Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Efficacy of an Intelligent Closed-Loop Warming System in Preventing Perioperative Hypothermia and Improving Recovery in Video-Assisted Thoracoscopic Surgery: A Randomized Controlled Trial
Authors Chen R, Du Y, He X ![]() , Fan J, Zhang Y
, Fan J, Zhang Y ![]() , Bai Y, Liu M
, Bai Y, Liu M ![]() , Shen W, Yu T
, Shen W, Yu T ![]() , Wang G
, Wang G ![]()
Received 24 November 2025
Accepted for publication 5 March 2026
Published 13 March 2026 Volume 2026:22 579479
DOI https://doi.org/10.2147/TCRM.S579479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Ruirong Chen,1,* Yingjie Du,1,* Xiongpeng He,2 Jinhan Fan,1 Yue Zhang,1 Yafan Bai,1 Min Liu,1 Wenjia Shen,1 Tiankuo Yu,1 Guyan Wang1
1Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Ultrasound Medicine; Guangdong Provincial Key Laboratory of Major Obstetric Diseases; Guangdong Provincial Clinical Research Center for Obstetrics and Gynecology; The Third Affiliated Hospital, Guangzhou Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guyan Wang, Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China, Email [email protected]
Purpose: To evaluate the efficacy of an intelligent closed-loop warming system compared with conventional warming methods in preventing perioperative hypothermia and improving postoperative recovery in patients undergoing video-assisted thoracoscopic surgery (VATS).
Patients and Methods: A total of 118 adult patients scheduled for elective VATS were randomly assigned to the conventional warming group (n = 59) or the intelligent closed-loop warming group (n = 59). Conventional warming management employed an underbody warming blanket, supplemented with blood and fluid warming when core temperature fell below 36.0°C. The intelligent closed-loop warming system utilized wireless sensors and an automated feedback-controlled warming unit to maintain core temperature between 36.5°C and 37.0°C. Core temperature was continuously monitored from anesthesia induction to post-anesthesia care unit (PACU) discharge. The primary outcome was the incidence of perioperative hypothermia (core temperature < 36.0°C). Secondary outcomes included mean and minimum intraoperative temperature, extubation time, PACU temperature, postoperative complications, length of hospital stay (HLOS), and hospitalization cost.
Results: Perioperative hypothermia occurred in significantly fewer patients in the intelligent group than in the conventional group (25.4% vs. 76.3%, p < 0.001). The intelligent closed-loop warming system maintained higher mean (36.40 ± 0.33°C vs. 35.96 ± 0.45°C, p < 0.001) and minimum (36.09 ± 0.35°C vs. 35.58 ± 0.58°C, p < 0.001) core temperatures. Extubation time was shorter (5.12 ± 2.31 min vs. 9.69 ± 8.27 min, p < 0.001), PACU temperature was higher (p = 0.001), postoperative fever incidence was lower (0% vs. 13.6%, p = 0.006), and HLOS was reduced (10.02 ± 3.87 vs. 11.63 ± 4.25 days, p = 0.034). No significant differences were observed in infection rate or hospitalization cost.
Conclusion: The intelligent closed-loop warming system effectively prevents perioperative hypothermia and enhances postoperative recovery in VATS patients. It provides precise thermal regulation and better clinical outcomes, supporting its application in perioperative temperature management.
Keywords: intelligent closed-loop warming, perioperative hypothermia, video-assisted thoracoscopic surgery, temperature management
Introduction
Perioperative hypothermia is defined as a core body temperature below 36°C occurring before, during, or after surgery.1 It can result from factors such as prolonged surgery, low operating room temperature,2,3 significant blood loss,4 effects of anesthesia, use of cold surgical fluids, and intravenous cold infusions.5 Patient-specific factors like age,4 body mass index(BMI),3 nutritional status, and pre-existing conditions affecting temperature regulation (eg., diabetes, polyneuropathy)2 also contribute. Perioperative hypothermia can lead to serious complications, including increased risk of surgical site infections,6 cardiovascular events,7 bleeding due to coagulopathy,8 postoperative nausea and vomiting,9 discomfort from shivering,10 and higher risk of postoperative delirium.11 Additionally, it is associated with longer recovery times, extended hospital stays, and increased medical costs.3 Longer recovery can further raise the risk of complications like deep vein thrombosis12 and pulmonary issues, creating a cycle of adverse effects.
In thoracic surgery, video-assisted thoracoscopic surgery (VATS) has gradually become the preferred method for the management of mediastinal tumors and lung cancer.13,14 Patients undergoing VATS are at increased risk of developing hypothermia due to extensive exposure of the pleural cavity to cool ambient air, resulting in substantial evaporative heat loss.15 The incidence of intraoperative hypothermia among patients undergoing VATS is notably high, with studies indicating rates up to 64%-72.7%.3,16 This highlights the significant challenge of managing hypothermia during these procedures. Research has demonstrated that intraoperative warming measures can effectively reduce hypothermia rates, decrease the risk of infections and complications, and improve postoperative recovery.17 Common warming devices include forced-air systems, warming blankets or pads, and fluid warmers.17,18
Active perioperative warming is essential for preventing hypothermia and its associated complications. Currently, self-warming or heating blankets and forced-air warming systems represent the two most commonly available techniques for perioperative temperature management.19 Although forced-air warming is often considered effective, evidence comparing heating blankets with forced-air systems remains inconsistent. Notably, a recent systematic review and meta-analysis suggested that heating blankets can achieve core temperature control comparable to forced-air warming devices, and in some clinical contexts may not be inferior.20
In our institution, patients undergoing VATS in the lateral decubitus position are routinely managed with an underbody self-warming blanket, with warmed intravenous fluids used when appropriate. This strategy is widely adopted in routine practice because it does not interfere with the surgical field, is easy to implement, and is compatible with lateral positioning.
Recently, closed-loop temperature management systems have been shown to improve perioperative thermal control in other surgical settings, such as elderly patients undergoing laparoscopic rectal cancer surgery.19 However, whether such closed-loop systems provide additional benefit over conventional underbody warming methods in VATS patients positioned laterally remains unclear. Moreover, conventional warming strategies largely rely on manual monitoring and adjustment, which may limit their ability to respond promptly to rapid intraoperative temperature fluctuations. Therefore, further evaluation of automated, closed-loop temperature management in this specific clinical context is warranted.
Intelligent closed-loop warming systems integrate wireless temperature sensors with medical warming devices to enable real-time monitoring and automatic adjustment, potentially optimizing perioperative thermoregulation and reducing the risk of hypothermia. Despite these theoretical advantages, their application in VATS remains limited, and robust clinical evidence supporting their effectiveness is still lacking.
Although various conventional warming strategies are widely used, they may not adequately address the distinctive thermal challenges of VATS, including single-lung ventilation and extensive pleural exposure, which substantially increase heat loss and demand more precise temperature control. Our previous study demonstrated that a resistive heating mattress effectively reduced intraoperative hypothermia and shivering in thyroid surgery.21 However, that study did not involve a closed-loop warming system and did not address the specific thermoregulatory demands of VATS.
These limitations underscore the need to determine whether an automated, feedback-controlled warming approach can provide superior protection against perioperative hypothermia compared with conventional methods. Therefore, we designed this randomized controlled trial to evaluate the effectiveness of an intelligent closed-loop warming system versus conventional warming management in patients undergoing VATS.
Materials and Methods
Participants
From September 1, 2025, to October 15, 2025, the participants included patients scheduled for elective VATS, classified as American Society of Anesthesiologists (ASA) Physical Status I–III, and aged over 18 years. This study was approved by the Ethics Committee of Beijing Tongren Hospital, Capital Medical University (Approval No. TREC2025-KY141; Date: 7 August 2025). Written informed consent was obtained from all participants before inclusion in the study.Exclusion criteria comprised patients with a history of VATS surgery, those with preoperative fever (body temperature > 37.3°C), individuals suffering from diseases that cause elevated body temperature, patients unable to effectively provide informed consent, and patients with damaged external ear canals, external ear inflammation (such as acute or chronic external otitis), excessive ear canal secretions, ear canal infections, ear canal deformities, or postoperative ear canal sequelae.
Randomization and Masking
After enrollment, patients were randomly assigned to either the conventional warming group or the intelligent closed-loop warming group. The randomization sequence was generated using SPSS 25.0 (IBM Inc., Chicago, IL, USA) and concealed in sealed, opaque envelopes. Group allocation was revealed intraoperatively by an anesthesia nurse who was responsible for operating the warming devices to ensure correct implementation of the assigned intervention and patient safety.
Given the characteristics of the warming interventions, a partial blinding strategy was implemented. The anesthesia nurse was aware of group allocation solely for device operation and safety monitoring and was not involved in anesthesia management, outcome assessment, or data analysis. All anesthesiologists responsible for intraoperative anesthesia management were blinded to group allocation and did not participate in the operation or adjustment of the warming devices. Patients were unaware of their treatment assignment. Outcome assessors, data collectors, and statisticians were blinded to group allocation throughout the study to minimize assessment and analysis bias.
General Procedure
Upon entering the operating room, all patients underwent standard monitoring, including non-invasive blood pressure (or invasive continuous arterial pressure monitoring), heart rate, pulse oximetry, 5-lead electrocardiograph, and bispectral index. Surgery was performed under combined intravenous and inhalation anesthesia. Induction medications included propofol (1.5–2.5 mg·kg−1), sufentanil (0.2–0.3 μg·kg−1), and cisatracurium (0.6 mg·kg−1). Three minutes later, a double-lumen endotracheal tube was inserted with the aid of a video laryngoscope, followed by positioning with a fiberoptic bronchoscope. Ventilation parameters were set as follows: volume-controlled ventilation with 100% oxygen, tidal volume of 6–8 mL·kg−1, respiratory rate of 12–15 min−1, positive end-expiratory pressure of 5 cmH2O, and an inspiratory to expiratory ratio of 1:2. Respiratory parameters were adjusted to maintain normal oxygen saturation (SpO2) (≥90%) and end-tidal carbon dioxide partial pressure (PetCO2) (35–45 mmHg). Anesthesia maintenance involved continuous infusion of propofol (4–12 mg·kg−1·h−1) and remifentanil (0.1–0.3 μg·kg−1·min−1), combined with 1% sevoflurane to maintain an appropriate depth of anesthesia. Intermittent muscle relaxation was maintained with cisatracurium (0.03 mg·kg−1) administered every 20 minutes. Fluid maintenance primarily consisted of lactated Ringer’s solution, with colloids supplemented as necessary. For both groups, all intravenous fluids were maintained at body temperature using an incubator (MIR-162; Sanyo, Osaka, Japan). Intraoperative blood pressure was maintained with a mean arterial pressure of 65–75 mmHg. Vasoactive medications were used as needed to ensure hemodynamic stability within 20% of the patient’s baseline levels. At the end of surgery, neuromuscular blockade was reversed with atropine (0.025 mg·kg−1) and neostigmine (0.05 mg·kg−1). After thorough suctioning of the oral cavity and upon the return of consciousness and spontaneous breathing, the endotracheal tube was removed. The patient was then transferred to PACU.
Temperature Monitoring and Perioperative Warming Strategies
Before anesthesia induction, a nurse placed a wireless continuous temperature monitoring sensor probe (WMT102, WISMED Medical Equipment Company, Heilongjiang, China) in the patient’s external ear canal to monitor tympanic temperature throughout the surgery (measured every 1 minute). The continuous temperature monitoring sensor probe was secured behind the ear with a hypoallergenic adhesive patch to prevent displacement. This device was approved by the China Food and Drug Administration as a Class II medical device.
The operating room temperature was set and maintained at approximately 22°C, with a humidity level of 40–60%.22 For patients in the intelligent closed-loop warming group, the intelligent closed-loop warming system was pre-installed on the operating table Once the patient was transferred to the operating table, the closed-loop warming devices (WMTC102, WISMED Medical Equipment Company, Heilongjiang, China) were activated immediately. The target temperature range for the patient’s body was set to 36.5°C-37.0°C. The target temperature for the medical warming blanket was set to 38°C, the blood and fluid warmer to 38°C, and the peripheral circulation heating device to 38°C. The system automatically stops warming when the patient’s body temperature exceeded the target range. For patients in the conventional warming group, a warming blanket device was activated immediately after the patient was transferred to the operating table, with the blanket placed underneath the patient. Warming was stopped when the body temperature exceeds 37°C. If the patient’s body temperature dropped below 36°C, a blood and fluid warmer was used.
Outcomes and Postoperative Evaluation
This study systematically documented a comprehensive array of critical perioperative information for each patient, including demographic characteristics, comorbidities, medical history, hospitalization-related data, and ASA physical status classification. Additionally, laboratory results were collected both preoperatively and 24 hours postoperatively. Intraoperatively, detailed records were kept of the type of surgery, blood loss, fluid intake, irrigation fluid usage, urine output, fluctuations in blood pressure and heart rate, temperature changes, duration of surgery and anesthesia, whether the patient received thoracic paravertebral nerve block (TPVB), and the time of extubation. Furthermore, upon entering the PACU, data on recovery time, average temperature, SpO2, incidence of hypertension, shivering, and delirium were collected. A follow-up was conducted within 30 days post-surgery, focusing on the occurrence of complications and adverse events, including cardiovascular complications, pulmonary embolism, cerebral infarction, surgical site infection, pulmonary infection, fever, and mortality. The primary outcome of the study was the incidence of perioperative hypothermia, while secondary outcomes included length of hospital stay (HLOS, days), total hospitalization cost (THC, CNY), and postoperative complications, such as shivering, delirium, cardiovascular complications, pulmonary embolism, cerebral infarction, incisional wound infection, pulmonary infection, fever, and death.
Statistical Methods
The sample size was determined based on previous studies and preliminary trial results, which indicated that approximately 60% of adult patients undergoing VATS experience intraoperative hypothermia.3,16 Based on the preliminary results, we assumed the incidence of hypothermia in the warming group is 30%. To assess the difference between the two groups, we set the significance level at α = 0.05 and the statistical power at 1 − β = 0.9. Sample size calculations using PASS 11.0 software (NCSS Statistical and Data Analysis, USA) indicated that 53 participants per group were needed. After accounting for a 10% dropout rate, the final sample size was adjusted to 59 per group, resulting in a total of 118 participants (59 in each group).
The homogeneity of variance was examined using the Levene test. Continuous data were analyzed using Student’s t-test or the Mann–Whitney U-test, depending on the normality assessed by the Kolmogorov–Smirnov test. The area under the curve (AUC) for hypothermia was calculated to quantify the cumulative duration that patients’ temperatures fell below a critical threshold (36.0°C) and compared between groups using the Mann–Whitney U-test. Categorical data were compared using the χ2-test or Fisher’s exact test. Potential confounding factors were first identified using univariable logistic regression analysis; variables with p < 0.1 were selected for further consideration. Subsequently, multivariable logistic regression analysis was performed, incorporating both the variables identified from univariable analysis (p < 0.1) and clinically relevant variables (even if p ≥ 0.1 in univariable analysis). A clinically significant temperature difference in hypothermic patients between intervention and control groups was defined as 0.2°C, in accordance with the guidelines of the National Institute for Health and Clinical Excellence in the UK. Statistical analyses were performed using SPSS 25.0 (IBM Inc., Chicago, IL, USA) and R software (version 4.3.1; R Foundation for Statistical Computing, Vienna, Austria).
Results
This study initially screened 130 patients, out of which 6 were excluded for not meeting the inclusion criteria. Ultimately, 124 patients were enrolled and randomly assigned to the conventional warming group (n = 62) and the intelligent closed-loop warming group (n = 62). In the conventional warming group (n = 62), 1 patient canceled the surgery before the operation, and 2 patients had their surgical procedures changed intraoperatively due to changing conditions. In the intelligent closed-loop warming group (n = 62), 1 patient canceled the surgery before the operation, 1 patient had the surgical procedure changed intraoperatively, and 1 patient had to discontinue warming intraoperatively due to equipment power failure and was withdrawn from the study. After excluding these cases, 118 patients completed the entire study protocol and were included in the final analysis, with 59 patients in both the intelligent closed-loop warming group and the conventional warming group (Figure 1).
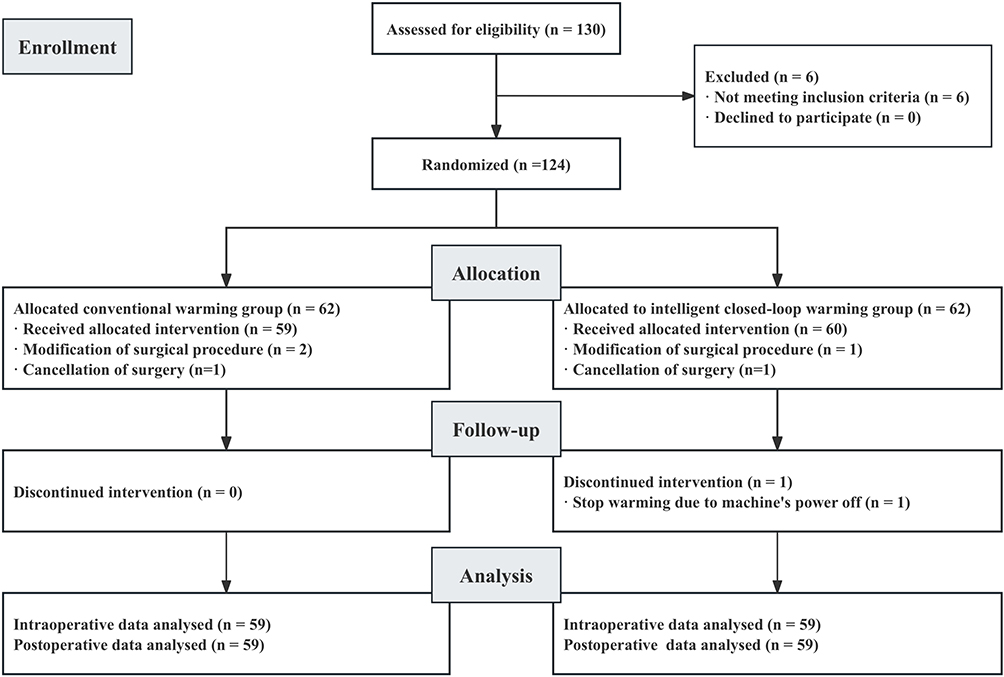 |
Figure 1 Flow diagram of participant enrollment, allocation, and analysis. A total of 130 participants were assessed for eligibility, with 6 excluded due to not meeting inclusion criteria. After randomization, 62 participants were allocated to the conventional warming group and 62 to the intelligent closed-loop warming group. In the conventional warming group, 59 participants received the allocated intervention, with 2 modifications in the surgical procedure and 1 surgery cancellation. In the intelligent closed-loop warming group, 60 participants received the allocated intervention, with 1 modification in the surgical procedure and 1 surgery cancellation. One participant in the intelligent closed-loop warming group discontinued the intervention due to a power failure. Data were analyzed for 59 participants in each group, both intraoperatively and postoperatively. |
There were no significant differences in demographic or perioperative baseline characteristics between the two groups (Table 1). Variables such as sex distribution, age, weight, height, BMI, and ASA physical status were comparable (p > 0.05). The prevalence of comorbidities—including hypertension, coronary heart disease, cerebrovascular disease, diabetes, respiratory disorders, and autoimmune diseases—did not differ significantly between groups. Likewise, lifestyle and medical history factors such as smoking, alcohol consumption, drug allergies, previous general anesthesia, and tumor history were similar (p > 0.05). Intraoperative parameters, including estimated blood loss, infusion volume, urine output, and operation and anesthesia duration, were also comparable between groups. The proportions of patients undergoing pulmonary lobectomy and receiving TPVB did not differ significantly (p > 0.05).
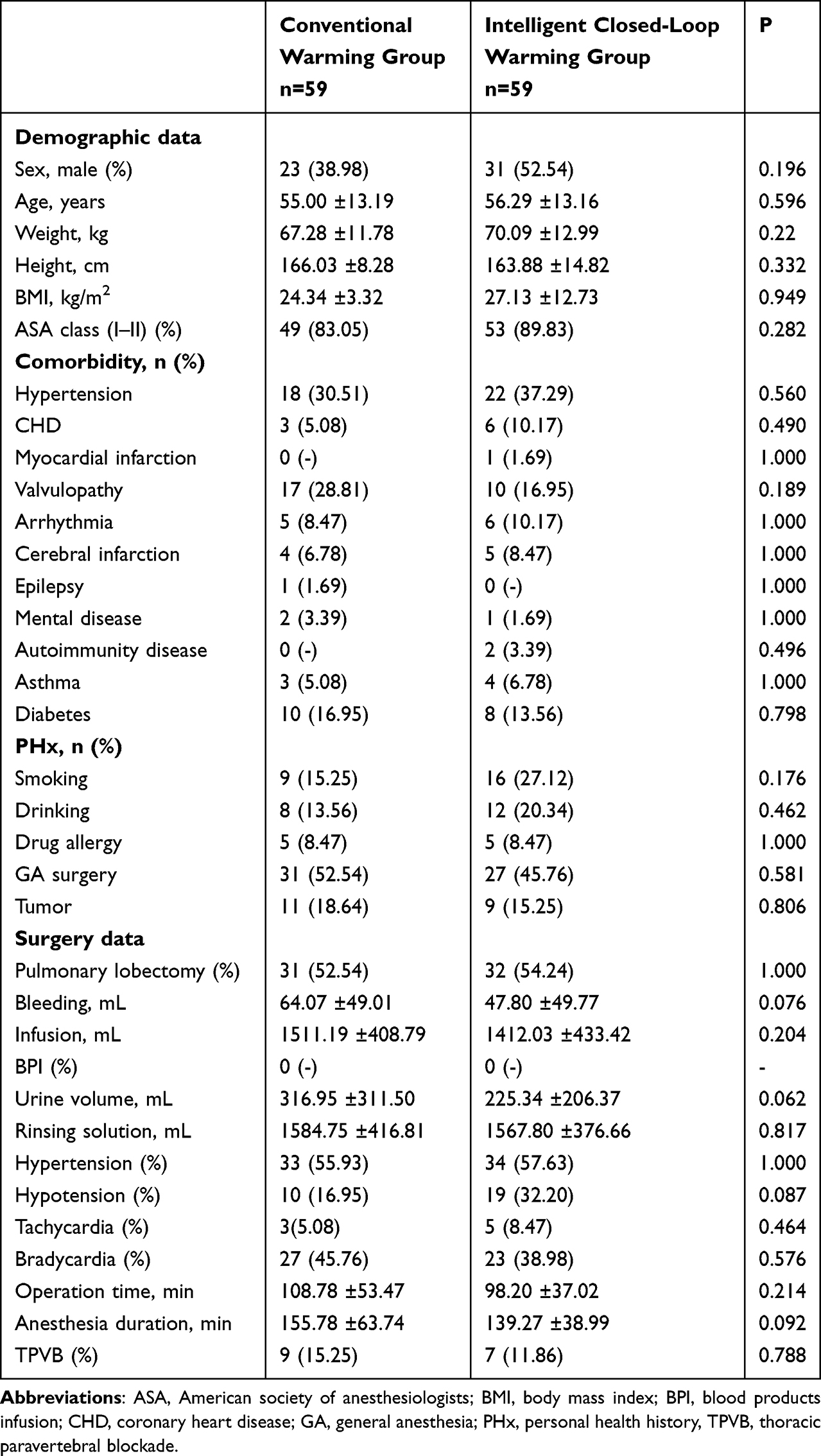 |
Table 1 Patient and Perioperative Characteristics |
The incidence of perioperative hypothermia (core temperature < 36.0°C) was significantly lower in the intelligent closed-loop warming group than in the conventional warming group (25.4% vs 76.3%, p < 0.001). Patients in the intelligent group also maintained higher minimum (36.09 ± 0.35°C vs 35.58 ± 0.58°C, p < 0.001) and mean intraoperative temperatures (36.40 ± 0.33°C vs 35.96 ± 0.45°C, p < 0.001) (Table 2). In the PACU, patients in the intelligent warming group had a significantly higher mean body temperature (36.28 ± 0.17°C vs 36.18 ± 0.12°C, p = 0.001), while PACU duration and the incidence of desaturation (SpO2 < 90%) or hypertension showed no significant differences (p> 0.05). Regarding secondary outcomes, extubation duration was markedly shorter in the intelligent warming group (5.12 ± 2.31 min vs 9.69 ± 8.27 min, p < 0.001). HLOS was reduced (10.02 ± 3.87 days vs 11.63 ± 4.25 days, p = 0.034), whereas THC was comparable between groups (p = 0.103). No significant differences were found in postoperative complications, including shivering, delirium, cardiovascular events, pulmonary embolism, cerebral infarction, wound infection, or pulmonary infection (all p > 0.05). However, the incidence of postoperative fever was significantly lower in the intelligent warming group (0% vs 13.6%, p = 0.006). No deaths occurred in either group.
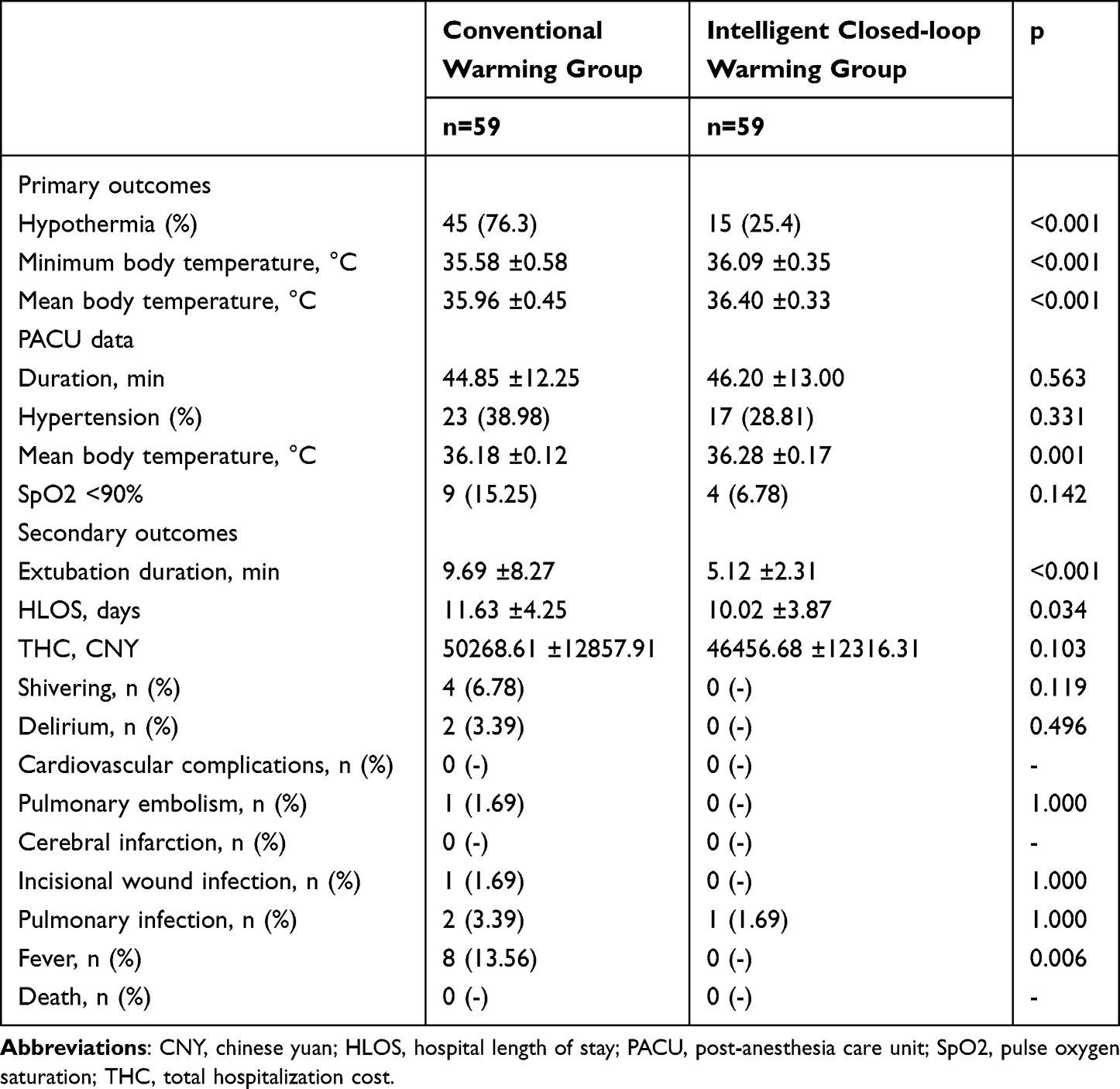 |
Table 2 Intraoperative and PACU Temperature Parameters and Postoperative Outcomes |
Table 3 illustrates the changes in core temperature over surgery time for both the conventional warming group and the intelligent closed-loop warming group. The results indicate that core temperature decreases over time in both groups, but the intelligent closed-loop warming group consistently maintains a higher core temperature throughout the procedure. At the 0-minute mark, the core temperature difference between the two groups is statistically significant (p < 0.001).Both groups exhibit a steady decline in temperature, with the conventional warming group experiencing a more pronounced drop, notably at the 150-minute mark (ΔTc = −1.12°C). Statistical analysis reveals significant temperature differences between the groups at most time points (p < 0.001), underscoring the superior efficacy of the Intelligent Closed-Loop Warming method in maintaining core temperature during surgery. However, the difference between the groups becomes less pronounced at later time points, such as at 240 minutes (p = 0.206).
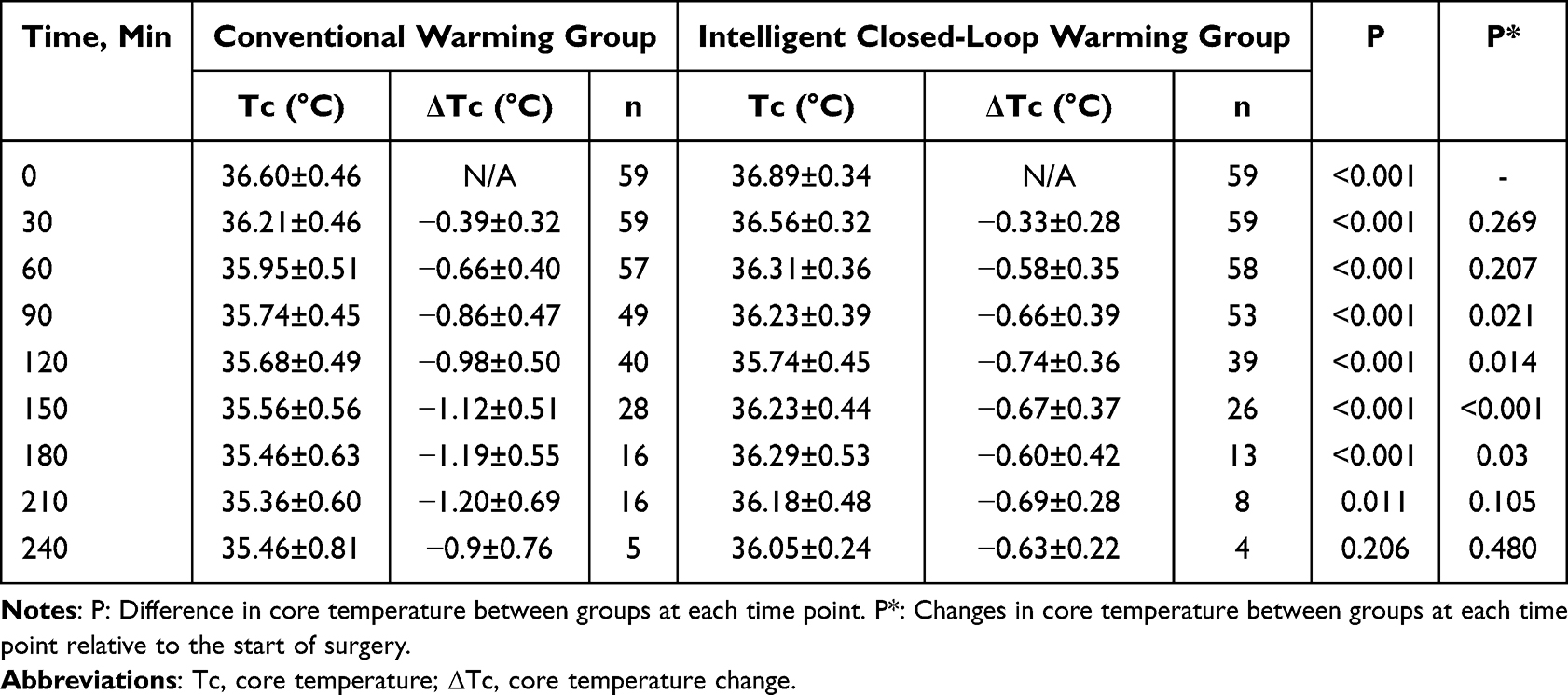 |
Table 3 Changes in Core Temperature Over Surgery Time |
Both groups showed a decrease in core temperature over time, but the intelligent closed-loop warming group consistently maintained a higher temperature compared to the conventional warming group (Figure 2). The conventional warming group exhibited a more significant drop in temperature, especially after 120 minutes, while the intelligent closed-loop warming group demonstrated more stable temperature regulation throughout the procedure.
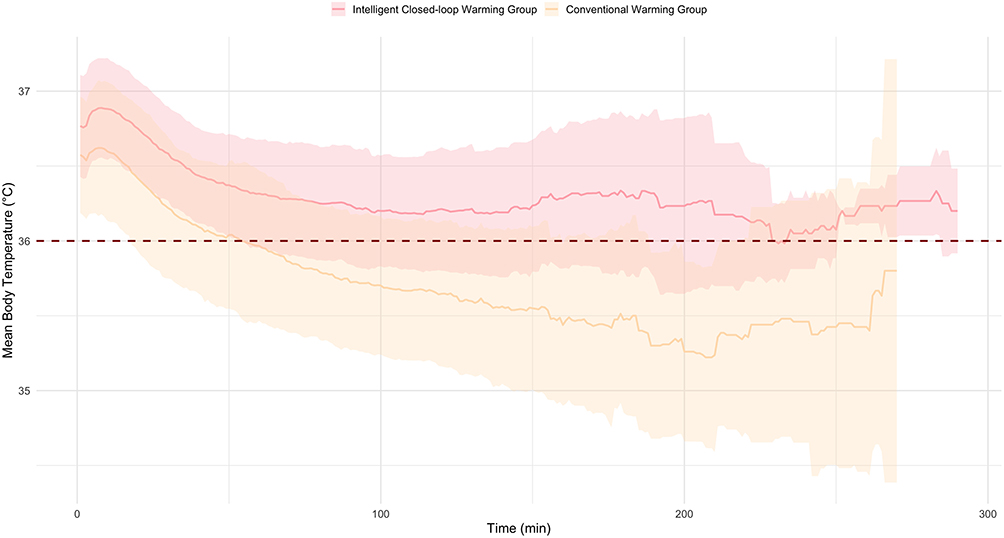 |
Figure 2 Trends in mean core temperature over time in conventional and intelligent closed-loop warming groups during surgery. Changes in mean core temperature over time for the conventional warming and intelligent closed-loop warming groups. The solid lines represent the average core temperature, while the shaded areas show the standard deviation. The intelligent closed-loop warming group maintained a higher core temperature throughout the surgery compared to the conventional warming group. |
In this study, we compared AUC for hypothermia between groups (U=726, p<0.001). Figure 3 illustrates the density distribution of the log-transformed, normalized AUC for the intelligent closed-loop warming group and the conventional warming group. The pink and orange shaded areas represent the density of AUC values for the intelligent closed-loop warming group and the conventional warming group, respectively. The intelligent closed-loop warming group shows a higher density of values near zero, while the conventional warming group has a more spread-out distribution with a peak around 0.6.
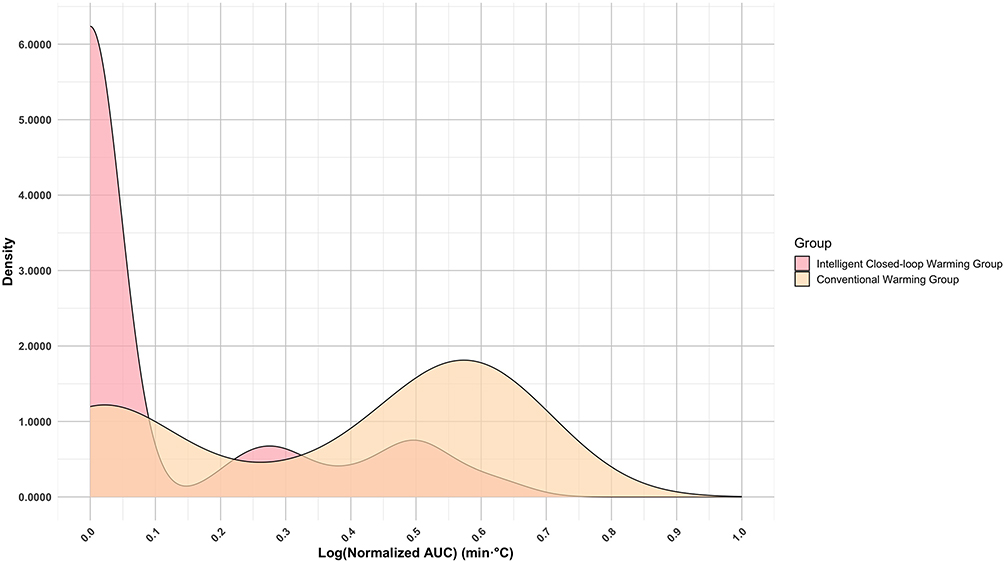 |
Figure 3 Density plot comparing log (normalized AUC) for the intelligent closed-loop warming group and the conventional warming group. The plot shows the density distribution of the log-transformed Normalized area under the curve (AUC) of low body temperature duration for patients in two different groups: the intelligent closed-loop warming group (shown in pink) and the conventional warming group (shown in Orange). The x-axis represents the Log (Normalized AUC) in min·°C, indicating both the duration and severity of low temperatures, while the y-axis represents the density. |
Table 4 presents the odds ratios (OR) for perioperative hypothermia. The crude OR for perioperative hypothermia is 0.106 (95% CI: 0.046–0.245), with a P-value of <0.001, indicating a significant association. After adjustment for BMI, age, sex, ASA physical status I–II, hypertension, valvular disease, coronary heart disease, arrhythmia, initial body temperature, and operating room ambient temperature, the adjusted OR was 0.088 (95% CI: 0.034–0.230), with a p-value of <0.001, suggesting that the association remains strong and significant after controlling for these variables.
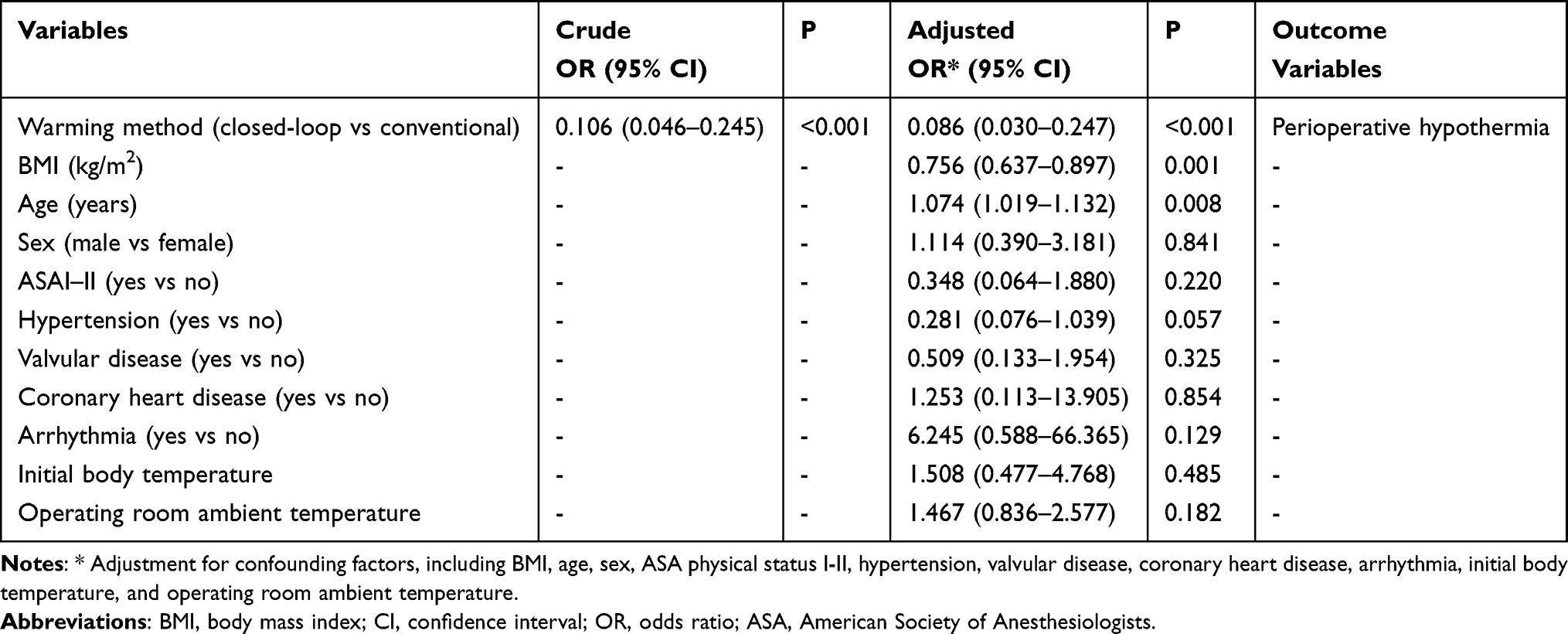 |
Table 4 Odds Ratios of Perioperative Hypothermia |
The preoperative and postoperative laboratory results are summarized in Supplementary Table 1. Preoperative results include white blood cell count (WBC), differential counts (neutrophils, lymphocytes, monocytes, eosinophils, basophils), red blood cell count (RBC), differential ratios, hemoglobin, platelet count, liver function tests (alanine aminotransferase, aspartate aminotransferase, total bilirubin, direct bilirubin), total protein, albumin, blood urea nitrogen (BUN), fasting serum glucose (FSG), serum creatinine (Scr), creatine kinase (CK), lactate dehydrogenase (LDH), lipoprotein, clotting times (prothrombin time activity, activated partial thromboplastin time, prothrombin time, thrombin time), fibrinogen, D-dimer, serum potassium (K+), total cholesterol (TC), triglycerides, high-density lipoprotein (HDL), low-density lipoprotein (LDL) and neutrophil-to-HDL ratio (NHR). Postoperative results encompass similar parameters. Notably, significant differences were observed in postoperative RBC (p = 0.017), hemoglobin (p = 0.013), and HDL levels (p = 0.018) between the groups.
Discussion
This study compared the efficacy of conventional warming and intelligent closed-loop warming in maintaining perioperative normothermia. The findings demonstrate that intelligent closed-loop warming significantly improves intraoperative temperature regulation, thereby enhancing patient outcomes. Key advantages of the intelligent closed-loop warming system included a lower incidence of hypothermia, higher minimum and mean core body temperatures, and improved thermal recovery in PACU. Additionally, the system reduced the AUC for hypothermia, indicating less cumulative time spent below 36.0°C. Further benefits included shorter extubation times, reduced incidence of postoperative fever, and decreased length of hospital stay. Nevertheless, complete prevention of perioperative hypothermia remains challenging.
Analysis of patients’ temperature-time curves during surgery reveals that both the intelligent closed-loop warming group and the conventional warming group exhibit an initial rapid temperature drop, followed by a slower decline and subsequent stabilization phase. This initial drop is primarily due to blood flow redistribution after anesthesia induction, while the subsequent decline is caused by continuous heat loss and the infusion of cold fluids.23,24 The conventional warming group may not adequately address these dynamic changes, leading to a more significant temperature decline. Conversely, the intelligent closed-loop warming group likely uses feedback mechanisms to adjust the warming rate in real time based on core temperature fluctuations, thus maintaining more stable temperatures throughout surgery. This approach is more effective at preventing intraoperative hypothermia compared to traditional methods. The area under the curve (AUC) for temperatures below 36°C, representing the temperature-time integral, is a more sensitive measure of hypothermia exposure.25,26 The AUC density plot reveals that the intelligent closed-loop warming group experienced shorter and milder hypothermia durations, whereas the conventional warming group showed greater variability with longer and more severe hypothermia. This underscores the superior performance of the intelligent closed-loop warming group in maintaining stable core temperatures during surgery through precise and responsive temperature management.
Beyond the mechanistic findings, this trial also expands upon our previous work on perioperative warming.21 Whereas our earlier study evaluated a resistive heating mattress in thyroid surgery, the present investigation examined an advanced closed-loop warming system in a thoracoscopic population. Several methodological improvements were introduced, including continuous tympanic core-temperature monitoring, use of hypothermia AUC as an integrated indicator of thermal burden, and multivariable modeling to identify independent predictors of hypothermia. These enhancements allow for a more comprehensive assessment of temperature management and provide new evidence supporting the use of closed-loop warming in thoracic surgery.
In thoracoscopic surgery, the incidence of hypothermia with intelligent closed-loop warming (without preoperative forced warming) was 25.4%, significantly lower than 76.3% with conventional warming, but higher than 12.24% with preoperative and intraoperative forced warming, yet better than 32.65% with intraoperative forced warming alone.27 This suggests that intelligent warming technology is more effective at preventing intraoperative hypothermia, even without preoperative forced warming, due to its precise temperature regulation. It remains a viable alternative when preoperative forced warming is not possible.
The intraoperative blood loss showed a difference between the two groups but was not statistically significant. However, there were significant differences in hemoglobin and red blood cell counts 24 hours postoperatively. This suggests that although the immediate blood loss during surgery might not have been substantial enough to show a statistical difference, the cumulative effect of blood loss over time,28 along with factors such as fluid shifts and hemodilution,29 became more apparent in the postoperative period. Previous studies have suggested that the duration of perioperative hypothermia may be associated with an increased relative risk of intraoperative blood loss and transfusion.30 This could be due to the negative impact on platelet function, reduced levels of various coagulation factors and fibrinogen, inhibition of coagulation cascade enzymes, and activation of the fibrinolytic system.31,32
Previous studies have shown that intraoperative heating can help reduce the risk of surgical site infections.17,33 However, our research found no significant difference in postoperative surgical site and pulmonary infections between the two groups. This finding is consistent with recent evidence suggesting that the association between perioperative hypothermia and surgical site infection may not be statistically significant in the overall surgical population, but may become more evident in specific surgical subgroups and at lower temperature thresholds (eg., <35°C).34 This may be attributed to the adherence to sterile practices during surgery and the effectiveness of postoperative infection prevention measures. Although the smart closed-loop heating system demonstrated certain advantages in maintaining temperature, it did not significantly impact the risk of infection under the current conditions, resulting in no observable differences.
HDL is a crucial component of plasma lipoproteins and possesses antioxidant, anti-inflammatory, anti-apoptotic, and antithrombotic properties.35 Studies have shown that HDL can inhibit the activation, adhesion, spreading, and migration of neutrophils.36,37 However, a large number of activated neutrophils can alter the structure and content of various lipoproteins, thereby affecting the function of HDL.38 Recently, the neutrophil-to-HDL ratio (NHR) has emerged as a novel biomarker associated with increased inflammatory states and has been linked to systemic inflammatory response syndrome (SIRS).39 In this study, the conventional warming group exhibited higher levels of HDL and NHR compared to the intelligent closed-loop warming group. This suggests that the conventional warming method was less effective, leading to a greater inflammatory response. Reducing systemic inflammation and immune-inflammatory activity helps limit rises in uric acid (UA).40 UA, in turn, directly influences immune cell populations, cytokine expression, chemotaxis and differentiation, and the activation of resident cells, thereby amplifying inflammation.41,42 The conventional warming group had higher postoperative UA levels than the intelligent closed-loop warming group, consistent with a stronger inflammatory response. This difference in inflammatory response may partially explain the significant disparity in the incidence of postoperative fever between the two groups.
Although previous studies have confirmed that perioperative forced warming reduces the incidence of shivering,17,33 our study found no significant difference in the occurrence of shivering between the two groups. This may be due to the fact that both groups in our study utilized heated intravenous fluids and irrigation solutions, as 1 liter of unheated crystalloid can lower core temperature by 0.25°C to 0.30°C, which has been shown in recent studies to effectively increase shivering.43 Consistent with this finding, the incidence of postoperative shivering in our trial was lower than that reported in studies where heated fluids were not used during surgery.44
We found that the extubation time, average temperature in the PACU, and length of hospital stay were significantly reduced in the intelligent closed-loop warming group. Additionally, there was a difference in hospitalization costs between the intelligent closed-loop warming group and the conventional warming group; however, this difference did not reach statistical significance.
Hypothermia can slow down the metabolism of anesthetic agents, prolonging their effects, delaying extubation and prolonging postoperative recovery.45 Improved circulation and oxygenation during warming enhance the body’s ability to recover, allowing for a quicker awakening from anesthesia.1 Consistent with previous studies showing that well-managed temperature control leads to quicker awakenings,46 better respiratory function recovery,47 and shorter hospital stays,25 this study suggests that the intelligent closed-loop warming system may enhance postoperative recovery by optimizing temperature management, resulting in shorter extubation times and reduced hospital stays. However, although there was a trend in hospitalization costs, many factors can influence these costs, and further research may be needed to determine the clinical significance of this difference.
In the context of thoracoscopic surgery, where patients are exposed to substantial heat loss due to pleural opening, prolonged anesthesia, and limited options for surface warming, maintaining stable perioperative normothermia remains a practical challenge. The findings of this study suggest that automated, feedback-controlled temperature management may offer a useful approach to address these challenges by reducing reliance on intermittent temperature assessment and manual adjustment during surgery. By directly linking continuous core temperature monitoring to automated warming regulation, closed-loop systems allow perioperative temperature control to follow a more continuous and physiologically guided course.
From a clinical perspective, the use of such systems may help standardize temperature management during VATS procedures, where workflow complexity and positioning constraints can limit the effectiveness of conventional warming strategies. Reduced dependence on repeated manual intervention may also simplify intraoperative management for anesthesia teams and support more consistent adherence to perioperative normothermia as a quality-of-care indicator. More broadly, although evaluated here in a thoracoscopic setting, this approach illustrates how intelligent temperature management may contribute to more data-informed and standardized perioperative care in surgical procedures associated with high thermal vulnerability.
While this study provides valuable insights into the benefits of intelligent closed-loop warming, there are some limitations. First, the study was conducted at a single center, which may limit the generalizability of the results. Second, while the intelligent closed-loop warming system demonstrated significant advantages in temperature regulation, further research is needed to investigate long-term outcomes such as post-surgical recovery time, complications, and overall patient satisfaction. Future studies should also explore the health economic impact of implementing intelligent closed-loop warming systems in clinical practice.
Conclusion
In conclusion, the intelligent closed-loop warming system is more effective than conventional warming methods in preventing perioperative hypothermia in patients undergoing video-assisted thoracoscopic surgery. This study demonstrates that the intelligent closed-loop warming system provides improved control of core temperature, reduces the incidence of hypothermia, and contributes to enhanced postoperative recovery. From a clinical perspective, these findings suggest that the implementation of intelligent closed-loop warming may facilitate more precise and efficient perioperative temperature management, thereby improving patient safety and supporting postoperative recovery in routine surgical practice. Further research is warranted to evaluate its cost-effectiveness and long-term clinical benefits.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Individual deidentified participant data will be shared. The study protocol, statistical analysis plan, and informed consent form will also be made available. Data will be accessible by contacting the corresponding author at [email protected]. The data will be available beginning 3 months after publication and will remain available for up to 5 years.
Ethics Statement
This prospective, randomized study was conducted in accordance with the Declaration of Helsinki. The study protocol received ethical approval from the Ethics Committee of Beijing Tongren Hospital, Capital Medical University (Approval No. TREC2025-KY141; Date: 7 August 2025),and written informed consent was obtained from all participants prior to study commencement. This trial was registered with the Chinese Clinical Trial Registry (Registration No. ChiCTR2500108325; Date: 28 August 2025).
Acknowledgments
We would like to extend our sincere gratitude to all participants and their families, as well as the professional research team for their invaluable contributions and support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project was supported by the Beijing High-level Public Health Technical Talent Training Plan (No. Lingjunrencai-03–01).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sessler DI. Mild perioperative hypothermia. N Engl J Med. 1997;336(24):1730–14. doi:10.1056/nejm199706123362407
2. Torossian A, Bräuer A, Höcker J, Bein B, Wulf H, Horn EP. Preventing inadvertent perioperative hypothermia. Dtsch Arztebl Int. 2015;112(10):166–172. doi:10.3238/arztebl.2015.0166
3. Li Y, Liang H, Feng Y. Prevalence and multivariable factors associated with inadvertent intraoperative hypothermia in video-assisted thoracoscopic surgery: a single-center retrospective study. BMC Anesthesiol. 2020;20(1):25. doi:10.1186/s12871-020-0953-x
4. Zhao B, Zhu Z, Qi W, et al. Construction and validation of a risk prediction model for intraoperative hypothermia in elderly patients undergoing total Hip arthroplasty. Aging Clin Exp Res. 2023;35(10):2127–2136. doi:10.1007/s40520-023-02500-0
5. Campbell G, Alderson P, Smith AF, Warttig S. Warming of intravenous and irrigation fluids for preventing inadvertent perioperative hypothermia. Cochrane Database Syst Rev. 2015;2015(4):Cd009891. doi:10.1002/14651858.CD009891.pub2
6. Walters MJ, Tanios M, Koyuncu O, Mao G, Valente MA, Sessler DI. Intraoperative core temperature and infectious complications after colorectal surgery: a registry analysis. J Clin Anesth. 2020;63:109758. doi:10.1016/j.jclinane.2020.109758
7. Frank SM, Fleisher LA, Breslow MJ, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial. JAMA. 1997;277(14):1127–1134. doi:10.1001/jama.1997.03540380041029
8. Kander T, Schött U. Effect of hypothermia on haemostasis and bleeding risk: a narrative review. J Int Med Res. 2019;47(8):3559–3568. doi:10.1177/0300060519861469
9. Liang D, Shan Y, Wang L. The effect of prophylactic rewarming on postoperative nausea and vomiting among patients undergoing laparoscopic hysterectomy: a prospective randomized clinical study. Sao Paulo Med J. 2020;138(5):414–421. doi:10.1590/1516-3180.2020.0059.R2.06072020
10. Kameda N, Okada S. Evaluation of postoperative warming care protocol for thermal comfort and temperature management immediately after surgery: nonrandomized controlled trial. J Perianesth Nurs. 2023;38(3):427–433. doi:10.1016/j.jopan.2022.07.001
11. Ju JW, Nam K, Sohn JY, et al. Association between intraoperative body temperature and postoperative delirium: a retrospective observational study. J Clin Anesth. 2023;87:111107. doi:10.1016/j.jclinane.2023.111107
12. Li L, Huang J, Chen X, Ma W, Hu Y, Li Y. A retrospective analysis of the postoperative effect of intraoperative hypothermia on deep vein thrombosis after intracranial tumor resection. World Neurosurg. 2022;167:e778–e783. doi:10.1016/j.wneu.2022.08.099
13. Sihoe ADL. Video-assisted thoracoscopic surgery as the gold standard for lung cancer surgery. Respirology. 2020;25 Suppl 2:49–60. doi:10.1111/resp.13920
14. Liu Q, Hong Z, Cao W, et al. Efficacy of the da vinci robot versus thoracoscopic surgery for patients with mediastinal tumors of different body mass index: a multicenter propensity score-matched study. World J Surg Oncol. 2024;22(1):257. doi:10.1186/s12957-024-03542-y
15. Miserocchi G. Physiology and pathophysiology of pleural fluid turnover. Eur Respir J. 1997;10(1):219–225. doi:10.1183/09031936.97.10010219
16. Emmert A, Gries G, Wand S, et al. Association between perioperative hypothermia and patient outcomes after thoracic surgery: a single center retrospective analysis. Medicine. 2018;97(17):e0528. doi:10.1097/md.0000000000010528
17. Madrid E, Urrútia G, Roqué I Figuls M, et al. Active body surface warming systems for preventing complications caused by inadvertent perioperative hypothermia in adults. Cochrane Database Syst Rev. 2016;4(4):Cd009016. doi:10.1002/14651858.CD009016.pub2
18. Xiong Z, Zhu J, Li Q, Li Y. The effectiveness of warming approaches in preventing perioperative hypothermia: systematic review and meta-analysis. Int J Nurs Pract. 2023;29(6):e13100. doi:10.1111/ijn.13100
19. Wang X, Xu J, Mo L, et al. Closed-loop temperature management with internet of things technology support in elderly laparoscopic rectal cancer surgery: a randomised controlled trial. PLoS One. 2025;20(11):e0335993. doi:10.1371/journal.pone.0335993
20. Al-Dardery NM, Abdelwahab OA, El-Samahy M, Seif AM, Mouffokes A, Khaity A. Self-warming blankets versus active warming by forced-air devices for preventing hypothermia: a systematic review and meta-analysis. Medicine. 2023;102(18):e33579. doi:10.1097/md.0000000000033579
21. Zhang Y, Bai Y, Zhang Y, et al. Effect of aggressive warming versus routine thermal management on the incidence of perioperative hypothermia in patients undergoing thyroid surgery: a prospective, randomized, double-blind controlled trial. Ther Clin Risk Manag. 2024;20:207–216. doi:10.2147/tcrm.S454272
22. Ingram A, Harper M. The health economic benefits of perioperative patient warming for prevention of blood loss and transfusion requirements as a consequence of inadvertent perioperative hypothermia. J Perioper Pract. 2018;28(9):215–222. doi:10.1177/1750458918776558
23. Sessler DI. Perioperative thermoregulation and heat balance. Lancet. 2016;387(10038):2655–2664. doi:10.1016/s0140-6736(15)00981-2
24. Peter J, Klingert K, Klingert W, et al. Automated closed-loop management of body temperature using forced-air blankets: preliminary feasibility study in a porcine model. BMC Anesthesiol. 2018;18(1):80. doi:10.1186/s12871-018-0542-4
25. Sun Z, Honar H, Sessler DI, et al. Intraoperative core temperature patterns, transfusion requirement, and hospital duration in patients warmed with forced air. Anesthesiology. 2015;122(2):276–285. doi:10.1097/aln.0000000000000551
26. Sessler DI, Akça O. Nonpharmacological prevention of surgical wound infections. Clin Infect Dis. 2002;35(11):1397–1404. doi:10.1086/344275
27. Xiao Y, Zhang R, Lv N, Hou C, Ren C, Xu H. Effects of a preoperative forced-air warming system for patients undergoing video-assisted thoracic surgery: a randomized controlled trial. Medicine. 2020;99(48):e23424. doi:10.1097/md.0000000000023424
28. Desai N, Schofield N, Richards T. Perioperative patient blood management to improve outcomes. Anesth Analg. 2018;127(5):1211–1220. doi:10.1213/ane.0000000000002549
29. Kreimeier U, Messmer K. Perioperative hemodilution. Transfus Apher Sci. 2002;27(1):59–72. doi:10.1016/s1473-0502(02)00027-7
30. Torossian A, Van Gerven E, Geertsen K, Horn B, Van de Velde M, Raeder J. Active perioperative patient warming using a self-warming blanket (barrier easywarm) is superior to passive thermal insulation: a multinational, multicenter, randomized trial. J Clin Anesth. 2016;34:547–554. doi:10.1016/j.jclinane.2016.06.030
31. Rajagopalan S, Mascha E, Na J, Sessler DI. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiology. 2008;108(1):71–77. doi:10.1097/01.anes.0000296719.73450.52
32. Spahn DR, Rossaint R. Coagulopathy and blood component transfusion in trauma. Br J Anaesth. 2005;95(2):130–139. doi:10.1093/bja/aei169
33. Ding N, Yang J, Wu C. Comparison of prewarming plus intraoperative warming with intraoperative warming alone in patients undergoing minimally invasive thoracic or abdominal surgery: a systematic review and meta-analysis. PLoS One. 2024;19(9):e0310096. doi:10.1371/journal.pone.0310096
34. Chen R, Du Y, Chen L, et al. The impact of perioperative hypothermia on surgical site infection risk: a meta-analysis. BMC Anesthesiol. 2025;25(1):443. doi:10.1186/s12871-025-03277-7
35. Drifte G, Dunn-Siegrist I, Tissières P, Pugin J. Innate immune functions of immature neutrophils in patients with sepsis and severe systemic inflammatory response syndrome. Crit Care Med. 2013;41(3):820–832. doi:10.1097/CCM.0b013e318274647d
36. Karathanasis SK, Freeman LA, Gordon SM, Remaley AT. The changing face of hdl and the best way to measure it. Clin Chem. 2017;63(1):196–210. doi:10.1373/clinchem.2016.257725
37. Murphy AJ, Woollard KJ, Suhartoyo A, et al. Neutrophil activation is attenuated by high-density lipoprotein and apolipoprotein a-i in in vitro and in vivo models of inflammation. Arterioscler Thromb Vasc Biol. 2011;31(6):1333–1341. doi:10.1161/atvbaha.111.226258
38. Liao XL, Lou B, Ma J, Wu MP. Neutrophils activation can be diminished by apolipoprotein a-i. Life Sci. 2005;77(3):325–335. doi:10.1016/j.lfs.2004.10.066
39. Chen J, Chen X, Xie H, Hei Z, Liu Z, Chen C. Relationship between preoperative neutrophil to high-density lipoprotein ratio and postoperative systemic inflammatory response syndrome in elderly patients: a retrospective cohort study. Lipids Health Dis. 2025;24(1):82. doi:10.1186/s12944-025-02460-6
40. Zhang Y, Han S, Duan Z, et al. Associations of systemic inflammation and systemic immune inflammation with serum uric acid concentration and hyperuricemia risk: the mediating effect of body mass index. Front Endocrinol. 2024;15:1469637. doi:10.3389/fendo.2024.1469637
41. Ghaemi-Oskouie F, Shi Y. The role of uric acid as an endogenous danger signal in immunity and inflammation. Curr Rheumatol Rep. 2011;13(2):160–166. doi:10.1007/s11926-011-0162-1
42. Li D, Yuan S, Deng Y, et al. The dysregulation of immune cells induced by uric acid: mechanisms of inflammation associated with hyperuricemia and its complications. Front Immunol. 2023;14:1282890. doi:10.3389/fimmu.2023.1282890
43. Min SH, Yoon S, Yoon SH, Bahk JH, Seo JH. Randomised trial comparing forced-air warming to the upper or lower body to prevent hypothermia during thoracoscopic surgery in the lateral decubitus position. Br J Anaesth. 2018;120(3):555–562. doi:10.1016/j.bja.2017.11.091
44. Steelman VM, Chae S, Duff J, Anderson MJ, Zaidi A. Warming of irrigation fluids for prevention of perioperative hypothermia during arthroscopy: a systematic review and meta-analysis. Arthroscopy. 2018;34(3):930–942.e932. doi:10.1016/j.arthro.2017.09.024
45. Sessler DI. Complications and treatment of mild hypothermia. Anesthesiology. 2001;95(2):531–543. doi:10.1097/00000542-200108000-00040
46. Pan Y, Zhang Y, Qian X. Effects of air-heated blankets on hypothermia and quality of recovery in patients undergoing radical resection for endometrial cancer: a randomized trial. Medicine. 2025;104(27):e42869. doi:10.1097/md.0000000000042869
47. Zhang J, Deng L, Wang X, Song F, Hou H, Qiu Y. Effect of forced-air warming blanket on perioperative hypothermia in elderly patients undergoing laparoscopic radical resection of colorectal cancer. Ther Hypothermia Temp Manag. 2022;12(2):68–73. doi:10.1089/ther.2021.0010
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.