Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Efficacy of Oxybrasion and Cosmetic Acids on Selected Skin Parameters in the Treatment with Acne Vulgaris
Authors Chilicka K ![]() , Rusztowicz M, Rogowska AM
, Rusztowicz M, Rogowska AM ![]() , Szyguła R, Nowicka D
, Szyguła R, Nowicka D
Received 10 March 2023
Accepted for publication 5 May 2023
Published 19 May 2023 Volume 2023:16 Pages 1309—1317
DOI https://doi.org/10.2147/CCID.S407976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Karolina Chilicka,1 Monika Rusztowicz,1 Aleksandra M Rogowska,2 Renata Szyguła,1 Danuta Nowicka3
1Department of Health Sciences, Institute of Health Sciences, University of Opole, Opole, Poland; 2Department of Social Sciences, Institute of Psychology, University of Opole, Opole, Poland; 3Department of Dermatology, Venereology and Allergology, Wrocław Medical University, Wrocław, Poland
Correspondence: Karolina Chilicka, Department of Health Sciences, Institute of Health Sciences, University of Opole, Katowicka 68 Street, Opole, 45-040, Poland, Tel +48665439443, Email [email protected]
Purpose: The present study aimed to evaluate the efficacy of an oxybrasion treatment applied alone and an oxybrasion treatment combined with cosmetic acids in improving acne-prone skin and selected skin parameters.
Patients and Methods: A single-blind placebo study in a sample of 44 women diagnosed with acne vulgaris was conducted. Group A (n = 22) had a series of five oxybrasion treatments, while group B (n = 22) received a synergy of five oxybrasion treatments and a mixture of phytic, pyruvic, and lactic and lactic ferulic acids at 40% pH 1.4. Cosmetic treatments were performed every 14 days, and The Derma Unit SCC3 apparatus (Courage & Khazaka, Cologne, Germany) Sebumeter SM 815 and Corneometer CM825 and GAGS scale were used to check their effectiveness.
Results: A Bonferroni post hoc test showed that group A and B did not differ from each other in acne severity before treatment (p = 1.00). However, these samples differed significantly after treatment (p < 0.001), suggesting that combined treatment of oxybrasion and cosmetic acids has a better effect than oxybrasion alone. Also, two treatment conditions (before and after) were statistically different for groups A and B separately (p < 0.001), indicating a similar efficacy of both treatments on acne severity.
Conclusion: Cosmetic treatments improved acne-prone skin and selected skin parameters. Better results were obtained by combining an oxybrasion treatment with cosmetic acids.
Clinical Trial Approval: The clinical trial with ID ISRCTN 28257448 approved this study.
Keywords: acne vulgaris, oxybrasion, cosmetic acids, sebumeter, corneometer
Introduction
Acne vulgaris is one of the most common skin conditions worldwide. It affects approximately 85% of people between 12 and 25, with moderate-to-severe cases accounting for 15–25%.1 Acne is caused by excessive sebaceous gland function, triggered by androgen hormones. These hormones contribute to increased sebum secretion. Another cause is a disturbance in the keratinization process of the sebaceous gland ducts. It leads to a narrowing of the sebaceous ducts, which clogs them and prevents sebum from reaching the skin surface properly. This promotes the formation of micro-blackheads and, later on, open and closed comedones, which give rise to other skin lesions such as pimples and papules. Other causes leading to the formation of the disease mentioned above include colonization of the sebaceous glands by Cutibacterium acnes, inflammation, and a hereditary factor. Factors that exacerbate acne lesions are a glycaemic diet, products with a high glycaemic index, fatty and spicy foods, and chocolate or dairy products.2–7
Cosmetology has developed remarkably in the last decade, with new treatments using active substances and modern cosmetic equipment. One such treatment is oxybrasion, which exfoliates dead skin and improves blood circulation. The procedure uses saline ejected under pressure from a special manipulator. As demonstrated by Chilicka et al,8 oxybrasion treatments reduce inflammation and also reduce sebum from the epidermal surface in people with acne vulgaris. When performing any cosmetology treatments for people with acne skin, photoprotection is extremely important, which will protect against the formation of discoloration and skin irritation.
The oxybrasion treatment is a relatively new procedure but significantly exfoliates the dead epidermis. Therefore, the authors decided to conduct research using the procedure mentioned above. In addition, using a mix of cosmetic acids with exfoliating, seboregulating, and anti-inflammatory properties seems to be an extremely promising solution for acne skin. The researchers decided to check whether the oxybrasion treatment and the combined oxybrasion treatment with acids would have good results in reducing skin eruptions and improving acne skin. The oxybrasion treatment exfoliates the dead epidermis, enabling faster penetration of cosmetic acids into the skin. Researchers decided to use a new method, which is oxybrasion, as well as the synergy of oxybrasion with an acid treatment that is already known. Many other researchers have shown excellent results when it comes to acne skin. It should be emphasized that a cosmetologist is a person whose task is not to treat but to care for the skin. Therefore, treatments were selected, aiming to care for acne skin by exfoliating dead epidermis. It is one of the most important skin care elements with eruptions such as blackheads, pustules, or papules. The treatments mentioned above are non-invasive. Both oxybrasion and acid mix does not affect the continuity of the skin. After the procedure, it is possible to return to normal functioning and activities of daily living. Cosmetic acids cause exfoliation of the dead epidermis, thanks to which the skin pores are cleansed, the incidence of inflammatory skin eruptions is reduced, and the secreted sebum is reduced on the surface of the epidermis. The acids most commonly used for acne skin include ferulic, azelaic, mandelic, glycolic, salicylic, pyruvic, lactic, and phytic acids.9–11
Materials and Methods
Study Design
A single-blind placebo study with follow-up was conducted at the Institute of Health Sciences of the University of Opole, Poland, from October 2022 to January 2023. The research was approved by the Human Research Ethics Committee at the Opole Medical School (No. KB/57/NOZ/2019) and conducted according to the principles of the Declaration of Helsinki. The study was registered at https://www.isrctn.com (No. ISRCTN 28257448) and accessed on 7th May 2020.
Participants signed a consent form before taking part in the study. They also consented to publish the facial photographs before the treatment series and after the study. In addition, they were informed about how the treatment would be carried out and knew they could withdraw from further participation in the study without giving a reason.
Fifty-five women were enrolled in the study, but due to exclusion criteria, 11 were rejected at the initial stage (Figure 1). No men entered the study, so the group was homogeneous. The 44 young women with clinician-diagnosed acne vulgaris were randomly divided into groups A or B. Group A had five oxybrasion treatments performed using 0.9% NaCl. Group B had five oxybrasion treatments (0.9% NaCl), and after drying the skin, a mixture of cosmetic acids (phytic, pyruvic, lactic, and ferulic acids 40% pH 1.4) was applied. The acids that were used were purchased from a cosmetics wholesaler and were from Apis Natural Cosmetics. The INCI of the acids was as follows: aqua, phytic acid, pyruvic acid, lactic acid, xanthan gum, sodium hydroxide, and phenoxyethanol. Intervals between treatments were 14 days. Subjects were informed that they could not undergo any other cosmetic or aesthetic treatments for the entire study duration. The use of cosmetics, as well as sebum-reducing dietary supplements, was prohibited. The use of cosmetics such as Cetaphil MD Dermoprotector, micellar water, SPF 50 cream, and Alantan Plus cream was recommended throughout the study period so that each subject had the same home care.
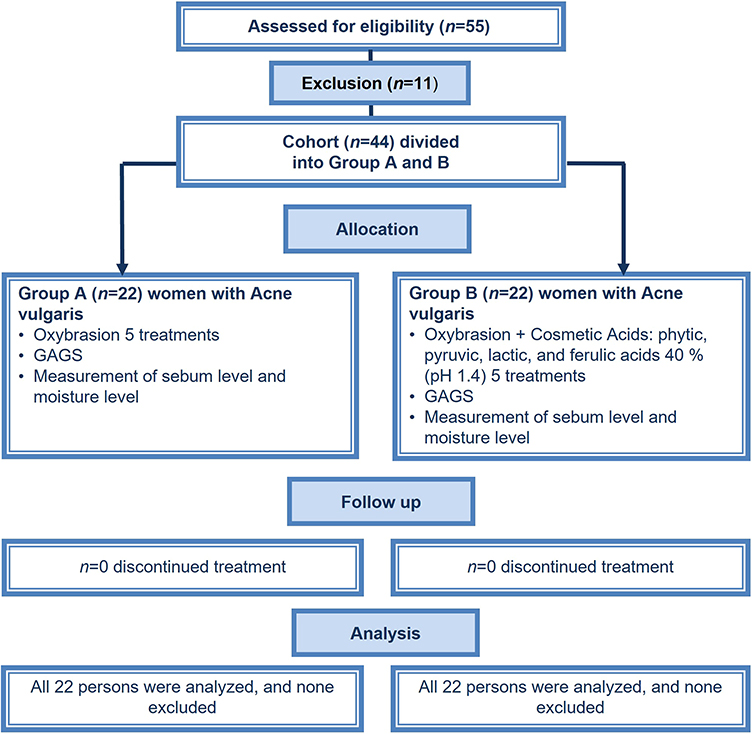 |
Figure 1 Participants follow in the study. |
Participants
Initially, 55 women were enrolled in the study, but after checking the exclusion criteria, 11 were excluded (9 due to recurrent sinusitis, and 2 had tanned skin). Forty-four women aged 20–21 (M = 20.55, SD = 0.50) diagnosed by a dermatologist with mild acne vulgaris using GAGS were included in the study.
The same rater dermatologist also used GAGS after finishing a series of cosmetic treatments. The mean disease duration was 7 years (M = 7.11, SD = 0.78). Inclusion criteria were as follows: age 19–22, mild acne on the GAGS scale, no use of hormonal contraception, no dermatological treatment for acne in the last 12 months, no supplementation with yeast tablets, sulfur, and use of herbal teas to reduce sebum production. The exclusion criteria for group A were as follows: claustrophobia, skin irritation, pregnancy, breastfeeding, isotretinoin within the last year, taking contraceptives, taking antibiotics within the last 6 months, tanned skin, skin cancers, viral, bacterial and fungal skin diseases, eczema, psoriasis, the tendency to having sinusitis, atopic dermatitis, rosacea, active inflammation, and skin damage. The exclusion criteria for group B were the same as group A plus numerous telangiectasias, melanocytic nevi, active herpes, reduced immunity, allergy to peeling ingredients, active rosacea, autoimmune diseases (pemphigus, collagenosis), severe acne and propensity to keloids. In addition, women with increased sebum on the epidermal surface (above 100 μg/cm2) were also included in the study.
Measures
Acne Vulgaris
The Global Acne Grading System (GAGS) was used to check the severity of acne vulgaris in 44 patients. This scale was used to determine the degree of acne and to check whether the treatments improved the skin. The scale includes the following areas: nose, cheeks, forehead, chin, as well as the back and chest. Each is assigned a number based on size: nose = 1; left cheek = 2; right cheek = 2; forehead = 2; chin = 1; and back and chest = 3. Depending on the severity, each lesion is graded: no cutaneous conditions—0, comedones—1, papules—2, pustules—3, and nodules—4. The local score calculated for each area has the following formula: Local score = factor × Grade (0–4). The global score is composed of the local results: 1–18—mild acne, 19–30—moderate acne, 31–38—severe acne, and above 39—acne with a very severe course.12 GAGS was determined twice: before and after a series of cosmetic treatments (30 days after finishing the last treatment).
Skin Parameters
Skin parameters were measured using a Derma Unit SCC3 (Courage & Khazaka, Cologne, Germany). Moisture was measured using a Corneometer CM 825, and sebum was measured using a Sebumeter SM 815. The measurement points were as follows: the forehead, nose tip, and chin. Measurements were taken before the treatment series and 30 days after the last treatment. The participants were informed in advance on how to prepare for the measurements. They were all asked to remove their facial makeup in the evening the day before the study and not to apply any skincare products such as creams, masks, serums, etc. After waking up, washing the face and applying cosmetic preparations and makeup to the face were prohibited in the morning. In addition, wiping the face with tissues, cotton wool, or paper towels was prohibited. Breaking the above procedures would lead to significant differences in measurements in the subjects. Measurements were taken by 10 am, and the subjects acclimatized to the room for 30 minutes upon arrival. Room humidity was 40–50%, and the temperature was 20–21°C.
Treatment Procedure
An oxybrasion device was used in the treatment. The device did not have an additional container of pure oxygen, so the oxygen generated by the device from the air did not affect reducing skin eruptions. The treatment used 0.9% NaCl ejected under pressure from the device. Initially, both groups A and B removed makeup using micellar fluid, and the skin was toned. After preparing the patients previously, performing makeup removal, and protecting the eyes with cotton pads and rubber goggles, group A had an oxybrasion treatment using only 0.9% NaCl at a pressure of 4 bar. The distance of the manipulator from the face was 2–3 cm, and the treatment length was always 5 minutes. After the treatment, the face was dried, and a cream with SPF 50 was applied. The treatment was repeated every 2 weeks, and the number in the series was five treatments. Group B also had an oxybrasion treatment (same treatment algorithm as group A). However, after the treatment, the face was dried and wiped using cotton wool soaked in pre-peel cleanser and pre-peel lotion. The corners of the eyes, the wings of the nose, and the lips were protected with Vaseline. Water-soaked cotton pads were applied to the eyes to protect them. Then, using a cotton bud, a mixture of cosmetic acids (phytic, pyruvic, lactic, and ferulic acids 40% pH 1.4) was applied to the entire face for 2 minutes for the first treatment. With each subsequent treatment, the period of acid exposure on the skin was extended by 25 seconds. At the end of the specified time, the neutralizing gel was applied to the entire face and washed off after 1 minute with cotton swabs soaked in cold water. Washing was repeated several times to wash off residual acid and neutralize the gel properly. At the end of the treatment, a cream with SPF 50 was applied to the whole treatment area.
For home care, Cetaphil MD Dermoprotector facial cleansing gel was recommended for each subject, as well as micellar lotion, SPF 50 sunscreen, and Alantan Plus cream. Any other cosmetic or aesthetic treatments were prohibited during the complete treatment series and 1 month after completion (until the second measurement).
Statistical Analysis
Descriptive statistics were performed initially, including mean (M), standard deviation (SD), median (Mdn), skewness, kurtosis, and Shapiro–Wilk test of normality, to check the parametric properties of the severity of acne (GAGS scores), and face moisturizing and greasing (forehead, nose, and chin), considering both treatment conditions (before and after). The scores were compared between groups A (oxybrasion) and B (oxybrasion and cosmetic acids). Since age and acne duration did not meet the assumption of a normal data distribution, a non-parametric Mann–Whitney U-test was used to compare the groups. A repeated measures 2 (Treatment: After Before) × 2 (Group: A, B) one-way ANOVA was performed to examine the effect of oxybrasion and acid cosmetic treatment on the acne severity (GAGS scores) and two parameters of face skin: moisturizing and greasing. The Bonferroni post hoc tests were applied to check a statistically significant difference. The effect size was assessed using η²p (with a 0.01 value interpreted as small, 0.06 as a medium, and above 0.14 as a large effect size). All statistics were performed using JASP software for Windows (JASP Team, Version 0.14.1, Computer software; Amsterdam, The Netherlands: Department of Psychological Methods, University of Amsterdam; 2020).
Results
Changes in Acne Severity After Oxybrasion and Oxybrasion with Cosmetic Acids
Preliminary, groups A and B were compared in terms of age, acne years, and acne severity before treatment. The Mann–Whitney U-test showed no differences in age (U = 242, p = 1.000) and acne duration (U = 279, p = 0.354) between samples A and B. Next, acne severity was measured in groups A and B before and after treatment, using repeated measures of one-way ANOVA (Table 1). Statistically significant and large effects were found for the group (p = 0.003, η²p = 0.19), treatment (p < 0.001, η²p = 0.90), and interaction between group and treatment (p < 0.001, η²p = 0.26). A Bonferroni post hoc test showed that group A and B did not differ from each other in acne severity before treatment (p = 1.00). However, these samples differed significantly after treatment (p < 0.001), suggesting that combined treatment of oxybrasion and cosmetic acids has a better effect than oxybrasion alone. Also, two treatment conditions (before and after) were statistically different for groups A (Figure 2) and B (Figure 3) separately, indicating a similar efficacy of both treatments on acne severity (p < 0.001).
 |
Table 1 Repeated Measures One-Way ANOVA for Acne Severity in Groups A and B, Before and After Treatment, Using the Global Acne Grading System (GAGS) |
 |
Figure 2 Acne severity (a) before treatment and (b) after treatment of oxybrasion in group A. |
 |
Figure 3 Acne severity (a) before treatment and (b) after treatment of oxybrasion and cosmetic acids in group B. |
Changes in Facial Skin Greasing After Oxybrasion and Oxybrasion with Cosmetic Acids
Considering forehead greasing, the repeated measures one-way ANOVA showed statistically significant effects for the group (p < 0.001, η²p = 0.47), treatment (p < 0.001, η²p = 0.96), and interaction between group and treatment (p < 0.001, η²p = 0.60), as shown in Table 2. Furthermore, post hoc tests indicated that although groups A and B did not differ significantly in forehead greasing before treatment (p = 1.00), statistically significant differences (p < 0.001) were found for groups A and B separately when treatment efficacy was tested.
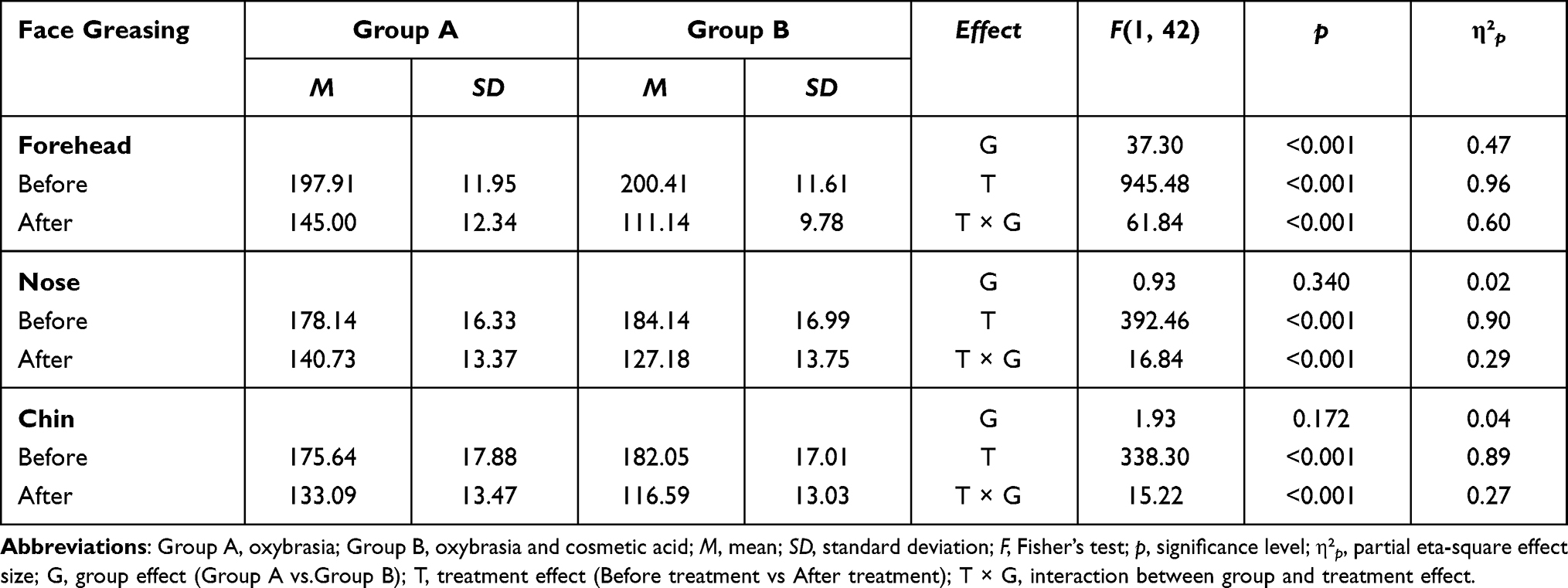 |
Table 2 Repeated Measures One-Way ANOVA for Face Greasing in Groups A and B, Before and After Treatment, Using Sebumeter SM815 (μg/cm2) |
When the greasing of the nose was analyzed (Table 2), the group effect was insignificant (p = 0.340, η²p = 0.02), showing that both types of treatment are similarly effective. However, significant effects were demonstrated for treatment (p < 0.001, η²p = 0.90) and interaction between treatment and group (p < 0.001, η²p = 0.29). Post hoc test showed that groups A and B did not differ in nose greasing before treatment (p = 1.000), but after treatment, slight group differences were found (p = 0.025). Moreover, between conditions (before and after treatment), the differences were more significant for groups A and B separately (p < 0.001).
Finally, we tested whether the treatment of oxybrasion and oxybrasion with cosmetic acids were equally effective in greasing the chin (Table 2). Significant effects were found for treatment (p < 0.001, η²p = 0.89) and interaction between group and treatment (p < 0.001, η²p = 0.27). Insignificant differences were presented for the group (p = 0.172, η²p = 0.04). However, post hoc tests showed that although chin greasing was similar between groups A and B before treatment (p = 1.000), after treatment, these differences were significant at p < 0.004. However, treatment (comparison of conditions before with after) was similarly effective for both groups A and B separately (p < 0.001).
Changes in Facial Moisture After Oxybrasion and Oxybrasion with Cosmetic Acids
Moisturizing of the forehead is not differentiated between groups A and B (Table 3), suggesting that the type of treatment is not especially important for those parts of the face (p = 0.746, η²p = 0.00). Also, the interaction effect was insignificant (p = 0.378, η²p = 0.02). However, the treatment was effective for participants in the study (p < 0.001, η²p = 0.59), with a large effect size. Furthermore, post hoc tests showed that groups A and B did not differ in moisturizing the forehead in both conditions before (p = 1.000) and after treatment (p = 1.000). In contrast, treatment was similarly effective for groups A and B (p < 0.001) if considered separately.
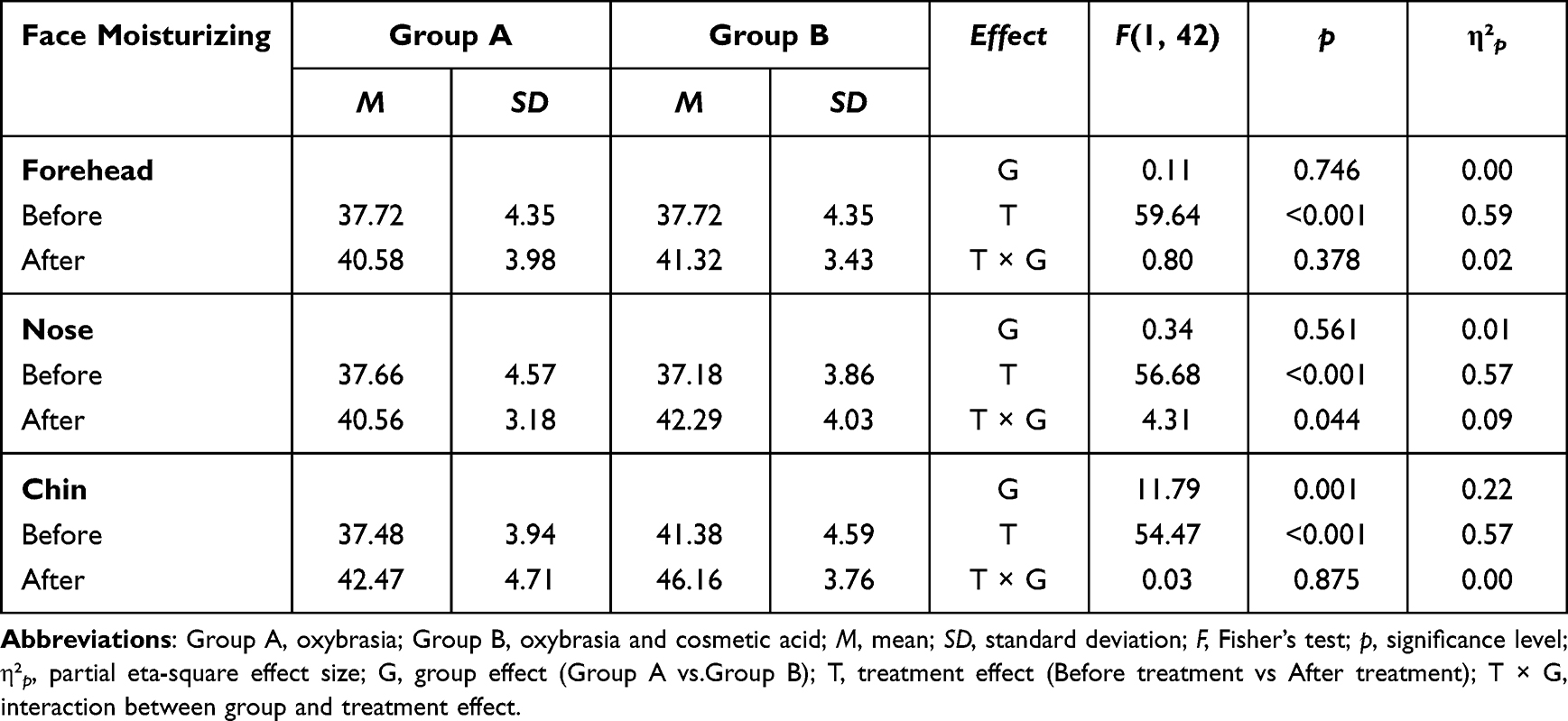 |
Table 3 Repeated Measures One-Way ANOVA for Face Moisturizing in Groups A and B, Before and After Treatment, Using Corneometer CM825 (g/m2) |
A group effect for nose moisturizing was insignificant (p = 0.561, η²p = 0.01), as shown in Table 3. However, a significant and large effect was found for the treatment (p < 0.001, η²p = 0.57). Also, the medium interaction effect was presented between the treatment and group (p < 0.001, η²p = 0.09). As suggested by post hoc tests, the nose in both groups was equally moisturized before treatment (p = 1.000) and after treatment (p = 0.907). However, moisturizing of the nose improved in group A (p = 0.002) and B (p < 0.001) separately, under the influence of treatment.
Significant and large effects of the group (p = 0.001, η²p = 0.22) and treatment (p < 0.001, η²p = 0.57) were presented for chin moisturizing in the study (Table 3). However, the interaction between treatment and group was not found (p = 0.875, η²p = 0.00). When post hoc tests were checked, group A slightly differed from group B before (p = 0.021) and after treatment (p = 0.033) in chin moisturizing. However, treatment similarly improved chin moisturizing in both groups (p < 0.001).
Discussion
Appropriate acne skin care is a crucial element that anyone suffering from this condition should pay more attention to. If inadequate cosmetics are incorporated into the daily routine (too much drying of the skin, clogging the skin pores), this can cause additional worsening of the skin condition. A well-qualified cosmetologist will properly educate on how to take care of this type of skin and suggest exfoliating treatments that will have good results in reducing skin lesions and improving skin parameters such as skin moisture, pH, and greasing.9
Pyruvic acid (PA, CH3–CO–COOH) is an α-keto-acid that has recently gained significant attention because of its various keratolytic, antimicrobial, and sebostatic properties as its ability to stimulate the formation of new collagen and elastic fibers. Phytic acid prevents the formation of discolorations and reduces the existing ones, brightens and whitens the skin, has a gentle exfoliating effect, regulates sebum secretion, moisturizes, and makes the skin smooth, elastic, and firm. Lactic acid affects the hydration and hydration of the skin, maintaining the correct moisture level in the epidermis. This action makes the skin soft, smooth, and radiant. Ferulic acid is a strong antioxidant, stimulates the synthesis of elastin and collagen fibers, has anti-inflammatory properties, eliminates erythema and redness, prevents the formation of discolorations, reduces existing ones, and optimally moisturizes the skin.13,14
In the study, Rusztowicz et al showed the positive effect of cosmetic treatments on acne-prone skin. Four treatments were performed on patients: on the left side of the face, only 40% pyruvic acid was applied, and on the right side of the face, microdermabrasion was performed, followed by the application of the same acid as on the left side. The study was designed to investigate whether the synergy of the treatments would have a better effect on the reduction of skin eruptions and selected facial skin parameters. After the entire treatment series, it was observed that microdermabrasion combined with pyruvic acid led to better results with increased hydration and reduced sebum secretion than using only the pyruvic acid treatment.15
Chilicka et al16 in a study using equipment for hydrogen purification and the mixture of cosmetic acids showed that hydrogen purification alone and combining this treatment with acids improved the patients’ skin condition. However, the combined treatments showed better results in reducing skin eruptions and improving hydration or reducing sebum from the epidermal surface.
Other equipment treatments such as intensive pulsing light and LED also have a good effect on acne skin and are often used.17–19 Lasers have also been widely used in dermatology, and several researchers have shown their positive effects on reducing skin lesions. Kwon et al used a 1450 nm diode laser in 24 Korean patients with acne. The study was randomized with facial division and lasted 20 weeks (three treatments at four-week intervals). The study showed that the laser effectively treated acne and reduced seborrhoea.20 Kang et al used a fractional laser with a combination of 589 nm and 1319 nm wavelengths. Nine patients underwent four treatments at 2- to 3-week intervals. Each patient received one pass with the 1319 nm laser and a pass with the 589 nm laser, only on a randomly selected side of the face. The study showed that the treatment was effective in people with moderate-to-severe acne. Kang et al used a fractional laser with a combination of 589 nm and 1319 nm wavelengths. Nine people underwent four treatments at 2–3-week intervals. Each patient underwent one pass with the 1319 nm laser and one pass with the 589 nm laser, only on a randomly selected side of the face. The study showed that the treatment was effective in people with moderate-to-severe acne.21
Chilicka et al8 conducted a study where group A (experimental) received the appropriate oxybrasion treatment using 0.9% sodium chloride solution and pure oxygen from a cylinder. Group B (placebo) had a “mock oxybrasion” procedure using still mineral water and oxygen from the compressor from the device (oxygen from the air). Patients from group B were unaware that they were a placebo group, and they were convinced that they were undergoing the procedure of oxybrasion. This study showed that the procedure performed in group A (experimental) contributed to a significant reduction in the number of skin eruptions (GAGS scale) and improved skin appearance in patients in this group.
Limitations
In the future, we would also like to conduct a study on a group of men. Other measurements could be included in the study, such as the skin’s pH or the amount of porphyrins on the epidermal surface. In addition, other types of cosmetic acids could be used to see if they would show even better treatment effects than those used in this study.
Conclusion
Treatment with oxybrasion and cosmetic acids is a safe cosmetic procedure. In both groups A and B, there was an improvement in skin parameters, namely a reduction in the amount of sebum on the epidermal surface, as well as an increase in skin hydration. The treatment procedures are straightforward and do not exclude patients from daily life or cause skin irritation or redness. However, a comparison of groups A and B showed that the synergy of the treatments and the use of oxybrasion and cosmetic acids produced better results in improving skin parameters. It should be remembered that cosmetic treatments cannot replace dermatological treatment; they are only part of acne skin care.
Data Sharing Statement
Data supporting this study’s findings are available from the corresponding author upon reasonable request. However, the data are not publicly available due to privacy or ethical restrictions.
Ethics
This study was conducted following the principles of the Declaration of Helsinki. All patients provided informed written consent before the study commencement. The Opole Medical School approved the protocol (No. KB/57/NOZ/2019).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Leung AK, Barankin B, Lam JM, et al. Dermatology: how to manage acne vulgaris. Drugs Context. 2021;10:8–16. doi:10.7573/dic.2021-8-6
2. Tan JK, Bhate K. A global perspective on the epidemiology of acne. Br J Dermatol. 2015;172(Suppl 1):3–12. doi:10.1111/bjd.13462
3. Thiboutot D, Dréno B, Sanders V, et al. Changes in the management of acne: 2009–2019. J Am Acad Dermatol. 2020;82(5):1268–1269. doi:10.1016/j.jaad.2019.04.012
4. Dall’Oglio F, Nasca MR, Fiorentini F, et al. Diet and acne: review of the evidence from 2009 to 2020. Int J Dermatol. 2021;60(6):672–685. doi:10.1111/ijd.15390
5. Baldwin H, Tan J. Effects of diet on acne and its response to treatment. Am J Clin Dermatol. 2021;22(1):55–65. doi:10.1007/s40257-020-00542-y
6. Proença AC, Â L, Duarte AP, Di Sotto A. The role of herbal medicine in the treatment of acne vulgaris: a systematic review of clinical trials. Evid Based Complement Alternat Med. 2022;2022:2011945. doi:10.1155/2022/2011945
7. Tobiasz A, Nowicka D, Szepietowski JC. Acne vulgaris-novel treatment options and factors affecting therapy adherence: a narrative review. J Clin Med. 2022;11(24):7535. doi:10.3390/jcm11247535
8. Chilicka K, Rogowska AM, Szyguła R, et al. Efficacy of oxybrasion in the treatment of acne vulgaris: a preliminary report. J Clin Med. 2022;11(13):3824. doi:10.3390/jcm11133824
9. Chilicka K, Rogowska AM, Szyguła R, et al. A comparison of the effectiveness of azelaic and pyruvic acid peels in the treatment of female adult acne: a randomized controlled trial. Sci Rep. 2020;10(1):12612. doi:10.1038/s41598-020-69530-w
10. Zdrada J, Odrzywołek W, Deda A, et al. A split-face comparative study to evaluate the efficacy of 50% pyruvic acid against a mixture of glycolic and salicylic acids in the treatment of acne vulgaris. J Cosmet Dermatol. 2020;19(9):2352–2358. doi:10.1111/jocd.13288
11. Adamski Z, Gornowicz-Porowska J, Sobkowska D, et al. Acne – therapeutic challenges to the cooperation between a dermatologist and a cosmetologist. Postep Dermatol Alergol. 2021;38:21–31. doi:10.5114/ada.2021.104273
12. Adityan B, Kumari R, Thappa DM. Scoring systems in acne vulgaris. Indian J Dermatol Venereol Leprol. 2009;75:324–326.
13. Hofmeister H. Superficial and medium-depth chemical peels. In: Issa MCA, Tamura B, editors. Clinical Approaches and Procedures in Cosmetic Dermatology. Cham: Springer; 2018:141–151.
14. Kontochristopoulos G, Platsidaki E. Chemical peels in active acne and acne scars. Clin Dermatol. 2017;35:179–182. doi:10.1016/j.clindermatol.2016.10.011
15. Rusztowicz M, Chilicka K, Szyguła R, et al. A split face comparative study to evaluate the efficacy of 40% pyruvic acid vs. microdermabrasion with 40% pyruvic acid on biomechanical skin parameters in the treatment of acne vulgaris. J Clin Med. 2022;11(20):6079. doi:10.3390/jcm11206079
16. Chilicka K, Rusztowicz M, Rogowska AM, et al. Efficacy of hydrogen purification and cosmetic acids in the treatment of acne vulgaris: a preliminary report. J Clin Med. 2022;11(21):6269. doi:10.3390/jcm11216269
17. El-Latif AA, Hassan FA, Elshahed AR, et al. Intense pulsed light versus benzoyl peroxide 5% gel in treatment of acne vulgaris. Lasers Med Sci. 2014;29(3):1009–1015. doi:10.1007/s10103-013-1440-0
18. Mohanan S, Parveen B, Annie Malathy P, et al. Use of intense pulse light for acne vulgaris in Indian skin—a case series. Int J Dermatol. 2012;51(4):473–476. doi:10.1111/j.1365-4632.2011.05295.x
19. Kwon HH, Lee JB, Yoon JY, et al. The clinical and histological effect of home-use, combination blue-red LED phototherapy for mild-to-moderate acne vulgaris in Korean patients: a double-blind, randomized controlled trial. Br J Dermatol. 2013;168(5):1088–1094. doi:10.1111/bjd.12186
20. Kwon HH, Choi SC, Jung JY, et al. Comparison of novel dual mode vs conventional single pass of a 1450-nm diode laser in the treatment of acne vulgaris for Korean patients: a 20-week prospective, randomized, split-face study. J Cosmet Dermatol. 2018;17(6):1063–1068. doi:10.1111/jocd.12788
21. Kang A, Lyons A, Herrmann J, et al. Treatment of moderate-to-severe facial acne vulgaris with solid-state fractional 589/1319-nm laser. J Clin Aesthet Dermatol. 2019;12(3):28–31.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Plasma Treatment – Results of Skin Microbiome Analysis
Watanabe C
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1269-1279
Published Date: 26 May 2025