools and interventions for elder abuse to be used by professionals and informal caregivers in the home environment. We identified the suitable assessment tools and interventions for use in the home environment included in the two previous systematic reviews; the study by Gallione et al13 focusing on assessment tools and the study by Fearing et al12 concerning interventions. In addition, we have updated the existing evidence with a new systematic literature search and focused specifically on assessment tools and interventions that can be used in the home environment. Also, we categorized all tools and interventions, according to a public health perspective, into primary, secondary, tertiary and quaternary prevention.
Need for More Rigorous Validation of Assessment Tools
Fifteen assessment tools met our inclusion criteria of which four were not included in the systematic review by Gallione et al:13 QualCare Scale,35 REAMI,33 ATDEA34 and EARAE tool.36 Seven and three of the available tools have been developed and tested in the USA and Canada, respectively. Only one tool has been developed and validated in a European country (Belgium), the REAMI.33 Exploration of the REAMI aimed at further validation including assessment by other care stakeholders (e.g. social workers) seems necessary.33 There is a need for a more rigorous validation of assessment tools, within different cultural contexts and specifically for caregivers in the home environment. In line with the review by Gallione et al,13 we conclude there is still no gold standard for assessment of elder abuse. A “gold standard” or reference standard is necessary to allow for comparison of other assessment tools against this standard in order to establish the validity of elder abuse screening tools. However, a gold standard that would definitively assess the presence or absence of elder abuse is difficult to determine due to the various legal definitions, a variety of clinical experiences and situations, signs of abuse having great overlap with markers of disease and other standards in different regions. More validity testing of the current assessment tools is needed – but when assessing elder abuse, a tool should not be used alone but rather combined with other data, longitudinal observation and review by experts in the field.
Given that cases of elder abuse are often left undetected, it is important for health care providers and social workers providing at-home care services, to equip them with validated tools to detect elder abuse as they are ideally placed to recognize a situation of abuse. In a study collecting the views of health professionals, none of the validated assessment tools were deemed suitable for use in their practice.17 This was due to outdated terminology, asking binary questions, asking multiple questions at once, failure to consider the older person’s cognitive status, failure to consider how culture mediates elder abuse, and failure to outline a referral pathway to those administering the tool. The health professionals recommended for a screening tool to promote trust and rapport between the assessor and the older person in order to solicit a story on this sensitive subject.17 Therefore, the authors recommend that a successful assessment instrument for elder abuse must be concise, easy to use, consider frailty of older people, and give direction to a pathway if there is a suspicion of elder abuse.17 A safe and calm environment together with formulating the questions in narrative and qualitative format could help the assessors to build trust and rapport.
Professionals are also insufficiently trained in detecting abuse, due to a lack of understanding and education into the signs and risk factors for older persons’ abuse, as well as a lack of identification skills and reporting procedures.13 Also, the level of perception and knowledge of elder abuse by healthcare workers are still poor; thus, there is still a strong need for education and specific training program.54
Besides allowing for detection of elder abuse, assessment tools should include a clear referral pathways on what to do when potential abuse is found—when to report, who to contact, and how to involve the older person in the referral process. A clear referral pathway has been previously identified as an important requirement for future developed assessment tools.17
The included assessment tools also lack adaptation to risk groups. Given that cognitive impairment and dementia symptoms constitute one of the most relevant risk factors for elder abuse, a disease-sensitive assessment tool specifically to elder abuse in persons with dementia is required to capture the specific characteristics of abuse involving older persons with different stages of dementia.55 Fang et al55 recommend in their review that detection and interventions of elder abuse take into account the stages of the disease. Furthermore, healthcare professionals should be educated on the nature and prognosis of dementia and when providing care at home be alert of the potential risk related to symptoms associated with different stages of dementia.55
Lack of Validated Interventions
Despite the serious impact on older persons and on society, there also remains a significant lack of validated community-based interventions for elder abuse. In total, we identified twelve intervention studies that met our inclusion criteria of which nine were identified previously by Fearing et al.12 Our additional literature search yielded three other interventions.42–44
Several systematic reviews report many difficulties in responding to elder abuse, which is due to a lack of evidence regarding the most effective ways to address elder abuse.11,12,19
In particular, the elder abuse intervention research field is constrained by a deficiency in validated and meaningful intervention outcome measures capable of systematically detecting the extent of case resolution over time.56 Burnes et al56 propose a severity framework as a guideline for outcome measurement and recommends qualitative research with professionals who work in the field and with victims of elder abuse themselves, to develop an outcome measure and understand how to conceptualize and operationalize the outcome construct of elder abuse severity.
In addition, given the complex nature of elder abuse and multidimensional needs and problems of victims, the use of a multidisciplinary team (MDT) approach is the recommended golden standard for interventions.57,58 As Blowers et al state:
Detecting and preventing elder mistreatment requires the involvement of professionals and community partners from many disciplines. It is a community problem, a legal issue, a social concern, and a medical matter.57
The responses required for elder abuse must come from different sectors, including criminal justice, health care, mental health care, victim services, civil legal services, adult protective services, financial services, long-term care, and proxy decision making.59 However, hardly any research has been done in this area. “As one of the field’s most promising practices, MDTs should be implemented and tested internationally”, according to Pillemer et al.59 As a result, there is a lack of coordinated care and a fragmentation of knowledge among health care, welfare and legal professionals. For instance, health care providers experience many barriers to collaborate with the professionals within the judicial field because of confidentiality issues.60 Healthcare providers, social workers and legal professionals hold complementary knowledge and skills in the context of elder abuse; however, they often address the abuse independently and without consultation, which creates barriers and inefficiencies. MDT intervention strategies should be tested to be applied in different societies, in the context of available resources and taking into account the different cultural manifestations of elder abuse.59 This would ideally result into multidisciplinary collaboration protocols to enhance coordination and reduce fragmentation.
Quaternary Prevention
Important to note is the deficiency of attention for quaternary prevention or preventing the adverse effects of assessment and interventions in current and within this review included elder abuse assessment tools or interventions.15 These side-effects may include, for example, inappropriate risk assessment, a breach of confidentiality, invasion of privacy, damaging the relationship between victim and abuser, and failure in safety plan.16,11 In future research projects aiming to prevent and intervene on elder abuse, older people and also their family caregivers should participate from the beginning to the end in the development of an intervention protocol.
Limitations
The search strategy applied for this review is not without limitations. First, no further efforts were made to retrieve unpublished studies such as contacting authors or searching in grey literature.
Moreover, EMBASE and Scopus databases were not accessed due to unavailability at our institution. However, four main databases, Medline, CINAHL, Web of Science and Cochrane Databases, were consulted applying a broad search strategy, as such, we feel that this review provides a comprehensive overview of assessment and intervention tools for elder abuse by caregivers in the home environment. Furthermore, a limitation for languages potentially may have excluded relevant papers in other languages. Finally, apart from the limitations of our own search strategy, it is important to note that we might have carried the limitations of the review studies we used as a starting point into this scoping review.
Conclusion
Given the significant number of older people staying at home and being dependent on formal and informal care or assistance, care providers in the home environment have an important role for detecting and responding to abuse. Both assessment tools and existing interventions for elder abuse need further testing in the setting of the home environment and over different cultural contexts and with risk groups. There is a need for intervention outcome measures to assess the extent of case resolution. Furthermore, more research is needed, in particular interdisciplinary research, in order to advance the knowledge for facilitating multidisciplinary team approaches.
Important is also that interventions need to address potential side-effects when responding to elder abuse (or quaternary prevention). In future studies, when developing an intervention protocol, the perspectives of (abused) older people and their environment should be accounted for.
Disclosure
Liesbeth De Donder reports the following as it might give an appearance of potential influence: the paper/literature review has found fifteen assessment tools that met our inclusion criteria of which four were not included in the systematic review by Gallione et al. These four instruments are discussed and one of these four is the Risk on Elder Abuse and Mistreatment Instrument (REAMI) of which I am the developer/first author of the validation paper (De Donder et al, 2018). The authors report no other potential conflicts of interest in this work.
References
1. United Nations. World population prospects: the 2017 revision, key findings and advance tables. Working Paper No. ESA/P/WP/248; 2017.
2. Cutchin M. The process of mediated aging-in-place: a theoretically and empirically based model. Soc Sci Med. 2003;57(6):1077–1090. doi:10.1016/S0277-9536(02)00486-0
3. Anker-Hansen C, Skovdahl K, McCormack B, Tønnessen S. The third person in the room: the needs of care partners of older people in home care services—a systematic review from a person-centred perspective. J Clin Nurs. 2018;27(7–8):e1309–e1326. doi:10.1111/jocn.14205
4. Genet N, Boerma W, Kroneman M, Hutchinson A, Saltman RB. Home Care Across Europe Current Structure and Future Challenges. Kopenhagen: WHO; 2012.
5. Yon Y, Mikton CR, Gassoumis ZD, Wilber KH. Elder abuse prevalence in community settings: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(2):e147–e156. doi:10.1016/S2214-109X(17)30006-2
6. De Donder L, Luoma ML, Penhale B, et al. European map of prevalence rates of elder abuse and its impact for future research. Eur J Ageing. 2011;8(2):129. doi:10.1007/s10433-011-0187-3
7. WHO. The Toronto Declaration on the Global Prevention of Elder Abuse. Geneva: World Health Organization; 2002.
8. Dong X, Chen R, Chang ES, Simon M. Elder abuse and psychological well-being: a systematic review and implications for research and policy–a mini review. Gerontology. 2013;59(2):132–142. doi:10.1159/000341652
9. Dong X, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013;173(10):911–917. doi:10.1001/jamainternmed.2013.238
10. Yunus RM, Hairi NN, Choo WY. Consequences of elder abuse and neglect: a systematic review of observational studies. Trauma Violence Abuse. 2019;20(2):197–213. doi:10.1177/1524838017692798
11. Baker PR, Francis DP, Mohd Hairi NN, Othman S, Choo WY. Interventions for preventing elder abuse in the elderly. Cochrane Database of Systematic Reviews. 2016;(8). Art. No: CD010321. doi:10.1002/14651858.CD010321.pub2
12. Fearing G, Sheppard CL, McDonald L, Beaulieu M, Hitzig SL. A systematic review on community-based interventions for elder abuse and neglect. J Elder Abuse Negl. 2017;29(2–3):102–133. doi:10.1080/08946566.2017.1308286
13. Gallione C, Dal Molin A, Cristina FVB, Ferns H, Mattioli M, Suardi B. Screening tools for identification of elder abuse: a systematic review. J Clin Nurs. 2017;26(15–16):2154–2176. doi:10.1111/jocn.13721
14. Twomey M. Elder Abuse. Center of Excellence on Elder Abuse and Neglect, Division of Geriatric Medicine and Gerontology, University of California, Irvine. 2014. https://www.giaging.org/issues/elder-abuse/
15. Martins C, Godycki-Cwirko M, Heleno B, Brodersen J. Quaternary prevention: reviewing the concept. Eur J Gen Pract. 2018;24(1):106–111. doi:10.1080/13814788.2017.1422177
16. Dugan L, Nagin DS, Rosenfeld R. Do domestic violence services save lives? Natl Inst Justice J. 2003;250:20–25.
17. Brijnath B, Gahan L, Gaffy E, Dow B. Build rapport, otherwise no screening tools in the world are going to help: frontline service providers’ views on current screening tools for elder abuse. Gerontologist. 2018.
18. Sooryanarayana R, Choo WY, Hairi NN. A review on the prevalence and measurement of elder abuse in the community. Trauma Violence Abuse. 2013;14(4):316–325.
19. Ayalon L, Lev S, Green O, Nevo U. A systematic review and meta-analysis of interventions designed to prevent or stop elder maltreatment. Age Ageing. 2016;45(2):216–227. doi:10.1093/ageing/afv193
20. Ploeg J, Fear J, Hutchison B, MacMillan H, Bolan G. A systematic review of interventions for elder abuse. J Elder Abuse Negl. 2009;21(3):187–210. doi:10.1080/08946560902997181
21. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
22. Sengstock M, Hwalek M. A review and analysis of measures for the identifications of elder abuse. J Gerontol Soc Work. 1987;10(3–4):21–36. doi:10.1300/J083V10N03_03
23. Schofield MJ, Mishra GD. Validity of self-report screening scale for elder abuse: women’s Health Australia Study. Gerontologist. 2003;43(1):110–120. doi:10.1093/geront/43.1.110
24. Yaffe MJ, Wolfson C, Lithwick M, Weiss D. Development and validation of a tool to improve physician identification of elder abuse: the Elder Abuse Suspicion Index (EASI). J Elder Abuse Negl. 2008;20(3):276–300. doi:10.1080/08946560801973168
25. Reis M, Nahmiash D. Validation of the Caregiver Abuse Screen (CASE). Can J Aging. 1995;14(Suppl 2):45–60. doi:10.1017/S0714980800005584
26. Reis M, Nahmiash D. When seniors are abused: an intervention model. Gerontologist. 1995;35(5):666–671. doi:10.1093/geront/35.5.666
27. Wang JJ, Lin JN, Lee FP. Psychologically abusive behavior by those caring for the elderly in a domestic context. Geriatr Nurs. 2006;27(5):
28. Conrad KJ, Iris M, Ridings JW, Langley K, Anetzberger GJ. Self-report measure of psychological abuse of older adults. Gerontologist. 2011;51(3):354–366. doi:10.1093/geront/gnq103
29. Conrad KJ, Iris M, Ridings JW, Langley K, Wilber KH. Self-report measure of financial exploitation of older adults. Gerontologist. 2010;50(6):758–773. doi:10.1093/geront/gnq054
30. Cohen M, Halevi-Levin S, Gagin R, Friedman G. Development of a screening tool for identifying elderly people at risk of abuse by their caregivers. J Aging Health. 2006;18(5):660–685. doi:10.1177/0898264306293257
31. Fulmer T, Street S, Carr K. Abuse of the elderly: screening and detection. J Emerg Nurs. 1984;10(3):131–140.
32. Wang -J-J, Tseng H-F, Chen K-M. Development and testing of screening indicators for psychological abuse of older people. Arch Psychiatr Nurs. 2007;21(1):40–47. doi:10.1016/j.apnu.2006.09.004
33. De Donder L, De Witte N, Van Regenmortel S, Dury S, Dierckx E, Verté D. Risk on elder abuse and mistreatment – instrument: development, psychometric properties and qualitative user evaluation. Educ Gerontol. 2018;44(2–3):108–118. doi:10.1080/03601277.2017.1417810
34. Yi Q, Honda J, Hohashi N. Development and validity testing of an assessment tool for domestic elder abuse. J Nurs Res. 2019;27(2):e12. doi:10.1097/jnr.0000000000000278
35. Pickering CEZ, Ridenour K, Salaysay Z, Reyes-Gastelum D, Pierce SJ. Identifying elder abuse & neglect among family caregiving dyads: a cross sectional study of psychometric properties of the QualCare scale. Int J Nurs Stud. 2017;69:41–46. doi:10.1016/j.ijnurstu.2017.01.012
36. Dauenhauer J, Heffernan K, Caccamise PL, et al. Preliminary outcomes from a community-based elder abuse risk and evaluation tool. J Appl Gerontol. 2017;733464817733105.
37. Beach SR, Liu PJ, DeLiema M, Iris M, Howe MJK, Conrad KJ. Development of short-form measures to assess four types of elder mistreatment: findings from an evidence-based study of APS elder abuse substantiation decisions. J Elder Abuse Negl. 2017;29(4):229–253. doi:10.1080/08946566.2017.1338171
38. Lichtenberg PA, Teresi JA, Ocepek-Welikson K, Eimicke JP. Reliability and validity of the Lichtenberg financial decision screening scale. Innov Aging. 2017;1(1). doi:10.1093/geroni/igx003
39. Ruelas-Gonzalez MG, Pelcastre-Villafuerte BE, Monterrubio-Flores E, et al. Development and validation of a screening questionnaire of family mistreatment against older adults for use in primary care settings in Mexico. Health Soc Care Community. 2018;26(1):102–112. doi:10.1111/hsc.12466
40. Phillips LR, Morrison EF, Chae YM. The QUALCARE scale: developing an instrument to measure quality of home care. Int J Nurs Stud. 1990;27(1):61–75. doi:10.1016/0020-7489(90)90024-D
41. Straus SE, Richardson W, Galasziou P, Haynes R. Evidence-Based Medicine: How to Practice and Teach EBM.
42. Khanlary Z, Maarefvand M, Biglarian A, Heravi-Karimooi M. The effect of a family-based intervention with a cognitive-behavioral approach on elder abuse. J Elder Abuse Negl. 2016;28(2):114–126. doi:10.1080/08946566.2016.1141738
43. Pickering CEZ, Ridenour K, Salaysay Z, Reyes-Gastelum D, Pierce SJ. EATI Island – a virtual-reality-based elder abuse and neglect educational intervention. Gerontol Geriatr Educ. 2018;39(4):445–463. doi:10.1080/02701960.2016.1203310
44. Ejaz FKPL-S, Rose MM, Anetzberger GPAL. Development and implementation of online training modules on abuse, neglect, and exploitation. J Elder Abuse Negl. 2017;29(2–3):73–101. doi:10.1080/08946566.2017.1307153
45. Cooper C, Barber J, Griffin M, Rapaport P, Livingston G. Effectiveness of START psychological intervention in reducing abuse by dementia family carers: randomized controlled trial. Int Psychogeriatr. 2016;28(6):881–887. doi:10.1017/S1041610215002033
46. Drossel C, Fisher JE, Mercer V. A DBT skills training group for family caregivers of persons with dementia. Behav Ther. 2011;42(1):109–119. doi:10.1016/j.beth.2010.06.001
47. Livingston G, Barber J, Rapaport P, et al. Clinical effectiveness of a manual based coping strategy programme (START, STrAtegies for RelaTives) in promoting the mental health of carers of family members with dementia: pragmatic randomised controlled trial. BMJ. 2013;347:f6276.
48. Alon S, Berg-Warman A. Treatment and prevention of elder abuse and neglect: where knowledge and practice meet – a model for intervention to prevent and treat elder abuse in Israel. J Elder Abuse Negl. 2014;26(2):150–171. doi:10.1080/08946566.2013.784087
49. Mariam LM, McClure R, Robinson JB, Yang JA. Eliciting change in at-risk elders (ECARE): evaluation of an elder abuse intervention program. J Elder Abuse Negl. 2015;27(1):19–33. doi:10.1080/08946566.2013.867241
50. Bagshaw D, Adams V, Zannettino L, Wendt S. Elder mediation and the financial abuse of older people by a family member. Conflict Resolut Q. 2015;32(4):443–480. doi:10.1002/crq.21117
51. Ernst JS, Smith CA. Assessment in adult protective services: do multidisciplinary teams make a difference? J Gerontol Soc Work. 2012;55(1):21–38. doi:10.1080/01634372.2011.626842
52. Gassoumis ZD, Navarro AE, Wilber KH. Protecting victims of elder financial exploitation: the role of an elder abuse forensic center in referring victims for conservatorship. Aging Ment Health. 2015;19(9):790–798. doi:10.1080/13607863.2014.962011
53. Navarro AE, Gassoumis ZD, Wilber KH. Holding abusers accountable: an elder abuse forensic center increases criminal prosecution of financial exploitation. Gerontologist. 2013;53(2):303–312. doi:10.1093/geront/gns075
54. Corbi G, Grattagliano I, Sabba C, et al. Elder abuse: perception and knowledge of the phenomenon by healthcare workers from two Italian hospitals. Intern Emerg Med. 2019;14(4):549–555. doi:10.1007/s11739-019-02038-y
55. Fang B, Yan E. Abuse of older persons with dementia: a review of the literature. Trauma Violence Abuse. 2018;19(2):127–147. doi:10.1177/1524838016650185
56. Burnes D, Lachs MS, Pillemer K. Addressing the measurement challenge in elder abuse interventions: need for a severity framework. J Elder Abuse Negl. 2018;30(5):402–407. doi:10.1080/08946566.2018.1510354
57. Blowers A, Davis B, Shenk D, Kalaw KJ, Smith M, Jackson K. A multidisciplinary approach to detecting and responding to elder mistreatment: creating a University-community partnership. Am J Crim Justice. 2012;37:276–290. doi:10.1007/s12103-012-9156-4
58. Twomey MS, Jackson G, Li H, et al. The successes and challenges of seven multidisciplinary teams. J Elder Abuse Negl. 2010;22(3–4):291–305. doi:10.1080/08946566.2010.490144
59. Pillemer K, Burnes D, Riffin C, Lachs MS. Elder abuse: global situation, risk factors, and prevention strategies. Gerontologist. 2016;56(Suppl 2):S194–S205. doi:10.1093/geront/gnw004
60. Saghafi A, Bahramnezhad F, Poormollamirza A, Dadgari A, Navab E. Examining the ethical challenges in managing elder abuse: a systematic review. J Med Ethics Hist Med. 2019;12:7.
61. Neale AV, Hwalek MA, Scott RO, Sengstock MC, Stahl C. Validation of the Hwalek-Sengstock elder abuse screening test. J Appl Gerontol. 1991;10(4):406–415. doi:10.1177/073346489101000403
62. Reis M, Nahmiash D. Validation of the indicators of abuse (IOA) screen. Gerontologist. 1998;38(4):471–480. doi:10.1093/geront/38.4.471
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.