Back to Journals » Clinical Ophthalmology » Volume 20
Efficacy of Continuous Pegcetacoplan Treatment for Subfoveal Geographic Atrophy in Age-Related Macular Degeneration: 36-Month Results from OAKS, DERBY, and GALE Open-Label Extension
Authors Dhoot DS, Garg SJ, Brown DM, Suñer IJ ![]() , Rahimy E, Boyer DS, Naidu K, Li C, Baumal CR, Guymer RH
, Rahimy E, Boyer DS, Naidu K, Li C, Baumal CR, Guymer RH ![]()
Received 5 November 2025
Accepted for publication 8 April 2026
Published 14 May 2026 Volume 2026:20 579237
DOI https://doi.org/10.2147/OPTH.S579237
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Video abstract of “Pegcetacoplan Treatment for Subfoveal Geographic Atrophy” [579237].
Views: 46
Dilsher S Dhoot,1 Sunir J Garg,2 David M Brown,3 Ivan J Suñer,4 Ehsan Rahimy,5,6 David S Boyer,7 Kineta Naidu,8 Chao Li,8 Caroline R Baumal,8,9 Robyn H Guymer10,11
1California Retinal Consultants/Retina Consultants of America, Santa Barbara, CA, USA; 2The Retina Service of Wills Eye Hospital, Thomas Jefferson University, Philadelphia, PA, USA; 3Retina Consultants of Texas, Houston, TX, USA; 4Retina Associates of Florida, Tampa, FL, USA; 5Department of Ophthalmology, Byers Eye Institute, Horngren Family Vitreoretinal Center, Stanford University School of Medicine, Palo Alto, CA, USA; 6Department of Ophthalmology, Palo Alto Medical Foundation, Palo Alto, CA, USA; 7Retina Vitreous Associates Medical Group, Los Angeles, CA, USA; 8Apellis Pharmaceuticals, Waltham, MA, USA; 9Retina Specialists of Boston and Wellesley, Wellesley, MA, USA; 10University of Melbourne, Melbourne, VIC, Australia; 11Centre for Eye Research Australia, Royal Victorian Eye and Ear Hospital, Melbourne, VIC, Australia
Correspondence: Dilsher S Dhoot, California Retinal Consultants/Retina Consultants of America, 525 East Micheltorena St, Suite A, Santa Barbara, CA, 93103, USA, Tel +1 805 9631648, Email [email protected]
Purpose: To report efficacy of intravitreal pegcetacoplan treatment over 36 months in eyes with subfoveal geographic atrophy (GA).
Patients and Methods: The GALE (NCT04770545) open-label extension trial adds 12 months of results to the 24-month Phase 3 OAKS (NCT03525613) and DERBY (NCT03525600) trials, representing up to 36 months of continuous pegcetacoplan treatment. They included a heterogeneous population of eyes with subfoveal GA (63%). Pegcetacoplan-treated eyes enrolling in GALE continued at the same interval of pegcetacoplan monthly (PM) or every other month (PEOM). Patients’ eyes in sham monthly or every-other-month arms crossed over to receive pegcetacoplan in GALE at the same interval (sham crossover). Consequently, projected sham, calculated from prior 24-month GA growth rate of sham-observed eyes in OAKS and DERBY averaged across four 6-month segments, was the comparator for the first 12 months of GALE (months 24– 36). This analysis reports results of eyes with subfoveal GA at baseline.
Results: In eyes with subfoveal GA, 84% had best corrected visual acuity (BCVA) ≥ 20/200 and 38% had BCVA ≥ 20/63 at OAKS and DERBY baseline. Pegcetacoplan reduced subfoveal GA growth rate by 21% (p< 0.0001) with PM and 19% (p=0.0001) with PEOM over 36 months. Increasing efficacy over time was noted between months 24 and 36; 31% reduction in subfoveal GA growth rate with PM and 25% reduction with PEOM (both p< 0.0001) compared with projected sham. Microperimetry demonstrated significant reduction in formation of absolute scotomas with PM at 24 months (– 2.5 number of scotomas formed; 95% confidence interval [CI]: – 4.5, – 0.4; p=0.0205) and 36 months (– 4.0 number of scotomas formed; 95% CI: – 6.8, – 1.2; p=0.0050), compared to sham crossover in subfoveal GA. Safety profile in GALE was consistent with OAKS and DERBY.
Conclusion: Long-term efficacy of pegcetacoplan in slowing GA progression was demonstrated over 36 months in eyes with subfoveal GA.
Plain Language Summary: Why was this study done?
Geographic atrophy (GA) is a progressive, permanent retinal degenerative disease that can lead to vision loss in patients over 60 years of age. This analysis was done to look at how pegcetacoplan, a treatment for GA, could help people with GA once it affected the center of their vision, called subfoveal GA. People with subfoveal GA are at risk of losing more of their central vision, which is important for reading, driving, and recognizing faces.
What did the researchers do and find?
Researchers looked at data from the GALE clinical trial, which followed people with GA for 3 years to see how well pegcetacoplan worked. They studied whether pegcetacoplan slowed down the growth of subfoveal GA and whether it helped lower the risk of forming new blind spots.
People with subfoveal GA retained some vision that could be protected. In fact, 84% of them had mild or moderate visual impairment at baseline. Researchers found that pegcetacoplan slowed the growth of subfoveal GA over 3 years, whether it was given every month or every other month. They also found that pegcetacoplan may have lowered the risk of forming new blind spots in the eye.
What do these results mean?
Pegcetacoplan treatment helped for people with subfoveal GA. Treating subfoveal GA is important because it can help people save the vision they still have and slow down further vision loss.
Keywords: pegcetacoplan, complement C3 inhibition, microperimetry, retinal degeneration, clinical trial
Introduction
Geographic atrophy (GA) is a late stage of age-related macular degeneration (AMD) characterized by irreversible outer retinal degeneration and is a major cause of significant vision impairment.1–4 Initially, foci of GA are typically located in the perifoveal retina. However, as GA progresses, atrophic GA lesions can grow to affect the fovea, leading to irreversible loss of central vision.5,6 Preserving central vision is crucial, as it is essential for performing everyday tasks such as reading, driving, and recognizing faces.7,8
The rate of GA lesion growth is influenced by a number of factors, including the location of GA in the retina.5,6 Nonsubfoveal GA, defined as lesions that do not involve the center point of the fovea, grows at a faster rate than subfoveal GA, defined as lesions that involve the center point of the fovea.5,6,9 Regardless of this difference in growth rate, eyes with subfoveal GA have poorer visual acuity compared with those with nonsubfoveal GA, and treatment with pegcetacoplan in subfoveal GA may preserve the functional vision that remains.10,11 A retrospective analysis of the IRIS Registry data found that eyes with nonsubfoveal GA had better mean visual acuity at baseline (mean, 20/50) than those with subfoveal GA (mean, 20/63); however, nearly half of those with subfoveal GA had visual acuity of 20/40 or greater at baseline and only 13% of those with subfoveal GA had visual acuity worse than 20/200.12 In addition, the average decline in visual acuity was similar for eyes with nonsubfoveal GA and eyes with subfoveal GA.12 These data highlight the potential of treatment to preserve functional vision in eyes whose GA has progressed to involve the fovea.
In natural history studies of GA, a discordance between lesion growth and changes in visual acuity has been noted, and is in large part due to factors such as lesion location and the heterogeneous nature of lesion growth.1,7,13–15 One functional method that is more robust at linking structure to function in retinal disease is microperimetry. Microperimetry links macular structure to function by assessing retinal sensitivity at specific macular loci, similar to a peripheral visual field test but for macular sensitivity.15–19 This methodology can be used to track visual function decline over time and patterns of GA progression, so it has been proposed as a way to measure functional outcomes in clinical trials for GA.20 In the CHROMA and SPECTRI trials, microperimetry showed the highest correlation of visual function with GA area compared with other measures of visual acuity, including best-corrected visual acuity (BCVA) and low-luminance visual acuity, which showed weak correlations with GA area.1
To preserve as much retinal tissue and vision as possible in as many patients as possible, it is crucial to understand the effectiveness of GA therapies in eyes with different GA phenotypes. The phase 3 OAKS (NCT03525613) and DERBY (NCT03525600) trials, which demonstrated the efficacy and safety of pegcetacoplan treatment for GA, included eyes with both subfoveal and nonsubfoveal GA.21 In contrast, eyes with subfoveal GA were not included in the GATHER 1 or GATHER 2 studies, and while the lampalizumab studies included eyes with subfoveal GA, they did not meet their primary efficacy outcomes.22,23 In the OAKS and DERBY trials, of the 1211 patient eyes in the modified intent-to-treat population in the two trials combined, 63% of eyes had subfoveal GA.21 These trials demonstrated that treatment with pegcetacoplan monthly (PM) or every other month (PEOM) reduced GA growth by 21% and 17%, respectively over 24 months compared with sham observed in the entire cohort, which included both subfoveal and nonsubfoveal GA eyes. In eyes with subfoveal GA, treatment with PM or PEOM reduced GA growth by 19% and 16%, respectively, over 24 months compared with sham.21 The efficacy of pegcetacoplan in these trials emphasizes a potential benefit of pegcetacoplan treatment in eyes with subfoveal GA meeting the study inclusion criteria, as this subgroup made up a majority of participants. GALE (NCT04770545), an ongoing 3-year open-label extension trial, is continuing to evaluate the long-term efficacy of pegcetacoplan in this heterogeneous population. The high proportion of eyes with subfoveal GA in these trials presents an opportunity to examine the anatomic and functional benefits of pegcetacoplan in this important subgroup. The objective of this subgroup analysis was to explore the effect of pegcetacoplan treatment through the first 12 months of GALE, representing up to 36 months of continuous treatment, in eyes with subfoveal GA.
Materials and Methods
Study Design
GALE is a 3-year open-label extension phase 3 trial following the 2-year pivotal OAKS and DERBY trials, providing a total of 5 years of continuous pegcetacoplan treatment. The GALE study design and methodology have been described previously.24 Briefly, GALE was designed to evaluate the long-term efficacy and safety of pegcetacoplan. Patients from the phase 3 OAKS and DERBY studies or the phase 1b APL2-103 study (NCT03777332) were eligible to participate in GALE. Eighty-three percent of patients who completed OAKS and DERBY elected to continue in GALE, and 92% of patients who enrolled in GALE completed the first 12 months of treatment, which are reported in the present study. In GALE, treatment was administered PM or PEOM in all study eyes. Specifically, eyes treated with pegcetacoplan in OAKS, DERBY, or the phase 1b APL2-103 study continued the same regimen in GALE (PM-PM and PEOM-PEOM), and eyes previously receiving sham monthly (SM) or sham every other month (SEOM) in the antecedent studies crossed over to pegcetacoplan at the same dosing interval in GALE (SM-PM and SEOM-PEOM). The eyes who crossed over to active treatment constituted the sham crossover group.
Participants
After completing either the 24-month phase 3 OAKS and DERBY trials or the phase 1b study (APL2-103; NCT03777332), patients with GA were eligible to enroll in GALE.11 In the OAKS and DERBY studies, patients were included if they were at least 60 years of age and had GA secondary to age-related macular degeneration; eyes could have subfoveal or nonsubfoveal GA.21 Patients were excluded if they had GA secondary to a condition other than age-related macular degeneration or a history of choroidal neovascularization in the study eye.21 Additional inclusion and exclusion criteria are detailed in a previous publication.21
GA Location
As was done in the antecedent OAKS and DERBY trials, optical coherence tomography and fundus autofluorescence were used to identify subfoveal GA, defined as involving the center point of the fovea (ie, distance of 0 microns from the foveal center to the nearest GA area border).21,25 Lesions not involving the foveal center were classified as nonsubfoveal.21,25 GA lesion size was evaluated via fundus autofluorescence (FAF). FAF images were graded by a central reading center by a minimum of two certified readers.
Outcomes
A key efficacy endpoint assessed in GALE was change in total area of GA in the study eye based on FAF. Key secondary endpoints in GALE included change in mean aggregate retinal sensitivity and the development of scotomas as assessed by microperimetry in OAKS participants who continued in GALE.21 The microperimetry endpoints evaluated in OAKS and GALE have been previously described.11 Briefly, microperimetry was conducted using the Macular Integrity Assessment confocal microperimeter (Macular Integrity Assessment SLO Microperimeter, Centervue, SpA, Padova, Italy) under mesopic testing conditions.26 Microperimetry testing was performed using a 10–2 grid (68 testing points, 2-degree spacing, 20-degree macular coverage) centered on the anatomic fovea using a 4–2 staircase strategy.26 As sensitivity deficits in the central macula are expected to have the most impact on central vision, the microperimetry analyses focused on the central 4 and central 16 macular points of the microperimetry grid (Figure 1). While the macular center is closely approximated by the 4 central macular points, the 16 central macular points have also demonstrated decreased sensitivity in macular disease and correlated with visual acuity.26,27
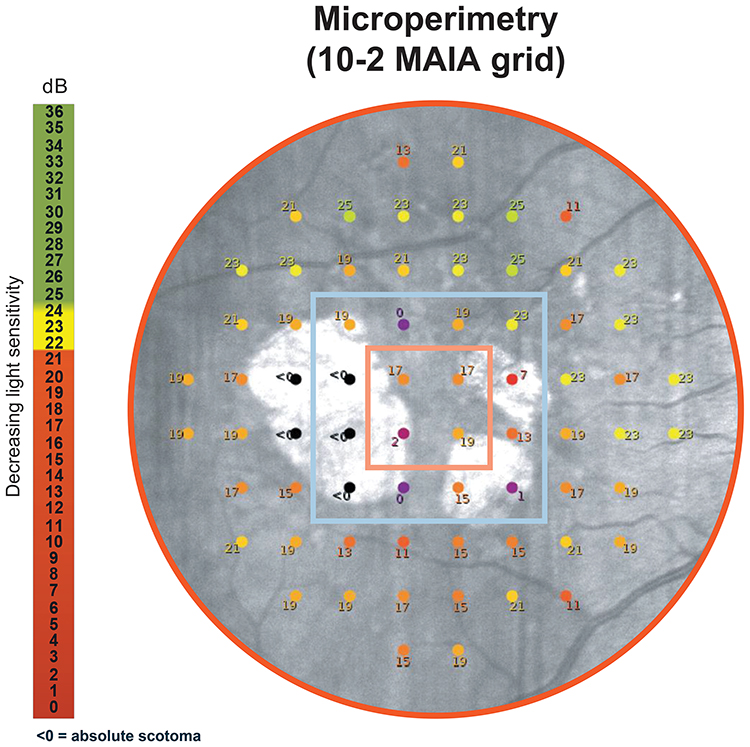 |
Figure 1 Microperimetry grid with the central 4 and 16 macular points evaluated in OAKS and GALE. The orange square denotes the central 4 macular points; the blue square denotes the central 16 macular points. Abbreviation: MAIA, Macular Integrity Assessment. |
Statistical Analysis
Efficacy outcomes were assessed using the modified full analysis set, which included patients who received at least one injection of pegcetacoplan in GALE and were in the intention-to-treat set in OAKS and DERBY. Participants from the phase 1b APL2-103 study were not included in the modified full analysis set but were included in the GALE safety set. Change in GA lesion size was assessed in the modified full analysis set, which was defined as patients with subfoveal GA lesions who received at least one pegcetacoplan injection during GALE and who were in the intention-to-treat dataset in OAKS and DERBY. The mean rate of change in GA area was calculated using a piecewise linear slope model and has been described previously.11 Because all eyes in GALE received active pegcetacoplan treatment, a projected sham comparator was used for the first 12 months of GALE (months 24–36) in this analysis while pooled sham was used for comparisons involving months 0–24. This projection was based on the average GA growth rate over four 6-month intervals from sham-treated eyes in the OAKS and DERBY trials, consistent with the documented linear growth rate pattern of GA.11,13,28,29 This method relies on natural history data and evidence that GA growth rates over a 2-year period are predictive of future growth and that GA growth follows a linear trend over time.11,30 Moreover, in the overall GALE population, the validity of projected sham was confirmed via comparisons of the GA growth rates in untreated fellow eyes (months 0–36), sham-observed eyes (months 0–24), and projected sham (months 24–36).11,31 Microperimetry analyses of the number of scotomatous points in the study eye were conducted in eyes from OAKS that were part of the GALE modified intent-to-treat set, and comparisons were made between pegcetacoplan-treated eyes and sham/crossover, defined as the sham pooled group (months 0–24) and the sham crossover group (months 24–36). The microperimetry analyses of the central 4 and central 16 macular points of the microperimetry grid were performed with data from the modified intent-to-treat population from OAKS, and comparisons were made between pegcetacoplan-treated eyes and the pooled sham group. All statistical analyses were performed using SAS, version 9.4.
Results
Patient Characteristics
Of the 792 eyes of patients enrolled in GALE, 780 eyes (all from OAKS and DERBY) were included in the modified full analysis set, and 790 eyes (780 from OAKS and DERBY; 10 from phase 1b APL2-103) were included in the safety analysis set. Among these patients, 63% (494/780) of eyes had subfoveal GA at the OAKS and DERBY baseline and 73% (567/780) had subfoveal GA at GALE study baseline. The antecedent study baseline patient demographics and clinical characteristics of the overall study population in GALE were consistent with the OAKS and DERBY antecedent study populations, which have been reported previously,21,24 and are reported for subfoveal GA eyes who continued into GALE across treatment groups in Table 1. Among subfoveal GA eyes, 84% had BCVA of at least 35 Early Treatment Diabetic Retinopathy Study (ETDRS) letters, or ≥20/200, at OAKS and DERBY baseline. At the same timepoint, 38% had normal luminance BCVA of at least 60 ETDRS letters (≥20/63) (Figure 2).
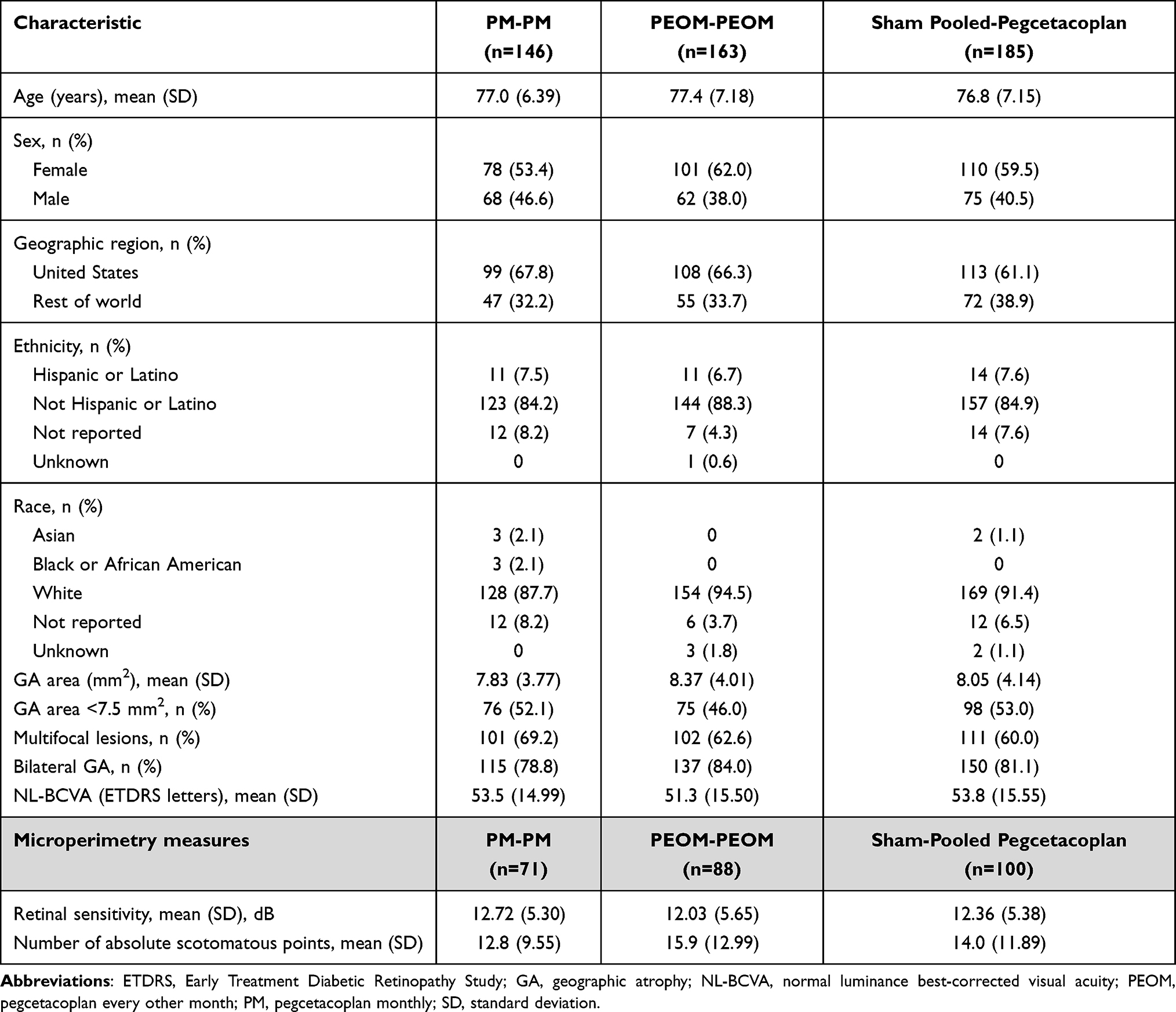 |
Table 1 Demographics and Study Eye Characteristics of Patients in GALE Who Had Subfoveal GA at OAKS or DERBY Baseline. Values Shown Correspond to Those Observed at OAKS and DERBY Baseline |
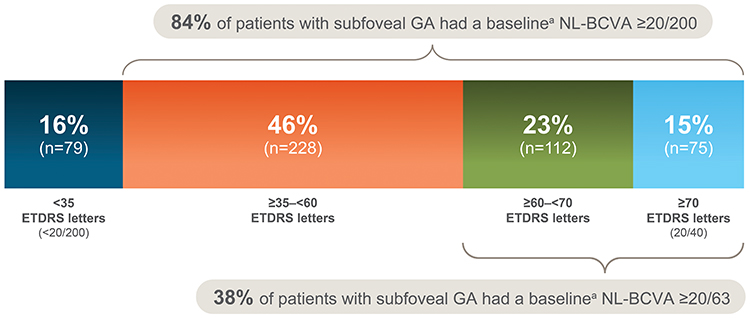 |
Figure 2 OAKS and DERBY baseline NL-BCVA in eyes with subfoveal GA (N=494). aAt baseline of the OAKS and DERBY studies. Abbreviations: NL-BCVA, normal luminance best-corrected visual acuity; ETDRS, Early Treatment Diabetic Retinopathy Study; GA, geographic atrophy. |
The safety of pegcetacoplan treatment over 36 months has been reported previously. The safety profile in the first 12 months of GALE was consistent with findings from the OAKS and DERBY trials.11
Efficacy Over 36 Months Among Eyes with Subfoveal GA
Among the subgroup of 494 participants who had subfoveal GA at OAKS and DERBY baseline, the percent reductions in GA growth rate compared with projected sham for months 0‒36 were 21% (p<0.0001) for PM-PM and 19% (p=0.0001) for PEOM-PEOM (Figure 3). Reductions in the mean rate of change in the first 12 months of GALE (months 24–36) were 31% (p<0.0001) for PM-PM and 25% (p<0.0001) for PEOM-PEOM compared with projected sham.
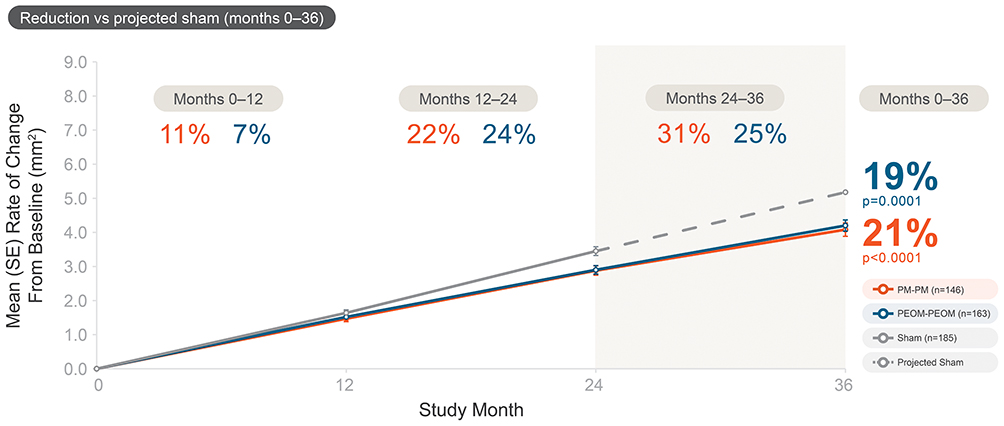 |
Figure 3 Mean rate of change in GA area growth over 36 monthsa in eyes with subfoveal GA. aMean rate of change in GA area between the pegcetacoplan treated eyes and sham-observed eyes from OAKS and DERBY antecedent study baseline to month 36, with knots at months 12 and 24 allowing for the slope to be linear over each of the 12-month segments but to differ between segments using piecewise slope analysis. Mean rate of change of projected sham from month 24 to month 36 was estimated from the mean rate of change in each 6-month period from month 0 to month 24 in the sham group. The modified full analysis set was used for the analysis, defined as eyes who were in the OAKS or DERBY antecedent study’s intent-to-treat set, had not been enrolled in the phase 1b APL2-103 study, and received ≥1 injection of pegcetacoplan in GALE. Projected sham is represented with a dashed line. The numbers shown with triangles between each time point represent the reduction in the mean rate of change in GA area compared with sham pooled (up to 24 months) and projected sham (months 24–36). The gray box denotes the time period for which projected sham was used. Adapted with permission from Wykoff CC et al. OAKS, DERBY, and GALE Investigators. Pegcetacoplan Treatment for Geographic Atrophy in Age-Related Macular Degeneration Over 36 Months: Data From OAKS, DERBY, and GALE. Am J Ophthalmol. 2025 Aug;276:350–364. Abbreviations: GA, geographic atrophy; PEOM, pegcetacoplan every other month; PM, pegcetacoplan monthly. |
Visual Function Over 36 Months Among Eyes with Subfoveal GA
In GALE, microperimetry was only performed in eyes from the OAKS trial, as patients in DERBY did not undergo microperimetry, as noted above. This included 116 eyes with subfoveal GA at the baseline of OAKS in the PM-PM group, 131 in the PEOM-PEOM group, and 147 in the sham crossover group.
Among this subgroup of eyes, a 24% reduction in the formation of absolute scotomas with PM compared with pooled sham at 24 months was observed as a functional microperimetry endpoint (−2.5 number of scotomas formed; 95% confidence interval [CI]: −4.5, −0.4; p=0.0205) and a 26% reduction was observed at 36 months (−4.0 number of scotomas formed; 95% CI: −6.8, −1.2; p=0.0050) compared with eyes in the sham crossover group with subfoveal GA. Similarly, PEOM demonstrated a 22% reduction in the formation of absolute scotomas at 24 months compared with pooled sham (−2.3 number of scotomas formed; 95% CI: −4.4, −0.01; p=0.0368) and a 14% reduction at 36 months (−2.1 number of scotomas formed; 95% CI: −5.2, 1.0; p=0.1876) compared with sham crossover among those with subfoveal GA (Figure 4).
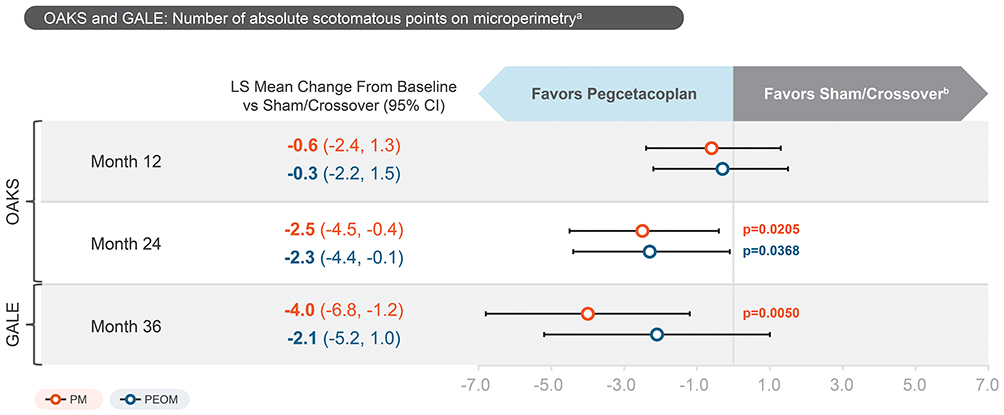 |
Figure 4 LS mean change in number of scotomatous points on microperimetry in eyes with subfoveal GA who continued into GALE from OAKS. Antecedent study baseline is defined as the OAKS baseline value. Model includes treatment, antecedent study baseline GA lesion area (<7.5 mm2 or ≥7.5 mm2), antecedent study baseline scotomatous points, analysis visit, antecedent study baseline presence of exudative AMD in the fellow eye (yes/no), analysis visit x treatment, antecedent study baseline scotomatous points x analysis visit. Data after integrated month 24 for eyes of patients who initially enrolled in OAKS, DERBY, and later enrolled in the phase 1b study were excluded from this analysis. Data through integrated month 36 consisted of all data collected through the analysis visit windowed integrated month 36 visit based on antecedent study baseline in the integrated month 36 dataset. The sham/crossover comparator corresponds to the sham pooled group (months 0–24) and sham crossover group (months 24–36). Abbreviations: AMD, age-related macular degeneration; CI, confidence interval; EOM, every other month; GA, geographic atrophy; LS, least-squares. |
Among subfoveal GA eyes from OAKS baseline, pegcetacoplan treatment reduced the risk of progression to absolute scotoma in the central 4 macular points by 32% (hazard ratio [HR]=0.68, p=0.0968) with PM and 29% (HR=0.71, p=0.1186) with PEOM during the 24 months of OAKS compared with pooled sham (Figure 5A). PEOM significantly reduced the risk of progression to absolute scotoma in the central 16 macular points by 54% (HR=0.46, p=0.0133) over 24 months compared with pooled sham. PM demonstrated a trend of risk reduction to absolute scotoma in the central 16 macular points (43% reduction; HR=0.57, p=0.1054) (Figure 5B).
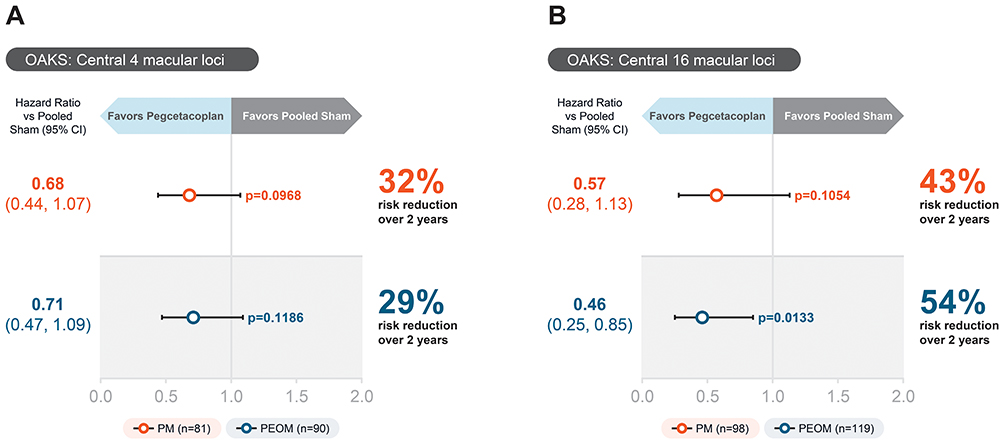 |
Figure 5 Development of central absolute scotoma among eyes with subfoveal GA in OAKS. Reduction in the development of absolute scotoma in the (A) central 4 macular points and (B) central 16 macular points over 24 months in eyes with subfoveal GA compared with pooled sham. Antecedent study baseline is defined as the OAKS baseline value. Model includes treatment, antecedent study baseline GA lesion area (<7.5 mm2 or ≥7.5 mm2), antecedent study baseline presence of exudative AMD in the fellow eye (yes/no), antecedent study baseline number of scotomatous points. Abbreviations: AMD, age-related macular degeneration; CI, confidence interval; EOM, every other month; GA, geographic atrophy. |
Discussion
The anatomic and functional benefits of pegcetacoplan in GA in a highly heterogeneous population of eyes with either nonsubfoveal or subfoveal GA have previously been reported.21 In this subgroup analysis, 36 consecutive months of pegcetacoplan treatment led to reductions in GA growth rate in eyes with subfoveal GA, including a 21% reduction with PM administration and a 19% reduction with PEOM administration over the course of the study compared with crossover sham (p<0.001 and p=0.001, respectively). Pegcetacoplan treatment demonstrated increasing efficacy over time in eyes with subfoveal GA, with reductions in GA growth rate of 31% with PM and 25% with PEOM (both p<0.0001) compared with projected sham in months 24‒36. In addition to these anatomic benefits, pegcetacoplan treatment also demonstrated functional benefit in a microperimetry analysis in subfoveal GA eyes, with significant reductions at 36 months in the overall formation of absolute scotomas with PM (26% reduction compared with sham crossover; p=0.0050), while PEOM did not reach statistical significance. There was also a trend showing reductions in the formation of absolute scotomas in the central 4 and 16 macular points, reaching significance with PEOM in the central 16 points (54% reduction compared with pooled sham; p=0.0133) at 24 months. This is clinically noteworthy, as a higher number of scotomas in the central macular region has been associated with poorer visual function, including BCVA.26
In this trial, 84% of eyes with subfoveal GA had mild to moderate visual impairment at baseline. In some cases of GA, eyes with moderate visual acuity, even with some involvement of the central macula, are at highest risk for further visual loss.32 In these eyes, reductions in lesion growth rate should potentially slow vision loss.32 If left untreated, visual acuity declines rapidly, particularly within the first 3 years, with patients losing an average of more than 15 ETDRS letters during this period.33 The results of this trial confirm that long-term pegcetacoplan treatment provides anatomic benefit and may contribute to maintaining visual function while slowing GA progression in eyes with subfoveal GA.
Limitations
Limitations of this analysis include those typical of open-label trials, such as selection bias and the lack of a control group. In addition, it may introduce performance bias among participants or investigators and possible assessment bias. At the onset of GALE, sham observed eyes were switched to active pegcetacoplan treatment and as a result, a projected sham comparator was utilized in this analysis. The use of this projected sham comparator is supported by findings in the OAKS and DERBY studies showing that the annual GA growth rate was linear at a rate of 2 mm2 among sham-treated eyes over the study duration. This aligns well with the projected sham growth rate utilized in this analysis, and is further validated by the observation that the GA growth trajectory in untreated fellow eyes was found to be linear over the 36 months of OAKS, DERBY, and GALE.11,21 While pegcetacoplan demonstrated increasing reductions in GA growth rates over 36 months, this pattern may reflect a regression to the mean or a boundary/ceiling effect and may warrant further exploration.
Conclusion
Over 36 months, long-term treatment with pegcetacoplan slowed the progression of GA with as few as 6 injections per year in this open-label subgroup analysis utilizing a projected comparator. Addressing subfoveal GA is essential, as a majority of eyes in this study had preservable visual acuity.
Abbreviations
BCVA, best-corrected visual acuity; ETDRS, Early Treatment Diabetic Retinopathy Study; GA, geographic atrophy; HR, hazard ratio; PEOM, pegcetacoplan every other month; PM, pegcetacoplan monthly; SEOM, sham every other month; SM, sham monthly.
Data Sharing Statement
The data reported in this article are available from the sponsor upon reasonable request. Individual participant data will not be made available. Requests for access to data from the OAKS, DERBY, and GALE trials should be addressed to [email protected]. The study protocol will be available with no end date. All proposals requesting data access will need to specify how the data will be used, and all proposals will need the approval of the trial investigator team before data release.
Ethics Approval and Informed Consent
This study adheres to the tenets of the Declaration of Helsinki. Institutional Review Board/Ethics Committee approval was obtained at each study site before study initiation. Study sites are listed in the supplementary materials for Wykoff CC, et al, Am J Ophthalmol 2025;276:350-364. Informed consent was obtained from all patients before enrollment.
Consent for Publication
The Authors hereby grant the publisher permission to publish this work. The Authors confirm that they have been shown the article contents prior to publication.
Acknowledgments
Professional medical writing support was provided by Charlotte Mitchell, PhD, and Elizabeth McSpiritt, MD, MPH, of Peloton Advantage, an OPEN Health company, and was funded by Apellis Pharmaceuticals.
Author Contributions
All authors made significant contributions to the work reported, including its conception, study design, execution, data acquisition, analysis, and interpretation. They also participated in drafting, revising, or critically reviewing the article, approved the final version for publication, agreed on the journal to which the article was submitted, and agreed to be accountable for all its aspects.
Funding
This study was funded by Apellis Pharmaceuticals.
Disclosure
DSD: Consultant: 4DMT, AbbVie, Adverum, Alcon, Alimera Sciences, Allergan, Alkeus, Annexin, Annexon, Apellis, Bausch and Lomb, Bayer, BioCryst, Coherus, EyePoint, Genentech, Iveric Bio/Astellas, Nanoscope, Neurotech, Novartis, Ocular Therapeutix, Oculis, Optos, Outlook Therapeutics, Oxular, Regeneron, RegenXBio, Retina-AI, Roche, Samsara, Sanofi, and Santen; Honoraria/speakers bureau: Alimera, ANI Pharmaceuticals, Apellis, Genentech, Regeneron, and Sandoz; Advisory board: Annexin, Apellis, Genentech/Roche, Ocular Therapeutix, and Oculis; Stockholder: Outlook Therapeutics, Revopsis, Vortex Surgical. SJG: Consultant: Allergan/AbbVie, American Academy of Ophthalmology, Apellis, Archimedic, Bausch & Lomb, Boehringer Ingelheim, Genentech/Hoffman LaRoche, Merck Manual, Regeneron, West Pharmaceuticals, and Zeiss; Contracted research: Alcon, American Academy of Ophthalmology, Apellis, Boehringer Ingelheim, Complement Therapeutics, Genentech/Hoffman LaRoche, Regeneron, and Sanofi. DMB: Consulting fees/honoraria for ongoing services: AAVantgarde Bio, AbbVie, Alexion, Apellis, Bayer, Biogen MA, Boehringer Ingelheim, Celltrion, Chengdu Kanghong, Clearside Biomedical, Heidelberg Engineering, Impact Education, Kowa, Medscape, Novartis, Ocular Therapeutix, Ocuphire Pharma, OPTOS, Pontifax, Regeneron, RetinAI Medical, Ray Therapeutics, RMEI, Senju, SIMR Biotech, Stealth BioTherapeutics, THEA, Topcon, WebMD Global, Xequel Bio, and Xfacto; Grants paid to institution for ongoing research support as a principal investigator: AffaMed Therapeutics, Alcon, Alexion, Allergan; Amgen, Annexon, Apellis, Astellas, Bayer, BIRC, Boehringer Ingelheim, Chengdu Kanghong Biotechnology, Clearside, Eyebiotech, EyePoint, Hoffmann-La Roche, Gemini Therapeutics, Genentech, Graybug Vision, Gyroscope Therapeutics, Heidelberg Engineering, and i-Lumen Scientific, IONIS, Jaeb-/DRCR, Jeff Heier, MD, Kodiak Sciences, LumiThera, MeiraGTx, Mylan, NEI/NIH, NGM Biopharmaceuticals, Novartis, Ocular Therapeutix, Ocuphire Pharma, OcuTerra Therapeutics, Opthea, OPTOS, Outlook Therapeutics, OXULAR, Pennsylvania State University, Regeneron, RegenXBio, Rezolute, SamChunDang Pharm, Samsung, Sandoz Biopharmaceuticals, Santen, SciFluor Life Sciences, Senju, Shanghai Henlius Biotech, Stealth BioTherapeutics, Taiwan Liposome Company, Thrombogenics, Xbrane, and Zeiss Meditec; Patient beneficiary: OPTOS- Camera Software (used to dewarp images); Stock options: Adverum, Clearside Biomedical, and Ocuphire Pharma. IJS: Advisory board: Alimera, Apellis, and Genentech/Roche; Consultant: Apellis, Allergan, Eclipse BioScience, Eyepoint, Genentech, IvericBio, Ocular Therapeutics, and Regeneron; Investigator: Alimera, Apellis, Aura Bioscience, Eclipse BioScience, Eyepoint, Genentech, Ocular Therapeutics, and Regeneron. ER: Consulting fees: AbbVie, Apellis, Genentech, Google, Iveric, Regeneron, and Zeiss; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events: AbbVie, Apellis, Genentech, and Regeneron; Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: Advisor for Sanro Health. DSB: Consultant: 4DMT, Acucela, Adverum, Aerpio, AiVia, Alcon, Alkahest, Allegro, Allergan, Alkahest, Allgenesis, Allegro, Amgen, Amydis, Annexon, Apellis, Asclepix, Aviceda, Bausch&Lomb, Bayer, BioMotiv, Chengdu Kanghong, Clearside, EyePoint, Genentech, Glaukos, InflammX, Iveric Bio/Astellas, jCyte, Kala, Kodiak, Lumithera, Nanoscope, Novartis, Ocugenix, Ocular Therapeutics, Oculis, ONL Therapeutics, Opthea, Oxurion, Perfuse, Perceive, Ray, Recens Medical, Regeneron, RegenXBio, Sanofi, Stealth, Sun, Thea, and Unity; Stockholder: InflammX and Oculis. KN and CL: Employees: Apellis. CRB: Employee and stockholder: Apellis. RHG: Advisory boards: AbbVie, Apellis, Astellas, Bayer, Belite Bio, Boehringer Ingelheim, Character Biosciences, Complement Therapeutics, Janssen, Novartis, Ocular Therapeutix, and Roche/Genentech. The authors report no other conflicts of interest in this work.
References
1. Heier JS, Pieramici D, Chakravarthy U, et al. Visual function decline resulting from geographic atrophy: results from the Chroma and Spectri phase 3 trials. Ophthalmol Retina. 2020;4(7):673–11. doi:10.1016/j.oret.2020.01.019
2. Holz FG, Strauss EC, Schmitz-Valckenberg S, van Lookeren Campagne M. Geographic atrophy: clinical features and potential therapeutic approaches. Ophthalmology. 2014;121(5):1079–1091. doi:10.1016/j.ophtha.2013.11.023
3. Boyer DS, Schmidt-Erfurth U, van Lookeren Campagne M, Henry EC, Brittain C. The pathophysiology of geographic atrophy secondary to age-related macular degeneration and the complement pathway as a therapeutic target. Retina. 2017;37(5):819–835. doi:10.1097/IAE.0000000000001392
4. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–e116. doi:10.1016/S2214-109X(13)70145-1
5. Shen LL, Sun M, Khetpal S, Grossetta Nardini HK, Del Priore LV. Topographic variation of the growth rate of geographic atrophy in nonexudative age-related macular degeneration: a systematic review and meta-analysis. Invest Ophthalmol Vis Sci. 2020;61(1):2. doi:10.1167/iovs.61.1.2
6. Fleckenstein M, Mitchell P, Freund KB, et al. The progression of geographic atrophy secondary to age-related macular degeneration. Ophthalmology. 2018;125(3):369–390. doi:10.1016/j.ophtha.2017.08.038
7. Bakri SJ, Bektas M, Sharp D, Luo R, Sarda SP, Khan S. Geographic atrophy: mechanism of disease, pathophysiology, and role of the complement system. J Manag Care Spec Pharm. 2023;29(5–a Suppl):S2–S11. doi:10.18553/jmcp.2023.29.5-a.s2
8. Gao Y. Analyzing the science of visual acuity and its role in eye health. J Clin Ophthalmol. 2024;8(6):493.
9. Lindner M, Böker A, Mauschitz MM, et al. Directional kinetics of geographic atrophy progression in age-related macular degeneration with foveal sparing. Ophthalmology. 2015;122(7):1356–1365. doi:10.1016/j.ophtha.2015.03.027
10. Colijn JM, Liefers B, Joachim N, et al. Enlargement of geographic atrophy from first diagnosis to end of life. JAMA Ophthalmol. 2021;139(7):743–750. doi:10.1001/jamaophthalmol.2021.1407
11. Wykoff CC, Holz FG, Chiang A, et al. Pegcetacoplan treatment for geographic atrophy in age-related macular degeneration over 36 months: data from OAKS, DERBY, and GALE. Am J Ophthalmol. 2025;276:350–364.
12. Rahimy E, Khan MA, Ho AC, et al. Progression of geographic atrophy: retrospective analysis of patients from the IRIS® registry (Intelligent Research in Sight). Ophthalmol Sci. 2023;3(4):100318. doi:10.1016/j.xops.2023.100318
13. Holz FG, Sadda SR, Busbee B, et al. Efficacy and safety of lampalizumab for geographic atrophy due to age-related macular degeneration: chroma and Spectri phase 3 randomized clinical trials. JAMA Ophthalmol. 2018;136(6):666–677. doi:10.1001/jamaophthalmol.2018.1544
14. Holekamp N, Wykoff CC, Schmitz-Valckenberg S, et al. Natural history of geographic atrophy secondary to age-related macular degeneration: results from the prospective Proxima A and B clinical trials. Ophthalmology. 2020;127(6):769–783. doi:10.1016/j.ophtha.2019.12.009
15. Chang DS, Callaway NF, Steffen V, et al. Macular sensitivity endpoints in geographic atrophy: exploratory analysis of Chroma and Spectri clinical trials. Ophthalmol Sci. 2023;4(1):100351. doi:10.1016/j.xops.2023.100351
16. Hanout M, Horan N, Do DV. Introduction to microperimetry and its use in analysis of geographic atrophy in age-related macular degeneration. Curr Opin Ophthalmol. 2015;26(3):149–156. doi:10.1097/ICU.0000000000000153
17. Csaky KG, Patel PJ, Sepah YJ, et al. Microperimetry for geographic atrophy secondary to age-related macular degeneration. Surv Ophthalmol. 2019;64(3):353–364. doi:10.1016/j.survophthal.2019.01.014
18. Yang Y, Dunbar H. Clinical perspectives and trends: microperimetry as a trial endpoint in retinal disease. Ophthalmologica. 2021;244(5):418–450. doi:10.1159/000515148
19. Wu Z, Hodgson LAB, Guymer RH. Targeted high-density microperimetry testing of nascent geographic atrophy in age-related macular degeneration. Ophthalmol Sci. 2023;4(2):100419. doi:10.1016/j.xops.2023.100419
20. Meleth AD, Mettu P, Agrón E, et al. Changes in retinal sensitivity in geographic atrophy progression as measured by microperimetry. Invest Ophthalmol Vis Sci. 2011;52(2):1119–1126. doi:10.1167/iovs.10-6075
21. Heier JS, Lad EM, Holz FG, et al. Pegcetacoplan for the treatment of geographic atrophy secondary to age-related macular degeneration (OAKS and DERBY): two multicentre, randomised, double-masked, sham-controlled, phase 3 trials. Lancet. 2023;402(10411):1434–1448. doi:10.1016/S0140-6736(23)01520-9
22. Jaffe GJ, Westby K, Csaky KG, et al. C5 inhibitor avacincaptad pegol for geographic atrophy due to age-related macular degeneration: a randomized pivotal Phase 2/3 trial. Ophthalmology. 2021;128(4):576–586. doi:10.1016/j.ophtha.2020.08.027
23. Khanani AM, Patel SS, Staurenghi G, et al. Efficacy and safety of avacincaptad pegol in patients with geographic atrophy (GATHER2): 12-month results from a randomised, double-masked, phase 3 trial. Lancet. 2023;402(10411):1449–1458. doi:10.1016/S0140-6736(23)01583-0
24. Goldberg RA, Boyer DS, Holz FG, et al. Pegcetacoplan for geographic atrophy over 30 months: data from OAKS, DERBY, and the GALE long-term extension study. Ophthalmic Surg Lasers Imaging Retina. 2025;56(7):398–406. doi:10.3928/23258160-20250217-01
25. Holz FG, Ho A, Khanani AM, et al. Efficacy of pegcetacoplan in subgroups defined by distance from the foveal center point in the phase 3 OAKS and DERBY studies of patients with geographic atrophy [oral presentation].
26. Chakravarthy U, Schwartz R, Guymer RH, et al. Visual function benefit after treatment with pegcetacoplan: microperimetry analysis from the phase 3 OAKS trial: microperimetry: visual function benefit with pegcetacoplan. Am J Ophthalmol. 2025;273:119–129. doi:10.1016/j.ajo.2025.02.012
27. Chen FK, Patel PJ, Webster AR, Coffey PJ, Tufail A, Da Cruz L. Nidek MP1 is able to detect subtle decline in function in inherited and age-related atrophic macular disease with stable visual acuity. Retina. 2011;31(2):371–379. doi:10.1097/IAE.0b013e3181e46af3
28. Dreyhaupt J, Mansmann U, Pritsch M, Dolar-Szczasny J, Bindewald A, Holz FG. Modelling the natural history of geographic atrophy in patients with age-related macular degeneration. Ophthalmic Epidemiol. 2005;12(6):353–362. doi:10.1080/09286580591005723
29. Sunness JS, Margalit E, Srikumaran D, et al. The long-term natural history of geographic atrophy from age-related macular degeneration: enlargement of atrophy and implications for interventional clinical trials. Ophthalmology. 2007;114(2):271–277. doi:10.1016/j.ophtha.2006.09.016
30. Shen L, Liu F, Grossetta Nardini H, Del Priore LV. Natural history of geographic atrophy in untreated eyes with nonexudative age-related macular degeneration: a systematic review and meta-analysis. Ophthalmol Retina. 2018;2(9):914–921. doi:10.1016/j.oret.2018.01.019
31. Albini T, Guymer R, MacCumber MW, et al. Fellow eye analysis in bilateral GA due to AMD: long-term data from the OAKS, DERBY, and GALE studies [oral presentation].
32. Anegondi N, Steffen V, Sadda SR, et al. Visual loss in geographic atrophy: learnings from the lampalizumab trials. Ophthalmology. 2025;132(4):420–430. doi:10.1016/j.ophtha.2024.11.017
33. Chakravarthy U, Bailey CC, Johnston RL, et al. Characterizing disease burden and progression of geographic atrophy secondary to age-related macular degeneration. Ophthalmology. 2018;125(6):842–849. doi:10.1016/j.ophtha.2017.11.036
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.