Back to Journals » Clinical Ophthalmology » Volume 20
Efficacy of Intraoperative 9-0 Nylon Thread Insertion for Preventing Hypotony-Related Complications Following PreserFlo MicroShunt Implantation in Japanese Patients: A Comparative Study
Authors Matsuoka T ![]() , Usami T, Kaneko H
, Usami T, Kaneko H ![]()
Received 14 January 2026
Accepted for publication 5 April 2026
Published 16 April 2026 Volume 2026:20 596071
DOI https://doi.org/10.2147/OPTH.S596071
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Takahiro Matsuoka,1,2 Takahiro Usami,1 Hiroki Kaneko1
1Department of Ophthalmology, Hamamatsu University School of Medicine, Hamamatsu, Japan; 2Department of Ophthalmology, Japanese Red Cross Shizuoka Hospital, Shizuoka, Japan
Correspondence: Takahiro Matsuoka, Japanese Red Cross Shizuoka Hospital, 8-2 Ōte-machi, Aoi-ku, Shizuoka, 420-0853, Japan, Tel +81 90 4268 3920, Email [email protected]
Background: Early postoperative hypotony remains a significant complication following PreserFlo MicroShunt (PMS) implantation, potentially leading to serious sequelae including choroidal detachment and hypotensive maculopathy. This study evaluated the effectiveness of intraoperative 9– 0 nylon thread insertion (NTI) technique in preventing hypotony-related complications.
Methods: This retrospective comparative study included 81 eyes of 63 patients who underwent PMS implantation with mitomycin C between September 2023 and June 2025. Eyes were divided into NTI group (59 eyes, 42 patients) and Non-NTI group (22 eyes, 21 patients). The primary outcome was the incidence of composite hypotony-related complications (choroidal detachment and/or hypotensive maculopathy) during 6-month follow-up. Secondary outcomes included intraocular pressure (IOP) changes, medication score reduction, and timing of suture removal. Statistical analyses incorporated cluster correction for bilateral cases.
Results: Baseline characteristics, including glaucoma subtype distribution, were comparable between groups. The composite hypotony-related complication rate was significantly lower in the NTI group (11.9% vs 54.5%, p< 0.001; odds ratio 0.112, 95% CI 0.039– 0.321). Kaplan-Meier analysis demonstrated superior complication-free survival in the NTI group (log-rank p< 0.001, hazard ratio 0.094, 95% CI 0.035– 0.252). The median IOP at postoperative day 1 was significantly higher in the NTI group (10.0 [8.0– 14.0] vs 5.8 [5.0– 8.5] mmHg, p< 0.001), indicating effective early hypotony prevention. At 6 months, both groups achieved comparable IOP control (13.0 [10.9– 14.0] vs 13.0 [11.0– 16.0] mmHg, p=0.324) with medication-free rates of 74.6% and 59.1%, respectively (p=0.190).
Conclusion: Intraoperative 9– 0 nylon thread insertion significantly reduces hypotony-related complications following PMS implantation without compromising IOP control at 6 months or medication reduction, representing a safe and effective surgical modification.
Keywords: PreserFlo MicroShunt, glaucoma surgery, hypotony prevention, nylon thread insertion, choroidal detachment, hypotensive maculopathy
Introduction
Glaucoma is a progressive optic neuropathy characterized by optic nerve damage and corresponding visual field defects, often associated with elevated intraocular pressure (IOP). It is a leading cause of irreversible blindness worldwide.1 While early-stage disease responds to pharmacological agents or laser treatments, moderate-to-advanced glaucoma often requires surgical intervention when conservative approaches fail.2
The PreserFlo MicroShunt™ (PMS, Santen Pharmaceutical Co., Ltd., Osaka, Japan) is a less-invasive bleb-forming glaucoma surgery device that reduces IOP by facilitating aqueous humor drainage from the anterior chamber to the subconjunctival space.3 Recent clinical studies in Japan have demonstrated the increasing adoption of less-invasive bleb-forming glaucoma surgeries, including PMS implantation, in Japanese ophthalmological practice.4 Compared to conventional trabeculectomy, PMS has been reported to cause less postoperative inflammation and scarring with potentially improved IOP control stability.5,6
However, early postoperative hypotony from excessive aqueous outflow remains a major concern with PMS implantation.7,8 This complication can lead to serious sequelae such as choroidal detachment, hypotensive maculopathy, anterior chamber shallowing, and vision loss.7–9
To address hypotony concerns, surgeons have adopted nylon suture insertion into the PMS tube to temporarily increase outflow resistance, based on principles established in tube shunt occlusion techniques.9,10 Previous reports have described the use of 8–0 or 10–0 nylon sutures; however, the physical characteristics of the suture material, such as thickness and stiffness, may influence both surgical handling and filtration resistance. However, the optimal suture caliber balancing flow restriction and surgical handling remains unclear. In contrast, 9–0 nylon suture offers intermediate thickness, potentially providing a balance between these factors.
Therefore, this study aimed to evaluate the clinical effectiveness of 9–0 nylon thread insertion (NTI) in reducing hypotony-related complications and to characterize its impact on postoperative IOP control and medication requirements.
Methods
Study Design
This retrospective comparative study was approved by the Ethics Committee of the Japanese Red Cross Shizuoka Hospital (approval number: 2024–42) and conducted in accordance with the principles of the Declaration of Helsinki. As this study involved retrospective analysis of anonymized clinical data only, written informed consent was waived under an opt-out approach.
Study Population
The study included adult patients who underwent glaucoma surgery using the PMS between September 2023 and June 2025 at our institution. Initially, surgery was performed without nylon thread insertion, but subsequently, the surgical technique was modified to include insertion of 9–0 nylon thread (Mani Nylon®, Mani, Inc., Utsunomiya, Japan; Product Number: ZE06-14) into the tube lumen (nylon thread insertion: NTI). Based on this change, cases were classified into NTI group (with nylon thread insertion) and Non-NTI group (without nylon thread insertion). A total of 81 eyes from 63 patients were included in the final analysis: NTI group (59 eyes, 42 patients) and Non-NTI group (22 eyes, 21 patients). Bilateral cases were included, but statistical analyses incorporated cluster correction at the patient ID level. Glaucoma subtype was determined based on medical record review and classified as primary open-angle glaucoma (excluding normal-tension glaucoma), normal-tension glaucoma, pseudo exfoliation glaucoma, primary angle-closure glaucoma, or unknown when classification was not possible. Secondary glaucoma, including uveitis, neovascular, and steroid-induced glaucoma, were excluded from the analysis.
Exclusion criteria included corneal disease affecting visual function, retinal disease, severe postoperative complications that interfered with follow-up, insufficient preoperative data necessary for analysis, and a history of uveitis. All included eyes had at least 6 months of postoperative follow-up and were evaluable at the 6-month time point.
Surgical Technique
All surgeries were performed by a single experienced surgeon (T.M.) who had completed approximately 30 PMS implantation procedures before introducing the NTI technique, ensuring procedural consistency across both groups. The sclera was exposed through conjunctival incision and Tenon’s capsule dissection, followed by application of 0.04% mitomycin C (MMC) solution (Kyowa Kirin Co., Ltd., Tokyo, Japan) to modulate wound healing and prevent excessive subconjunctival fibrosis.11 A scleral tunnel was created 3.5 mm posterior to the corneal limbus using a bevel-up knife, and the PMS was inserted. After confirming proper placement of the fin portion within the scleral tunnel, aqueous outflow was verified.
In the NTI group, a 9–0 nylon thread was inserted into the MicroShunt lumen and externalized at the corneal limbus, forming a J-loop configuration to provide temporary intraluminal resistance to aqueous outflow and allow controlled postoperative removal (Figure 1). The conjunctiva was sutured with 9–0 nylon thread with the thread end exposed at the corneal limbus to enable outpatient suture removal. Finally, the absence of leakage was confirmed before completion of the surgery.
 |
Figure 1 Intraoperative Technique of 9–0 Nylon Thread Insertion (NTI) in PreserFlo MicroShunt Implantation. (A) Schematic illustration of intraoperative 9–0 nylon thread insertion into the lumen of the PreserFlo MicroShunt. The nylon thread is externalized 4 mm from the limbus as a J-shaped loop to facilitate postoperative removal. Arrows indicate the PreserFlo MicroShunt and the 9–0 nylon thread. (B) Intraoperative photograph before conjunctival coverage, showing the intraluminal 9–0 nylon within the PreserFlo MicroShunt and the externalized J-loop (arrows). (C) Final intraoperative appearance after conjunctival coverage, showing the 9–0 nylon loop positioned beneath the conjunctiva to allow postoperative removal (arrow). |
Suture removal was performed during postoperative follow-up at the surgeon’s discretion based on intraocular pressure and clinical course. Removal was typically considered when intraocular pressure exceeded the target range for the individual patient based on postoperative course. In most cases, removal was performed during the early postoperative period. Because this was a retrospective study, no strict predefined protocol for suture removal was applied.
Outcome Measures
In this study, hypotony was defined as an intraocular pressure (IOP) of ≤6 mmHg.
Primary outcome measures were: (1) Composite hypotony-related complications, defined as occurrence of choroidal detachment and/or hypotensive maculopathy at any postoperative timepoint during the 6-month follow-up period; (2) Postoperative intraocular pressure (IOP) changes at day 1, day 7, months 1, 3, and 6.
Secondary outcome measures were: (1) IOP changes before and after suture removal in the NTI group; (2) Changes in medication scores (combination drugs and oral carbonic anhydrase inhibitors counted as 2 medications); (3) Medication-free rates at 6 months. All IOP measurements were performed by experienced orthoptists using Goldmann applanation tonometry.
Statistical Analysis
Continuous variables were expressed as median (interquartile range [IQR]). Between-group comparisons used Mann–Whitney U-test for continuous variables and Fisher’s exact test for categorical variables. For complication incidence rates, odds ratios (OR) and 95% confidence intervals were calculated. Time to complication development was evaluated using Kaplan-Meier method with Log rank test, and hazard ratios (HR) were calculated using Cox proportional hazards model. All analyses incorporated cluster correction at the patient level to account for bilateral cases. Statistical significance was set at p<0.05. All analyses were performed using R software (version 4.3.0).
Reporting Guideline
This observational study adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for reporting observational studies.
Results
Patient Characteristics
A total of 81 eyes from 63 patients were included in this study: 59 eyes (42 patients) in the NTI group and 22 eyes (21 patients) in the Non-NTI group (Table 1). Baseline characteristics, including age, sex, preoperative IOP, medication score, and glaucoma subtype distribution, were comparable between groups. There was no significant difference in glaucoma subtype distribution between the groups (p = 0.740). The median age was 76.0 (75.0–81.5) years in the NTI group and 80.0 (64.3–84.0) years in the Non-NTI group (p = 0.306). Preoperative IOP was 19.5 (16.0–21.5) mmHg in the NTI group and 19.0 (15.5–24.0) mmHg in the Non-NTI group (p = 0.395). The preoperative medication score was 3.0 (3.0–4.0) in both groups (p = 0.967). All eyes completed the 6-month follow-up period, and no cases were censored before the final time point.
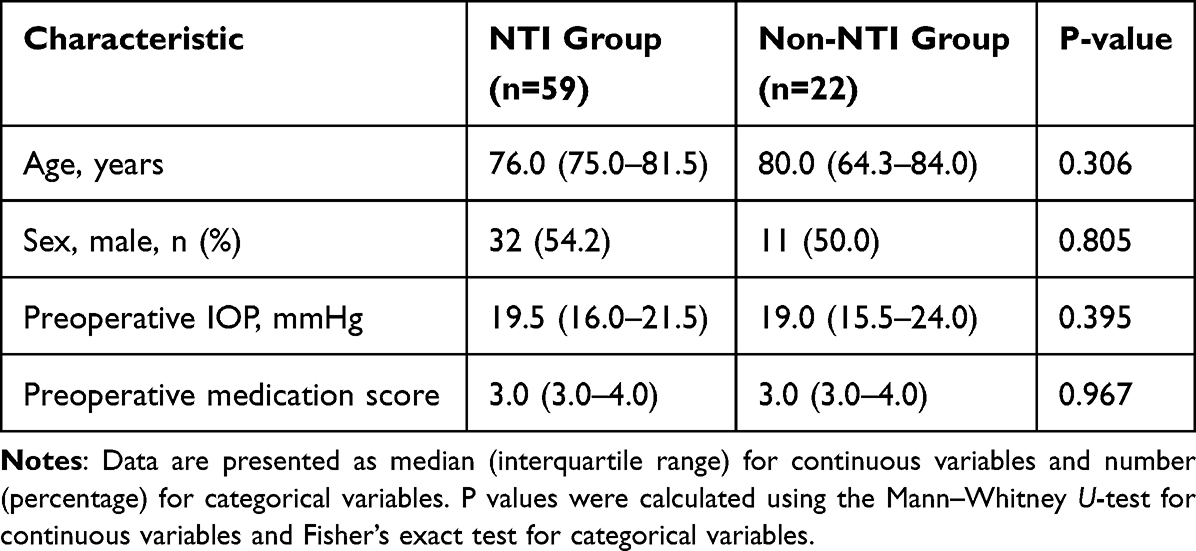 |
Table 1 Baseline Characteristics of Eyes Undergoing PreserFlo MicroShunt Implantation with or Without Nylon Thread Insertion |
Primary Outcomes
Postoperative IOP Changes
Postoperative IOP trends differed between groups during the early postoperative period (Table 2 and Figure 2). The NTI group showed higher IOP at postoperative day 1 (10.0 [8.0–14.0] vs 5.8 [5.0–8.5] mmHg, p<0.001) and day 7 (10.0 [8.6–13.0] vs 8.9 [7.0–9.0] mmHg, p=0.001), indicating effective early hypotony prevention. From month 1 onwards, no significant differences were observed between groups (month 1: 11.0 [8.4–13.0] vs 10.0 [7.0–11.8] mmHg, p=0.264;month 3: 12.0 [9.0–13.8] vs 12.0 [10.0–13.8] mmHg, p=0.823; month 6: 13.0 [10.9–14.0] vs 13.0 [11.0–16.0] mmHg, p=0.324). All cases of numerical hypotony (IOP ≤6 mmHg) in both groups were transient and resolved spontaneously within a few days without requiring additional interventions such as viscoelastic injection, suturing, or needling. No cases required surgical or procedural intervention for hypotony management.
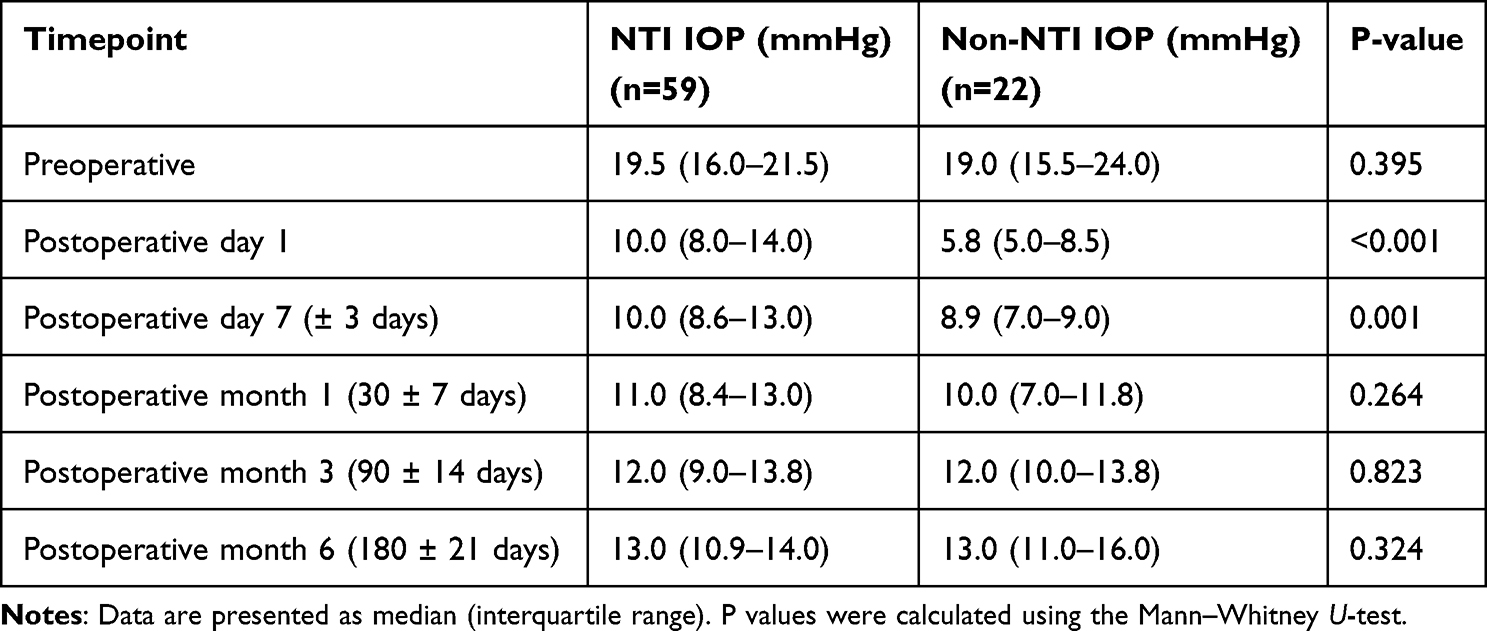 |
Table 2 Intraocular Pressure Changes Over Time |
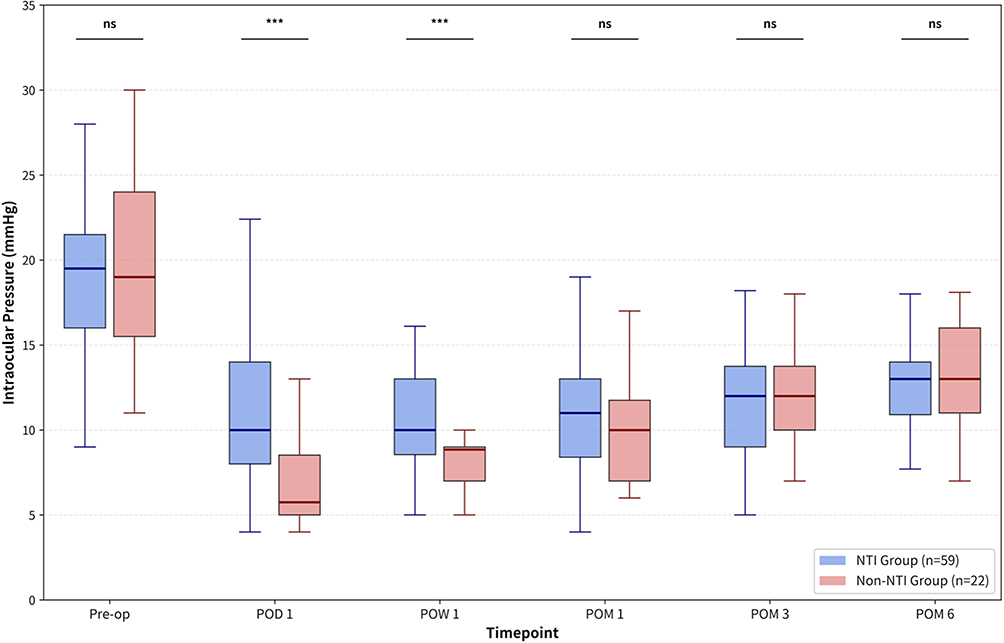 |
Figure 2 Intraocular Pressure Changes Over Time. Box-and-whisker plots showing intraocular pressure (IOP) over 6 months in the NTI (nylon thread insertion) group (blue) and the non-NTI group (red). Significant between-group differences were observed at postoperative day 1 (P < 0.001) and postoperative week 1 (P = 0.001), indicating effective early hypotony prevention in the NTI group. From postoperative month 1 onward, no significant between-group differences were observed, indicating comparable IOP control at 6 months. Between-group comparisons at each time point were performed using the Mann–Whitney U-test. ns, not significant; ***P ≤ 0.001. |
In contrast, hypotony associated with structural complications, including choroidal detachment and hypotensive maculopathy, was considered clinically significant. Among these, all cases of hypotensive maculopathy were associated with decreased visual acuity.
Hypotony-Related Complications
The incidence of composite hypotony-related complications was significantly lower in the NTI group compared to the Non-NTI group. Numerical hypotony (IOP ≤6 mmHg) occurred in 9 of 59 eyes (15.3%) in the NTI group and in 14 of 22 eyes (63.6%) in the Non-NTI group. The composite outcome (choroidal detachment and/or hypotensive maculopathy) occurred in 7 of 59 eyes (11.9%) in the NTI group versus 12 of 22 eyes (54.5%) in the Non-NTI group (odds ratio 0.112, 95% CI 0.039–0.321, p<0.001). Specifically, choroidal detachment occurred in 3.4% vs 31.8% (p=0.001), and hypotensive maculopathy in 10.2% vs 54.5% (p<0.001). No shallow anterior chamber was observed in either group.
Kaplan-Meier survival analysis revealed a significantly lower cumulative incidence of hypotony-related complications in the NTI group over the 6-month follow-up period (Figure 3). Cox proportional hazards analysis demonstrated that the NTI group had a significantly reduced risk of developing complications (hazard ratio 0.094, 95% CI 0.035–0.252, log-rank p<0.001).
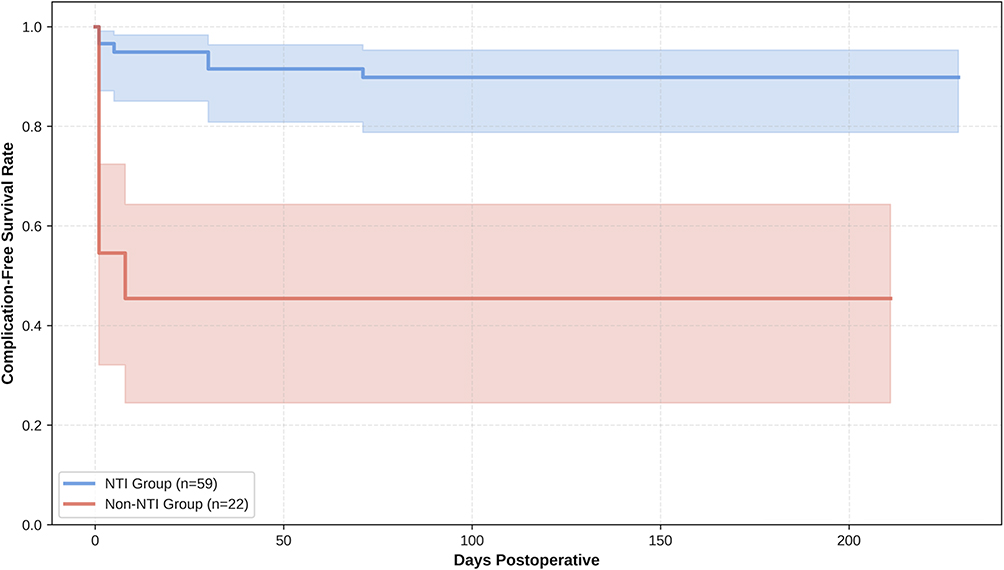 |
Figure 3 Kaplan-Meier Survival Curve for Hypotony-Related Complication-Free Survival. Kaplan–Meier analysis showed significantly higher hypotony-related complication-free survival in the NTI group than in the non-NTI group (log-rank P < 0.001; hazard ratio, 0.094; 95% confidence interval, 0.035–0.252). |
Secondary Outcomes
IOP Changes Around Suture Removal
Changes in intraocular pressure before and after suture removal were analyzed in the NTI group (n=59). The median intraocular pressure before suture removal was 12.0 (10.0–15.0) mmHg and decreased to 9.4 (8.0–12.0) mmHg after removal. The median IOP reduction associated with suture removal was −2.0 (−4.4–0.0) mmHg (p<0.001). Suture removal was performed in all eyes in the NTI group. The median time to suture removal was 8 days (IQR 4.5–18 days; range 1–71 days). Hypotony (IOP ≤6 mmHg) occurred in 6 eyes immediately after suture removal. All cases of hypotony observed immediately after suture removal were transient and resolved without requiring additional intervention.
Medication Requirements
Medication requirements were substantially reduced in both groups following surgery. Both groups showed decreased medication scores from baseline, with no significant between-group differences during the postoperative course. At 6 months, median medication scores were 0 (0–1) in the NTI group and 1 (0–2) in the Non-NTI group (p=0.076). Medication-free rates at 6 months were 74.6% in the NTI group and 59.1% in the Non-NTI group (p=0.190).
No additional surgical revisions, bleb needling procedures, or reoperations were required in either group during the follow-up period. Importantly, no cases of persistent hypotony or structural complications were observed following suture removal.
Discussion
This study demonstrates that intraoperative 9–0 nylon thread insertion (NTI) significantly reduces the incidence of hypotony-related complications following PMS implantation while maintaining effective IOP control and allowing predictable pressure reduction upon suture removal. Our findings contribute important evidence to the evolving literature on hypotony prevention strategies in less-invasive bleb-forming glaucoma surgery.
The most significant finding of our study was the substantial reduction in composite hypotony-related complications with NTI (11.9% vs 54.5%, OR 0.112, p<0.001). This substantial reduction is clinically relevant when compared to reported complication rates in the literature. Previous studies have reported variable rates of hypotony-related complications following PMS implantation.7,8,12 Al Habash and Alshaibani reported similar complication rates in their recent series, which closely align with our Non-NTI group.13 The significantly lower rate in our NTI group suggests that prophylactic nylon insertion represents a highly effective preventive strategy.
In the present study, all cases of numerical hypotony were transient and resolved spontaneously within a few days without requiring any additional intervention. No cases required surgical or procedural management for hypotony. In contrast, hypotony associated with structural complications, such as choroidal detachment and hypotensive maculopathy, represented clinically significant hypotony. Notably, hypotensive maculopathy was accompanied by visual acuity reduction, highlighting its clinical relevance. These findings indicate that numerical hypotony alone does not adequately reflect clinically meaningful hypotony following PMS implantation, as clinically significant hypotony is primarily defined by associated structural complications.9 Therefore, our analysis focused on complication-associated hypotony as the primary outcome rather than numerical hypotony alone.
The temporal pattern of IOP control observed in this study provides insight into both the mechanism of action and potential sources of bias. The higher early postoperative IOP in the NTI group suggests that intraluminal nylon insertion effectively provides temporary resistance to aqueous outflow, thereby preventing excessive early filtration. In contrast, the gradual increase in IOP observed in the Non-NTI group over time may reflect the natural wound healing process, including subconjunctival fibrosis and reduction of filtration. In addition, externalization of the nylon thread at the limbus enables simple and safe postoperative removal in an outpatient setting, enhancing the practicality of this technique.
However, this temporal pattern should also be interpreted in the context of the study design. Because the Non-NTI group was operated earlier in the study period and the NTI group later, a chronological bias related to surgical experience cannot be excluded and may have partially influenced the early postoperative outcomes, particularly in the Non-NTI group. It is possible that improvements in surgical technique, perioperative management, or case selection over time contributed in part to the observed differences. Nevertheless, the magnitude of the reduction in hypotony-related complications in the NTI group suggests that the effect of the intraluminal nylon technique is clinically meaningful beyond the influence of surgical experience alone.
Our approach using 9–0 nylon suture represents a variation of the intraluminal stenting concept previously described with different suture calibers. Previous reports have described the use of both thicker sutures such as 8–0 and thinner sutures such as 10–0 for temporary flow restriction in glaucoma drainage procedures. Similar intraluminal stenting techniques have been reported in glaucoma drainage device surgery to reduce early postoperative hypotony,14 particularly in Ahmed valve implantation.15 In the context of PreserFlo MicroShunt, Verma-Fuehring et al reported successful hypotony prevention using 10–0 nylon sutures, achieving a reduction in adverse events from 15.8% to 6.2%.10 While thinner sutures may allow finer flow modulation, the use of 9–0 nylon in our study may provide a balance between effective outflow restriction and surgical handling characteristics. The slightly larger diameter of 9–0 nylon may offer sufficient temporary resistance to aqueous outflow while remaining technically manageable during insertion and removal.
The concept of systematic tube occlusion for hypotony prevention has been established in traditional tube shunt surgery.14 Studies on drainage devices have demonstrated that choroidal effusion commonly occurs in association with early postoperative hypotony, emphasizing the importance of preventive strategies.14
The controlled IOP reduction following suture removal (median Δ −2.0 mmHg [IQR −4.4 to 0.0], p<0.001) demonstrates an additional advantage of the NTI technique: it allows surgeons to titrate postoperative IOP through selective suture removal. This feature provides flexibility in postoperative management and may be particularly valuable in cases where IOP remains elevated after the initial healing period. The timing of suture removal in our study was determined based on postoperative IOP and clinical course, typically during the early postoperative period. The observed IOP reduction following removal, together with the absence of intervention-requiring hypotony, suggests that this strategy allows controlled modulation of aqueous outflow without compromising safety. These findings indicate that individualized timing of suture removal may be an effective approach to balancing early hypotony prevention and subsequent IOP reduction.
Regarding medication burden reduction, both groups achieved substantial decreases in medication requirements, with the NTI group showing a numerically higher medication-free rate at 6 months (74.6% vs 59.1%), although this did not reach statistical significance (p=0.190). Importantly, no additional surgical or procedural interventions were required to achieve comparable IOP control between the groups, suggesting that the NTI technique does not appear to increase postoperative management burden. The trend toward better medication independence in the NTI group, combined with the dramatic reduction in complications, supports the clinical value of this technique.
Limitations
First, the retrospective design and non-randomized allocation may introduce selection bias and limit our ability to establish definitive causal relationships. In addition, NTI was introduced later during the study period (Non-NTI group operated earlier, NTI group later), and therefore a chronological bias related to surgical experience cannot be excluded. Some of the Non-NTI cases may have been performed during the initial learning phase of PMS implantation, which could have influenced early postoperative outcomes, although the surgeon (T.M.) had already completed approximately 30 PMS procedures before introducing the NTI technique. Although all cases of numerical hypotony resolved spontaneously, the retrospective design limited the precise temporal characterization of hypotony duration.
Second, although glaucoma subtype was retrospectively classified based on medical record review, some degree of misclassification or incomplete information may remain due to the retrospective nature of data collection and reliance on clinical documentation. Although baseline subtype distribution was comparable between groups, residual confounding related to specific subtypes, such as pseudo exfoliation glaucoma, cannot be completely excluded.
Third, the Non-NTI group had a smaller sample size (22 eyes vs 59 eyes), which may have limited statistical power for detecting differences in secondary outcomes such as medication-free rates. However, the dramatic and statistically significant reduction in primary outcomes (hypotony-related complications) demonstrates robust clinical efficacy despite this limitation.
Fourth, all surgeries were performed by a single experienced surgeon at a single institution, potentially limiting the generalizability of our findings to other surgical practices. Multicenter studies would help validate these results across different surgical skill levels and practice settings. Recent multicenter analyses have demonstrated variability in outcomes across different institutions.12
Finally, the relatively short follow-up period of 6 months may not capture late complications or efficacy outcomes. Longer follow-up studies will be necessary to establish the durability of these benefits and to assess any delayed complications associated with the NTI technique. In addition, medication adherence patterns over time may also influence surgical outcomes.16
Despite these limitations, the substantial and statistically significant reduction in hypotony-related complications demonstrates the clinical value of the NTI technique. Future research should focus on prospective randomized controlled trials, longer-term outcomes, multicenter validation, and optimization of suture removal timing.17
Another limitation of this study is that the need for additional postoperative interventions was not pre-specified as a formal outcome measure. However, no cases required bleb needling, surgical revision, or reoperation during the follow-up period, suggesting a low procedural burden in both groups.
Conclusion
This study demonstrates that intraoperative 9–0 nylon thread insertion significantly reduces the hazard of hypotony-related complications following PreserFlo MicroShunt implantation (hazard ratio, 0.094; 95% CI, 0.035–0.252) while preserving surgical efficacy in IOP control and medication reduction. The technique represents a practical and valuable addition to less-invasive bleb-forming glaucoma surgery.
Based on our findings, we recommend considering 9–0 nylon thread insertion as a useful prophylactic option for PreserFlo MicroShunt implantation, particularly in patients at higher risk for hypotony complications.
Future research should focus on longer-term follow-up and multicenter validation to establish the generalizability and durability of these benefits.
Abbreviations
CD, Choroidal detachment; CI, Confidence interval; GEE, Generalized estimating equations; HR, Hazard ratio; IOP, Intraocular pressure; IQR, Interquartile range; MMC, Mitomycin C; NTI, Nylon thread insertion; OR, Odds ratio; PMS, PreserFlo MicroShunt; SD, Standard deviation; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
Data Sharing Statement
De-identified individual-level clinical data are available from the corresponding author on reasonable request due to patient privacy and institutional restrictions. Access may be granted to qualified researchers for non-commercial use upon submission of a brief proposal and a signed data use agreement.
Ethics Approval and Consent to Participate
This retrospective study was approved by the Institutional Review Board (IRB)/Ethics Committee of the Japanese Red Cross Shizuoka Hospital (approval No. 2024-42). The IRB waived the requirement for individual informed consent because only de-identified clinical data were analyzed and the research involved no deviation from standard clinical practice, in accordance with the Japanese Ethical Guidelines for Medical and Biological Research Involving Human Subjects (2021, and subsequent amendments). An opt-out notice was posted on the hospital website and within the facility; patients who declined participation were excluded. The study adhered to the tenets of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Stein JD, Khawaja AP, Weizer JS. Glaucoma in adults-screening, diagnosis, and management: a review. JAMA. 2021;325(2):164–10. PubMed PMID: 33433580. doi:10.1001/jama.2020.21899
2. Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma. JAMA. 2014;311(18):1901–1911. PubMed PMID: 24825645; PubMed Central PMCID: PMC4523637. doi:10.1001/jama.2014.3192
3. Baker ND, Barnebey HS, Moster MR, et al. Ab-Externo MicroShunt versus trabeculectomy in primary open-angle glaucoma. Ophthalmology. 2021;128(12):1710–1721. doi:10.1016/j.ophtha.2021.05.023
4. Yamae T, Sakata R, Suzuki H, et al. Short-term outcomes of the PreserFlo MicroShunt in Japanese patients with exfoliation glaucoma: a comparison with primary open-angle glaucoma using propensity score matching. Jpn J Ophthalmol. 2025. doi:10.1007/s10384-025-01265-5
5. Khan A, Khan AU. Comparing the safety and efficacy of Preserflo Microshunt implantation and trabeculectomy for glaucoma: a systematic review and meta-analysis. Acta Ophthalmologica. 2024;102(4). doi:10.1111/aos.16658
6. Batlle J, Corona A, Albuquerque R. Long-term results of the PRESERFLO® MicroShunt in patients with primary open-angle glaucoma from a single-center non-randomized study. J Glaucoma. 2020. Publish Ahead of Print. doi:10.1097/IJG.0000000000001734
7. Schlenker MB, Durr GM, Michaelov E, Ahmed IIK. Intermediate outcomes of a novel standalone Ab Externo SIBS microshunt with Mitomycin C. Am J Ophthalmol. 2020;215:141–153. doi:10.1016/j.ajo.2020.02.020
8. Nasyrov E, Kommerell I, Schleicher I, Merle DA, Wenzel CJ, Voykov B. Incidence, risk factors, and outcomes of numerical hypotony and choroidal effusion following
9. Sharkawi E, Artes PH, Oleszczuk JD, et al. Systematic occlusion of shunts: control of early postoperative IOP and hypotony-related complications following glaucoma shunt surgery. J Glaucoma. 2016;25(1):54–61. PubMed PMID: 25383464. doi:10.1097/IJG.0000000000000135
10. Verma-Fuehring R, Dakroub M, Bamousa A, Kann G, Hillenkamp J, Kampik D. The use of intraluminal PRESERFLO stenting in avoiding early postoperative hypotony. Graefes Arch Clin Exp Ophthalmol. 2024;262(12):3925–3932. doi:10.1007/s00417-024-06567-x
11. Nassiri N, Sheibani K, Kavousnezhad S, Nassiri S, Azemati A, Nassiri N. Use of Mitomycin C in ophthalmic surgery. J Curr Ophthalmol. 2025;36(3):211–222. PubMed PMID: 40557398; PubMed Central PMCID: PMC12184863. doi:10.4103/joco.joco_283_23
12. Tanner A, Haddad F, Fajardo-Sanchez J, et al. One-year surgical outcomes of the PreserFlo MicroShunt in glaucoma: a multicentre analysis. Br J Ophthalmol. 2023;107(8):1104–1111. PubMed PMID: 35365491; PubMed Central PMCID: PMC10359526. doi:10.1136/bjophthalmol-2021-320631
13. Al Habash A, Alshaibani AK. Safety and efficacy of Preserflo Microshunt in different subtypes of glaucoma. Clin Ophthalmol. 2025;19:3215–3226. PubMed PMID: 40932893; PubMed Central PMCID: PMC12417707. doi:10.2147/OPTH.S551700
14. Gedde SJ, Herndon LW, Brandt JD, et al. Postoperative complications in the tube versus trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814.e1. PubMed PMID: 22244522; PubMed Central PMCID: PMC3653167. doi:10.1016/j.ajo.2011.10.024
15. Abd Elfattah D, Wagdy F, Mokbel T, Elsorogy H, Elhesy AEA. Intraluminal stenting versus external ligation of Ahmed glaucoma valve in prevention of postoperative hypotony. Int J Ophthalmol. 2021;14(10):1560–1564. PubMed PMID: 34667733; PubMed Central PMCID: PMC8481999. doi:10.18240/ijo.2021.10.13
16. Kolko M, Faergemann Hansen R, Dal LG, et al. Predictors and long-term patterns of medication adherence to glaucoma treatment in Denmark—an observational registry study of 30 100 Danish patients with glaucoma. BMJ Open Ophth. 2024;9(1):e001607. doi:10.1136/bmjophth-2023-001607
17. Cunha B, Gil P, Lopes E, et al. PRESERFLO MicroshuntTM versus non-penetrating deep sclerectomy for glaucoma management, one-year results. Clin Ophthalmol. 2025;19:1377–1386. PubMed PMID: 40303579; PubMed Central PMCID: PMC12039835. doi:10.2147/OPTH.S514126
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
One-Year Outcome of PreserFlo MicroShunt Implantation in Patients with Open Angle Glaucoma: Real-World Data from a Tertiary Centre
Cheng TC, Ng KV, Che Hamzah J
Clinical Ophthalmology 2026, 20:605606
Published Date: 10 July 2026