Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
Efficient Method for Rapid Diagnosis of Streptococcal Pneumoniae in the Context of Co-Infection in Children-Case Report
Authors Stavar-Matei L ![]() , Mihailov OM, Crestez AM, Alexandru AM, Popescu CM, Nechita A
, Mihailov OM, Crestez AM, Alexandru AM, Popescu CM, Nechita A
Received 15 May 2024
Accepted for publication 27 July 2024
Published 13 August 2024 Volume 2024:15 Pages 273—278
DOI https://doi.org/10.2147/PHMT.S467351
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Laurens Holmes, Jr
Loredana Stavar-Matei,1,2 Oana-Mariana Mihailov,1 Alexandra-Mihaela Crestez,1,2 Anamaria Madalina Alexandru,1 Cristina-Mihaela Popescu,1,2 Aurel Nechita1,2
1Dunarea de Jos” University of Galati, Faculty of Medicine and Pharmacy, Galati,Romania; 2Sf. Ioan“ Children’s Clinical Emergency Hospital, Galati, Romania
Correspondence: Loredana Stavar-Matei, Email [email protected]
Background: Bacterial pneumonia caused by Streptococcus pneumoniae continues to be one of the most common medical conditions in the pediatric population under 5 years of age, sometimes requiring prolonged hospitalizations and high costs. The time period (3 to 7 days) from the collection of biological samples (ie nasal exudate, pharyngeal exudate, sputum, blood culture and various secretions) to the arrival of the results has been a much discussed issue. Thus, the use of a rapid diagnostic test for Streptococcus pneumoniae urinary antigen, which is easy to use, may lead after the result is known to a targeted therapeutic management and thus to a favorable prognosis of the disease for the patient.
Methods: This case report presents the case of a 4 years and 5 months old patient diagnosed with invasive pneumococcal-associated pneumococcal infection in the context of SARS-COV2 infection.
Results: The clinical course was slowly favorable with complications that required a long hospitalization.
Conclusion: In conclusion, some rapid diagnostic techniques, clinician judgment and some prevention methods, such as vaccination, can improve a patient’s quality of life. One prospect for the future would be the development of new vaccines covering other aggressive Streptococcus pneumoniae serotypes.
Keywords: co-infections, pneumococcal urinary antigen test, therapeutic management, vaccination
Introduction
Streptococcus pneumoniae is a human-specific pathogen that normally colonizes the rhinopharynx. It is primarily responsible for invasive infections, namely community-acquired pneumonia, acute otitis, bacteremia, and meningitis among the pediatric population in combination with certain risk factors. There are certain prone categories that have an increased risk of developing invasive pneumococcal disease: small age, artificial food in the first year of life, immunosuppressed patients, low birth weight, low vaccination rate, and social group.1 The determination of the Urinary Antigen of Streptococcus pneumoniae and Legionella pneumophila may be a diagnostic test for this entity, as it is accessible, non-invasive, and rapid, generating a result that may influence the therapeutic decision in favor of the patient.2,3
Adopting the pneumococcal conjugated vaccine (PCV) in national programs for immunization was an effective measure in terms of the incidence of invasive infections in children and in terms of hospitalization costs. This project should continue in low- and middle-income countries too, where access is still limited.4,5 The increased mortality and morbidity rate continues to be high in the least developed countries: India, Nigeria, Pakistan and the Democratic Republic of Congo.6
Case Presentation
To analyze the importance of the immunochromatographic urinary test for the detection of Streptococcus pneumonia antigen, we shall present the case of a patient aged 4 years and 5 months, living in the city, hospitalized in the “Sf. Ioan” Emergency Clinical Hospital for children in Galati for respiratory symptoms – fever, productive cough, and chest pain that started a week before coming to the hospital. She received at-home antibiotic treatment with macrolides and symptomatic treatment without relief of the symptoms. The patient did not have a significant pathological history, no previous hospitalization, and she had the complete immunization schedule under the National Program. It is worth mentioning that the National Immunization Schedule did not include at that time the pneumococcal vaccine, which had been recently introduced and applicable at the level of our country since August 2017.
The clinical examination revealed that the patient came in with a mediocre health condition, afebrile, pale, facies showing suffering, polyp dyspnea, intercostal and subcostal retraction, prolonged slow expiration, SpO2 = 93% in atmospheric air, pulmonary auscultation – bilateral crackles, tachycardia, digestive balance, no signs of meningeal irritation.
As for the lab tests, we mention an important neutrophilic leukocytosis, marked inflammatory syndrome (including high procalcitonin and interleukin 6 far above the normal values), normocytic normochromic anemia, coagulation disorders, and hepatic cytolysis syndrome. Additionally, due to the present Pandemic Covid-19 situation, the patient was RT-PCR tested for SARS-COV2, and the result was positive. (Table 1)
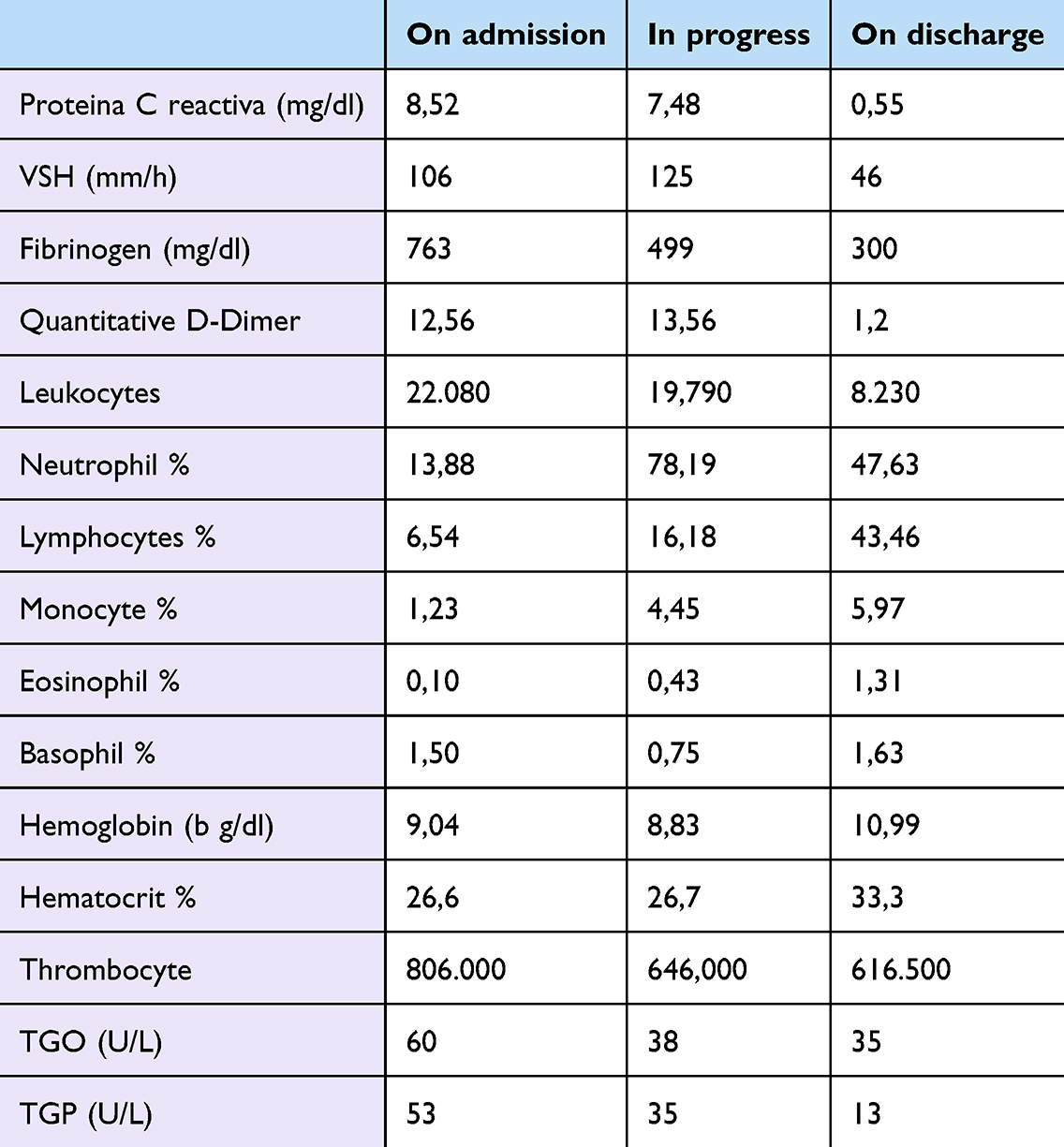 |
Table 1 The Table Highlights the Main Results of Laboratory Tests in the Morning from Hospitalization to Discharge |
Serial chest X-rays were performed to show the progress. The chest X-ray at the time of hospitalization showed a medium opacity, imprecisely delimited, right paracardiac and accentuation of bilateral infrahilar interstice. (Figure 1)
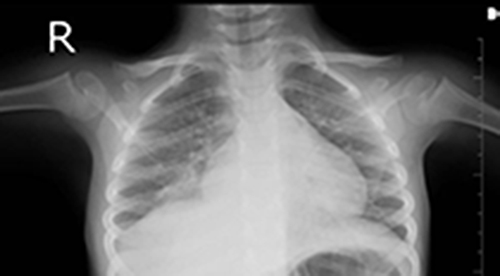 |
Figure 1 Initial X-ray at the time of hospitalization shows right pneumonia. |
Initially, broad-spectrum antibiotic therapy (3rd generation Cephalosporins and aminoglycoside) was applied, corticotherapy, oxygen therapy, bronchodilator, loop diuretic, human immunoglobulin and infusions for hydro-electrolyte and acid-basic rebalancing. The patient’s clinical course remained average in the clinical evolution, with a septic condition, persistence of fever and respiratory symptomatology, and from a paraclinical and imaging point of view with increasing inflammatory syndrome and with a change in the X-ray, with right pleuresy associated. (Figure 2)
 |
Figure 2 Chest X-ray in evolution with right pleurisy. |
Imaging investigations were completed with a native CT (computed tomography) scan and with the non-ionic contrast agents that highlighted pulmonary consolidation in the lower right lobe with pneumatoceles and small rear basal abscesses, pulmonary empyema in small amounts, and a few consolidation opaque areas in the lower left lobe. (Figure 3)
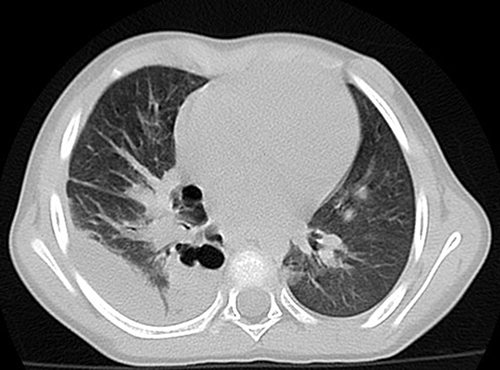 |
Figure 3 CT Chest region- Right lower lobe pneumonia with pneumatocele and small abscesses, pulmonary empyema. |
It was decided to take the Streptococcus pneumonia/Legionella pneumophila antigen test on the urine sample. It showed a positive result for Streptococcus pneumoniae. It is worth mentioning that the test was collected on the 7th day of hospitalization and under the already initiated antibiotic therapy. Among the pathologically significant cultures, we had the following: nasal discharge analysis - Streptococcus pneumoniae present, Laryngeal-tracheal secretion - Streptococcus pneumoniae present with antibiotic sensitivity in Levofloxacin, Linezolid, Vancomycin, Moxifloxacin, and Tetracycline. Another aspect is the resistance of this pneumococcus to the following: Clindamycin, Cotrimoxazole, and all classes of Cephalosporins. A blood culture (aerobic) was collected and the result was negative.
Therefore, it was imperative to change the therapeutic management according to the evolution in the clinical and paraclinical dynamics, but also according to the identified pathogenic agent, namely Streptococcus pneumoniae. The following treatment scheme was established: Linezolid and Vancomycin for 21 days with associated symptomatic and supportive medication. Subsequently, in the dynamics following the initiation of this treatment, the clinical evolution of the patient began to be slowly favorable with the gradual decrease in biological laboratory samples until reaching normal ranges. The X-ray image also showed at the time of discharge an accentuated pulmonary interstitium in the hilar and infrahilar regions predominantly on the right side, and the above-described changes disappeared. As for the co-infection associated with SARS-COV2, the patient has benefited from isolation measures during hospitalization and adequate supportive medication. On discharge, the patient was in good condition, afebrile, with the recommendation not to attend social groups for a period and to return periodically to medical check-ups, to be examined.
Discussions
Streptococcus pneumoniae is a pathogenic agent commonly found in pediatric pathology, still being responsible for 80% of bacterial pneumonia in the US and Europe, especially in small ages.7 Streptococcus pneumoniae is part of the nasopharyngeal commensal microflora, and this is a mandatory condition for the further development of pneumococcal invasive diseases. Nasopharyngeal colonization is usually asymptomatic.8 Ventilation was an effective preventive method against invasive infections determined by Streptococcus pneumoniae. The first pneumococcal vaccine was authorized in the United States in 1977, and the first conjugated pneumococcal vaccine was only authorized in 2000, and in Europe in 2009.9 In Romania, vaccination with the 13-valent pneumococcal conjugated vaccine has been included in the national schedule since August 2017.10,11
Although Streptococcus pneumoniae and coronaviruses cause invasive respiratory tract infections in children, especially during co-infection, the incidence and the dynamics of systemic dissemination are due to the bacterial strain. The mechanisms that lead to bacterial-viral co-pathogenesis are diverse and complex, resulting in abnormal immune responses, thus increasing the adhesion and invasion of bacteria. Due to this viral-bacterial association, there has been an increase in the use of large-scale antibiotics that will increase antimicrobial resistance worldwide. Thus, a method of preventing this situation may be the continuation of the National Pneumococcal Vaccination Program, and not only, but other types of vaccine (flu, coronavirus) may also be included herein, which can substantially reduce the socioeconomic implications of the co-infection. The current information on bacterial infections in COVID-19 patients is still limited, hence identifying and tracking such cases can bring many benefits in terms of diagnostic and therapeutic management.12
In the previously exposed case, the clinician’s decision to determine the Streptococcus pneumoniae antigen from the urine sample until the arrival of the cultures in biological samples was the key to unraveling the case, modifying the entire therapeutic scheme for a final favorable prognosis. It is true that the clinical and paraclinical evolution, by the rise of complications, has been greatly aggravated by certain pre-existing conditions patient-related (unvaccinated) but also by association with other viral infections, in our case SARS-COV2. Thus, a correct and prompt diagnosis can greatly reduce the evolution of the disease and implicitly prevent complications. An essential aspect of medical practice is the determination of common pneumonia etiology both in ambulatory pediatric patients but also in hospitalized patients, by including a non-invasive diagnostic protocol using the detection of Streptococcus Pneumonia and Legionella pneumophila from urine samples when there is clinical suspicion for this pathology. This immunochromatographic technique for qualitative-simultaneous detection of Streptococcus pneumoniae and Legionella pneumophila serogroup 1 in urine samples should be seen as a complementary diagnostic method and not as an alternative to the detriment of other microbiology tests.13–15
There are, however, controversial opinions and studies related to this diagnostic test, which state that its routine implementation in hospitalized patients with common pneumonia would not bring benefits because of its association with the higher risk of clinical recurrence. This fact was highlighted in a prospective study carried out in Spain, and Catalonia by the Department of Internal Medicine in the University Hospital. Thus, the decision to use this test lies with the clinician depending on clinical, paraclinical, and epidemiological elements.16
Identification and research of such invasive pneumococcal cases associated with various co-infections both in terms of classical or modern diagnosis, but also from the point of view of the therapeutic approach plan remains a challenge and a curiosity for the future.
Conclusions
Increased mortality and morbidity due to invasive pneumococcal infections may be closely linked to underlying viral co-infections and also to the need to implement new diagnostic and treatment protocols. Thus, the clinician’s decision to use certain rapid diagnostic tests may lead to the initiation of correct treatment, judicious use of antibiotic therapy and prevention of possible complications of the disease. Thus, all these measures together with pneumococcal vaccination can lead to a decrease of these invasive infections in the pediatric population.
Institutional Review Board Statement
The ethics committee of the “Sf. Ioan” Children’s Emergency Clinical Hospital in Galati approved this study. The subsequent research was carried out under the conditions agreed in this informed consent, which was drawn up in accordance with the current legislation of the World Health Organization and the European Union on research on human subjects in the field of medicine, taking into account the most recent version of the Declaration of Human Rights in Helsinki.
Informed Consent Statement
The patient’s mother provided verbal informed consent for publication of this case report. Written informed consent could not be obtained from the minor patient’s guardian, as his mother was uneducated, could not read or write. All the family members were ethnic and came from rural areas with difficult access to schooling, due to the poor financial situation. She was given extensive details on her understanding of the publication of this case and she agreed. Thus, the informed, attested and documented verbal consent of the patient’s mother for publication of the case details was obtained.
Acknowledgments
All authors have read and agreed to the published version of the manuscript.
Funding
No funding or not able to provide at the moment.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Loughran AJ, Orihuela CJ, Tuomanen EI. Streptococcus pneumoniae: invasion and Inflammation. Microbiol Spectr. 2019;7(2). doi:10.1128/microbiolspec.GPP3-0004-2018
2. Ferrer C, Gutiérrez Rodero F, Rodríguez Díaz JC, Royo García G, Shum Fhunk C, Martín Hidalgo A. Etiology of community-acquired pneumonia in ambulatory patients. Usefulness of a diagnostic investigation protocol using detection of Streptococcus pneumoniae and Legionella pneumophila antigens in urine samples. Med Clin. 2001;117(17):657–659. doi:10.1016/s0025-7753(01)72212-9
3. Evaluarea testului antigen urinar pneumococic (PUT): un studiu retrospectiv - PMC.
4. Chaiyakunapruk N. Cost Effectiveness of Pneumococcal Vaccination in Children in Low- and Middle-Income Countries: a Systematic Review. Pharmacoeconomics. 2016;34(12):1211–1225. doi:10.1007/s40273-016-0439-3
5. Pleşca D. Vaccinarea antipneumococică la copilul cu astm bronşic. Pediatru.ro. 2017;4:1.
6. Wahl B, O’Brien KL, Greenbaum A, et al. Burden of Streptococcus pneumoniae and Haemophilus influenzae type b disease in children in the era of conjugate vaccines: global, regional, and national estimates for 2000–15. Lancet Glob Health. 2018;6(7):e744–e757. doi:10.1016/S2214-109X(18)30247-X
7. SERBENCO L, RUSU G, Bîrca L, Roşca A. Universitatea de Stat de Medicină şi Farmacie Nicolae Testemiţanu. Centrul National Stiintifico-Practic de Medicina Preventiva.2019;1:1.
8. Jullien S, Sharma R, Lhamu Mynak M, Henares D, Muñoz-Almagro C, Bassat Q. Pneumococcal nasopharyngeal carriage among Bhutanese children hospitalized with clinical pneumonia: serotypes and viral co-infection. BMC Infect Dis. 2020;20(1):940. doi:10.1186/s12879-020-05674-4
9. Castagna S. A reflection on invasive pneumococcal disease and pneumococcal conjugate vaccination coverage in children in Southern Europe. Hum Vaccin Immunother. 2017;13(6):1–12. doi:10.1080/21645515.2016.1263409
10. A Brief History of Vaccination. 2024. 1:1.
11. Pneumococcal vaccination coverage. Accessed March. 19. 2024. https://immunizationdata.who.int/pages/coverage/pcv.html.
12. Virus-Induced Changes of the Respiratory Tract Environment Promote Secondary Infections With Streptococcus pneumoniae. Front Cell Infect Microbiol. 2021;11:643326. doi:10.3389/fcimb.2021.643326
13. Domínguez J, Blanco S, Rodrigo C, et al. Usefulness of urinary antigen detection by an immunochromatographic test for diagnosis of pneumococcal pneumonia in children. J Clin Microbiol. 2003;41(5):2161–2163. doi:10.1128/JCM.41.5.2161-2163.2003
14. Garman SF, Liu RL, Levine G, Yang OS, Yang Y-H. Evaluation of Binax NOW, an assay for the detection of pneumococcal antigen in urine samples, performed among pediatric patients. Clin Infect Dis. 2001;32(5):824–825. doi:10.1086/319205
15. Arosio C, Vailati M, Moioli F. Urinary detection of Streptococcus pneumoniae antigen for diagnosis of pneumonia. New Microbiol. 2002;25(2):259–263.
16. Falguera M, Ruiz-González A, JA S, et al. Prospective, randomised study to compare empirical treatment versus targeted treatment on the basis of the urine antigen results in hospitalised patients with community-acquired pneumonia. Thorax. 2010;65(2):101–106. doi:10.1136/thx.2009.118588
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.