Back to Journals » Clinical Ophthalmology » Volume 19
Efficacy of Intravitreal Conbercept in Vitrectomy for Proliferative Diabetic Retinopathy: An Integrated Meta-Analysis and Bibliometric Study
Authors Li G, Zhang M, Ke Y, Zheng C, Tan L, Li Y, Pazo EE ![]() , Chen C, Ren X
, Chen C, Ren X ![]()
Received 14 January 2025
Accepted for publication 22 July 2025
Published 19 September 2025 Volume 2025:19 Pages 3465—3486
DOI https://doi.org/10.2147/OPTH.S516425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Guangda Li,1,* Mingxuan Zhang,2,* Yifeng Ke,2 Chuanzhen Zheng,3 Liangzhang Tan,2 Yongtao Li,2 Emmanuel Eric Pazo,2 Chunli Chen,4 Xinjun Ren2
1Department of Ophthalmology, Linyi People’ s Hospital, Linyi, Shandong, People’s Republic of China; 2Tianjin Key Laboratory of Retinal Functions and Diseases, Tianjin Branch of National Clinical Research Center for Ocular Disease, Eye Institute and School of Optometry, Tianjin Medical University Eye Hospital, Tianjin, People’s Republic of China; 3Department of Ophthalmology, Sichuan Provincial People’s Hospital, Chengdu, People’s Republic of China; 4Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunli Chen, Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University, Beijing, 100010, People’s Republic of China, Email [email protected] Xinjun Ren, Tianjin Medical University Eye Hospital, 251 Fu Kang Road, Tianjin, 300384, People’s Republic of China, Email [email protected]
Purpose: To evaluate the effectiveness of intravitreal Conbercept administered before or during vitrectomy in patients with proliferative diabetic retinopathy (PDR), additionally, a bibliometric analysis was performed.
Methods: The literature search was conducted using keywords and terms combined as follows: “conbercept”, “vitrectomy”, and “proliferative diabetic retinopathy”, from January 2012 to August 2024. Additionally, we conducted three different comparisons. Data for the bibliometric analysis were obtained from the Web of Science database and analyzed using VOSviewer and Bibliometrix applications.
Results: A total of 16 studies encompassing 1,215 cases were analyzed in this review. Patients in the Conbercept group demonstrated significantly greater improvements in best corrected visual acuity (BCVA) compared to the no injection group at six-month follow-ups (MD = – 0.36, 95% CI – 0.45 to – 0.28, P < 0.01). Additionally, the Conbercept group experienced fewer intraoperative complications, including reduced incidences of intraoperative bleeding (OR = 0.12, 95% CI 0.07 to 0.21), use of endodiathermy (OR = 0.26, 95% CI 0.15 to 0.47), silicone oil tamponade (OR = 0.50, 95% CI 0.35 to 0.73), and iatrogenic breaks (OR = 0.25, 95% CI 0.13 to 0.48). Both early and late postoperative vitreous hemorrhages were less common in the Conbercept group. When administered during vitrectomy, Conbercept still showed superior BCVA improvement at six months (MD = – 0.32, 95% CI – 0.46 to – 0.18, P < 0.01). No significant difference was found between Conbercept and Ranibizumab in BCVA or intraoperative outcomes. From 2015 to 2025, 5,065 publications on Conbercept emerged, with declining growth but strong global collaboration and relevance in anti-VEGF ocular therapy.
Conclusion: This systematic review revealed that, similarly to other anti-VEGF injections, Conbercept injection improved BCVA and had lower rates of intraoperative and postoperative complications. Conbercept research shows strong global collaboration and evolving focus on clinical applications in retinal vascular disease management.
Keywords: proliferative diabetic retinopathy, conbercept, ranibizumab, vitrectomy, BCVA
Introduction
Diabetic retinopathy (DR) is a frequently occurring microvascular consequence of diabetes, affecting around 34.6% of individuals. Proliferative diabetic retinopathy (PDR) is the advanced stage of DR, representing 6.96% of cases.1,2 PDR is one of the leading causes of blindness in adults and is associated with vitreous hemorrhage, tractional retinal detachment, and neovascular glaucoma.3,4 Pars plana vitrectomy remains one of the most effective therapeutic options for the treatment of PDR. However, neovascularization increases the risk of vitreous hemorrhage both intraoperatively and postoperatively.5 Therefore, reducing preoperative and intraoperative neovascularization is crucial to the success of vitrectomy.6 Vascular endothelial growth factor (VEGF) has been shown to play a vital role in the development of PDR, and therefore, anti-VEGF agents are effective in reducing the growth of neovascular vessels in eyes with PDR.7,8
Conbercept is an anti-VEGF agent that has a higher binding affinity for all VEGF isoforms comparing with other anti-VEGF agents, and a longer half-life in the vitreous humour.9,10 The effect of Conbercept on the complications of vitrectomy for PDR has been frequently reported recently. A previous study showed that administration of Conbercept could be an effective complement to vitrectomy, resulting in reduced recurrence of vitreous haemorrhage (VH) and restoration of visual acuity in eyes with PDR.11
This study aimed to evaluate the efficacy of Conbercept administration before or during vitrectomy for PDR, comparing its effectiveness with Ranibizumab. Additionally, a bibliometric analysis of Conbercept-related literature was conducted to identify global trends, key contributors, sources, collaborations, thematic focuses, and evolving research impact.
Materials and Methods
The study adhered to the guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The literature search was conducted on PubMed, EMBASE, Cochrane Central Database, ProQuest, CNKI, and ScienceDirect databases, using keywords and terms combined as follows: “Conbercept”, “Vitrectomy”, and “Proliferative diabetic retinopathy”, from January 2012 to August 2024. The inclusion criterion for this review was that all studies performed the intravitreal injection of Conbercept for patients who underwent vitrectomy for PDR. We included all related original articles in the initial search and excluded case reports, review articles, and non-English language articles. The included records were then systematically evaluated following the standard process of meta-analysis. Two researchers assessed the methodological qualities of the included studies separately.
Data extraction and quality assessment were performed by two independent authors using a standardised extraction form, which included information on author names, year of publication, study design, follow-up, number of samples, mean age, sex, Conbercept regimen, best corrected visual acuity (BCVA) in logMAR scale, neovascular glaucoma, central retinal thickness (CRT), use of endodiathermy, use of silicone oil tamponade, and early and late postoperative VH. VH within 4 weeks after operation was defined as early VH, and the VH more than 4 weeks was defined as late VH. Additionally, the study involved three comparative analyses: preoperative administration of Conbercept intravitreal injection versus no treatment; intraoperative Conbercept injection immediately following vitrectomy completion versus no intervention; and preoperative Conbercept injection versus Ranibizumab injection.
To perform the meta-analysis, we used the software of RevMan 5.3 (Cochrane Collaboration) and StataMP 16 (StataCorp LLC). The randomised controlled trial and observational studies were assessed with Cochrane Risk of Bias Assessment Tool and Newcastle-OttawaScale (NOS, Table S1), respectively. The dichotomous data were pooled and measured with odds ratios (OR) and 95% confidence intervals (CI); the continuous data were pooled and analysed with mean difference (MD) and its standard deviation (SD). The Inconsistency index (I2) test was used to assess heterogeneity among studies. I2> 50% or P <0.10 indicated statistically significant heterogeneity. P values <0.05 were considered statistically significant. A regression-based Egger’s test was performed to assess the potential for small-study effects of continuous outcomes, and the Harbord test was performed for binary outcomes.
The search strategy for bibliometric analysis was performed as follows. Figure 1 presents the PRISMA flow diagram that was developed to guide the detection and inclusion of research studies for bibliometric analysis on Conbercept research. The search of the literature was carried out utilizing the Web of Science database, which provided results based on the following keyword string: ((((((((TS=(Conbercept)) OR TS= (VEGF Inhibitors)) AND TS= (Ocular Vasculopathies)) OR TS=(nAMD)) OR TS=(PCV)) OR TS=(DR)) OR TS=(RVO)) AND TS= (Anti-VEGF Therapy)) OR TS= (Intravitreal Injections). This search strategy was formulated to cover all the studies pertaining to Conbercept, VEGF inhibitors and related eye vascular diseases such as neovascular age-related macular degeneration (nAMD), polypoidal choroidal vasculopathy (PCV), diabetic retinopathy (DR), and retinal vein occlusion (RVO). The first search yielded a total of 18,382 records. Once a publication date filter from 2015 to 2025 was applied, the total studies available further narrowed down to 10,690. Further refinement by document type, restricting to articles, resulted in 8,474 records. Applying the Web of Science category filter to focus solely on ophthalmology yielded 5,262 records, and finally, limiting the language to English led to 5,065 eligible records. All of these were deemed highly relevant and included in the final analysis. This rigorous and structured filtering process ensured that only the most pertinent studies were considered for evaluating the trends, impact, and thematic focus of Conbercept research in ophthalmology.
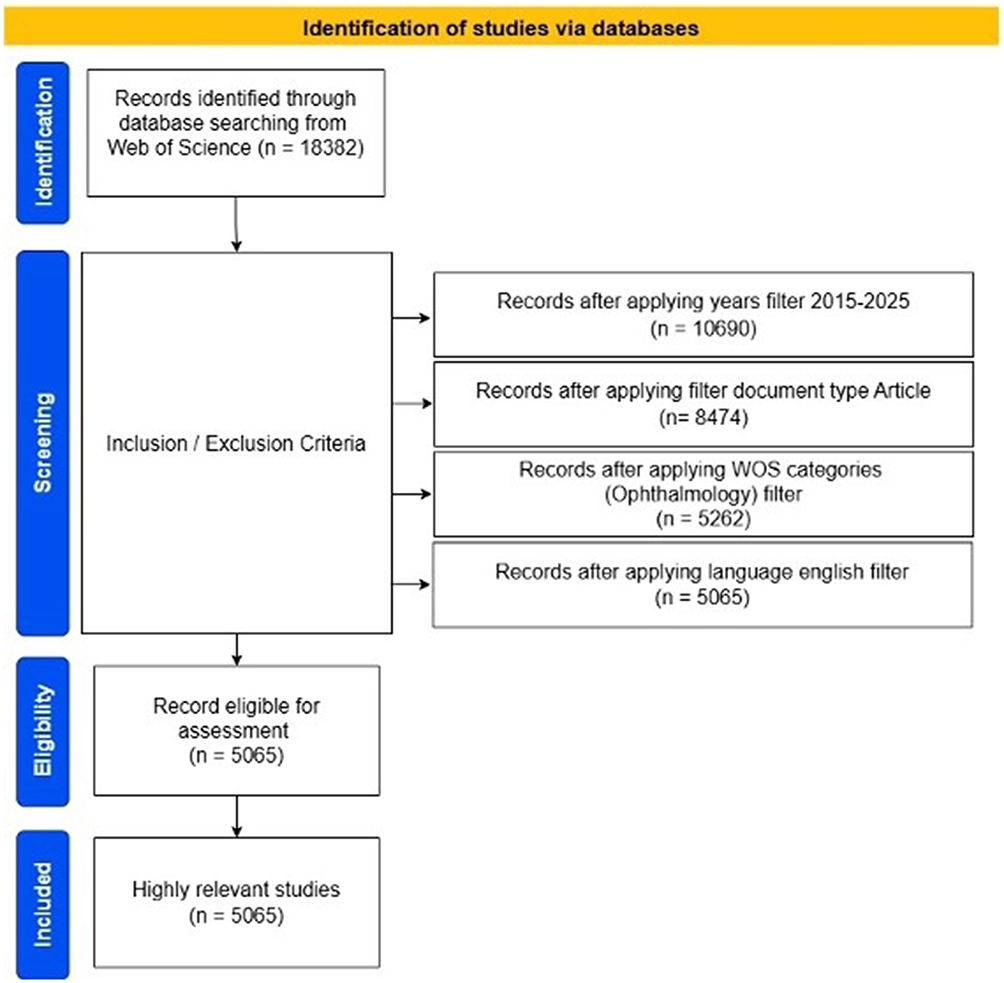 |
Figure 1 PRISMA flow diagram. |
Results (Meta-Analysis)
The comprehensive search in this meta-analysis yielded a total of 384 potential articles. After removing duplicates, only 250 articles remained. We excluded 232 articles after screening titles and abstracts. Thereafter, 18 potentially relevant articles remained. Upon assessing the full texts of these articles, we excluded two studies that did not have sufficient data. Sixteen studies were finally included for qualitative synthesis and meta-analysis (Figure 2). The Sixteen studies involved 1215 cases, of which 12 were randomized controlled studies and 4 were retrospective studies (Table S2).10–25
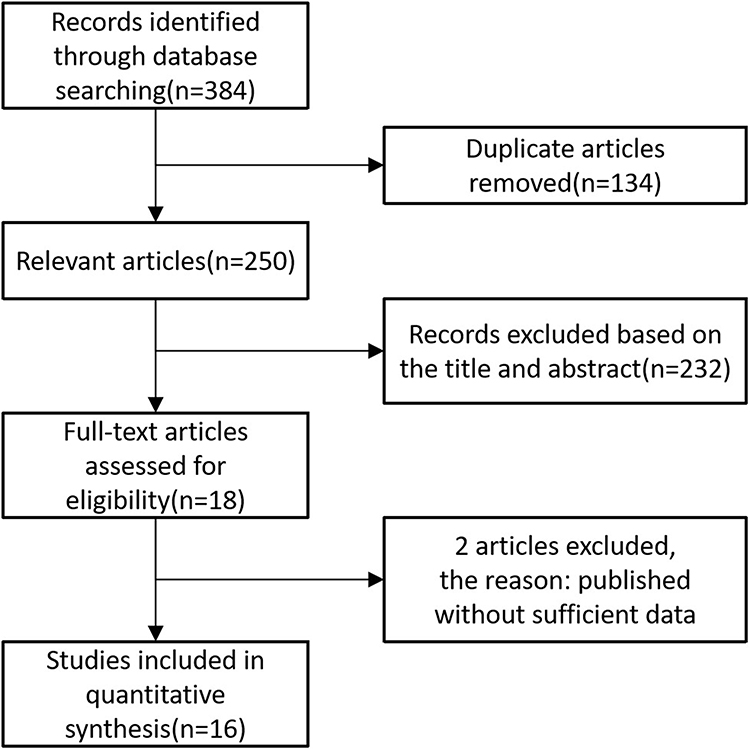 |
Figure 2 Flow chart of literature search and study selection. |
The timing of Conbercept administration varied across studies. In fourteen studies, 0.5 mg of Conbercept was administered 3 to 14 days prior to vitrectomy, while in two studies, it was given immediately after the procedure. In the control groups, intravitreal Ranibizumab was administered in five studies, whereas no intravitreal injection was given in the remaining eleven studies.
The mean age of the participants in the studies ranged from 50 to 60 years, and males were almost equally distributed among the studies. The average NOS score for six cohort studies was 6.5±0.4, indicating that the studies were of high quality.
Intravitreal Injection of Conbercept versus no Injection Control Before Vitrectomy
Best Corrected Visual Acuity
In our study, baseline BCVA was similar in both groups (MD = 0.04, 95% CI –0.06 to 0.14, P =0.41) (Figure 3A). The Conbercept group showed greater BCVA improvement than the control group at the one-month (MD = –0.18, 95% CI –0.23 to –0.13, P<0.01), three-month (MD = –0.19, 95% CI –0.25 to –0.13, P <0.01), and six-month (MD = –0.36, 95% CI –0.45 to –0.28, P<0.01) follow-ups (Figure 3B).
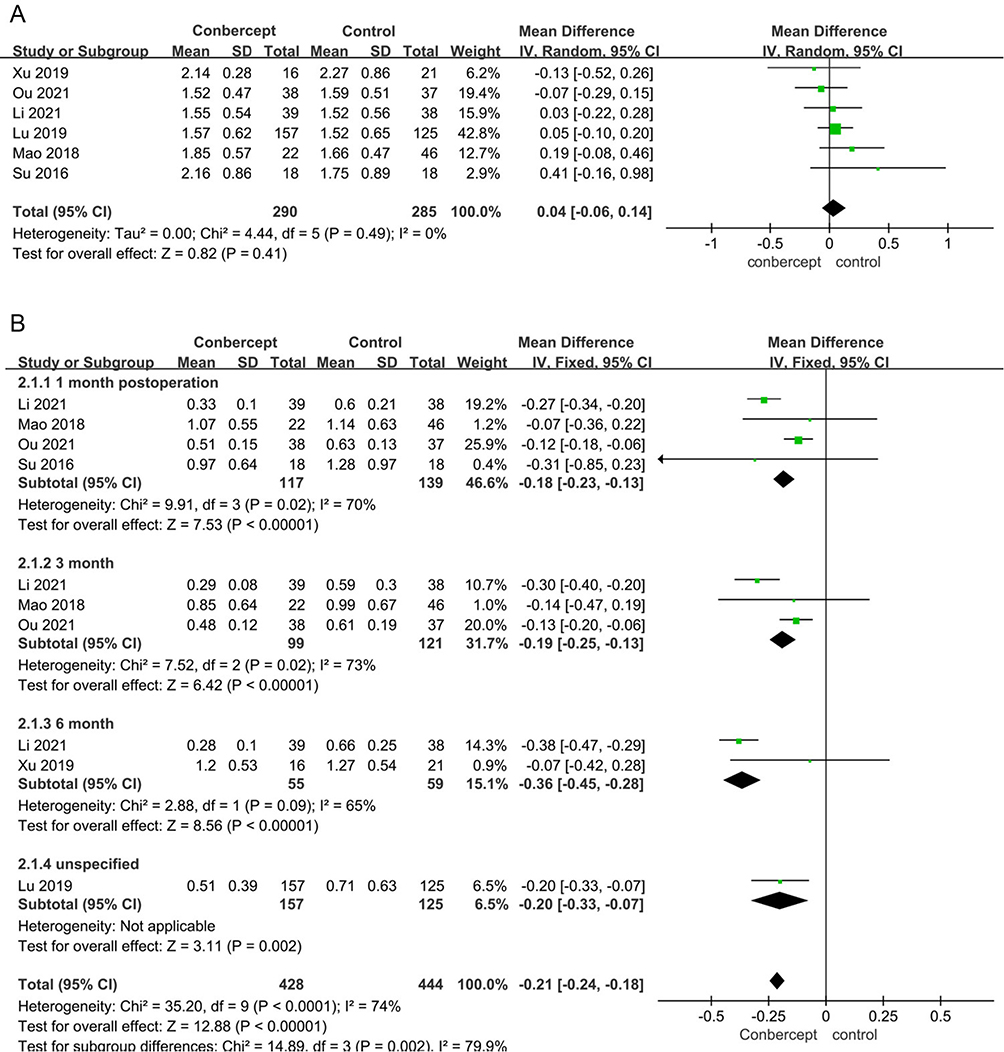 |
Figure 3 BCVA in patients of intravitreal Conbercept and no treatment before vitrectomy of proliferative diabetic retinopathy. (A) The mean change in best corrected visual acuity (logMAR units) from baseline. (B) The mean change in best corrected visual acuity (logMAR units) in the Conbercept group on 1-, 3-, and 6-month follow-up. |
Intraoperative Outcomes and Recurrence of Vitreous Haemorrhage
Intraoperative bleeding (OR = 0.12, 95% CI 0.07 to 0.21, P <0.01), use of endodiathermy (OR = 0.26, 95% CI 0.15 to 0.47, P <0.01), silicone oil tamponade (OR = 0.50,95% CI 0.35 to 0.73, P < 0.01) and iatrogenic break (OR = 0.25, 95% CI 0.13 to 0.48, P <0.01) were less frequent in the Conbercept group than in the control group (Figure 4). Cases of early (OR = 0.22, 95% CI 0.13 to 0.37, P <0.01) and late (OR = 0.53, 95% CI 0.28 to 0.99, P = 0.05) postoperative VH were less in the Conbercept group than in the control group (Figure 5).
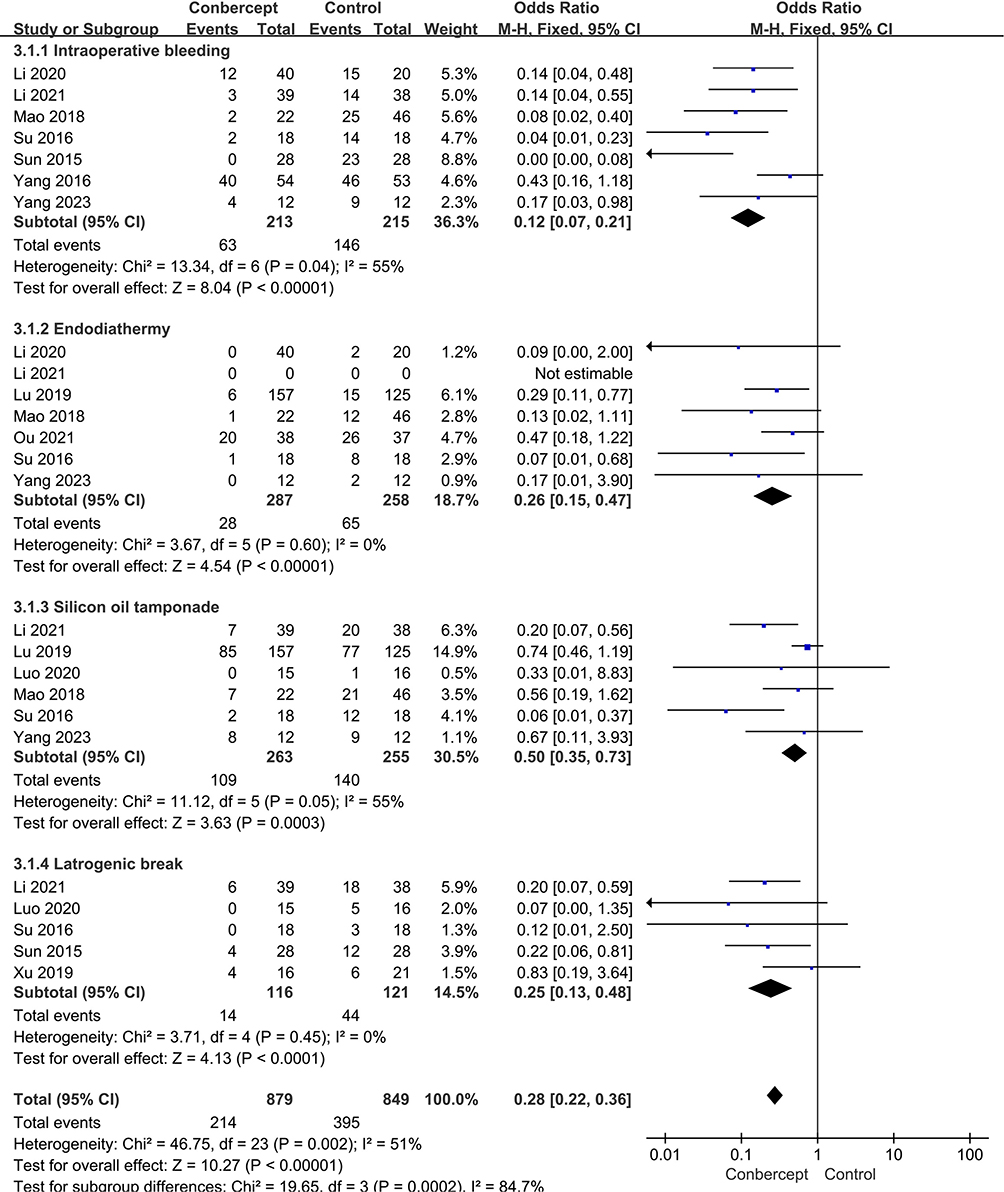 |
Figure 4 The outcomes of endodiathermy and silicone oil tamponade along with intraoperative bleeding in patients of intravitreal Conbercept and no treatment before vitrectomy of proliferative diabetic retinopathy. |
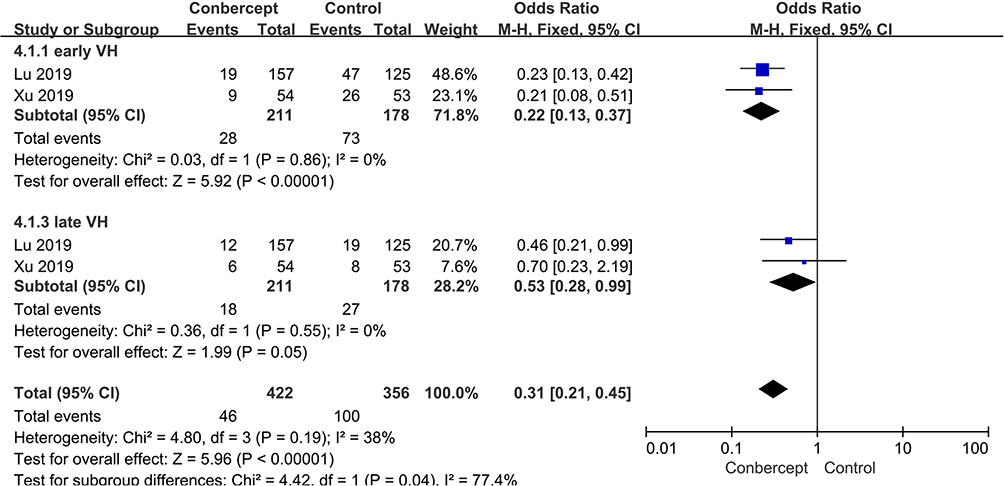 |
Figure 5 Early and late vitreous hemorrhage recurrence in patients of intravitreal Conbercept and no treatment before vitrectomy of proliferative diabetic retinopathy. |
Intravitreal Injection of Conbercept versus Ranibizumab Before Vitrectomy
Best Corrected Visual Acuity
The mean BCVA (logMAR)of both groups was similar at baseline (MD = 0.01, 95% CI –0.11 to 0.13, P = 0.87) and at follow-up (MD = –0.01, 95% CI –0.10 to 0.08, P = 0.85) (Figure 6).
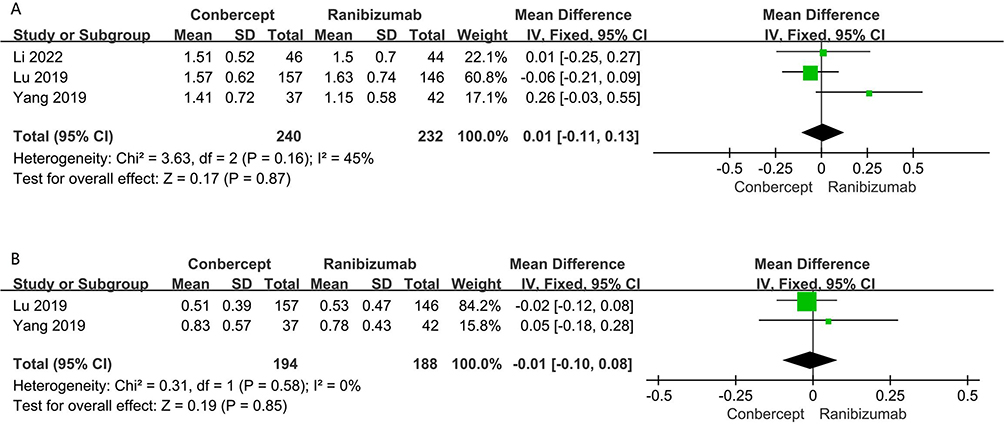 |
Figure 6 BCVA logMAR scale in patients of intravitreal Conbercept and Ranibizumab before vitrectomy of proliferative diabetic retinopathy. (A) Baseline BCVA. (B) BCVA improvement during follow-up. |
Intraoperative Outcomes and Postoperative Neovascular Glaucoma
Iatrogenic retinal breaks (OR = 1.11, 95% CI 0.52 to 2.36, P = 0.78), intraoperative use of endodiathermy (OR = 0.89, 95% CI 0.46 to 1.69, P = 0.71), and the use of silicone oil tamponade (OR = 0.83, 95% CI 0.57 to 1.22, P = 0.35) were similar in both groups (Figure 7). The incidence of neovascular glaucoma was not significantly different between the two groups (OR = 0.48, 95% CI 0.14 to 1.63, P = 0.24) (Figure 8).
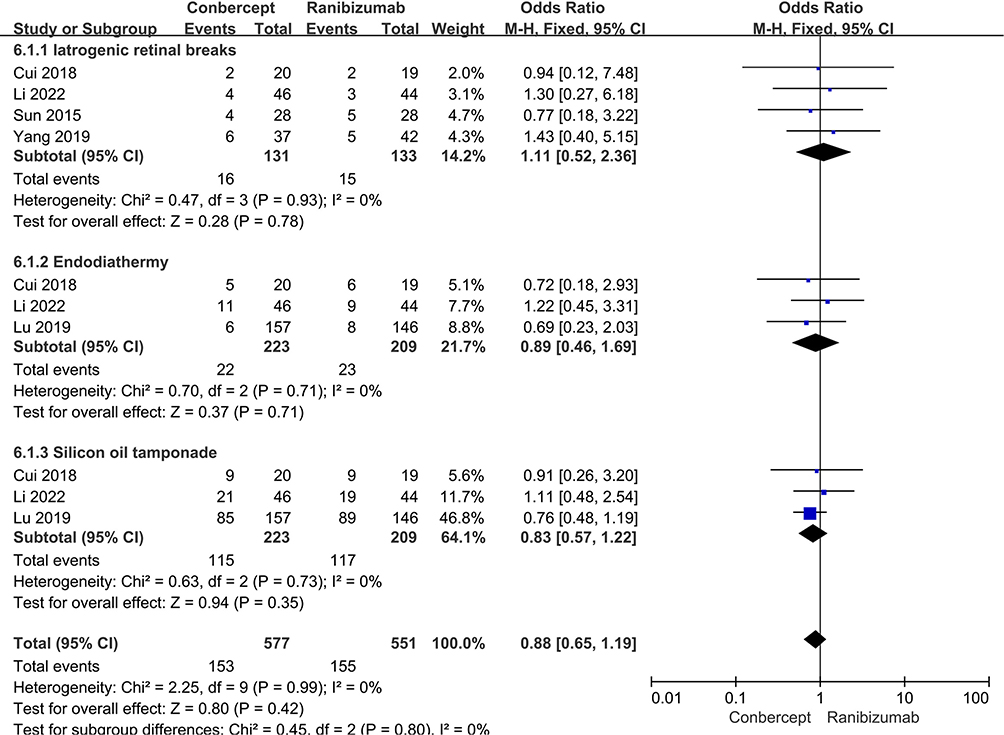 |
Figure 7 The outcomes of iatrogenic retinal breaks, endodiathermy and silicone oil tamponade in patients of intravitreal Conbercept and Ranibizumab before vitrectomy of proliferative diabetic retinopathy. |
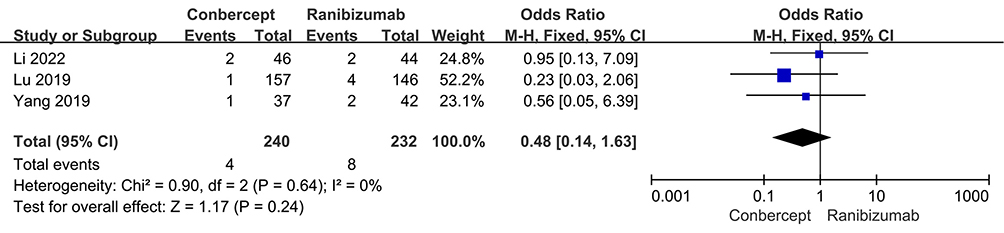 |
Figure 8 Neovascularization glaucoma incidence in patients of intravitreal Conbercept and Ranibizumab before vitrectomy of proliferative diabetic retinopathy. |
Intravitreal Injection of Conbercept versus no Conbercept Control During Vitrectomy
Best Corrected Visual Acuity
Baseline BCVA was similar (MD = 0.14, 95% CI –0.20 to 0.47, P =0.42) (Figure 9A). Greater BCVA improvement was observed in the Conbercept group than in the control group at the one-week (MD = –0.29, 95% CI –0.41 to –0.16, P<0.01), one-month (MD = –0.25, 95% CI –0.37 to –0.13, P<0.01), three-month (MD = –0.28, 95% CI –0.40 to –0.15, P<0.01), and six-month (MD = –0.32, 95% CI –0.46 to –0.18, P<0.01) follow-ups (Figure 9B).
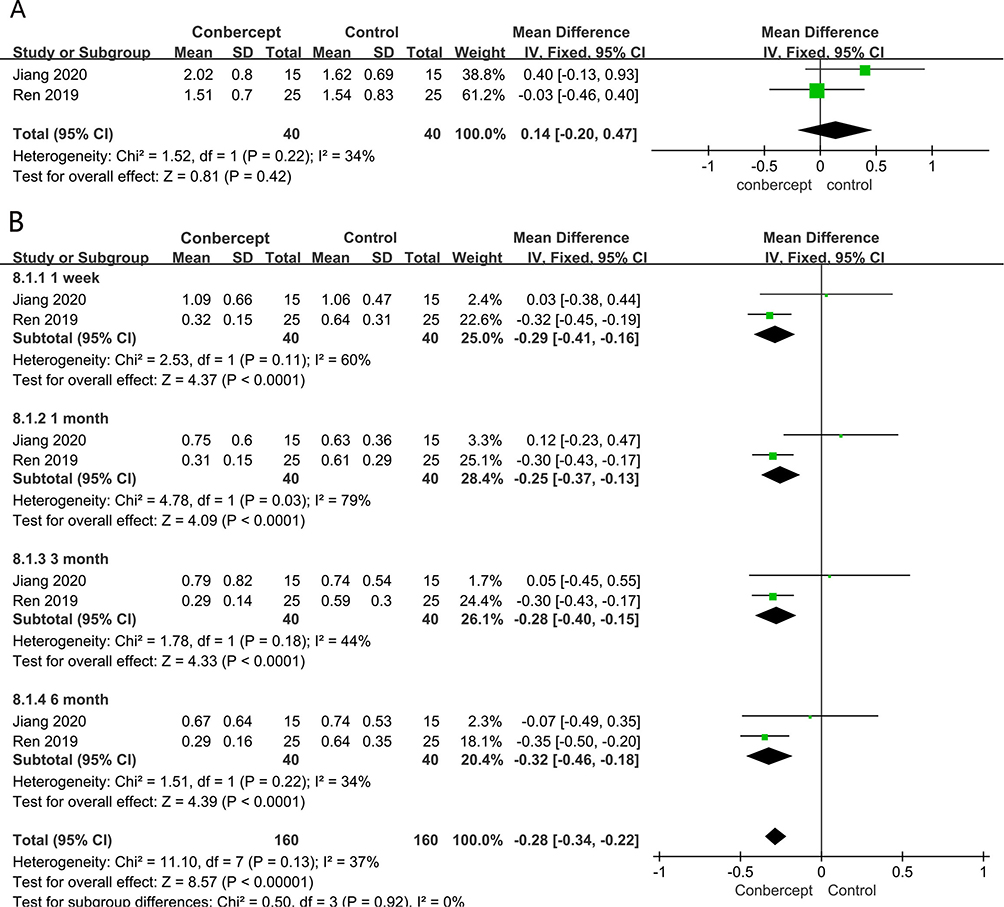 |
Figure 9 BCVA logMAR scale in patients of intravitreal Conbercept and no treatment during vitrectomy of proliferative diabetic retinopathy. (A) Baseline BCVA. (B) BCVA improvement on 1week, 1-month, 3-month and 6-month follow-up. |
Central Retinal Thickness
A greater decrease in CRT was observed in the Conbercept group than in the control group at the one-week (MD = –31.36, 95% CI –55.78 to –6.95, P=0.01), one-month (MD = –34.68, 95% CI –56.32 to –13.04, P=0.002), three-month (MD = –43.03, 95% CI –62.50 to –23.56, P<0.01), and six-month (MD = –35.15, 95% CI –52.35 to –17.95, P<0.01) follow-ups (Figure 10).
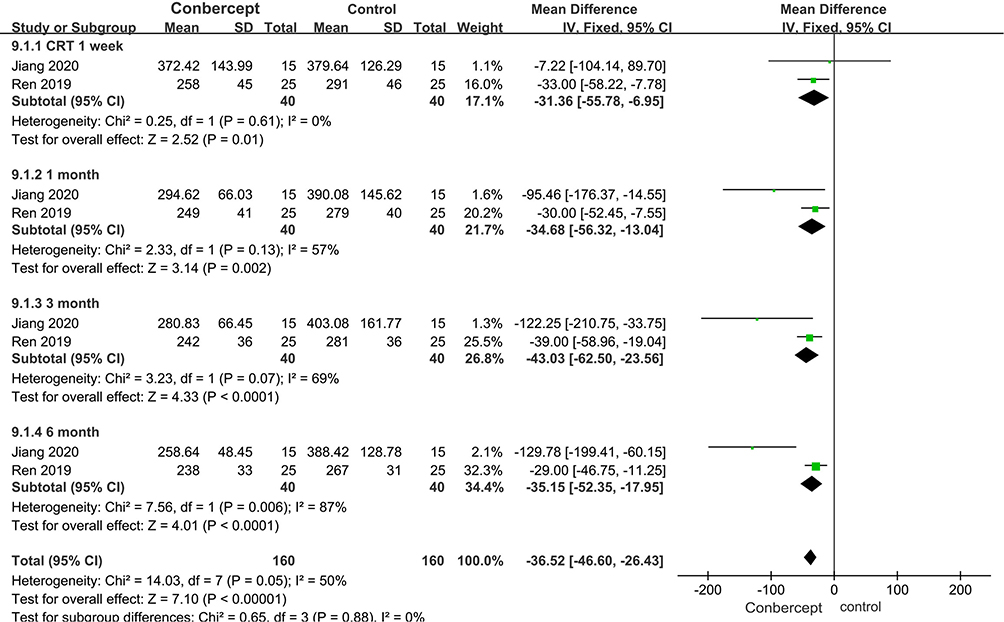 |
Figure 10 CRT changes on 1-week, 1-month, 3-month and 6-month follow-up in patients of intravitreal Conbercept and no treatment during vitrectomy of proliferative diabetic retinopathy. |
Recurrence of Vitreous Haemorrhage
A higher VH recurrence was observed in the control group than in the Conbercept group at the one-week (MD = 0.62, 95% CI 0.09 to 4.34, P=0.63), one-month (MD = 0.30, 95% CI 0.03 to 3.05, P=0.31), three-month (MD = 0.27, 95% CI 0.05 to 1.45, P=0.13), and six-month (MD = 0.19, 95% CI 0.04 to 0.98, P=0.05) follow-ups (Figure 11).
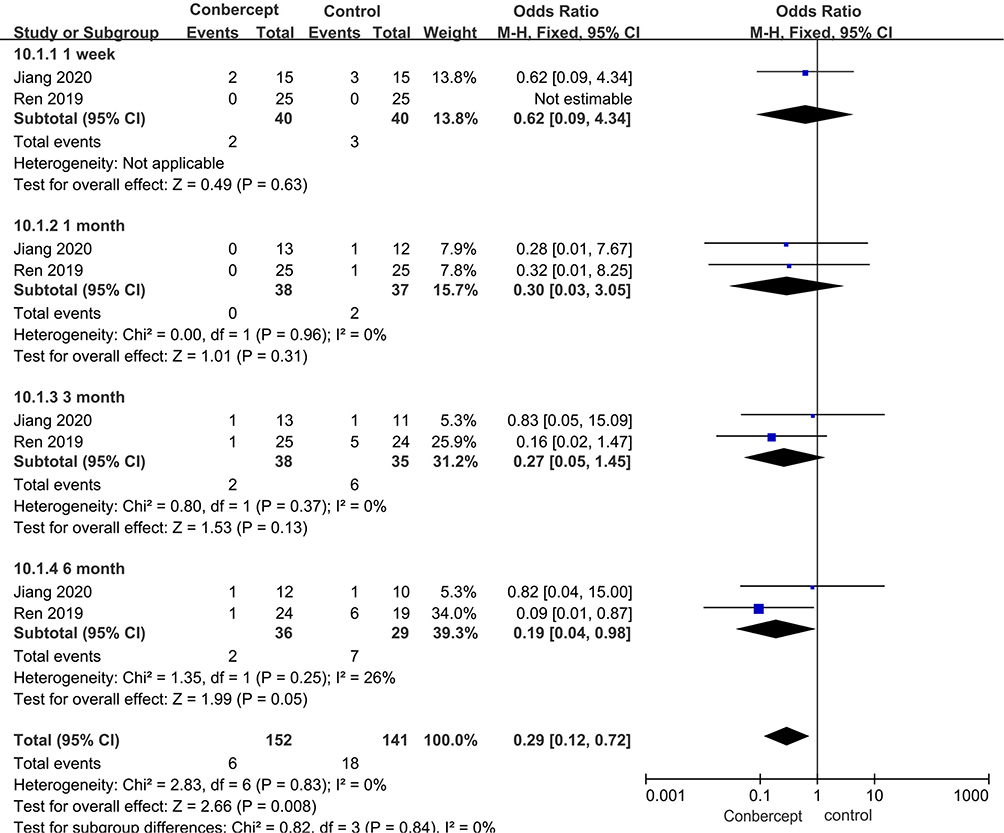 |
Figure 11 Vitreous hemorrhage recurrence on 1-week, 1-month, 3-month and 6-month follow-up in patients of intravitreal Conbercept and no treatment during vitrectomy of proliferative diabetic retinopathy. |
Publication Bias
Regression-based Harbord’s test demonstrated no indication for small-study effects of the use of endodiathermy (P = 0.16), use of silicone oil tamponade (P =0.49), and intraoperative bleeding (P = 0.09), indicating that the included studies were of high quality. We could not use Egger’s test for continuous outcomes due to the insufficient data available for each calculation.
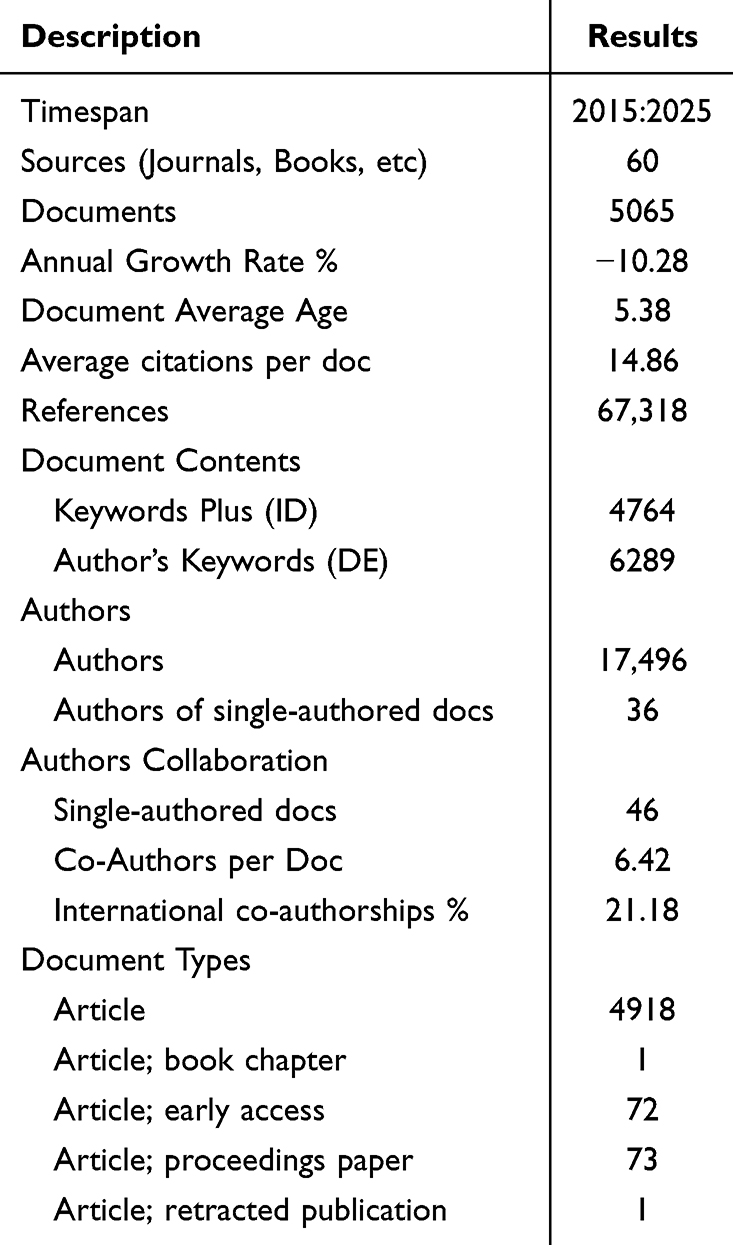 |
Table 1 Main Information About Data on Conbercept Research Using Biblioshiny |
Results (Bibliometric Analysis)
Table 1 provides a comprehensive overview of the bibliometric data on Conbercept research between 2015 and 2025. A total of 5,065 documents were published across 60 sources, with a −10.28% annual growth rate, indicating a decline in research output over the period. The average age of documents is 5.38 years, with each document receiving an average of 14.86 citations. In total, these documents have referenced 67,318 sources. The research includes 4,764 “Keywords Plus” and 6,289 “Author’s Keywords” with 17,496 authors contributing to these publications. Single-authored documents are rare, comprising only 46 documents, while the average number of co-authors per document is 6.42, with 21.18% of the collaborations being international. The majority of documents are articles (4,918), with smaller numbers of book chapters, early access articles, proceedings papers, and retracted publications.
Figure 12 illustrates the publication trend and the corresponding mean total citations per article for Conbercept research from 2015 to 2025. The blue bars represent the number of documents published each year, showing a peak in 2020 with 564 publications. However, there is a clear downward trend in the number of publications after 2020, culminating in just 174 documents by 2025. On the other hand, the orange line shows the mean total citations per article, which starts high in 2015 at 29.59 but gradually decreases over the years, reaching only 0.22 by 2025. This suggests that while the volume of publications initially increased, the citations per article have decreased significantly, indicating a potential shift in the impact or relevance of more recent research.
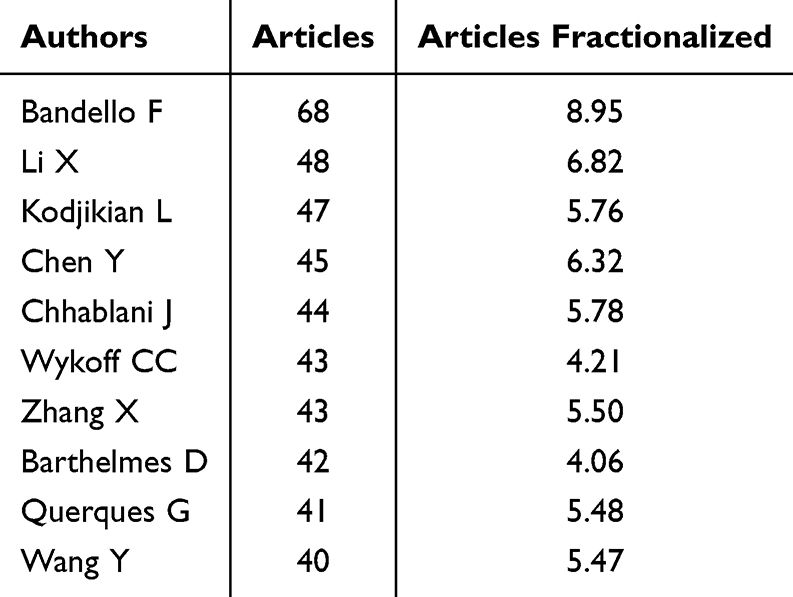 |
Table 2 Top Relevant Authors on Conbercept Research Using Biblioshiny |
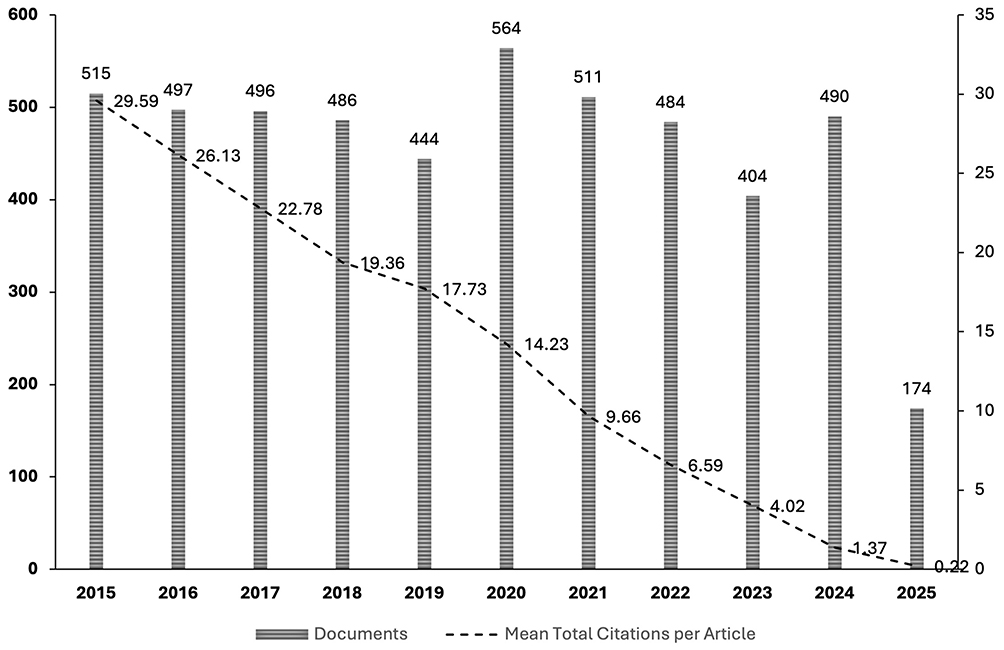 |
Figure 12 Publication trend over time using Biblioshiny. |
Table 2 highlights the top relevant authors in Conbercept research, providing both the number of articles they have published and the fractionalized contribution of their work to the field. Among the leading contributors, Bandello F stands out with 68 articles, which accounts for 8.95% of all the research published on Conbercept. Following closely, Li X has published 48 articles, contributing 6.82% to the overall body of work. Kodjikian L is another prominent author with 47 articles, which represent 5.76% of the total.
Other significant authors in this field include Chen Y with 45 articles (6.32%), Chhablani J with 44 articles (5.78%), and Wykoff CC and Zhang X, both of whom have published 43 articles, contributing 4.21% and 5.50%, respectively. Barthelmes D follows with 42 articles, representing 4.06% of the total, while Querques G has 41 articles (5.48%). Lastly, Wang Y has published 40 articles, accounting for 5.47% of the research.
These authors play a central role in the development of Conbercept research, demonstrating substantial involvement in the key studies and clinical trials that explore the use of VEGF inhibitor Conbercept in treating ocular vasculopathies. Their prolific contributions underscore their influence in shaping the current landscape of ocular disease management, particularly in the area of retinal disorders.
Figure 13 presents the publication trend from various top sources on Conbercept research over time, showing annual occurrences of articles in prominent journals. The graph tracks the publications from five major journals: BMC Ophthalmology, European Journal of Ophthalmology, Graefe’s Archive for Clinical and Experimental Ophthalmology, Investigative Ophthalmology & Visual Science, and Retina - The Journal of Retinal and Vitreous Diseases.
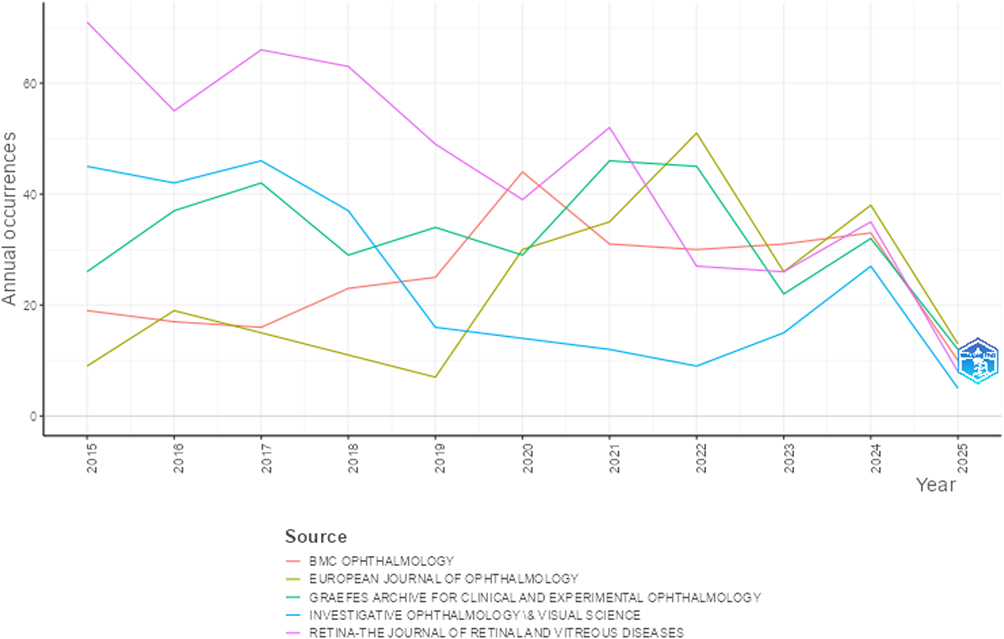 |
Figure 13 Top source publishing on Conbercept research using Biblioshiny. |
From the graph, it is evident that BMC Ophthalmology (depicted in green) consistently published the most articles on Conbercept, with a notable peak in 2020, followed by a decline in the subsequent years. European Journal of Ophthalmology (represented by red) also experienced a significant increase in publications around 2019 and 2020, after which its publications began to decrease. Graefe’s Archive for Clinical and Experimental Ophthalmology (yellow) showed a steady rise in publications until 2020, after which the trend started to level off. Investigative Ophthalmology & Visual Science (blue) maintained moderate publication levels with minor fluctuations, while Retina - The Journal of Retinal and Vitreous Diseases (purple) had the highest peaks in 2021 and 2022, but the number of annual publications started to decrease significantly in 2023 and 2024.
The analysis highlights that, while all the top sources initially had strong contributions, the number of publications on Conbercept began to dwindle in recent years, reflecting the broader trend of diminishing research output on the subject. BMC Ophthalmology and European Journal of Ophthalmology were the most consistent sources, although the overall trend shows a decline across all journals, especially towards 2025.
Figure 14 represents the co-authorship network analysis based on the Conbercept research, with the criteria of a minimum of 10 documents and 10 citations per author. Out of the 18,857 authors, 275 authors met these thresholds, forming a network of 266 items and 1730 links, with a total link strength of 5683. This visualization, created using VoSviewer, categorizes the authors into 15 distinct clusters.
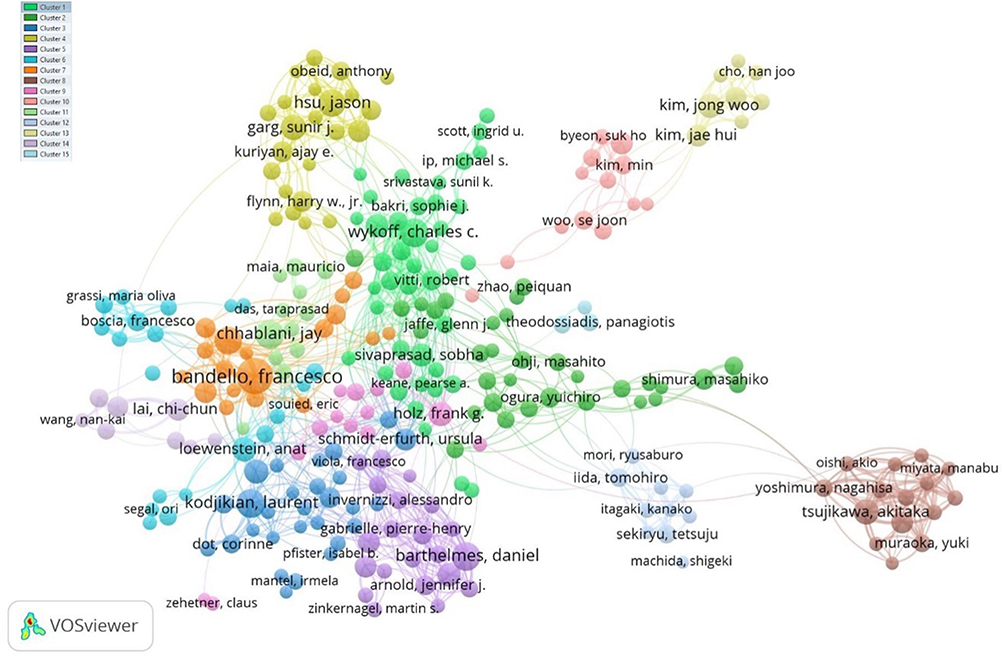 |
Figure 14 Co-authorship network visualization. |
The nodes (authors) are organized by color, with each color denoting a distinct cluster of collaborators. Central nodes denote the strong collaboration ties Franceso Bandello and Jay Chabklani possess in the field of Conbercept research. These authors are placed together at the edges of their individual clusters, and the lines connecting them indicate the co-authorships and collaborations they hold with other authors in the network, who constitute their clusters. The author’s activity and contribution in the network is indicated by the size of the node, which increases proportionally with more publications and impact, thus node size increases with increase in network impact.
The network has revealed the most well-connected research groups, and it can be seen that there are definitive collaborations between the authors in the same cluster. For example, green cluster with verifiable links within the cluster and collaboration with prominent authors such as Charles Wykoff is another reason as to why they stand out. Other distinct colors such as purple and red represent smaller features that still suggest these are teams of researchers that are less connected but still important, and thus make the cluster is less densely connected.
This visualization offers important perspectives concerning the Conbercept research landscape, which includes prominent authors, collaborative networks, and how research is integrated within those networks. It shows important contributors to the literature, as well as how the literature is fragmented among various collaboration clusters.
Using VOSViewer, Figure 15 illustrates the network of major institutions involved in Conbercept research. This analysis considers organizations that have made a minimum contribution of 10 documents and have received at least 10 citations. Out of 4,915 organizations that were analyzed, only 315 satisfied the criteria. The network has 315 items, 5 clusters, and 20,297 links, with a total link strength of 56,074. In the visualization, each node corresponds to an organization, with the node size reflecting the publication and citation volume. Various colors signify different clusters, denoting the cooperative links among institutions in Conbercept research. For example, Moorfields Eye Hospital and Johns Hopkins University are shown to be central nodes, signifying their considerable contribution to the research. The network showcases the collaborative nature of Conbercept research globally, with major institutions from Europe, North America, and Asia prominently participating.
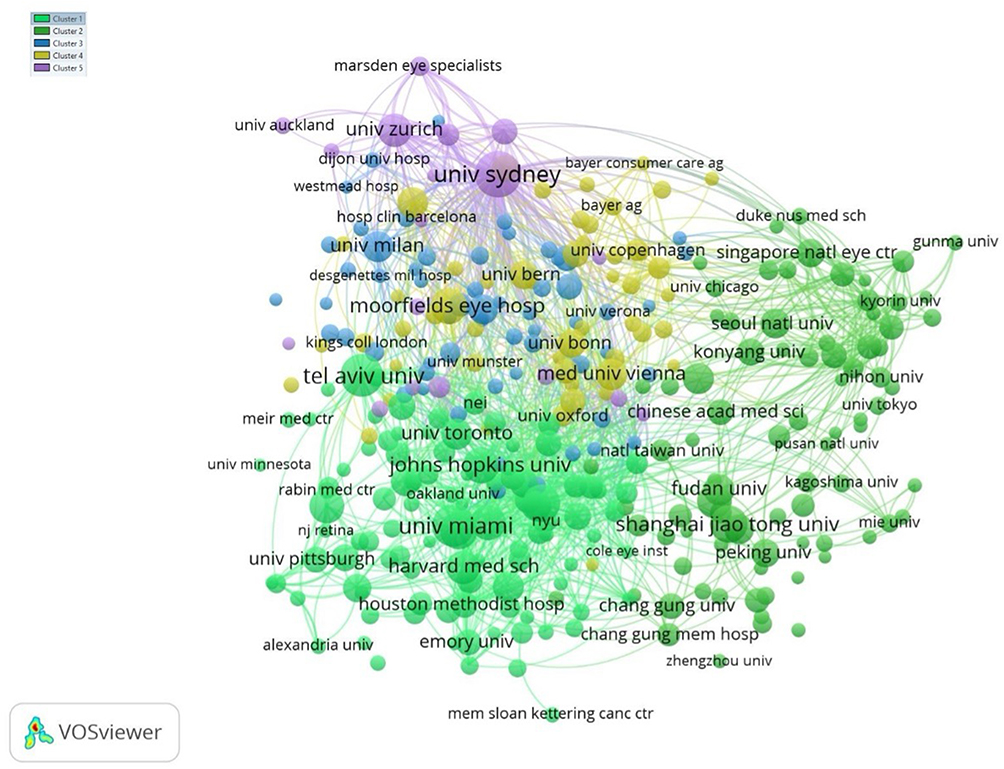 |
Figure 15 Network of key organizations in Conbercept research. |
A significant number of links and a higher-than-average link strength represent an active research community where institutions work together on Conbercept studies. This exemplifies the interdisciplinary collaboration toward the understanding of VEGF inhibitors in ocular vasculopathies. This network reveals the most important organizations in Conbercept research along with their relations, which are essential for progress in the field.
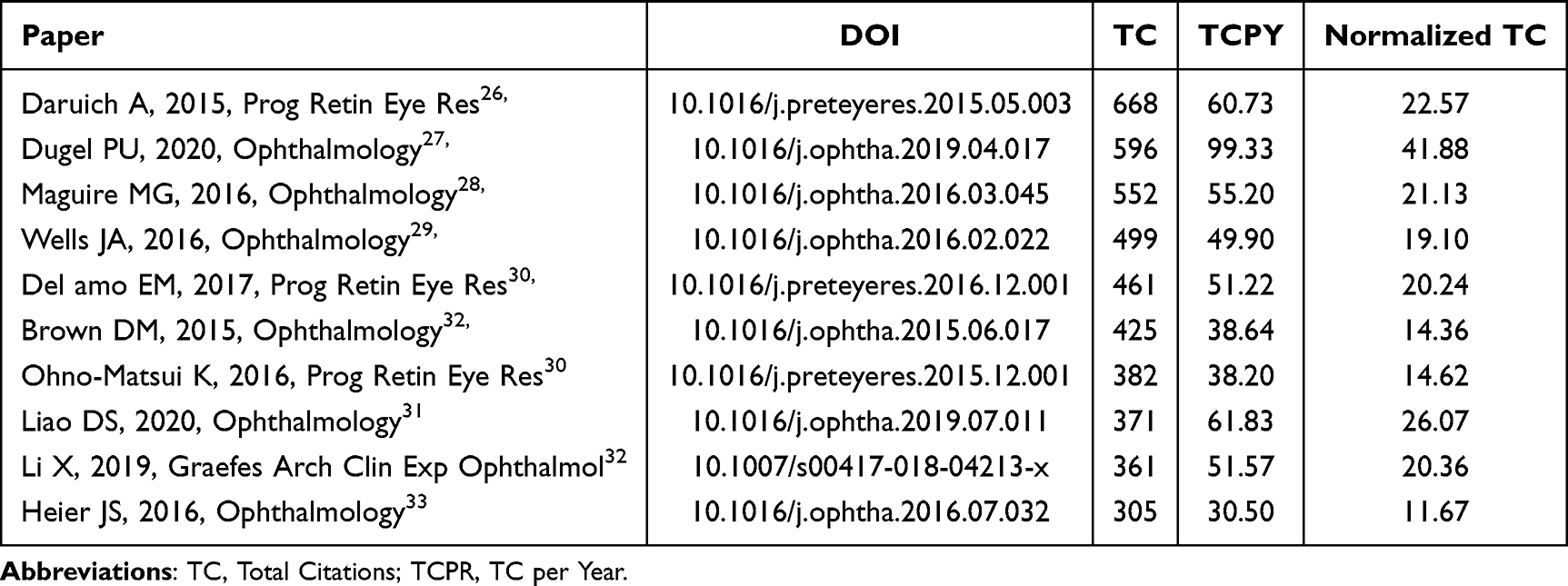 |
Table 3 Top Cited Papers on Conbercept Using Biblioshiny |
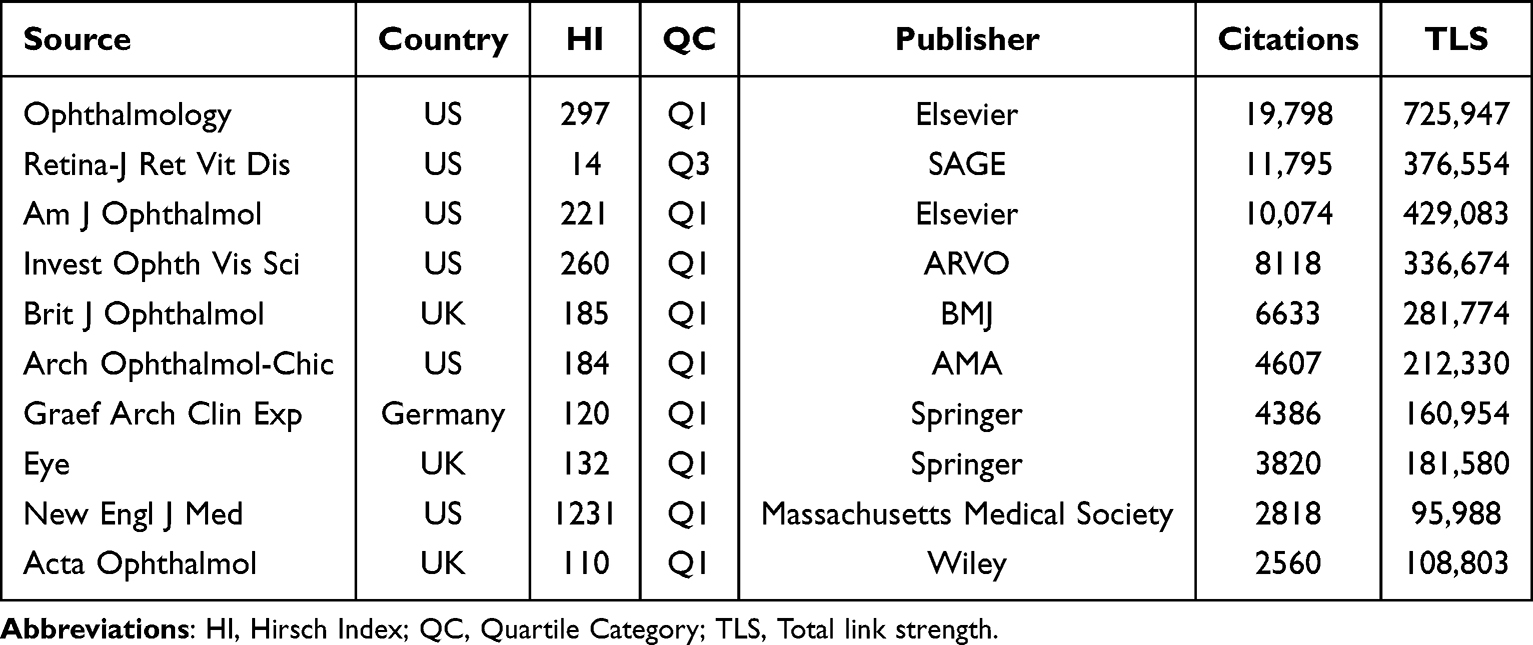 |
Table 4 Most Cited Journals in Conbercept Research |
Table 3 displays the top ten most cited papers on Conbercept in relation to their impact in the ophthalmology research community as measured by total citations, citations per year, and normalized total citations. The most cited paper is by Daruich et al (2015)26 in Progress in Retinal and Eye Research with total citations equaling 668, and a normalized TC of 22.57, while Dugel et al (2020)27 in Ophthalmology outdid others for his normalized TC of 41.88. Other notable contributions include Maguire et al (2016),28 Wells et al (2016),29 and Del Amo et al (2017)30, each surpassing 450 citations, which shows the sustained scholarly interest. The data processed through Biblioshiny indicates an increasing interest in researching Conbercept, particularly in more recent studies like Liao et al (2020),31 which also had high annual and normalized citation rates, indicating continuous relevancy in research.
Figure 16 shows the citation network map produced in VOSviewer, showing the most important references in Conbercept research and how they are interconnected. Of a total of 67,264 cited references, only 755 received a minimum of 20 citations, and they are represented in 10 different clusters, each colored differently. The network features 59,358 citation links with a total link strength of 180,919, signifying strong interconnectivity among the cited works. Central and highly cited nodes like Rosenfeld PJ (2006, New England Journal of Medicine),32 Boyar DS (2014, Ophthalmology),33 and Nguyen QD (2012, Ophthalmology)34 appear prominently, suggesting their foundational role in guiding subsequent research. The proximity of items and clustering reveals topical groupings and thematic focuses, such as anti-VEGF therapy, macular degeneration, and retinal diseases. Outlier nodes like Munier FL (2012)35 are positioned distantly, indicating relatively isolated citation patterns or niche subtopics. Overall, the visualization captures the structure of scholarly influence and the evolution of key research themes in ophthalmology related to Conbercept.
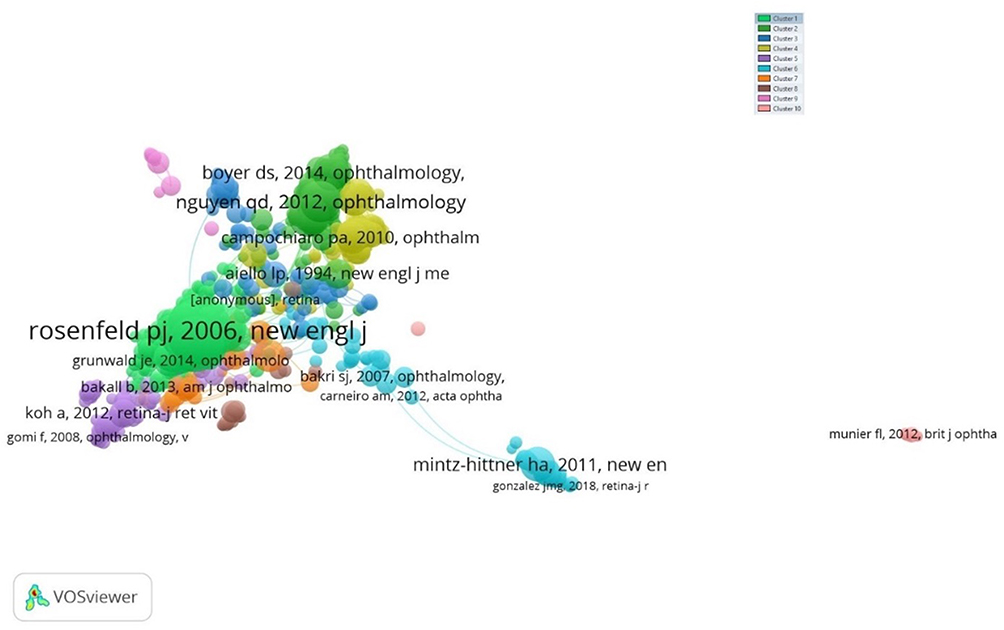 |
Figure 16 Citation network of key papers. |
Table 4 presents the most cited journals contributing to Conbercept research, based on a VOSviewer analysis of 7,919 cited sources, where 509 met the citation threshold of 20. These journals are grouped into five clusters and collectively form 69,074 links with a total link strength of 3,089,867, indicating a dense citation network. Ophthalmology (Elsevier, US) dominates the landscape with 19,798 citations and the highest total link strength (725,947), reflecting its central role in publishing impactful Conbercept-related studies. It is followed by Retina – The Journal of Retinal and Vitreous Diseases (SAGE, US), which despite a lower H-Index (14), amassed 11,795 citations, showcasing its niche relevance. Other top-tier Q1 journals such as American Journal of Ophthalmology, Investigative Ophthalmology & Visual Science, and British Journal of Ophthalmology also feature prominently with high citation counts and robust link strengths, underlining their influence. International journals like Graefe’s Archive for Clinical and Experimental Ophthalmology (Germany) and Eye (UK) further broaden the scope. Notably, New England Journal of Medicine stands out with a high H-Index of 1231 but lower citation count (2,818), suggesting foundational but less frequently cited contributions in this specific field. Overall, the data underscores a strong concentration of impactful research published in high-ranking, primarily Q1 ophthalmology journals.
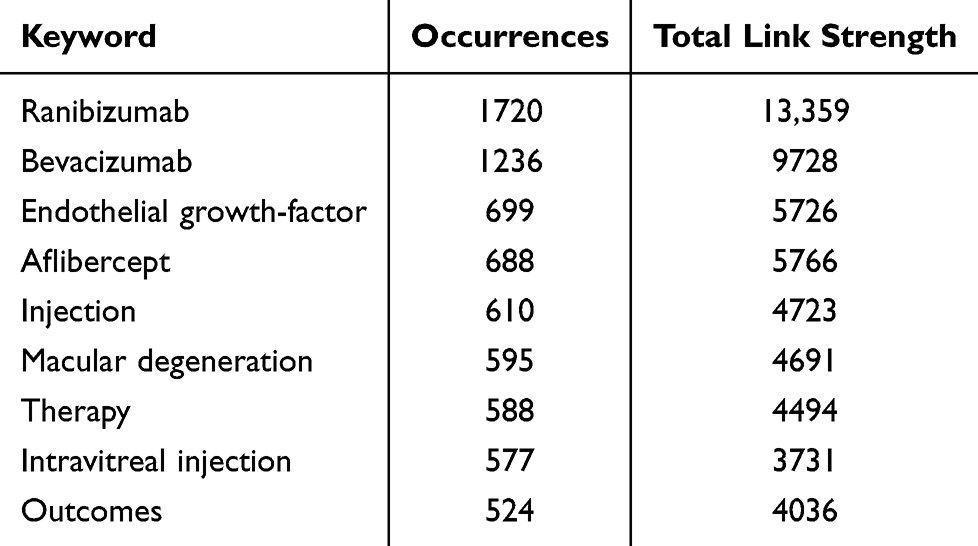 |
Table 5 Most Frequent Keywords in Conbercept Research Using VOSViewer |
Table 5 displays the most frequently occurring keywords in Conbercept-related research, as visualized using VOSviewer. The keyword “ranibizumab” is leading with 1,720 occurrences and the highest total link strength of 13,359 which indicates how central it is for anti-VEGF treatment discussions. “Bevacizumab” comes second with 1,236 occurrences and link strength of 9,728 which captures the degree of co-citation and topical overlap. Other such as “endothelial growth factor” “aflibercept” and “injection” also made Keywords ragged high presence capturing the biological target and common treatment associated with Conbercept. Macular degeneration, intravitreal injection, and integration of clinical diagnosis also show high recurrence pointing out the importance of drug in retinal diseases. The word “outcomes” also has significance as it depicts interest in research about clinical and treatment results. All of these highlighted keywords suggest that there is focus in anti-VEGF literature describing the relevance of age-related macular degeneration and other similar diseases.
Figure 17 visualizes the keyword co-occurrence network in Conbercept research, based on 9,283 identified keywords, of which 658 met the minimum occurrence threshold of 10. The network is grouped into 10 distinct clusters, shown in different colors, forming 38,573 links with a total link strength of 134,007, reflecting strong interconnectivity among research topics. Dominant keywords such as “ranibizumab” “endothelial growth-factor” “macular degeneration” “intravitreal injection” and “outcomes” appear in large nodes at the center of the map, highlighting their central role in the thematic structure of the field. These core terms are surrounded by related concepts like “diabetic macular edema” “retinopathy of prematurity” “glaucoma” and “monotherapy” which branch into subtopics across various clusters. The dense clustering around anti-VEGF agents and retinal disease treatments indicates a concentrated research focus on pharmacologic interventions and their clinical outcomes. The co-occurrence map provides a comprehensive overview of how key themes are interconnected, with terms like “COVID-19” “real-world” and “adherence” suggesting emerging and applied research directions within the broader field of ophthalmic therapeutics.
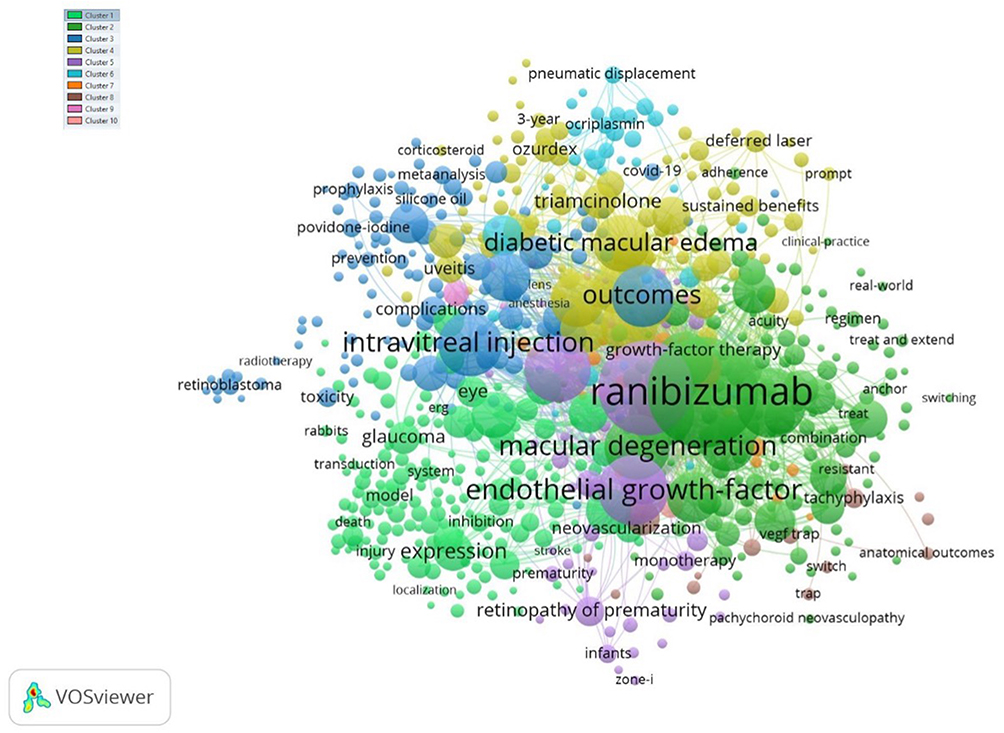 |
Figure 17 Keyword co-occurrence network. |
Figure 18 presents a global collaboration map illustrating the top contributing countries in Conbercept research. The visualization, created using Biblioshiny, reveals the geographical distribution and international co-authorship links, with darker blue shades indicating higher publication volumes. The United States emerges as the leading contributor, depicted in the darkest blue, and functions as a central node interacting with many countries in Europe, Asia, and Oceania. China, Germany, the United Kingdom, and Australia also make notable contributions, underscoring their importance in the collaboration towards advancing ophthalmologic research. The network of red lines shows strong international collaborations, notably between North America, Western Europe, and East Asia. This collaboration reveals the Conbercept’s widespread scientific interest, research undertakings, and combined efforts towards its clinical applications. As is clear, countries from Africa and some regions of the Middle East tend to be less engaged, which highlights the need for fostering research engagement and knowledge exchange in future investigations.
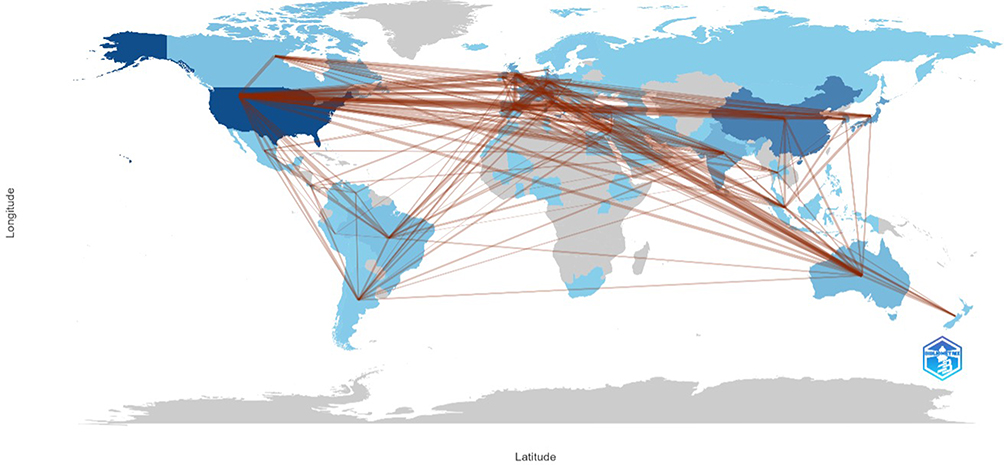 |
Figure 18 Top contributing countries in Conbercept research using Biblioshiny. |
Discussion
This meta-analysis evaluated the efficacy of administering Conbercept before or during vitrectomy for PDR and compared its efficacy with Ranibizumab. The results of this review showed that the patients in the Conbercept group had less intraoperative bleeding, less need for endodiathermy and silicone oil tamponade, and less recurrence of VH than patients in the control group. Preoperative Conbercept injection demonstrated strong effectiveness in preventing intraoperative and postoperative complications in these surgical cohorts. This high efficacy is associated with the strong affinity of Conbercept for all VEGF isoforms and its ability to suppress VEGF for up to one month on account of its longer half-life.12,14–25,36 However, there was no significant difference in BCVA changes recorded between patients injected with Conbercept and those injected with Ranibizumab in this study. This may be due to the lack of articles on studies conducted using the two groups in the present study. Moreover, the BCVA results in the present study were different from those of a previous study.22,25
Our present study showed that preoperative injection of Conbercept is associated with less intraoperative bleeding, less use of endodiathermy and silicone oil tamponade, and less recurrence of VH. Wang’s study reported that Conbercept could change the expression of long noncoding RNAs in the fibrovascular membrane, and its strong affinity for all VEGF isoforms was shown to reduce the symptoms of DR and its complications.26 However, there was no significant difference between the outcomes of the Conbercept and Ranibizumab groups in that study. While having a higher affinity and longer half-life, Conbercept achieved outcomes comparable to Ranibizumab and current evidence indicates similar efficacy, with no consistent superiority. Nevertheless, larger studies are needed to confirm the results of the difference between these agents.
Another finding in our present study demonstrated that intraoperative injection of Conbercept is associated with better BCVA improvement, decreased CRT, and less recurrence of VH. Two studies reported that administering Conbercept immediately after vitrectomy improves visual outcome, reduces the recurrence of VH, and decreases CRT.11,13–17 However, the postoperative administration of Conbercept lacks the advantages of the intraoperative administration of Conbercept, such as reduction of intraoperative bleeding and endodiathermy. Administration of Conbercept before and after vitrectomy should be considered for its advanced benefits in patients with severe PDR.
The limitations of this systematic review include reported results at different time intervals. The outcomes of follow-up intervals, especially preoperative outcomes, differ from one study to another. Therefore, pooling the relative data for the subgroup meta-analysis is difficult. Furthermore, comparative studies between Conbercept and other anti-VEGF agents remain scarce, potentially attributable to its predominant clinical employment being concentrated in China; existing evidence is limited to Conbercept versus Ranibizumab comparisons characterized by small sample sizes and abbreviated follow-up durations. More research on different anti-VEGF agents and follow-up intervals is needed to investigate whether Conbercept is superior to other anti-VEGF agents. This study focuses on the efficacy of vitrectomy with Conbercept for PDR rather than the general efficacy of Conbercept. Further studies are needed to investigate the efficacy of Conbercept.
This bibliometric analysis offers a comprehensive overview of the global research landscape on Conbercept, a VEGF inhibitor prominently used in treating ocular vasculopathies such as nAMD, DR, and RVO. The findings highlight not only the evolving trends in research output but also key contributors, sources, thematic focuses, and collaborative patterns that shape the field.
One of the most striking findings is the marked decline in the annual growth rate of Conbercept-related publications (−10.28%) over the 2015–2025 period, despite the initial surge in activity peaking around 2020. This may suggest a plateau in novel insights or a redirection of research efforts toward alternative therapies or next-generation anti-VEGF agents. Although publication volume has decreased, the average number of citations per document (14.86) indicates sustained academic interest, particularly for earlier studies that have established foundational knowledge in the field.
The authorial landscape shows a strong concentration of influential researchers, with contributors such as Bandello F, Li X, and Kodjikian L leading the field. Their substantial publication volume and frequent authorship of highly cited studies underscore their central role in advancing the clinical and pharmacologic understanding of Conbercept. Furthermore, the dense co-authorship and institutional collaboration networks indicate a mature and interconnected research ecosystem, with significant contributions from institutions in the United States, China, and Western Europe. These patterns reflect the global nature of Conbercept research and its translational relevance across diverse healthcare systems.
In terms of publication sources, high-impact ophthalmology journals, including Ophthalmology, Retina, and Investigative Ophthalmology & Visual Science, have been primary platforms for widely disseminating peer-reviewed research findings on Conbercept. These journals not only amplify the visibility of research findings but also ensure that clinically relevant studies reach a broad ophthalmologic audience. The dominance of top-tier journals suggests that the field has maintained rigorous scientific standards.
Thematic analysis through keyword co-occurrence revealed that research has centered primarily around established anti-VEGF agents such as ranibizumab, bevacizumab, and aflibercept, alongside Conbercept. Keywords like “macular degeneration” “intravitreal injection” and “clinical outcomes” emphasize the strong clinical orientation of this research domain. Interestingly, emerging themes such as “real-world evidence” and “adherence” point to a gradual expansion of focus beyond controlled clinical trials toward practical implementation and patient-centered outcomes.
Globally, although the United States and China dominate scholarly output, the underrepresentation of Africa and the Middle East underscores persistent inequities in research participation. This underlines the need for more inclusive international collaboration and capacity-building efforts to diversify contributions and perspectives in ophthalmology research.
Finally, the citation analysis confirms the enduring influence of early landmark studies. Papers by Daruich et al (2015)26 and Dugel et al (2020),27 among others, continue to anchor scholarly discourse, shaping both research direction and clinical practice. These high-impact works are central in the citation network and have fostered subsequent studies on the efficacy, safety, and comparative performance of Conbercept.
Conclusion
This meta-analysis revealed that administering Conbercept before vitrectomy for PDR reduces intraoperative and postoperative complications. And the use of Conbercept during vitrectomy also improves BCVA, decreases CRT, and reduces the recurrence of VH. A comparison of Conbercept and Ranibizumab injection before vitrectomy demonstrated no significant difference in their outcomes; however, more studies are needed to investigate the efficacy of using Conbercept before or during vitrectomy compared with other anti-VEGF agents. Overall, this bibliometric review elucidates the maturation and shifting dynamics of Conbercept research over the past decade. While the field shows signs of declining output, its foundational influence, international reach, and alignment with clinical priorities underscore its ongoing relevance. Future research could benefit from addressing geographical gaps and expanding into new domains such as long-term outcomes, biosimilars, and cost-effectiveness analyses in real-world settings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by the National Natural Science Foundation of China (Grant No.82160202), Tianjin Education Commission Research Program Project (Grant No. 2023ZD016), Bethune Langmu Young and middle-aged Scientific research fund (Grant No. BJ-LM2018011J).
Disclosure
All authors have no financial disclosures and potential conflicts of interest relevant to this article.
References
1. Yau JW, Rogers SL, Kawasaki R. et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556–564. doi:10.2337/dc11-1909
2. Zhou J, Liu Z, Chen M, et al. Concentrations of VEGF and PlGF Decrease in Eyes After Intravitreal Conbercept Injection. Diabetes Ther. 2018;9(6):2393–2398. doi:10.1007/s13300-018-0527-9
3. Bressler SB, Qin H, Melia M, et al. Exploratory analysis of the effect of intravitreal ranibizumab or triamcinolone on worsening of diabetic retinopathy in a randomized clinical trial. JAMA Ophthalmol. 2013;131(8):1033–1040. doi:10.1001/jamaophthalmol.2013.4154
4. Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis. 2015;2(1):17. doi:10.1186/s40662-015-0026-2
5. Manabe A, Shimada H, Hattori T, Nakashizuka H, Yuzawa M. Randomized Controlled Study of Intravitreal Bevacizumab 0.16 Mg Injected One Day before Surgery for Proliferative Diabetic Retinopathy. Retina. 2015;35(9):1800–1807. doi:10.1097/IAE.0000000000000577
6. Fallico M, Maugeri A, Romano GL, et al. Epiretinal Membrane Vitrectomy With and Without Intraoperative Intravitreal Dexamethasone Implant: a Systematic Review With Meta-Analysis. Front Pharmacol. 2021;12:635101. doi:10.3389/fphar.2021.635101
7. Moshfeghi AA, Khurana RN, Moini H, et al. Impact of anti-VEGF treatment on development of proliferative diabetic retinopathy in routine clinical practice. BMC Ophthalmol. 2024;24(1):229. doi:10.1186/s12886-024-03491-w
8. Simmonds M, Llewellyn A, Walker R, et al. Anti-VEGF drugs compared with laser photocoagulation for the treatment of proliferative diabetic retinopathy: a systematic review and individual participant data meta-analysis. Health Technol Assess. 2025;2025:1.
9. Li H, Lei N, Zhang M, Li Y, Xiao H, Hao X. Pharmacokinetics of a long-lasting anti-VEGF fusion protein in rabbit. Exp Eye Res. 2012;97(1):154–159. doi:10.1016/j.exer.2011.09.002
10. Yang X, Xu J, Wang R, et al. A Randomized Controlled Trial of Conbercept Pretreatment before Vitrectomy in Proliferative Diabetic Retinopathy. J Ophthalmol. 2016;2016:2473234. doi:10.1155/2016/2473234
11. Cui J, Chen H, Lu H, et al. Efficacy and Safety of Intravitreal Conbercept, Ranibizumab, and Triamcinolone on 23-Gauge Vitrectomy for Patients with Proliferative Diabetic Retinopathy. J Ophthalmol. 2018;2018:4927259. doi:10.1155/2018/4927259
12. Jiang T, Gu J, Zhang P, Chen W, Chang Q. The effect of adjunctive intravitreal conbercept at the end of diabetic vitrectomy for the prevention of post-vitrectomy hemorrhage in patients with severe proliferative diabetic retinopathy: a prospective, randomized pilot study. BMC Ophthalmol. 2020;20(1):43. doi:10.1186/s12886-020-1321-9
13. Li B, Li MD, Ye JJ, Chen Z, Guo ZJ, Di Y. Vascular endothelial growth factor concentration in vitreous humor of patients with severe proliferative diabetic retinopathy after intravitreal injection of conbercept as an adjunctive therapy for vitrectomy. Chin Med J. 2020;133(6):664–669. doi:10.1097/CM9.0000000000000687
14. Lu Q, Lu L, Chen B, Chen W, Lu P. Efficacy comparison of intravitreal injections of conbercept and ranibizumab for severe proliferative diabetic retinopathy. Can J Ophthalmol. 2019;54(3):291–296. doi:10.1016/j.jcjo.2018.06.010
15. Mao JB, Wu HF, Chen YQ, et al. Effect of intravitreal conbercept treatment before vitrectomy in proliferative diabetic retinopathy. Int J Ophthalmol. 2018;11(7):1217–1221. doi:10.18240/ijo.2018.07.23
16. Ren X, Bu S, Zhang X, et al. Safety and efficacy of intravitreal conbercept injection after vitrectomy for the treatment of proliferative diabetic retinopathy. Eye. 2019;33(7):1177–1183. doi:10.1038/s41433-019-0396-0
17. Su L, Ren X, Wei H, et al. Intravitreal Conbercept (Kh902) for Surgical Treatment of Severe Proliferative Diabetic Retinopathy. Retina. 2016;36(5):938–943. doi:10.1097/IAE.0000000000000900
18. Xu W, Cheng W, Yao Y, Guo J, Xu G. Preoperative Intravitreal Conbercept Facilitates Vitrectomy in Proliferative Diabetic Retinopathy: is Attention Required for the Fellow Eye? J Ophthalmol. 2019;2019(1):2923950. doi:10.1155/2019/2923950
19. Yang KB, Zhang H, Li SJ, et al. Conbercept and Ranibizumab Pretreatments in Vitrectomy with Silicone Oil Infusion for Severe Diabetic Retinopathy. J Ocul Pharmacol Ther. 2019;35(3):161–167. doi:10.1089/jop.2018.0093
20. Li S, Guo L, Zhou P, et al. Comparison of efficacy and safety of intravitreal ranibizumab and conbercept before vitrectomy in Chinese proliferative diabetic retinopathy patients: a prospective randomized controlled trial. Eye Vis. 2022;9(1):44. doi:10.1186/s40662-022-00316-z
21. Li C-S. Effect and safety of PPV assisted by intravitreal injection of conbercept in the treatment of PDR combined with vitreous hemorrhage. Int Eye Sci. 2021;2021:1597–1600. doi:10.3980/j.issn.1672-5123.2021.9.21
22. Luo LH, Duan GP, Zeng Q, et al. Efficacy of Conbercept Combined with Vitrectomy in the Treatment of Proliferative Diabetic Retinopathy. J Chin Physician. 2018. doi:10.3760/cma.j.issn.1008-1372.2018.05.030
23. Ou Z. Intravitreal injection of conbercept combined with PPV in the treatment of proliferative diabetic retinopathy. Int Eye Sci. 2021;2021 986–990.
24. Sun M, Li M. Study of anti-vascular endothelial growth factor medicine for proliferative diabetic retinopathy at perioperative period. Int Eye Sci. 2015;15:1772–1774.
25. Yang Z, Di Y, Ye J, Yu W, Guo Z. Comparison of the adjuvant effect of conbercept intravitreal injection at different times before vitrectomy for proliferative diabetic retinopathy. Front Endocrinol. 2023;14:1171628. doi:10.3389/fendo.2023.1171628
26. Daruich A, Matet A, Dirani A, et al. Central serous chorioretinopathy: recent findings and new physiopathology hypothesis. Prog Retin Eye Res. 2015;48:82–118. doi:10.1016/j.preteyeres.2015.05.003
27. Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: Phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127(1):72–84. doi:10.1016/j.ophtha.2019.04.017
28. Maguire MG, Martin DF, Ying G-S, Group CoA-rMDTTR. 5-year outcomes with anti-VEGF treatment of neovascular Age-related Macular Degeneration (AMD): the comparison of AMD treatments trials. Ophthalmology. 2016;123(8):1751. doi:10.1016/j.ophtha.2016.03.045
29. Wells JA, Glassman AR, Ayala AR, Network DRCR. Aflibercept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema Two-Year Results from a Comparative Effectiveness Randomized Clinical Trial. Ophthalmology. 2016;123(6):1351–1359. doi:10.1016/j.ophtha.2016.02.022
30. Del Amo EM, Rimpelä A-K, Heikkinen E, et al. Pharmacokinetic aspects of retinal drug delivery. Prog Retinal Eye Res. 2017;57:134–185. doi:10.1016/j.preteyeres.2016.12.001
31. Liao DS, Grossi FV, El Mehdi D, et al. Complement C3 inhibitor pegcetacoplan for geographic atrophy secondary to age-related macular degeneration: a randomized Phase 2 trial. Ophthalmology. 2020;127(2):186–195. doi:10.1016/j.ophtha.2019.07.011
32. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
33. Boyer DS, Yoon YH, Belfort JR, et al. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology. 2014;121(10):1904–1914. doi:10.1016/j.ophtha.2014.04.024
34. Nguyen QD, Brown DM, Marcus DM, et al. Ranibizumab for diabetic macular edema: results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology. 2012;119(4):789–801. doi:10.1016/j.ophtha.2011.12.039
35. Munier FL, Gaillard M-C, Balmer A, et al. Intravitreal chemotherapy for vitreous disease in retinoblastoma revisited: from prohibition to conditional indications. Br J Ophthalmol. 2012;96(8):1078–1083. doi:10.1136/bjophthalmol-2011-301450
36. Jin E, Bai Y, Luo L, et al. Serum Levels of Vascular Endothelial Growth Factor before and after Intravitreal Injection of Ranibizumab or Conbercept for Neovascular Age-Related Macular Degeneration. Retina. 2017;37(5):971–977. doi:10.1097/IAE.0000000000001274
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.