Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Efficacy of Emerging Technologies to Manage Childhood Obesity
Authors Alotaibi M ![]() , Alnajjar F
, Alnajjar F ![]() , Cappuccio M, Khalid S, Alhmiedat T
, Cappuccio M, Khalid S, Alhmiedat T ![]() , Mubin O
, Mubin O
Received 5 January 2022
Accepted for publication 13 April 2022
Published 21 April 2022 Volume 2022:15 Pages 1227—1244
DOI https://doi.org/10.2147/DMSO.S357176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Mohammad Alotaibi,1 Fady Alnajjar,2 Massimiliano Cappuccio,3 Sumaya Khalid,2 Tareq Alhmiedat,1,4 Omar Mubin5
1Faculty of Computers and Information Technology, University of Tabuk, Tabuk, Saudi Arabia; 2College of Information Technology, United Arab Emirates University, Abu Dhabi, United Arab Emirates; 3School of Engineering and IT, University of New South Wales Canberra, Canberra, Australia; 4Industrial Innovation & Robotics Center, University of Tabuk, Tabuk, Saudi Arabia; 5School of Computer, Data and Mathematical Sciences, Western Sydney University, Sydney, Australia
Correspondence: Fady Alnajjar, Email [email protected]
Abstract: Childhood obesity is a widespread medical condition and presents a formidable challenge for public health. Long-term treatment strategies and early prevention strategies are required because obese children are more likely to carry this condition into adulthood, increasing their risk of developing other major health disorders. The present review analyses various technological interventions available for childhood obesity prevention and treatment. It also examines whether machine learning and technological interventions can play vital roles in its management. Twenty-six studies were shortlisted for the review using various technological strategies and analysed regarding their efficacy. While most of the selected studies showed positive outcomes, there was a lack of studies using robots and artificial intelligence to manage obesity in children. The use of machine learning was observed in various studies, and the integration of social robots and other efficacious strategies may be effective for treating childhood obesity in the future.
Keywords: childhood obesity, intervention, exergaming, machine learning, artificial intelligence
Corrigendum for this paper has been published.
Introduction
Childhood obesity is a major concern for healthcare systems and remains a challenge for medical innovation.1 Cases of overweight or obese children (infant and young) have significantly increased worldwide to 41 million and are continuously increasing.2 The huge socioeconomic transformations have significantly affected the nutrition and development of children and adolescents, particularly in developing countries. Increasing rates of urbanization has had a global effect on lifestyle, reducing the frequency of physical activity and increasing the calorie intake of nontraditional foods and “fast foods” rather than fruits and vegetables.3,4 In addition to children showing a greater frequency of being overweight or obese, these food choices lead to nutritional deficits in growing children, which may lead to future health issues.5
Without intervention, overweight or obese children are more prone to carrying their condition into adulthood, possibly increasing their chances of developing diseases such as diabetes, cardiovascular diseases, and cancer.6–8 Approximately 33% of preschool-aged children who are obese or overweight become obese adults, and 50% of obese school-aged children and 80% of adolescents carry obesity into adulthood.9 Therefore, it is crucial to develop strategies for the early diagnosis, prevention, and management of childhood obesity.
Currently available conventional interventions to manage weight are not always feasible as they are often inaccessible because of high cost, commute inconveniences, and lack of facilities.10 Extreme cases may require bariatric surgery, which is both expensive and risky.11 Approximately 80% of children aged 12–17 years are hesitant to engage in any kind of coordinated activities, such as sports; therefore, a need for creative intervention is yet required.12
Over the past decade, advances in portable digital technologies that provide personalized access to relevant information have facilitated the evolution of preventive strategies and interactive aids and have become readily available. Smart digital health interventions are designed to cater to a wide number of issues because they help track and monitor health as well as collect information for analysis by a specialist to determine the required treatment strategy. These interventions include weight management programs based on websites13 or social media.14 They are wearable15 and are easily accessible via websites and mobile applications. These interventions are easily adaptable to different environments, affordable and time saving. Most importantly, strategies based on these technological tools keep children motivated and engaged while enjoying the comfort of their homes. Technology-based interventions for childhood obesity can be mainly classified into the following categories: (1) active video games or exergaming; (2) website, social media-based activities16 or mobile application-based activities;17 (3) machine learning (ML)-based strategies.18 A combination of those categories does also exists.
Mobile phones are the most readily and commonly available gadgets. They can be conveniently connected to wearables and sensors, providing the user with real-time data and monitoring physiological changes with internet cloud connectivity. Combining sensors and connectivity enables behavior (eg, physical activity and diet) to be monitored and influenced, and health care providers or experimenters can be alerted to changes (eg, weight and glucose). This technology offers a great opportunity to tap into new media channels that are integral to the youth culture because mobile phones are already widely used by children.19
The use of exergames, which combine exercise and video games, is another concept that is gaining popularity. These games are designed to encourage children to perform physical exercise or execute certain movements to clear levels and earn rewards in the game. They keep children motivated and engaged over time, making it easier for them to consistently follow a regular fitness program. Many available applications use this concept in combination with a wearable device. Exergames are suitable for every age group. For example, Let us move (To move!) is a program designed in the form of a video game to prevent and treat obesity in children.20 Zamzee is another application for adolescents21 that records physical activity via a device. The number of points earned is calculated by the computer and can be exchanged for goods from partnering companies.
ML is an emerging strategy22,23 implemented by many computerized systems used in a clinical context.24,25 An ML-based approach provides beneficial insight into data to extract relevant information and has been actively used for the prognosis and diagnosis of several chronic conditions, particularly in patients with diabetes and sepsis.26,27
Despite being potentially very efficacious in obesity, there are surprisingly few reviews in the literature regarding the application of ML for childhood obesity management and treatment. Available reviews mainly focus on mobile devices, wearables, and interactive electronic media or predictive models based on statistics. One review28 addressed the potential use of computer decision systems (CDS) showing the main features and results of studies that use ML techniques and CDS.
Social robots are also being developed and tested in various healthcare concepts. Social robots have significant potential to assist healthcare workers and deliver customized care to children because they are more capable than other types of interactive technologies to positively influence the behavior and motivation of the human interactants. This superior potential derives from the fact that social robots, unlike other assistive technologies, are embodied agents with anthropomorphic or zoomorphic features. In some cases, robots also have a limited ability to navigate or manipulate the physical environment, enabling them to engage in embodied interaction with humans and share a concrete focus of attention (object or activity) with them. Furthermore, the ability to express emotions and interest is much more developed in person-like agents, such as robots, compared with impersonal technologies, such as mobile phone or tablet applications.
Robinson et al29 described the potential of robots and demonstrated that an autonomous social robot can efficaciously motivate adults to reduce the consumption of high-calorie snacks, aiding a low-powered therapy on dietary intake with no human intervention. Building on this and analogous examples of robots acting as coaches and lifestyle advisors, a “virtuous” theoretical approach to robot design has been proposed.30,31 This “virtuous robotics” approach can be applied to obesity management where robots can be programmed and deployed to cater to specific health and psychological requirements, motivate children to perform physical activities, and encourage healthier eating habits. Robots are suited for this motivational/assistive role because they are perceived as toys by children and can be a source of companionship, provide comfort and relief, and gain the trust of children, which is indispensable to give children explicit instructions and help in reforming their dietary habits.
Several reviews have explored obesity management using different technologies in children and adolescents and compared their efficacy in managing and preventing obesity via various channels.32,33 No reviews were specifically dedicated to analyzing the efficacy of robots and AI-based strategies compared with other technology-based techniques for obesity management in children and adolescents that have received more attention to date. The present systematic review aims to fill the gap by analyzing and comparing research studies published between the years 2010–2021 to map how ML techniques are used and how they compare with non-AI-based technological strategies in obesity management for children.
Materials and Methods
The present review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines using the following strategic approach. Studies included in this review were identified systematically by searching databases using the following keywords: obesity, obesity management, children, technology, exergaming, robots, machine learning, and overweight. The databases consulted were PubMed, IEEE Xplore, Scopus, and Google Scholar. Moreover, a few references of significant studies34,35 were scrutinized to extract more relevant articles suited to our review for further investigation and were shortlisted according to our criteria.
Inclusion and Exclusion Criteria
Studies fulfilled the inclusion criteria if they were (1) published in English; (2) published within the years 2010–2021; (3) based on obesity prevention or management (4) included participants aged ≤18 years; (5) were randomized controlled trials (RCTs) or interventions; (6) Used AI, robots or ML techniques.
Studies were excluded if they were (1) not in English; (2) had no reliable outcomes; (3) had participants aged >18 years; (4) did not use any types of technology in their research; and (5) were reviews, book chapters, thesis or conference material.
Quality Assessment Strategy
A modified Delphi list was used to assess the quality of each study.36 The assessment quality was improved by considering the following elements: age range, sample size, and intervention duration. The latter two were considered with the understanding that a smaller sample size and a shorter intervention duration might negatively impact generalizability and reproducibility.
Additional considerations were given to a study’s purpose, whether they were preventive, screening-based, experimental or treatment-based. Also, the methods of the study were taken into consideration if they were activity/video game based, web/mobile based or ML based. The choice of elements included in the quality assessment was guided by a previously published systematic review conducted by Nouchi et al.34
Results
A total of 1244 articles obtained from various databases were screened and duplicate articles were rejected. The titles and abstracts of the remaining 250 articles were screened for relevancy, and 75 articles were identified for full-text reading, 26 were finalized for review. A review of each study was performed, and information related to the layout and purpose of the study, as well as details of the participants (age, gender, size, and characteristics) were extracted.
The selection strategy for our review is illustrated (Figure 1). Table 1 shows an overview of the study characteristics, Table 2 outlines the key findings of the included literature, and Table 3 shows the assessment of the quality of studies using a delphi list. The studies were of various types, such as RCTs, experimental studies, or screening studies. The overall sample size analyzed ranged from 17 to 18,818, and the age of the participants ranged from 9 months to 18 years. Most studies were not gender specific and included both males and females, except for one study by Staiano et al that only included females.42
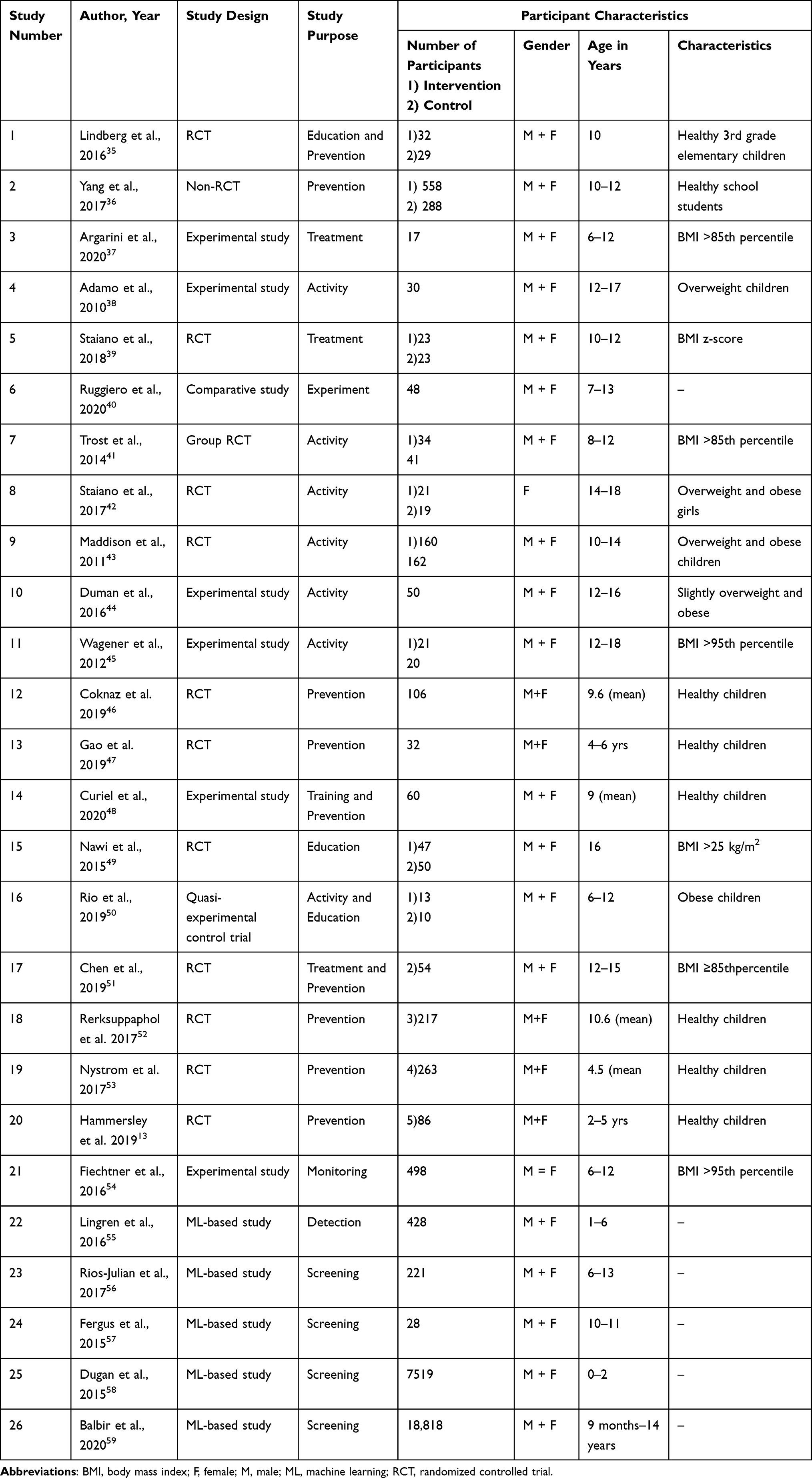 |
Table 1 Characteristics of the Included Literature |
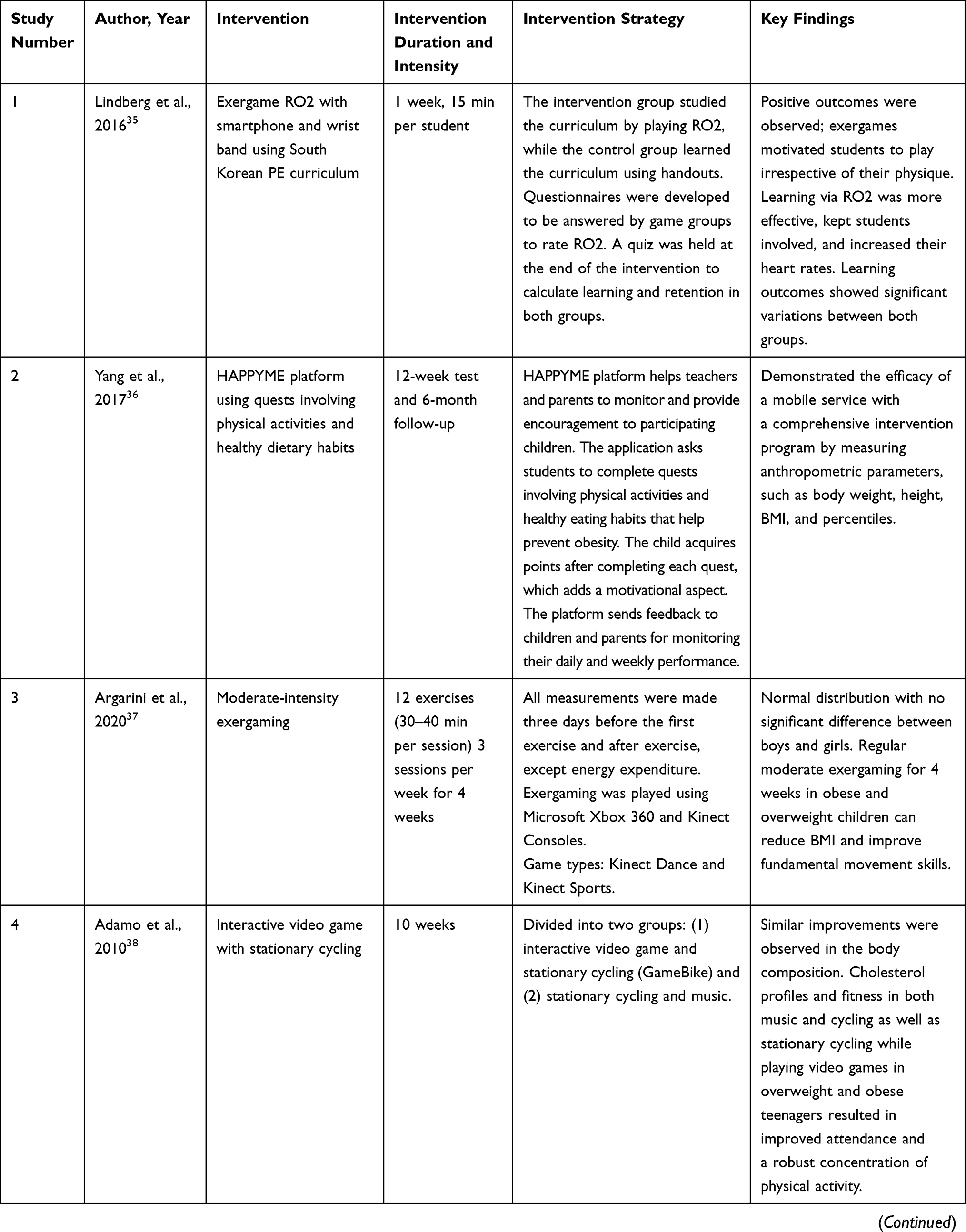 | 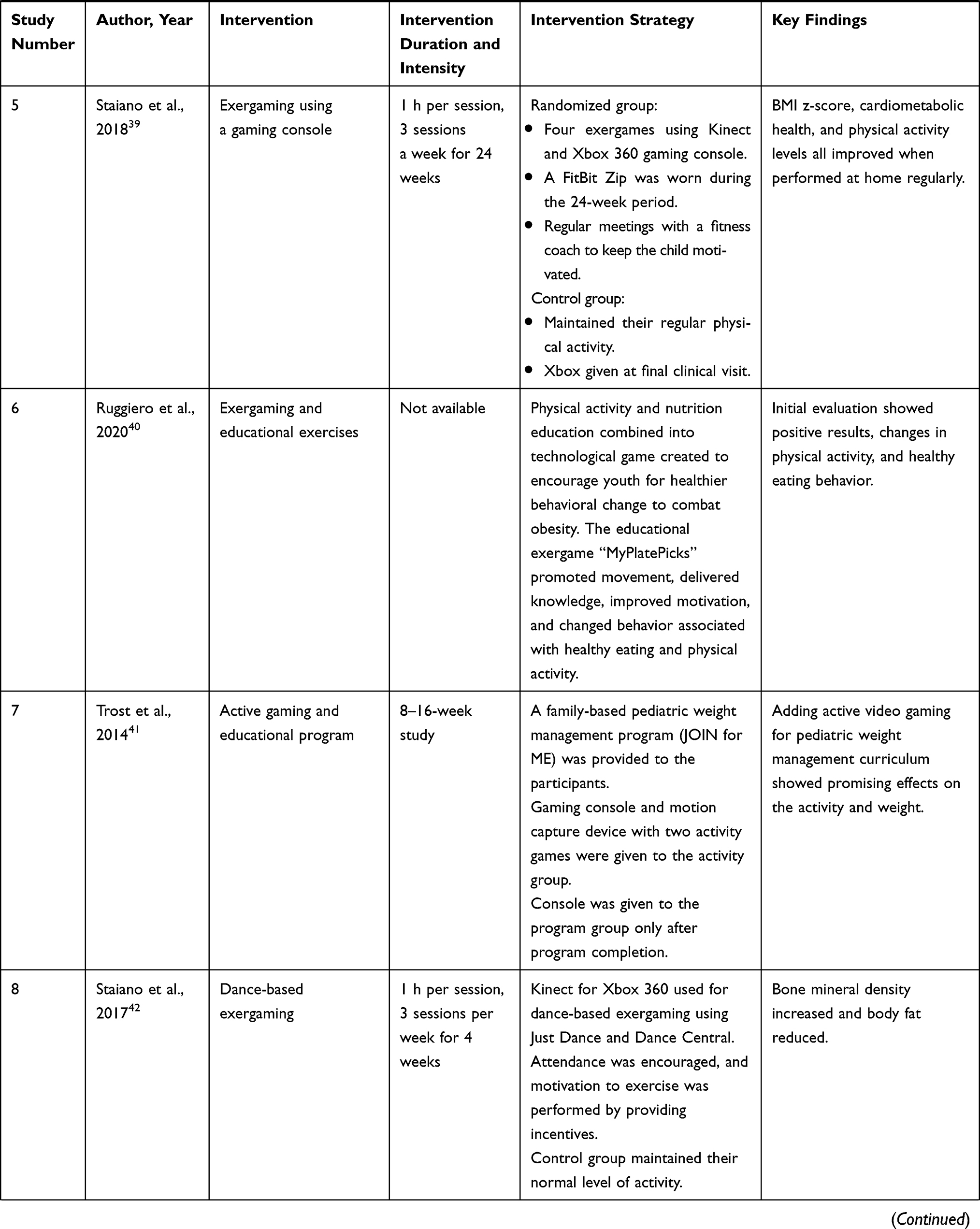 |  | 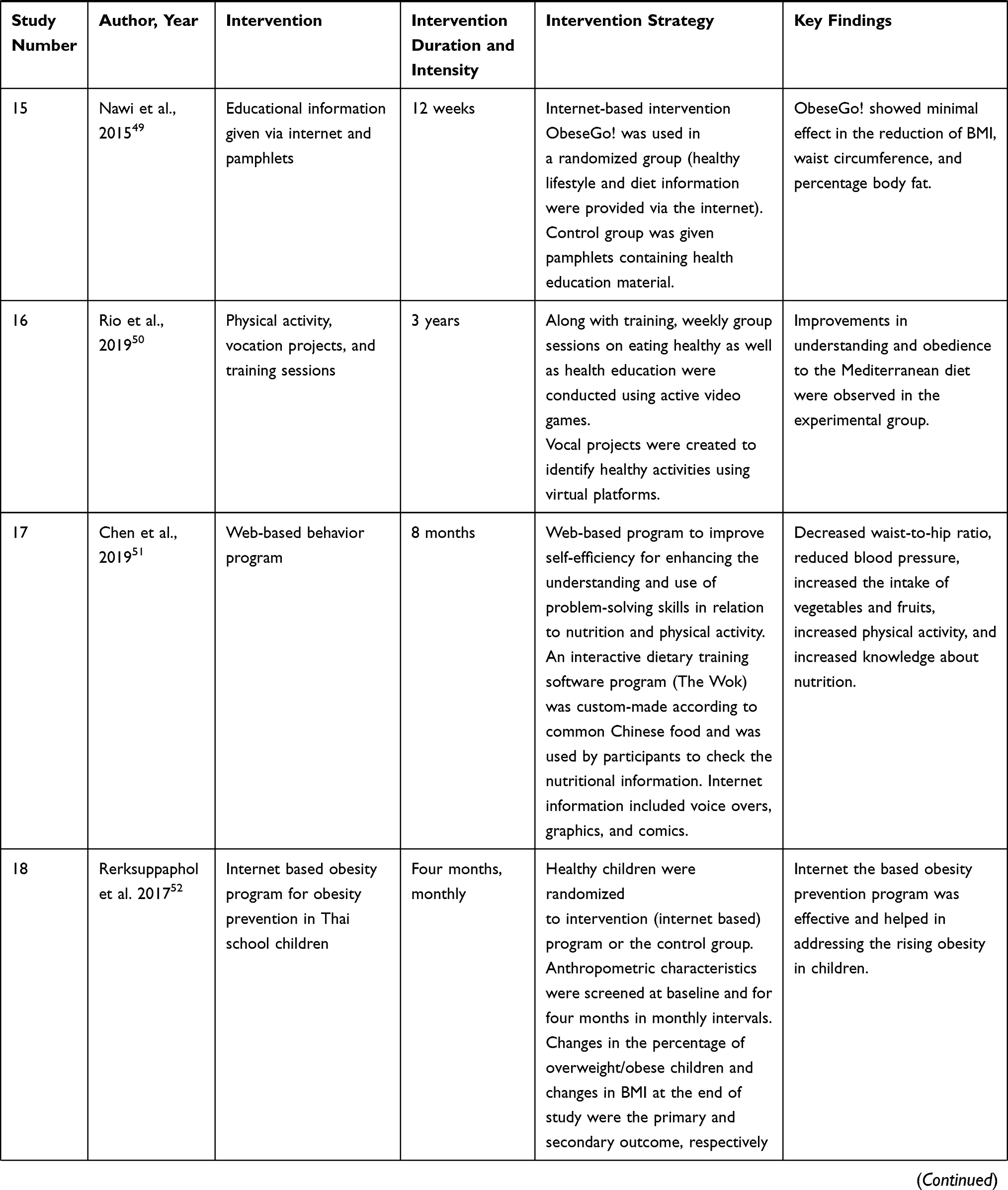 | 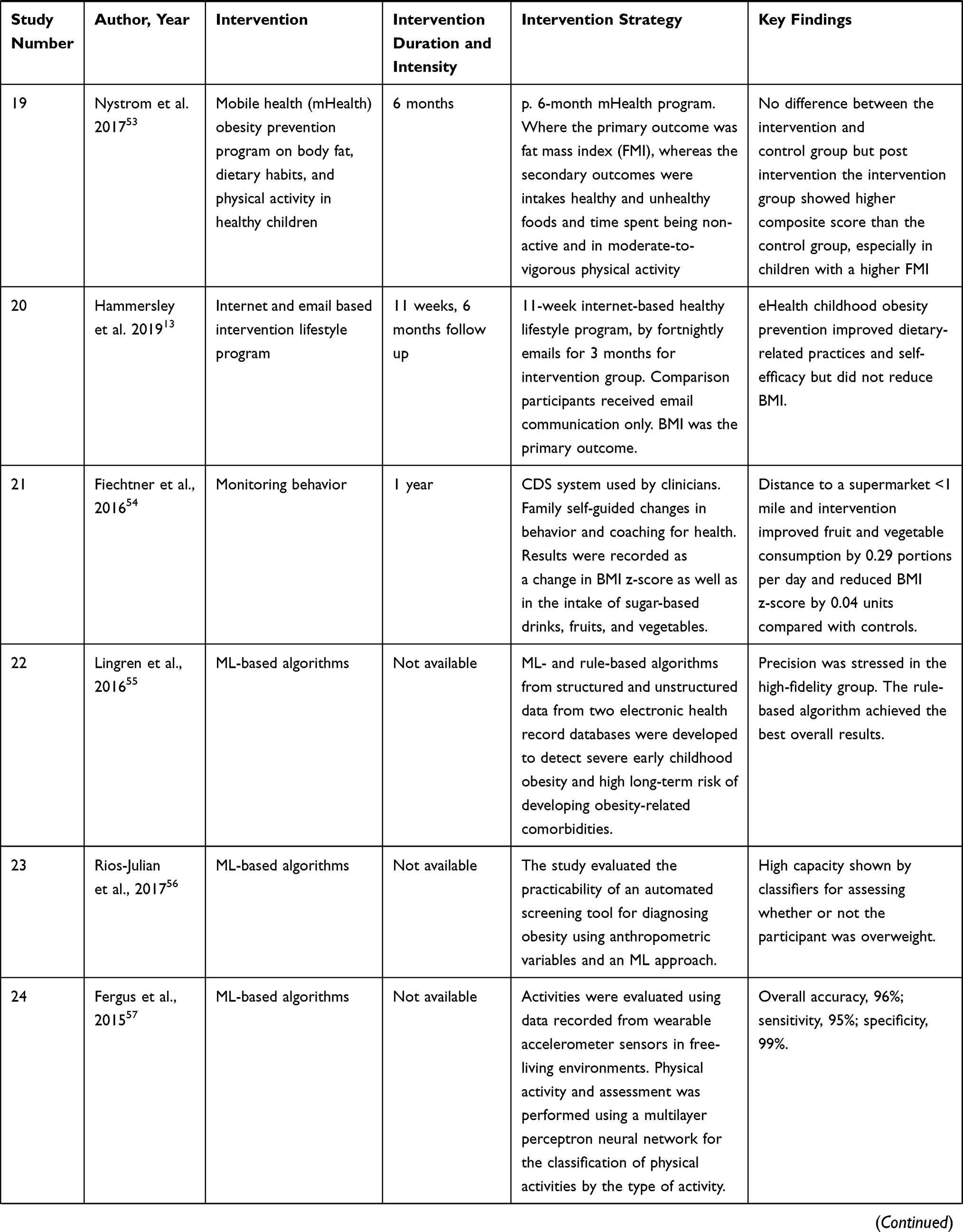 | 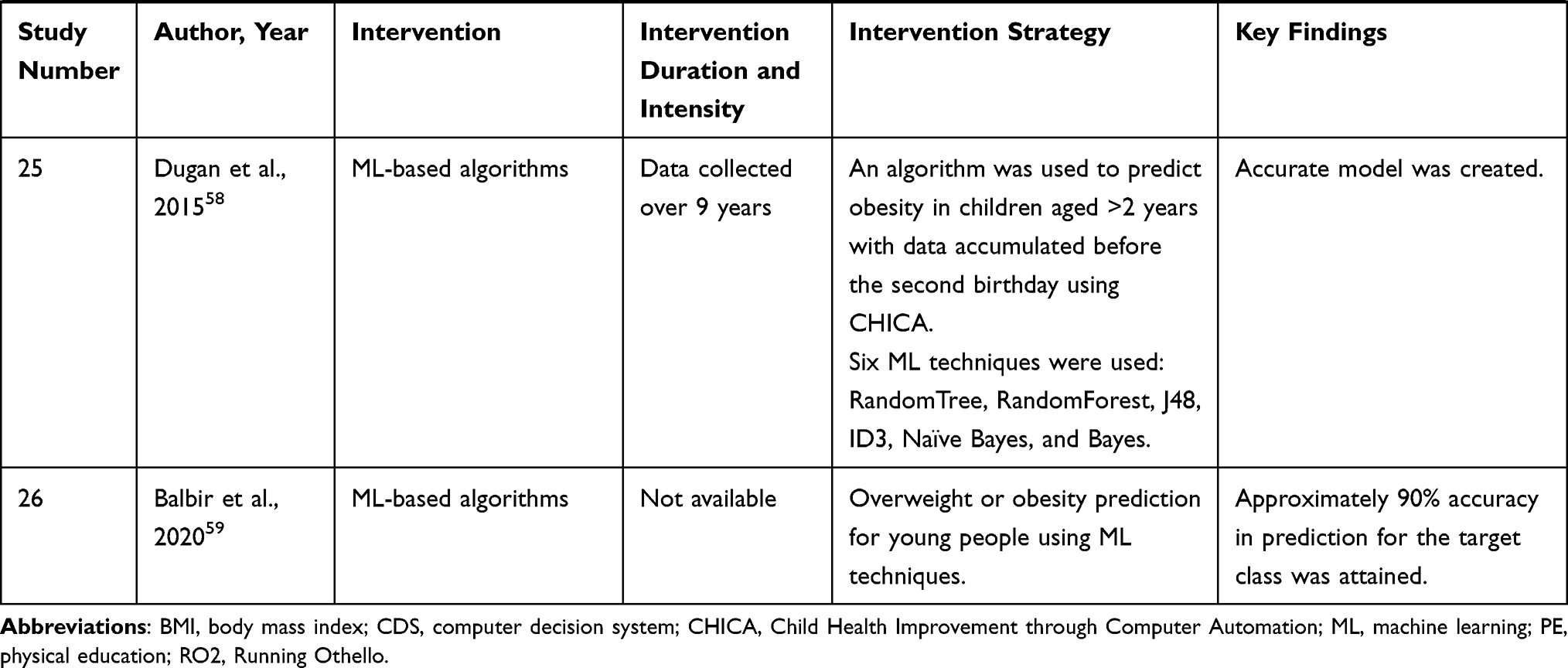 |
Table 2 Key Findings of the Studies |
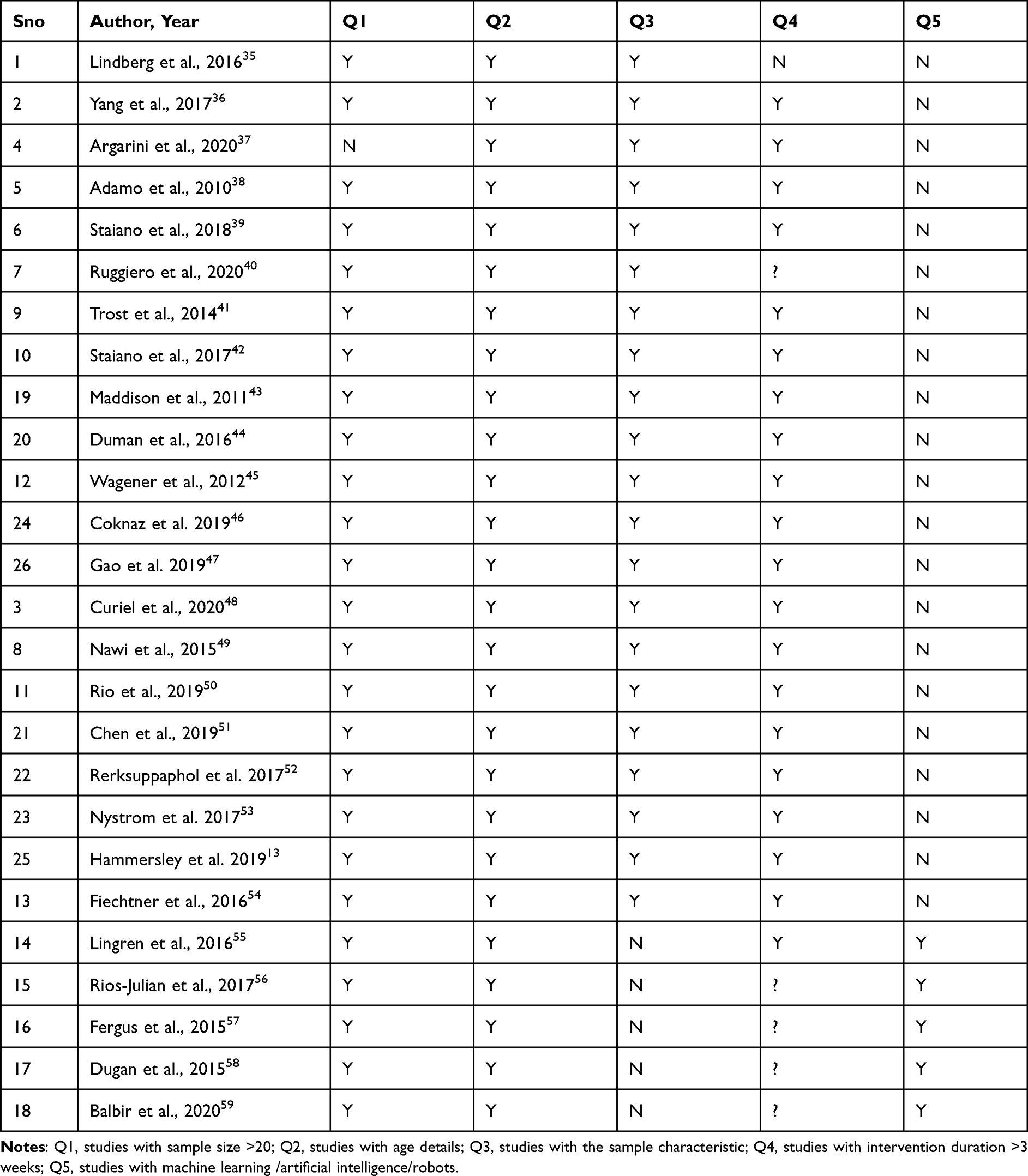 |
Table 3 Quality Assessment of Included Studies |
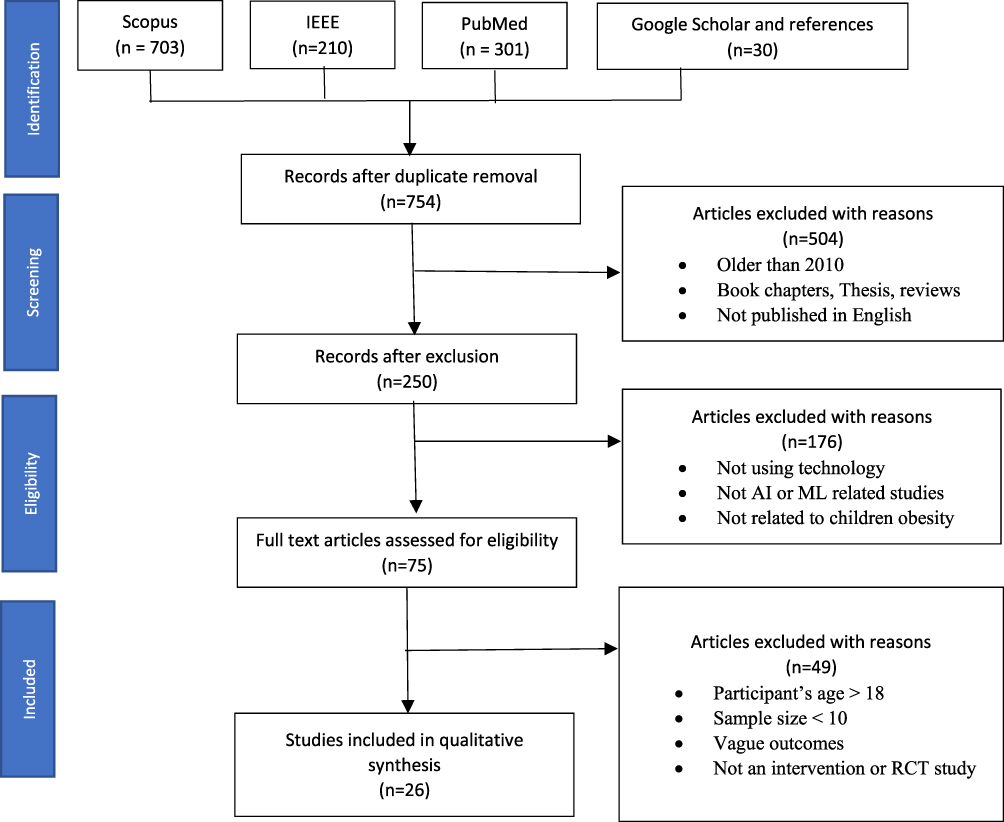 |
Figure 1 Search strategy used for selection of studies. |
All studies focused on technology-based interventions. Most studies13,37–39,41–45,49–54 involved overweight or obese participants, a few13,35,36,46–48,52,53 included healthy participants, and others did not specify the characteristics of the participants.40,55–59 The technology-based interventions were classified into three categories: (1) active video games or exergaming; (2) web, internet-based activities or mobile application-based activities; (3) ML-based strategies;
The duration of the intervention ranged from 1 week35 to 3 years,41 and the studies that used ML-based algorithms did not always specify the time period for data collection. Intervention intensity was reported in most studies, but not all,40,54–59 and was highly heterogeneous. Ten studies13,35,41,42,46,47,49,51–53 were RCTs that compared technology-driven intervention with a control group and used a non-technology-based intervention56 in which the control group played video games that were sedentary compared with the intervention group. The outcome of the studies varied according to the aim, but all comprised a body mass outcome, such as body mass index (BMI), BMI z-score, or BMI percentile. Other outcomes commonly observed included other anthropometrical, diet-based, and physical activity measurements.
Active Video Game Interventions
Twelve studies35,37–47 investigated the efficacy of active video games or exergaming. Lindberg et al35 incorporated the gaming program Running Othello into the South Korean school physical education (PE) curriculum for the intervention group, while the control group used printed leaflets and the regular curriculum. Positive results were observed in the intervention group as children were more engaged and showed increased heart rates compared with the control group. In another study, Argarini et al37 investigated the efficacy of moderate intensity exergaming on children with a BMI in the 85th percentile. Exergames were played using Xbox 360, and dance and sports-based games were played for four weeks. The results showed reduced BMI and improved fundamental movement skill, with no significant discrepancy between male and female participants. Adamo et al38 used the interactive video game, “GameBike” and included stationary cycling for two groups: one group performed stationary cycling with music and the other group used GameBike while performing stationary cycling. Regularity of exercise, energy consumption, aerobic fitness, body composition, and the risk of heart disorder in overweight and obese children were monitored. The music group performed considerably better and used more strength than the GameBike group. There were no statistically significant differences between or within groups with respect to BMI.
Staiano et al39 performed exergaming with Kinect and Xbox 360 gaming consoles using four simultaneous exergames, whereas the control group was required to maintain their regular level of physical activity. Statistically significant differences were observed in the intervention group, which showed improved scores, increased physical activity, and improved cardiometabolic health. Ruggiero et al40 developed the exergame “MyPlatePick” that combines nutrition education and physical activity to promote movement and encourage healthy behavioral changes. Positive changes in eating behavior and increased physical activity were noticed.
Trost et al41 evaluated the effect of exergaming on children participating in a group-based program for managing weight. Improvements in physical activity were observed in the gaming group compared with the control group, which only took part in the program and not in the exergaming. The active video game group showed reduced weight and BMI. Another study by Staiano et al42 examined the effects of dance-based exergaming on females matched to a control group who followed their normal level of physical activity. No statistically significant differences were observed between the groups at follow-up.
Rio et al50 tested a platform in which weekly group sessions with training were conducted on healthy-eating habits and active video games, and the participants developed their own vocal projects based on healthy activities. This study documented a positive effect on the intervention group in terms of nutritional knowledge and adherence to Mediterranean diet. Wagner et al45 studied the efficacy of dance-based exergaming on obese adolescents’ observed capability to exercise, self-regulation, and BMI compared with a wait-list control group. A statistically significant increase in the perceived ability to exercise was found based on self-reporting by the participants in the intervention group compared with the control group. However, no major variations were found for BMI z-score.
Duman et al44 used aerobics along with music and video games in their eight-week study and found a positive outcome in the final measurements with the exercise program using video games. Maddison et al43 investigated the effect of video games on physical activity and fitness compared with standard video games. They found a decrease in BMI and BMI z-score of active group participants compared with the children in the control group.
Web-Based/Mobile-Based Studies
Eight studies13,36,48–53 used interventions based on internet or smart phone applications. Yang et al36 developed a mobile-based HAPPYME platform that asks students to complete quests involving physical activity and healthy eating habits. The platform sends feedback to their parents who can then monitor the performance. Curiel et al48 developed a video game-based mobile application that enabled participants to complete quests based on physical activity and healthy eating. Another study by Nawi et al49 used the internet-based intervention ObeseGo! that provides information about healthy lifestyle and diet nutrition via the internet. This intervention showed no significant effect on BMI scores. Chen et al56 developed a web-based program that comprised self-assessment activities to determine problem-solving skills and an interactive software program customized to Chinese food that allowed the user to check nutritional information about the food they ate. Fiechtner et al54 developed a computerized clinician decision support system that monitored family behavior and found that living within one mile of a supermarket encouraged healthy eating habits.
ML-Based Studies
Five studies55–59 used ML-based strategies for their interventions. Lingren et al55 created both rule-based and ML-based algorithms using structured and unstructured data from two large electronic health records to detect severe early childhood obesity and children at a long-term risk of developing complications. The rule-based algorithms performed better overall. Rios-Julian et al56 used ML to estimate the feasibility of developing an automated screening tool for diagnosing obesity using anthropometric variables. Fergus et al57 used a wearable accelerometer to collect data that was used to evaluate physical tasks, and a multilayer perceptron neural network was used to classify physical activities according to type of activity. Dugan et al58 used ML on the collected data to develop an algorithm that could predict childhood obesity in children aged >2 years using data collected before their second birthday. Six different ML techniques, namely, RandomTree, RandomForest, J48, ID3, Naïve Bayes, and Bayes, trained using the Child Health Improvement through Computer Automation system data showed that a precise, sensitive model could be formed. Balbir et al59 developed ML algorithms to predict the risk of young people becoming obese in the future with a 90% accuracy.
Discussion
The objective of this systematic review was to assess the use of technology-based interventions in the management and prevention of childhood obesity and evaluate the use of ML and other technological strategies. Various technologies have been used, including video game-based interventions, mobile-based interventions, web-based interventions, phone communication-based interventions and machine learning-based interventions. It is important to note that along with these, multicomponent mediations, including both dietary intake and physical activity, are required to effectively overcome obesity.
Various parameters, such as BMI, body fat percentage, weight, heart rate, and BMI z-scores, have been used in these interventions to measure the progress and success of the interventions. Among the 26 studies under review, 21 studies showed positive significant outcomes on their respective outcome measures.
The present review classified the selected literature broadly into three categories: active video games or exergaming; internet or mobile-based interventions; and ML-based interventions. The two categories of web- or internet-based and mobile-based strategies were combined as one. The search did not yield any articles based on robot-based techniques to manage obesity in children; therefore, no such studies were included for that category, but one study60 was found to be using a social robot to manage and spread awareness about obesity in children of Saudi Arabia; however, since it was not an RCT or an intervention with outcomes, it was not included in the review literature.
Because of the complex etiology of childhood and adolescence obesity and the diversity of its possible influencing factors (eg, biological, psychological, dietary, behavioral, and cultural), conventional statistical methods, relying on linear models, have limitations as the analyses they offer typically have a limited predictive power. Most cases use the same prediction values transformed slightly, and it is difficult to find models capable of handling multidimensional data. In contrast, ML-based strategies are valuable tools for multidimensional datasets that involve complex relationships among multidomain variables. ML techniques can search for complicated nonlinear relations between prediction variables and response variables in an automated manner and do not require manual predefinition.61 Thus, the predictivity, ease of use, and robustness of ML-based models are superior to those of conventional models.36 Five studies incorporated ML strategies in their interventions. Most of these studies scanned existing electronic health records to prevent or detect obesity. Lingren et al55 detected severe cases of childhood obesity, and Rios-Julian et al56 determined the possibility of developing automated screening tools to detect obesity based on anthropometric variables using ML. Dugan et al58 and Singh et al59 developed algorithms to predict obesity in children and youngsters.
If a comparison is to be made between ML-based techniques and the other technological methods, it is difficult at this point in the research as ML studies are more focused on screening the databases to identify patterns, which can help in prediction and other strategies involving a different approach by various methods of training, games and information communication. It is not possible to compare two entirely different methods with different objectives, even though the main objective stands in managing and prevention of obesity, the method used is vastly different for them. Since the search did not reveal any AI and robot-based interventions, it can be concluded that this area has a lot of potential for future and needs to be actively researched.
On observing closely most of the studies, it can be broadly recognized as preventive, educational, activity-based, data screening, and treatment-based studies. It was perceived that the preventive and educational interventions were focused more on making the participants aware of the different kinds of food and their impacts on the body. They used various gaming methods to educate children, or internet/telephone-based methods to make children aware of the evil effects of unhealthy foods, high sugar diets, etc. They also highlighted the importance of physical activities and their rewards.
Michie62 outlines effective techniques in healthy eating and physical activity interventions, stating what makes an intervention effective in successfully changing the lifestyle or behavior of the participants for the better. These were the basic techniques according to S. Michie to bring about change in behavior: formation of an intention, setting up a specific goal, providing performance feedback, behavior self-monitoring and behavior goal reviews. Most of our studies did follow this pattern to some extent, where they had a targeted goal, set up intervention, tracked performance and feedback was taken even after post-intervention to assess self-monitoring efficacy.
Activity-based intervention were focused on exergaming, which kept children engaged and motivated to continue the program. The games came with levels and rewards, which kept the child interested and as a result, continued to play games. These activity-based methods were used for both managing obesity and in prevention strategies.
Even though varied in nature, the studies included mostly had very similar primary outcome measures like BMI score, body fat, BMI-z score, physical activity duration, weight measures, etc. Most studies focused on both the genders and did not do any gender-specific study except one study, which was a female-based study.42
The studies included in this review were of average quality, as only 5 of the 26 studies used ML or advanced techniques to detect or prevent obesity and did not specify the intervention duration. Furthermore, five studies did not define the characteristics of the participants. None of the studies used simple robots (without AI) or AI-based robots for the management of childhood obesity.
Overall, it can be seen that these different approaches to cater well to the childhood obesity issue have been effectively using technologies to keep children engaged and motivated when carrying out the required activities. Overall, it can be seen that these different approaches to cater well to the childhood obesity issue have been effective using creative methods to keep children engaged and motivated to carry out the required activities, using standard measures as primary outcomes, it gives a standardized way of evaluating the efficacy of each of these studies. Most studies showed positive results in both preventive and management-based approaches.
However, children require a different type of care than elderly people, and robots may be a good platform to fulfill these unique needs.63,64 Diseases, such as cancer and diabetes, can disrupt a child’s normal life, affect their social needs, and pose various challenges during the treatment of illness and change in lifestyle, which in turn also affect the mental health of the child.65,66 Social robots may prove to be helpful in the management of chronic illnesses because they can provide effective support through encouragement, education to adhere to healthy behaviors, and entertainment useful to mitigate stress thereby providing a sense of comfort and companionship.67 As such, robots have been shown to be helpful for treating various conditions,68 and it is reasonable to expect that they can have similar effects on the treatment of obesity, helping children emotionally and motivating them and subsequently leading them to a healthier lifestyle. While ML helps screening datasets to identify children at risk and make predictions about their condition, AI and robotics could be used to develop user-centric strategies based on the real-time customization of the treatment program.
Conclusion
Although almost all the studies analyzed were statistically sound and showed positive outcomes, our review shows that this area still lacks the use of robots and AI-based technologies.
A more efficacious intervention should be developed in the future by combining a more diverse set of techniques. Studies should focus on the positive aspects of each category and develop an integrated system where there is a physical entity, such as a robot with AI and ML capabilities, that can conduct a physical activity program for the participants and educate them regarding good eating habits. These robots can be implemented with adaptive and real-time feedback techniques, making it easier to monitor the progress in real-time from home. Most of the studies included in the present review showed positive statistical outcomes. Exergaming is the most popular strategy among the literature published in the past 10 years. Thus, our review indicates that technology-based interventions have great potential in terms of efficacy in monitoring and managing obesity in children and adolescents, but its potential has not been reached. This area of research still lacks AI and robot-based interventions, which could be combined with exergaming and ML techniques to maximize their effectiveness and establish a strategic synergy to promote children’s health. As for the future direction, we are currently at the stage of introducing an adaptable intelligent robot that can personalize the extent of interaction based on the child’s personal interest and level of obesity. Such personalization could enhance the benefits of using robots in the management of childhood obesity.
Funding
The authors would also like to acknowledge the financial support for this work from the Deanship of Scientific Research (DSR) university of Tabuk, Tabuk, Saudi Arabia, under grant no. [1440-258].
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
1. Wolfenden L, Ezzati M, Larijani B, Dietz W. The challenge for global health systems in preventing and managing obesity. Obesity Rev. 2019;20:185–193.
2. World Health Organization. Facts and figures on childhood obesity. Available from: https://www.who.int/end-childhood-obesity/facts/en/. Accessed March 2021.
3. Sahoo K, Sahoo B, Choudhury AK, et al. Childhood obesity: causes and consequences. J Fam Med Prim Care. 2015;4:187–192. doi:10.4103/2249-4863.154628
4. Spear BA, Barlow SE, Ervin C, et al. Recommendations for treatment of child and adolescent overweight and obesity. Pediatrics. 2007;120(Suppl 4):S254–S288. doi:10.1542/peds.2007-2329F
5. Prangthip, P., Soe, Y. M., & Signar, J. F. (2021). Literature review: nutritional factors influencing academic achievement in school-age children. International Journal of Adolescent Medicine and Health, 33(2). Available from: https://www.rch.org.au/kidsinfo/fact_sheets/Nutrition_older_children/.
6. Simmonds M, Burch J, Llewellyn A, et al. The use of measures of obesity in childhood for predicting obesity and the development of obesity-related diseases in adulthood: a systematic review and meta-analysis. Health Technol Assess (Rockv). 2015;19:1–336. doi:10.3310/hta19430
7. Shields M, Tremblay MS, Connor Gorber S, Janssen I. Abdominal obesity and cardiovascular disease risk factors within body mass index categories. Health Rep. 2012;23:7–15.
8. Vucenik I, Stains JP. Obesity and cancer risk: evidence, mechanisms, and recommendations. Ann NY Acad Sci. 2012;1271:37–43. doi:10.1111/j.1749-6632.2012.06750.x
9. Hoey H. Management of obesity in children differs from that of adults. Proc Nutr Soc. 2014;73:519–525. doi:10.1017/S0029665114000652
10. Jones M, Luce KH, Osborne MI, et al. Randomized, controlled trial of an internet-facilitated intervention for reducing binge eating and overweight in adolescents. Pediatrics. 2008;121:453–462. doi:10.1542/peds.2007-1173
11. Childhood and Adolescent Obesity. Available from: https://asmbs.org/patients/adolescent-obesity. Accessed March 2021.
12. Slater A, Tiggemann M. “Uncool to do sport”: a focus group study of adolescent girls’ reasons for withdrawing from physical activity. Psychol Sport Exerc. 2010;11:619–626. doi:10.1016/j.psychsport.2010.07.006
13. Hammersley ML, Okely AD, Batterham MJ, Jones RA. An internet-based childhood obesity prevention program (Time2bHealthy) for parents of preschool-aged children: randomized controlled trial. J Med Internet Res. 2019;21:e11964.
14. Li JS, Barnett TA, Goodman E, et al. Approaches to the prevention and management of childhood obesity: the role of social networks and the use of social media and related electronic technologies: a scientific statement from the American Heart Association. Circulation. 2013;127:260–267. doi:10.1161/CIR.0b013e3182756d8e
15. Schulz L, Spil AAMT, de Vries SAS. Changing behavior of kids with obesity with gamified wearables. In: Wickramasinghe N, Bodendorf F, editors. Delivering Superior Health and Wellness Management with IoT and Analytics. Springer Nature Switzerland AG. Springer International Publishing; 2020: 145–169.
16. Pretlow RA. Addiction to highly pleasurable food as a cause of the childhood obesity epidemic: a qualitative internet study. Eat Disord. 2011;19:295–307. doi:10.1080/10640266.2011.584803
17. Datta AK, Sumargo A, Jackson V, Dey PP. mCHOIS: an application of mobile technology for childhood obesity surveillance. Procedia Comput Sci. 2011;5:653–660. doi:10.1016/j.procs.2011.07.085
18. Daley AJ. Can exergaming contribute to improving physical activity levels and health outcomes in children? Pediatrics. 2009;124:763–771. doi:10.1542/peds.2008-2357
19. Radesky JS, Schumacher J, Zuckerman B. Mobile and interactive media use by young children: the good, the bad, and the unknown. Pediatrics. 2015;135:1–3. doi:10.1542/peds.2014-2251
20. Miller GF, Sliwa S, Michael S, et al. Evaluation of Let’s move! Active schools activation grants. Prev Med. 2018;108:36–40. doi:10.1016/j.ypmed.2017.12.024
21. Schuman AJ. Improving patient care: smartphones and mobile medical devices: mobile medical gadgetry is in its infancy, yet these devices can help you motivate pediatric patients and their parents to adopt healthier lifestyles. Contemp Pediatr. 2013;30:33–38.
22. Cruz JA, Wishart DS. Applications of machine learning in cancer prediction and prognosis. Cancer Inform. 2007;2:59–77.
23. Mirzaei G, Adeli A, Adeli H. Imaging and machine learning techniques for diagnosis of Alzheimer’s disease. Rev Neurosci. 2016;27:857–870. doi:10.1515/revneuro-2016-0029
24. Donsa K, Spat S, Beck P, et al. Towards personalization of diabetes therapy using computerized decision support and machine learning: some open problems and challenges. In: Holzinger A, Röcker C, Ziefle M, editors. Smart Health. Lecture Notes in Computer Science. Springer, Cham; 2015: 237–260.
25. Gultepe E, Green JP, Nguyen H, et al. From vital signs to clinical outcomes for patients with sepsis: a machine learning basis for a clinical decision support system. J Am Med Inform Assoc. 2014;21:315–325. doi:10.1136/amiajnl-2013-001815
26. Obermeyer Z, Emanuel EJ. Predicting the future - big data, machine learning, and clinical medicine. N Engl J Med. 2016;375:1216–1219. doi:10.1056/NEJMp1606181
27. Salvatore C, Cerasa A, Battista P, et al. Magnetic resonance imaging biomarkers for the early diagnosis of Alzheimer’s disease: a machine learning approach. Front Neurosci. 2015;9:307. doi:10.3389/fnins.2015.00307
28. Triantafyllidis A, Polychronidou E, Alexiadis A, et al. Computerized decision support and machine learning applications for the prevention and treatment of childhood obesity: a systematic review of the literature. Artif Intell Med. 2020;104:101844. doi:10.1016/j.artmed.2020.101844
29. Robinson NL, Connolly J, Hides L, Kavanagh DJ. Social robots as treatment agents: pilot randomized controlled trial to deliver a behavior change intervention. Internet Interv. 2020;21:100320. doi:10.1016/j.invent.2020.100320
30. Cappuccio ML, Sandoval EB, Mubin O, et al. Can robots make us better humans? Int J Soc Robotics. 2020;13:7–22. doi:10.1007/s12369-020-00700-6
31. Sandoval EB, Mubin O. Virtuous robotics: artificial agents and the good life. Int J Soc Robotics. 2021;4:54.
32. Chen JL, Wilkosz ME. Efficacy of technology-based interventions for obesity prevention in adolescents: a systematic review. Adolesc Health Med Ther. 2014;5:159–170. doi:10.2147/AHMT.S39969
33. McMullan M, Millar R, Woodside JV. A systematic review to assess the effectiveness of technology-based interventions to address obesity in children. BMC Pediatr. 2020;20:242. doi:10.1186/s12887-020-02081-1
34. Nouchi R, Kawashima R. Improving cognitive function from children to old age: a systematic review of recent smart ageing intervention studies. Adv Neurosci. 2014;2014:1–15. doi:10.1155/2014/235479
35. Lindberg R, Seo J, Laine TH. Enhancing physical education with exergames and wearable technology. IEEE Trans Learning Technol. 2016;9:328–341. doi:10.1109/TLT.2016.2556671
36. Yang HJ, Kang JH, Kim OH, et al. Interventions for preventing childhood obesity with smartphones and wearable device: a protocol for a non-randomized controlled trial. Int J Environ Res Public Health. 2017;14:184.
37. Argarini R, Herawati L, Irwadi I, et al. Fundamental movement skill approach to combat childhood obesity in Surabaya, Indonesia: potential effects of video games based ex ercises (Exergaming). J Talent Dev Excell. 2020;12:3026–3034.
38. Adamo KB, Rutherford JA, Goldfield GS. Effects of interactive video game cycling on overweight and obese adolescent health. Appl Physiol Nutr Metab. 2010;35:805–815. doi:10.1139/H10-078
39. Staiano AE, Beyl RA, Guan W, et al. Home‐based exergaming among children with overweight and obesity: a randomized clinical trial. Pediatr Obes. 2018;13:724–733. doi:10.1111/ijpo.12438
40. Ruggiero L, Seltzer ED, Dufelmeier D, et al. MyPlate picks: development and initial evaluation of feasibility, acceptability, and impact of an educational exergame to help promote healthy eating and physical activity in children. Games Health J. 2020;9:197–207. doi:10.1089/g4h.2019.0056
41. Trost SG, Sundal D, Foster GD, et al. Effects of a pediatric weight management program with and without active video games: a randomized trial. JAMA Pediatr. 2014;168:407–413. doi:10.1001/jamapediatrics.2013.3436
42. Staiano AE, Marker AM, Beyl RA, et al. A randomized controlled trial of dance exergaming for exercise training in overweight and obese adolescent girls. Pediatr Obes. 2017;12:120–128. doi:10.1111/ijpo.12117
43. Maddison R, Foley L, Ni Mhurchu C, et al. Effects of active video games on body composition: a randomized controlled trial. Am J Clin Nutr. 2011;94:156–163. doi:10.3945/ajcn.110.009142
44. Duman F, Kokaçya MH, Doğru E, et al. The role of active video-accompanied exercises in improvement of the obese state in children: a prospective study from Turkey. J Clin Res Pediatr Endocrinol. 2016;8:334–340. doi:10.4274/jcrpe.2284
45. Wagener TL, Fedele DA, Mignogna MR, et al. Psychological effects of dance‐based group exergaming in obese adolescents. Pediatr Obes. 2012;7:e68–e74. doi:10.1111/j.2047-6310.2012.00065.x
46. Coknaz D, Mirzeoglu AD, Atasoy HI, Alkoy S, Coknaz H, Goral K. A digital movement in the world of inactive children: favourable outcomes of playing active video games in a pilot randomized trial. Eur J Pediatr. 2019;178(10):1567–1576. doi:10.1007/s00431-019-03457-x
47. Gao Z, Lee JE, Zeng N, Pope ZC, Zhang Y, Li X. Home-based exergaming on preschoolers’ energy expenditure, cardiovascular fitness, body mass index and cognitive flexibility: a randomized controlled trial. J clin med. 2019;8(10):1745. doi:10.3390/jcm8101745
48. Espinosa-Curiel IE, Pozas-Bogarin EE, Lozano-Salas JL, et al. Nutritional education and promotion of healthy eating behaviors among Mexican children through video games: design and pilot test of FoodRateMaster. JMIR Serious Games. 2020;8:e16431. doi:10.2196/16431
49. Nawi AM, Jamaludin FIC. Effect of internet-based intervention on obesity among adolescents in Kuala Lumpur: a school-based cluster randomised trial. Malays J Med Sci MJMS. 2015;22:47–56.
50. Del Río NG, González-González CS, Martín-González R, et al. Effects of a gamified educational program in the nutrition of children with obesity. J Med Syst. 2019;43:198. doi:10.1007/s10916-019-1293-6
51. Chen JL, Guedes CM, Lung AE. Smartphone-based healthy weight management intervention for Chinese American adolescents: short-term efficacy and factors associated with decreased weight. J Adolesc Health. 2019;64:443–449. doi:10.1016/j.jadohealth.2018.08.022
52. Rerksuppaphol L, Rerksuppaphol S. Internet based obesity prevention program for Thai school children-a randomized control trial. JCDR. 2017;11(3):SC07. doi:10.7860/JCDR/2017/21423.9368
53. Nyström CD, Sandin S, Henriksson P, et al. Mobile-based intervention intended to stop obesity in preschool-aged children: the MINISTOP randomized controlled trial. Am J Clin Nutr. 2017;105:1327–1335.
54. Fiechtner L, Kleinman K, Melly SJ, et al. Effects of proximity to supermarkets on a randomized trial studying interventions for obesity. Am J Public Health. 2016;106:557–562. doi:10.2105/AJPH.2015.302986
55. Lingren T, Thaker V, Brady C, et al. Developing an algorithm to detect early childhood obesity in two tertiary pediatric medical centers. Appl Clin Inform. 2016;7:693–706. doi:10.4338/ACI-2016-01-RA-0015
56. Ríos-Julián N, Alarcón-Paredes A, Alonso GA, et al. Feasibility of a screening tool for obesity diagnosis in Mexican children from a vulnerable community of Me’Phaa ethnicity in the State of Guerrero, Mexico.
57. Fergus P, Hussain A, Hearty J, et al. A machine learning approach to measure and monitor physical activity in children to help fight overweight and obesity.
58. Dugan TM, Mukhopadhyay S, Carroll A, Downs S. Machine learning techniques for prediction of early childhood obesity. Appl Clin Inform. 2015;6:506. doi:10.4338/ACI-2015-03-RA-0036
59. Singh B, Tawfik H. Machine learning approach for the early prediction of the risk of overweight and obesity in young people.
60. Alotaibi M. A social robotic obesity management and awareness system for children in Saudi Arabia. Int J Online Eng. 2018;14(9):45.
61. Colmenarejo G. Machine learning models to predict childhood and adolescent obesity: a review. Nutrients. 2020;12:2466. doi:10.3390/nu12082466
62. Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol. 2009;28(6):690. doi:10.1037/a0016136
63. Alnajjar F, Cappuccio M, Renawi A, Mubin O, Loo CK. Personalized robot interventions for autistic children: an automated methodology for attention assessment. Int J Soc Robotics. 2021;13(1):67–82. doi:10.1007/s12369-020-00639-8
64. Vogan AA, Alnajjar F, Gochoo M, Khalid S. Robots, AI, and cognitive training in an era of mass age-related cognitive decline: a systematic review. IEEE Access. 2020;8:18284–18304. doi:10.1109/ACCESS.2020.2966819
65. Israels T, Challinor J, Howard S, Arora RH. Treating children with cancer worldwide—challenges and interventions. Pediatrics. 2015;136(4):607–610. doi:10.1542/peds.2015-0300
66. Wolpert, M., Curtis-Tyler, K., & Edbrooke-Childs, J. (2016). A qualitative exploration of patient and clinician views on patient-reported outcome measures in child mental health and diabetes services. Administration and Policy in Mental Health and Mental Health Services Research, 43(3), 309-315. Available from: https://www.betterhealth.vic.gov.au/health/ConditionsAndTreatments/diabetes-issues-for-children-and-teenagers#childrens-reactions-to-a-diabetes-diagnosis.
67. Dawe J, Sutherland C, Barco A, Broadbent E. Can social robots help children in healthcare contexts? A scoping review. BMJ Paediatr Open. 2019;3:e000371. doi:10.1136/bmjpo-2018-000371
68. Alahbabi M, Almazroei F, Almarzoqi M, et al. Avatar based interaction therapy: a potential therapeutic approach for children with Autism.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.