Back to Journals » Medical Devices: Evidence and Research » Volume 14
Efficacy of Intraoperative Hemodynamic Optimization Using FloTrac/EV1000 Platform for Early Goal-Directed Therapy to Improve Postoperative Outcomes in Patients Undergoing Coronary Artery Bypass Graft with Cardiopulmonary Bypass: A Randomized Controlled Trial
Authors Tribuddharat S, Sathitkarnmanee T ![]() , Ngamsangsirisup K, Nongnuang K
, Ngamsangsirisup K, Nongnuang K
Received 16 April 2021
Accepted for publication 10 June 2021
Published 28 June 2021 Volume 2021:14 Pages 201—209
DOI https://doi.org/10.2147/MDER.S316033
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sirirat Tribuddharat,1 Thepakorn Sathitkarnmanee,1 Kriangsak Ngamsangsirisup,1 Krisana Nongnuang2
1Department of Anesthesiology, Faculty of Medicine, Khon Kaen University, Khon Kaen, 40002, Thailand; 2Phramongkutklao Hospital, Bangkok, 10400, Thailand
Correspondence: Thepakorn Sathitkarnmanee
Department of Anesthesiology, Faculty of Medicine, Khon Kaen University, 123 Mitrapap Road, Ampur Muang, Khon Kaen, 40002, Thailand
Tel +66 81 954 7622
Fax +66 43 348 390
Email [email protected]
Purpose: Early goal-directed therapy (EGDT) using the FloTrac system reportedly improved postoperative outcomes among high-risk patients undergoing non-cardiac surgery. This study’s objective was to evaluate the FloTrac/EV1000 platform’s efficacy for improving postoperative outcomes in cardiac surgery.
Patients and Methods: Eighty-six adults undergoing coronary artery bypass graft (CABG) with cardiopulmonary bypass (CPB) in 2 tertiary referral centers were randomized to the EGDT or Control group. The Control group was managed with standard care to achieve the following goals: mean arterial pressure 65– 90 mmHg; central venous pressure 8– 12 mmHg; urine output ≥ 0.5 mL·kg− 1·h− 1; oxygen saturation > 95%; and hematocrit 26– 30%. The EGDT group was managed to reach similar goals using information from the FloTrac/EV1000 monitor. The targets were stroke volume variation < 13%; stroke volume index 33– 65 mL·beat− 1·m− 2; cardiac index 2.2– 4.0 L·min− 1·m− 2; and systemic vascular resistance index 1600– 2500 dynes·s·cm-5·m-2.
Results: The intensive care unit (ICU) stay of the EGDT group was significantly shorter (mean difference − 29.5 h; 95% CI − 17.2 to − 41.8, P < 0.001). The mechanical ventilation time was also shorter in the EGDT group (mean difference − 11.3 h; 95% CI − 2.7 to − 19.9, P = 0.011). The hospital LOS was shorter in the EGDT group (mean difference − 1.1 d; 95% CI − 0.1 to − 2.1, P = 0.038).
Conclusion: EGDT using FloTrac/EV1000 can be applied in CABG with CPB to improve postoperative outcomes.
Keywords: length of stay, ICU stay, hospital LOS, mechanical ventilation, postoperative complication
Introduction
Cardiac surgery is a high-risk surgery involving high-risk patients leading to high morbidity and mortality. Recently, perioperative mortality has decreased due to improved patient care; however, the morbidity rate remains substantial.1 As a consequence, 10% of patients undergoing cardiac surgery have required prolonged postoperative care due to hemodynamic instability, organ dysfunction, and/or multiorgan failure, leading to increased cost in intensive care and hospital care.2 Early goal-directed therapy (EGDT) involves detecting alterations in hemodynamic parameters in order to guide intravenous fluid and inotropic or vasoactive therapy. These interventions enable early manipulation of cardiac preload, contractility, and afterload so as to achieve predefined goals for balancing tissue oxygen supply with demand.3 Among high-risk patients undergoing non-cardiac surgery, EGDT is reported to decrease mortality, morbidity, and length of stay (LOS) in intensive care unit (ICU) and hospital.4,5 A few small studies have assessed the benefits of EGDT in cardiac surgery.3,6–9 A systematic review including all five randomized controlled trials revealed that the use of EGDT might reduce morbidity and hospital LOS among patients undergoing cardiac surgery.2
There are several platforms used to define the goals for EGDT (viz PICCO Plus, FloTrac/EV1000, esophageal Doppler, and thermodilution pulmonary artery catheter).2 Among them, FloTrac/EV1000 (Edwards Life Sciences, Irvine, CA, USA) is minimally invasive monitoring that requires no calibration. FloTrac/EV1000 is relatively easily operated: connect it to (a) the radial artery catheter used for direct arterial pressure monitoring and (b) a central venous cannula. FloTrac/EV1000 then provides real-time information (updated every 20 s) on the stroke volume variation (SVV), stroke volume index (SVI), cardiac index (CI), and systemic vascular resistance index (SVRI). Initially, the SVV validation for predicting fluid responsiveness was performed in closed-chest patients, so it was not recommended in open-chest situations. Recently, many studies have validated the use of SVV in open-chest contexts, concluding that SVV and pulse pressure variation (PPV) can be used for fluid responsiveness assessment in patients under either open-chest or open-pericardium conditions.10,11 EGDT using the FloTrac/Vigileo (an earlier version of FloTrac/EV1000) was reported to reduce postoperative complications and LOS in hospital among high-risk patients undergoing major abdominal surgery.12,13 The benefit of this system in cardiac surgery, however, is unsettled. A report using FloTrac/Vigileo information for postoperative hemodynamic stabilization in patients who underwent cardiac surgery revealed inconclusive beneficial effects including decreased hospital LOS.3 A study on the clinical benefit of applying EGDT using the FloTrac/EV1000 in cardiac surgery is needed. We therefore aimed to assess the benefit of applying the FloTrac/EV1000 as a tool for EGDT in this group of patients, hypothesizing that EGDT—using the FloTrac/EV1000 for hemodynamic optimization during the intraoperative period—would reduce morbidity, ICU LOS, and hospital LOS.
This study’s objective was to compare postoperative outcomes between applying EGDT using the FloTrac/EV1000 platform vs standard care as a tool to manage hemodynamic parameters in patients undergoing coronary artery bypass graft (CABG) with cardiopulmonary bypass (CPB). The primary outcome was ICU LOS—namely, the difference between the intervention and standard care. The secondary outcomes were duration of mechanical ventilation in the ICU, hospital LOS, number of inotropic and/or vasoactive drugs used during different stages, and postoperative complications.
Materials and Methods
The study was reviewed and approved by the Khon Kaen University Ethics Committee in Human Research (HE611321) and registered at www.ClinicalTrials.gov (NCT04292951) on March 1, 2020. The study was conducted as per the Declaration of Helsinki and the ICH GCP. Written informed consent was obtained from all subjects. This study was reported according to the CONSORT (Consolidated Standards of Reporting Trials) guidelines.
Our study was a multi-center, prospective randomized controlled trial. The sample size calculation was based on ICU LOS (4.9 ± 1.8 d) after cardiac surgery in a previous study.3 We determined that we needed a sample size of 42 per group to detect a 25% decrease in ICU LOS with an α-value of 0.05, a power (1-ß) of 0.80, and a 20% dropout. Block-of-4 randomization was performed using a computer-generated list kept in sealed opaque envelopes. We included patients of either sex who: 1) were 18 years or older who underwent elective CABG with CPB under general anesthesia at Srinagarind Hospital, Khon Kaen University, Khon Kaen, Thailand or Phramongkutklao Hospital, Bangkok, Thailand; and, 2) had an American Society of Anesthesiologists (ASA) classification between II and IV. We excluded patients needing redo surgery, having a contra-indication to central venous cannulation, requiring intra-aortic balloon pump, or having ventricular arrhythmias. All surgeons and anesthesiologists in the study were qualified personnel for cardiac surgery and anesthesia with > 5 years’ experience.
The patients were randomized to the EGDT or Control group. The patients and outcome assessors were blinded. All patients received standard cardiac anesthesia care as per our institution’s protocol. The monitoring in the operation theater included electrocardiogram, pulse oximeter, non-invasive blood pressure, temperature, capnography, and urine output. The radial artery was cannulated and connected to a pressure transducer in the Control group to measure invasive blood pressure (IBP) or a FloTrac transducer (Edwards Life Sciences, Irvine, CA, USA) in the EGDT group to measure IBP as well as SVV, SVI, and CI. The internal jugular vein was cannulated and connected to another pressure transducer in the Control group to measure central venous pressure (CVP) or a pressure transducer connected to the FloTrac/EV1000 (Edwards Life Sciences, Irvine, CA, USA) in the EGDT group to measure SVRI. All patients received fentanyl 2–3 µg·kg−1 and midazolam 1 mg as a premedication. Propofol 2–3 mg·kg−1 or etomidate 0.3 mg·kg−1 was used as an induction agent. Endotracheal intubation was facilitated using cis-atracurium 0.2 mg·kg−1. Anesthesia was maintained with 50% oxygen in air and 1–2% sevoflurane or 3–6% desflurane adjusted to achieve 1 minimum alveolar concentration (MAC) on the monitor to maintain the depth of anesthesia. CPB was initiated after heparin 3–4 mg·kg−1 was administered via the CVP catheter with an activated clotting time (ACT) > 480 s, with supplemental doses of 1–2 mg·kg−1 to maintain ACT > 400–480 s. Mild hypothermia (32°C) was maintained during CPB. Cardioplegia solution was infused via an aortic root catheter after aortic cross-clamping. Supplemental cardioplegia was administered at the discretion of the cardiac surgeon. During CPB, mean arterial pressure (MAP) was maintained in the range of 45–75 mmHg. After terminating the CPB, protamine 1 mg per 1 mg of pre-CPB heparin dose was slowly injected to reverse the effect of heparin. All patients were transferred to the ICU and mechanically ventilated. All patients received standard ICU care. The criteria for ventilator weaning and extubation were: good consciousness and motor power, stable cardiovascular status, a PaO2/FiO2 ratio ≥ 250 mmHg, and a respiratory rate of 10–25 times·min−1. The criteria for ICU discharge were: good consciousness and neurological signs, stable cardiovascular status with no need for inotropic or vasopressor drugs and ICU monitoring, and stable respiratory status with oxygen requirement not more than 60%. Hospital discharge criteria were: stable cardiovascular and respiratory status, no drain or catheter retained, normal ambulation, no infection or serious complications, wound-stitch removed, and normal diet.
During the intraoperative period, both before and after CPB, the Control group received fluid, inotropic, and/or vasoactive drugs at the discretion of the attending anesthesiologists to achieve the following goals: MAP 65–90 mmHg; CVP 8–12 mmHg; urine output ≥ 0.5 mL·kg−1·h−1; SpO2 > 95%; and hematocrit 26–30%. Arterial blood gas (ABG) and electrolytes were monitored and corrected hourly. In the EGDT group, the patients were managed to achieve similar goals: MAP 65–90 mmHg; urine output ≥ 0.5 mL·kg−1·h−1; SpO2 > 95%; and hematocrit 26–30%, using information from the FloTrac/EV1000. The EGDT group received: fluid to maintain a SVV < 13%; inotropic drugs to achieve a SVI of 33–65 mL·beat−1·m−2 and CI of 2.2–4.0 L·min−1·m−2; and/or vasoactive drugs to achieve a SVRI of 1600–2500 dynes·s·cm-5·m-2. ABG and electrolytes were monitored and corrected in the same manner.
Parameters recorded included: the volume of fluid, amount of inotropic and/or vasoactive drugs used during pre-CPB, post-CPB, transfer to the ICU, and in the ICU. Also recorded were time of mechanical ventilation in the ICU, ICU and hospital LOS, and all complications.
Statistical Analysis
Continuous data were tested for Gaussian distribution using the Shapiro–Wilk test. Data with a normal distribution were presented as a mean ± standard deviation (SD) and compared using the unpaired Student’s t-test. Data with a non-Gaussian distribution were presented as a median (inter-quartile range) and compared using the Mann–Whitney U-test. Categorical data were presented as a number (%) and compared using a χ2 test. The primary outcome was presented as a mean difference with a 95% confidence interval (CI). P < 0.05 was considered statistically significant. All data were analyzed using SPSS 16.0 (SPSS Inc., Chicago, IL, USA).
Results
Eighty-six patients were recruited between March 2020 and December 2020 with 44 and 42 patients in the EGDT and Control group, respectively (Figure 1). Patient characteristics and clinical data were similar between the two groups except for more crystalloid intake, and more urine output in the EGDT group (Table 1).
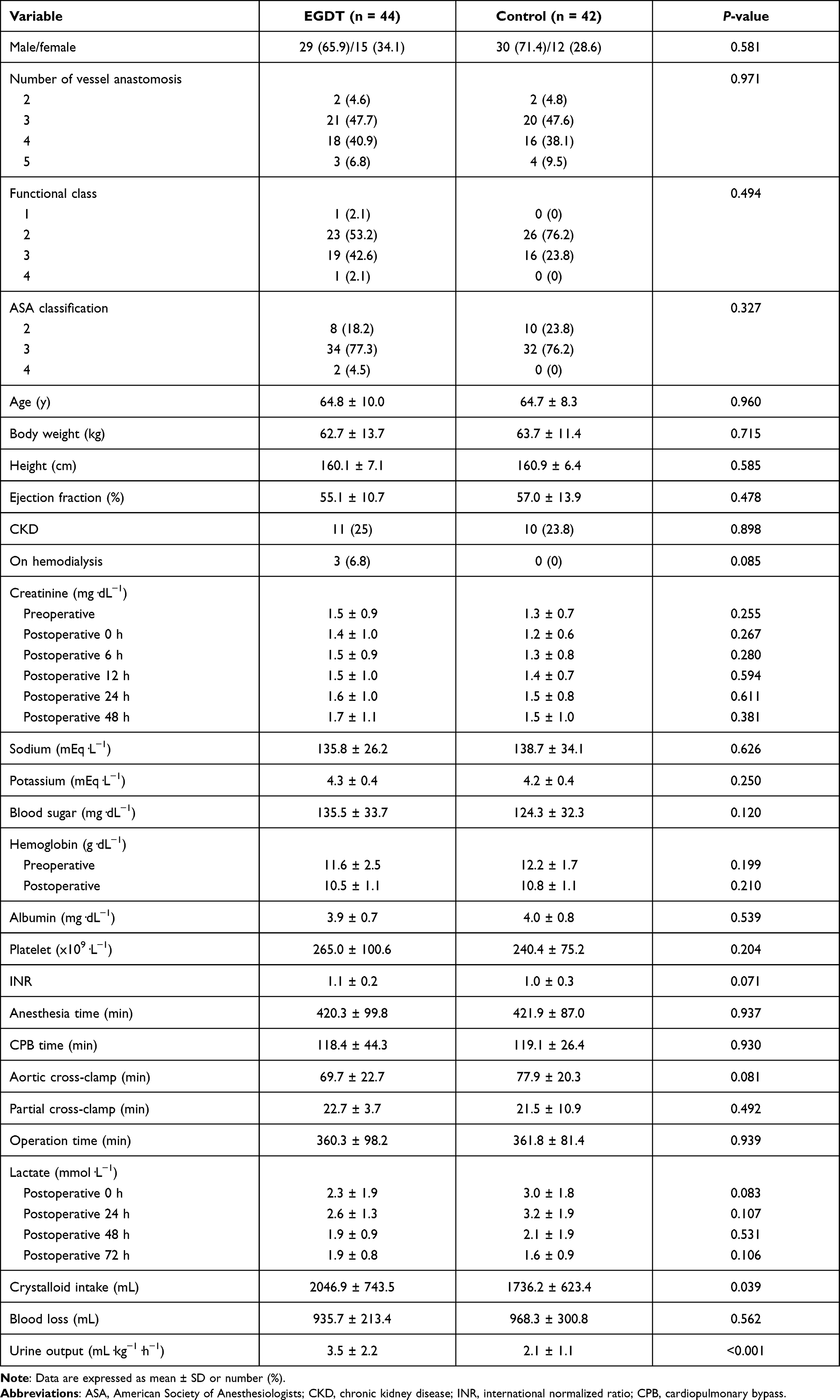 |
Table 1 Characteristics and Clinical Data of Patients (n = 86) |
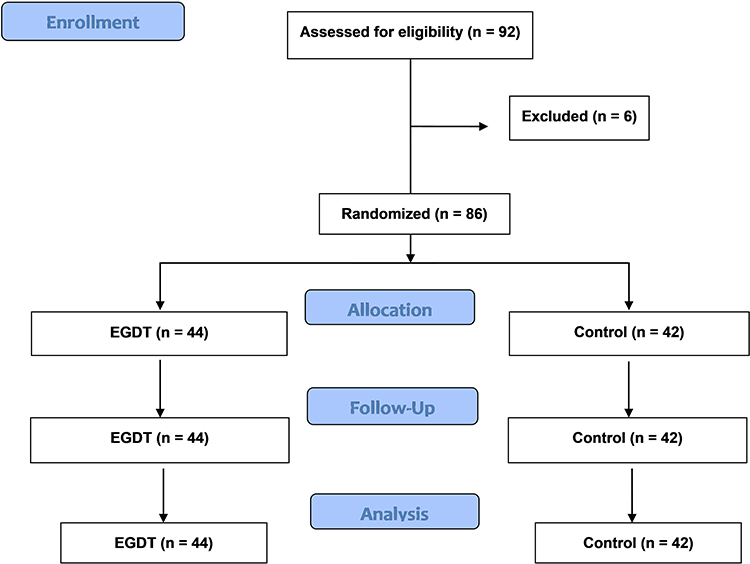 |
Figure 1 CONSORT diagram of the study. Abbreviation: CONSORT, Consolidated Standards of Reporting Trials. |
The ICU LOS of the EGDT group was significantly shorter than the Control group (mean difference −29.5 h; 95% CI −17.2 to −41.8, P < 0.001). The mechanical ventilation time was also less in the EGDT group (mean difference −11.3 h; 95% CI −2.7 to −19.9, P = 0.011). The hospital LOS was shorter in the EGDT group than in the Control group (mean difference −1.1 d; 95% CI −0.1 to −2.1, P = 0.038) (Table 2).
 |
Table 2 Postoperative Outcomes (n = 86) |
The EGDT group received a higher number of inotropic and/or vasoactive drugs than the Control group in the pre-bypass period (P <0.001), but required less in the post-bypass (P = 0.002) and postoperative period before transfer to the ICU (P <0.001) (Table 3). In the ICU, the EGDT group required less and a shorter duration of inotropic and/or vasoactive drugs than the Control group (Table 4).
 |
Table 3 Number of Drugs Required at Different Stages for Each Group (n = 86) |
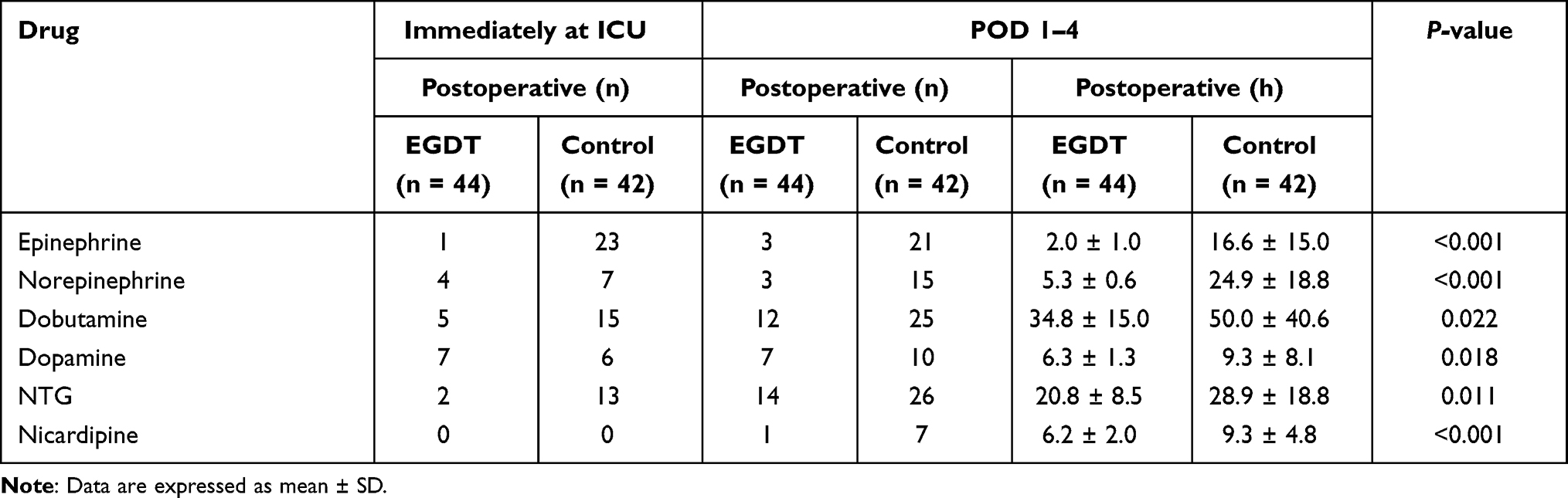 |
Table 4 Duration of Inotropic and Vasoactive Drugs Used in ICU |
The postoperative complications are presented in Table 5. The EGDT group had less atrial fibrillation (AF) with rapid ventricular response (RVR), acute respiratory distress syndrome (ARDS), and acute renal injury (AKI) than the Control group.
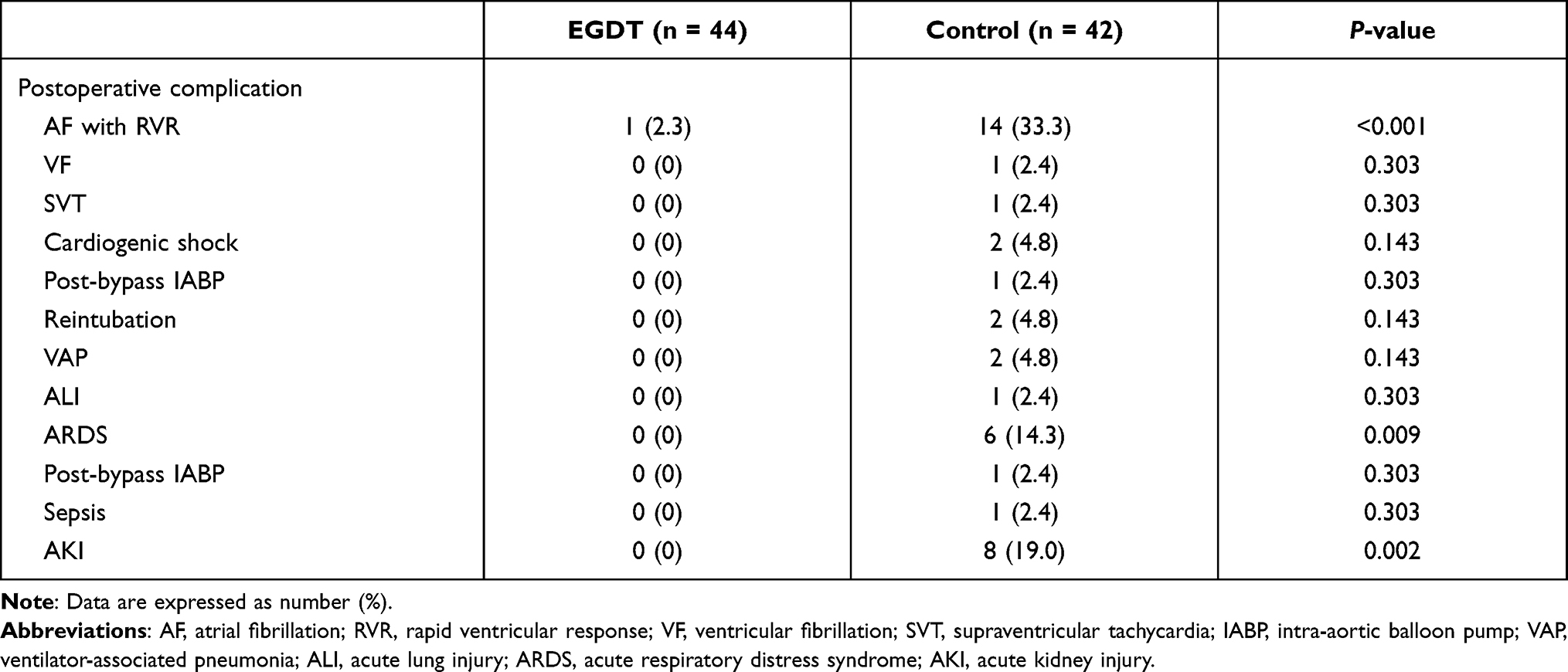 |
Table 5 Postoperative Complications |
Discussion
The current study demonstrates that intraoperative hemodynamic optimization using a EGDT-driven protocol via the FloTrac/EV1000 system can decrease ventilator time, reduce ICU and hospital LOS, and lower postoperative complications in patients undergoing CABG with CPB. Our results are similar to a systematic review including 5 randomized controlled trials which concluded that the use of EGDT in cardiac surgery reduced complication and hospital LOS.2 Patients with ischemic heart disease may experience low cardiac output at different stages during CABG leading to intraoperative hypotension (IOH), which further compromises myocardium oxygen supply, increasing the need for inotropic and/or vasoactive drugs and leading to postoperative complications. Early recognition and treatment of low cardiac output results in better outcomes.3 Most anesthesiologists set MAP at between 90–105 mmHg as the principal goal for managing low cardiac output.3 The MAP, however, does not always represent cardiac output. MAP depends on two factors—viz cardiac output and systemic vascular resistance (SVR)—while cardiac output relies on preload and contractility. Thus, there are three variables that affect MAP—viz preload, contractility, and afterload or SVR. A normal MAP can be found in situations of low cardiac output with a high SVR resulting in tissue hypoperfusion. Treatment of IOH without precise information regarding these three variables may lead to mismanagement which may increase pharmacologic requirement, complications, and ICU and hospital LOS. In EGDT, these three variables are continuously monitored and early manipulated to optimize pressure and flow to perfuse body organs resulting in better outcomes.
EGDT applied intraoperatively has been reported to improve postoperative outcomes in non-cardiac major surgery,4,5 as well as cardiac surgery.2,14 There are several means for determining the goals of EGDT—ie, PICCO Plus, FloTrac/EV1000, esophageal Doppler, and thermodilution pulmonary artery catheter.2 We chose a fourth-generation FloTrac with EV1000 to provide the goals for EGDT because this platform is less invasive, relatively easy to use, and can provide continuous real-time data. Although one of the limitations of the SVV is that it is not recommended in patients with an open thorax, many studies have confirmed its efficacy for assessing fluid responsiveness and improving postoperative outcomes in open-chest surgery.10,11,14 One study reported on the use of the FloTrac/Vigileo system for EGDT in moderate to high-risk cardiac surgery during the postoperative period in the ICU. Their approach demonstrated significantly more extra volume used and a greater number of times inotropic agents needed to be changed. Their EGDT group had a shorter duration of inotropic agent used, a shorter duration of ventilator support, and a shorter ICU and hospital LOS. The difference between groups was clinically but not statistically significant, owing to the small sample size.3
Differently, our study applied the EGDT protocol from the beginning until the end of the surgery, resulting in similar outcomes with statistical significance. The EGDT group required more fluid and drug requirements during the pre-bypass period to optimize the SVV, SVI, CI, and SVRI based on information from the FloTrac/EV1000 to achieve a target MAP. These achievements resulted in better myocardium perfusion leading to less drug requirement during post-bypass and before transfer to the ICU. The EGDT group also required significantly fewer and a shorter duration of inotropic and/or vasoactive drugs in the ICU, leading to a shorter requirement for ventilator support, as well as a shorter ICU and hospital LOS. The EGDT group developed fewer postoperative complications than the Control group, as in a previous study.3 The assumption is that the fewer complications in the EGDT group are the result of more optimized tissue perfusion in the EGDT group during the intraoperative period than in the Control group.
The cardiac output measurement agreement between the FloTrac/Vigileo system and the thermodilution technique in cardiac surgery is inconclusive.15–17 Nevertheless, our study shows that using the FloTrac/EV1000 system in cardiac surgery results in better postoperative clinical outcomes.
Although we did not use the bi-spectral index (BIS) to control anesthesia depth, we used the MAC value to monitor and control depth of anesthesia. The end-tidal concentration of sevoflurane or desflurane was adjusted to achieve 1 MAC for a given age (MACage) on the monitor.18 With the additive effect of fentanyl (~0.5 MAC) and cisatracurium (~0.5 MAC),19,20 the total depth of anesthesia was approximately 2 MAC (~MAC-BAR99), which is optimal.
This study has a few limitations. The attending anesthesiologists could not be blinded. Although we recruited 86 patients from two tertiary hospitals in Thailand, the sample size was relatively small, so a multi-center study with a larger sample size is recommended. The FloTrac/EV1000 platform requires a substantial initial capital investment; however, it reduces ICU and hospital LOS with off-setting cost savings. A cost-effectiveness study regarding this aspect is suggested.
Conclusion
Compared with standard care, intraoperative hemodynamic optimization using the FloTrac/EV1000 platform for EGDT protocol in patients undergoing CABG with CPB resulted in shorter ventilator time, shorter ICU and hospital LOS, and fewer postoperative complications. The FloTrac/EV1000 can be applied in CABG with CPB to improve postoperative outcomes.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgments
The authors thank Mr. Bryan Roderick Hamman under the aegis of the Publication Clinic Khon Kaen University Thailand for assistance with the English-language presentation of the manuscript. We also thank Cardiovascular and Thoracic Surgery Research Group, Khon Kaen University for supporting this study.
Funding
This study was supported by an unrestricted university grant from the Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand (Grant number: IN63109). The funding body had no role in (a) designing the study, (b) collecting, analyzing, and interpreting the data, or (c) writing the manuscript.
Disclosure
The authors report no competing interests in this work.
References
1. Ferguson TB
2. Aya HD, Cecconi M, Hamilton M, et al. Goal-directed therapy in cardiac surgery: a systematic review and meta-analysis. Br J Anaesth. 2013;110(4):510–517. doi:10.1093/bja/aet020
3. Kapoor PM, Kakani M, Chowdhury U, et al. Early goal-directed therapy in moderate to high-risk cardiac surgerents. Ann Card Anaesth. 2008;11(1):27–34. doi:10.4103/0971-9784.38446
4. Chong MA, Wang Y, Berbenetz NM, et al. Does goal-directed haemodynamic and fluid therapy improve peri-operative outcomes?: a systematic review and meta-analysis. Eur J Anaesthesiol. 2018;35(7):469–483. doi:10.1097/EJA.0000000000000778
5. Giglio M, Manca F, Dalfino L, et al. Perioperative hemodynamic goal-directed therapy and mortality: a systematic review and meta-analysis with meta-regression. Minerva Anestesiol. 2016;82(11):1199–1213.
6. Polonen P, Ruokonen E, Hippelainen M, et al. A prospective, randomized study of goal-oriented hemodynamic therapy in cardiac surgical patients. Anesth Analg. 2000;90(5):1052–1059. doi:10.1097/00000539-200005000-00010
7. Mythen MG, Webb AR. Perioperative plasma volume expansion reduces the incidence of gut mucosal hypoperfusion during cardiac surgery. Arch Surg. 1995;130(4):423–429. doi:10.1001/archsurg.1995.01430040085019
8. McKendry M, McGloin H, Saberi D, et al. Randomised controlled trial assessing the impact of a nurse delivered, flow monitored protocol for optimisation of circulatory status after cardiac surgery. BMJ. 2004;329(7460):258. doi:10.1136/bmj.38156.767118.7C
9. Smetkin AA, Kirov MY, Kuzkov VV, et al. Single transpulmonary thermodilution and continuous monitoring of central venous oxygen saturation during off-pump coronary surgery. Acta Anaesthesiol Scand. 2009;53(4):505–514. doi:10.1111/j.1399-6576.2008.01855.x
10. Reuter DA, Goepfert MSG, Goresch T, et al. Assessing fluid responsiveness during open chest conditions. Br J Anaesth. 2005;94(3):318–323. doi:10.1093/bja/aei043
11. Sander M, Spies CD, Berger K, et al. Prediction of volume response under open-chest conditions during coronary artery bypass surgery. Crit Care. 2007;11(6):R121. doi:10.1186/cc6181
12. Mayer J, Boldt J, Mengistu AM, et al. Goal-directed intraoperative therapy based on autocalibrated arterial pressure waveform analysis reduces hospital stay in high-risk surgical patients: a randomized, controlled trial. Crit Care. 2010;14(1):R18. doi:10.1186/cc8875
13. Weinberg L, Mackley L, Ho A, et al. Impact of a goal directed fluid therapy algorithm on postoperative morbidity in patients undergoing open right hepatectomy: a single centre retrospective observational study. BMC Anesthesiol. 2019;19(1):135. doi:10.1186/s12871-019-0803-x
14. Giglio M, Dalfino L, Puntillo F, et al. Haemodynamic goal-directed therapy in cardiac and vascular surgery. A systematic review and meta-analysis. Interact Cardiovasc Thorac Surg. 2012;15(5):878–887. doi:10.1093/icvts/ivs323
15. Cannesson M, Attof Y, Rosamel P, et al. Comparison of FloTrac cardiac output monitoring system in patients undergoing coronary artery bypass grafting with pulmonary artery cardiac output measurements. Eur J Anaesthesiol. 2007;24(10):832–839. doi:10.1017/S0265021507001056
16. Lin SY, Chou AH, Tsai YF, et al. Evaluation of the use of the fourth version FloTrac system in cardiac output measurement before and after cardiopulmonary bypass. J Clin Monit Comput. 2018;32(5):807–815. doi:10.1007/s10877-017-0071-6
17. Kusaka Y, Ohchi F, Minami T. Evaluation of the Fourth-Generation FloTrac/Vigileo system in comparison with the intermittent bolus thermodilution method in patients undergoing cardiac surgery. J Cardiothorac Vasc Anesth. 2019;33(4):953–960. doi:10.1053/j.jvca.2018.06.017
18. Nickalls RW, Mapleson WW. Age-related iso-MAC charts for isoflurane, sevoflurane and desflurane in man. Br J Anaesth. 2003;91(2):170–174. doi:10.1093/bja/aeg132
19. Vereecke HE, Proost JH, Heyse B, et al. Interaction between nitrous oxide, sevoflurane, and opioids: a response surface approach. Anesthesiology. 2013;118(4):894–902. doi:10.1097/ALN.0b013e3182860486
20. Sebel PS, Glass PS, Fletcher JE, et al. Reduction of the MAC of desflurane with fentanyl. Anesthesiology. 1992;76(1):52–59. doi:10.1097/00000542-199201000-00008
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.