Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Efficacy of low-dose D2/D3 partial agonist pramipexole on neuroleptic-induced extrapyramidal symptoms and symptoms of schizophrenia: a stage-1 open-label pilot study
Authors Weng JJ, Wang LH, Zhu H, Xu WR, Wei YM, Wang ZY ![]() , Yu WJ, Li HF
, Yu WJ, Li HF ![]()
Received 21 February 2019
Accepted for publication 3 July 2019
Published 7 August 2019 Volume 2019:15 Pages 2195—2203
DOI https://doi.org/10.2147/NDT.S205933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jun Chen
Jia Jun Weng,*,1 Li Hua Wang,*,1 Hao Zhu,2 Wen Rong Xu,1 Yu Mei Wei,1 Zhi Yang Wang,1 Wen Juan Yu,1 Hua Fang Li1,3–4
1Department of Psychiatry, Shanghai Mental Health Center, Shanghai Jiao Tong University of Medicine, Shanghai, People’s Republic of China; 2Department of Anesthesiology, Renji Hospital, Shanghai Jiao Tong University of Medicine, Shanghai, People’s Republic of China; 3Shanghai Key Laboratory of Psychotic Disorders, Shanghai, People’s Republic of China; 4Clinical Research Center, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Objective: Some lines of evidence show that D2/D3 receptor partial agonist pramipexole may be effective in the treatment of extrapyramidal symptoms (EPS) and psychiatric symptoms of schizophrenia. Therefore, we analyzed whether a low dose of pramipexole (0.375–0.75 mg/day) has efficacy on EPS and symptoms of schizophrenia while maintaining tolerability.
Methods: Ten subjects with EPS [including drug-induced parkinsonism (DIP) and akathisia] were recruited in a stage-1, open-label pilot study. All the subjects were treated with a low dose of pramipexole. The evaluations were performed at baseline, day 3, week 1, week 2, week 4, week 6, and week 8. The ratings of SAS, BARS, PANSS, CDSS, and CGI-S and adverse effects (AE) were recorded in every visit.
Results: SAS total scores decreased significantly during the study in patients with DIP (P<0.001), and mild AEs were detected. Treatments with pramipexole did not show an anti-akathisia effect during the study, while 2 subjects experienced deterioration of akathisia and mood symptoms. The psychiatric symptoms of schizophrenia showed a trend of improvement during the study, but there was no improvement in depressive mood.
Conclusion: A low dose of pramipexole can significantly relieve antipsychotic-induced parkinsonism, but not akathisia. Improvements in psychiatric symptoms of schizophrenia were found, but the results of this study need to be validated in a larger sample. No improvement of mood disorder was detected.
Keywords: extrapyramidal symptoms, antipsychotics, pramipexole, clinical trial
Introduction
Drug-induced extrapyramidal symptoms (EPS) is a neurological adverse effect (AE) caused by the over-blockade of D2 receptor in the substantia nigra-striatum pathway by antipsychotics.1 Various factors including drug overdose, long-term use of antipsychotics, use of first-generation antipsychotics, age, and gender are correlated with the incidence of EPS.2,3 Schizophrenia patients with EPS often have more severe psychiatric symptoms and poorer social functions.4,5 The treatment and prevention of EPS is of great importance in the treatment outcome of patients with schizophrenia.
The current treatment of EPS in China contains anticholinergics including benzoyl.6,7 However, the side effects of anticholinergics can deteriorate the physical condition and cognition of patients with schizophrenia, especially elderly patients, which strongly restrict its clinical application.8,9 Finding a safer and better-tolerated treatment of EPS is therefore warranted.
Pramipexole is a novel, highly active, partial dopamine (DA) receptor agonist that acts on the D2 receptor family with a preferential affinity for the D3 receptor. Pramipexole is widely used in the treatment of DA-related neurological disorder including Parkinson disease, restless leg syndrome, and EPS. The antiparkinson effect of pramipexole is correlated with its stimulation effect of the postsynaptic D2 receptor.10 The incidence of EPS is significantly correlated with the D2 receptor occupancy in the substantia nigra and striatum areas.11 Approximately, 75–80% blockade of D2 receptors by antipsychotics could lead to the induction of EPS.12 The partial D2 receptor agonist effect of pramipexole may reverse the over-blockade of D2 receptor in the substantia nigra and striatum areas and therefore reverse the symptoms of EPS.
Studies have found pramipexole can also relieve mood disorders and anhedonia symptoms of Parkinson disease, which may be related to its partial agonist effect on the D3 receptors.13,14 Moreover, pramipexole may be effective in the treatment of schizophrenia considering its modulation effect on DA transmission through partial agonist effect of D2 and D3 receptors.15 Last but not least, pramipexole’s efficacy on negative symptoms also deserves to be investigated, depending on the facts antipsychotics with D2/D3 partial agonist effect, such as cariprazine, have better treatment outcome than other atypical antipsychotics.16 Therefore, symptoms of schizophrenia, especially negative symptoms that are difficult to relieve depending on the current treatment of atypical antipsychotics, might benefit from the use of the D2/D3 receptor partial agonist pramipexole.
The primary outcome of this study is to investigate whether the D2/D3 receptor partial agonist pramipexole could relieve EPS, and the secondary outcome is to evaluate the effect of low-dose pramipexole for the psychiatric and mood symptoms of schizophrenia. We hypothesized that a low dose of pramipexole may be effective in the treatment of EPS and schizophrenia.
Patients and methods
Patients
This study is a stage-1 pilot study of a two-stage clinical trial. In the stage-1 study, 10 subjects were recruited to preliminarily explore the efficacy and safety of pramipexole. All subjects were recruited in Shanghai Mental health center. The inclusion criteria were as follows: 1) 18–65 years of age; 2) met the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria for drug-induced parkinsonian and akathisia17; and 3) a 6-item Simpson–Angus Scale (SAS) total score above 2 or a score of 2 (mild) or above on the global subscale of the Barnes Akathisia Rating Scale (BARS). If any of the following events occurred, the subject was withdrawn from the study: 1) a serious AE (ie, death, rehospitalization, physical disability, etc.) 2) poor compliance, obvious protocol violation, or those who did not take the drugs continuously for 4 days; and 3) scored (mild) on at least two Abnormal Involuntary Movement Scale items or three (moderate) on one of the items that are considered to be tardive dyskinesia. All the subjects did not receive any treatment of EPS before entering the study.
Among the 10 subjects included in this study, 7 of them were diagnosed with schizophrenic disorder according to the DSM-IV; 1 subject was diagnosed with obsessive-compulsive disorder, 1 subject was diagnosed with major depressive disorder (MDD); and 1 was diagnosed with mental retardation. Seven subjects were diagnosed with drug-induced parkinsonism (DIP); 2 subjects were diagnosed with akathisia, and 1 subject fitted both the criteria. Most of the subjects were taking antipsychotic polytherapy. Four subjects were treated with risperidone (mean, 4.3±0.5 mg; range, 4–5 mg); four subjects were treated with aripiprazole (mean, 11.3±6.3; range, 5–20 mg); and three subjects were treated with quetiapine (mean, 366.7±251.7; range, 100–600) and clozapine (mean, 166.7±57.8; range 100–200 mg). Amisulpride (1000 mg), Olanzapine (20 mg), and Fluphenazine injection (25 mg qw) were used in one subject. The demographics and mean scale ratings are shown in Table 1, and clinical variables and drug characteristics of each subject are shown in Table 2. The drug dose of pramipexole and change in antipsychotics of each subject during the trial are shown in Table 3.
 |
Table 1 Demographics and baseline scale ratings of all subjects |
 |
Table 2 Clinical and drug characteristics of each subject |
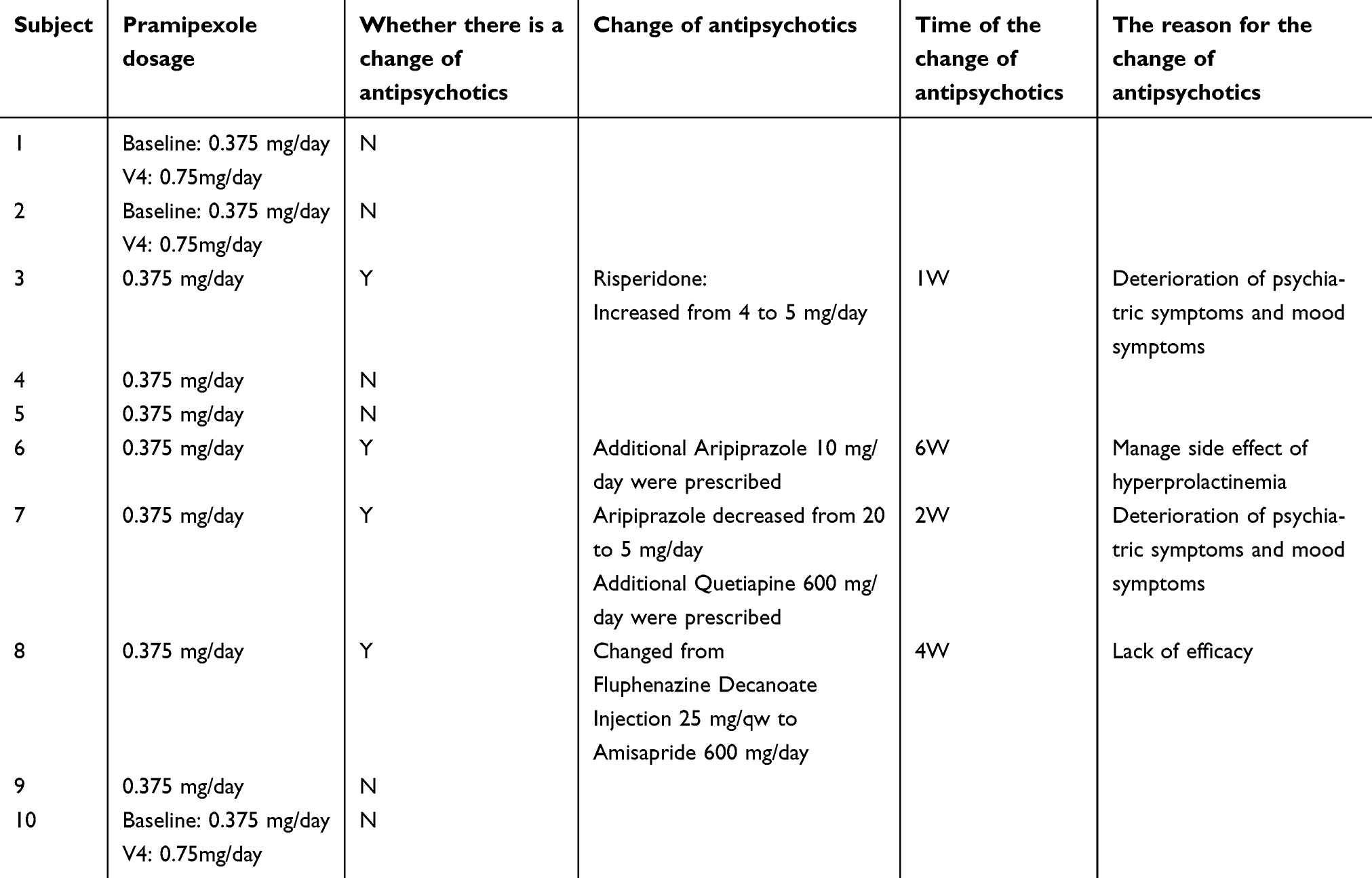 |
Table 3 Drug dose of pramipexole and change in antipsychotics of subjects during the trial |
Treatment protocol
Considering that pramipexole was being used for the first time in Chinese patients with schizophrenia, low dose of pramipexole was used for safety considerations (0.375–0.75 mg/day). Subjects took 0.375 mg/day of pramipexole (0.135 mg thrice per day) on week 1, and the dose was increased to 0.75 mg/day (0.25 mg thrice per day) after week 1 depending on the researchers’ decision. Treatment protocol was based on the treatment of Parkinson disease by pramipexole.17
The evaluations of SAS and BARS were used to assess the severity of EPS. SAS is a 10-item rating scale that is frequently used to assess DIP and muscle rigidity in clinical practice.18 One item measure gait, 6 items measure stiffness, and 3 items measure tremor, salivation, and palpebral reflex (each item ranging from 0 to 4). BARS is a scale used to assess akathisia, and it consists of 4 items, including objective symptoms, subjective symptoms, subjective distress, and global evaluations items (the score of each item ranges from 0 to 4).19 Positive and Negative Syndrome Scale (PANSS) is a 30-item rating scale designed to assess dimensions of schizophrenia symptoms. Its items were originally grouped into scales for Positive Symptoms (7 items), Negative Symptoms (7 items), and General Psychopathology (16 items). Calgary Depression Scale for Schizophrenia (CDSS) is a 9-item rated scale specifically designed to assess depression in patients with schizophrenia with high sensitivity rate and high specificity rate.20,21 The CGI-S scale is a valid, reliable instrument to evaluate severity and treatment response in schizophrenia, and its score ranges from 0 (no illness) to 7 (severe illness).22 PANSS, CDSS, and Clinical Global Impression Scale (CGI-S) were used to access the psychiatry symptoms and mood symptoms of schizophrenia. Assessments were conducted at baseline, day 3, week 1, week 2, month 1, week 6, and month 2. The laboratory measurements, vital signs, and electrocardiogram were recorded at baseline and endpoint of the study to see whether pramipexole can deteriorate the physical status of the subjects.
Ethics approval and informed consent
All subjects and their guardians signed a written informed consent, and all the assessment was conducted by trained psychiatrists who have underwent scale consistency training before the first subjects were enrolled. This study was approved by the Shanghai Mental Health Center ethics committees (No. 2017-40), and this trial has been registered in the Clinical Trial website (NCT03430596). This study was conducted in accordance with the Declaration of Helsinki.
Statistical analysis
All statistical analyses were performed using SPSS 23.0 (SPSS Inc., Chicago, IL, USA). All data are expressed as mean ± SEM. ANOVA tests with post hoc analyses were used to examine differences in EPS, psychiatric symptoms, and mood symptoms of schizophrenia among the different visits. The Bonferroni correction was used to perform post hoc analysis for the chi-square tests, and statistical significance was set at P<0.007 (0.05/number of comparisons=0.007).
Results
Primary outcome
The ratings of SAS decreased significantly during the visit [5.9±3.2 vs 1.1±0.6, respectively, F(6,7)=9.46, P<0.007] among subjects with DIP. The ratings of the BARS global subscale [2.3±0.3 vs 2.0±0.7, respectively, F(6,3)=0.12, P=0.99], objective subscale [1.3±1.3 vs 0.7±0.7, respectively, F(6,3)=0.16, P=0.98], subjective subscale [1.7±0.3 vs 1.3±0.9, respectively, F(6,3)=0.18, P=0.98], and distress subscale [1.3±0.3 vs 1.3±0.9, respectively, F(6,3) =0.09, P=099] did not significant change during the visit. The changes in the SAS and BARS scores are shown in Table 4.
 |
Table 4 The change in rating score in subjects with drug-induced parkinsonian and akathisia |
Secondary outcome
The PANSS negative subscale [27.4±3.1 vs 24.3±3.5, respectively, F(6,7)=0.26, P=0.95], PANSS positive subscale [16.1±1.6 vs 13.7±1.6, respectively, F(6,7)=1.03,P=0.49], PANSS general psychopathological subscale [42.9±3.0 vs 41.6±5.6, respectively, (F6,7)=0.24, P=0.96], PANSS total score [86.4±6.9 vs 79.4±10.1, respectively, F(6,7)=0.38, P=0.89], CDSS [3.7±1.8 vs 5.0±1.6, respectively, F(6,7) =0.08, P=0.99], CGI-S [5.0±0.3 vs 4.9±0.6, respectively, F(6,7)=0.44, P=0.85] did not significant change during the study. The changes in psychiatric rating scales of schizophrenia during the study are shown in Figure 1.
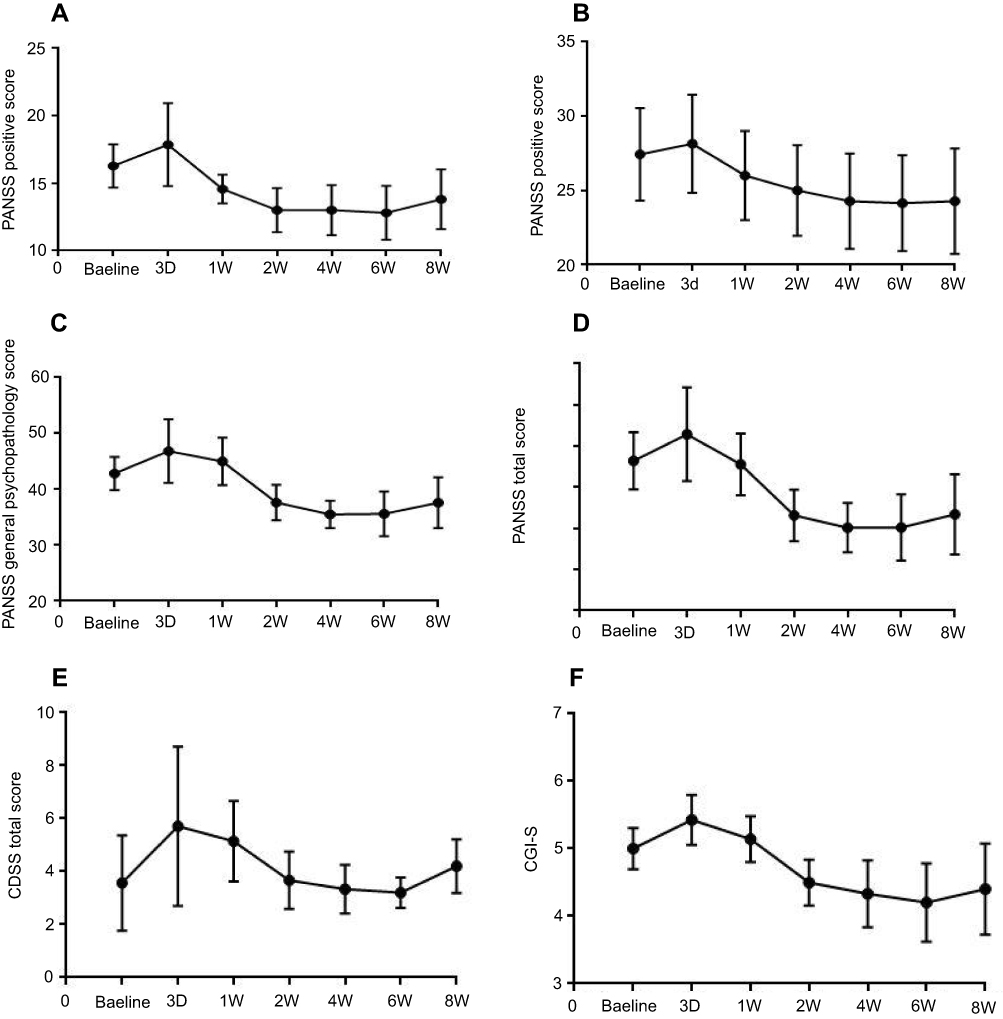 |
Figure 1 Changes in (A) PANSS positive score, (B) PANSS negative score, (C) PANSS general psychopathological score, (D) PANSS total score, (E) CDSS total score and (F) CGI-S. Abbreviations: PANSS, Positive and Negative Sydrome Scale; CDSS, Calgary Depression Scale for Schizophrenia; CGI-S, Clinical Global Impression Scale. |
Adverse effect
The main AEs of pramipexole in this study include depressed mood (2 subjects), suicidal ideation (2 subjects), drowsiness (1 subject), and nausea (1 subject). Depressed mood occurred in two subjects with akathisia. Both of them showed the deterioration of psychiatric symptoms and mood symptoms. One of them withdrew from the study, and in other patient, drug switch and MECT were performed to manage AEs. Drowsiness and nausea occurred in two subjects with DIP. Two other subjects withdrew from the study: one subject discontinued the drug intake because of nausea, and the other one withdrew the consent. All the side effects were relieved after the measurements. The adverse events that occurred during the study are shown in Table 5. The laboratory measurements, vital signs, and electrocardiogram did not change significantly during the trial.
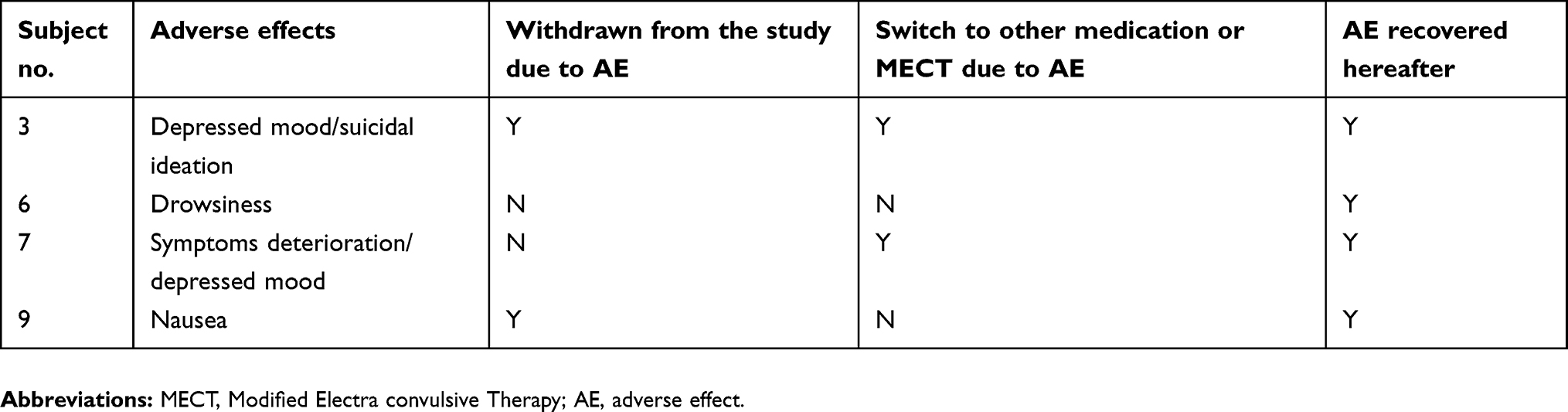 |
Table 5 Adverse effects |
Discussion
Our study has shown that low doses of D2 and D3 receptor partial agonists, ranging from 0.375 to 0.75 mg/day, may be beneficial in the treatment of DIP. SAS score decreased over 80% during the visit, without worsening of psychiatric symptoms and with low dropout rate (14.2%, 1 of 7). Pramipexole was well tolerated among subjects with DIP, and side effects, primarily drowsiness and nausea, were reported. A previous study showed that the D3/D2 receptor partial agonist rotigotine in low doses is safe and effective in patients with EPS including antipsychotic-induced parkinsonism and akathisia.23 Rotigotine significantly decreased the ratings of Unified Parkinson’s Disease Rating Scale total (a scale used to evaluate the symptoms of Parkinson disease), SAS total score, and BARS global subscale. One study showed that pramipexole can relieve haloperidol-induced catalepsy and tremor in mice.24 Haloperidol-induced catalepsy is used as an animal model of extrapyramidal side effects. This relief of catalepsy by pramipexole confirmed that it may be beneficial in symptoms of antipsychotic-induced parkinsonism including dystonia, akinesia, and slowness of movement.
The mechanisms underlying the antiparkinson effect of pramipexole are complicated. Despite its partial agonistic effect on the postsynaptic D2 receptor, pramipexole can also reduce DA uptake and increase DA neurotransmission through its long-term interaction of the presynaptic D3 autoreceptor.25 The agonism of the postsynaptic D2 receptor and increase in the DA neurotransmission may reverse the phenomenon of “dopamine-acetylcholine” imbalance caused by the blockade of D2 receptor which is the key phenomenon of DIP.26 Furthermore, the neuroprotective and antioxidant effects of pramipexole can also explain its efficacy.27,28 Overall, the mechanisms of pramipexole in its treatment effect of DIP merit further investigation.
Treatments with pramipexole did not show an anti-akathisia effect during the study, regardless of subjective pain, distress, or objective observation symptoms of akathisia. Nevertheless, two subjects (four subjects with akathisia in total) experienced an AE during the study. One subject (No. 3) had a depressed mood and suicidal ideation, with a deterioration of the akathisia syndrome. Another subject (No. 7) experienced a recurrence of her psychiatric symptoms, consisting of auditory hallucination and delusional thoughts. After the MECT treatment, No. 3 patients’ symptoms were immediately relieved. After a slow exchange of antipsychotics from Aripiprazole 20 mg/day to Quetiapine 600 mg/day combined with aripiprazole 5 mg/day polytherapy, symptoms of No.7’s psychiatri syndromes are stabilized and akathisia syndromes disappeared. In general, pramipexole did not show efficacy and safety in subjects with akathisia in the step 1 trial.
The immediate deterioration of akathisia and mood symptoms indicates that the partial agonist effect of the DA receptor does no good in treating the symptoms of akathisia. A previous study showed that antipsychotics with a partial DA receptor agonistic effect (ie, aripiprazole, brexpiprazole, and cariprazine) and high D2 receptor antagonist effect (ie, risperidone and haloperidol) are more risky for inducing akathisia than antipsychotics (ie, olanzapine and quetiapine).29 The relation between the partial DA receptor agonist effect and akathisia is complicated and remains unknown, especially considering the relatively high D2 receptor binding ability and both partial agonist and antagonist effect on the D2 receptor of this kind of antipsychotics.30,31 Besides, the short-term administration of pramipexole can spontaneously decrease the synaptic release of DA and firing rate of DA and norepinephrine (NE) neurons.32 The decrease of the firing rate of DA, NE neurons, and DA release may account for the spontaneous deterioration of mood symptoms and akathisia. Nevertheless, considering the relatively small sample of subjects with akathisia in step 1, this phenomenon will be observed, monitored, and validated in the step 2 study.
All the psychiatric rating scales including PANSS, CDSS, and CGI-S did not change significantly during the trial. All the psychiatric rating scales showed an increasing trend on day 3 and at 1 week, which is due to the immediate deterioration of the symptoms in two subjects with akathisia. After one subjects’ withdrawal and management of another subjects’ AE, the PANSS positive score, PANSS negative score, PANSS general psychopathology score, PANSS total score, and CGI-S all showed a trend of improvement during the remaining follow-up. The mild improvement of positive symptoms, negative symptoms, and general psychopathology symptoms of patients proved that pramipexole may be beneficial to the psychiatric symptoms of schizophrenia. The results of our trial are consistent with those of a previous study, with a higher dose range and higher rating improvement of the PANSS rating scale.15,33 Unexpectedly, we did not see improvement of mood symptoms of patients with schizophrenia in this trial. After the management of akathisia symptoms, the CDSS total score slowly decreased but remained higher than the baseline score until the endpoint. Pramipexole has shown efficacy on mood symptoms of MDD, bipolar disorder, and Parkinson disease.34–36 But the dose of pramipexole in these studies is relatively higher, ranging from 1.0 to 3.0 mg/day. The lack of efficacy on depression mood may be due to low drug dose and relatively mild depression mood of our subjects. Considering the complicated mechanism of depression mood of schizophrenia patients, whether a low dose of pramipexole can be effective in mood symptoms will be further validated in the step 2 study.
Limitations and further study
The limitations of the study are small sample size (n=10), wide age range (18–65 years), and the open-label design. Depending on the preliminary results of the current study, we will enlarge the sample size and make a single-blind study design in Phase II study, which will further validate pramipexole’ s efficacy on EPS and symptoms of schizophrenia.
Conclusion
In conclusion, a low dose of pramipexole is efficacious in the treatment of antipsychotic-induced parkinsonism, but it did not show efficacy on akathisia. Our study also demonstrated that co-medication with pramipexole may be effective on psychiatric symptoms of schizophrenia, although the improvements are not very significant probably due to the low dose. The symptoms of mood are not improved after combining with the treatment of pramipexole. In general, the findings of this study suggest that the usage of the D2/D3 partial agonist pramipexole could be beneficial in the treatment of neuroleptic-induced EPS, especially DIP, and show a trend of improvement of schizophrenia symptoms. The results of this study need to be validated in a larger sample.
Acknowledgments
The authors thank the staff of Drug Clinical Trial Institution of Shanghai Mental Health Center and Dr Lu WH, Dr ZLP, Dr SY, and Dr CY for their contribution to the recruitment of subjects and valuable suggestions. This study is supported by Shanghai Collaborative Innovation Center for Translational Medicine and National Science (Grant No. TM201624), Technology Major Project for Investigational New Drug (Grant No. 2018ZX09734-005), Multi-center Clinical Study of Shanghai Jiao Tong University School of Medicine (Grant No. DLY201620) and Shanghai Committee of Science and Technology Research Project (Grant No. 17411970300).
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Divac N, Prostran M, Jakovcevski I, Cerovac N. Second-generation antipsychotics and extrapyramidal adverse effects. Biomed Res Int. 2014;2014:656370. doi:10.1155/2014/656370
2. Mehta SH, Morgan JC, Sethi KD. A positron emission tomography study of quetiapine in schizophrenia: a preliminary finding of an antipsychotic effect with only transiently high dopamine D2 receptor occupancy. Neurol Clin. 2015;33(1):153–174. doi:10.1016/j.ncl.2014.09.011
3. Miller DD, McEvoy JP, Davis SM, et al. Clinical correlates of tardive dyskinesia in schizophrenia: baseline data from the CATIE schizophrenia trial. Schizophr Res. 2005;80(1):33–43. doi:10.1016/j.schres.2005.07.034
4. Mentzel TQ, Lieverse R, Bloemen O, Viechtbauer W, van Harten PN, Incidence H. Prevalence of drug-related movement disorders in young patients with psychotic disorders. J Clin Psychopharmacol. 2017;37(2):231–238. doi:10.1097/JCP.0000000000000666
5. Park IJ, Jung DC, Hwang SS, et al. The longitudinal trends in the relationship between drug-induced extrapyramidal symptoms and personal and social performance in a population of the patients with schizophrenia: A latent growth model. Psychiatry Res. 2016;238:33–39. doi:10.1016/j.psychres.2016.01.069
6. Su YA, Yan F, Li Q, et al. Anticholinergic use trends in 14,013 patients with schizophrenia from three national surveys on the use of psychotropic medications in China (2002–2012). Psychiatry Res. 2017;257:132–136. doi:10.1016/j.psychres.2017.07.038
7. Pristed SG, Correll CU, Nielsen J. Frequency and correlates of anticholinergic use among patients with schizophrenia in Denmark: a nation-wide pharmacoepidemiological study. Psychiatry Res. 2017;255:198–203. doi:10.1016/j.psychres.2017.05.033
8. Vinogradov S, Fisher M, Warm H, Holland C, Kirshner MA, Pollock BG. The cognitive cost of anticholinergic burden: decreased response to cognitive training in schizophrenia. Am J Psychiatry. 2009;166(9):1055–1062. doi:10.1176/appi.ajp.2009.09010017
9. Kreyenbuhl J, Buchanan RW, Dickerson FB, Dixon LB. The Schizophrenia Patient Outcomes Research Team (PORT): updated treatment recommendations 2009. Schizophr Bull. 2010;36(1):94–103. doi:10.1093/schbul/sbp130
10. Oertel W, Schulz JB. Current and experimental treatments of Parkinson disease: A guide for neuroscientists. J Neurochem. 2016;139(Suppl 1):325–337. doi:10.1111/jnc.13750
11. Mehta SH, Morgan JC, Sethi KD. Drug-induced movement disorders. Neurol Clin. 2015;33(1):153–174. doi:10.1016/j.ncl.2014.09.011
12. Kapur S, Zipursky R, Jones C, Shammi CS, Remington G, Seeman P. A positron emission tomography study of quetiapine in schizophrenia: a preliminary finding of an antipsychotic effect with only transiently high dopamine D2 receptor occupancy. Arch Gen Psychiatry. 2000;57(6):553–559.
13. Barone P, Poewe W, Albrecht S, et al. Pramipexole for the treatment of depressive symptoms in patients with Parkinson’s disease: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2010;9(6):573–580. doi:10.1016/S1474-4422(10)70106-X
14. Berghauzen-Maciejewska K, Kuter K, Kolasiewicz W, et al. Pramipexole but not imipramine or fluoxetine reverses the “depressive-like” behaviour in a rat model of preclinical stages of Parkinson’s disease. Behav Brain Res. 2014;271(1):343-353 doi: 10.1016/j.bbr.2014.06.029.
15. Kasper S, Barnas C, Heiden A, et al. Pramipexole as adjunct to haloperidol in schizophrenia. Safety and efficacy. Eur Neuropsychopharmacol. 1997;7(1):65–70.
16. Nemeth G, Laszlovszky I, Czobor P, et al. Cariprazine versus risperidone monotherapy for treatment of predominant negative symptoms in patients with schizophrenia: a randomised, double-blind, controlled trial. Lancet (London, England). 2017;389(10074):1103–1113. doi:10.1016/S0140-6736(17)30060-0
17. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
18. Clarke CE, Guttman M. Dopamine agonist monotherapy in Parkinson’s disease. Lancet (London, England). 2002;360(9347):1767–1769. doi:10.1016/s0140-6736(02)11668-0
19. Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatrica Scandinavica Supplementum. 1970;212:11–19.
20. Barnes TR. A rating scale for drug-induced akathisia. Br J Psychiatry. 1989;154:672–676. doi:10.1192/bjp.154.5.672
21. Addington D, Addington J, Schissel B. A depression rating scale for schizophrenics. Schizophr Res. 1990;3(4):247–251.
22. Addington D, Addington J, Maticka-Tyndale E, Joyce J. Reliability and validity of a depression rating scale for schizophrenics. Schizophr Res. 1992;6(3):201–208.
23. Haro JM, Kamath SA, Ochoa S, et al.The Clinical Global Impression-Schizophrenia scale: a simple instrument to measure the diversity of symptoms present in schizophrenia. Acta Psychiatr ScandSuppl. 2003;(416):16–23. doi:10.1034/j.1600-0447.107.s416.5.x
24. Di Fabio R, De Filippis S, Cafariello C, et al. Low doses of rotigotine in patients with antipsychotic-induced parkinsonism. Clin Neuropharmacol. 2013;36(5):162–165. doi:10.1097/WNF.0b013e3182a2ce3f
25. Ferger B, Buck K, Shimasaki M, Koros E, Voehringer P, Buerger E. Continuous dopaminergic stimulation by pramipexole is effective to treat early morning akinesia in animal models of Parkinson’s disease: a pharmacokinetic-pharmacodynamic study using in vivo microdialysis in rats. Synapse (New York, NY). 2010;64(7):533–541. doi:10.1002/syn.v64:7
26. Castro-Hernandez J, Afonso-Oramas D, Cruz-Muros I, et al. Prolonged treatment with pramipexole promotes physical interaction of striatal dopamine D3 autoreceptors with dopamine transporters to reduce dopamine uptake. Neurobiol Dis. 2015;74(2):325–335. doi:10.1016/j.nbd.2014.12.007
27. Kharkwal G, Brami-Cherrier K, Lizardi-Ortiz JE, et al. Parkinsonism driven by antipsychotics originates from dopaminergic control of striatal cholinergic interneurons. Neuron. 2016;91(1):67–78. doi:10.1016/j.neuron.2016.06.014
28. Wang Y, Yu X, Zhang P, et al. Neuroprotective effects of pramipexole transdermal patch in the MPTP-induced mouse model of Parkinson’s disease. J Pharmacol Sci. 2018;138(1):31–37. doi:10.1016/j.jphs.2018.08.008
29. Shibagaki K, Okamoto K, Katsuta O, Nakamura M. Beneficial protective effect of pramipexole on light-induced retinal damage in mice. Exp Eye Res. 2015;139:64–72. doi:10.1016/j.exer.2015.07.007
30. Juncal-Ruiz M, Ramirez-Bonilla M, Gomez-Arnau J, et al. Incidence and risk factors of acute akathisia in 493 individuals with first episode non-affective psychosis: a 6-week randomised study of antipsychotic treatment. Psychopharmacology. 2017;234(17):2563–2570. doi:10.1007/s00213-017-4646-1
31. Brust TF, Hayes MP, Roman DL, Watts VJ. New functional activity of aripiprazole revealed: robust antagonism of D2 dopamine receptor-stimulated Gbetagamma signaling. Biochem Pharmacol. 2015;93(1):85–91. doi:10.1016/j.bcp.2014.10.014
32. Stahl SM. Mechanism of action of cariprazine. CNS Spectr. 2016;21(2):123–127. doi:10.1017/S1092852916000043
33. Chernoloz O, El Mansari M, Blier P. Sustained administration of pramipexole modifies the spontaneous firing of dopamine, norepinephrine, and serotonin neurons in the rat brain. Neuropsychopharmacology. 2009;34(3):651–661. doi:10.1038/npp.2008.114
34. Kelleher JP, Centorrino F, Huxley NA, et al. Pilot randomized, controlled trial of pramipexole to augment antipsychotic treatment. Eur Neuropsychopharmacol. 2012;22(6):415–418. doi:10.1016/j.euroneuro.2011.10.002
35. Cusin C, Iovieno N, Iosifescu DV, et al. A randomized, double-blind, placebo-controlled trial of pramipexole augmentation in treatment-resistant major depressive disorder. J Clin Psychiatry. 2013;74(7):e636–e641. doi:10.4088/JCP.12m08093
36. Zarate CA
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.