Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Efficacy and Safety of Neuromodulation Interventions for Autism Spectrum Disorders with Comorbidities: A Systematic Review
Authors Wu X ![]() , Huangfu J, Zhang W, Hu Y, Yang L, Wei J, Chen Z, Geng S, Xue S, Yi P, Mao Y, Qian D, Wang X, Zhang P
, Huangfu J, Zhang W, Hu Y, Yang L, Wei J, Chen Z, Geng S, Xue S, Yi P, Mao Y, Qian D, Wang X, Zhang P ![]() , Long H
, Long H
Received 4 September 2025
Accepted for publication 18 November 2025
Published 4 December 2025 Volume 2025:21 Pages 2759—2782
DOI https://doi.org/10.2147/NDT.S565304
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Xiaoyan Wu,1– 3,* Junnan Huangfu,1– 3,* Wanghao Zhang,1– 3 Yuchen Hu,1– 3 Lu Yang,1,2 Jiezuo Wei,1,2 Zijian Chen,1– 3 Shiqin Geng,1,2 Shuaishuai Xue,1,2 Peiyao Yi,1,2 Yangqi Mao,1,2 Dadi Qian,1,2 Xingqin Wang,1,2 Peidong Zhang,1,2 Hao Long1,2
1Department of Neurosurgery, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 2Institute of Brain Diseases, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 3The First Clinical Medical College, Southern Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peidong Zhang, Department of Neurosurgery, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China, Email [email protected] Hao Long, Department of Neurosurgery, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China, Email [email protected]
Purpose: Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by impairments in social communication and stereotyped, repetitive behaviors or interests. Neuromodulation interventions have been employed in ASD, which can improve behavioral and cognitive outcomes in ASD, especially relief of comorbidities, as shown in preliminary evidence. However, their efficacy and safety remain unclear owing to the lack of high-quality synthetic evidence. We aim to systematically evaluate the therapeutic potential of neurostimulation in ASD and explore its underlying mechanisms.
Patients and Methods: A narrative synthesis of peer-reviewed literature from 2000 to 2025 was conducted, sourced from the PubMed, Web of Science, and Cochrane Library. Seventy-three relevant studies were identified in this paper.
Results: Up to date, noninvasive brain stimulation has become a potential intervention to reduce autism-related symptoms and improve neuropsychological function in ASDs, while a marked alleviation of comorbidities including aggression, anxiety and epilepsy was observed following invasive brain stimulation interventions. Both of the neuromodulation techniques are believed to be safe and well-tolerated.
Conclusion: Neuromodulation interventions could be a hopeful option to improve patients’ symptoms and control comorbidities of ASD. Further high-quality trials should be conducted to optimize long-term prognosis of ASD.
Keywords: autism spectrum disorder, comorbidities, noninvasive brain stimulation, invasive brain stimulation
Introduction
As a neurodevelopmental disorder characterized by impairments in social communication and stereotyped, repetitive behaviors or interests, autism spectrum disorder (ASD) affects approximately 1/100 children around the world.1 Together with these core symptoms, co-occurring psychiatric or neurological disorders are more common in people with ASD, of which attention deficit hyperactivity disorder (ADHD), sleep difficulties, anxiety, depression, and epilepsy are fairly prevalent. Almost 70% of people with ASD experience at least one comorbid psychiatric disorder, whereas nearly 40% individuals may have two or more psychiatric disorders.2 These coexisting disorders significantly contribute to reduced quality of life and increased mortality of ASDs.
The significant economic effect of ASDs emphasizes the need to explore effective interventions. Now, the major treatments of ASD are based on psychotherapy, such as early intensive behavioral intervention (EIBI), cognitive behavioral therapy (CBT), etc., while only small-to-medium effects of improvement have been achieved.3 However, recent decades have witnessed a growing interest in neurostimulation techniques in the treatment of ASD. The stimulation techniques can be broadly divided into noninvasive brain stimulation (NIBS) and invasive brain stimulation (IBS). The procedures of NIBS are safe and well-tolerated and can be performed in ambulatory settings without requiring sedation. On the other hand, IBS techniques are neurosurgical procedures that implant pulse generators connected to the vagus nerve or brain structures.
In the neurobiology of ASD, it is believed that alterations in whole-brain connectivity during early neurodevelopment contribute to neuropsychiatric symptoms.4 Some neuroimaging studies have observed abnormal growth in the cortical surface between 6 and 12 months of age and greater brain volume between 12 and 24 months of age in children who were later diagnosed with autism.5 Neuropathologic studies have demonstrated the presence of an excitation-inhibition (E/I) imbalance within the cerebral cortex in ASDs.6 Both NIBS and IBS could induce neural activation and modify abnormal brain activity by the use of electricity, which aligns with the pathological neuroplasticity in children with ASD. Additionally, as the major excitatory neurotransmitter in central nervous system, glutamate may be a key neurotransmitter involved in ASD, and abnormal increased levels of the amino acid in ASD patients have been described.7 Multiple Ankyrin repeat domains 3 (SHANK3), a post-synaptic protein at excitatory glutamatergic synapses, plays a pivotal role in ASD symptoms,8 and the whole-cell voltage clamp recordings of SHANK3 mutant mice showed that the disruption of the E/I balance may generally be attributed to an enhancement of the glutamatergic activity.9 In 2021, Moxon-Emre et al found that rTMS treatment course could modulate glutamatergic levels in adults with ASD, which aligned with the hyperglutamate theory of ASD.10
Due to a lack of high-quality synthetic evidence, the application of neuromodulation interventions has not been recommended in the guidelines for ASD. Therefore, a systematic review of the up-to-date literature on the therapeutic uses of NIBS and IBS in ASD is still warranted. The primary objective of this systematic review is to evaluate the therapeutic efficacy of NIBS and IBS on core ASD symptoms and common comorbidities in ASDs, and the secondary objective is to assess the safety and tolerability of the interventions.
Materials and Methods
Study Eligibility
We conducted a systematic review of peer-reviewed international literature, utilizing the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.11 A comprehensive literature search was conducted on studies published from January 2000, to December 2024 (updated May 2025), in the PubMed, Web of Science, and Cochrane Library databases. Search terms indicated the diagnoses and interventions of interest: [autism OR autism spectrum disorder OR ASD OR autistic disorder OR autistic spectrum disorder OR Asperger’s syndrome] AND [Transcranial Direct Current Stimulation OR tDCS OR Transcranial Electrical Stimulation OR Transcranial Alternating Current Stimulation OR Anodal Stimulation tDCS OR Cathodal Stimulation tDCS OR Repetitive Transcranial Electrical Stimulation]; [autism OR autism spectrum disorder OR ASD OR autistic disorder OR autistic spectrum disorder OR Asperger’s syndrome] AND [repetitive Transcranial Magnetic Stimulation OR rTMS OR TMS OR Transcranial Magnetic Stimulation]; [autism OR autism spectrum disorder OR ASD OR autistic disorder OR autistic spectrum disorder OR Asperger’s syndrome] AND [electroconvulsive therapy OR ECT OR Electroshock Therapy OR Electric Convulsive Therapy OR Electric Shock Therapy]; [autism OR autism spectrum disorder OR ASD OR autistic disorder OR autistic spectrum disorder OR Asperger’s syndrome] AND [Vagus nerve stimulation OR VNS OR Vagal Nerve Stimulation]; [autism OR autism spectrum disorder OR ASD OR autistic disorder OR autistic spectrum disorder OR Asperger’s syndrome] AND [Deep brain stimulation OR DBS].
Inclusion Criteria
Articles were included if they met the following criteria: (1) original research in a peer-reviewed journal, (2) the study sample included individuals with ASD, and (3) investigated noninvasive or invasive neurostimulation interventions as a therapeutic modality in the management of ASD via open-label trials, controlled trials, or crossover studies.
Exclusion Criteria
Articles were excluded if they met the following exclusion criteria: (1) focused on other disorders that were not ASD, (2) were published in a language other than English, (3) did not include interpretable data, or (4) performed a literature review or meta-analysis.
Screening and Selection of Studies
According to PRISMA guidelines, the literature was collected, read, screened, and extracted independently by two persons, following the principles of extraction. We assessed the reference lists of the retrieved papers to ensure that all relevant articles were included in our review and excluded additional articles that did not meet the inclusion criteria.
Quality Assessment
The selected studies were appraised for quality using the Joanna Briggs Institute (JBI) critical appraisal checklist.12 The quality appraisal stage was done independently by two authors. The articles were then scored based on their quality scores and classified as having a quality score of less than 50% (low-quality studies), 50% to 75% (moderate-quality studies), or greater than 75% (high-quality studies). Due to the limited number of relevant reports, no studies were excluded based on their quality ratings. However, the quality ratings were used to guide the interpretation of the results.
Data Extraction and Synthesis
Two authors collaborated on each selected article. In cases of disagreement, the decision was made based on the opinion of a third member in the research team. Extracted contents include basic characteristics of the included literature, such as author, year, sample size, age, diagnosis, study design, intervention measures, procedure, outcome, and safety assessment indicators. Extracted data from the studies were analyzed through a narrative synthesis to explore the neuromodulation options for core symptoms and ASD-related comorbidities given the inclusion of a variety of study designs. We synthesized the trials grouped by the types of intervention (NIBS including TMS, tDCS, ECT vs IBS including DBS, VNS). Tables were constructed based on the information extracted, which include key study characteristics such as population, diagnosis, study design, intervention parameters, sham stimulation methods and outcomes.
Results
Study Characteristics
A total of 1722 records were retrieved through electronic and manual searches. Figure 1 shows a schematic overview of the study selection process. After removing duplicate results and excluding studies with irrelevant title and abstract, the results were reduced to 185. The rest of the studies were assessed for eligibility, and a further 112 studies were excluded for reasons indicated in the PRISMA flow diagram. Finally, 73 articles were included and analyzed in this study after excluding those records that did not fulfill the inclusion criteria. Of the total 73 articles, 57 studies primarily described NIBS interventions, and 16 studies described IBS interventions. 27/73 of the included articles were sham-controlled trials. Others included case reports or reviews of case series. The characteristics, design, technical parameters, and outcomes of the included studies are shown in Tables 1–4. The quality ratings of included studies are shown in Appendix 1, Appendix 2 and Appendix 3 in the Supplementary Material. The 25 selected studies were appraised for quality by utilizing the JBI critical appraisal checklist for randomized control trials (RCTs), 22 selected studies were appraised for quality and by utilizing the JBI critical appraisal checklist for case reports, 22 selected studies were appraised for quality by utilizing the JBI critical appraisal checklist for quasi-experimental studies. The majority of the studies (81%) were of a high-quality, 13 studies (19%) were of a moderate-quality. None of the studies were eliminated based on methodological quality evaluation outcomes as the authors wanted to compile a comprehensive list of all potentially effective therapeutic managements.
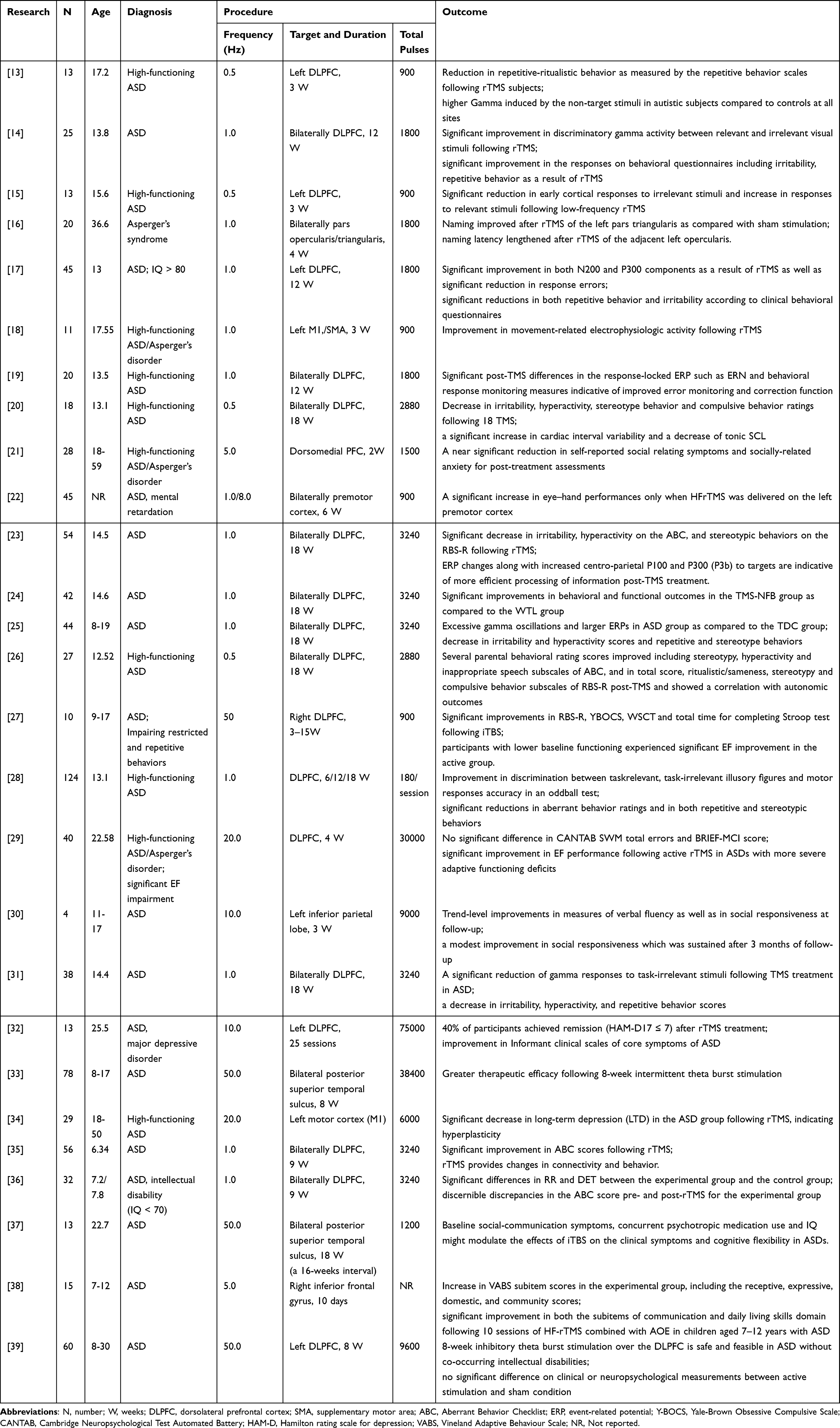 |
Table 1 Qualitative Summary of TMS Studies with Waitlist or Sham Controls for ASD |
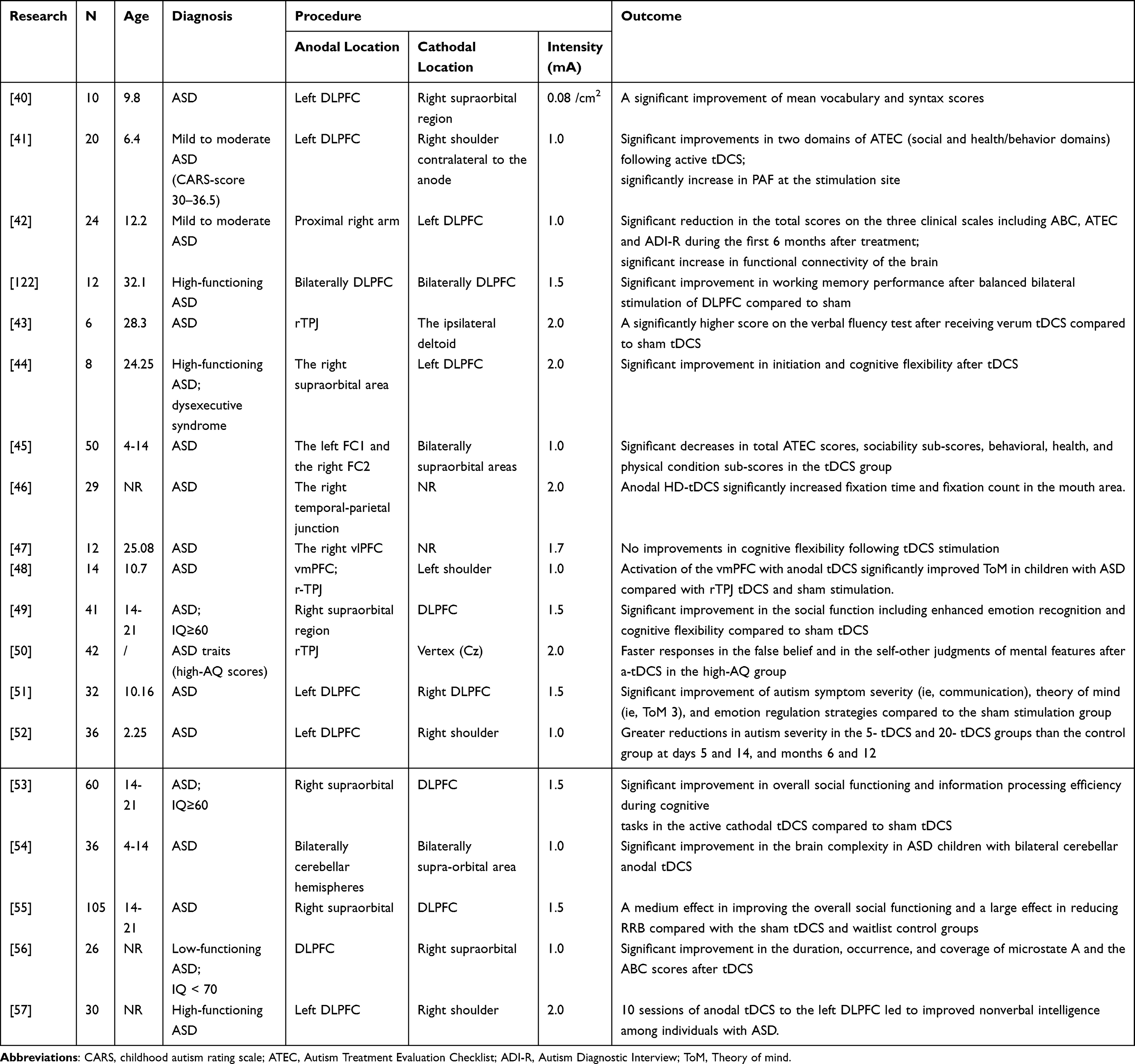 |
Table 2 Qualitative Summary of tDCS Studies with Waitlist or Sham Controls for ASD |
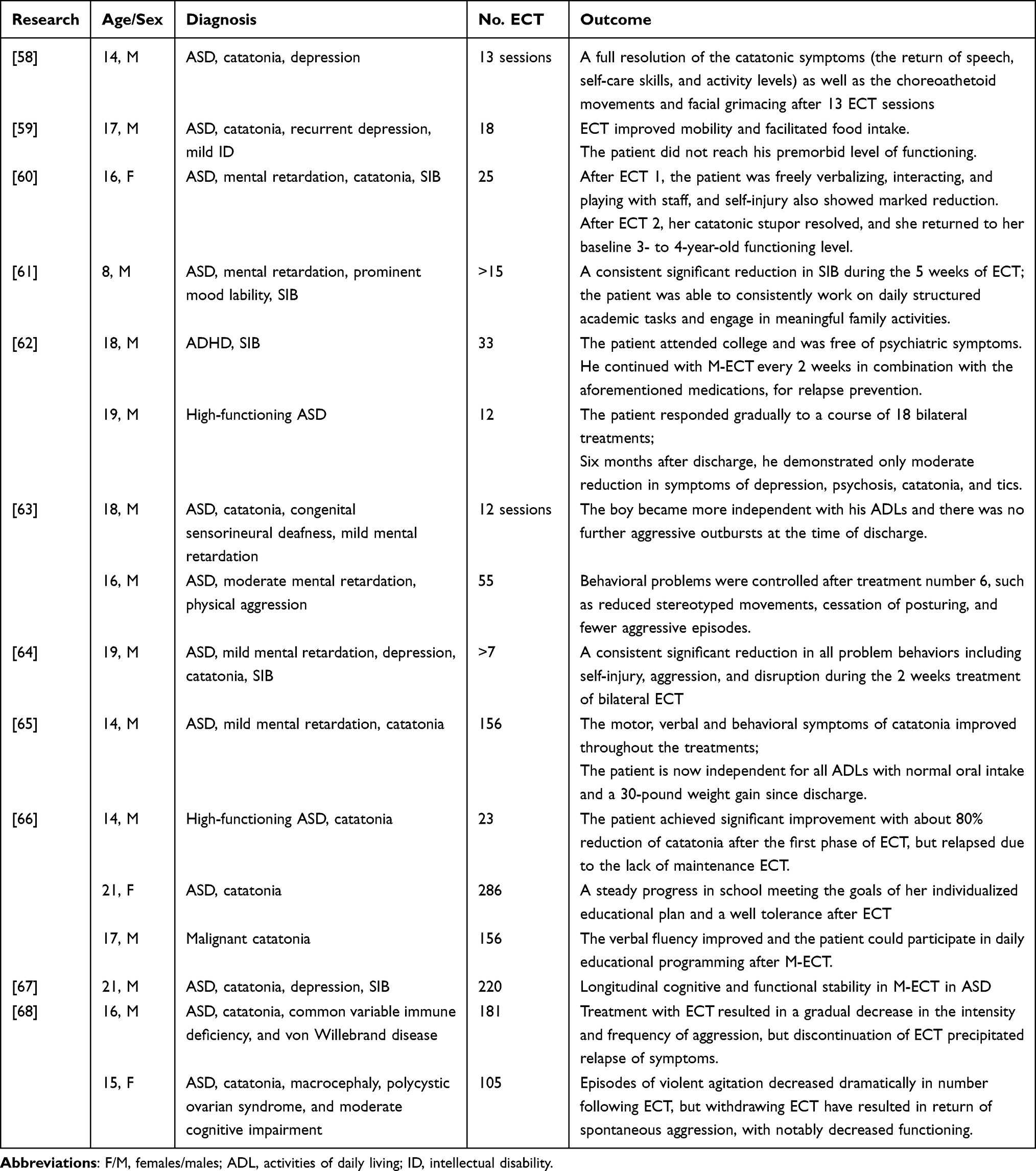 |
Table 3 Qualitative Summary of ECT Studies for ASD |
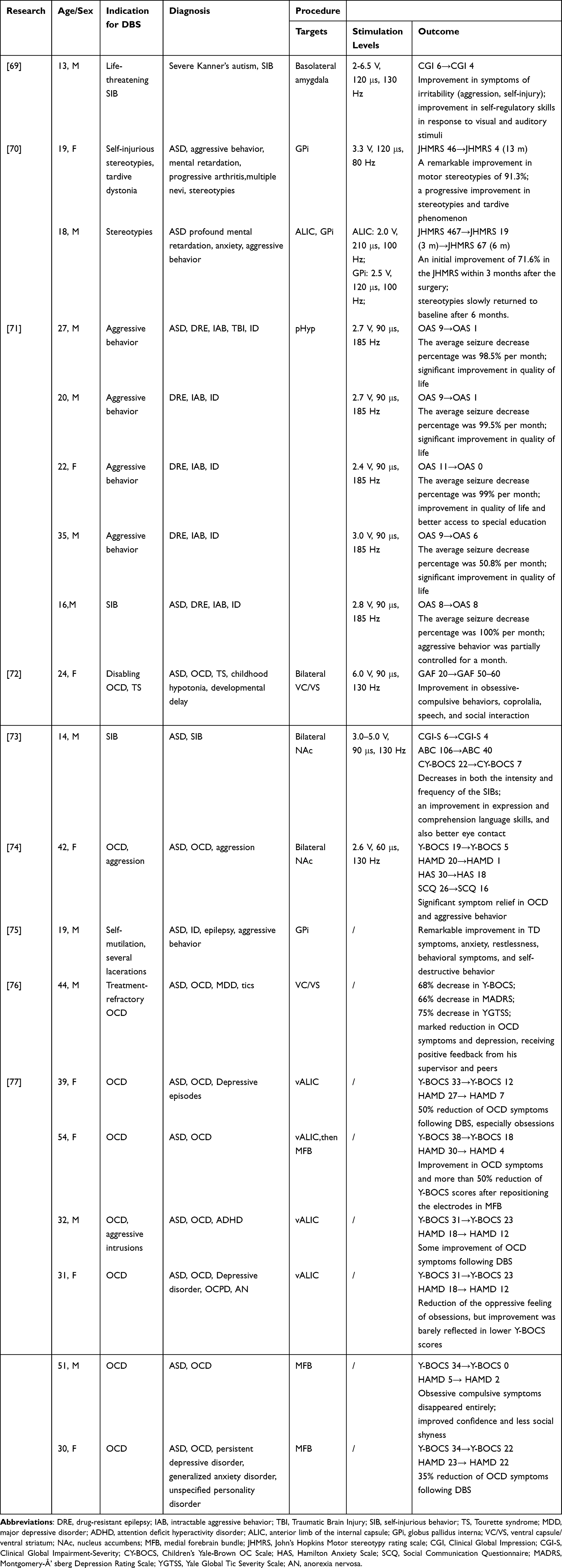 |
Table 4 Qualitative Summary of DBS Studies for ASD |
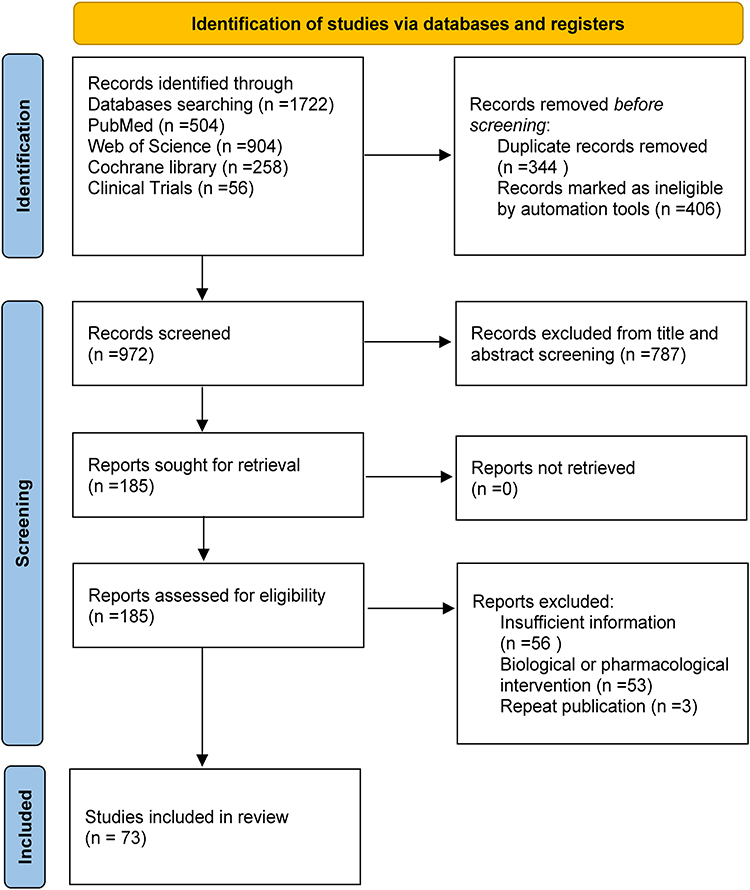 |
Figure 1 PRISMA 2020 flow diagram for systematic reviews which included searches of databases. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71T. |
Regarding the stimulation parameters of TMS and tDCS, there was a large variability. In the NIBS technique, most studies (31/46) chose the left/right dorsolateral prefrontal cortex (DLPFC) as the stimulation target. Four studies employed theta burst stimulation (TBS) protocols, while the remaining 23 studies utilized more conventional rTMS approaches. The main stimulation frequencies were set at 0.5−1 Hz, and the duration of the procedure lasted from 2 to 18 weeks.
On the other hand, IBS, including DBS and VNS, mainly targeted improving the therapeutic effects of comorbidities or specific symptoms in ASD, such as drug-resistant epilepsy and self-injurious behaviors (SIB). A total of seven studies of VNS all focused on patients with both epilepsy and ASD. In 19 cases that were reported in 9 DBS literatures reviewed, validated targets in DBS contain the posterior hypothalamus (pHyp; 5/19),71 ventral anterior limb of the internal capsule (vALIC; 3/19),77 nucleus accumbens (NAc; 2/19),73,74 globus pallidus internus (GPi; 2/19),70,75 medial forebrain bundle (MFB; 2/19),77 ventral capsule and ventral striatum (VC/VS; 2/19),76 anterior limb of the internal capsule (ALIC; 1/19),70 and basolateral amygdala (1/19).69
Efficacy
Noninvasive Neurostimulation
TMS
TMS is placed on the human scalp to activate the targeted cortex using rapidly changing extracranial magnetic fields.78 The size and direction of the effect can be controlled by varying the frequency and number of stimulation sessions. It is believed that low-frequency repetitive TMS (LF-rTMS, ≤1 Hz) reduces cortical excitability through the activation of inhibitory GABAergic interneurons.79 This effect was observed in a series RCT studies and also supported by some open-label studies. In RCTs, Baruth et al assessed the effect of twelve 1 Hz rTMS, which showed significant improvement in discriminatory gamma activity at the early stages of visual processing in ASD.14 Fecteau et al randomly assigned twenty adults to receive four sessions of 30-min 1 Hz of both active and sham rTMS stimulation over Broca’s area, and naming skills improved after rTMS in Asperger’s syndrome participants. Another early open-label study by Sokhadze et al (2009) found that 0.5 Hz of rTMS could improve the inappropriate neuron activation in response to non-target items and reduce repetitive-ritualistic behavior in ASDs.13 In follow-up studies by Sokhadze et al, individuals with ASD who received 0.5 Hz rTMS over the DLPFC showed improvements in executive functioning, error correction, and a reduction in repetitive and stereotypical behaviors.15 In 2012, by measuring event-related potentials (ERP) indices during attentional processing in 25 participants with ASD, they confirmed a significant improvement at early and later stages (eg, N200, P300) of visual processing as a result of rTMS, making it possible to deal with visuoperceptual abnormalities in autism.17 Regarding how to choose the appropriate treatment sessions, Sokhadze et al assigned 124 high functioning ASD children using randomization to receive different number of weekly 1 Hz rTMS sessions (ie, 6, 12, and 18), and argued that the behavior improvements increased with the total number of sessions to some extent, and 18 sessions best facilitate cognitive control and attention.28
As a patterned rTMS, intermittent theta burst stimulation (iTBS) is capable of producing a robust physiological plasticity effect in the human cortex.80 Compared to rTMS, iTBS is shorter in duration and lower in intensity, making it a more convenient choice for sensitive populations, such as children. Ni et al conducted a series of RCTs to evaluate the feasibility and efficacy regarding iTBS. In 2021, they applied iTBS over the bilateral posterior superior temporal sulcus and found that longer courses of iTBS (8 weeks in total) may produce greater efficacy on core symptoms and social cognitive performance in children with ASD.33 However, they also demonstrated that the impacts of multi-session iTBS on clinical symptoms may be affected by the psychotropic medication use and baseline autistic deficits.37,39 In a case-control pilot study, Pedapati et al found a difference during the post-iTBS time course of M1 excitability between youth with ASD and their healthy peers, and this might become a potential physiological biomarker of cortical plasticity in ASDs.81 Another open-label study in 2018 demonstrated improvements in restricted, repetitive behaviors, compulsions, and neurocognitive functioning following 15 sessions of iTBS targeting the right DLPFC in individuals with ASDs.27
Behavioral deficiencies, including characteristic symptoms of ASD, motor dysfunction, abnormal reactions to the sensory environment, and visuo-perceptual abnormalities, are common in ASD. Enticott et al conducted a double-blind RCT to demonstrate that deep rTMS to bilateral dmPFC improves social-related impairments.21 A recent study demonstrated that rTMS could improve movement-related cortical potentials (MRCPs) and eye-hand performance in ASDs.18,22 Decreasing sympathetic arousal indices has a positive correlation with repetitive and stereotypical behaviors of ASD, whereas rTMS could reverse the effect by increasing parasympathetic tone. Casanova et al found that 18 sessions of low-frequency rTMS resulted in increased cardiac vagal control and decreased sympathetic arousal, which had positive and negative correlations with repetitive and stereotyped behaviors, respectively.20,26 Otherwise, Wang et al proposed that 12 sessions of weekly inhibitory low-frequency rTMS, bilaterally applied to the DLPFC, will improve autonomic balance.82
rTMS could also be a potential therapy for individuals with ASD and comorbidities, which were validated through a series of pilot studies. Gwynette et al in 2010 concluded that 40% of participants with ASD and major depressive disorder achieved remission after rTMS targeting the left DLPFC.32 Another Japanese research applied the iTBS treatment targeting the left DLPFC on ASDs with depressive symptoms, and the remission rate was 67%.83 In 2022, 32 autistic children with intellectual disability who participated in a pilot study to receive 1 Hz rTMS treatment reported a positive influence on brain activity and behaviors.36
In recent years, several novel therapies have been developed. In 2023, an RCT study conducted on 15 children with ASD, and combined high-frequency rTMS with action observation and execution (AOE) treatment, which has recently emerged as a mechanism for promoting neuroplasticity in motor function.38 Another pilot study by Sokhadze et al explored the effects of combining rTMS and neurofeedback in 20 children with ASD and 22 children in the waitlist groups, aiming to upregulate gamma oscillations and operantly condition them.24 The study showed significant behavioral and functional outcomes compared to the waitlist groups. The results showed improvement in both the subitems of communication and the daily living skills domain. These findings highlight the promising therapeutic potential of TMS, and larger randomized trials are needed to inform clinical recommendations.
tDCS
Another mode of noninvasive neurostimulation is tDCS, which is a similar approach to rTMS but involves passing weak electric currents directly through two electrodes (in the range of 1–2 mA) instead of a coil.84 It has been shown to modulate neuronal membrane potentials, such that neurons near the anode tend to fire more frequently, while those near the cathode may be less likely to fire.85 Researchers proposed a series of RCT studies to observe the modulating effects of tDCS through various targets. Hadoush et al applied bilateral anodal stimulation over the left and right prefrontal and motor areas in 50 children with ASD diagnoses, which significantly improved social responsiveness (as evaluated by ATEC scores).45 Additionally, another RCT study investigated the effects of bilateral anodal tDCS stimulation over the cerebellar hemispheres using resting-state electroencephalography (EEG).54 Notably, the modulation increased the brain complexity in children with ASD, suggesting alternative neuromodulation pathways beyond traditional cortical targets. Salehinejad et al investigated the contribution of the vmPFC and right TPJ in theory of mind (ToM) abilities of 16 ASD children, which showed the vmPFC could be a potential better target region for the reduction of ASD symptoms.48 Han et al applied multiple sessions of prefrontal tDCS coupled with cognitive remediation training, which resulted in a marked improvement in social functioning compared to the sham-tDCS group, as measured by the Social Responsiveness Scale-2nd edition (SRS-2), among 105 individuals with ASD.53,55 In the choice of sessions, Auvichayapat et al compared the efficacy of 0, 5, and 20 sessions of tDCS over the DLPFC in 36 male children with ASD, which demonstrated that both 5- and 20-tDCS significantly reduced autism severity compared to the sham group with sustained improvements for 12 months, however, there was no significant difference between 5- and 20-tDCS groups.52
Due to higher levels of spatial focus and cortical excitability, high-definition transcranial direct current stimulation (HD-tDCS) was applied to better elucidate the causality of the correlation between brain excitability and behavioral or cognitive changes in individuals with autism.86 Two RCT studies examined the effect of HD-tDCS over different targets. Qiao et al demonstrated that right TPJ anodal HD-tDCS can facilitate emotional face processing in 29 participants with high autistic traits.46 Another RCT study compared the cognitive effects of active and sham anodal HD-tDCS over the right ventrolateral prefrontal cortex (vlPFC), although improvements in cognitive flexibility following stimulation were not observed.47
To assess neurophysiological correlates of ASD, some studies reported changes in EEG activity. An RCT study conducted by Amatachaya et al revealed that a single session of anodal tDCS over F3 increased peak alpha frequency (PAF), correlating with improved social and behavioral outcomes.41 Differences in EEG microstates before and after tDCS were also compared in a pilot study, revealing a marked difference during the treatment period in children with ASD.56 Integration with neuroimaging, such as fNIRS, allowed researchers to explore the possible neurophysiological mechanisms underlying the effects of tDCS.49
ECT
Catatonia has been increasingly recognized as a comorbid syndrome of ASD, which a meta-analysis in 2021 showed that 10.4% of individuals with ASD have catatonia.87 ECT has been included in treatment algorithms for acute presentations of catatonia in autism, which was supported by a series of case reports.88 Zaw et al reported in 1999 on a 14-year-old boy with catatonic stupor and autism who experienced remission of such with bilateral ECT, although the core symptoms of autism were not affected.58 Ghaziuddin et al presented a 17-year-old white male with autistic disorder, depression, and catatonia who received a course of 18 ECTs, which proved life-saving due to his severe weight loss and declining self-care.59 Similarly, Dhossche et al reported that two men responded to ECT in tics along with other catatonic symptoms and SIBs.62 He further discussed 2 patients with ASD and mental retardation who experienced persistent symptoms of motor disturbance, functional decline, and episodic aggression.63 Since 2008, Wachtel et al have reported a series of results about applying ECT in autistic adolescents to improve social activities and reduce SIBs.60,61,64–67 A 10-year retrospective review of the use of ECT in ASD and/or intellectual disability (ID) analyzed 32 patients, of which 30 (94%) experienced a positive clinical response.89 Therefore, if catatonia is present in ASDs, ECT may provide a safe alternative to pharmacotherapy or psychosurgery.
Invasive Neurostimulation
DBS
DBS is a surgical alternative that modulates specific brain regions and neurological circuits by applying chronic electrical impulses, which have been reported to be effective in treating hyperkinetic movement disorders. There are several studies on the effects of DBS on the aggressive behavior of ASDs, which mainly have focused on basal ganglia circuits. Sturm et al reported a 13-year-old boy with Kanner’s autism and serious SIB, with DBS targeting the amygdaloid complex as well as the supra-amygdaloid projection system, and the stimulation of basolateral (BL) was proven to be beneficial to SIB, emotional, social, and cognitive symptoms of ASD.69 Two studies targeted GPi DBS to improve movement deficits.70,75 Kakko et al presented a 19-year-old male with ASD and ID, whose severe movement symptoms led to self-mutilation and sepsis.75 After implanting electrodes in the GPi target, his anxiety, behavioral symptoms, and self-destructive behavior ceased remarkably. The other research evaluated the effects of stereotypies in two teenagers with autism after implanting electrodes in the GPi or anterior limb of the internal capsule (ALIC).70 Both patients experienced an initial improvement in motor stereotypies of over 70% within the first few months after DBS surgery, but only one of them maintained this improvement during follow-up.
In addition, the nucleus accumbens (NAc) has been demonstrated to be a key hub for the modulation of aggression and social response in ASD, which was supported by some case reports. Park et al applied bilateral NAc DBS in a 14-year-old boy with ASD and SIB.73 The remarkable clinical improvement in the frequency of SIBs, as well as expression and comprehension language skills, was observed at the 2-year post-operative evaluation. The other case also targeted NAc as the electrode implantation location for a 42-year-old woman with autism and the comorbidities of obsessive-compulsive disorder (OCD) and aggression, which showed significant symptom relief for severe obsessive-compulsive behaviors, social communication, and stereotyped patterns at the 1-year follow-up.74 In a middle-aged man with multiple comorbidities (including refractory OCD, epilepsy, tic disorder, autism, and major depressive disorder (MDD)), he received DBS targeted at the vc/vs and reported a significant reduction in OCD symptoms and depression.76 In 2022, a case series first examined the effectiveness of DBS on OCD symptoms and the safety of DBS in patients with OCD and ASD specifically, which showed that 2/3 patients with OCD and comorbid ASD responded to DBS (decrease ≥35% in Y-BOCS).77 A study conducted by Benedetti et al analyzed the impact of DBS targeting the posteromedial hypothalamus (pHyp) in nine patients with DRE and intractable aggressive behavior (IAB).71 The results showed that seizure frequency and aggressiveness were significantly controlled after a follow-up of up to 4 years.
VNS
VNS therapy has been proven safe and effective in reducing seizure frequency and duration in individuals with pharmacoresistant epilepsy. Notably, ASDs have higher rates of epilepsy compared with individuals without ASD (21% in people with ASD and intellectual disability and 0.8% in a general population sample).90 Preliminary studies also indicated that VNS may improve neurocognitive performance and quality of life in individuals with ASDs.88,91 A cohort of 59 autistic patients was identified to assess seizure frequency and quality of life after being implanted with a pulse generator.92 Notably, 58% of the autism patients experienced at least a 50% reduction in seizure frequency, and 76% reported improvement in alertness at 12 months of follow-up. In the largest study to date of VNS therapy in ASDs, there was no significant difference in seizure reduction between individuals with and without autism at 12 months post-implantation, but almost 62% of the patients in the autism group had greatly improved mood compared with the control group (p = 0.0437).93 In addition, Wang et al conducted an observational study of 10 children with drug-resistant epilepsy (DRE) to confirm that VNS therapy makes seizure control stable and has a positive effect on autistic behaviors.94 However, a prospective study in 8 autistic children with DRE indicated that seizure frequency had not decreased, and cognitive effects had not improved at the 2-year follow-up.95 There is still limited data on VNS therapy in ASD, which emphasizes the need to evaluate the efficacy of this technique further. Figure 2 shows the indications of neuromodulation techniques and potential mechanisms that lead to the effects.
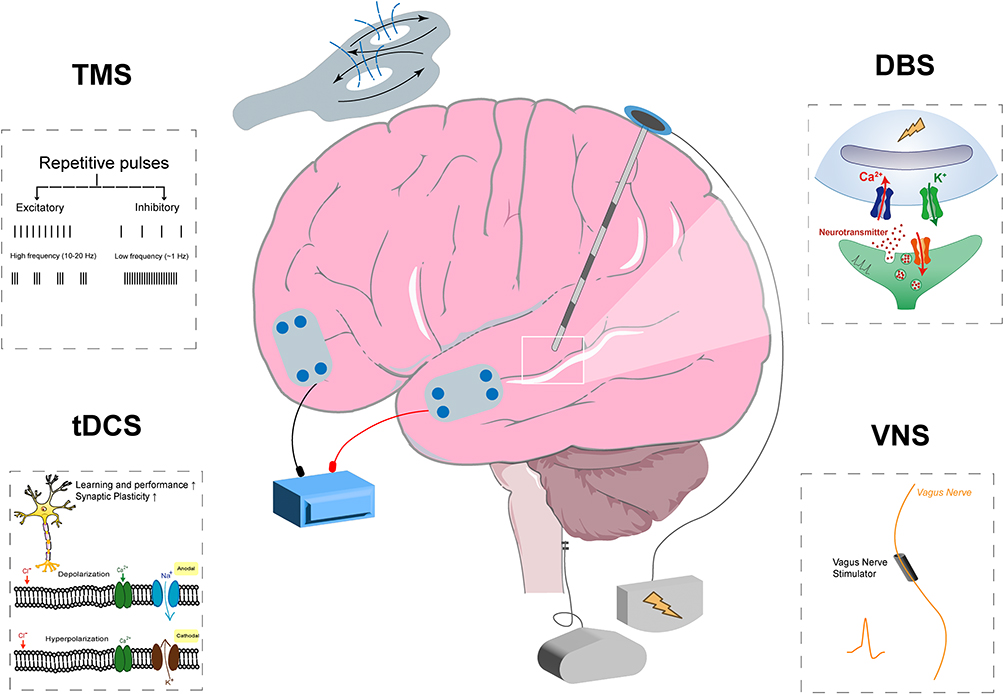 |
Figure 2 A schematic representation, mechanisms and indications of NIBS and IBS techniques. In TMS, HF-rTMS (5–20 Hz) induces to cortical facilitation, whereas LF-rTMS (≤1 Hz) reduces cortical excitability through the activation of inhibitory GABAergic interneurons; conditions treatable with TMS including: 1) social-related impairments; 2) executive function deficits; 3) abnormal reactions to the sensory environment; 4) combined with neurofeedback therapies; In tDCS, membrane potentials could be influenced at a cellular level under weak currents, which may improve neural plasticity and ability of learning and performance (upward arrow); conditions treatable with tDCS including: 1) social-related impairments; 2) cognitive flexibility deficits; 3) impairments in motor and behavioral skills; 4) combined with cognitive remediation training; in DBS, neurotransmitters are released in response to stimulation (the white box indicates the magnified area), leading to changes in synaptic plasticity; conditions treatable with DBS including: 1) Comorbidities: serious self-injurious behaviors, seizure, obsessive-compulsive disorder, depression; 2) motor stereotypies; in VNS, stimulation of the vagus nerve could influence the activation of noradrenergic system, which may promote enhancement of plasticity; conditions treatable with VNS including: 1) Comorbidities: pharmacoresistant epilepsy; 2) abnormal behaviors and emotional areas; 3) autistic behaviors, but the positive effect of VNS on autistic behaviors requires further evidence. |
Safety
Noninvasive Neurostimulation
TMS and tDCS are considered quite safe even in pediatric populations. However, some potential risks for adverse side effects cannot be ruled out due to the heterogeneity of the patients. Induction of seizure represents the most serious adverse event related to TMS, with a reported risk of less than 0.01% across all patients and all paradigms. Other mild and transient side effects include mild headache, pain, and facial discomfort at the TMS application site.29,33 Only minor adverse effects were observed during tDCS application, including mild skin irritation, short-term itchiness, and buzzing sensations.42,44,49
ECT is recognized to influence autonomic stability during electrical stimulation, which could bring the risk of potential arrhythmias.96 Adequate IV hydration, commencing at least 12 hours prior to ECT treatment, likely reduced the risk, as conducted by Wachtel et al.65 Additionally, common and self-limiting adverse effects associated with ECT include headache, muscle soreness, and post-procedural nausea or vomiting.97 Cognitive side effects such as anterograde and/or retrograde amnesia are also frequently observed. These cognitive impairments could resolve in the weeks following treatment and have no significant difference compared to other groups.98
Invasive Neurostimulation
Few studies reported complications of DBS that interrupted therapy. One patient had an infection of the DBS system that required removal of the system.77 A mild serous drainage was observed in a 27-year-old man around the electrode implantation site.71 Another 24-year-old female also experienced a recurrence of symptoms due to lead fracture and dislodgement, which symptoms were alleviated with a new battery replacement.72 Many studies have demonstrated the safety of VNS therapy, which can be delivered to adults as well as children.99–101 Some reported adverse effects, such as intermittent coughing and hoarseness, are usually slight and transient.95
In summary, the safety of neuromodulation interventions has been demonstrated in numerous studies, with minimal side effects. The summary of adverse events reported in various neuromodulation techniques is shown in Table 5. However, nearly half of the existing studies have not reported adverse effects, while the remaining studies have often failed to use valid scales to assess adverse effects. Therefore, the risk of overall adverse events associated with neuromodulation techniques may be underestimated, especially in vulnerable populations. Future studies should utilize standard side effect questionnaires to evaluate the tolerability of the neuromodulation technique, and further long-term follow-up is also essential.
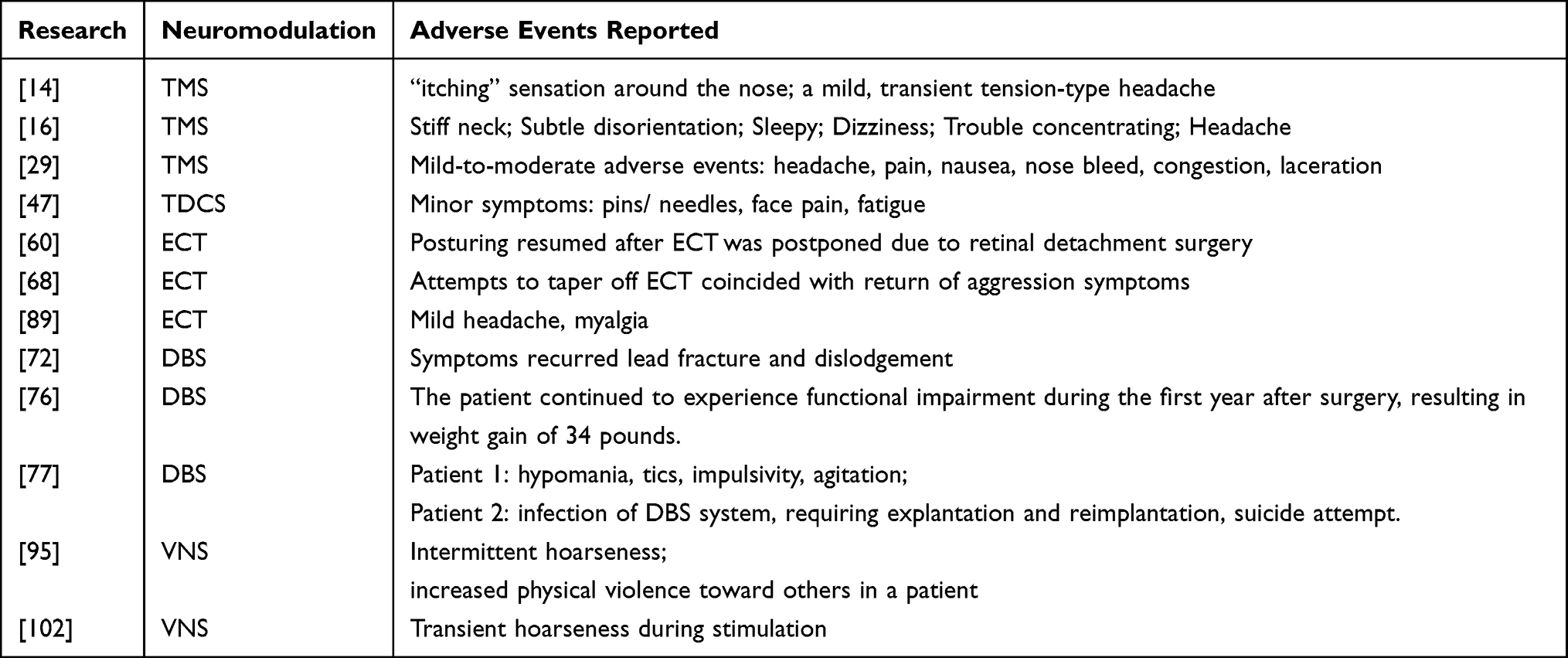 |
Table 5 Adverse Events Reported in Various Neuromodulation Techniques |
Discussion
In this review, we comprehensively and systematically evaluate the clinical efficacy and safety of neuromodulation interventions in patients with ASD and other comorbidities. Finding innovative therapies is a fundamental aspect for individuals with autism and comorbid conditions resistant to conventional treatments. It demonstrates that both NIBS and IBS can help to improve neuropsychological function and reduce core symptoms of ASD as potential adjunctive therapies. A series of RCT and pilot studies demonstrated that NIBS may improve specific core or associated symptoms related to an alteration in the functioning of a specific cortical region or circuit, but the optimal stimulus parameters still remain unclear. On the other side, IBS are primarily aimed at alleviating severe comorbidities associated with ASD, such as SIBs, refractory epilepsy, major depressive disorder, etc. Due to the inherent risks of invasive interventions, current clinical studies are mostly case reports and observational studies, indicating a lack of higher-level clinical evidence. There remains significant heterogeneity in clinical phenotypes between studies, particularly in terms of patient profiles, study designs, stimulation protocols, and outcome measurements. Overall, the lack of standardized protocols for the neuromodulation techniques makes it difficult to compare different results directly. Therapeutic use of neuromodulation interventions would likely be described as possibly effective. Researchers should corroborate their findings with larger sample sizes and longer follow-up to recognize true benefits of neuromodulation interventions. Some potential breakthroughs such as TI should also be considered carefully in the treatments of autism, which could provide a deeper understanding of the mechanism of ASD.103
A major hypothesis suggests that the behavioral symptoms of ASD are explained by abnormal resting-state functional connectivity (rsFC), especially long-range disconnection that may occur as a result of developmental events.4 Growing evidence indicates that sociability, cognitive, and sensorimotor impairments are related to abnormalities of distributed networks, rather than of single brain loci.104 Social behavior is mediated by a distributed, large-scale network of multiple brain structures, including areas of the prefrontal cortex, subcortex, and areas that integrate information, which is commonly observed to be dysfunctional in individuals with ASD.105 An fMRI study showed that deficits in the mesolimbic reward pathway (especially key subcortical nodes including VTA and NAc) contribute to impaired social skills in childhood autism.106 Collectively, these studies suggest the presence of disrupted neural pathways before the emergence of behavioral symptoms in patients with ASD and might provide clues about the underlying neural mechanisms of autism, thus suggesting that stimulation approaches may yield promising results, as they seem to be able to modulate the brain’s functional connectivity via normalizing the E/I balance.
TMS and tDCS can induce activity in neurons and changes in neuroplasticity via generating magnetic fields or weak currents, which is believed to reverse underlying neuroplasticity deficits in autism.107 To gain a deeper understanding of the short-term and long-term effects of tDCS and TMS on ASD, more well-designed, longitudinal, randomized, double-blind, sham-controlled trials with an adequate follow-up period after treatment are needed. In 2017, Grossman et al developed Temporal Interference Stimulation (TI) to stimulate further specific deep brain regions, which could produce an LF envelope and modulate the activity of neurons.103 We believe that TI is a promising technology for treating ASD due to its superior focus and steerability. Further animal experiments and clinical trials are required to be conducted.
There has been increasing interest in the overlap of catatonia and ASD.108,109 Over the past decade, an increasing number of reports have shown the swift and well-tolerated resolution of catatonia with ECT.110 Although the mechanism by which ECT relieves catatonia remains unclear, several hypotheses have been proposed. The neuroendocrine studies of melancholia found that repeated seizures normalize hypothalamic-pituitary-adrenal axis functions and correct neuroendocrine abnormalities, which may offer a standard explanation for autism.111 Another mechanism originates from a study showing the increase in new brain cells after induced seizures.112 Future research and clinical application are needed to expand our knowledge regarding optimal utilization of ECT in ASDs with catatonia and treatment-refractory SIB.
In IBS, with direct intervention in pathological neural circuits, DBS has changed the way that brain disorders are treated and understood and is considered one of the most promising therapeutic applications for clinical neuroscience.113–115 In line with our expanding understanding of pathophysiology, the DBS community has moved toward developing “connectomic” neurosurgical targeting approaches. A connectomic analysis in 8 patients with ASD and extreme behaviors revealed a shared functional network upon which 3 of the DBS targets converge (NAcc, VC/VS, pHyp), which provided crucial insight into the brain networks involved in symptom improvement with DBS.116 Of note, DBS has now been used in ASDs only to treat comorbid conditions, which have obtained optimal results for drug-resistant OCD and SIBs.69,76,77 Positive effects on core symptoms of ASD have only occasionally been reported.72,73 Therefore, among the emerging therapeutic approaches, DBS represents a promising intervention for alleviating comorbidities associated with autism, potentially enhancing both clinical outcomes and quality of life for patients.
Epilepsy has been the most frequently studied topic among the physical conditions that co-occur with ASD. It is reported that almost 60% of EEG records from children with ASD have interictal spikes, and a higher percentage of interictal spikes in the frontal lobe.117–119 Due to the high comorbidity rate between ASD and epilepsy, both diseases possibly share common pathophysiological properties. A hypothesis suggests that early-life seizures induce an imbalance in the excitatory/inhibitory (E/I) ratio in specific brain regions, which may alter the dynamic flexibility of brain connectivity in ASDs.120,121 The effects are putatively mediated by the vagus nerve’s numerous interconnections with brain structures thought to be involved with mood and emotional regulation. Meanwhile, VNS could be paired with well-established, existing rehabilitative interventions, holding potential to treat dysfunction that accompanies neurodevelopmental disorders.123 Future clinical trials are crucial for evaluating the benefits of paired VNS therapies.
However, most studies were case reports and open-label trials, with low levels of evidence for clinical application. Ethical and legal concerns persist regarding potential misuse of DBS or VNS, which reminds us to carefully assess the risk-benefit ratio of invasive therapies.
In the future, more advanced techniques such as functional imaging and connectomics will be needed to evaluate the impact of neurostimulation interventions for ASDs, thereby optimizing clinical responses.
Limitations
This systematic review has certain limitations. First, we drew conclusions based on a limited sample size, and most included studies were case reports and not controlled studies. Given that we did not consider any limitations regarding the study design or the age or sex of participants, these results must be interpreted with caution regarding the potential effect of confounding factors. Second, many studies have not been designed using clear and objective primary clinical endpoints. The clinical outcome measures that have been utilized are often subjective self- or observer-based reports, which threaten to mask or undermine assessment of change. Third, ASD is often associated with co-occurring psychiatric or neurological disorders, and this can likely generate confounding effects in clinical neuromodulation studies. Overall, we have attempted to include all relevant research in this work to provide a comprehensive picture of the current state of this new therapeutic field, in order to review its findings and describe its strengths and weaknesses.
Conclusion
Recent decades have witnessed a growing interest in the efficiency and safety of neurostimulation interventions for autism, yet stronger evidence base for treating ASD in individual studies are needed. The current quality for neuromodulation interventions in ASD is mixed, which requires a wider range of such a clinically heterogeneous population to test the validity and reliability of these measures, thereby increasing the generalizability of the results. Therefore, further studies should focus on establishing a solid consensus regarding optimal stimulation parameters, cumulative doses, stimulation targets and longer follow-up duration for neurostimulation in ASD, which may provide patients with highly personalized and targeted therapeutic strategies.
Data Sharing Statement
All data extracted or analyzed during this study are included in the manuscript and the supplementary materials.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Science and Technology Projects in Guangzhou (no.2024A04J5231), the Science and Technology Foundation of Guangdong Province (no.2023A1515012382), the Clinical Research Program of Nanfang Hospital, Southern Medical University (no.2023CR030), the Science and Technology Planning Project of Ganzhou (no. 2023LNS17464), and the Clinical Characteristic Technology Project in Guangzhou Area (no. 2026P-TS069)..
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zeidan J, Fombonne E, Scorah J, et al. Global prevalence of autism: a systematic review update. Autism Research. 2022;15(5):778–790. doi:10.1002/aur.2696
2. DeFilippis M. Depression in children and adolescents with autism spectrum disorder. Children. 2018;5(9):112. doi:10.3390/children5090112
3. Koenig K, Levine M. Psychotherapy for individuals with autism spectrum disorders. J. Contemp. Psychother. 2011;41(1):29–36. doi:10.1007/s10879-010-9158-9
4. Lord C, Brugha TS, Charman T, et al. Autism spectrum disorder. Nat Rev Dis Primers. 2020;6(1):5. doi:10.1038/s41572-019-0138-4
5. Hazlett HC, Gu H, Munsell BC, et al. Early brain development in infants at high risk for autism spectrum disorder. Nature. 2017;542(7641):348–351. doi:10.1038/nature21369
6. Rippon G, Brock J, Brown C, Boucher J. Disordered connectivity in the autistic brain: challenges for the “new psychophysiology”. Int J Psychophysiol. 2007;63(2):164–172. doi:10.1016/j.ijpsycho.2006.03.012
7. Rojas DC. The role of glutamate and its receptors in autism and the use of glutamate receptor antagonists in treatment. J Neural Transm. 2014;121(8):891–905. doi:10.1007/s00702-014-1216-0
8. Nisar S, Bhat AA, Masoodi T, et al. Genetics of glutamate and its receptors in autism spectrum disorder. Mol Psychiatry. 2022;27(5):2380–2392. doi:10.1038/s41380-022-01506-w
9. Chiesa M, Nardou R, Lozovaya N, et al. Enhanced glutamatergic currents at birth in Shank3 KO mice. Neural Plast. 2019;2019:2382639. doi:10.1155/2019/2382639
10. Moxon-Emre I, Daskalakis ZJ, Blumberger DM, et al. Modulation of dorsolateral prefrontal cortex glutamate/glutamine levels following repetitive transcranial magnetic stimulation in young adults with autism. Front Neurosci. 2021;15.
11. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. doi:10.1136/bmj.b2700
12. Porritt K, Evans CB, Loveday C, et al. Systematic reviews of qualitative evidence. In: Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z, editors. JBI Manual for Evidence Synthesis; 2024.
13. Sokhadze EM, El-Baz A, Baruth J, Mathai G, Sears L, Casanova MF. Effects of low frequency repetitive transcranial magnetic stimulation (rTMS) on gamma frequency oscillations and event-related potentials during processing of illusory figures in autism. J Autism Dev Disord. 2009;39(4):619–634. doi:10.1007/s10803-008-0662-7
14. Baruth JM, Casanova MF, El-Baz A, et al. Low-Frequency Repetitive Transcranial Magnetic Stimulation (rTMS) modulates evoked-gamma frequency oscillations in Autism Spectrum Disorder (ASD). J. Neurother. 2010;14(3):179–194. doi:10.1080/10874208.2010.501500
15. Sokhadze E, Baruth J, Tasman A, et al. Low-frequency repetitive transcranial magnetic stimulation (rTMS) affects event-related potential measures of novelty processing in autism. Applied Psychophysiology and Biofeedback. 2010;35(2):147–161. doi:10.1007/s10484-009-9121-2
16. Fecteau S, Agosta S, Oberman L, Pascual-Leone A. Brain stimulation over Broca’s area differentially modulates naming skills in neurotypical adults and individuals with Asperger’s syndrome. Eur. J. Neurosci. 2011;34(1):158–164. doi:10.1111/j.1460-9568.2011.07726.x
17. Casanova MF, Baruth JM, El-Baz A, Tasman A, Sears L, Sokhadze E. Repetitive Transcranial Magnetic Stimulation (rTMS) Modulates Event-Related Potential (ERP) Indices of Attention in Autism. Transl. Neurosci. 2012;3(2):170–180. doi:10.2478/s13380-012-0022-0
18. Enticott PG, Rinehart NJ, Tonge BJ, Bradshaw JL, Fitzgerald PB. Repetitive transcranial magnetic stimulation (rTMS) improves movement-related cortical potentials in autism spectrum disorders. Brain Stimulation. 2012;5(1):30–37. doi:10.1016/j.brs.2011.02.001
19. Sokhadze EM, Baruth JM, Sears L, Sokhadze GE, El-Baz AS, Casanova MF. Prefrontal neuromodulation using rTMS improves error monitoring and correction function in autism. Applied Psychophysiology and Biofeedback. 2012;37(2):91–102. doi:10.1007/s10484-012-9182-5
20. Casanova MF, Hensley MK, Sokhadze EM, et al. Effects of weekly low-frequency rTMS on autonomic measures in children with autism spectrum disorder. Front Hum Neurosci. 2014;8:851. doi:10.3389/fnhum.2014.00851
21. Enticott PG, Fitzgibbon BM, Kennedy HA, et al. A double-blind, randomized trial of deep Repetitive Transcranial Magnetic Stimulation (rTMS) for Autism Spectrum Disorder. Brain Stimulation. 2014;7(2):206–211. doi:10.1016/j.brs.2013.10.004
22. Panerai S, Tasca D, Lanuzza B, et al. Effects of repetitive transcranial magnetic stimulation in performing eye-hand integration tasks: four preliminary studies with children showing low-functioning autism. Autism. 2014;18(6):638–650. doi:10.1177/1362361313495717
23. Sokhadze EM, El-Baz AS, Sears LL, Opris I, Casanova MF. rTMS neuromodulation improves electrocortical functional measures of information processing and behavioral responses in autism. Front. Syst. Neurosci. 2014;8:134. doi:10.3389/fnsys.2014.00134
24. Sokhadze EM, El-Baz AS, Tasman A, et al. Neuromodulation integrating rTMS and neurofeedback for the treatment of autism spectrum disorder: an exploratory study. Applied Psychophysiology and Biofeedback. 2014;39(3–4):237–257. doi:10.1007/s10484-014-9264-7
25. Sokhadze E, Casanova M, El-Baz A, Farag HE, Li X, Wang Y. TMS-based neuromodulation of evoked and induced gamma oscillations and event-related potentials in children with autism. NeuroRegulation. 2016;3(3):101–126. doi:10.15540/nr.3.3.101
26. Sokhadze G, Casanova M, Kelly D, Casanova E, Russell B, Sokhadze E. neuromodulation based on rTMS affects behavioral measures and autonomic nervous system activity in children with autism. NeuroRegulation. 2017;4(2):65–78. doi:10.15540/nr.4.2.65
27. Abujadi C, Croarkin PE, Bellini BB, Brentani H, Marcolin MA. Intermittent theta-burst transcranial magnetic stimulation for autism spectrum disorder: an open-label pilot study. Rev Bras Psiquiatr. 2018;40(3):309–311. doi:10.1590/1516-4446-2017-2279
28. Sokhadze EM, Lamina EV, Casanova EL, et al. Exploratory study of rTMS neuromodulation effects on electrocortical functional measures of performance in an oddball test and behavioral symptoms in autism. Front. Syst. Neurosci. 2018;12:20. doi:10.3389/fnsys.2018.00020
29. Ameis SH, Blumberger DM, Croarkin PE, et al. Treatment of Executive Function Deficits in autism spectrum disorder with repetitive transcranial magnetic stimulation: a double-blind, sham-controlled, pilot trial. Brain Stimulation. 2020;13(3):539–547. doi:10.1016/j.brs.2020.01.007
30. Assadi M, Dave J, Leone P, Redjal N, Curtin A. Enhancement of behavioral and linguistic outcome measures in autism spectrum disorder through neuro-navigated transcranial magnetic stimulation: a pilot study. J Clin Neurosci. 2020;74:151–154. doi:10.1016/j.jocn.2020.02.005
31. Casanova MF, Shaban M, Ghazal M, et al. Effects of transcranial magnetic stimulation therapy on evoked and induced gamma oscillations in children with autism spectrum disorder. Brain Sci. 2020;10(7):423. doi:10.3390/brainsci10070423
32. Gwynette MF, Lowe DW, Henneberry EA, et al. Treatment of adults with autism and major depressive disorder using transcranial magnetic stimulation: an open label pilot study. Autism Res. 2020;13(3):346–351. doi:10.1002/aur.2266
33. Ni HC, Chen YL, Chao YP, et al. Intermittent theta burst stimulation over the posterior superior temporal sulcus for children with autism spectrum disorder: a 4-week randomized blinded controlled trial followed by another 4-week open-label intervention. Autism. 2021;25(5):1279–1294. doi:10.1177/1362361321990534
34. Desarkar P, Rajji TK, Ameis SH, et al. Assessing and stabilizing atypical plasticity in autism spectrum disorder using rTMS: results from a proof-of-principle study. Clin Neurophysiol. 2022;141:109–118. doi:10.1016/j.clinph.2021.03.046
35. Kang J, Li X, Casanova MF, Sokhadze EM, Geng X. Impact of repetitive transcranial magnetic stimulation on the directed connectivity of autism EEG signals: a pilot study. Med Biol Eng Comput. 2022;60(12):3655–3664. doi:10.1007/s11517-022-02693-y
36. Kang J, Zhang Z, Wan L, Casanova MF, Sokhadze EM, Li X. Effects of 1Hz repetitive transcranial magnetic stimulation on autism with intellectual disability: a pilot study. Comput. Biol. Med. 2022;141:105167. doi:10.1016/j.compbiomed.2021.105167
37. Ni HC, Lin HY, Chen YL, et al. 5-day multi-session intermittent theta burst stimulation over bilateral posterior superior temporal sulci in adults with autism-a pilot study. Biomed J. 2022;45(4):696–707. doi:10.1016/j.bj.2021.07.008
38. Kaokhieo J, Tretriluxana J, Chaiyawat P, et al. Effects of repetitive transcranial magnetic stimulation combined with action-observation-execution on social interaction and communication in autism spectrum disorder: feasibility study. Brain Res. 2023;1804:148258. doi:10.1016/j.brainres.2023.148258
39. Ni HC, Chen YL, Chao YP, et al. A lack of efficacy of continuous theta burst stimulation over the left dorsolateral prefrontal cortex in autism: a double blind randomized sham-controlled trial. Autism Res. 2023;16(6):1247–1262. doi:10.1002/aur.2954
40. Schneider HD, Hopp JP. The use of the Bilingual Aphasia Test for assessment and transcranial direct current stimulation to modulate language acquisition in minimally verbal children with autism. Clin. Linguist. Phon. 2011;25(6–7):640–654. doi:10.3109/02699206.2011.570852
41. Amatachaya A, Jensen MP, Patjanasoontorn N, et al. The short-term effects of transcranial direct current stimulation on electroencephalography in children with autism: a randomized crossover controlled trial. Behav. Neurol. 2015;2015:928631. doi:10.1155/2015/928631
42. Gómez L, Vidal B, Maragoto C, et al. Non-invasive brain stimulation for children with autism spectrum disorders: a short-term outcome study. Behav Sci. 2017;7(3):63. doi:10.3390/bs7030063
43. Esse Wilson J, Trumbo MC, Wilson JK, Tesche CD. Transcranial direct current stimulation (tDCS) over right temporoparietal junction (rTPJ) for social cognition and social skills in adults with autism spectrum disorder (ASD). J Neural Transm. 2018;125(12):1857–1866. doi:10.1007/s00702-018-1938-5
44. Rothärmel M, Moulier V, Vasse M, et al. A prospective open-label pilot study of transcranial direct current stimulation in high-functioning autistic patients with a dysexecutive syndrome. Neuropsychobiology. 2019;78(4):189–199. doi:10.1159/000501025
45. Hadoush H, Nazzal M, Almasri NA, Khalil H, Alafeef M. Therapeutic effects of bilateral anodal transcranial direct current stimulation on prefrontal and motor cortical areas in children with autism spectrum disorders: a pilot study. Autism Res. 2020;13(5):828–836. doi:10.1002/aur.2290
46. Qiao YX, Hu Q, Xuan RR, et al. High-definition transcranial direct current stimulation facilitates emotional face processing in individuals with high autistic traits: a sham-controlled study. Neurosci lett. 2020;738.
47. Parmar D, Enticott PG, Albein-Urios N. Anodal HD-tDCS for cognitive inflexibility in autism spectrum disorder: a pilot study. Brain Stimulation. 2021;14(5):1298–1300. doi:10.1016/j.brs.2021.08.020
48. Salehinejad MA, Paknia N, Hosseinpour AH, et al. Contribution of the right temporoparietal junction and ventromedial prefrontal cortex to theory of mind in autism: a randomized, sham-controlled tDCS study. Autism Res. 2021;14(8):1572–1584. doi:10.1002/aur.2538
49. Han YMY, Chan MMY, Shea CKS, et al. Neurophysiological and behavioral effects of multisession prefrontal tDCS and concurrent cognitive remediation training in patients with autism spectrum disorder (ASD): a double-blind, randomized controlled fNIRS study. Brain Stimulation. 2022;15(2):414–425. doi:10.1016/j.brs.2022.02.004
50. Padrón I, García-Marco E, Moreno I, et al. Multisession Anodal tDCS on the right temporo-parietal junction improves mentalizing processes in adults with autistic traits. Brain Sciences. 2022;12(1). doi:10.3390/brainsci12111506.
51. Zemestani M, Hoseinpanahi O, Salehinejad MA, Nitsche MA. The impact of prefrontal transcranial direct current stimulation (tDCS) on theory of mind, emotion regulation and emotional-behavioral functions in children with autism disorder: a randomized, sham-controlled, and parallel-group study. Autism Res. 2022;15(10):1985–2003. doi:10.1002/aur.2803
52. Auvichayapat P, Intayot K, Udomchat C, et al. Long-term effects of transcranial direct current stimulation in the treatment of autism spectrum disorder: a randomized controlled trial. Dev Med Child Neurol. 2023;65(6):811–820. doi:10.1111/dmcn.15457
53. Chan MMY, Choi CXT, Tsoi TCW, Shea CKS, Yiu KWK, Han YMY. Effects of multisession cathodal transcranial direct current stimulation with cognitive training on sociocognitive functioning and brain dynamics in autism: a double-blind, sham-controlled, randomized EEG study. Brain Stimulation. 2023;16(6):1604–1616. doi:10.1016/j.brs.2023.10.012
54. Hadoush H, Hadoush A. Modulation of resting-state brain complexity after bilateral cerebellar anodal transcranial direct current stimulation in children with autism spectrum disorders: a randomized controlled trial study. Cerebellum. 2023;22(6):1109–1117. doi:10.1007/s12311-022-01481-6
55. Han YM, Chan MM, Shea CK, et al. Effects of prefrontal transcranial direct current stimulation on social functioning in autism spectrum disorder: a randomized clinical trial. Autism. 2023;27(8):2465–2482. doi:10.1177/13623613231169547
56. Kang J, Fan X, Zhong Y, et al. Transcranial direct current stimulation modulates EEG microstates in low-functioning autism: a pilot study. Bioengineering. 2023;10(1):98. doi:10.3390/bioengineering10010098
57. Ratsapbhayakul T, Keeratitanont K, Chonprai C, et al. Anodal transcranial direct-current stimulation and non-verbal intelligence in autism spectrum disorder: a randomized controlled trial. Dev Med Child Neurol. 2024;66:1244–1254. doi:10.1111/dmcn.15874
58. Zaw FK, Bates GD, Murali V, Bentham P. Catatonia, autism, and ECT. Dev Med Child Neurol. 1999;41(12):843–845. doi:10.1111/j.1469-8749.1999.tb00552.x
59. Ghaziuddin M, Quinlan P, Ghaziuddin N. Catatonia in autism: a distinct subtype? J. Intellect. Disabil. Res. 2005;49(Pt 1):102–105. doi:10.1111/j.1365-2788.2005.00666.x
60. Wachtel LE, Kahng S, Dhossche DM, Cascella N, Reti IM. ECT for catatonia in an autistic girl. Am J Psychiatry. 2008;165(3):329–333. doi:10.1176/appi.ajp.2007.07081246
61. Wachtel LE, Contrucci-Kuhn SA, Griffin M, Thompson A, Dhossche DM, Reti IM. ECT for self-injury in an autistic boy. Eur Child Adolesc Psychiatry. 2009;18(7):458–463. doi:10.1007/s00787-009-0754-8
62. Dhossche DM, Reti IM, Shettar SM, Wachtel LE. Tics as signs of catatonia: electroconvulsive therapy response in 2 men. The Journal of ECT. 2010;26(4):266–269. doi:10.1097/YCT.0b013e3181cb5f60
63. Ghaziuddin N, Gih D, Barbosa V, Maixner DF, Ghaziuddin M. Onset of catatonia at puberty: electroconvulsive therapy response in two autistic adolescents. The Journal of ECT. 2010;26(4):274–277. doi:10.1097/YCT.0b013e3181de332e
64. Wachtel LE, Griffin M, Reti IM. Electroconvulsive therapy in a man with autism experiencing severe depression, catatonia, and self-injury. The Journal of ECT. 2010;26(1):70–73. doi:10.1097/YCT.0b013e3181a744ec
65. Wachtel LE, Griffin MM, Dhossche DM, Reti IM. Brief report: electroconvulsive therapy for malignant catatonia in an autistic adolescent. Autism. 2010;14(4):349–358. doi:10.1177/1362361309350135
66. Wachtel LE, Hermida A, Dhossche DM. Maintenance electroconvulsive therapy in autistic catatonia: a case series review. Prog Neuro Psychopharmacol Biol Psychiatry. 2010;34(4):581–587. doi:10.1016/j.pnpbp.2010.03.012
67. Wachtel LE, Reti IM, Dhossche DM, Slomine BS, Sanz J. Stability of neuropsychological testing during two years of maintenance electroconvulsive therapy in an autistic man. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):301–302. doi:10.1016/j.pnpbp.2010.11.013
68. Haq AU, Ghaziuddin N. Maintenance electroconvulsive therapy for aggression and self-injurious behavior in two adolescents with autism and catatonia. J Neuropsychiatry Clin Neurosci. 2014;26(1):64–72. doi:10.1176/appi.neuropsych.12110284
69. Sturm V, Fricke O, Bührle CP, et al. DBS in the basolateral amygdala improves symptoms of autism and related self-injurious behavior: a case report and hypothesis on the pathogenesis of the disorder. Front Hum Neurosci. 2012;6:341. doi:10.3389/fnhum.2012.00341
70. Stocco A, Baizabal-Carvallo JF. Deep brain stimulation for severe secondary stereotypies. Parkinsonism Related Disord. 2014;20(9):1035–1036. doi:10.1016/j.parkreldis.2014.06.019
71. Benedetti-Isaac JC, Torres-Zambrano M, Vargas-Toscano A, et al. Seizure frequency reduction after posteromedial hypothalamus deep brain stimulation in drug-resistant epilepsy associated with intractable aggressive behavior. Epilepsia. 2015;56(7):1152–1161. doi:10.1111/epi.13025
72. Segar DJ, Chodakiewitz YG, Torabi R, Cosgrove GR. Deep brain stimulation for the obsessive-compulsive and Tourette-like symptoms of Kleefstra syndrome. Neurosurgical Focus. 2015;38(6):E12. doi:10.3171/2015.3.FOCUS1528
73. Park HR, Kim IH, Kang H, et al. Nucleus accumbens deep brain stimulation for a patient with self-injurious behavior and autism spectrum disorder: functional and structural changes of the brain: report of a case and review of literature. Acta Neurochirurgica. 2017;159(1):137–143. doi:10.1007/s00701-016-3002-2
74. Doshi PK, Hegde A, Desai A. Nucleus accumbens deep brain stimulation for obsessive-compulsive disorder and aggression in an autistic patient: a case report and hypothesis of the role of nucleus accumbens in autism and comorbid symptoms. World Neurosurg. 2019;125:387–391. doi:10.1016/j.wneu.2019.02.021
75. Kakko K, Bjelogrlic-Laakso N, Pihlakoski L, Lehtimäki K, Järventausta K. tardive dyskinesia should not be overlooked. J Child Adolesc Psychopharmacol. 2019;29(1):72–74. doi:10.1089/cap.2018.0084
76. Davis RA, Winston H, Gault JM, Kern DS, Mikulich-Gilbertson SK, Abosch A. deep brain stimulation for ocd in a patient with comorbidities: epilepsy, tics, autism, and major depressive disorder. J Neuropsychiatry Clin Neurosci. 2021;33(2):167–171. doi:10.1176/appi.neuropsych.20060153
77. Graat I, Balke S, Prinssen J, et al. Effectiveness and safety of deep brain stimulation for patients with refractory obsessive compulsive disorder and comorbid autism spectrum disorder; A case series. J Affective Disorders. 2022;299:492–497. doi:10.1016/j.jad.2021.12.089
78. Wagner T, Valero-Cabre A, Pascual-Leone A. Noninvasive human brain stimulation. Annu. Rev. Biomed. Eng. 2007;9:527–565. doi:10.1146/annurev.bioeng.9.061206.133100
79. Pascual-Leone A, Tormos JM, Keenan J, Tarazona F, Cañete C, Catalá MD. Study and modulation of human cortical excitability with transcranial magnetic stimulation. J Clin Neurophysiol. 1998;15(4):333–343. doi:10.1097/00004691-199807000-00005
80. Suppa A, Huang YZ, Funke K, et al. Ten years of theta burst stimulation in humans: established knowledge, unknowns and prospects. Brain Stimulation. 2016;9(3):323–335. doi:10.1016/j.brs.2016.01.006
81. Pedapati EV, Gilbert DL, Erickson CA, et al. Abnormal cortical plasticity in youth with autism spectrum disorder: a transcranial magnetic stimulation case-control pilot study. J Child Adolesc Psychopharmacol. 2016;26(7):625–631. doi:10.1089/cap.2015.0183
82. Wang Y, Hensley MK, Tasman A, Sears L, Casanova MF, Sokhadze EM. Heart rate variability and skin conductance during repetitive tms course in children with autism. Applied Psychophysiology and Biofeedback. 2016;41(1):47–60. doi:10.1007/s10484-015-9311-z
83. Noda Y, Fujii K, Mimura Y, Taniguchi K, Nakajima S, Kitahata R. A case series of intermittent theta burst stimulation treatment for depressive symptoms in individuals with autistic spectrum disorder: real world tms study in the tokyo metropolitan area. J. Pers. Med. 2023;13(1).
84. Sousa B, Martins J, Castelo-Branco M, Gonçalves J. Transcranial Direct Current Stimulation as an Approach to Mitigate Neurodevelopmental Disorders Affecting excitation/inhibition balance: focus on autism spectrum disorder, schizophrenia, and attention deficit/hyperactivity disorder. J Clin Med. 2022;11(10):2839. doi:10.3390/jcm11102839
85. Nitsche MA, Cohen LG, Wassermann EM, et al. Transcranial direct current stimulation: state of the art 2008. Brain Stimul. 2008;1(3):206–223. doi:10.1016/j.brs.2008.06.004
86. Dmochowski JP, Datta A, Bikson M, Su Y, Parra LC. Optimized multi-electrode stimulation increases focality and intensity at target. J. Neural Eng. 2011;8(4):046011. doi:10.1088/1741-2560/8/4/046011
87. Vaquerizo-Serrano J, Salazar De Pablo G, Singh J, Santosh P. Catatonia in autism spectrum disorders: a systematic review and meta-analysis. European Psychiatry. 2021;65(1):e4. doi:10.1192/j.eurpsy.2021.2259
88. Fink M, Taylor MA, Ghaziuddin N. Catatonia in autistic spectrum disorders: a medical treatment algorithm. Int. Rev. Neurobiol. 2006;72:233–244.
89. Smith JR, Hopkins CE, Xiong J, Luccarelli J, Shultz E, Vandekar S. Use of ECT in Autism spectrum disorder and/or intellectual disability: a single site retrospective analysis. J Autism Dev Disord. 2024;54(3):963–982. doi:10.1007/s10803-022-05868-6
90. Amiet C, Gourfinkel-An I, Fau - Bouzamondo A, et al. Epilepsy in autism is associated with intellectual disability and gender: evidence from a meta-analysis. (1873-2402 (Electronic).
91. Dhossche DM, Shah A, Wing L. Blueprints for the assessment, treatment, and future study of catatonia in autism spectrum disorders. Int. Rev. Neurobiol. 2006;72:267–284.
92. Park YD. The effects of vagus nerve stimulation therapy on patients with intractable seizures and either Landau-Kleffner syndrome or autism. Epilepsy Behav. 2003;4(3):286–290. doi:10.1016/S1525-5050(03)00080-5
93. Levy ML, Levy KM, Hoff D, et al. Vagus nerve stimulation therapy in patients with autism spectrum disorder and intractable epilepsy: results from the vagus nerve stimulation therapy patient outcome registry. J Neurosurg Pediatr. 2010;5(6):595–602. doi:10.3171/2010.3.PEDS09153
94. Wang Z, Yuan X, Zhang Q, et al. Effects of stable vagus nerve stimulation efficacy on autistic behaviors in ten pediatric patients with drug resistant epilepsy: an observational study. Front. Pediatr. 2022;10:846301. doi:10.3389/fped.2022.846301
95. Danielsson S, Viggedal G, Gillberg C, Olsson I. Lack of effects of vagus nerve stimulation on drug-resistant epilepsy in eight pediatric patients with autism spectrum disorders: a prospective 2-year follow-up study. Epilepsy Behav. 2008;12(2):298–304. doi:10.1016/j.yebeh.2007.10.007
96. Abrams R. Electroconvulsive Therapy. Oxford University Press; 2002.
97. Espinoza RT, Kellner CH. Electroconvulsive Therapy. New Engl J Med. 2022;386(7):667–672. doi:10.1056/NEJMra2034954
98. Luccarelli J, McCoy TH Jr, Seiner SJ, Henry ME. Real-world evidence of age-independent electroconvulsive therapy efficacy: a retrospective cohort study. Acta Psychiatrica Scandinavica. 2022;145(1):100–108. doi:10.1111/acps.13378
99. Zamponi N, Rychlicki F, Corpaci L, Cesaroni E, Trignani R. Vagus nerve stimulation (VNS) is effective in treating catastrophic 1 epilepsy in very young children. Neurosurg. Rev. 2008;31(3):291–297. doi:10.1007/s10143-008-0134-8
100. Hauptman JS, Mathern GW. Vagal nerve stimulation for pharmacoresistant epilepsy in children. Surg. Neurol. Int. 2012;3(Suppl 4):S269–274. doi:10.4103/2152-7806.103017
101. Orosz I, McCormick D, Zamponi N, et al. Vagus nerve stimulation for drug-resistant epilepsy: a European long-term study up to 24 months in 347 children. Epilepsia. 2014;55(10):1576–1584. doi:10.1111/epi.12762
102. Hull MM, Madhavan D, Zaroff CM. Autistic spectrum disorder, epilepsy, and vagus nerve stimulation. Child’s Nervous System. 2015;31(8):1377–1385. doi:10.1007/s00381-015-2720-8
103. Grossman N, Bono D, Dedic N, et al. Noninvasive deep brain stimulation via temporally interfering electric fields. Cell. 2017;169(6):1029–1041.e1016. doi:10.1016/j.cell.2017.05.024
104. Müller R-A, Fishman I. Brain connectivity and neuroimaging of social networks in autism. Trends Cogn Sci. 2018;22(12):1103–1116. doi:10.1016/j.tics.2018.09.008
105. Sato M, Nakai N, Fujima S, Choe KY, Takumi T. Social circuits and their dysfunction in autism spectrum disorder. Mol Psychiatry. 2023;28(8):3194–3206. doi:10.1038/s41380-023-02201-0
106. Supekar K, Kochalka J, Schaer M, et al. Deficits in mesolimbic reward pathway underlie social interaction impairments in children with autism. Brain. 2018;141(9):2795–2805. doi:10.1093/brain/awy191
107. Griff JR, Langlie J, Bencie NB, et al. Recent advancements in noninvasive brain modulation for individuals with autism spectrum disorder. Neural Regen Res. 2023;18(6):1191–1195. doi:10.4103/1673-5374.360163
108. Wing L, Shah A. Catatonia in autistic spectrum disorders. Br J Psychiatry. 2000;176:357–362. doi:10.1192/bjp.176.4.357
109. Billstedt E, Gillberg C, Gillberg C. Autism after adolescence: population-based 13- to 22-year follow-up study of 120 individuals with autism diagnosed in childhood. J Autism Dev Disor. 2005;35(3):351–360. doi:10.1007/s10803-005-3302-5
110. Withane N, Dhossche DM. Electroconvulsive treatment for catatonia in autism spectrum disorders. Child Adolesc Psychiatr Clin N Am. 2019;28(1):101–110. doi:10.1016/j.chc.2018.07.006
111. Grob GN. Endocrine psychiatry: solving the riddle of melancholia. J. Hist. Med. Allied Sci. 2011;66(2):272–274. doi:10.1093/jhmas/jrq070
112. Madsen TM, Treschow A, Bengzon J, Bolwig TG, Lindvall O, Tingström A. Increased neurogenesis in a model of electroconvulsive therapy. Biol. Psychiatry. 2000;47(12):1043–1049. doi:10.1016/S0006-3223(00)00228-6
113. Lozano AM, Lipsman N. Probing and regulating dysfunctional circuits using deep brain stimulation. Neuron. 2013;77(3):406–424. doi:10.1016/j.neuron.2013.01.020
114. Lipsman N, Woodside DB, Giacobbe P, et al. Subcallosal cingulate deep brain stimulation for treatment-refractory anorexia nervosa: a Phase 1 pilot trial. Lancet. 2013;381(9875):1361–1370. doi:10.1016/S0140-6736(12)62188-6
115. Ballanger B, Lozano AM, Moro E, et al. Cerebral blood flow changes induced by pedunculopontine nucleus stimulation in patients with advanced Parkinson’s disease: a [(15)O] H2O PET study. Human Brain Mapp. 2009;30(12):3901–3909. doi:10.1002/hbm.20815
116. Yan H, Elkaim LM, Venetucci Gouveia F, et al. Deep brain stimulation for extreme behaviors associated with autism spectrum disorder converges on a common pathway: a systematic review and connectomic analysis. J Neurosurg. 2022;137(3):699–708. doi:10.3171/2021.11.JNS21928
117. Hughes JR, Melyn M. EEG and seizures in autistic children and adolescents: further findings with therapeutic implications. Clin EEG Neurosci. 2005;36(1):15–20. doi:10.1177/155005940503600105
118. Matsuo M, Maeda T, Sasaki K, Ishii K, Hamasaki Y. Frequent association of autism spectrum disorder in patients with childhood onset epilepsy. Brain Dev. 2010;32(9):759–763. doi:10.1016/j.braindev.2010.05.005
119. Hashimoto T, Sasaki M, Sugai K, Hanaoka S, Fukumizu M, Kato T. Paroxysmal discharges on EEG in young autistic patients are frequent in frontal regions. J. Med. Invest. 2001;48(3–4):175–180.
120. Holmes GL, Tian C, Hernan AE, Flynn S, Camp D, Barry J. Alterations in sociability and functional brain connectivity caused by early-life seizures are prevented by bumetanide. Neurobiol Dis. 2015;77:204–219. doi:10.1016/j.nbd.2015.02.015
121. Hernan AE, Holmes GL, Isaev D, Scott RC, Isaeva E. Altered short-term plasticity in the prefrontal cortex after early life seizures. Neurobiol Dis. 2013;50:120–126. doi:10.1016/j.nbd.2012.10.007
122. van Steenburgh JJ, Varvaris M, Schretlen DJ, Vannorsdall TD, Gordon B. Balanced bifrontal transcranial direct current stimulation enhances working memory in adults with high-functioning autism: a sham-controlled crossover study. Molecular Autism. 2017;8. doi:10.1186/s13229-017-0152-x
123. Engineer CT, Hays SA, Kilgard MP. Vagus nerve stimulation as a potential adjuvant to behavioral therapy for autism and other neurodevelopmental disorders. J. Neurodev. Disord. 2017;9(1):20. doi:10.1186/s11689-017-9203-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.