Back to Journals » Clinical Ophthalmology » Volume 17
Efficacy of Prophylactic Anti-VEGF in Preventing Radiation Retinopathy: A Systematic Review and Meta-Analysis
Authors Victor AA ![]() , Andayani G
, Andayani G ![]() , Djatikusumo A, Yudantha AR, Hutapea MM, Gunardi TH, Soetjoadi H
, Djatikusumo A, Yudantha AR, Hutapea MM, Gunardi TH, Soetjoadi H ![]()
Received 2 August 2023
Accepted for publication 4 October 2023
Published 11 October 2023 Volume 2023:17 Pages 2997—3009
DOI https://doi.org/10.2147/OPTH.S433531
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract of "Prophylactic Anti-VEGF in preventing RR" [ID 433531].
Views: 127
Andi Arus Victor,1 Gitalisa Andayani,1 Ari Djatikusumo,1 Anggun Rama Yudantha,1 Mario Marbungaran Hutapea,1 Triana Hardianti Gunardi,2 Hannah Soetjoadi2
1Department of Ophthalmology, Faculty of Medicine, Universitas Indonesia, Dr. Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia; 2Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
Correspondence: Andi Arus Victor, Department of Ophthalmology, Faculty of Medicine, Universitas Indonesia, Dr. Cipto Mangunkusumo National General Hospital, Jalan Kimia No. 8, Menteng, Central Jakarta, 10320, Indonesia, Tel +62818875677, Email [email protected]
Background: In patients predisposed to radiation retinopathy (RR), administration of therapy after apparent clinical signs and symptoms are considered too late, resulting in substantial vision loss and blindness. Early initiation of anti-vascular endothelial growth factor (anti-VEGF) might serve as a strategy to slow disease progression and prolong good eyesight.
Objective: To evaluate the efficacy of prophylactic anti-VEGF in preventing RR and preserving vision in patients at high risk of radiation-induced vision loss.
Methods: A systematic literature search was performed from inception to 4 June 2023 using Cochrane Library, EMBASE, PubMed (MEDLINE), and Scopus. Eligible studies were clinical trials and observational studies investigating the incidence of radiation maculopathy (RM), radiation optic neuropathy (RON), moderate vision loss (loss of more than or equal to 3 lines of baseline visual acuity [VA]) and final VA, whether good (20/40 or better) or poor (20/200 or worse), following prophylactic anti-VEGF. Three reviewers independently conducted article screening, data extraction and risk of bias assessment. Random effects models were used to determine the cumulative effects of each outcome.
Results: Four studies (one clinical trial and three observational studies), involving 2109 patients, were included in our analysis. Across all studies, there were significant reductions in the events of RM (pooled odds ratio [OR] 0.50; 95% CI, 0.34– 0.74; p = 0.001), RON (pooled OR 0.62; 95% CI, 0.42– 0.90; p = 0.012) and poor final VA (pooled OR 0.50; 95% CI, 0.37– 0.68; p = 0.003). The association of moderate vision loss and good final VA with the use of prophylactic anti-VEGF between the groups was unclear owing to the high level of heterogeneity.
Conclusion: Prophylactic anti-VEGF therapy might delay RM and RON, preventing high-risk patients from developing poor VA by approximately 50%. However, this evidence should be interpreted with caution because of its low level of certainty. Future robust studies are warranted to confirm this finding.
Keywords: prophylaxis, prevention, anti-vascular endothelial growth factor, radiation injuries, retinal diseases
Introduction
In the management of ocular malignancies, radiation therapy is preferred to enucleation because it preserves the vision and thereby improves the quality of life.1 However, a dose-dependent, continuous radiation exposure to the eyes inevitably induces local vascular injury and intraocular anti-vascular endothelial growth factor (VEGF) overproduction. This breakdown of blood-retina barrier leads to increased vascular permeability, closure and proliferation, which ultimately results in ocular complications associated with irreversible visual impairment.2 The Collaborative Ocular Melanoma Study (COMS) group demonstrated that 43% of 602 patients with uveal melanoma developed visual acuity of more than or equal to 20/200 three years after plaque radiotherapy.3 This poor visual prognosis is typically attributed to radiation retinopathy (RR), which manifests as radiation maculopathy (RM) and radiation optic neuropathy (RON).
In the absence of a standardized treatment for RM and RON, therapeutic approaches similar to those used for diabetic retinopathy have been proposed because of their resemblance in disease development. A periodic, off-labelled use of intravitreal anti-VEGF agents has been demonstrated to regress RM and RON findings as well as stabilize or improve visual acuity (VA).4,5 Unfortunately, these beneficial effects were affected by the total doses of radiation and timing of anti-VEGF administration. While a higher dose of radiation negatively correlates with anti-VEGF efficacy, earlier treatment yields better visual prognosis because if anti-VEGF is administered when radiation-related clinical findings are present, some degree of retinal injuries remain and often relapse with resultant vision loss over time.6 In addition, optical coherence tomography angiography (OCT-A), a highly sensitive modality of microvascular imaging, revealed that immediately after radiation therapy has started, subclinical retinal vasculopathy develops and will continue for approximately 23.2 months (range 3–72 months) until RR and ocular signs or symptoms are evident.7–9
Therefore, patients treated with a radiotherapy dose of more than or equal to 50–70 Gy to the fovea have an exceptionally high risk of developing RR and receiving delayed treatment.10,11 Initiation of anti-VEGF before the presence of apparent retinal damage or radiation-associated vision loss has been proposed to slow the nature of the disease and prolong the retention of VA. As studies investigating this hypothesis have emerged in recent years, this paper aims to systematically review and conduct a pooled analysis regarding the efficacy of prophylactic intravitreal anti-VEGF in preventing RR and preserving vision among high-risk patients.
Methods
The current review followed the predefined protocol of Prepared Items for Systematic Reviews and Meta-Analysis (PRISMA) 202012 and has been registered in PROSPERO (CRD42023432544).
Eligibility Criteria
All clinical trials and observational studies that used prophylactic intravitreal anti-VEGF in individuals at high risk of radiation-induced vision loss were eligible for inclusion. High-risk patients were those who had subfoveal or juxtafoveal tumor location, or had received a radiation therapy dose of more than or equal to 50–70 Gy to the fovea.10,11 The main exclusion criteria were pre-existing macular diseases, prior treatment for ocular malignancies, and previous administration of intravitreal injections. We also excluded studies performed on animals or adolescents (less than 18 years of age), presented in case reports, and published in languages other than English.
Eligible studies reported at least one of the following outcomes: (1) clinically evident RM, defined as ophthalmoscopic findings of macular edema, exudation, hemorrhage, or nerve fiber layer infarction; (2) clinically evident RON, defined as ophthalmoscopic findings of optic disc congestion, edema, pallor, or peripapillary retinal nerve fiber layer hemorrhage or infarction; (3) moderate vision loss, defined as loss of more than or equal to 3 lines of best-corrected visual acuity (BCVA) from baseline on the Snellen chart;13 (4) good final VA, defined as a final BCVA 20/40 or better vision on the Snellen chart; (5) poor final VA, defined as a final BCVA 20/200 or worse vision on the Snellen chart.
Search Method
A literature search was conducted using four electronic databases: Cochrane Library, Embase, PubMed (MEDLINE), and Scopus. We obtained all articles from the date of inception to 4 June 2023. The keywords included “radiation retinopathy”, “anti-VEGF”, and their respective MeSH terms and synonyms. Studies that were not widely available were identified using ProQuest, an online repository of global academic, corporate, governmental, public, and school libraries. We also searched ClinicalTrials.gov for unpublished results of clinical trials. A manual search of relevant review papers and websites of small ophthalmology journals and magazines was performed to find additional articles. Table 1 details the search strategy.
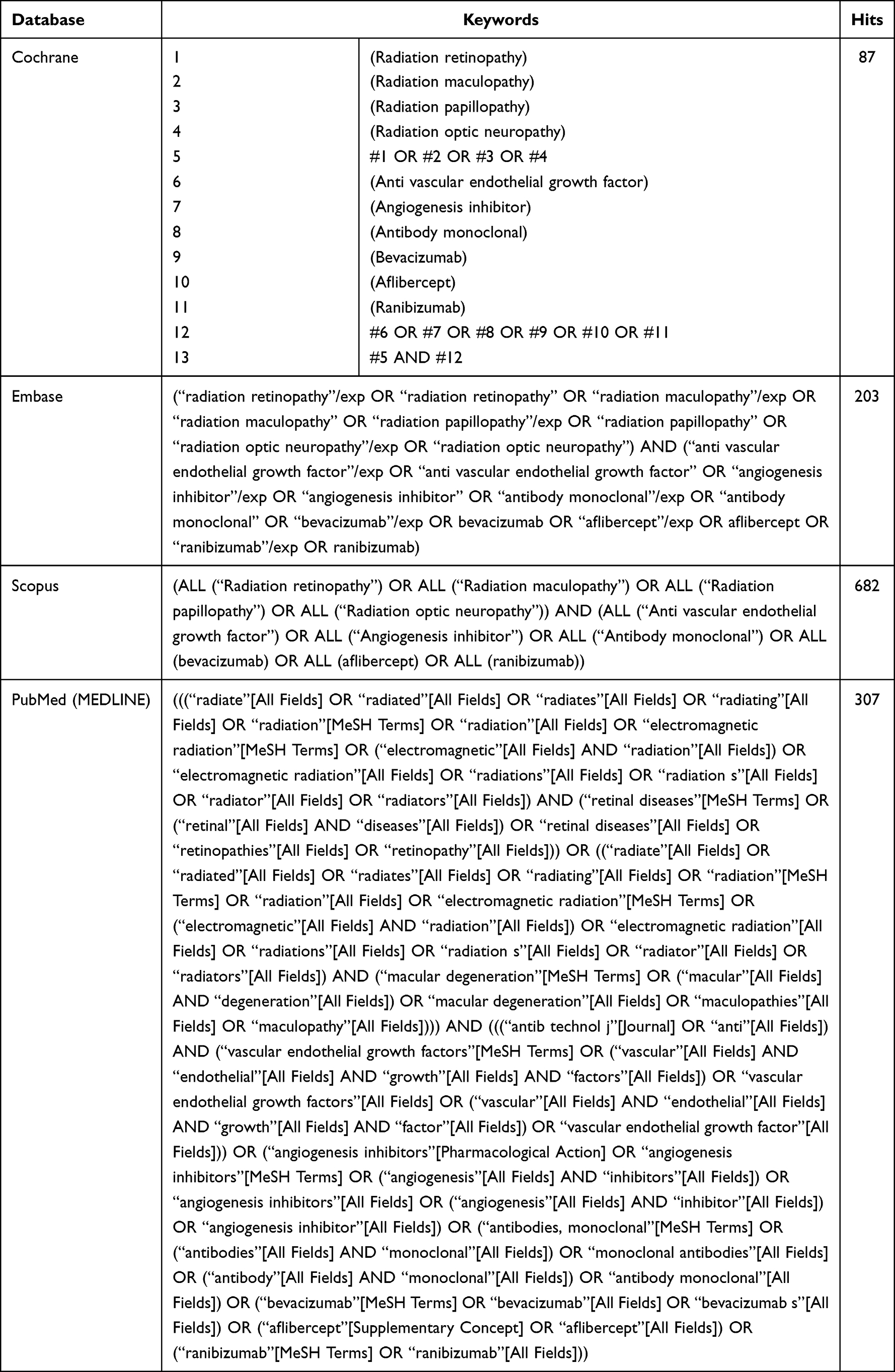 |
Table 1 Search Strategy |
Study Selection
All search results were incorporated into reference management software (EndNote version X9.3.3, Clarivate Analytics, 2013), and duplicates were removed. Three reviewers (AAV, THG, HS) independently screened study eligibility based on the title and abstract, followed by the full text. Any disagreements between the reviewers were resolved by consulting with other reviewers (GLS, AD, ARY, MMH). When multiple reports of the same trial were discovered, only the primary report was included, whereas the other reports were considered companion reports.
Data Collection and Risk of Bias Assessment
Data from the included studies were extracted using a standardized abstraction table. These data included the first author, year of publication, study location, study design, number of enrolled subjects, baseline characteristics (age, underlying ocular malignancy, type and dose of radiation therapy), treatment details (regimen, dose, and duration), treatment response (events of RM and RON, presence of visual loss, and final VA), duration of follow-up, and adverse effects. To show the magnitude of the intervention effect, the baseline BCVA and its mean change were converted to approximate Early Treatment Diabetic Retinopathy Study (ETDRS) letter scores.14
The methodological quality of each included study was discussed among the three authors (AAV, THG, HS) using the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool.15 The assessment covered seven domains: bias due to confounding, bias in selection of participants into the study, bias in classification of interventions, bias due to deviations from intended interventions, bias due to missing data, bias in measurement of outcomes, and bias in selection of reported results. Each domain was rated as low, moderate, serious, or critical risk of bias, with the worst value representing the overall rating of each study. The certainty of evidence for each outcome was assessed in a manner similar to the risk of bias using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.
Data Synthesis and Statistical Analysis
To estimate the size of the treatment effect in each individual study, odds ratios (OR) and relative risks (RR) were used accordingly. If the data were not readily available, manual calculations and/or conversions were appropriately performed. Records at the longest treatment duration were taken, allowing trials that reported outcome data at different time points to be included in the pooled analysis. The data were combined and analyzed using STATA 14.0 (StataCorp, 2015). Random-effects models (DerSimonian-Laird [DL]) were used for the meta-analysis of each outcome. A priori subgroup analysis, based on the type of effect estimate, was performed. An overall pooled effect estimate across the different types of effect estimates was computed for comparison. Statistical heterogeneity was examined using the I2 statistic and chi-square test. I2 more than 50% demonstrates substantial heterogeneity, while a p-value less than 0.1 indicates statistically significant heterogeneity. High levels of heterogeneity were assessed to determine the potential causes.
Results
Literature Search
As shown in Figure 1, the search strategy retrieved 1,301 citations from major databases and other sources. After screening titles and abstracts, 121 articles were assessed based on the eligibility criteria. The final review obtained four qualified studies for further analysis. One compatible publication was excluded because it originated from the same trial in one of the selected studies and reported similar data.16
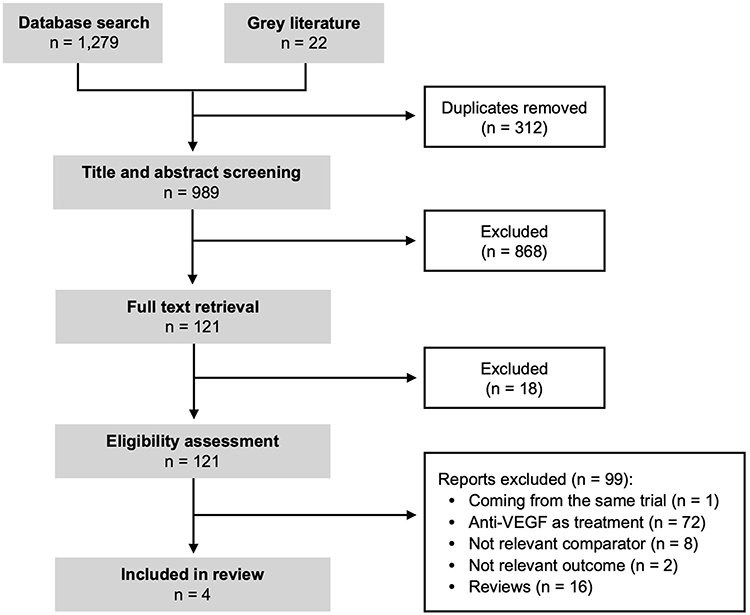 |
Figure 1 Study selection process. |
Study Characteristics
The detailed characteristics of the four studies, consisting of a Phase I clinical trial17 and three retrospective cohorts,18–20 are summarized in Table 2. These studies were conducted in the United States, ranging from 2014 to 2020. A total of 13,609 participants were included in this meta-analysis. All studies recruited middle-aged adults and elderly people, with an average age of 60 years. No statistical difference was found in the participant age between the intervention and control groups. Unlike most studies that were performed in choroidal melanoma patients and plaque radiotherapy recipients, Shah et al investigated individuals with uveal melanoma18 and Kim et al explored those who underwent proton beam radiotherapy.17 The mean dose of radiation therapy to the fovea (87 Gy across studies) did not significantly differ between groups.
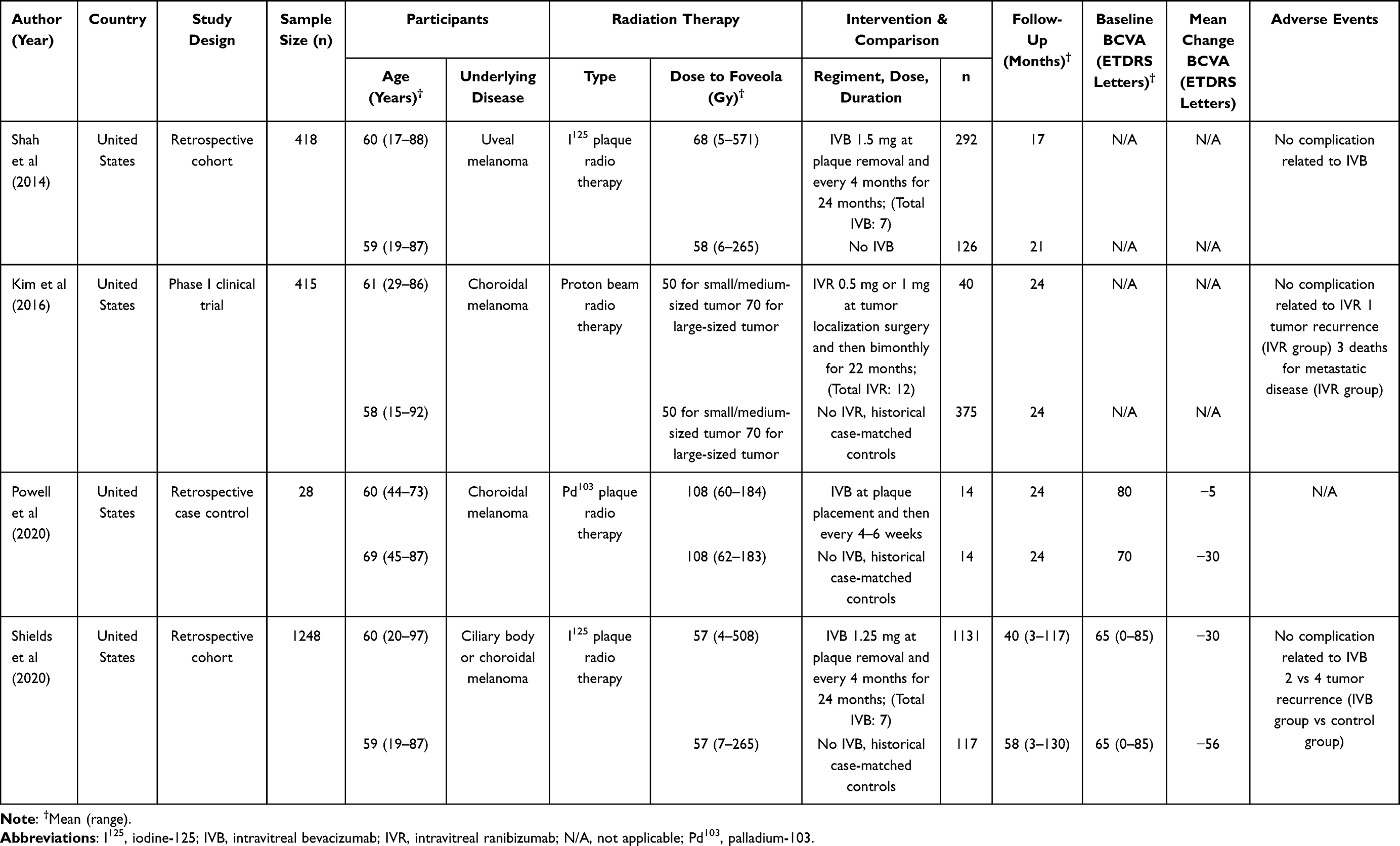 |
Table 2 Study Characteristics |
The therapeutic interventions used were intravitreal bevacizumab (IVB) or intravitreal ranibizumab (IVR), given in varying delivery protocols and doses for two years (average time for RR and vision loss to occur7–9). The mean follow-up duration was 26 months (range 3–117 months). Patients in the intervention arm were compared to those who underwent observation only. Three studies used historical (before the advent of anti-VEGF therapy) case-matched controls who met the criteria for tumor location, tumor size, and radiation dose to the fovea.17,19,20 BCVA was not statistically different at baseline in two studies, but there was a greater mean reduction in BCVA in the control group.21,22 No adverse events associated with intravitreal injections were reported among three studies.17,18,20
Risk of Bias Assessment
Overall, the included studies had a moderate-to-serious risk of bias (Table 3). At the pre-intervention stage, bias due to confounding was moderate in three studies since they did not adjust the outcomes with the confounders despite appropriate matching. Only Shields’ study had a low risk of bias because the outcomes were adjusted for age, tumor thickness or diameter, as well as dose and distance to the foveola or disc. For selection bias, three studies were graded as moderate because they used historical controls, which may have inflicted some degree of bias, instead of concurrent controls like in Shah’s study. Moreover, all studies had a low risk of intervention bias. At the post-intervention stage, two studies had a moderate risk of bias due to deviations from the intended interventions. Shah et al reported that only 9% (24/292) of patients received complete 7-dosed therapy, while Shields et al reported that they could not ascertain the number of periodic interventions missed within the total study duration. Considering that the assessment of RM, RON, and BCVA was subjective to some extent, bias in outcome measurement was moderate in three retrospective studies because the assessors used objective data from medical records to retrieve the outcomes of interest. However, Kim’s study had a serious risk of bias owing to the nature of the early phase trial (no blinding to both the participants and assessors).
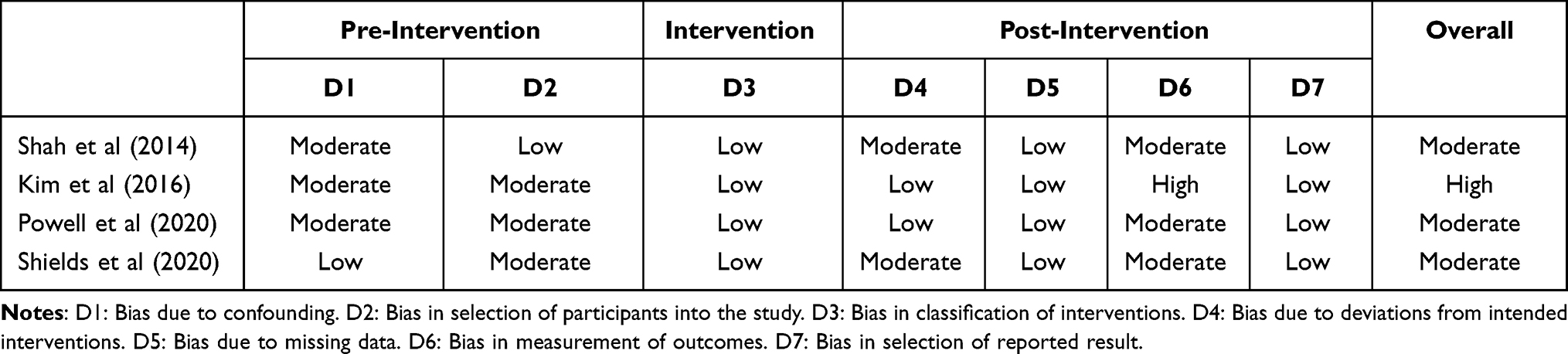 |
Table 3 Risk of Bias Assessment Using ROBINS-I Tool |
Effectiveness of Prophylactic Anti-VEGF in Preventing Events of RM and RON
The use of prophylactic anti-VEGF significantly reduced the presence of RM by half (pooled OR, 0.50; 95% CI, 0.34–0.74; p = 0.001) at the end of the study (Figure 2). Low heterogeneity was detected among the observational studies (I2 = 27.1%, p = 0.25). When combined with one study presented in RR, the overall pooled effect estimate was 0.51 (95% CI, 0.39–0.67). Similarly, the incidence of RON in the intervention group significantly decreased by 38% (pooled OR, 0.62; 95% CI, 0.42–0.90; p = 0.012), with no evidence of heterogeneity (I2 = 0%, p = 0.44) (Figure 3). The overall pooled effect estimate was 0.58 (95% CI, 0.40–0.83).
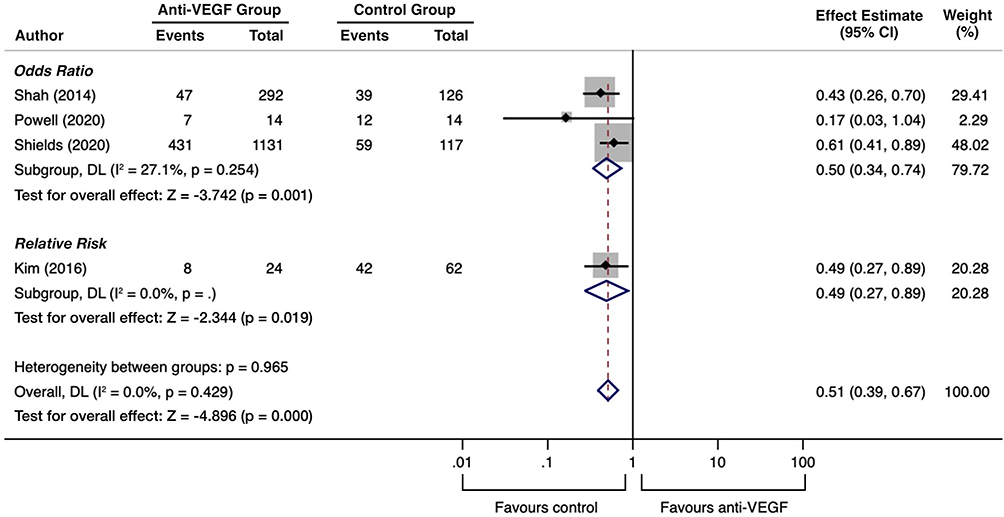 |
Figure 2 Forest plot for events of RM following prophylactic anti-VEGF. |
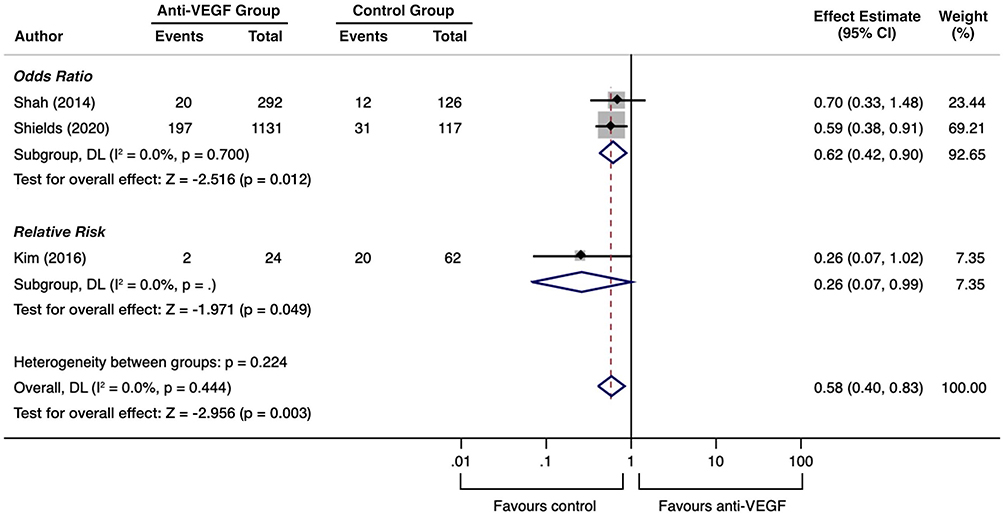 |
Figure 3 Forest plot for events of RON following prophylactic anti-VEGF. |
Effectiveness of Prophylactic Anti-VEGF in Preserving Vision
Although there was a decreasing trend in moderate vision loss favoring the control group, the difference was not significant (pooled OR, 0.12; 95% CI, 0.01–1.97; p = 0.139) (Figure 4). A high level of heterogeneity (I2 = 74.3%, p = 0.05) was identified in two studies reporting this outcome. Moreover, at the final examination, good VA was considerably found in patients treated with prophylactic anti-VEGF. However, the results were not significantly different (pooled OR, 4.03; 95% CI, 0.47–34.68; p = 0.204) or homogenous (I2 = 80.3%, p = 0.02) (Figure 5). In contrast, those who received preventive therapy showed a significant 50% reduction in the odds of developing poor final VA (0.05; 95% CI, 0.37–0.68; p = 0.003). The result showed no heterogeneity (I2 = 0%, p = 0.75) and was consistent with the overall pooled effect estimate (pooled OR, 0.41; 95% CI, 0.23–0.74) (Figure 6).
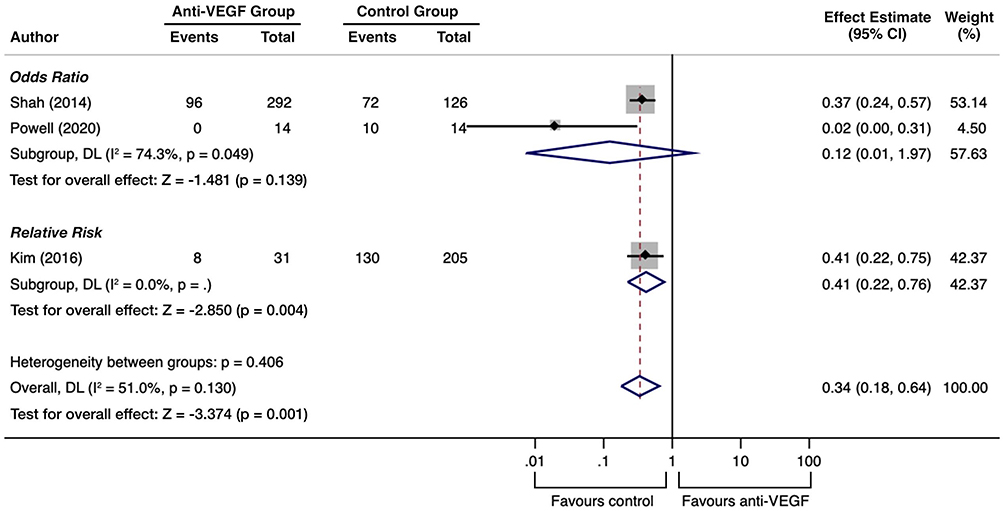 |
Figure 4 Forest plot for risk of moderate vision loss following prophylactic anti-VEGF. |
 |
Figure 5 Forest plot for risk of good final VA following prophylactic anti-VEGF. |
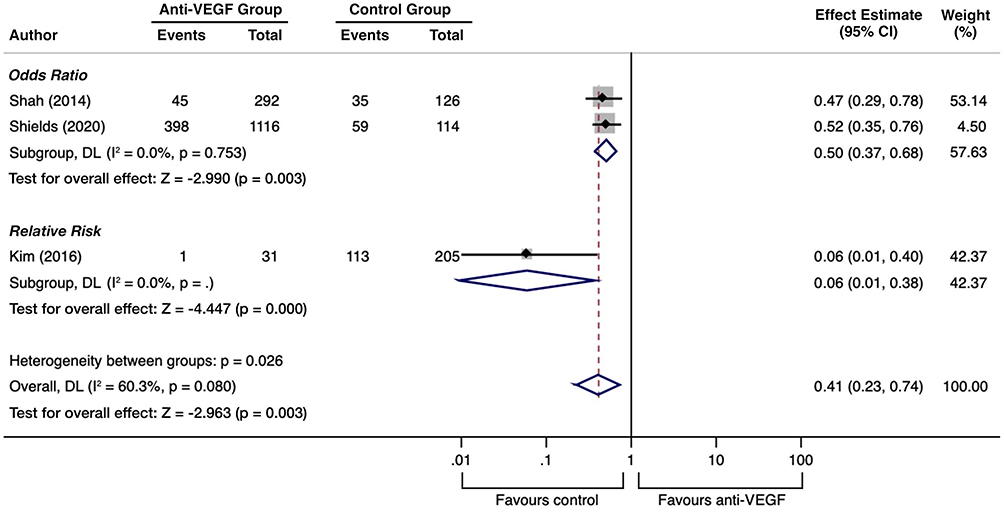 |
Figure 6 Forest plot for risk of poor final VA following prophylactic anti-VEGF. |
Discussion
Our meta-analysis included one clinical trial and three observational studies that investigated the effects of prophylactic intravitreal anti-VEGF in individuals at high risk of radiation-induced vision loss. As the included studies had different effect estimates, we used only the pooled OR, which was presented in more than one study, to draw conclusions for each outcome.
The results of this review demonstrated that preventive anti-VEGF therapy significantly reduced the events of RM, RON, and poor final VA in high-risk patients compared to observation alone. Higher reductions were noted for RM (50%; 95% CI, 26–66%) and poor final VA (50%; 95% CI, 32–63%), whereas the reduction rate for RON was 38% (95% CI 10–58%). However, the certainty of evidence for these outcomes was low (Table 4) because of the nature of the observational study and the lack of large effects, dose responses, opposing residual confounders, and other biases.
 |
Table 4 Summary of Certainty of Evidence Using GRADE Approach |
We also showed that although moderate vision loss was likely to be experienced by the control group and a good final VA was likely to be found in the intervention group, the difference was not significant (Table 4). This finding may be explained by the small sample size in one of the included studies (Powell’s study had only 28 subjects in total19), which caused the CI to be wide and the statistical heterogeneity to be large. Moreover, some degree of clinical heterogeneity should be noted since most studies used different drug types and doses, as well as frequency of therapy. Only Shah et al and Shields et al conducted their studies in a similar manner: IVB injections 1.25–1.5 mg every 4 months for 24 months. Subgroup analysis of different clinical protocols was not performed due to the limited number of studies, but it can be seen that when comparing the results between Shah’s study18 and Shields’ study,20 the CI of each outcome overlapped. With such a high degree of imprecision and inconsistency, the certainty of outcomes is downgraded. Given that the strength of the evidence is very low, it is unclear whether prophylactic anti-VEGF can prevent substantial vision loss and preserve the initial good VA.
Our findings are consistent with those of a previous systematic review by Fallico et al (2021).21 While their review examines all therapeutic options for the treatment and prevention of RM, our review focuses on the use of anti-VEGF as prophylaxis and adds valuable analysis on the cumulative effect of each clinically important outcomes in hopes to draw conclusions and make clinical evidence-based recommendations. Moreover, previous early studies using anti-VEGF as treatment for RM and RON agree with our findings with respect to the regression of radiation-induced vasculopathy (ie edema, hemorrhage, and neovascularization) and the absence of adverse effects related to repetitive injections.4,5,22,23 Other prospective studies also consistently reported that the majority of patients with RR had better mean BCVA and central macular thickness (CMT) after treatment with anti-VEGF.24–26
However, in a subset of patients, their VA still worsens despite adequate therapy. Even though we could not determine these findings, it appears that the visual response of RM to anti-VEGF may decline as the baseline condition deteriorates, similar to that of diabetic macular edema.27 Matet et al (2017) revealed that vision loss in RM may be influenced not only by retinal anatomical factors but primarily by microvascular factors, including foveal avascular zone (FAZ) area and retinal vascular density (VD).28 Cennamo et al (2020) also reported that when starting a monthly IVR for patients with RM, there was a thinning in CMT but no significant improvement in FAZ area, retinal VD, and BCVA.29 Given that anti-VEGF agent acts on the vascular permeability and affects the retinal exudation rather than the vascular blood flow, it may fail to improve the injured retinal vascular network, which translates into VA stabilization. This finding suggests that those with advanced disease (ie FAZ area has enlarged and/or retinal VD has decreased due to retinal ischemia following radiotherapy) are more likely to tolerate treatment compared to those with early stage. Hence, both retention of initial good VA and reduction of vision loss should theoretically be achieved in high-risk patients who receive early preventive therapy.
Evidence that prophylactic anti-VEGF may preserve vision from RM and RON should be carefully implemented as it has a low level of certainty and is currently limited to the United States. Based on this review, the recommended protocol for RR prevention is IVB injections of 1.25–1.5 mg every four months for a minimum of 24 months. However, to date, the use of anti-VEGF as prophylaxis for RR is still off-label, with no coverage from medical insurance. In addition to financial burden, multiple office visits per year may significantly lower patient compliance. It should also be emphasized that not only periodic injections are required for the effect to occur but also the existing therapies are aimed at preventing disease deterioration, not restoring the full visual function. Therefore, a clear discussion with patients addressing the current state of treatment and their visual goals is imperative because RR is almost always unilateral and progressive despite adequate therapy.
Our meta-analysis has some limitations. First, all studies had at least a moderate risk of bias due to the use of historical controls and lack of randomization and blinding. Second, the global generalizability of the results is still questionable since all studies were performed in the United States. Third, the certainty of each outcome was low to very low because the included studies were mostly observational, had small sample sizes, and were prone to bias. Given that the use of prophylactic anti-VEGF has only been studied for a decade, it is reasonable that currently available studies are limited. Therefore, multicenter, double-blind, randomized, placebo-controlled clinical trials with relatively long follow-up period and adequate sample size are warranted. However, the need for a control group to receive sham therapy may inhibit participant enrolment and study feasibility.
Conclusion
RR begins subclinically, progresses continuously (despite adequate treatment) and eventually causes irreversible loss of vision. This meta-analysis shows that IVB injections of 1.25–1.5 mg every 4 months for a minimum of 24 months are safe and may delay the development of RM and RON in high-risk patients. The amount of VA retained remains uncertain; however, after 2 years of prophylactic anti-VEGF, the risk of BCVA less than or equal to 20/200 may be reduced by approximately 50%.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest or financial support for this study. Ethical approval was not required for this study.
References
1. Melia M, Moy CS, Reynolds SM, et al. Quality of life after iodine 125 brachytherapy vs enucleation for choroidal melanoma: 5-year results from the Collaborative Ocular Melanoma Study: COMS QOLS Report No. 3. Arch Ophthalmol. 2006;124(2):226–238.
2. Groenewald C, Konstantinidis L, Damato B. Effects of radiotherapy on uveal melanomas and adjacent tissues. Eye. 2013;27(2):163–171. doi:10.1038/eye.2012.249
3. Melia BM, Abramson DH, Albert DM, et al. Collaborative ocular melanoma study (COMS) randomized trial of I-125 brachytherapy for medium choroidal melanoma. I. Visual acuity after 3 years COMS report no. Ophthalmology. 2001;108(2):348–366.
4. Finger PT, Chin K. Anti-vascular endothelial growth factor bevacizumab (Avastin) for radiation retinopathy. Arch Ophthalmol. 2007;125(6):751–756. doi:10.1001/archopht.125.6.751
5. Finger PT. Anti-VEGF bevacizumab (Avastin) for radiation optic neuropathy. Am J Ophthalmol. 2007;143(2):335–338. doi:10.1016/j.ajo.2006.09.014
6. Finger PT, Chin KJ, Semenova EA. Intravitreal anti-VEGF therapy for macular radiation retinopathy: a 10-year study. Eur J Ophthalmol. 2015;26(1):60–66. doi:10.5301/ejo.5000670
7. Shields CL, Say EA, Samara WA, Khoo CT, Mashayekhi A, Shields JA. Optical coherence tomography angiography of the macula after plaque radiotherapy of choroidal melanoma: comparison of irradiated versus nonirradiated eyes in 65 patients. Retina. 2016;36(8):1493–1505. doi:10.1097/IAE.0000000000001021
8. Skalet AH, Liu L, Binder C, et al. Longitudinal detection of radiation-induced peripapillary and macular retinal capillary ischemia using OCT angiography. Ophthalmol Retina. 2020;4(3):320–326. doi:10.1016/j.oret.2019.10.001
9. Fam A, Tomar AS, Finger PT. OCT-A evaluation of radiation vasculopathy following slotted plaque brachytherapy. Eur J Ophthalmol. 2022;32(4):2459–2568. doi:10.1177/11206721211044339
10. Finger PT, Chin KJ, Yu GP. Risk factors for radiation maculopathy after ophthalmic plaque radiation for choroidal melanoma. Am J Ophthalmol. 2010;149(4):608–615. doi:10.1016/j.ajo.2009.11.006
11. Finger PT. Tumour location affects the incidence of cataract and retinopathy after ophthalmic plaque radiation therapy. Br J Ophthalmol. 2000;84(9):1068–1070. doi:10.1136/bjo.84.9.1068
12. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
13. Joussen AM, Lehmacher W, Hilgers RD, Kirchhof B. Is significant relevant? Validity and patient benefit of randomized controlled clinical trials on age-related macular degeneration. Surv Ophthalmol. 2007;52(3):266–278. doi:10.1016/j.survophthal.2007.02.010
14. Gregori NZ, Feuer W, Rosenfeld PJ. Novel method for analyzing Snellen visual acuity measurements. Retina. 2010;30(7):1046–1050. doi:10.1097/IAE.0b013e3181d87e04
15. Sterne JAC, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi:10.1136/bmj.i4919
16. Yang X, Dalvin LA, Mazloumi M, et al. Impact of uveal melanoma thickness on post-plaque radiotherapy outcomes in the prophylactic anti-vascular endothelial growth factor era in 1131 patients. Clin Exp Ophthalmol. 2020;48(5):610–623. doi:10.1111/ceo.13758
17. Kim IK, Lane AM, Jain P, Awh C, Gragoudas ES. Ranibizumab for the prevention of radiation complications in patients treated with proton beam irradiation for choroidal melanoma (An American ophthalmological society thesis). Trans Am Ophthalmol Soc. 2016;114.
18. Shah SU, Shields CL, Bianciotto CG, et al. Intravitreal bevacizumab at 4-month intervals for prevention of macular edema after plaque radiotherapy of uveal melanoma. Ophthalmology. 2014;121(1):269–275. doi:10.1016/j.ophtha.2013.08.039
19. Powell BE, Finger PT. Anti–VEGF therapy immediately after plaque radiation therapy prevents or delays radiation maculopathy. Ophthalmol Retina. 2020;4(5):547–550. doi:10.1016/j.oret.2020.01.010
20. Shields CL, Dalvin LA, Chang M, et al. Visual outcome at 4 years following plaque radiotherapy and prophylactic intravitreal bevacizumab (every 4 months for 2 years) for uveal melanoma: comparison with nonrandomized historical control individuals. JAMA Ophthalmol. 2020;138(2):136–146. doi:10.1001/jamaophthalmol.2019.5132
21. Fallico M, Chronopoulos A, Schutz JS, Reibaldi M. Treatment of radiation maculopathy and radiation-induced macular edema: a systematic review. Surv Ophthalmol. 2021;66(3):441–460. doi:10.1016/j.survophthal.2020.08.007
22. Finger PT. Radiation retinopathy is treatable with anti-vascular endothelial growth factor bevacizumab (Avastin). Int J Radiat Oncol Biol Phys. 2008;70(4):974–977. doi:10.1016/j.ijrobp.2007.11.045
23. Finger PT, Chin KJ. Intravitreous ranibizumab (Lucentis) for radiation maculopathy. Arch Ophthalmol. 2010;128(2):249–252. doi:10.1001/archophthalmol.2009.376
24. Finger PT, Chin KJ. High-dose (2.0 mg) intravitreal ranibizumab for recalcitrant radiation retinopathy. Eur J Ophthalmol. 2013;23(6):850–856. doi:10.5301/ejo.5000333
25. Fallico M, Reibaldi M, Avitabile T, et al. Intravitreal aflibercept for the treatment of radiation-induced macular edema after ruthenium 106 plaque radiotherapy for choroidal melanoma. Graefes Arch Clin Exp Ophthalmol. 2019;257(7):1547–1554. doi:10.1007/s00417-019-04347-6
26. Murray TG, Latiff A, Villegas VM, Gold AS. Aflibercept for radiation maculopathy study: a prospective, randomized clinical study. Ophthalmol Retina. 2019;3(7):561–566. doi:10.1016/j.oret.2019.02.009
27. Elnahry AG, Noureldine AM, Abdel-Kader AA, Sorour OA, Ramsey DJ. Optical coherence tomography angiography biomarkers predict anatomical response to bevacizumab in diabetic macular edema. Diabetes Metab Syndr Obes. 2022;15:395–405. doi:10.2147/DMSO.S351618
28. Matet A, Daruich A, Zografos L. Radiation maculopathy after proton beam therapy for uveal melanoma: optical coherence tomography angiography alterations influencing visual acuity. Invest Ophthalmol Vis Sci. 2017;58(10):3851–3861. doi:10.1167/iovs.17-22324
29. Cennamo G, Montorio D, Bernardo R, et al. Retinal vascular changes in radiation maculopathy after intravitreal ranibizumab by optical coherence tomography angiography. J Clin Med. 2020;9(6):1618. doi:10.3390/jcm9061618
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.