Back to Journals » Patient Preference and Adherence » Volume 17
Efficacy of Two Different Hydrodynamic Sinus Lift Systems for Atraumatic Elevation in Immediate Implant Placement
Authors Praveen AA ![]() , Venkadassalapathy S, Victor DJ, Prakash PSG, Umesh SG, Ali Baeshen H, Balaji TM, Patil S
, Venkadassalapathy S, Victor DJ, Prakash PSG, Umesh SG, Ali Baeshen H, Balaji TM, Patil S ![]() , Reda R
, Reda R ![]() , Testarelli L
, Testarelli L ![]()
Received 29 December 2022
Accepted for publication 3 May 2023
Published 5 May 2023 Volume 2023:17 Pages 1197—1207
DOI https://doi.org/10.2147/PPA.S403036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Arockia Antony Praveen,1 Santhosh Venkadassalapathy,1 Dhayanand John Victor,1 PSG Prakash,1 Santo Grace Umesh,1 Hosam Ali Baeshen,2 Thodur Madapusi Balaji,3 Shankargouda Patil,4 Rodolfo Reda,5 Luca Testarelli5
1Department of Periodontics, SRM Dental College, Chennai, TN, India; 2Department of Orthodontics, Faculty of Dentistry, King Abdulaziz University, Jeddah, 21589, Saudi Arabia; 3Department of Dentistry, Bharathiraja Hospital, Chennai, TN, India; 4College of Dental Medicine, Roseman University of Health Sciences, South Jordan, UT, 84095, USA; 5Department of Oral and Maxillofacial Sciences, Sapienza University of Rome, Rome, 00161, Italy
Correspondence: Shankargouda Patil, College of Dental Medicine, Roseman University of Health Sciences, South Jordan, UT, AH 84095, USA, Email [email protected] PSG Prakash, Department of Periodontics, SRM Dental College, SRM IST, Ramapuram, Chennai, Tamil Nadu, India, Email [email protected]
Purpose: To evaluate the efficacy of two hydrodynamic sinus lifting procedures and to successfully place immediate implants in maxillary posterior sites that have a compromised native bone as a result of periodontal or endodontic disease.
Patients and Methods: A total of 26 patient sites were enrolled with 13 sites each in the Minimally Invasive Antral Membrane Balloon Elevation (MIAMBE) and Drill Integrated Hydrodynamics for the transcrestal sinus floor elevation (DIHSFE) groups who received transcrestal sinus floor elevation followed by immediate implant placement. Clinical parameters such as sinus membrane perforations, nasal bleeding, postoperative sinusitis, VAS scores at Day-7 for pain and discomfort, primary implant stability and time taken were evaluated.
Results: The DIHSFE had greater sinus membrane perforations and incidence of nasal bleeding when compared with MIAMBE with (p = 0.066) and (p = 0.141). Post-operative sinusitis was evident in both the groups with (p = 0.619). The mean VAS score was statistically significant between both the groups (p ≤ 0.005). The insertion torque values, and mean time taken for surgical procedure was not statistically significant between groups.
Conclusion: The present study highlighted that MIAMBE is superior to DIHSFE in its ability to cause less severe patient morbidities and post-operative complications.
Keywords: immediate implants, insertion torque values, Minimally Invasive Antral Membrane Balloon Elevation, postoperative sinusitis, sinus membrane perforation
Introduction
The posterior maxilla is a potential minefield for the placement of dental implants because of the critical concerns regarding the quantity and quality of bone available in this region. The ravaging of the periodontium by periodontal disease is a further confounder to the placement of dental implants in the posterior maxilla that sets a quantitative deficit to the level of bone available. When the periodontally compromised tooth is extracted, the socket remodeling introduces further dynamics that results in significantly greater loss of the residual alveolus, thereby greatly compromising the dimensions of the residual ridge, and severely detracting from the ability to place implants into this resorbed ridge.1,2 While it is possible to place shorter implants in sites with deficient bone volume, the presence of bone with lesser bone density in the posterior maxilla makes these sites not suitable for shorter implants. Numerous studies have found that shorter implants (<10 mm) are less successful than longer implants.3 Therefore, in the rehabilitation of the posterior maxilla, techniques like Sinus Floor Elevation (SFE), which make it possible to place longer implants in the region, have gained profound interest.4–9 The traditional modes of site development prior to implant placement in the posterior maxilla are the lateral window approach of sinus elevation and the Osteotome Mediated Sinus Floor Elevation (OMSFE), but these techniques are associated with greater patient morbidity and post-operative complications.10,11 To overcome the potential shortcomings associated with the traditional sinus lifts, a technique for the transcrestal sinus floor elevation by hydrodynamics called Minimally Invasive Antral Membrane Balloon Elevation (MIAMBE) was introduced in 2006, which consisted of a balloon inflated by normal saline, to elevate the sinus membrane in an atraumatic manner.12 Several other studies have been performed with the MIAMBE technique and all of these studies have shown that this technique is minimally invasive, safe, and reliable, which results in reduced postoperative pain and morbidity.13–20 A further novel hydrodynamic transcrestal sinus floor elevation was the evolution of the Drill Integrated Hydrodynamics for the transcrestal sinus floor elevation, which has been advocated as being capable of atraumatically lifting the sinus membrane by hydrodynamic pressure, that is allowed to build up between the sinus floor and the Schneiderian membrane, thereby gently elevating the sinus floor in a minimally invasive manner.21–26 While most of the studies evaluated the long-term effects of the techniques and implant stability, limited light is thrown on the immediate complications of the sinus floor elevation techniques. The current study sought to compare the peri-operative complications and post-operative morbidity of two hydrodynamic transcrestal sinus floor elevation techniques that enable the placement of implants at periodontally and endodontically compromised fresh extraction sites with insertion torque 35 Ncm.
Materials and Methods
Ethical Approval
The study was performed in the outpatient clinics at the Department of Periodontics, S.R.M Dental College, Ramapuram, Chennai, Tamil Nadu, India. Ethical and scientific committee approval was obtained from the institutional review board (SRMDC/IRB/2019/MDS/No.502) and was registered in the clinical trials registry (CTRI/2020/01/030595). The study conducted followed the Helsinki Declaration 1964 for ethical human trial.
Study Population
Inclusion and Exclusion Criteria
The inclusion criteria were: 1. Patients greater than 18 years of age. 2. Patients with no systemic diseases that could affect the surgical intervention and wound healing. 3. Patients who had an isolated tooth in the posterior maxilla with periodontal disease reaching up to the apical third of the root, and with native bone of between 3 and 6mm from the alveolar crest to the sinus floor. 4. Patients with a perio-endo lesion in the posterior maxilla that required extraction and that had similar bone dimensions. The exclusion criteria were: 1. Patients with large periapical lesions. 2. Patients who were current or former smokers. 3. Patients with systemic diseases such as diabetes mellitus, bleeding disorders, medications such as immune suppressants that affect the wound healing and that would contraindicate periodontal surgery. 4. Patients with septa at the level of the sinus lift. 5. Pregnant and lactating women. 6. Patients with rhinitis, sinusitis, or maxillary sinus pathology. 7. Patients who had previous implant placement or bone augmentation procedures in the target region.
All the participants willing to take part in the study were explained about the purpose and procedures of study and their possible surgical complications, following which a written informed consent was obtained.
Sample Size Calculation
The outcome of sinus membrane perforations in DIHSFE by Garbacea et al21 and MIAMBE by Kfir et al12 were utilized by the software G-Power version 3.1.9.2 to calculate the sample size. With the power of the study and α error set at 80% and 5%, respectively, the obtained sample size was 26 sites in total and 13 sites per group.
Study Design
An initial recruitment of thirty patient sites was performed based on the stated inclusion and exclusion criteria and were taken up for Phase I therapy with CBCT evaluation followed by atraumatic extraction. Of the initially selected thirty patient sites, four patient sites were excluded following the extraction, due to the deficient native bone in the buccal aspect of the targeted tooth. Hence, a total of twenty-six patient sites that were affected by periodontal disease and had an inadequate alveolar bone along the roots, due to the proximity of the maxillary sinus were included for this randomized clinical trial.
Randomization
The selected patient sites were randomized using an online randomization software tool (http://www.graphpad.com/quickcalcs/index.cfm) into the following study groups and were matched based on the demographic characteristics to avoid bias.
Control Group – Minimally Invasive Antral Membrane Balloon Elevation (MIAMBE) was performed through a transcrestal access, to enable the placement of immediate implants for thirteen patient sites (n = 13).
Test Group – Drill Integrated Hydrodynamic Sinus Floor Elevation (DIHSFE) was performed through a transcrestal access, so as to place immediate implants for thirteen patient sites (n = 13).
Interventions
All the surgical procedures were performed by one of two, well-experienced periodontists. The clinical parameters evaluated were the incidence of sinus membrane perforations, incidence of nasal bleeding, primary implant stability and time taken for the surgical procedure. At one week follow-up point, incidence of post-operative sinusitis and patient’s subjective perception of pain, discomfort, swelling that disrupted day-to-day function was assessed through Visual Analogue Scale (VAS) score. Patients who were recruited for the surgical procedure were administered antibiotic prophylaxis of 1gm of amoxicillin, two hours prior to the surgical procedure. Topical anesthetic gel was applied followed by local infiltration using 2% local anesthesia with 1:80,000 adrenaline and the patients were instructed to rinse with 0.12% chlorhexidine solution, following which atraumatic extraction was carried out using periotomes and luxators.
Surgical Procedure for the Test Group (DIHSFE)
After thorough debridement of the socket, initial osteotomy was performed with the pilot drill. The initial osteotomies was performed up to a dimension that was equivalent to the dimension of drill #1 leaving 2mm of native bone beneath the sinus floor. Following this, drills with hydrodynamics performed the initial sinus penetration. Initially, membrane elevation was performed with the drills #1 and #2 in an atraumatic manner till the floor of the sinus got breached. Drill #3 with drill integrated hydrodynamics was used to complete the initial elevation of the sinus membrane (DASK-Dentium, Korea). Then, transcrestal sinus elevators were utilized to create a uniform membrane separation in an atraumatic manner and autologous fibrin integrated Beta-Tricalcium Phosphate (Sticky bone) was grafted into the sinus (OsteonII-Dentium, Korea). The selected implant was thereafter driven into the osteotomy site with the torque reading in the implant stability initially set at 30 Ncm. When the implant seized, the torque setting on the motor was sequentially increased by 5 Ncm, until the implant was driven 1mm subcrestal to the prepared osteotomy (Superline Implants-Dentium, Korea). The insertion torque reading just before the final torque adjustment was then recorded as the insertion torque value for the patient. All implants placed were specifically designed for immediate implant placement in the posterior segments, in poor quality. The jumping distance between the socket and the implant, as well as the adjoining sockets was also grafted with the fibrin integrated Beta-Tricalcium Phosphate graft that was used to graft the sinus. This matrix was thereafter overlaid with an A-PRF membrane. When primary closure was difficult, a horizontal incision was placed approximately 8mm from the crest of the palatal marginal gingiva to enhance the ability for primary closure. The flap margins were approximated with 3’0 black silk sutures (Figure 1).
 |
Figure 1 DIHSFE (Drill Integrated Hydrodynamic Sinus Floor Elevation) - Test group. (A) Periodontally compromised tooth. (B) CBCT showing deficient native bone and vertical root fracture. (C) Atraumatic extraction showing the intact interradicular bone. (D) DIHSFE technique performed with the insertion of hydrodynamic drills. (E) IOPA showing the breaching of sinus floor with drill integrated hydrodynamics. (F) Autologous fibrin integrated ẞ-TCP (Sticky bone) for sinus augmentation. (G) Immediate implant placement and jumping distance between the socket and the implant, as well as the adjoining sockets was also grafted with the fibrin integrated ẞ-TCP (Sticky bone). (H) A-PRF was laid over followed by flap approximation and sutured. |
Surgical Procedure for the Control Group (MIAMBE)
After thorough debridement of the sockets, initial osteotomy was performed with the pilot drill. The subsequent osteotomy was carried out using implant drills to one size short of the body of the implant, according to the drilling protocol given by the manufacturer, leaving a thin wafer of native bone underneath the sinus floor. A concave osteotome was thereafter utilized to gently fracture-in the sinus floor using a fiber mallet, to breach into the sinus. After this a Minimally Invasive Antral Membrane balloon was inflated with a 3cc syringe containing saline for the atraumatic elevation of the sinus membrane (Sinus Elevator Balloon-Dentium, Korea). Following this, an autologous fibrin integrated Beta-Tricalcium Phosphate (Sticky bone) was grafted into the sinus (OsteonII-Dentium, Korea). The implant placement and grafting of the sockets for the MIAMBE sites was similar to that which was explained in detail for the DIHSFE sites. Briefly, all the implants were placed sub-crestally, and the insertion torque values were noted (Superline Implants-Dentium, Korea). This was followed by grafting of the jumping distance and the adjoining sockets with fibrin integrated ẞ-TCP matrix. This matrix was thereafter overlaid with an A-PRF matrix and the flaps were coronally advanced and passively approximately with 3’0 silk sutures (Figure 2).
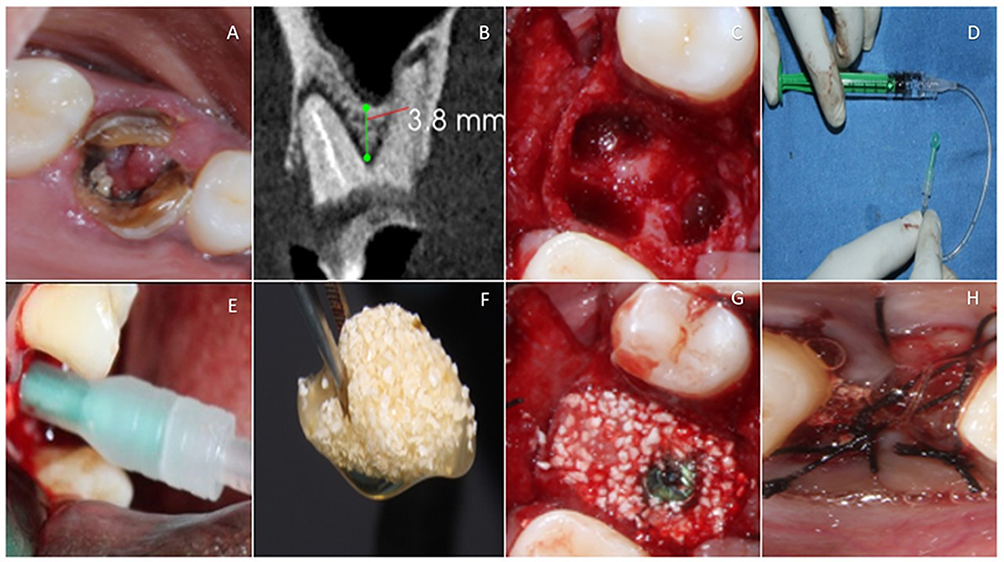 |
Figure 2 MIAMBE (Minimally Invasive Antral Membrane Balloon Elevation) - Control group. (A) Periodontally and endodontically compromised tooth. (B) CBCT showing deficient native bone. (C) Atraumatic extraction showing the intact interradicular bone. (D) Minimally Invasive Antral Balloon with Inflated saline solution. (E) MIAMBE Technique for transcrestal sinus floor elevation. (F) Autologous fibrin integrated ẞ-TCP (Sticky bone) for sinus augmentation. (G) Immediate implant placement and jumping distance between the socket and the implant, as well as the adjoining sockets was also grafted with the fibrin integrated ẞ-TCP (Sticky bone). (H) A-PRF was laid over with flap approximation and sutured. |
Post-Surgical Instructions
All patients were instructed to apply ice intermittently, for the first 3–4 hours on the external surface of the surgical site. Gentle tooth brushing using extra-soft toothbrush and Chlorhexidine gluconate 0.12% mouthwash every 8 hours for two weeks were advocated. They were asked to avoid any negative or positive pressure like blowing the nose, drinking with a straw, spitting out vigorously, for the first week. Oral antibiotics and analgesics were prescribed for all patients post surgically. Nasal decongestants Oxymetazoline HCl 0.25% were prescribed to be used as nasal drops for the first week.
Measurement of Clinical Parameters
The peri-operative clinical parameters were measured at the time of the surgery. The Valsalva Maneuver technique was used to measure the presence of Sinus Membrane Perforations; visual examination of the nasal mucosa was used for the incidence of nasal bleeding. The final insertion torque reading was used to measure the level of primary stability of the implants.
Recall Visits
Patients were asked to report to the department of periodontics for the evaluation of signs and symptoms regarding post-operative sinusitis, and the evaluation of pain, swelling, and discomfort using the VAS score on the Day 7. Sutures were removed two weeks following the surgery.
Statistical Analysis
The statistical analysis was performed using Statistical package for social sciences (SPSS, version 26) statistical software (IBM, Kormonk, New York, US). The descriptive statistics of demographic data (mean age group) and gender were expressed as mean, standard deviation and p-value. The normality of the data distribution pertaining to the evaluated study variables (primary stability, time taken for surgery, VAS scores day-7) was tested using Shapiro Wilk test and skewness/kurtosis test. Data pertaining to primary stability were found to be normally distributed, hence unpaired t-test was performed to test the significance between the compared groups. Whereas the data pertaining to two variables (time taken for surgery, VAS scores day-7) was found to be non-normally distributed (skewed and heavy tailed), Mann–Whitney U-test was performed to test the significance between the compared groups. Levene’s test was performed to test the equality of variances between the compared groups. Intergroup comparison for discrete variables (membrane perforation, nasal bleeding, and post-operative sinusitis) was performed using Chi square test after applying Yates continuity correction; p-value ≤0.05 was considered to be statistically significant.
Results
Descriptive Statistics of the Study Patients – Age; Gender and the Clinical Parameters (Between Control and Test Groups)
The demographic data were evaluated for a difference between the groups with regard to age and gender did not reveal any statistical significance (p ≤ 0.851) and (p ≤ 1.000), respectively (Table 1).
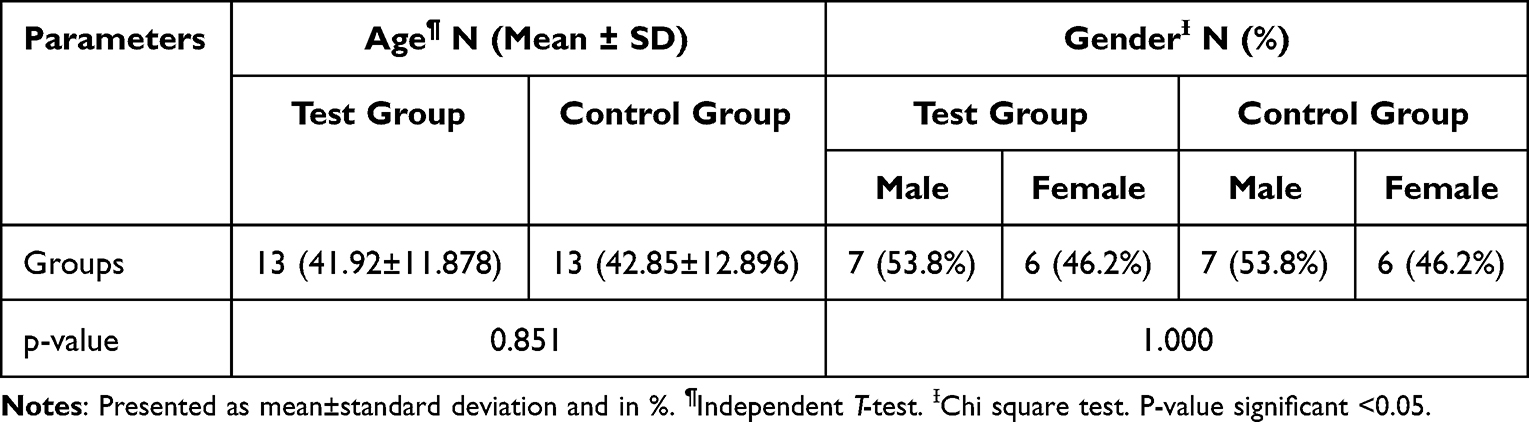 |
Table 1 Descriptive Statistics of the Study Patients – Age; Gender (Between Control and Test Groups) |
Comparison of Incidence of Sinus Membrane Perforations; Nasal Bleeding; Post-Operative Sinusitis – Between Control and Test Groups
The incidence of sinus membrane perforations was compared between the two groups, no statistical significance was found (p ≤ 0.066). The Test group (DIHSFE) had three perforations out of the thirteen patient sites and the incidence of perforations in this group was 23.1%. Control group (MIAMBE) had no perforations with 0% incidence of perforation. The incidence of nasal bleeding was compared between the two groups, which did not reveal statistical significance (p ≤ 0.141). The Control group (MIAMBE) had no peri-operative epistaxis, whereas the Test group (DIHSFE) had an incidence of epistaxis of 2 out 13 patient sites. The incidence of post-operative sinusitis was compared between the two groups which did not reveal any statistical significance (p≤ 0.619). Three of the Test group (DIHSFE) patients and two of the control group (MIAMBE) patients reported with signs and symptoms of post-operative sinusitis. This placed the incidence of postoperative sinusitis at 23.1% in the Test group and 15.4% for the Control group (Table 2). All statistical significance noted between the groups.
 |
Table 2 Comparison of Incidence of Sinus Membrane Perforations; Nasal Bleeding; Post-Operative Sinusitis – Between Control and Test Groups |
Comparison of Primary Implant Stability; Time Taken for Surgery (Minutes); VAS Score – Between Control and Test Groups
All the implants placed had an insertion torque >35Ncm, and the mean insertion torque in the Test group (DIHSFE) was 38.85±7.116 Ncm, whereas in the Control group (MIAMBE) it was 43.46±5.911 Ncm. There was, however, no statistically significant difference between the two groups with regard to insertion torque values (p≤ 0.085). The mean time taken for the Test group (DIHFSE) was 1.731 hours (103.81 minutes), whereas for the Control group (MIAMBE) it was 1.154 hours (69.24 minutes). However, there was no statistically significant difference between the intervention groups for time taken for surgery (p ≤ 0.068). On comparing the VAS score between the two groups, the Test group (DIHSFE) patient sites had a mean VAS score of 4.92, whereas the control group (MIAMBE) patient sites had it was 3.77. The VAS score revealed a statistically highly significant difference between the Test group and Control group (p ≤ 0.005) (Table 3).
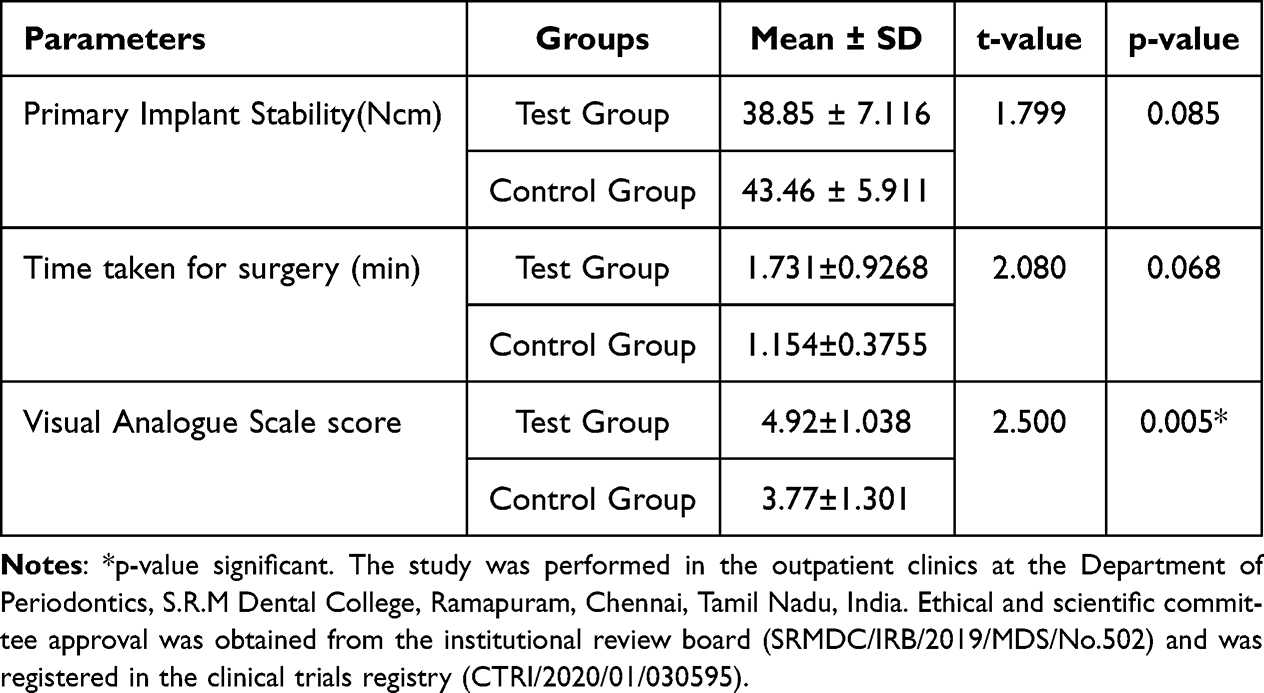 |
Table 3 Comparison of Primary Implant Stability; Time Taken for Surgery (Minutes); Visual Analogue Scale score – Between Control and Test Groups |
The time taken for the surgery was thereafter correlated with the patients’ perception of the morbidity that the patient suffered as evaluated on the Visual Analogue Scale (Figure 3).
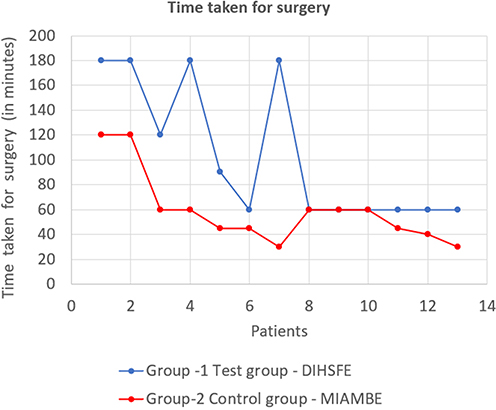 |
Figure 3 Line graph representation of Time taken for the surgery – between control and test groups. |
The Control - MIAMBE group showed negative correlation between time taken, pain and discomfort perceived, but this was not statistically significant (p ≤ 0.9070) (Figure 4).
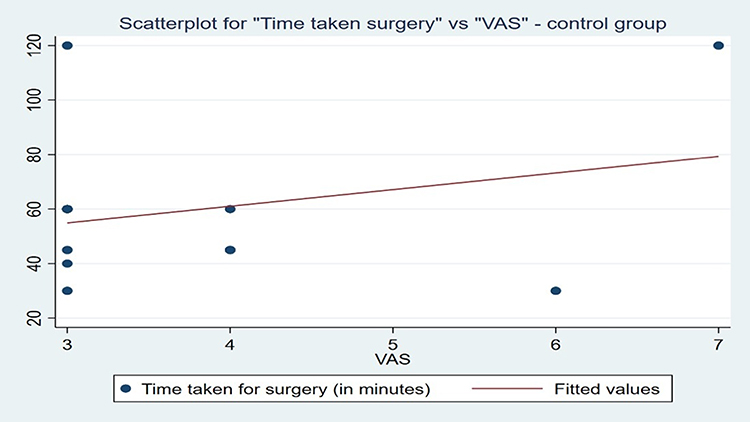 |
Figure 4 Scatter plot representation of correlation between time taken for surgery and Visual Analogue Scale (VAS) – Control group MIAMBE (with Minimally Invasive Antral Membrane Balloon Elevation). |
In the Test - DIHSFE group there was a positive correlation between time taken and pain and discomfort perceived. This was also, however, not statistically significant (p ≤ 0.0662) (Figure 5).
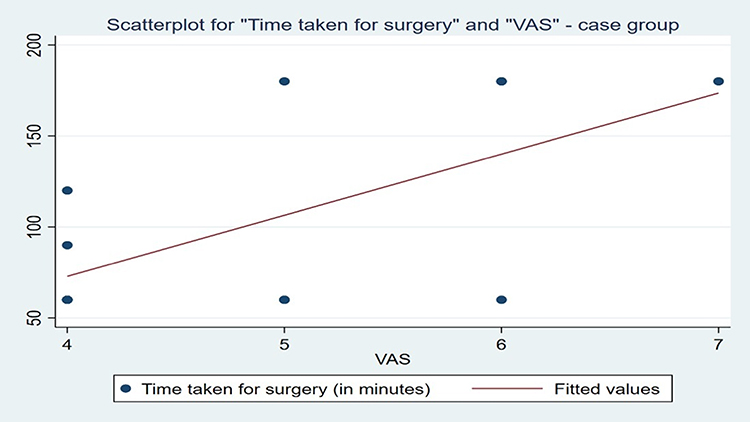 |
Figure 5 Scatter plot representation of correlation between time taken for surgery and Visual Analogue Scale (VAS) – Test group DIHSFE (Drill Integrated Hydrodynamic Sinus Floor Elevation). |
This indicates that certain patients had greater pain and discomfort in sites where MIAMBE technique was performed, and this did not correlate with the time taken. Whereas in the DIHSFE group there was a positive correlation with time taken for surgery and patient pain and discomfort which also affirms the influence of the steeper learning curve.
Discussion
Various studies have highlighted that immediate implant placement into an extraction site does not prevent the loss of bundle bone or buccal bone during both phlogistic and non-phlogistic remodeling processes.27 However, immediate implant placement offers the advantage of placing the implant in superior quality bone before osteoclastic resorption sets in, reducing the quality and even quantity of the bone.28–34 The rationale of the present study was to compare the efficacy of Drill Integrated Hydrodynamics for Sinus Floor Elevation with Minimally Invasive Antral Membrane Balloon Elevation for atraumatic elevation of the sinus membrane through a transcrestal access as well as assess the ability of these techniques to facilitate the placement of an immediate implant of sufficient primary implant stability.
The incidence of membrane perforation in both the control MIAMBE group was 0%, whereas in Test group it was clinically 23.1% (3 out of 13 patients). This difference although being statistically not significant, with a p-value of (p ≤ 0.066), is clinically significant, for sinus membrane perforation which is associated with significantly greater sinusitis, sinus graft mobility and graft infection in the Test group. The results of this study regarding no perforation in the MIAMBE is similar to multiple studies that reported no incidence of sinus membrane perforation.12–20 Garbacea et al,21 did a pilot study in 2012 on the occurrence of Maxillary Sinus Membrane Perforation, with the use of Drill Integrated Hydrodynamics, which were assessed endoscopically, and concluded that there was no sinus membrane perforation with sinus floor elevation utilizing drill integrated hydrodynamics. These authors stated that there was no membrane perforation up to the membrane elevation of 5.0mm. In our study, all the patients had a sinus floor elevation greater than 5.0mm.
The incidence of nasal bleeding in the Control group was 0%, whereas in the Test group it was 15.4% (two patients). This difference though was not statistically significant (p ≤ 0.141). The two patients who had nasal bleeding were also among the three patients with sinus membrane perforation. The nasal bleeding in these patients was present intra-operatively for one and three minutes and was arrested when light pressure was applied at the bridge of the nose. The presence of post-operative sinusitis was evaluated by signs and symptoms such as fever, headache, and poor sense of smell, sore throat, nasal mucus, plugged nose, facial pain and cough, which was evaluated on Day-7. Post-operative sinusitis was evident in both the Control and Test groups, 15.4% (two patients) in the Control group, and 23.1% (three patients) in the Test group. This difference was not statistically significant (p ≤ 0.619).
The patient’s perception of pain and discomfort was graded on a Visual Analogue Scale (VAS), which was evaluated at 1-week post-surgery. Subjective assessment of pain, discomfort and swelling that interfered with daily activity was used to record the VAS score. The VAS score in both the control and test groups was evaluated on a score of 1 to 10, ranging from no discomfort, to a high of 10 indicating worst possible pain. The MIAMBE group had a mean VAS score of 3.77±1.301, whereas in the DIHSFE group it had a mean VAS score of 4.92±1.038. This difference was statistically highly significant, indicating that the MIAMBE group was associated with statistically significant levels of lesser discomfort (p ≤ 0.005). The discomfort and pain experienced by the control MIAMBE group patients, despite having no perforations could be possibly attributed to the force exerted to fracture the native bone by the mallet during the procedure. These results regarding significantly lesser pain and discomfort in the MIAMBE group is similar to other studies utilizing MIAMBE, which indicate an excellent success rate with lesser patient morbidity and low complication rate, minimal discomfort, and bleeding12–20 The mean insertion torque value for the MIAMBE group was 43.46±5.91 Ncm, whereas for the DIHSFE group it was 38.85±7.116 Ncm. The comparable insertion torque values that did not have statistically significant differences (p ≤ 0.085) highlighted the similar potential for both the hydrodynamic techniques to modulate the native bone to place implants, whilst retaining the potential to be successfully osseointegrated, as identified by the primary stability acquired.
Studies regarding the MIAMBE technique with concomitant implant placement have shown that MIAMBE enables adequate primary implant stability.14,15 All our patients had acceptable primary stability as assessed by insertion torque values, and this is probably due to the placement of immediate implants into fresh extraction sockets, for the residual alveolus frequently has lesser density when the alveolar bone is allowed to remodel prior to implant placement. As far as we are aware, no earlier studies have assessed the primary implant stability with Ncm values in relation to Drill Integrated Hydrodynamics for Sinus Floor Elevation with the concomitant implant placement. This is an additional novelty to this study.
The mean time taken for the surgical procedure for the MIAMBE group was 1.154±0.3755 hours which is 69.24 minutes. The Test group, however, had a mean time taken of 1.731±0.9268 hours which is 103.86 minutes. This indicates that there was a mean difference of 34.62 minutes by which the DIHSFE was longer in this study. This was not statistically significant (p ≤ 0.068), but is clinically relevant. It also shows that when the learning curve is breached it has comparable time taken, when compared to MIAMBE. Kfir et al13,14 performed a study with Minimally Invasive Antral Membrane Balloon Elevation and evaluated the procedural time along with the implant placement. The mean time taken in these studies were of 1.5 hours for the surgical procedure with the (mean ± SD) of (48 ± 23) minutes. The mean time taken for the MIAMBE group in the current study is comparable with these earlier studies.
Our study hypothesized that Drill Integrated Hydrodynamics technique for the transcrestal sinus floor elevation could be similar to the Minimally Invasive Antral Membrane Balloon Elevation technique in its ability to atraumatically perform transcrestal sinus floor. The current study has shown that the greater number of sinus membrane perforations and bleeding from the nose are possibly attributable to this steep learning curve to appropriate the technique for effective sinus floor elevation with drill integrated hydrodynamics. A second and perhaps more important factor that must be highlighted based on this study is that though these sites that have been ravaged by periodontal disease, it is possible to place implants into fresh extraction sockets with adequate primary stability, with transcrestal sinus floor elevation to augment the deficiency caused by the periodontal destruction. The possible limitations of the current study include lack of assessment of the anatomic variables of the sinus floor and its inclination which might impact the sinus membrane perforation.28 Also, since the drill integrated hydrodynamic techniques followed requires precise skills and experience, it is difficult for beginners to effectively manage without a greater degree of patient morbidity. Furthermore, long-term follow-up to assess implant success and survival has been a shortcoming of the current study.
Conclusion
Despite the promising findings presented in the study, the Drill Integrated Hydrodynamics procedure for the transcrestal sinus floor elevation is a technique sensitive procedure, and beginners or less experienced operators may find it difficult to perform this without a greater degree of patient morbidity. The combination of both the hydrodynamic techniques with DIHSFE for atraumatic breaching of the sinus floor at the osteotomy site and MIAMBE for atraumatic elevation of the sinus floor could be the best possible treatment protocol to overcome the peri-operative and post-operative complications. Future studies need to be longitudinally monitored to evaluate appropriately the efficacy of such implants to function in health for a longer period of time.
Data Sharing Statement
The data availability statement is on request available with the author – Arockia Antony Praveen, email id: [email protected]. The Demographic data and the clinical parameters can be shared on request. The informed consent and radiographic documents shall be shared and all the data will be shared in a common linked drive for a period of 4 weeks from the time of publication.
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cao Z, Yuan J. Changes in maxillary sinus mucosal thickening following the extraction of teeth with advanced periodontal disease: a retrospective study using cone-beam computed tomography. Biomed Res Int. 2021;2021:1–8. doi:10.1155/2021/4014797
2. Lim HC, Kim S, Kim DH, Herr Y, Chung JH, Shin S. Il Factors affecting maxillary sinus pneumatization following posterior maxillary tooth extraction. J Periodontal Implant Sci. 2021;51:285–295. doi:10.5051/jpis.2007220361
3. Thoma DS, Zeltner M, Hüsler J, Hämmerle CHF, Jung RE. EAO supplement working Group 4 - EAO CC 2015 short implants versus sinus lifting with longer implants to restore the posterior maxilla: a systematic review. Clin Oral Implants Res. 2015;26(Suppl 1):154–169. doi:10.1111/clr.12615
4. Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg. 1980;38:613–616.
5. Summers RB. The osteotome technique: part 3--less invasive methods of elevating the sinus floor. Compendium. 1994;15:
6. Guarnieri R, Reda R, Di Nardo D, Miccoli G, Zanza A, Testarelli L. Clinical, radiographic, and biochemical evaluation of two-piece versus one-piece single implants with a laser-microgrooved collar surface after 5 years of functional loading. Clin Implant Dent Relat Res. 2022;24(5):676–682. doi:10.1111/cid.13118
7. Guarnieri R, Zanza A, D’Angelo M, et al. Correlation between peri-implant marginal bone loss progression and peri-implant sulcular fluid levels of metalloproteinase-8. J Pers Med. 2022;12(1):58. doi:10.3390/jpm12010058
8. Lundgren S, Cricchio G, Hallman M, Jungner M, Rasmusson L, Sennerby L. Sinus floor elevation procedures to enable implant placement and integration: techniques, biological aspects and clinical outcomes. Periodontol. 2017;73:103–120. doi:10.1111/prd.12165
9. Cha J-K, Kim C, Pae H-C, Lee J-S, Jung U-W, Choi S-H. Maxillary sinus augmentation using biphasic calcium phosphate: dimensional stability results after 3–6 years. J Periodontal Implant Sci. 2019;49:47–57. doi:10.5051/jpis.2019.49.1.47
10. Calin C, Petre A, Osteotome-Mediated Sinus DS. Floor elevation: a systematic review and meta -analysis. Int J Oral Maxillofac Implant. 2014;29(3):558–576. doi:10.11607/jomi.3206
11. Stacchi C, Andolsek F, Berton F, Perinetti G, Navarra CO. Intraoperative complications during sinus floor elevation with lateral approach: a systematic review. Int J Oral Maxillofac Implant. 2017;32(3):e107–e118. doi:10.11607/jomi.4884
12. Kfir E, Kfir V, Mijiritsky E, Rafaeloff R, Kaluski E. Minimally invasive antral membrane balloon elevation followed by maxillary bone augmentation and implant fixation. J Oral Implantol. 2006;32:26–33. doi:10.1563/782.1
13. Kfir E, Goldstein M, Yerushalmi I, et al. Minimally invasive antral membrane balloon elevation - results of a multicenter registry. Clin Implant Dent Relat Res. 2009;11(Suppl 1):e83–e91. doi:10.1111/j.1708-8208.2009.00213.x
14. Kfir E, Kfir V, Kaluski E, Mazor Z, Goldstein M. Minimally invasive antral membrane balloon elevation for single-tooth implant placement. Quintessence Int. 2011;42:645–650.
15. Kfir E, Goldstein M, Rafaelov R, et al. Minimally invasive antral membrane balloon elevation in the presence of antral septa: a report of 26 procedures. J Oral Implantol. 2009;35:257–267. doi:10.1563/AAID-JOI-D-09-00024.1
16. Mazor Z, Kfir E, Lorean A, Mijiritsky E, Horowitz RA. Flapless approach to maxillary sinus augmentation using minimally invasive antral membrane balloon elevation. Implant Dent. 2011;20:434–438. doi:10.1097/ID.0b013e3182391fe3
17. Peñarrocha-Diago M, Galán-Gil S, Carrillo-García C, Peñarrocha-Diago D, Peñarrocha-Diago M. Transcrestal sinus lift and implant placement using the sinus balloon technique. Med Oral Patol Oral Cir Bucal. 2012;17:e122–e128. doi:10.4317/medoral.17268
18. ElAbbasy S. Efficacy of hydraulic pressure in transcrestal sinus membrane elevation followed by immediate implant placement without bone graft. Egypt J Oral Maxillofac Surg. 2019;10:27–33. doi:10.21608/omx.2019.13288.1028
19. Elbareki AA, Darwish SA. Transcrestal sinus lift and implant placement using the sinus balloon technique. Alexandria Dent J. 2016;41:245–252. doi:10.21608/adjalexu.2016.58034
20. Asmael HM. Is antral membrane balloon elevation truly minimally invasive technique in sinus floor elevation surgery? A systematic review. Int J Implant Dent. 2018;4:1–8. doi:10.1186/s40729-018-0123-9
21. Garbacea A, Lozada JL, Church CA, et al. The incidence of maxillary sinus membrane perforation during endoscopically assessed crestal sinus floor elevation: a pilot study. J Oral Implantol. 2012;38:345–359. doi:10.1563/AAID-JOI-D-12-00083
22. Chen Y, Yuan S, Zhou N, Man Y. Transcrestal sinus floor augmentation with immediate implant placement applied in three types of fresh extraction sockets: a clinical prospective study with 1-year follow-up. Clin Implant Dent Relat Res. 2017;19:1034–1043. doi:10.1111/cid.12529
23. Jang JW, Chang H-Y, Pi S-H, Kim Y-S, You H-K. Alveolar crestal approach for maxillary sinus membrane elevation with <4 mm of residual bone height: a case report. Int J Dent. 2018;2018:1063459. doi:10.1155/2018/1063459
24. Zhao X, Gao W, Liu F. Clinical evaluation of modified transalveolar sinus floor elevation and osteotome sinus floor elevation in posterior maxillae: study protocol for a randomized controlled trial. Trials. 2018;19:1–7. doi:10.1186/s13063-018-2879-x
25. An X, Lee C, Fang Y, Choi B-H. Immediate nonfunctional loading of implants placed simultaneously using computer-guided flapless maxillary crestal sinus augmentation with bone morphogenetic protein-2/collagen matrix. Clin Implant Dent Relat Res. 2019;21:1054–1061. doi:10.1111/cid.12831
26. Gong T, Hu C, Chen Y, Zhou N, Wu H, Man Y. Raising the transcrestal sinus floor in the presence of antral pseudocysts, and in sinus floors with a normal schneiderian membrane: a retrospective cohort study. Br J Oral Maxillofac Surg. 2019;57:466–472. doi:10.1016/j.bjoms.2019.04.007
27. Baskaran P, Prakash PSG, Appukuttan D, et al. Clinical and radiological outcomes for guided implant placement in sites preserved with bioactive glass bone graft after tooth extraction: a controlled clinical trial. Biomimetics. 2022;7:43. doi:10.3390/biomimetics7020043
28. Choi YJ, Kim YH, Han -S-S, et al. Alveolar bone height according to the anatomical relationship between the maxillary molar and sinus. J Periodontal Implant Sci. 2020;50:38–47. doi:10.5051/jpis.2020.50.1.38
29. Huynh-Ba G, Pjetursson BE, Sanz M, et al. Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement. Clin Oral Implants Res. 2010;21:37–42. doi:10.1111/j.1600-0501.2009.01870.x
30. Blanco J, Nuñez V, Aracil L, Muñoz F, Ramos I. Ridge alterations following immediate implant placement in the dog: flap versus flapless surgery. J Clin Periodontol. 2008;35:640–648. doi:10.1111/j.1600-051X.2008.01237.x
31. Clementini M, Tiravia L, De Risi V, VittoriniOrgeas G, Mannocci A, de Sanctis M. Dimensional changes after immediate implant placement with or without simultaneous regenerative procedures: a systematic review and meta-analysis. J Clin Periodontol. 2015;42:666–677. doi:10.1111/jcpe.12423
32. Chappuis V, Araújo MG, Buser D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontol. 2017;73:73–83. doi:10.1111/prd.12167
33. Guarnieri R, Reda R, Zanza A, Miccoli G, Nardo DD, Testarelli L. Can peri-implant marginal bone loss progression and a-MMP-8 be considered indicators of the subsequent onset of peri-implantitis? A 5-year study. Diagnostics. 2022;12(11):2599. doi:10.3390/diagnostics12112599
34. Araújo MG, Silva CO, Souza AB, Sukekava F. Socket healing with and without immediate implant placement. Periodontol. 2019;79:168–177. doi:10.1111/prd.12252
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.