Back to Journals » Journal of Pain Research » Volume 19
Efficacy of a Modified Three-in-One Puncture Technique for Genicular Nerve Ablation in Knee Osteoarthritis
Authors Lai J ![]() , Wu Y, Xiang Y, Lu G, Zhou X, Wang W, Zuo L, Li YL, Ke C
, Wu Y, Xiang Y, Lu G, Zhou X, Wang W, Zuo L, Li YL, Ke C
Received 27 January 2026
Accepted for publication 23 May 2026
Published 3 June 2026 Volume 2026:19 584559
DOI https://doi.org/10.2147/JPR.S584559
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Jinyu Lai,1,2 Yijun Wu,3 Yong Xiang,2 Guoqiang Lu,2 Xiaofeng Zhou,2 Wenchen Wang,4 Liangyi Zuo,4 Yu-Lan Li,5 Changbing Ke6
1The First School of Clinical Medicine, Lanzhou University, Lanzhou, People’s Republic of China; 2Department of Pain, Taihe Hospital, Hubei University of Medicine, Shiyan, Hubei, People’s Republic of China; 3Department of Radiology, Taihe Hospital, Hubei University of Medicine, Shiyan, Hubei, People’s Republic of China; 4The First School of Clinical Medicine,Hubei University of Medicine, Shiyan, Hubei, People’s Republic of China; 5Department of Anaesthesiology, The First Hospital of Lanzhou University, Lanzhou, People’s Republic of China; 6Institute of Anesthesiology & Pain (IAP), Department of Anesthesiology and Neurosurgery, Taihe Hospital, College of Pharmacy, Hubei University of Medicine, Shiyan, Hubei, People’s Republic of China
Correspondence: Yu-Lan Li, Department of Anaesthesiology, The First Hospital of Lanzhou University, Lanzhou, 730000, People’s Republic of China, Email [email protected] Changbing Ke, Institute of Anesthesiology & Pain (IAP), Department of Anesthesiology and Neurosurgery, Taihe Hospital, College of Pharmacy, Hubei University of Medicine, Shiyan, Hubei, People’s Republic of China, Email [email protected]
Introduction: Conventional approaches targeting the superior medial genicular nerve (SMGN), superior lateral genicular nerve (SLGN), and inferior medial genicular nerve (IMGN) have demonstrated favourable outcomes in knee joint. However, because the inferior lateral genicular nerve (ILGN) and the joint capsule branch are not intervened, radiofrequency ablation of the knee joint cannot completely alleviate knee pain. Our research team has developed an innovative three-in-one puncture technique for the knee, by altering the puncture entry point, simultaneous intervention of three nerves—the SLGN, the inferior lateral genicular nerve, and the joint capsule branch—is enabled. The three-in-one puncture technique has shown preliminarily promising results in patients with knee osteoarthritis (OA).
Methods: We included 57 patients for retrospective analysis. All patients underwent knee nerve radiofrequency ablation(RFA) at the Pain Department of Taihe Hospital, from March 2021 to March 2023. Among them, 30 patients received treatment using the innovative three-in-one method, and 27 received treatment using the traditional method. Follow-up assessments were performed preoperatively and at postoperative Day 1, week 1, month 1, month 3, and month 6 using the numerical rating scale (NRS) for pain, surgical complications, and patient satisfaction.
Results: NRS scores significantly decreased in both groups at all postoperative time points. Intergroup comparisons revealed statistically significant differences in the NRS scores between the three-in-one group and the traditional group at postoperative months 1, 3, and 6 (P< 0.05). No severe adverse events were observed in either group. At 6 months postsurgery, 93.3% of patients in the three-in-one group were satisfied with the outcomes, compared to 74.1% satisfaction in the traditional group.
Conclusion: The three-in-one method significantly reduced chronic peri-knee pain intensity. Long-term follow-up demonstrates its longer-lasting analgesic effects and higher patient satisfaction, indicating substantial clinical applicability.
Plain Language Summary: Traditional treatments targeting the superior medial genicular nerve (SMGN), superior lateral genicular nerve (SLGN), and inferior medial genicular nerve (IMGN) have demonstrated favorable outcomes. However, in our clinical practice, we have observed that pain relief in patients remains incomplete, as the inferior lateral genicular nerve (ILGN) and the joint capsule branch are not addressed. The innovative three-in-one approach enables the simultaneous intervention of three nerves—the SLGN, the inferior lateral genicular nerve, and the joint capsule branch—with a single puncture. This method ensures more thorough and safer radiofrequency management of pain caused by knee osteoarthritis. We hope this minor technical improvement can become the new standard for knee joint radiofrequency.
Keywords: knee osteoarthritis, puncture technique, radiofrequency ablation, common fibular nerve
Introduction
Knee osteoarthritis (KOA) is a degenerative whole-joint disease involving progressive articular cartilage wear alongside subchondral bone remodeling, meniscal degeneration, and biomechanical and biochemical changes of the infrapatellar fat pad. KOA-related degeneration leads to bone-on-bone friction and inflammatory reactions, accompanied by cartilage destruction and osteophyte formation, and may even affect the entire joint.1–3 The most common clinical manifestation of KOA is chronic pain in and around the knee joint, with symptoms prone to recurrence. Functional limitations gradually progress to a loss in independent living ability, and patients with moderate to severe KOA may ultimately become disabled.4 Studies have shown that globally, prevalent cases of OA increased by 113.25%, from 247.51 million in 1990 to 527.81 million in 2019. Among individuals older than 60 years, approximately 10% of men and 13% of women suffer from symptomatic KOA, imaging is an important method for confirming the diagnosis.5–7
Depending on disease severity, treatment options for knee osteoarthritis (KOA) range from lifestyle modifications to surgery.6 Currently, non-pharmacological interventions for knee osteoarthritis (KOA), including therapeutic exercise, weight management, and self-management programs, are strongly recommended. Pharmacological interventions, including topical and oral non-steroidal anti-inflammatory drugs (NSAIDs), are also strongly recommended.8–10 It should be noted that although NSAIDs can provide rapid symptom relief, their duration of action is short and attention should be paid to their potential cardiovascular and gastrointestinal side effects.11 Intra-articular corticosteroid injections are also a relatively recommended treatment option, providing relief for 2 to 10 weeks.8–10 Evidence suggests that genicular nerve block may provide pain relief for approximately 6 weeks,12 studies have shown that radiofrequency ablation (RFA) has the potential to become the preferred conservative treatment for patients with KOA, and an ongoing multicenter randomized controlled trial will further elucidate its clinical value.13,14
RFA achieves long-term pain relief by thermally ablating nociceptive afferent nerves through localised coagulation. In accordance with the approach proposed by Choi et al15 in 2011, targeting three primary nerves innervating the knee joint—the superior medial genicular nerve (SMGN), superior lateral genicular nerve (SLGN), and inferior medial genicular nerve (IMGN). However, because the traditional knee joint radiofrequency method does not intervene in the inferior lateral genicular nerve (ILGN) and the joint capsule branch, knee pain relief remains incomplete, not only because of safety concerns regarding the common fibular nerve injury, but also due to historical limitations in anatomical understanding at the time the conventional approach was established. Our research team improved upon the traditional three-in-one method after studying the anatomical review by Roberts et al16 and conducting clinical practice. The key innovation involves shifting the traditional lateral superior puncture entry point in a posterior manner to target the main articular branch of the common fibular nerve (CFN) via RFA, thereby blocking signal transmission from the SLGN, terminal articular branches, and ILGN. This modification provides more comprehensive pain relief for patients with KOA. We hypothesized that the modified three-in-one method is an accurate, safe, and effective treatment for refractory KOA.
Materials and Methods
This retrospective clinical analysis was approved by the Ethics Committee of Taihe Hospital (Approval No. WZ2025034). All patient data were anonymised, and personal information remained confidential.
Participants
The sample size of this retrospective study was determined based on previous similar clinical studies. Specifically, studies by Wang XC et al17 reported sample sizes ranging from 20 patients per group for comparable KOA treatment outcomes, and we therefore aimed for a similar range, a total of 70 hospitalised patients with chronic knee pain who underwent RFA at the Pain Department of Taihe Hospital from March 2021 to March 2023 were included (Figure 1). All patients exhibited typical signs of KOA, with exclusion criteria including infection, lumbar disc herniation compressing nerves, trauma, or surgical indications. Symptomatology, physical examinations, and imaging findings were consistent with the diagnosis of KOA. All patients signed informed consent forms prior to surgery.
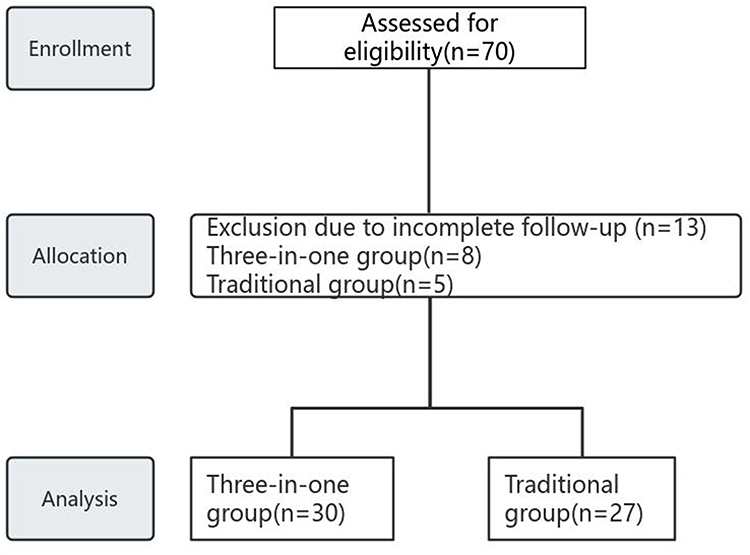 |
Figure 1 Flow chart of patient selection. After excluding patients with incomplete medical records (making follow-up impossible) or other reasons for loss to follow-up, 57 patients were included in the final analysis (30 in the traditional group, 27 in the triple combination group). |
The inclusion criteria were a diagnosis consistent with KOA, the diagnosis of KOA was confirmed by reviewing radiology reports from weight-bearing knee radiographs. Only patients with a documented Kellgren-Lawrence grade of 2 or 3 (moderate osteoarthritis) were included. disease duration >3 months. the patients received only radiofrequency treatment and did not undergo total knee arthroplasty (TKA).
The exclusion criteria were knee pain unexplained by osteoarthritis alone. inability to complete follow-up.
Procedure
Ultrasound-guided localisation of the SMGN, SLGN, and IMGN via a high-frequency linear ultrasound probe (8–12 MHz, Mindray L15-3WU, China) was used to identify the SMGN, SLGN and IMGN near the branches of the knee joint arteries. The SMGN and SLGN are located at the junction between the femoral shaft and the medial/lateral femoral condyles (MFC and LFC), and the IMGN is situated at the junction between the tibial shaft and the medial tibial condyle (MTC). During ultrasound examination, the MFC, MTC, and LFC were first identified in the sagittal plane, after which the corresponding arterial branches were localised to pinpoint the target nerves. Ultrasound-guided conventional scanning method for the SLGN is demonstrated in (Figure 2A and B).
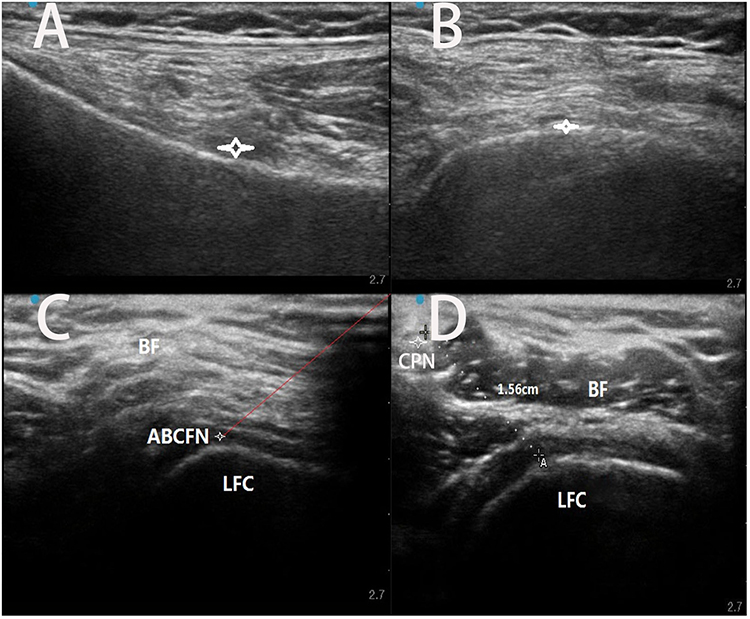 |
Figure 2 The conventional method involves ultrasound imaging of the SLGN (A and B), whereas the three-in-one approach involves ultrasound visualisation of the ABCFN (C and D). Red lines represent the puncture routes; dashed lines represent the safe distance from the puncture target to the common fibular nerve. |
Equipment ultrasound system: Mindray L15-3WU (China) with a high-frequency linear probe (8–12 MHz). RFA device: Cosman RFG-4 (Cosman Medical, USA).
Operative Steps
Patient Preparation: The patient was placed supine on the operating table Intravenous access was established with 0.9% isotonic saline. Electrocardiogram (ECG), pulse rate, oxygen saturation, and noninvasive blood pressure were continuously monitored. Mild sedation was induced with 2 mg midazolam via intravenous injection, and the patient maintained consciousness. Oxygen was administered via nasal cannula at 2–3 L/min. The affected knee was flexed at 20° with a pillow placed under the popliteal fossa.
Puncture Path Design and Sterilisation: The treatment area was disinfected with iodophor and covered with sterile drapes. Local anaesthesia was administered subcutaneously using a mixture of 2.5 mL 2% lidocaine hydrochloride and 2.5 mL 0.9% saline (Xuzhou Lion Pharmaceutical Co., Ltd., China), followed by 2 mL lidocaine (10 mL/vial; Guangzhou Baiyunshan Mingxing Pharmaceutical Co., Ltd., China) to avoid interference with subsequent electrical stimulation. Needle Insertion: A 16-gauge radiofrequency cannula (10 cm long, 2 mm active tip; Beijing Neo Science Co., Ltd., China) was inserted approximately 5 cm lateral to the ultrasound probe, ensuring that the target nerve was centred in the visual field while the visibility of surrounding vascular structures was maintained.
SMGN Localisation and Ablation: The ultrasound probe was positioned sagittally over the MFC to locate the transition zone between the femoral shaft and the MFC. The probe was then rotated to the horizontal plane, and colour Doppler was used to identify the pulsating superior medial genicular artery as the SMGN target. After superficial anaesthesia via 1 mL 1% lidocaine (25G needle), needle insertion was advanced in-plane to the SMGN. Motor stimulation (2 Hz, 1.0–1.5 V) confirmed that no muscle twitching occurred, whereas sensory stimulation (50 Hz, ≤0.5 V) elicited pain or paraesthesia in the target area. Following stimulation, the needle stylet was removed, and 1 mL 2% lidocaine was injected. RFA was initiated using the following parameters: 45 °C (60 s), 60 °C (60 s), 70 °C (60 s), and 80 °C (120 s). The same protocol was applied for the IMGN. This section covers the conventional puncture technique for the medial genicular nerves (SMGN and IMGN). Next, the conventional technique for SLGN puncture is described, followed by our innovative three-in-one modified technique. Based on the conventional method but with an altered puncture location, our modified technique allows for simultaneous and safe treatment of the SLGN, ILGN, and the articular branch of the anterior branch of the common fibular nerve (ABCFN) in a single puncture, providing more comprehensive pain control around the knee joint.
SLGN localisation and modified technique: The traditional approach targeted the SLGN at the midpoint at the junction of the femoral shaft and LFC by identifying the superior lateral genicular artery. However, anatomical variations in the SLGN and failure to address the ILGN often reduce treatment efficacy. In the modified method, the ultrasound probe was moved laterally, parallel to the femoral shaft to locate the ABCFN at the transition between the lateral and posterior femoral cortices (Figure 2C and D) (Figure 3A–C). Direct visualisation of the nerve structure eliminated the reliance on arterial pulsations, which are often undetectable in peripheral vessels. Sensory stimulation (50 Hz, ≤0.5 V) confirmed target accuracy by eliciting pain or paraesthesia, whereas motor stimulation (2 Hz, 1.5–2.0 V) ensured no muscle contraction. This was done to ensure a safe distance between the puncture target and the CPN, thereby avoiding CPN injury during radiofrequency treatment. After validation, pulsed radiofrequency (PRF) was applied to reconfirm the target, followed by application of the following RFA parameters: 60 °C (60 s), 70 °C (60 s), and 80 °C (120 s). This approach simultaneously ablated the SLGN, terminal articular branches, and ILGN of the CFN, enhancing analgesic precision and efficacy.
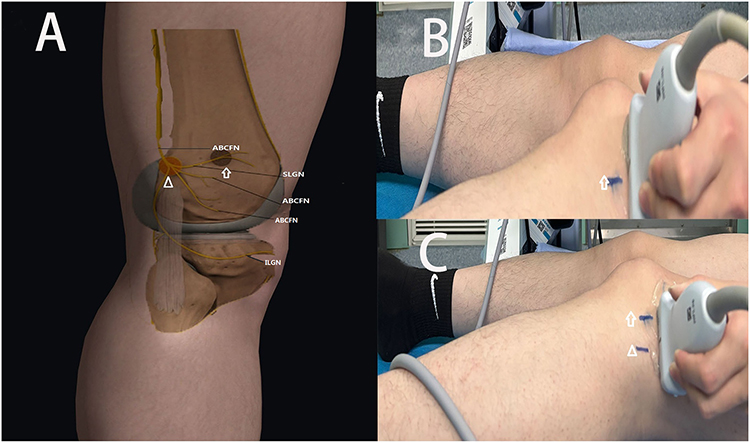 |
Figure 3 (A) Superolateral conventional RFA targets (arrow symbols) and three-in-one RFA ablation sites (triangle symbols) of the knee. (B and C) Probe positioning: conventional vs. three-in-one techniques. |
Postablation Management: Post-RFA, 5 mL anti-inflammatory analgesic solution containing methylprednisolone (40 mg each; Pfizer, Dalian, China) was injected after confirmation of no blood aspiration. The puncture site was covered with sterile dressing and packed with ice to promote closure.
Observation Indicators and Follow-Up
Patient baseline data were collected via the hospital’s electronic medical records system, while outcome data were obtained through telephone and outpatient follow-ups. Follow-up assessments were conducted at the following time points: preoperatively, and at postoperative Day 1, week 1, month 1, month 3, and month 6. The primary outcome measure was the change in pain intensity via NRS assessment, in which pain severity was quantified from 0 to 10 (0: no pain; 1–3: mild pain [no sleep disturbance]; 4–6: moderate pain; 7–10: severe pain [inability to sleep or pain-induced awakening]).18,19 Secondary outcome measures included surgical complications such as postoperative puncture site pain, aggravated pain, hypoaesthesia, localised numbness, bleeding, and infection. Patient satisfaction was evaluated using a 5-point Likert scale: very satisfied, satisfied, neutral, dissatisfied, and very dissatisfied.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism (USA).20 Continuous data are presented as means ± standard deviations ( ) if normally distributed or medians (interquartile ranges) for skewed distributions. Categorical data are expressed as counts and percentages. Normality was assessed using the Shapiro‒Wilk test. For continuous variables, an independent samples t test was used for normally distributed data. The Mann‒Whitney-U test was applied to skewed data. Pretreatment and posttreatment. For the baseline characteristics table, the statistical test results (P values) for between-group comparisons should be provided to demonstrate comparability of key variables between the two groups. Comparisons employed repeated-measures ANOVA or the Friedman test. For categorical variables, differences were analysed using the chi-square test or Fisher’s exact test. A two-tailed P < 0.05 was considered to indicate statistical significance.
) if normally distributed or medians (interquartile ranges) for skewed distributions. Categorical data are expressed as counts and percentages. Normality was assessed using the Shapiro‒Wilk test. For continuous variables, an independent samples t test was used for normally distributed data. The Mann‒Whitney-U test was applied to skewed data. Pretreatment and posttreatment. For the baseline characteristics table, the statistical test results (P values) for between-group comparisons should be provided to demonstrate comparability of key variables between the two groups. Comparisons employed repeated-measures ANOVA or the Friedman test. For categorical variables, differences were analysed using the chi-square test or Fisher’s exact test. A two-tailed P < 0.05 was considered to indicate statistical significance.
Results
Participants and Clinical Characteristics of the Two Groups
Among them, 38 patients received treatment using the innovative three-in-one method, and 32 received treatment using the traditional approach. Because follow-up data could not be obtained, 8 patients in the three-in-one group and 5 patients in the traditional group were excluded from the analysis.
An analysis of demographic characteristics (eg., sex, age, body mass index [BMI]), disease duration and preoperative NRS scores revealed no statistically significant differences between the two groups (Table 1).
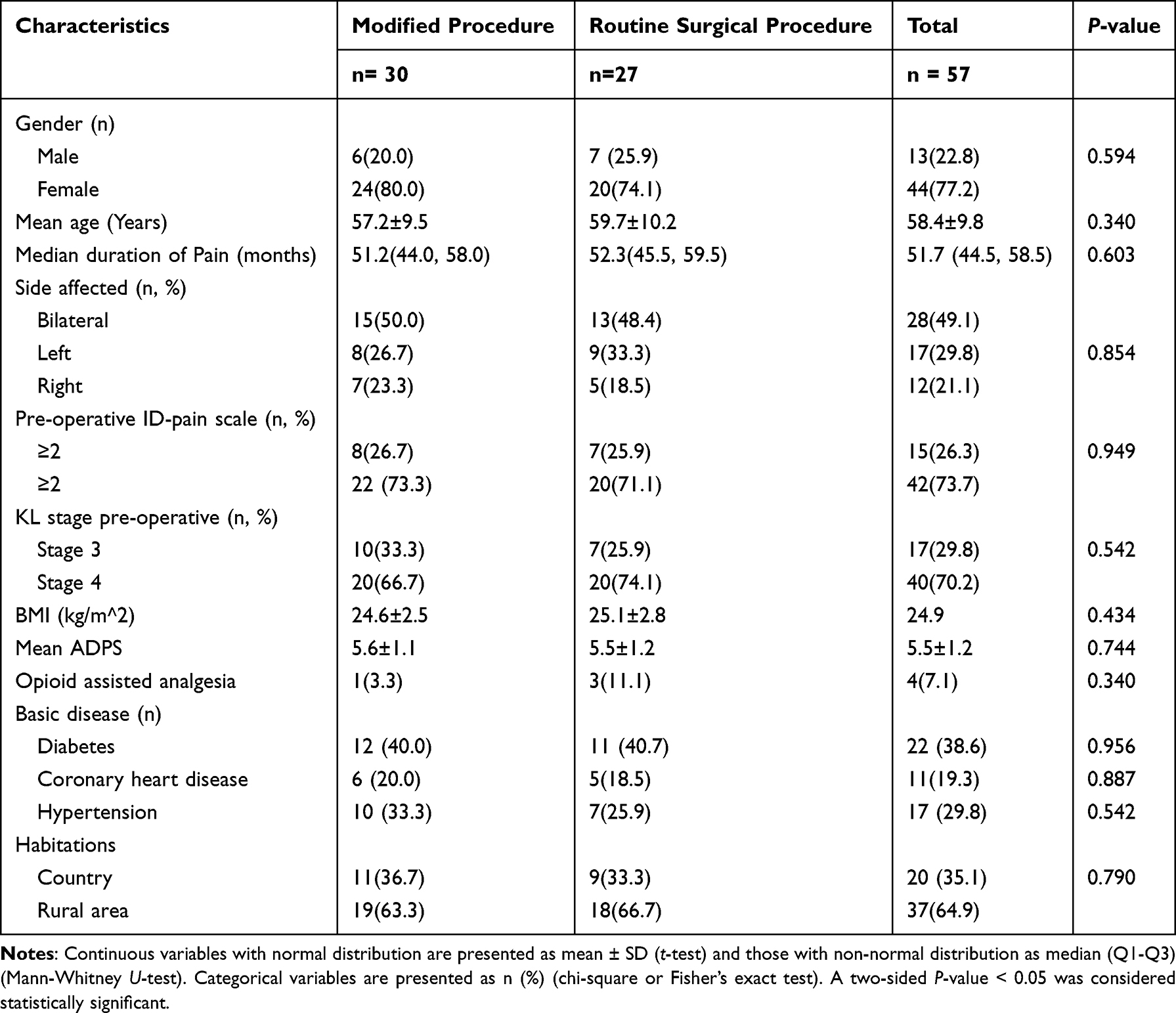 |
Table 1 Demographic and Clinical Characteristics of the Two Groups |
Primary Outcome
Compared with the preoperative baseline scores, both the three-in-one group and the traditional group exhibited significant reductions in NRS scores at postoperative Day 1, week 1, month 1, month 3, and month 6. Notably, the magnitude of the reduction in NRS score was significantly greater in the three-in-one group than in the traditional group at postoperative week 1, month 1, month 3, and month 6 (P<0.05; Figure 4).
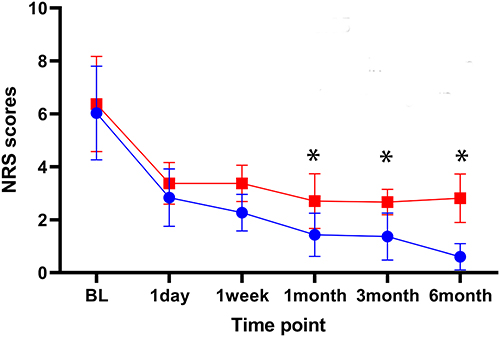 |
Figure 4 Progression of NRS scores over six months illustrating differences between groups. Blue: traditional group; red: three-in-one group. P < 0.05. |
Secondary Outcomes
In the three-in-one group, 2 cases of puncture site pain and 1 case of localised skin ecchymosis were observed postoperatively. No adverse reactions, such as lower limb numbness, weakness, hypoaesthesia, paraesthesia, or neuropathic pain, were reported. In the traditional group, 4 cases of puncture site pain and 3 cases of skin ecchymosis were noted, with no other complications observed. The comparison of complications between the two groups revealed no statistically significant differences (Table 2).
 |
Table 2 The Comparison of Complications Between the Two Groups |
 |
Table 3 The Difference in Satisfaction Rates Between the Two Groups |
At 6 months post-operatively, 28 patients (93.3%) in the three-in-one group reported being “satisfied” or “very satisfied” with the outcomes, while 2 patients (6.7%) considered the effects equivocal. In the traditional group, 20 patients (74.1%) expressed satisfaction, and 7 patients (25.9%) reported equivocal results. The difference in satisfaction rates between the two groups was statistically significant (P<0.05; Table 3).
Discussion
Pain in patients with KOA can occur in any region of the knee joint. Neuropathic pain accounts for approximately 23–40% of pain types and is characterised by limitations in stair climbing, morning stiffness, and discomfort during walking, which can severely impair daily activities.21,22 With the widespread adoption of minimally invasive interventions in chronic pain management, RFA has emerged as an effective solution for refractory or end-stage KOA patients who fail to see results from conventional therapies or are ineligible for surgery.14 RFA delivers controlled electrical currents to nociceptive nerve fibres, inducing thermal coagulation to disrupt pain signal transmission to the central nervous system, thereby achieving long-term pain relief.22,23 Notably, these targeted nerve fibres are typically not involved in somatic motor functions.
Precise identification of knee joint innervation is critical for preoperative planning and prognostic evaluation. According to Hilton’s law, nerves innervating a joint also supply the muscles that move the joint and the overlying skin. Sensory innervation of the knee involves the articular branches of the FN, CFN, saphenous nerve (a branch of the FN), tibial nerve, and obturator nerve. Traditional RFA for treating KOA focuses on three primary nerves—SMGN, SLGN, and IMGN—which have been shown to provide short-term pain and functional improvement.24,25 Roberts et al16 identified the terminal articular branches of the ABCFN innervating the joint capsule, along with the SLGN and ILGN, during cadaveric dissection. Building on these findings, our team improved the three-in-one technique by modifying the lateral superior puncture approach. The target site was shifted posteriorly to the transition zone between the lateral and posterior femoral cortices, allowing ultrasound-guided precise ablation of the main articular branch of the CFN. This simultaneously blocks pain transmission from the SLGN, ILGN, and terminal articular branches.
Our retrospective analysis of patients treated with the three-in-one method (2021–2023) showed significantly greater improvements in NRS scores at all postoperative follow-up intervals (from postoperative day 1 to month 6) compared with the traditional method. This finding suggests that the three-in-one technique provides more effective and sustained pain relief after knee radiofrequency treatment.
The superior efficacy may be explained by the more comprehensive blockade of sensory nerves innervating the knee joint. Given the complex innervation of the knee, the traditional technique does not adequately address pain in the inferolateral region or the joint itself, which likely contributes to its inferior pain control. In contrast, the three-in-one technique targets the main articular branch of the common fibular nerve (ABCFN), thereby simultaneously blocking the joint capsule branch, the ILGN, and the SLGN.
The three-in-one technique offers distinct advantages: . precision: direct ablation of the main articular branch of the CFN achieves simultaneous targeting of the joint capsule branch, ILGN, and SLGN, surpassing the fragmented approach of traditional methods. technical refinement: High-resolution ultrasound visualisation and operator expertise minimise procedural failure risks. Safety: Intraoperative adjustments (eg., anteroposterior scanning of the lateral knee) ensure real-time visualisation of the CFN, maintaining a safe distance (~1.56 cm) from the ablation site. Combined with sensory/motor stimulation tests, this also prevents CFN injury.
Throughout follow-up, the three-in-one group exhibited significantly greater pain reduction than the traditional group did, with no severe adverse events (eg., lower limb numbness, weakness, or neuropathic pain) in either group. The higher patient satisfaction in the three-in-one group (93.3% vs. 74.1%, P<0.05) suggests that this approach may offer clinical advantages in terms of patient-reported outcomes, warranting further investigation.
This study has several limitations. First, the exclusive use of NRS may not fully capture functional outcomes; inclusion of more comprehensive scores, such as KOOS, would strengthen the evaluation. Second, the proposed mechanism of action does not fully incorporate the anatomical variability of knee innervation. Third, the clinical applicability of the technique is not clearly defined, particularly regarding patient selection and its role relative to established treatment strategies. Fourth, this was a retrospective, single‑center study, which may introduce selection bias and limit the generalizability of the findings. Fifth, multivariate regression analysis was not performed, which may limit the ability to control for potential confounding factors. Additionally, the small sample size and short follow‑up further limit the generalizability of the results. Future prospective, multicenter studies with larger sample sizes, longer follow‑up periods, standardized assessments, and multivariate analyses are warranted to address these limitations.
Conclusion
Compared with traditional radiofrequency methods for the knee, the modified triple-one puncture technique enables more comprehensive RFA of the sensory nerves around the knee joint under full ultrasound guidance. Compared with conventional radiofrequency methods, this novel approach demonstrates superior long-term analgesic efficacy and enhanced procedural safety. We preliminarily validated the advantages and efficacy of this method, and no significant complications were observed. Therefore, this innovative three-in-one approach holds promise as a prospective method for pain management in patients with chronic knee pain.
Abbreviations
Radiofrequency ablation (RFA); superior medial genicular nerve (SMGN); superior lateral genicular nerve (SLGN); intermediate genicular nerve (IMGN); inferior lateral genicular nerve (ILGN); knee osteoarthritis (OA); numerical rating scale (NRS).
Data Sharing Statement
We agree to share all the data for this article. The data that support the findings of this study are available from the first corresponding author, Professor Yulan Li, upon reasonable request.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki. This study was a retrospective clinical analysis and was approved by the Ethics Committee of Taihe Hospital, Hubei University of Medicine (Approval No. WZ2025034). In this case, the patients consented to share their deidentified medical records for educational and exchange purposes.
Consent for Publication
We all agree to share all the data for this article. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
Thank you to Dr. Yu-Lan Li for providing writing and operational guidance, and to Dr. Xiang Yong for providing technical guidance.
Funding
This work was supported by the Guiding Research Project of the Shiyan Science and Technology Bureau (24Y073) and Jointly supported by the Hubei Provincial Natural Science Foundation and the Shiyan Innovation Development Joint Fund of China (JCZRLH202600029).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pettenuzzo S, Berardo A, Belluzzi E, et al. Mechanical insights into fat pads: a comparative study of infrapatellar and suprapatellar fat pads in osteoarthritis. Connect Tissue Res. 2025;66(4):272–10. doi:10.1080/03008207.2025.2502591
2. Vincent TL, Alliston T, Kapoor M, Loeser RF, Troeberg L, Little CB. Osteoarthritis pathophysiology: therapeutic target discovery may require a multifaceted approach. Clin Geriatr Med. 2022;38(2):193–219. doi:10.1016/j.cger.2021.11.015
3. Qiu L, Alhaskawi A, Moqbel SAA. Osteoarthritis: multitissue pathology, molecular mechanisms, clinical management, and emerging precision and regenerative therapies. Front Pharmacol. 2026;16:1697192. doi:10.3389/fphar.2025.1697192
4. Thirumaran AJ, Deveza LA, Atukorala I, D.j H. Assessment of pain in osteoarthritis of the knee. J Pers Med. 2023;13:1139. doi:10.3390/jpm13071139
5. Long H, Liu Q, Yin H, et al. Prevalence trends of site-specific osteoarthritis from 1990 to 2019: findings from the global burden of disease study 2019. Arthritis Rheumatol. 2022;74(7):1172–1183. doi:10.1002/art.42089
6. Favreau H, Chennen K, Feruglio S, et al. Knee osteoarthritis diagnosis: future and perspectives. Biomedicines. 2025;13(7):1644. doi:10.3390/biomedicines13071644
7. Sukerkar PA, Doyle Z. Imaging of osteoarthritis of the knee. Radiol Clin North Am. 2022;60(4):605–616. doi:10.1016/j.rcl.2022.03.004
8. Kolasinski SL, Neogi T, Hochberg MC, et al. American college of rheumatology/arthritis foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2020;72(2):149–162. doi:10.1002/acr.24131
9. Osteoarthritis in Over 16s: Diagnosis and Management. London: National Institute for Health and Care Excellence; 2022.
10. Brophy RH, Fillingham YA. AAOS clinical practice guideline summary: management of osteoarthritis of the knee (Nonarthroplasty). J Am Acad Orthop Surg. 2022;30(9):e721–e729. doi:10.5435/JAAOS-D-21-01233
11. Davis A, Robson J. The dangers of NSAIDs: look both ways. Br J Gen Pract. 2016;66(645):172–173. doi:10.3399/bjgp16X684433
12. Shanahan EM, Robinson L, Lyne S, et al. Genicular nerve block for pain management in patients with knee osteoarthritis: a randomized placebo-controlled trial. Arthritis Rheumatol. 2023;75(2):201–209. doi:10.1002/art.42384
13. Liu Y, Zhao X, Zhou J, Dou C, Zhang Y. Radiofrequency ablation therapy for knee osteoarthritis: a systematic review and meta-analysis. Terapia de ablación por radiofrecuencia para la osteoartritis de rodilla: revisión sistemática y metaanálisis. Cir Cir. 2024;92(4):456–468. doi:10.24875/CIRU.23000395
14. Wit PR, Beek RV, Schokker M, et al. Genicular nerve radiofrequency ablation, phenol neurolysis or conservative medical management in patients with knee osteoarthritis: protocol for the RADIOPHENOL randomised controlled multicentre trial with three parallel groups. BMJ Open. 2025;15(7):e094576. doi:10.1136/bmjopen-2024-094576
15. Choi WJ, Hwang SJ, Song JG, et al. Radiofrequency treatment relieves chronic knee osteoarthritis pain: a double-blind randomized controlled trial. Pain. 2011;152(3):481–487. doi:10.1016/j.pain.2010.09.029
16. Roberts SL, Stout A, Dreyfuss P. Review of knee joint innervation: implications for diagnostic blocks and radiofrequency ablation. Pain Med. 2020;21(5):922–938. doi:10.1093/pm/pnz189
17. Wang XC, Sun YZ, Ma JY, et al. Clinical observation of intra-articular pulsed radiofrequency treatment for knee osteoarthritis. Chin J Pain Med. 2021;27(10):785–788.
18. National health commission of the people’s republic of china. clinical practice guideline for cancer pain management. J clin oncol. 2018;23(10):937–944.
19. Serlin RC, Mendoza TR, Nakamura Y, Edwards KR, Cleeland CS. When is cancer pain mild, moderate or severe? Grading pain severity by its interference with function. Pain. 1995;61(2):277–284. doi:10.1016/0304-3959(94)00178-H
20. One-Way ANOVA Followed by Dunnett’s Multiple Comparisons Test Was Performed Using GraphPad Prism Version 11.0.0 for Windows. Boston, Massachusetts USA, Available from: https://www.graphpad.com:GraphPad Software.
21. Geng R, Li J, Yu C, et al. Knee osteoarthritis: current status and research progress in treatment (Review). Exp Ther Med. 2023;26(4):481. doi:10.3892/etm.2023.12180
22. Strand NH, Hagedorn JM, Dunn T, et al. Advances in radiofrequency ablation: mechanism of action and technology. Ann Palliat Med. 2024;13(4):1028–1034. doi:10.21037/apm-23-457
23. Idahor CO, Mokobia S, Ogbonna N, et al. Radiofrequency ablation for chronic pain: mechanistic insights and emerging innovations. Cureus. 2025;17(12):e99056. doi:10.7759/cureus.99056
24. Hébert-Blouin MN, Tubbs RS, Carmichael SW, Spinner RJ. Hilton’s law revisited. Clin Anat. 2014;27(4):548–555. doi:10.1002/ca.22348
25. Tran J, Peng PWH, Lam K, Baig E, Agur AMR, Gofeld M. Anatomical study of the innervation of anterior knee joint capsule: implication for image-guided intervention. Reg Anesth Pain Med. 2018;43(4):407–414. doi:10.1097/AAP.0000000000000778
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cooled Radiofrequency Ablation Provides Prolonged Pain Relief Compared to Traditional Radiofrequency Ablation: A Real-World, Large Retrospective Clinical Comparison from a Single Practice
Kapural L, Minerali A, Sanders M, Matea M, Dua S
Journal of Pain Research 2022, 15:2577-2586
Published Date: 31 August 2022