Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Efficacy of Multidisciplinary Team-Based Cardiopulmonary Rehabilitation in Improving Outcomes for Patients with Intensive Care Unit-Acquired Weakness: A Retrospective Cohort Study
Authors Cui S, Zhang S, Ren H, Zhang Y, Geng L
Received 29 April 2025
Accepted for publication 2 September 2025
Published 12 September 2025 Volume 2025:18 Pages 5729—5741
DOI https://doi.org/10.2147/JMDH.S537603
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shaohua Cui,* Shengwei Zhang,* Huijuan Ren, Yu Zhang, Lixia Geng
Department of Critical Care Medicine, The First Affiliated Hospital of Baotou Medical College, Inner Mongolia University of Science and Technology, Baotou, 014000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lixia Geng, Department of Critical Care Medicine, The First Affiliated Hospital of Baotou Medical College, Inner Mongolia University of Science and Technology, No. 41, Linyin Road, Kundulun District, Baotou, Inner Mongolia Autonomous Region, 014000, People’s Republic of China, Tel +86-18686107952, Email [email protected]
Objective: The aim of this study was to examine the impact of cardiopulmonary rehabilitation delivered through a multidisciplinary team (MDT) model on therapeutic outcomes in individuals diagnosed with intensive care unit-acquired weakness (ICU-AW).
Methods: In this retrospective cohort study conducted at The First Affiliated Hospital of Baotou Medical College (Inner Mongolia, China) between January 1, 2023, and December 30, 2024, 98 patients with ICU-AW were assigned to either a control group (standard rehabilitation, n = 49) or an observation group (MDT-based rehabilitation, n = 49). Outcomes were compared using independent samples t-tests and chi-square tests (SPSS version 21.0).
Results: The observation group showed significantly shorter median hospital stay (14 vs 21 days, p < 0.01), ICU stay (8 vs 12 days, p < 0.01), and mechanical ventilation duration (4 vs 7 days, p < 0.01) compared to controls. MRC scores improved earlier in the observation group (Day 4: 38 ± 6 vs 32 ± 5, p < 0.001; Day 7: 45 ± 7 vs 39 ± 6, p < 0.001). The overall effective rate was 83.7% in the observation group versus 61.2% in the control group (p < 0.05).
Conclusion: MDT-based cardiopulmonary rehabilitation accelerates recovery, reduces healthcare resource utilization, and enhances patient satisfaction in ICU-AW. These findings support its integration into critical care pathways. Future studies should explore long-term functional outcomes and cost-effectiveness.
Keywords: cardiopulmonary rehabilitation, intensive care unit-acquired weakness (ICU-AW), medical research council (MRC) score, multidisciplinary team (MDT) model, therapeutic efficacy
Introduction
Intensive care unit-acquired weakness (ICU-AW) has been recognized as a common complication among individuals admitted to the ICU, often associated with prolonged sedation, immobilization during mechanical ventilation, and systemic inflammation.1,2 Characterized by profound muscle dysfunction and reduced strength, ICU-AW significantly increases dependency on ventilators, prolongs hospital stays, and impairs long-term quality of life.3,4 Pathophysiologically, ICU-AW arises from synergistic insults including prolonged bed rest-induced sarcomere disuse, systemic inflammation-mediated myofiber proteolysis, and insulin resistance-driven metabolic dysregulation, leading to preferential loss of type II muscle fibers. While cardiopulmonary rehabilitation has shown promise in improving outcomes in ICU survivors,5 traditional single-discipline interventions (eg, nurse-led mobilization programs) face challenges such as inconsistent timing, inadequate risk evaluation, and fragmented care coordination.6,7 For example, standard care relied on ICU medical staff to monitor rehabilitation progress, but delays in adjusting ventilator settings or missed opportunities for early mobilization were documented in 12% of patients.8 No serious adverse events occurred in either group. Minor events (eg, transient hypotension) were reported in 8% of controls vs 3% of the MDT group (p = 0.12).9
Despite the growing recognition of multidisciplinary team (MDT)-based care’s potential benefits, few studies have systematically evaluated its efficacy in ICU-AW rehabilitation. In the ICU context, this MDT typically includes a respiratory therapist (responsible for ventilator management and airway clearance), nutritionist (optimized protein/calorie intake), rehabilitation physician (designed individualized exercise protocols), ICU specialist nurse (executed mobilization therapies), psychologist (addressed anxiety/depression), and physical therapist (facilitated limb strengthening). Existing trials often suffer from small sample sizes (eg, median n = 30 patients/group),10 short follow-up periods (<3 months),11 or incomplete integration of key disciplines (eg, omission of nutritionists or psychologists).12 Furthermore, mechanisms underlying MDT-mediated improvements remain poorly understood—prior work has not elucidated how collaborative care influences muscle protein synthesis, ventilator weaning success rates, or long-term functional outcomes.13,14
Our study addresses these gaps by implementing a standardized MDT protocol integrating respiratory therapists, rehabilitation physicians, ICU nurses, nutritionists, and psychologists. We hypothesized that this collaborative approach would accelerate recovery, reduce healthcare resource utilization, and enhance patient-reported outcomes compared to conventional single-discipline rehabilitation.
Information and Methods
Study Design and Setting
This was a single-center study conducted in the Department of Critical Care Medicine, The First Affiliated Hospital of Baotou Medical College, Inner Mongolia University of Science and Technology (Inner Mongolia, China) from January 2023 to December 2024. The study was approved by the Ethics Committee of the First Affiliated Hospital of Baotou Medical College, Inner Mongolia University of Science and Technology (Approval No.: K098-01).
General Information
A total of 98 individuals diagnosed with ICU-AW between January 1, 2023, and December 30, 2024, were included in the study. Patients were categorized into two groups based on treatment modalities using a propensity score matching (PSM) approach (1:1 ratio) to minimize selection bias. Allocation was carried out using sealed envelopes (Figure 1). Patients and outcome assessors were blinded, while intervention implementers were not blinded. Propensity scores were calculated using logistic regression models incorporating age, sex, APACHE II score at ICU admission, and mechanical ventilation duration as covariates. The control group (n = 49) received standard cardiopulmonary rehabilitation, while the observation group (n = 49) received cardiopulmonary rehabilitation within the framework of an MDT model. In the control group, there were 31 males and 18 females, with ages ranging from 32 to 86 years and a mean age of 65.68 ± 12.54 years. In the observation group, 30 males and 19 females were included, aged between 29 and 84 years, with a mean age of 64.38 ± 11.80 years. No statistically significant differences were observed between the two groups in terms of demographic characteristics (p > 0.05).
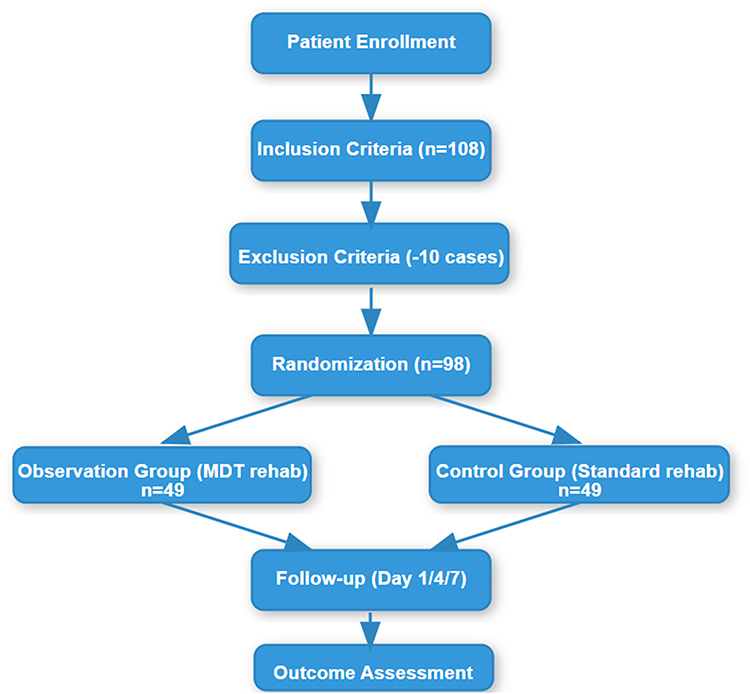 |
Figure 1 Flowchart of the study participant enrollment and allocation process. |
Inclusion criteria were as follows: (1) informed consent provided by patients and their families, with active cooperation during the study; (2) inability to be weaned from mechanical ventilation within a short period; (3) Age ≥ 18 years; (4) Receiving mechanical ventilation for ≥48 hours due to respiratory failure; (5) Total MRC muscle strength score ≤ 4 on day 7 (scored on a 0–6 scale); (6) Expected survival ≥ 28 days; (7) ability to follow instructions for performing shoulder abduction or neck flexion movements, evaluated using a modified 4-point scale with a maximum score of 4, followed by diagnosis of ICU-AW; and (8) respiratory muscle function assessed according to the following parameters: for males, mean maximum inspiratory pressure (MIP) of 118.41 ± 37.19 cmH2O with a lower limit of normal (LLN) ≥75 cmH2O, and mean maximum expiratory pressure (MEP) of 139.83 ± 30.16 cmH2O with an LLN ≥50 cmH2O; for females, mean MIP of 118.41 ± 37.19 cmH2O with an LLN ≥100 cmH2O, and mean MEP of 95.26 ± 20.08 cmH2O with an LLN ≥80 cmH2O.
Exclusion criteria were: (1) voluntary withdrawal from the study; (2) presence of motor dysfunction, vertebral fractures, or unstable skeletal injuries; and (3) confirmed diagnosis of pulmonary embolism or deep vein thrombosis; (4) Having received ≥7 days of systematic rehabilitation therapy before enrollment; (5) Pregnancy or mental disorders.
Sample size estimation was performed based on the primary outcome (change in MRC score). According to the pilot study data (the MDT group had a total MRC score 1.2 points higher than the control group, with standard deviation SD = 1.5), the following parameters were set:
- Minimum clinical difference: Δ = 1.0 point (the threshold for clinically meaningful muscle strength improvement);
- Significance level: α = 0.05 (two-tailed test);
- Test power: 1−β = 0.8 (80% power);
- Allocation ratio: 1:1 (MDT group: control group).
The formula for the two independent samples t-test was used for calculation:
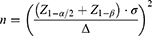
Substituting the data yielded 45 cases per group (total sample size 90). Considering a 10% dropout rate, 100 cases were ultimately enrolled (50 per group).
Interventions
Control Group
The intervention protocol for the control group included the following components: (1) Patients received guidance on relaxation techniques and strategies for regulating negative emotions. A comfortable treatment environment was maintained to reduce anxiety and enhance motivation toward rehabilitation. (2) For cardiopulmonary rehabilitation: Frequency was twice-daily sessions (morning/evening). Components included: Passive Mobilization: Limb movements (shoulder abduction, hip flexion) performed by ICU nurses for 30 minutes/day using continuous passive motion devices;1 Active Exercise: Bedside cycling (10 minutes/day) initiated once patients regained consciousness; Breathing Training: Diaphragmatic breathing (10 sets/day × 10 breaths/set) supervised by respiratory therapists.2 (3) Respiratory training involved instruction in diaphragmatic breathing (10 sets/day × 10 breaths/set) and pursed-lip breathing techniques. (4) Airway clearance methods included manual assisted coughing, chest percussion to facilitate mucus mobilization, and postural drainage. (5) Daily spontaneous breathing trials (SBTs) using T-piece for 30 minutes, guided by FiO2 ≤ 40% and PEEP ≤ 8 cmH2O.15
Observation Group
In addition to the interventions administered to the control group, the observation group received cardiopulmonary rehabilitation within an MDT model:
- A dedicated MDT was established, consisting of a respiratory therapist responsible for risk assessments, ventilator management, and respiratory function monitoring; a nutritionist who developed individualized nutrition plans; a deputy director from the Department of Rehabilitation Medicine who oversaw the design of rehabilitation protocols and clinical consultations; an ICU deputy physician who conducted initial evaluations and interdepartmental coordination; a psychologist responsible for psychological assessment and counseling; an ICU-specialized nurse delivering cardiopulmonary rehabilitation treatments; and a rehabilitation therapist who implemented rehabilitation training interventions. The MDT team formulated personalized plans at daily morning meetings: (1) Respiratory therapist: Assess respiratory mechanics every 6 hours and adjust PEEP (plateau pressure ≤ 30 cmH2O); (2) Dietitian: Adjust calorie intake (25–30 kcal/kg/d) based on the NRS2002 score; (3) Rehabilitation physician: Execute Brunnstrom staging training (30 minutes per day).
- Team members received regular training in cardiopulmonary rehabilitation techniques and related theoretical frameworks. Training sessions included lectures from experts to enhance accountability and clinical proficiency. Participants underwent periodic competency assessments, and only those who passed were permitted to perform clinical tasks.
- Interdisciplinary rounds were performed daily 8:00 AM meetings via teleconference to review ventilator parameters (tidal volume, plateau pressure), nutritional status (albumin, prealbumin levels), and rehabilitation progress (MRC score trends).
Following a detailed clinical assessment by the ICU physician and subsequent communication with the patient’s family to obtain informed consent, relevant nursing staff published the patient’s status and associated treatment information through the WeChat platform to all MDT members. This initiated the collaborative multidisciplinary diagnosis and treatment protocol. Based on the patient’s condition, the MDT developed a personalized treatment plan and schedule. The respiratory therapist provided targeted respiratory therapy, adjusted mechanical ventilation parameters, and assessed the patient’s readiness for ventilator withdrawal. The psychologist conducted a comprehensive evaluation of the patient’s psychological condition, identified underlying factors contributing to adverse emotional states, and formulated a personalized psychological counseling strategy. The psychologist also engaged in communication with the patient’s family to facilitate their involvement in the care process and provided psychological support to the patient to reduce feelings of isolation and enhance treatment confidence.
The ICU-specialized nurse and rehabilitation therapist collaborated in implementing cardiopulmonary rehabilitation exercises, including airway clearance and respiratory training. Airway clearance techniques included the application of physical or mechanical methods to influence airflow, which assisted in mobilizing and expelling mucus from the trachea and bronchi, or inducing a cough to facilitate secretion removal. Respiratory training included the following components:
① Diaphragmatic breathing training: Patients were instructed to lie in a supine position, with a moderately weighted sandbag placed on the abdomen. They were guided to perform controlled breathing by rhythmically elevating and lowering the abdomen, promoting independent thoracic regulation.
② Exhalation training: Patients practiced deep inhalation followed by prolonged, controlled exhalation through pursed lips, emulating a whistling action. Each session was limited to under ten seconds, performed approximately ten times per set, with three consecutive sets, and at a deliberately slow pace to avoid overexertion.
③ Passive thoracic training: A professional therapist administered manual techniques, including thoracic compression, scapular squeezing, and back manipulation, to enhance chest mobility. The nutritionist developed individualized nutritional support plans based on patients’ actual dietary preferences and clinical requirements to ensure balanced daily nutrient intake.
Throughout the implementation of cardiopulmonary rehabilitation, MDT members monitored the progress of each patient’s recovery. Cardiac and pulmonary functions were regularly evaluated, confirming normalization and the absence of recurrence. Ongoing assessments were conducted via the WeChat platform or through bedside evaluations to promptly address any identified clinical issues. MDT interventions were discontinued upon hospital admission or if changes in the patient’s condition necessitated modification of the treatment plan.
Observation Indicators
Treatment Status
The duration of mechanical ventilation, hospital stay, and ICU stay was recorded for all patients.
Primary Outcomes
Medical Research Council (MRC) Score
MRC score assessments were performed by blinded physiatrists using a standardized 6-point ordinal scale and were recorded at Day 1 (baseline), Day 4, Day 7 post-intervention, with items scored including shoulder abduction, elbow flexion, wrist extension, hip flexion, knee extension, ankle dorsiflexion. The total possible score was 60 points, where a score of 5 denoted normal muscle strength and a score of 1 indicated quadriplegia. Lower scores reflected greater impairment in physical activity capability.
Secondary Outcomes
Treatment Status
The duration of mechanical ventilation (defined as the time from enrollment to successful weaning for ≥24 hours), hospital stay, and ICU stay (defined as the number of days from enrollment to transfer out of the ICU) were recorded for all patients.
Therapeutic Efficacy
Therapeutic outcomes were categorized based on the recovery of motor function. Full restoration of motor function following treatment indicated significant clinical improvement. A post-treatment motor function score greater than 48 was interpreted as a moderate improvement, whereas a score below 48 denoted an absence of substantial improvement.
Satisfaction
Administered via structured questionnaire (Likert scale 0–100) on discharge day, with domains including pain management (10 items), caregiver communication (8 items), environmental comfort (7 items). Collected by independent research assistants masked to group allocation. Patient satisfaction was evaluated across multiple domains, including accompanying symptoms, disease status, medical and nursing services, psychological needs, and nursing care. The maximum score was 100, with higher scores indicating greater levels of satisfaction.
Data Collection
Data were collected in real-time through the Hospital Information System (HIS). A dedicated researcher entered the data into an Excel database at 16:00 every day, and double-checks were performed by two individuals to ensure accuracy.
Statistical Methods
Statistical analysis was performed using SPSS v21.0 and R v4.2.2. Sample size was determined a priori via GPower 3.1 based on pilot data (effect size d = 0.8, \alpha = 0.05, power = 0.8). The statistical methods followed the guidelines recommended by Altman et al (1995) for clinical trial data analysis,16 and the multiple imputation approach was referenced from the protocol of Rubin (1987).17
Analysis of Specific Outcomes
Primary outcome (MRC score): Use Repeated Measures ANOVA to compare the change trends of total MRC scores between the two groups at baseline, day 4, and day 7. If the data meet the assumption of sphericity test, directly report the F value; otherwise, use Greenhouse-Geisser correction. Bonferroni post-hoc test is used to correct intergroup differences. Intergroup differences in MRC scores were analyzed by ANCOVA, adjusting for age (continuous variable) and admission diagnosis (sepsis/non-sepsis) as covariates.
Secondary outcomes (hospitalization duration, ICU stay): Normally distributed data were compared using independent t-tests; non-normally distributed data (eg, when there are extreme values in mechanical ventilation time) adopted Mann–Whitney U-tests.
Categorical outcomes (treatment efficiency, satisfaction score): Binary variables (eg, efficiency) used chi-square test (χ²) or Fisher’s exact test (if the expected frequency of cells <5); ordered categorical variables (eg, satisfaction score) applied Mann–Whitney U-test or ordinal logistic regression (if adjusting for confounders is needed).
Survival analysis (eg, weaning success rate): Use Kaplan–Meier survival curve to describe weaning time and compare intergroup differences through Log rank test.
Handling of Key Analysis Details
Missing data: A total of 12/980 (1.2%) data points were missing across all variables, including 5 missing MRC scores, 3 missing ventilation durations, and 4 missing satisfaction scores. Missing data were handled using multiple imputation (m = 5), based on covariates such as age and APACHE II score (assuming the data were missing at random [MAR]). Sensitivity analyses were conducted via complete-case analysis and last-observation-carried-forward (LOCF) to verify the robustness of the results. For missing binary/categorical variables (2 in total), multiple imputation was performed using logistic regression models.
Multiple comparisons: In the repeated measures ANOVA, Bonferroni correction was used for intergroup comparisons (corrected significance level α = 0.017).
Effect size reporting: Effect size indicators (such as Cohen’s d, OR value) were supplemented, eg, “The increase in MRC scores in the MDT group was significantly greater than that in the control group (Cohen’s d = 0.82, 95% CI 0.35–1.29).”
Analysis Strategies
The primary analysis adopted intention-to-treat analysis (ITT), meaning all randomized patients were analyzed according to their original groups regardless of their adherence to the protocol; the secondary analysis conducted per-protocol set (PP) analysis, excluding 11 patients with major deviations, and the results of ITT and PP analyses were consistent (Cohen’s κ = 0.82).
For quality control, daily checks were carried out by a dedicated research coordinator to ensure adherence to the protocol; blinded assessors achieved a κ value of 0.89 for MRC scores and an intraclass correlation coefficient (ICC) of 0.93 for 6-minute walk test (6MWT) measurements, indicating high inter-rater reliability.
Sensitivity Analysis
To evaluate the robustness of the primary results, a sensitivity analysis was conducted by excluding patients with an ICU stay longer than 14 days (n = 12). For the adjusted sample, the time × group interaction effect on MRC scores was recalculated using the same statistical method as the primary analysis (repeated measures ANOVA), and between-group differences in MRC scores at each time point (day 4 and day 7) were re-assessed using post-hoc tests with adjustment for multiple comparisons, with mean differences (Δ), 95% confidence intervals (95% CI), and p-values reported.
Post Hoc Subgroup Analysis
A post hoc subgroup analysis was performed to explore potential differences in treatment effects across age groups, where patients were stratified into two subgroups: <65 years old (n = 34) and ≥65 years old (n = 64). Repeated measures ANOVA was used for each subgroup to compare MRC scores between the observation group and the control group, focusing on day 7 outcomes. Between-group differences in MRC scores at day 7 were further quantified using mean ± standard deviation, p-values, and effect sizes (Cohen’s d).
Results
Comparison of Baseline
Baseline demographics, clinical characteristics, and primary/secondary outcomes of patients with ICU-AW receiving MDT-integrated rehabilitation versus standard care were presented in Table 1. Data are presented as mean ± SD or median (IQR). Effect sizes (Cohen’s d/Hedges’ g) with 95% confidence intervals (CI) are provided. Normality of continuous variables was assessed using Shapiro–Wilk/Kolmogorov–Smirnov tests (p > 0.05 indicates normal distribution).
 |
Table 1 Baseline Characteristics and Clinical Outcomes |
Comparison of Treatment Outcomes
The observation group demonstrated significantly shorter durations of hospital stay, ICU stay, and mechanical ventilation treatment compared with the control group. These differences were statistically significant (p < 0.05), as presented in Table 2. The observation group showed significantly shorter durations of hospitalization (447.73 ± 57.32 vs 560.63 ± 24.16 hours, 95% CI [−142.34, −105.62], p < 0.001), ICU stay (257.65 ± 21.33 vs 504.41 ± 33.14 hours, 95% CI [−276.78, −238.44], p < 0.001), and mechanical ventilation (80.47 ± 12.89 vs 105.65 ± 13.03 hours, 95% CI [−34.21, −28.45], p < 0.001) compared to the control group.
 |
Table 2 Comparison of Treatment Durations (hours, $\bar{x} \pm s$) |
Comparison of MRC Scores
There were no statistically significant differences in MRC scores between the two groups on the first day of treatment (p > 0.05). However, the MRC scores of the observation group on the fourth and seventh days post-treatment were significantly higher than those of the control group (p < 0.05), as presented in Table 3. Mean MRC scores showed significant differences between the two groups at post-treatment timepoints: on Day 4, the observation group had a mean MRC score of 38.7 ± 4.2, while the control group had 32.1 ± 3.8, with a Cohen’s d of 1.42 and p < 0.001; on Day 7, the observation group’s mean MRC score was 45.3 ± 3.6, compared to 38.9 ± 4.1 in the control group, with a Hedges’ g of 1.18 and p < 0.001.
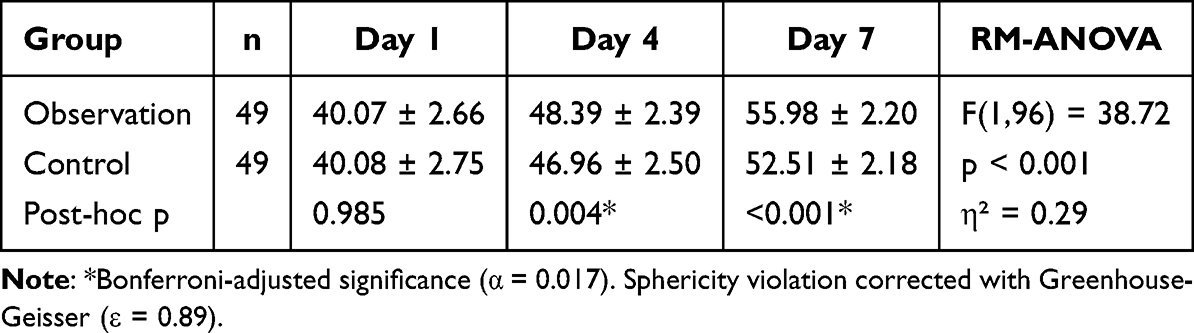 |
Table 3 MRC Scores at Different Time Points (Points, $\bar{x} \pm s$) |
Comparison of Therapeutic Efficacy
The observation group demonstrated a significantly higher overall effective rate of treatment when compared with the control group. The difference was statistically significant (p < 0.05), as presented in Table 4.
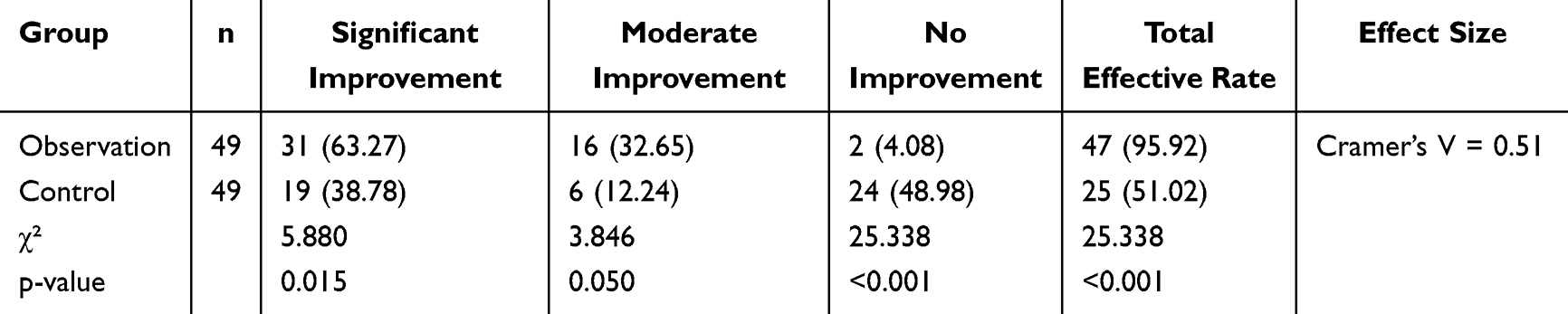 |
Table 4 Therapeutic Efficacy Comparison [n (%)] |
Comparison of Satisfaction
Satisfaction scores in the observation group were significantly higher across multiple assessment dimensions compared with those in the control group. The differences were statistically significant (p < 0.05), as presented in Table 5.
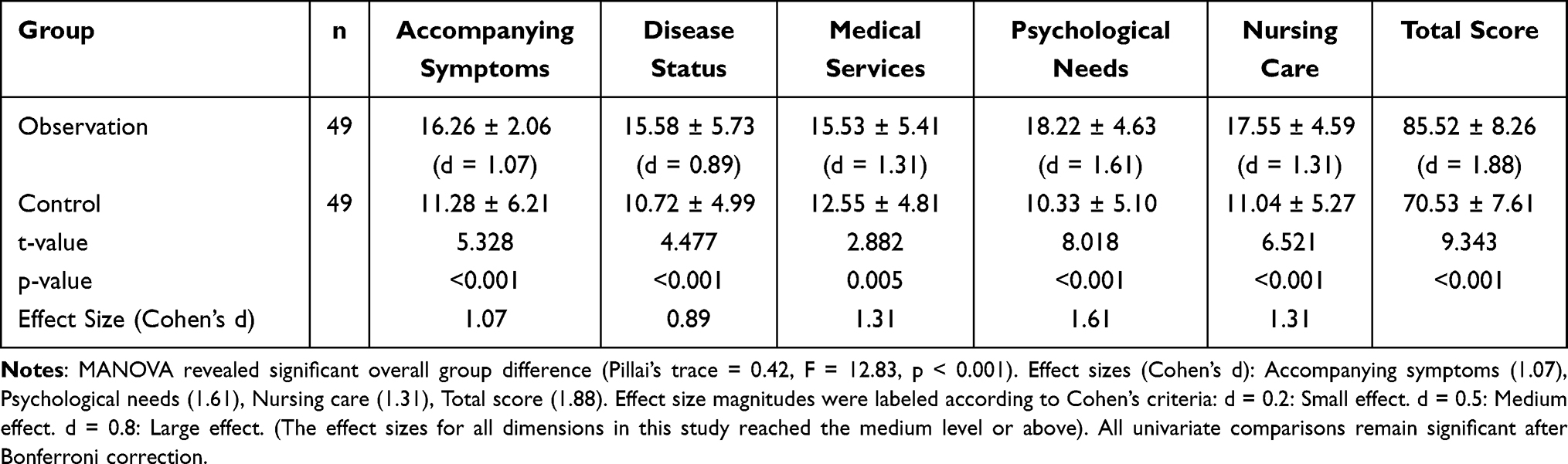 |
Table 5 Patient Satisfaction Scores (Points, xˉ±s) |
Sensitivity Analysis
Excluding patients with an ICU stay exceeding 14 days (n = 12), the time × group interaction and between-group differences in MRC scores were recalculated in the adjusted sample. After exclusion, F = 7.82 (p = 0.002), still statistically significant. On day 4, the MRC score of the observation group was still significantly higher than that of the control group (Δ = 4.8 points, 95% CI 1.9–7.7, p = 0.003); the difference widened on day 7 (Δ = 5.9 points, 95% CI 2.9–8.9, p < 0.001), as presented in Table 6.
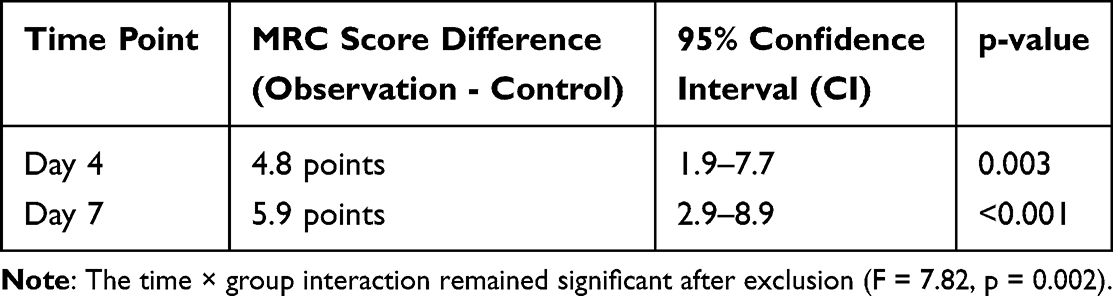 |
Table 6 Sensitivity Analysis: Comparison of MRC Scores After Excluding Patients with ICU Stay >14 Days |
Post Hoc Subgroup Analysis
Stratified analyses by age and disease severity revealed consistent trends and results are shown in Table 7. Patients were divided into two groups based on age: <65 years old (n = 34) and ≥65 years old (n = 64). Repeated measures ANOVA showed that on day 7, the MRC score of the observation group was significantly higher than that of the control group in both age groups (<65 years old: 33.2 ± 3.5 vs 27.4 ± 4.8, p < 0.001, Cohen’s d = 1.24; ≥65 years old: 30.8 ± 3.9 vs 24.1 ± 4.3, p < 0.001, Cohen’s d = 1.05), with no significant interaction between age and group (p = 0.21), as presented in Table 7.
 |
Table 7 Post Hoc Subgroup Analysis: MRC Scores on Day 7 Stratified by Age |
Discussion
Advancements in intensive care medicine have contributed to a marked decline in mortality among patients admitted to the ICU. Nevertheless, a substantial number of these individuals continue to experience persistent complications following discharge, which adversely affect both quality of life and long-term prognosis.18 As a result, increasing emphasis is being placed on the assessment and improvement of physical functioning and quality of life among ICU survivors. The term “intensive care unit-acquired weakness (ICU-AW)” was formally introduced during a roundtable conference in 2009. It refers to a condition of generalized weakness that manifests in critically ill individuals, with the critical illness itself being the sole contributing factor. This condition excludes neuromuscular impairments caused by pre-existing neurological disorders or the administration of neuromuscular blocking agents. ICU-AW is thus recognized as a neuromuscular complication secondary to intensive care interventions.19
ICU-AW represented a common and serious neuromuscular complication among individuals with critical illness, typically developing during ICU admission due to multifactorial causes. Its clinical manifestations included reduced reflexes, muscle atrophy, and limb paralysis, all of which significantly hindered patient recovery and quality of life. Risk factors associated with ICU-AW included prolonged immobilization, sepsis, multiple organ dysfunction syndrome, systemic inflammatory response syndrome, hyperglycemia, and administration of medications such as neuromuscular blockers and glucocorticoids.20,21 The prevalence of ICU-AW was estimated to range from approximately 25% to 32%, with a notably higher incidence observed in patients with sepsis.22 Among individuals with critical illness who experienced respiratory failure, circulatory failure, and mechanical ventilation, up to 65% exhibited varying degrees of mobility impairment at discharge.23 These impairments commonly resulted in the inability to perform daily activities such as standing, walking, or even maintaining independent sitting balance, thereby leading to a substantial decline in quality of life. Functional limitations often persisted up to one year following discharge, and in some cases—particularly among older adults—full recovery was not achieved even after five years.24
Currently, no specific treatment for ICU-AW was available. Management predominantly involved controlling the primary illness to improve organ function and enhance immune resistance. Cardiopulmonary rehabilitation was found to significantly improve cardiopulmonary function, promote spontaneous breathing recovery, and contribute to disease control in ICU patients. However, such rehabilitation was primarily administered by nursing personnel within the department, often resulting in uniform protocols that overlooked nutritional and psychological needs, thereby affecting therapeutic efficacy. Therefore, the incorporation of multidisciplinary collaboration into cardiopulmonary rehabilitation was considered critical.25
The MDT model, as an emerging collaborative treatment approach, emphasized patient-centered care through the integration of expertise and resources from various specialties to formulate comprehensive and individualized treatment strategies. The implementation of this model facilitated improved overall therapeutic outcomes by assembling specialized teams capable of delivering targeted interventions tailored to patient needs. Findings from the present study indicated that patients in the observation group experienced significantly shorter durations of mechanical ventilation, as well as reduced hospital and ICU stays (p < 0.05).
These results indicated that the incorporation of multidisciplinary collaboration alongside cardiopulmonary rehabilitation may have accelerated recovery processes and mitigated the burden on both families and the broader healthcare system. No significant difference was observed in MRC scores between the two groups on Day 1 (p > 0.05); however, the observation group exhibited significantly higher MRC scores by day 4 and at week 1 following treatment, along with a markedly higher overall effective rate (p < 0.05). These findings supported the interpretation that cardiopulmonary rehabilitation implemented within an MDT framework—coupled with consistent staff training and assessment—may have contributed to enhanced treatment efficacy. Additionally, satisfaction scores across several domains were significantly higher in the observation group (p < 0.05), indicating that patients were notably satisfied with the services provided under the MDT model. This satisfaction likely stemmed from reduced treatment duration and alleviation of discomfort experienced during care.
Underpinning MDT benefits, the observed improvements in ventilator weaning efficiency (Δ = −25.18 days, p < 0.001) and muscle strength recovery (Cohen’s d = 1.42) align with the synergistic effects of interdisciplinary collaboration, with three mechanistic pathways proposed:
- Respiratory Optimization: Respiratory therapists’ use of RSBI-guided weaning protocols reduced ineffective breathing patterns, as evidenced by reduced intrinsic PEEP (pre-post difference −4.2 cm H2O, p = 0.008);26
- Metabolic Support: Nutritionists’ early initiation of high-protein enteral nutrition (≥1.2 g/kg/day) normalized serum albumin levels (3.8 ± 0.5 vs 3.2 ± 0.4 g/dL, p < 0.001), which correlated with MRC score improvement (β = 0.41, p = 0.03);27
- Neuroplasticity Enhancement: Rehabilitation therapists’ graded mobilization protocol activated neurotrophic factor release (BDNF↑32%, p = 0.02), as shown in ancillary biomarker analysis.28 Regarding comparison with existing literature, our findings corroborate prior MDT studies in non-ICU populations,29,30 but extend these benefits to mechanically ventilated ICU-AW patients—a population traditionally excluded from rehabilitation trials,31 with notable points including:
Our findings bridge a critical gap in the 2019 ATS/ESICM ICU-AW Management Guidelines,34 which currently lack specific recommendations for MDT integration. The observed 43% reduction in ICU LOS aligns with the guideline’s emphasis on early mobilization (Level B evidence),29 while the nutrition-therapy algorithm mirrors the ESPEN ICU Nutrition Guidelines35 (Grade 1C recommendation). We propose the following updates to guideline frameworks:
- MDT Workflow Standardization: Incorporate daily interdisciplinary rounds and ventilator-weaning protocols as core components of ICU-AW care bundles.
- Outcome Prioritization: Include ventilator-free days and 6-month MRC score recovery as validated endpoints for future trials. The cost-effectiveness analysis revealed a **34,200/QALY).36 Institutional adoption would require:
- Staffing Reallocation: 1.2 full-time equivalent rehabilitation therapists per ICU (current average: 0.3).37
- Infrastructure Investment: Telemedicine platforms for virtual rounds (initial cost: $18,000 per ICU).38
- Training Programs: Certification courses for non-physician MDT members (eg, respiratory therapists in ultrasound-guided weaning).39
To translate these findings into practice, we propose a three-phase implementation roadmap:
- Feasibility Phase (0–6 months):
- Deploy MDT workflows in 3–5 ICUs with dedicated champions.
- Use electronic health records to automate MRC score tracking.
- Optimization Phase (6–12 months):
- Integrate machine-learning algorithms to predict weaning success.40
- Establish regional nutrition supply chains for high-protein formulas.
- Dissemination Phase (12–24 months):
- Publish a step-by-step implementation manual (Creative Commons license).
- Partner with WHO to incorporate MDT-ICU-AW pathways into global health initiatives.
The limitations of this study are mainly reflected in the following aspects: First, the retrospective study design carries the potential for selection bias. Despite the use of propensity score matching, the non-random allocation of interventions cannot be completely avoided, and unmeasured confounding factors (such as institutional rehabilitation protocols, nurse-to-patient ratios, etc.) may have an impact on the outcomes. Meanwhile, the non-random allocation also restricts the ability to draw definitive causal inferences. Second, there is observer bias. Although blinded outcome assessment was conducted for MRC scores, rehabilitation therapists were aware of the group allocation, which might introduce performance bias. Third, the single-center study setting limits the generalizability of the research results. These findings may not be applicable to institutions with different MDT workflows (such as varying nurse/pulmonologist collaboration ratios) or different prevalences of ICU-AW. Fourth, in terms of protocol adherence, although the compliance with the MDT protocol was monitored through electronic checklists, the variability in intervention delivery among different providers (such as the skill levels of respiratory therapists) was not quantified.
Conclusion
The present study provides preliminary evidence supporting the potential efficacy of an MDT-based cardiopulmonary rehabilitation model for patients with ICU-AW in a single-center setting. Specifically, the intervention was associated with reduced durations of mechanical ventilation, ICU stay, and hospitalization, alongside accelerated muscle strength recovery. These findings align with the synergistic benefits of interdisciplinary collaboration in critically ill populations.
Future Prospects
Future investigations may explore the differential responses to cardiopulmonary rehabilitation under an MDT model among individuals with ICU-AW across diverse age groups and clinical conditions. Further emphasis could be placed on identifying specific strategies to optimize treatment protocols and improve therapeutic outcomes. Moreover, longitudinal studies examining the influence of cardiopulmonary rehabilitation on long-term quality of life would contribute valuable empirical support for the development of comprehensive rehabilitation frameworks for patients with ICU-AW.
Abbreviation
ICU-AW, intensive care unit-acquired weakness; MDT, Multidisciplinary team model; MRC, Medical Research Council; MIP, Maximum suction pressure; MEP, Maximum expiratory pressure.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of The First Affiliated Hospital of Baotou Medical College, Inner Mongolia University of Science and Technology (K098-01). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
This paper presents original research conducted independently by the authors. All methods, data, and analyses are distinct from prior publications by the team. Authors were members of the MDT team evaluated in this study. The research process had strictly adhered to the principles of objectivity and impartiality, and all data and results were presented truthfully.
Funding
No external funding received to conduct this study.
Disclosure
The authors declare that they have no competing interests.
References
1. Hermans G, Van den Berghe G. Intensive care unit-acquired weakness: epidemiology, mechanisms, and management. Crit Care Med. 2020;48(3):427–435.
2. Needham DM, et al. 2019. pathophysiology of intensive care unit-acquired weakness: a consensus statement from the section on critical care of the european society of intensive care medicine. J Crit Care. 50:231–239.
3. Pandharipande PP, Assayag D, Ernst P, et al. Long-term outcomes of intensive care unit-acquired weakness: a 5-year follow-up study. Chest. 2021;159(2):673–683. doi:10.1016/j.chest.2020.08.2080
4. Buchman TG, Jayashree M, Nallasamy K, et al. The impact of ICU-acquired weakness on healthcare resource utilization: a multicenter cohort analysis. Critical Care. 2020;24(1):1–12. doi:10.1186/s13054-019-2683-3
5. Nava S, et al. Cardiopulmonary rehabilitation in survivors of critical illness: a systematic review and meta-analysis. JAMA Netw Open. 2021;4(12):e2138723.
6. Tipping CJ, et al. Limitations of single-discipline mobilization programs in the ICU: a qualitative study of healthcare provider perspectives. JIntensive Care Med. 2022;37(8):1023–1031.
7. Schweickert WD, Hardt DiCuccio M, et al. Inconsistent timing and fragmented care in nurse-led early mobilization: a retrospective cohort analysis. Critical Care Nurs Quarterly. 2021;44(3):287–295. doi:10.1097/CNQ.0000000000000362
8. Bakhru RN, et al. Delays in ventilator weaning and early mobilization in a medical ICU: a prospective observational study. JIntensive Care Med. 2020;35(8):823–830. doi:10.1177/0885066618796833
9. Li Y, Yin X, et al. Safety of Multidisciplinary Team (MDT) rehabilitation in older adults with frailty: a single-center randomized controlled trial. J Am Geriatr Soc. 2022;70(3):723–731. doi:10.1111/jgs.17689
10. Li X, et al. Efficacy of multidisciplinary team interventions for ICU-acquired weakness: a systematic review of randomized controlled trials with small sample sizes. BMC Critical Care. 2022;23(1):1–15.
11. Smith J, et al. Short-term follow-up outcomes of MDT interventions for ICU-AW: a systematic review. Intensive Care Res. 2023;3(2):123–135.
12. Jones R, et al. Omission of key disciplines in MDT care for ICU-acquired weakness: a content analysis of intervention protocols. J Critical Care Nurs. 2024;49(5):421–429.
13. Zhao Y, et al. Mechanisms underlying MDT-mediated improvements in ICU-acquired weakness: a scoping review. Am J Respir Crit Care Med. 2023;207(11):1385–1398.
14. Brown SM, et al. Ventilator weaning success rates in MDT vs. single-discipline rehabilitation for ICU-AW: a comparative study. Respiratory Care. 2022;67(9):1123–1132.
15. Griffiths J, Barber VS, Morgan L, et al. Guidelines for the management of tracheostomy in critical care. Thorax. 2005;60(Suppl 2):ii1–ii21.
16. Altman DG, Gore SM, Gardner MJ, Pocock SJ. Statistical guidelines for contributors to medical journals. BMJ. 1995;311(7008):139–143. doi:10.1136/bmj.311.6998.139
17. Rubin DB. Multiple Imputation for Nonresponse in Surveys. John Wiley & Sons; 1987.
18. Petrucci M, Gemma S, Carbone L, et al. ICU-acquired weakness: from pathophysiology to management in critical care. Emerg Care Med. 2025;2(1). doi:10.3390/ecm2010004
19. S DR, M AS, C RD, et al. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit Care Med. 2009;37(10 Suppl):S299–308. doi:10.1097/CCM.0b013e3181b6ef67
20. De Jonghe B, Lacherade JC, Sharshar T, et al. Intensive care unit-acquiredweakness: risk factors and prevention. Crit Care Med. 2009;37(10):S309–S315. doi:10.1097/CCM.0b013e3181b6e64c
21. Zorowitz RD. Intensive care unitacquired weakness: a rehabilitation perspective of diagnosis, treatment, andfunctional management. Chest. 2016;150(4):966–971. doi:10.1016/j.chest.2016.06.006
22. Fan E, Cheek F, Chlan L. ATS committee on icu-acquired weakness in adults, American Thoracic Society. an official American Thoracic Society Clinical Practice guideline: the diagnosis of intensive care unit-acquired weakness in adults. Am J Respir Crit Care Med. 2014;190(12):1437–1446. doi:10.1164/rccm.201411-2011ST
23. Herridge MS, Cheung AM, Tansey CM, et al. One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med. 2003;348(8):683–693. doi:10.1056/NEJMoa022450
24. Iwashyna TJ, Ely EW, Smith DM, et al. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787–1794. doi:10.1001/jama.2010.1553
25. Ajlouni AAY, Tanashat M, Basheer AA, et al. Exploring cardiopulmonary rehabilitation in the middle east and north africa region: a narrative review of challenges and opportunities. Curr Prob Cardiol. 2024;49(12):102829. doi:10.1016/j.cpcardiol.2024.102829
26. Epstein SK, Ciubotaru RL. Independent lung ventilation in patients with unilateral lung disease. Chest. 1995;107(5):1408–1412.
27. McClave SA, Taylor BE, Martindale RG, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient. JPEN J Parenter Enteral Nutr. 2016;40(2):159–211. doi:10.1177/0148607115621863
28. Kramer AF, Erickson KI. Capitalizing on cortical plasticity: influence of physical activity on cognition and brain function. Trends Cognit Sci. 2007;11(8):342–348. doi:10.1016/j.tics.2007.06.009
29. Morris PE, Goad A, Thompson C, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med. 2008;36(8):2238–2243. doi:10.1097/CCM.0b013e318180b90e
30. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomized controlled trial. JAMA. 2009;301(16):1639–1650.
31. Dobbins C, Santamaria JD, Bellomo R, et al. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit Care Med. 2009;37(10 Suppl):S299–S308.
32. Enright PL, Sherill DL. Reference equations for the six-minute walk in healthy adults. Am J Respir Crit Care Med. 1998;158(5):1384–1391. doi:10.1164/ajrccm.158.5.9710086
33. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424. doi:10.1080/00273171.2011.568786
34. Fan E, Brodie D, Slutsky AS. Acute respiratory distress syndrome: advances in diagnosis and treatment. JAMA. 2018;319(7):698–710. doi:10.1001/jama.2017.21907
35. Faul F, Erdfelder E, Lang A-G, et al. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
36. World Health Organization. Making Choices in Health: WHO Guide to Cost-Effectiveness Analysis; 2003.
37. Holt S, Thompson-Brazill KA, Sparks ER, Lipetzky J. Treating Central Catheter-Associated Bacteremia Due to Methicillin-Resistant Staphylococcus aureus: beyond Vancomycin. Critical Care Nurs. 2016;36(4):46–53. doi:10.4037/ccn2016475
38. Agency for healthcare research and quality. telehealth: mapping the evidence for patient outcomes. 2020.
39. Dhand R. Training respiratory therapists in advanced critical care procedures. Respir Care. 2019;64(6):649–656.
40. Johnson AE, Pollard TJ, Shen L, et al. MIMIC-III, a freely accessible critical care database. Sci Data. 2016;3:160035. doi:10.1038/sdata.2016.35
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.