")
Back to Journals » Clinical Ophthalmology » Volume 17
Efficacy of Interleukin-1β Inhibitor on Dry Eye Disease in Patients with Degenerative Arthritis
Authors Treewipanon N , Kasetsuwan N , Reinprayoon U, Satitpitakul V , Uthaithammarat L, Tanpowpong T
Received 2 May 2023
Accepted for publication 6 September 2023
Published 9 October 2023 Volume 2023:17 Pages 2967—2974
DOI https://doi.org/10.2147/OPTH.S419310
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Nathapon Treewipanon,1 Ngamjit Kasetsuwan,1,2 Usanee Reinprayoon,1,2 Vannarut Satitpitakul,1,2 Lita Uthaithammarat,1 Thanathep Tanpowpong3
1Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Bangkok, Thailand; 2Excellence Center for Cornea Transplantation, Department of Ophthalmology, King Chulalongkorn Memorial Hospital, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 3Department of Orthopaedics, Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Bangkok, Thailand
Correspondence: Ngamjit Kasetsuwan, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Pathumwan, Bangkok, 10330, Thailand, Tel +6681-920-0553, Fax +662-256-4142, Email [email protected]
Purpose: To evaluate diacerein (interleukin-1β inhibitor) efficacy on ocular surface disease (OSD).
Patients and Methods: This prospective observational study included patients who received diacerein for osteoarthritis and had dry eye (DE). The primary outcome was corneal staining score. Secondary outcomes were ocular surface disease index (OSDI) score, tear breakup time (TBUT), tear osmolarity (Osm), Schirmer’s test results, interleukin-1α (IL-1α), interleukin-1β (IL-1β), and interleukin-1 receptor antagonist (IL-1Ra) levels in tears. All measurements were done at baseline and 2-month follow-up visits. Linear mixed models were used to examine the effect of all parameters, and log-transformed models were used for IL-1α, IL-1β, and IL-1Ra analyses.
Results: Thirty-four patients (31 females and 3 males) were enrolled. The corneal staining score improved by 1.29 points (P=0.022, 95% confidence interval [95% CI] 0.19 to 2.40) after 2 months, and the OSDI score improved by 17.2 points (P< 0.001, 95% CI 10.82 to 23.58) but TUBT decreased by 0.66 seconds (P=0.021, 95% CI 0.10 to 1.22). No significant differences were observed in the tear Osm and Schirmer’s test. IL-1Ra demonstrated no statistical difference, IL-1α was significantly increased by 80% (P=0.260), and IL-1β was significantly decreased by 99.21% (P< 0.001).
Conclusion: Diacerein can improve corneal staining and decrease IL-1β levels in tears, which reflects better DE symptoms. Diacerein may be a promising alternative treatment for patients with OSD and osteoarthritis.
Keywords: diacerein, dry eye diseases, interleukin-1, ocular surface disease
Introduction
Ocular surface diseases (OSD) are a group of diseases wherein dry eye disease (DED) is included.1 According to the Tear Film and Ocular Surface Society (TFOS) Dry Eye Workshop II (DEWS II), ‘dry eye is a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film, and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play aetiological roles’.2 DED is a common disease encountered by all ophthalmologists in their clinical practice. Studies in Bangkok, Thailand, showed that the prevalence of DED in hospital-based patients was 34%,3 whereas that in the community was 14.2%, according to the Romklao eye study.4 Patients with DED experience symptoms such as dryness, foreign body sensation, burning sensation, and blurred vision, which leads them to visit their ophthalmologists.5 This chronic disease may gradually worse if not treated. The economic burden from DED can be estimated at approximately US$1200 per year.6
The pathophysiology of DED can start at multiple levels; one of the most critical steps is the loss of tear film homeostasis. As a result of loss of tear film homeostasis in DED, tear film instability and hyperosmolarity could directly damage the ocular tissue and through the inflammation process. Tear hyperosmolarity induces inflammation via pro-inflammatory cytokines, including interleukin-1α (IL-1α), interleukin-1β (IL-1β), tumor necrosis factor-α (TNF-α), and matrix metallopeptidase 9 (MMP-9), which causes corneal epithelial disruption that can be evaluated through fluorescein staining. Clinically, fluorescein stains the area of corneal or conjunctival epithelial tight junction disruption, which is shown as punctate epithelial erosion.7 Additionally, increased interleukin-1 (IL-1) levels in tears can stimulate pain receptors in patients with DED, leading to chronic pain.8
IL-1 has a significant role in the inflammatory process, not only in OSD but also osteoarthritis. IL-1 involves cartilage destruction and perpetual inflammatory processes in joints.9 Diacerein is the treatment of choice for osteoarthritis, and its active metabolite is rhein.10,11 Diacerein has two major effects on IL-1. First, it decreases the active form of IL-1β level by inhibiting the interleukin-1-converting enzyme (ICE). Moreover, diacerein also reduces interleukin-1 receptor (IL-1R) level and indirectly enhances the production of interleukin-1 receptor antagonist (IL-1Ra).10,12–14 Diacerein is a symptomatic slow-acting drug for osteoarthritis, and the onset of action is 1–2 months. It is administered by oral ingestion at a dosage of 50–100 mg/day; however, the recommended starting dose is usually half of this dose because of its side effects, including urine discoloration and diarrhea that generally subsides 2 weeks after ingestion.11,13,14
Few drugs involving IL-1 effects have shown benefits for OSD treatment, including topical anakinra, which is an IL-1Ra. A Phase I/II clinical study showed that DED symptoms and corneal epitheliopathy improved after 12 weeks of topical anakinra treatment.12 Another topical IL-1R inhibitor is isunakinra, which elicited improvement in both symptoms and corneal fluorescein staining signs in a phase Ib/IIa trial.8 However, canakinumab, the only systemic drug that modulates IL-1, is a monoclonal antibody against IL-1β and has not improved corneal staining.15 There has been no evidence for the use of systemic diacerein for OSD. Therefore, in this study, we aimed to evaluate the effectiveness of diacerein in alleviating the signs and symptoms of OSD.
Materials and Methods
Study Design and Participants
This prospective observational study involved patients who received diacerein for osteoarthritis and had any type of DED. In this study, we observed the effects of diacerein for 2 months. Thirty-four patients were enrolled in this study, and all of them returned for the 2-month follow-up. This study was conducted at the King Chulalongkorn Memorial Hospital in Bangkok, Thailand, between October 2019 and July 2020. The study was approved by the institutional review board of the Faculty of Medicine, Chulalongkorn University (IRB no.469/62, approved on 27 Aug 2019) and followed the tenets of the Declaration of Helsinki. Written informed consent was obtained from all the participants before enrolment. The study was registered at ClinicalTrials.gov (NCT04351100). The eligibility criteria included age >18 years with an ocular surface disease index (OSDI) score ≥13 and corneal staining score (National Eye Institute score) ≥3, which at least consisted of one area ≥2 points and one area ≥1 point. Patients were excluded if they met the following criteria: allergic to diacerein, used topical cyclosporine within 30 days before enrolment, had eyelid problems (lagophthalmos, trichiasis, entropion, and ectropion), had active ocular inflammation or infection, used drugs that may interfere with tear production (ie, anti-depressives, anticholinergics, anti-histamine medications, antihypertensives, calcium channel blockers, antacids, systemic corticosteroids, and retinoids) within the past 3 months, had previous ocular surgery or contact lens use within the past 6 months with changes in tear substitutes between the two visits, were pregnant or breastfeeding, and had no history of systemic autoimmune diseases.
Ocular Surface Assessments
The same investigator (N.T.) assessed the ocular surface using tear osmolarity (Osm), Schirmer’s I test, corneal staining score, and tear breakup time (TBUT) for each participant. At first, we intended to assess only the right eye. However, after considering the potential of their left eye if their right eye did not meet the inclusion criteria, we decided to modify the protocol. We obtained approval from the IRB before the left eye was assessed. We considered the right eye for study enrolment if it passed the inclusion criteria; otherwise, we assessed the left eye.
The primary outcome was the corneal staining score, which was measured using a single drop of normal saline to a fluorescein strip, then touching the fluorescein strip to the lower lid and asking the patient to blink. After several blinks, corneal staining was examined under a slit-lamp biomicroscope (TOPCON, Tokyo, Japan) using cobalt blue light. The scoring system was based on the National Eye Institute guidelines by dividing the corneal surface into five areas, each with a score of 0–3, with 0 indicating no corneal fluorescein staining and 3 indicating severe staining. The scoring was guided using a standard picture.16
TBUT was assessed after fluorescein corneal staining by measuring the time (in seconds) since the eye had been widely opened until a corneal dry spot was detected. A slit-lamp biomicroscope using cobalt blue light was used to examine the TBUT. TBUT was measured thrice, and the mean value was calculated.17
Tear Osm was assessed using Tear lab® (TearLab Corp., San Diego, CA, United States) by placing the pin of the test card at the tear lake that stayed over the lower lid. The test was delayed for 2 hours when prior fluorescein was used to eliminate dye interference.18,19
The Schirmer’s I test was used to measure basic and reflex tear secretion. It was performed by placing a filter paper (Schirmer strip, 32 K Supply, Bangkok, Thailand) at the lower fornix between the eyelids and conjunctiva for 5 minutes. Then, the filter paper was removed, and the wet part was measured.
To evaluate the tear cytokines (IL-1α, IL-1β, IL-1Ra), the Schirmer’s I test filter papers were preserved in Eppendorf tubes at −80°C until processing. The papers were collected between 1 p.m. and 3 p.m. to reduce intraday variation. We followed the protocol for extracting cytokines as previously described by VanDerMeid et al.20 However, we changed the centrifuge rate to 300 ×g for 30 seconds to maximize the fluid extracted from the filter paper. We did not dilute the sample after centrifugation because the sample was sufficient for cytokine extraction. For cytokine measurement, we use Bio-Plex multiplex system (Bio-Rad, Hercules, California, USA) following protocol from the manufacturer.
Assessments of the Symptoms and Frequency of Artificial Tear Use
A research assistant assessed all participants for their symptoms using the OSDI score. The OSDI score consisted of 12 items, and the total score ranged from 0 to 100. Scores range for severity: normal (0–12), mild (13–22), moderate (23–32), and severe (≥33).21 The patients were also asked about the artificial tears they used at the first visit and the 2-month follow-up.
Statistical Analyses
Demographic data were reported using frequency and mean with standard deviation (SD). The estimated mean changes in all parameters after treatment were analyzed using linear mixed models and expressed as means with 95% confidence intervals (CI) and SD. The cytokine concentrations were logarithmically transformed and analyzed using linear mixed models. The geometric mean and mean ratio were used to describe the cytokine concentrations. Spearman’s rank correlation coefficient was used to analyze the correlation between tear interleukin levels and other factors.
To obtain the study power, the sample size was calculated based on the decrease in the corneal fluorescein staining score as described in a previous study.22,23 The pooled mean ± SD was 3.5 ± 2.8. Corneal specialists defined a minimal clinically significant effect of adding diacerein as a 1.5 decrease in corneal fluorescein staining score. For a power of 80% to detect a difference of 1.5 at a significance level of 0.05 (two-sided), 28 participants were needed. Three participants were added to mitigate the risk of loss to follow-up, with an estimated drop-out rate of 10%.
For all analyses, an alpha level of 0.05 was adopted for statistical significance, and Stata version 15.1 (Stata Corp Release 15, Stata Corp LLC; College Station, TX, USA) was used.
Results
Thirty-four patients were recruited, and all patients completed a 2-month follow-up period (Figure 1). The mean age of the patients was 54.71 ± 3.79 years, 31 (91.18%) patients were female, and 3 (8.82%) patients were male. The right eye was examined in 27 (79.41%) patients, and the left eye was examined in 7 (20.59%) patients. Underlying diseases were found in 23 (67.65%) patients, including hypertension, allergy, osteoporosis, diabetes, dyslipidemia, anemia, asthma, and psoriasis.
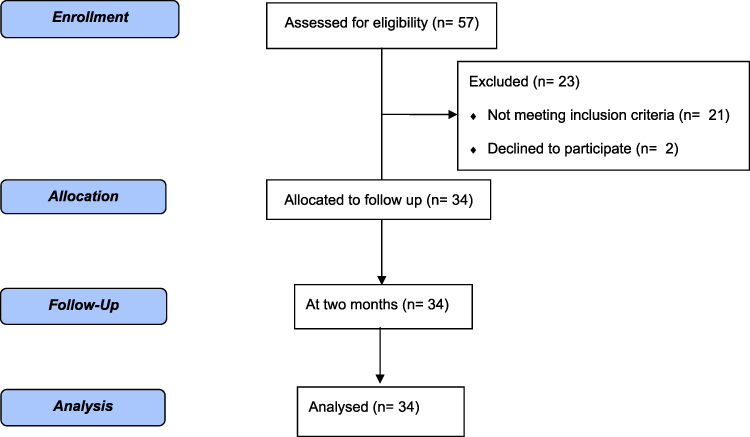 |
Figure 1 CONSORT flow diagram. |
The OSD symptoms and signs data were compared at the baseline and 2-month follow-up after systemic diacerein intake, as shown in Table 1. The corneal staining score significantly improved (P=0.026). Similarly, the OSDI score (P<0.001) improved. Additionally, patients used artificial tears less frequently, from 5.05 to 2.47 drops/week. But TBUT significantly dropped from 4.17 to 3.51 sec (P=0.021). However, the tear Osm and Schirmer’s I test results showed no statistical difference after 2 months. For tear interleukin levels, IL-1β was significantly decreased by 99.21% compared to IL-1α, which increased by 80%; however, no significant changes were observed for IL-1Ra.
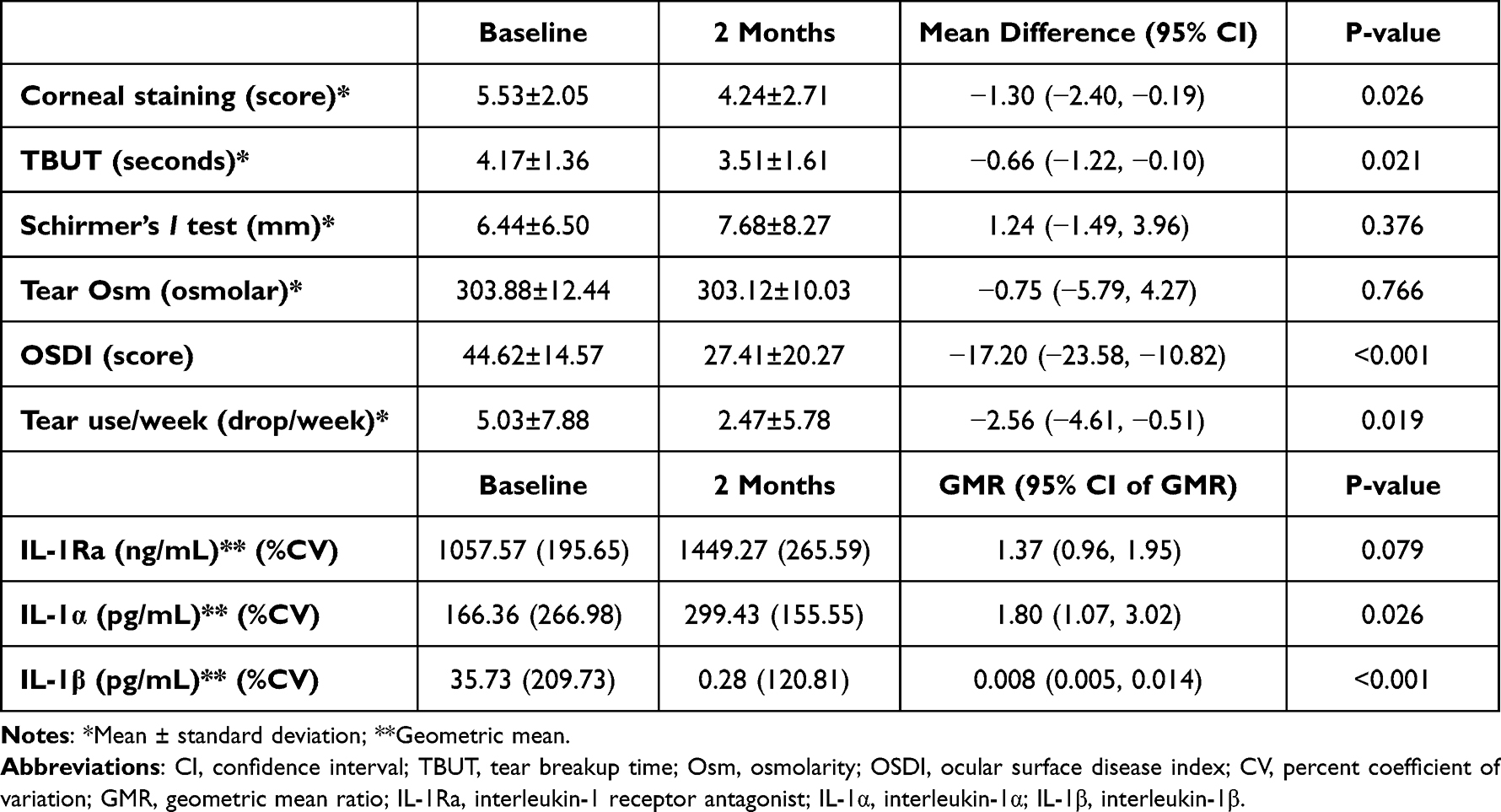 |
Table 1 Outcomes at the Baseline and After 2 Months |
The correlations between tear interleukin levels (IL-1Ra, IL-1α, IL-1β) and other factors were analyzed and are shown in Table 2. The OSDI score showed a moderate positive correlation with IL-1β (correlation coefficient 0.40, P<0.001), but a weak negative correlation with IL-1Ra and IL-1α (correlation coefficient −0.30, P=0.014 and −0.25, P=0.039, respectively). Ocular surface staining showed a moderate positive correlation with IL-1β (correlation coefficient 0.44, P<0.001). Schirmer’s test showed a strong negative correlation with IL-1Ra and IL-1α (correlation coefficient −0.66, P<0.001 and −0.78, P<0.001, respectively) and a weak negative correlation with IL-1β (correlation coefficient −0.26, P=0.035). There were no significant correlations between TBUT or tear Osm and all interleukins.
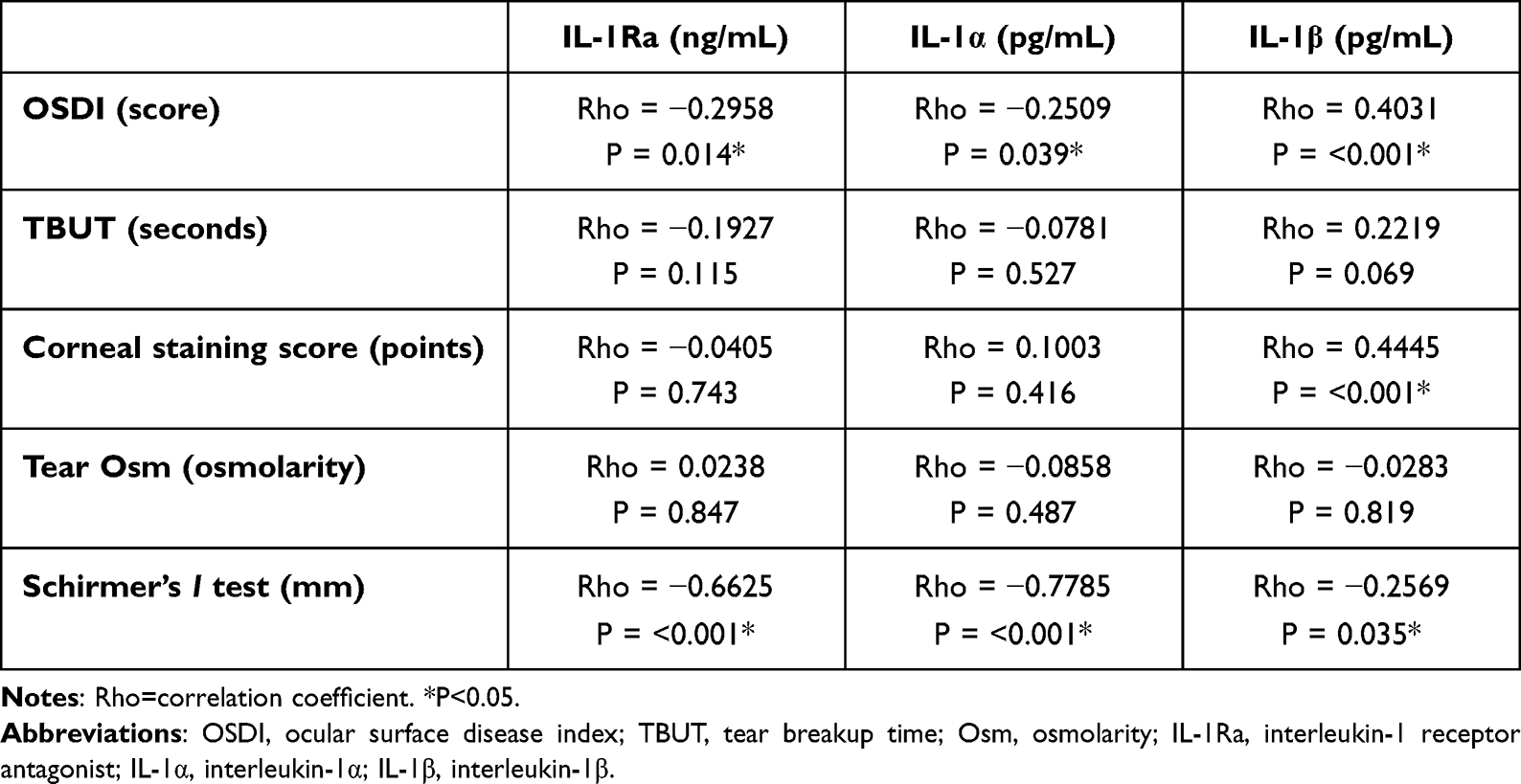 |
Table 2 Correlation Between OSDI, TBUT, Corneal Staining Score, Tear Osm, Schirmer’s I Test, and Interleukins (IL-1Ra, IL-1α, IL-1β) |
Discussion
Tear hyperosmolarity, which may initiate the pathological process involved in inflammation, leads to a vicious cycle of DED. The mitogen-activated protein kinase and nuclear factor kappa B signaling pathways are stimulated by tear hyperosmolarity, which leads to an increase in inflammatory cytokines in the ocular surface, including IL-1α, IL-1β, TNF-α, and MMP-9. These mediators induce a cascade of inflammation, which in turn causes damage to apoptotic and non-apoptotic death (ie, necrosis) of epithelial and goblet cells.7
Previous studies have shown that topical IL-1 receptor inhibitors (isunakinra) and topical IL-1Ra (anakinra) improve OSD symptoms and signs after treatment.8,12 However, systemic monoclonal antibodies against IL-1β (canakinumab) did not affect the signs and symptoms of DED.15
Our study showed improvements in corneal staining and OSDI scores but not in the Schirmer’s test. Corneal staining showed a statistically significant improvement of 1.30 scores (23.5%). Meanwhile, isunakinra can improve corneal staining by 33%. This may be a result of different routes of administration. Oral intake of diacerein may not reach the ocular surface as compared to topical isunakinra, which directly contacts the ocular surface.8 The OSDI also showed a statistically significant improvement (score of 17.2) with a shift from severe DED to moderate DED, as determined by the criteria recommended by Schiffman et al.21 Nonetheless, the tear breakp time (TBUT) exhibited a statistically significant decline of 0.66 seconds. This may not be clinically significant. In addition, Schirmer’s test and tear Osm results did not show significant changes; this may be because our study population had a mild disease that might have a slight improvement margin. Many reports have also demonstrated an inconsistent association between signs and symptoms and disagreement among signs in DED.24–27
A strong evidence indicated that artificial tear could alleviate symptoms and signs of dry eye disease including TBUT, tear meniscus height, and tear ferning pattern.28,29 As artificial tear use might interfere with the signs and symptoms of DED, this study also recorded the amount of artificial tear use. Participants used artificial tears significantly less than before the diacerein treatment, which was in accordance with the significantly improved OSDI score.
The present study was conducted over 2 months according to the onset of diacerein on osteoarthritis.10,13 However, the onset of diacerein effects on the ocular surface remains unknown, so a more extended period may be needed to observe the enhancement of sensory-stimulated reflex tearing, leading to improved lacrimal gland function, such as the cyclosporin-A mechanism (up to 8 months after initiation), which might improve the Schirmer’s test results.30,31
Diacerein exhibits potential benefits over canakinumab due to its dual action of reducing IL-1β and increasing IL-1Ra, as opposed to canakinumab solely reducing IL-1β.15 As a result, diacerein can better reduce the inflammatory effect. In addition, diacerein is easy to use because it is administered orally compared to canakinumab, which requires a subcutaneous injection. Furthermore, diacerein is also a common drug used in orthopedic guidelines for osteoarthritis, with a lower price of US$ 26 per 30 tablets as compared to the cost of canakinumab (US$ 17,000/dose, injected every 4–8 weeks).
Interleukin-1 is a family of proteins in which major members are IL-1α, IL-1β, and IL-1RA. Each cytokine could be found in various tissue conditions. IL-1α is found in the cytoplasm of healthy keratinocytes, thymic epithelium, mucous epithelium as well as epithelium at ocular surfaces.32 Previous studies have shown that IL-1α levels were higher in DED than in healthy eyes,33,34 consistent with our results. From our knowledge, the mechanism of diacerein does not inhibit IL-1α, so the elevating IL-1α levels after diacerein administration in our experiment cannot be explained. Further study is needed to investigate the influence of diacerein on the mechanism of IL-1α. It is evident that IL-1β could be found only in the inflammatory process.35 After administering diacerein for 2 months, the level of IL-1β significantly declined. This is a result of restriction effect of diacerein on ICE.36–38 Previous in vivo studies reported that ICE knockout mice had not exported IL-1α and IL-1β, whereas our study showed that IL-1α was upregulated.39 IL-1Ra, a natural pro-inflammatory antagonist, is indirectly increased after diacerein intake;38 however, our study showed an insignificant increase in IL-1Ra levels in tears. A previous study reported that tear cytokines could vary during the days.40,41 Nevertheless, our results are considered reliable because we collected tears from the same afternoon period to reduce the effect of varying levels of interleukin during the day. Although the influence of diacerein is great on IL-1β, the clinical examination like corneal staining, improved. Diacerein may be a promising treatment modality for DED.
A previous study demonstrated that tear hyperosmolarity could stimulate tear cytokine production.42 However, our study showed no correlation between tear osmolarity and IL-1α, IL-1β, or IL-1Ra. The TFOS DEWS II stated that tear inflammatory mediators lead to epithelial cell loss, which was observed through corneal staining.7 Our study also showed that corneal staining and OSDI scores have moderate positive correlations with IL-1β levels in tears. Moreover, Schirmer’s test results showed a strong negative correlation with IL-1α, IL-1β, and IL-1Ra, which could be from lower tear volume inducing the release of inflammatory cytokines, including IL-1Ra, to encounter inflammation. In addition, IL-1Ra reportedly negatively correlates with Schirmer’s test results.43 The positive correlation between DE symptoms and IL-1β was in accordance with a previous study.43 Moreover, IL-1β was found to contribute to the loss of corneal epithelial barrier function in a previous study,44 which supports the positive correlation between IL-1β and corneal staining score in our study.
Some limitations may have influenced our results. First, this was an observational study with no comparison to a placebo group. Second, the small sample size may have influenced this study. Third, most participants were female; hence, it might be difficult to generalize the results to the entire population. We suggest conducting a randomized controlled clinical trial for future research to provide a robust outcome.
Conclusion
This is the first study to investigate the efficacy of short-term (2 months) systemic diacerein treatment on ocular surface health from a clinical and basic science perspective. Diacerein demonstrated a positive effect on ocular surface damage by statistically significant improvement in symptoms (OSDI) and signs (corneal staining), as confirmed by the decreased levels of inflammatory cytokines (IL-1β) and insignificantly increased IL-1Ra. Hence, diacerein may benefit patients with osteoarthritis and OSD. Based on this finding, other ocular inflammatory diseases involving IL-1β can be investigated in the future.
Data Sharing Statement
The raw data used in this study are available upon reasonable request from the corresponding author.
Acknowledgments
The authors would like to acknowledge Dr Nipan Israsena for helping us with the cytokine extraction process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Ratchadapiseksompotch Fund, Chulalongkorn University, Bangkok, Thailand. [grant number CU_GR_63_134_30_41].
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Lee WB, Mannis MJ. Historical Concepts of Ocular Surface Disease. Elsevier; 2013:3–10. doi:10.1016/b978-1-4557-2876-3.00001-8
2. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
3. Lekhanont K, Rojanaporn D, Chuck RS, Vongthongsri A. Prevalence of dry eye in Bangkok, Thailand. Cornea. 2006;25(10):1162–1167. doi:10.1097/01.ico.0000244875.92879.1a
4. Ngamjit K, Suchaya G, Suphawadee E, Pamornsak T, Sutthichai J. Prevalence of dry eyes in elderly Thai population (the Romklao eye study). Asian Biomed. 2012;6(6):875–882. doi:10.5372/1905-7415.0606.134
5. Kelley J, Bohm ARD, Stephen C, Christopher E. Dry eye. In: Cornea. Elsevier; 2017:377–395. chap Chapter 33 Dry Eye.
6. McDonald M, Patel DA, Keith MS, Snedecor SJ. Economic and humanistic burden of dry eye disease in Europe, North America, and Asia: a systematic literature review. Ocul Surf. 2016;14(2):144–167. doi:10.1016/j.jtos.2015.11.002
7. Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pathophysiology report. Ocul Surf. 2017;15(3):438–510. doi:10.1016/j.jtos.2017.05.011
8. Goldstein MH, Martel JR, Sall K, et al. Multicenter study of a novel topical interleukin-1 receptor inhibitor, isunakinra, in subjects with moderate to severe dry eye disease. Eye Contact Lens. 2017;43(5):287–296. doi:10.1097/icl.0000000000000276
9. Kapoor M, Martel-Pelletier J, Lajeunesse D, Pelletier JP, Fahmi H. Role of proinflammatory cytokines in the pathophysiology of osteoarthritis. Nat Rev Rheumatol. 2011;7(1):33–42. doi:10.1038/nrrheum.2010.196
10. Spencer CM, Wilde MI. Diacerein. Drugs. 1997;53(1):98–106. doi:10.2165/00003495-199753010-00007
11. Thai Rheumatism Association. Guideline for the treatment of osteoarthritis of knee; 2010. Available from: https://thairheumatology.org/phocadownload/36/Guideline_003.pdf.
12. Amparo F, Dastjerdi MH, Okanobo A, et al. Topical interleukin 1 receptor antagonist for treatment of dry eye disease: a randomized clinical trial. JAMA Ophthalmol. 2013;131(6):715–723. doi:10.1001/jamaophthalmol.2013.195
13. Fidelix TS, Macedo CR, Maxwell LJ, Fernandes Moça Trevisani V. Diacerein for osteoarthritis. Cochrane Database Syst Rev. 2014;(2). doi:10.1002/14651858.CD005117.pub3
14. Pavelka K, Bruyère O, Cooper C, et al. Diacerein: benefits, risks and place in the management of osteoarthritis. An opinion-based report from the ESCEO. Drugs Aging. 2016;33(2):75–85. doi:10.1007/s40266-016-0347-4
15. Grosskreutz CL, Hockey H-U, Serra D, Dryja TP. Dry eye signs and symptoms persist during systemic neutralization of IL-1β by canakinumab or IL-17A by secukinumab. Cornea. 2015;34(12):1551–1556. doi:10.1097/ICO.0000000000000627
16. Lemp A. Report of the national eye institute/industry workshop on clinical trials in dry eyes. Eye Contact Lens. 1995;21(4):221–232.
17. Bron AJ, Abelson MB, Ousler G, et al. Methodologies to diagnose and monitor dry eye disease: report of the diagnostic methodology subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):108–152. doi:10.1016/S1542-0124(12)70083-6
18. Keech A, Senchyna M, Jones L. Impact of time between collection and collection method on human tear fluid osmolarity. Curr Eye Res. 2013;38(4):428–436. doi:10.3109/02713683.2013.763987
19. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II diagnostic methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
20. VanDerMeid KR, Su SP, Krenzer KL, Ward KW, Zhang JZ. A method to extract cytokines and matrix metalloproteinases from Schirmer strips and analyze using Luminex. Mol Vis. 2011;17:1056–1063.
21. Schiffman RM, Christianson M, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
22. Park Y, Song JS, Choi CY, Yoon KC, Lee HK, Kim HS. A randomized multicenter study comparing 0.1%, 0.15%, and 0.3% sodium hyaluronate with 0.05% cyclosporine in the treatment of dry eye. J Ocul Pharmacol Ther. 2017;33(2):66–72. doi:10.1089/jop.2016.0086
23. Kheirkhah A, Di Zazzo A, Satitpitakul V, Fernandez M, Magilavy D, Dana R. A pilot randomized trial on safety and efficacy of a novel topical combined inhibitor of Janus Kinase 1/3 and spleen tyrosine kinase for GVHD-associated ocular surface disease. Cornea. 2017;36(7):799–804. doi:10.1097/ico.0000000000001206
24. Bartlett JD, Keith MS, Sudharshan L, Snedecor SJ. Associations between signs and symptoms of dry eye disease: a systematic review. Clin Ophthalmol. 2015;9:1719–1730. doi:10.2147/opth.S89700
25. Kyei S, Dzasimatu SK, Asiedu K, Ayerakwah PA. Association between dry eye symptoms and signs. J Curr Ophthalmol. 2018;30(4):321–325. doi:10.1016/j.joco.2018.05.002
26. Onwubiko SN, Eze BI, Udeh NN, Onwasigwe EN, Umeh RE. Dry eye disease: concordance between the diagnostic tests in African eyes. Eye Contact Lens. 2016;42(6):395–400. doi:10.1097/icl.0000000000000218
27. Unlu C, Guney E, Akcay BI, Akcali G, Erdogan G, Bayramlar H. Comparison of ocular-surface disease index questionnaire, tearfilm break-up time, and Schirmer tests for the evaluation of the tearfilm in computer users with and without dry-eye symptomatology. Clin Ophthalmol. 2012;6:1303–1306. doi:10.2147/opth.S33588
28. Che Arif FA, Hilmi MR, Kamal MK, Ithnin MH. Comparison of immediate effects on usage of dual polymer artificial tears on changes in tear film characteristics. Malaysian J Med Health Sci. 2021;17(3):252–258.
29. Che Arif FA, Hilmi MR, Kamal KM. A prospective contralateral eye comparison of the tolerability of two artificial tears with different physical properties in patients with dry eye disease. Med Hypothesis Discov Innov Optom. 2023;4(1):1–6. doi:10.51329/mehdioptometry167
30. Wan KH, Chen LJ, Young AL. Efficacy and safety of topical 0.05% cyclosporine eye drops in the treatment of dry eye syndrome: a systematic review and meta-analysis. Ocul Surf. 2015;13(3):213–225. doi:10.1016/j.jtos.2014.12.006
31. Rao SN. Topical cyclosporine 0.05% for the prevention of dry eye disease progression. J Ocul Pharmacol Ther. 2010;26(2):157–164. doi:10.1089/jop.2009.0091
32. Dinarello CA, Netea MG. The interleukin-1 family. In: Fundamental Immunology.
33. Zhao H, Li Q, Ye M, Yu J. Tear luminex analysis in dry eye patients. Med Sci Monit. 2018;24:7595–7602. doi:10.12659/msm.912010
34. Solomon A, Dursun D, Liu Z, Xie Y, Macri A, Pflugfelder SC. Pro- and anti-inflammatory forms of interleukin-1 in the tear fluid and conjunctiva of patients with dry-eye disease. Invest Ophthalmol Vis Sci. 2001;42(10):2283–2292.
35. Dinarello CA. Overview of the IL-1 family in innate inflammation and acquired immunity. Immunol Rev. 2018;281(1):8–27. doi:10.1111/imr.12621
36. Moldovan F, Pelletier JP, Jolicoeur FC, Cloutier JM, Martel-Pelletier J. Diacerhein and rhein reduce the ICE-induced IL-1beta and IL-18 activation in human osteoarthritic cartilage. Osteoarthritis Cartilage. 2000;8(3):186–196. doi:10.1053/joca.1999.0289
37. Martel-Pelletier J, Mineau F, Jolicoeur FC, Cloutier JM, Pelletier JP. In vitro effects of diacerhein and rhein on interleukin 1 and tumor necrosis factor-alpha systems in human osteoarthritic synovium and chondrocytes. J Rheumatol. 1998;25(4):753–762.
38. Yaron M, Shirazi I, Yaron I. Anti-interleukin-1 effects of diacerein and rhein in human osteoarthritic synovial tissue and cartilage cultures. Osteoarthritis Cartilage. 1999;7(3):272–280. doi:10.1053/joca.1998.0201
39. Chiu JW, Binte Hanafi Z, Chew LCY, Mei Y, Liu H. IL-1α processing, signaling and its role in cancer progression. Cells. 2021;10(1):92. doi:10.3390/cells10010092
40. Uchino E, Sonoda S, Kinukawa N, Sakamoto T. Alteration pattern of tear cytokines during the course of a day: diurnal rhythm analyzed by multicytokine assay. Cytokine. 2006;33(1):36–40. doi:10.1016/j.cyto.2005.11.013
41. Benito MJ, González-García MJ, Tesón M, et al. Intra- and inter-day variation of cytokines and chemokines in tears of healthy subjects. Exp Eye Res. 2014;120:43–49. doi:10.1016/j.exer.2013.12.017
42. Luo L, Li DQ, Corrales RM, Pflugfelder SC. Hyperosmolar saline is a proinflammatory stress on the mouse ocular surface. Eye Contact Lens. 2005;31(5):186–193. doi:10.1097/01.icl.0000162759.79740.46
43. Chen H, Chen H, Liang L, et al. Evaluation of tear protein markers in dry eye disease with different lymphotoxin-alpha expression levels. Am J Ophthalmol. 2020;217:198–211. doi:10.1016/j.ajo.2020.03.013
44. Kimura K, Teranishi S, Nishida T. Interleukin-1beta-induced disruption of barrier function in cultured human corneal epithelial cells. Invest Ophthalmol Vis Sci. 2009;50(2):597–603. doi:10.1167/iovs.08-2606
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.