Back to Journals » Clinical Ophthalmology » Volume 19
Efficacy and Safety of Initial Outflow Reconstruction Using Ab Interno Microhook Trabeculotomy: A Retrospective Study in Secondary Glaucoma
Authors Aoyama Y, Aihara M, Sakata R ![]()
Received 13 July 2025
Accepted for publication 10 October 2025
Published 12 November 2025 Volume 2025:19 Pages 4219—4229
DOI https://doi.org/10.2147/OPTH.S553475
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yurika Aoyama, Makoto Aihara, Rei Sakata
Department of Ophthalmology, Graduate School of Medicine and Faculty of Medicine, The University of Tokyo, Tokyo, Japan
Correspondence: Rei Sakata, Department of Ophthalmology, Graduate School of Medicine and Faculty of Medicine, The University of Tokyo Hospital, 7-3-1 Hongo, Bunkyo-ku, Tokyo, 113-8655, Japan, Tel +81-3-3815-5411, Fax +81-3-3817-0798, Email [email protected]
Purpose: Establishing effective surgical interventions for secondary glaucoma (SG) remains a significant clinical challenge. We evaluated the efficacy and safety of initial outflow reconstruction using ab interno microhook trabeculotomy in patients with SG.
Patients and Methods: This retrospective study included 39 eyes from 39 patients who underwent either standalone microhooktrabeculotomy or a combined triple procedure with cataract surgery in 2021. The cohort consisted of 18 eyes with exfoliation glaucoma, 15 with uveitic glaucoma, and 6 with steroid-induced glaucoma. Intraocular pressure (IOP) and glaucoma medication scores were recorded preoperatively and at 1, 3, 6, and 12 months postoperatively. Primary outcomes included the IOP reduction rate at 12 months, assessed using mixed effects analysis, and IOP control over time, analyzed via Kaplan–Meier survival curves (failure defined as < 20% IOP reduction or IOP > 21 mmHg on two consecutive visits). Risk factors for surgical failure were analyzed using Cox proportional hazards models. Furthermore, postoperative complications and the need for additional surgical interventions were evaluated.
Results: The mean patient age was 65.1 ± 13.6 years, with 24 male participants. The mean preoperative IOP was 25.4 ± 9.3 mmHg, and the mean medication score was 4.2 ± 1.3 at 12 months postoperatively; these values significantly decreased to 14.9 mmHg and 3.1, respectively (P < 0.05). The mean IOP reduction rate at 12 months was 32.4%, and the Kaplan–Meier survival rate for IOP control was 60.3%. Cox hazard analysis indicated that older age and pseudophakia were associated with improved postoperative IOP control. The most common complication was anterior chamber hemorrhage (35.9%).
Conclusion: Ab interno microhook trabeculotomy may represent an effective initial surgical strategy for lowering IOP and reducing the reliance on glaucoma medications in patients with SG, particularly among older individuals and those with pseudophakia.
Keywords: microhook trabeculotomy, secondary glaucoma, intraocular pressure, medication score
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Haque has been published for this article.
Introduction
Glaucoma comprises a heterogeneous group of optic neuropathies characterized by progressive degeneration of the optic nerve head, ultimately resulting in irreversible visual field loss if left untreated. Secondary glaucoma (SG), a subset of glaucomatous disorders, develops in association with pre-existing ocular or systemic conditions, such as uveitis,1 steroid application (steroid-induced glaucoma: SIG),2 or exfoliation syndrome (exfoliation glaucoma: XFG),3 and is characterized by a more complex and multifactorial pathophysiology. These forms of glaucoma often involve increased resistance, as compared with eyes without such conditions, to aqueous humor outflow due to trabecular meshwork (TM) inflammation, fibrosis, and pigment deposition, diminishing the efficacy of pharmacologic treatment alone.4,5 Consequently, surgical intervention is frequently required to achieve and maintain adequate intraocular pressure (IOP) control.
Trabeculectomy remains the gold standard filtering procedure for most forms of glaucoma; however, in eyes where trabeculectomy carries a higher risk of failure or complications, glaucoma drainage devices are regarded as the preferred surgical option.6,7 However, these procedures are frequently associated with elevated complication rates due to heightened inflammatory responses and an increased propensity for postoperative scarring. Such factors can compromise bleb function and contribute to long-term surgical failure.8–10 In some instances, severe hypotony may ensue, leading to progressive deterioration of visual function. Therefore, minimally invasive glaucoma surgery (MIGS) has emerged as a less invasive and potentially safer alternative.11 MIGS is generally associated with shorter operative times, minimal tissue disruption, and a reduced risk of serious postoperative complications compared to traditional filtering surgeries.12–14
Among the various MIGS techniques, ab interno trabeculotomy using microhook has garnered increasing attention for its ability to enhance aqueous outflow by incising the TM and providing direct access to Schlemm’s canal, facilitating effective IOP reduction.15 This approach is designed to lower IOP without inducing significant hypotony and may decrease the dependence on topical antiglaucoma medications. Despite its increasing clinical adoption, studies evaluating the long-term efficacy and safety of ab interno trabeculotomy in SG patients remain limited.16,17 In particular, evidence regarding the durability of IOP control and the sustained reduction in medication burden remains insufficient.
Thus, we evaluated the efficacy of initial ab interno microhook trabeculotomy for secondary glaucoma, focusing on three subtypes, uveitic glaucoma, SIG, and XFG, with subgroup analyses by subtype. We also explored potential predictors of favorable IOP control to optimize patient selection and surgical outcomes, and assessed postoperative IOP and medication score changes stratified by baseline IOP.
Materials and Methods
This retrospective study reviewed the medical records of Japanese patients with glaucoma who underwent initial ab interno trabeculotomy using the Tanito Micro-hook (Inami & Co., Ltd., Japan) at the University of Tokyo Hospital (Tokyo, Japan) between 1 January and 31 December 2021. SG in this study was referred as glaucoma attributable to uveitis, steroid use, or exfoliation syndrome. In eyes with preoperative IOP less than 21 mmHg (10–20 mmHg), the surgery was indicated for cases in which the target IOP was not achieved or when patients developed intolerance or allergy to topical medications. Patients with a history of cataract surgery were included; however, patients with prior glaucoma surgery, vitreous surgery, SG due to other causes, primary angle closure glaucoma, or childhood glaucoma were excluded. Patients with a history of glaucoma laser treatments were included. No minimal duration of uveitis quiescence was required for inclusion in this study. The study was conducted in accordance with the Declaration of Helsinki. The Ethics Committee of the Graduate School of Medicine, The University of Tokyo, approved the study protocol (approval ID: 2217). Written informed consent was obtained from all participants.
Ophthalmic Examinations
At each visit, slit-lamp and fundus examinations were performed. Preoperative gonioscopy was conducted using a Sussman four-mirror or Goldmann two-mirror lens. IOP was measured with a calibrated Goldmann applanation tonometer after topical anesthesia in the seated position. Refractive error, axial length, and central corneal thickness (CCT) were assessed with an autorefractor keratometer, optical biometer, and specular microscope, respectively. Visual fields were tested within 6 months before surgery using the Humphrey SITA 24–2 program. Glaucoma severity was classified by mean deviation (MD): early (≥ –6 decibels [dB]), moderate (–6 to –12 dB), and advanced (≤ –12 dB).
Surgical Technique
Ab interno trabeculotomy was performed using a microhook. The procedure was conducted as follows. Following the instillation of topical anesthesia, a 2.4-mm temporal clear corneal incision was made. In eyes undergoing trabeculotomy alone, 1% Healon ophthalmic viscoelastic substance (AMO, Tokyo, Japan) was injected into the anterior chamber, and a nasal TM incision of ≥ 120 degrees was made under direct visualization using a Swan- Jacob gonioprism lens (Ocular Instruments, Bellevue, WA, USA). If peripheral anterior synechiae were present at the incision site, goniosynechialysis using Tanito microhook (Inami, Tokyo, Japan) was performed before completing the TM incision. Upon completion of the procedure, the viscoelastic material was removed by irrigation and aspiration, and IOP was normalized to physiological levels using balanced salt solution (BSS). In cases of triple surgery, cataract extraction was performed using the soft-shell technique with Shellgan 0.5 ophthalmic viscoelastic substance (Alcon, Tokyo, Japan). The sequence of cataract and glaucoma surgeries was determined at the discretion of the operating surgeon.
Postoperative Management
Postoperative management included topical administration of 0.1% betamethasone and moxifloxacin ophthalmic solution four times daily, along with 1% pilocarpine three times daily. In cases of combined surgery, 0.1% diclofenac sodium ophthalmic solution was administered twice daily. All eye drops, with the exception of diclofenac, were discontinued within 1 month postoperatively. When postoperative recurrence of inflammation was observed, topical steroids were restarted at the discretion of the treating physician. In instances of postoperative IOP elevation, additional antiglaucoma medications (type unspecified) were prescribed at the discretion of the surgeon.
Statistical Analysis
If both eyes underwent surgery, only the first operated eye was included in the analysis. IOP changes were evaluated for the entire cohort and further stratified by surgical procedure (single vs combined surgery). IOP and medication scores were assessed preoperatively and at 1 month (± 2 weeks), 3 months (± 2 weeks), 6 months (± 2 months), and 12 months (± 2 months) postoperatively. To assess postoperative complications, IOP was measured at 1 week following surgery to identify IOP spikes. In contrast, ocular hypotony is another potential complication that may appear late after surgery; therefore, it was monitored and confirmed at 1, 3, 6, and 12 months postoperatively.
Mixed effects analysis was used to compare IOP and medication scores between preoperative and postoperative time points. Absolute IOP reduction was defined as the difference between preoperative and postoperative IOP values. Survival analysis for IOP control at 12 months was conducted using Kaplan–Meier survival curves. Surgical failure was defined as not achieving the prespecified IOP target at two consecutive visits, in line with the 2024 AAO recommendations.18 Three thresholds based on IOP levels and reduction rates were applied:19 Criterion A was defined as an IOP ≤ 21 mmHg and/or a reduction of ≥ 20% from preoperative IOP with the use of glaucoma medications. Criterion B applied a stricter threshold of IOP ≤ 18 mmHg and/or ≥ 20% IOP reduction, whereas Criterion C further reduced the threshold to IOP ≤ 15 mmHg and/or ≥ 20% IOP reduction, both with the use of glaucoma medications. Any reoperation involving the same procedure, glaucoma filtration surgery, transscleral micropulse cyclophotocoagulation, or other ocular surgeries was also considered a surgical failure. Eyes that developed persistent hypotony or lost light perception were also categorized as failures.19 Risk factors associated with surgical failure were evaluated using Cox proportional hazards regression models. Covariates included age, sex, refractive error, glaucoma type (uveitic glaucoma, SIG, or XFG), postoperative lens status (phakic or pseudophakic), surgical technique (single or combined), baseline IOP, baseline medication score, and CCT. For medication scoring, fixed-combination eye drops were counted as two agents, and oral acetazolamide was counted as one. Postoperative complications, including re-inflammation, IOP spikes (defined as > 25 mmHg), hypotony (< 5 mmHg), and hyphema, were documented. The need for additional glaucoma surgery during the follow-up period was assessed.
The correlation coefficient between preoperative and 12-month postoperative IOP values was low (r = 0.045). Based on this, a power analysis indicated that, with 39 eyes, a paired t-test (α = 0.05, power = 0.80) could detect a minimal mean difference of approximately 5.8 mmHg. The observed mean IOP reduction from baseline to 12 months was 10.5 mmHg, exceeding this threshold. For between-subgroup comparisons, the uveitis (n = 15) vs XFG (n = 18) analysis required a difference of about 8.2 mmHg to achieve 80% power, whereas comparisons involving SIG (n = 6) would require even larger differences. Therefore, statistical analyses were conducted only between the Inflammatory and XFG groups using the chi-square test and the Wilcoxon rank-sum test.
Statistical analyses were performed using JMP Pro (version 17.0; SAS Institute, Cary, NC, USA), JMP Student Edition (version 18.0; SAS Institute, Cary, NC, USA), and SPSS Statistics (version 23.0; IBM Corp., Armonk, NY, USA). Mixed model analyses were conducted with SPSS, whereas the Wilcoxon rank-sum test and the chi-square tests were performed using JMP.
Results
In total, 40 patients who underwent standalone MIGS or combined cataract surgery were initially enrolled. One patient with a history of vitrectomy for a macular hole was excluded. Therefore, 39 eyes from 39 patients were included in the final evaluation. The cohort consisted of 24 males and 15 females, with a mean age of 65.1 ± 13.6 years. The mean preoperative IOP was 25.4 ± 9.3 mmHg, and the mean number of glaucoma medications used was 4.2 ± 1.3. Table 1 presents the demographics and baseline characteristics of the study participants.
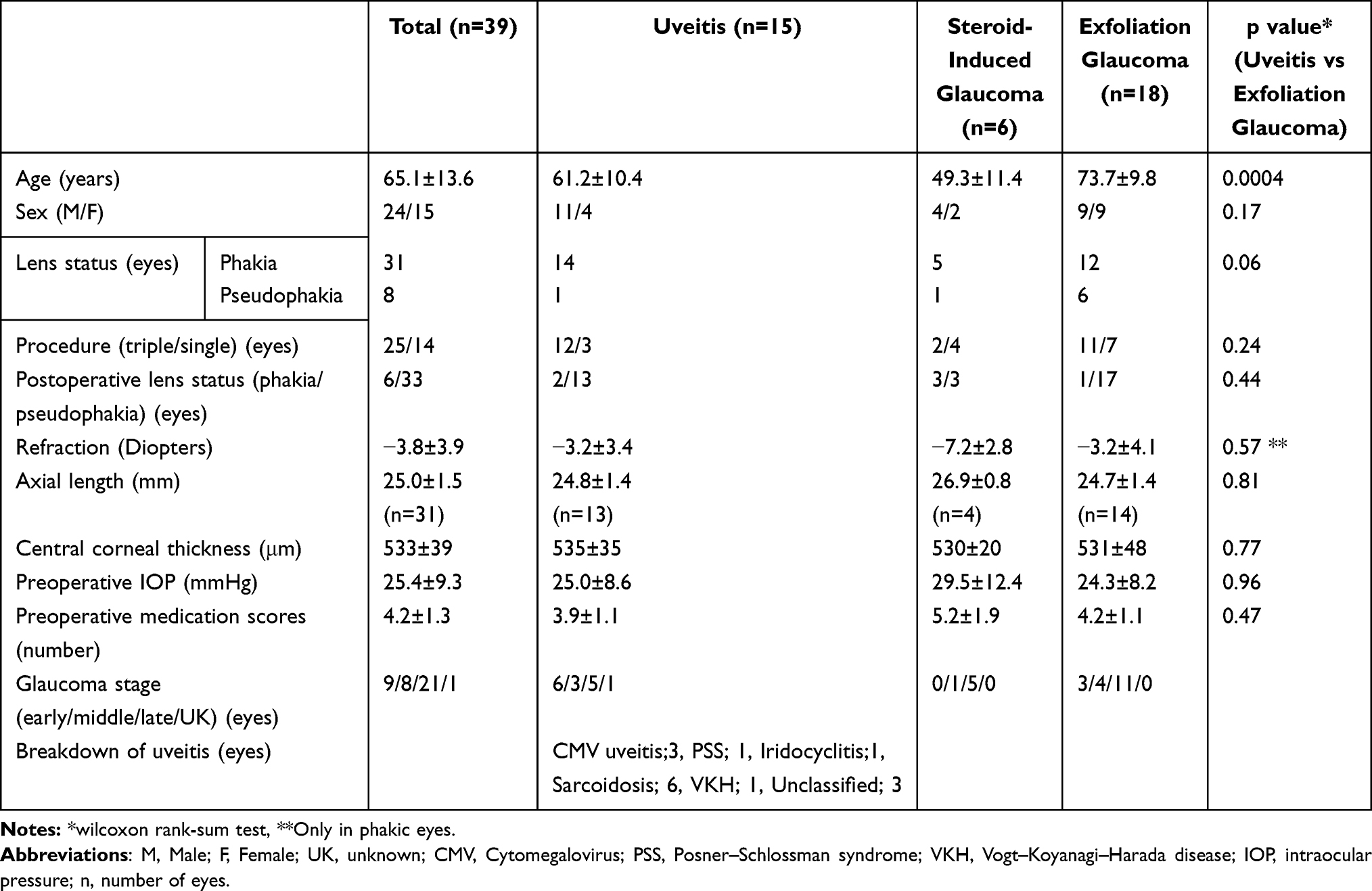 |
Table 1 Clinical Characteristics in Study Participants |
IOP and Medication Score
The mean postoperative IOP values at 1, 3, 6, and 12 months were 16.0 ± 6.5 (mean ± standard deviation), 14.9 ± 4.9, 14.2 ± 4.7, and 14.9 ± 5.5 mmHg, respectively. At 12 months, the mean IOP reduction rate was 32.4 ± 29.4%, representing a statistically significant decrease from baseline (p < 0.05, mixed effects analysis). Postoperative IOP was significantly lower than preoperative IOP at all evaluated time points (p < 0.05; Figure 1). However, no significant differences were observed between postoperative time points from 1 to 12 months. The mean number of glaucoma medications required at 1, 3, 6, and 12 months postoperatively was 2.5 ± 1.8, 3.2 ± 1.5, 3.4 ± 1.4, and 3.1 ± 1.5, respectively, representing a statistically significant decrease from baseline as well (p < 0.05). Similar to IOP, there were no significant differences in the number of medications between postoperative time points from 1 to 12 months.
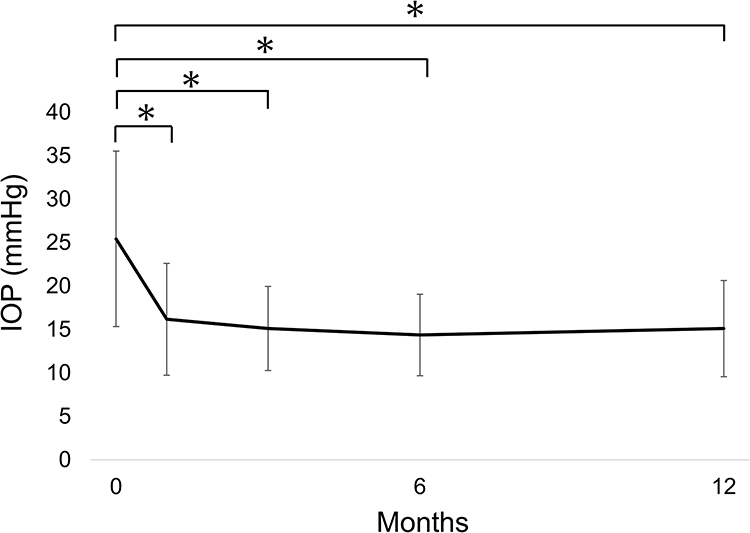 |
Figure 1 Time course of intraocular pressure before and after microhook trabeculotomy. A significant reduction in intraocular pressure (IOP) was observed at each postoperative follow-up compared to the preoperative baseline. Error bars indicate standard deviation. The y-axis represents IOP (mmHg), and the x-axis represents time (months). Asterisks (*) denote statistically significant differences from the baseline (P < 0.05). |
When stratified by baseline IOP into three groups (< 19, 20–29, and ≥ 30 mmHg), all groups exhibited a significant reduction in IOP at 12 months. Regarding the medication score, a significant overall reduction was observed in the entire 39 eyes. When stratified by baseline IOP, the medication scores significantly decreased in eyes with baseline IOP < 19 mmHg and ≥ 30 mmHg, whereas no significant change was observed in the 20–29 mmHg group (Table 2 and Figure 2). Postoperative IOP, IOP reduction, and medication score according to glaucoma subtype are presented in Table 3 and Figure 3. There was a significant reduction in both IOP and medication score before and after surgery (P < 0.05), except for the SIG group (P > 0.1).
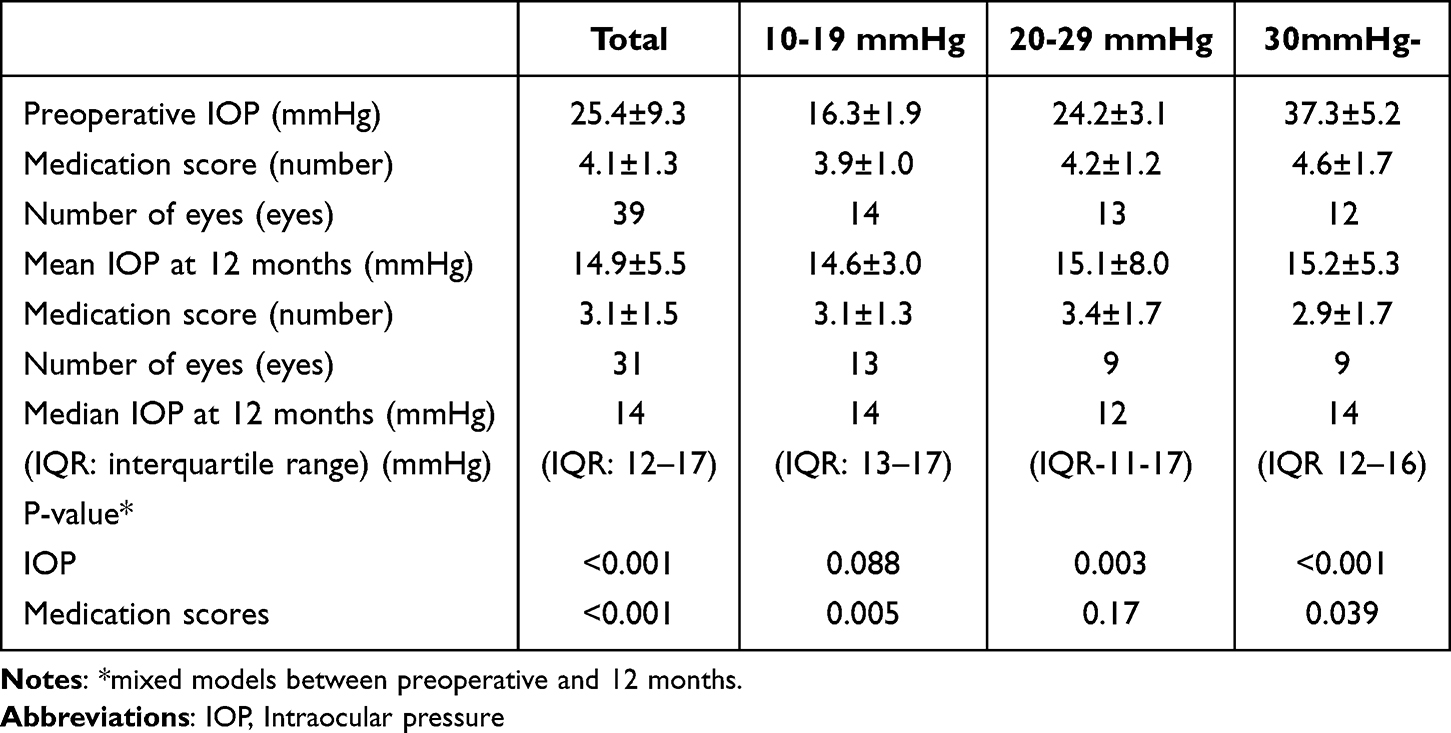 |
Table 2 Intraocular Pressure (IOP) and Medication Scores at Preoperative and 12 months, Stratified by Preoperative IOP Level |
 |
Table 3 Mean Intraocular Pressure and Medication Score Before and After the Surgery |
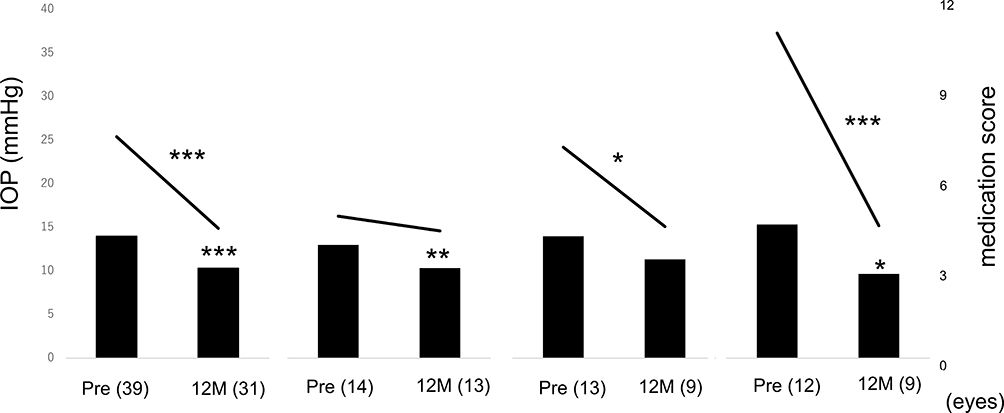 |
Figure 2 Mean intraocular pressure (IOP) and medication score before and after surgery, stratified by baseline IOP. The leftmost column represents the overall cohort; the second, third, and fourth columns represent subgroups with preoperative IOP of 10–19 mmHg, 20–29 mmHg, and ≥30 mmHg, respectively. Lines indicate intraocular pressure (scale on the left axis), and bars indicate medication score (scale on the right axis). Statistical significance is denoted as follows: *P < 0.05, **P < 0.01, ***P < 0.001. Pre = preoperative; 12M = 12 months after surgery. |
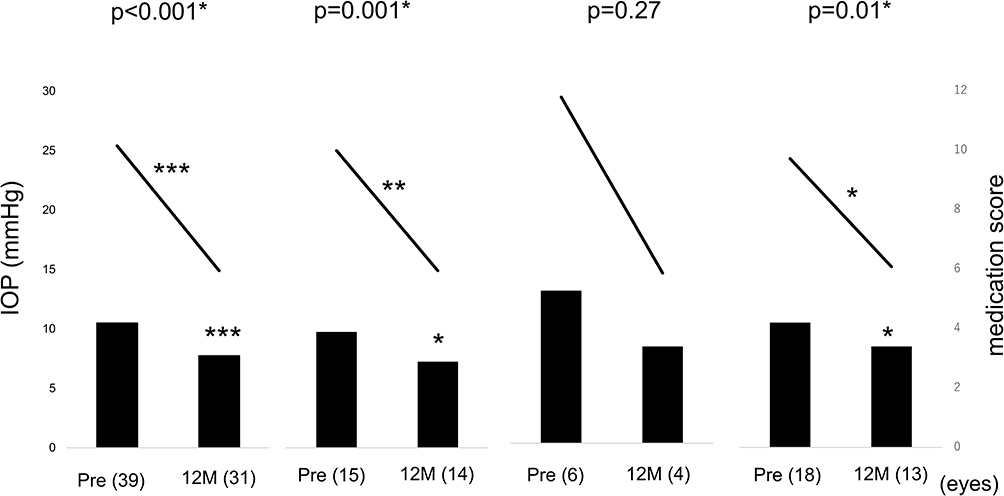 |
Figure 3 Mean intraocular pressure (IOP) and medication score before and after surgery, stratified by underlying disease. The leftmost column represents the overall cohort; the second, third, and fourth columns represent subgroups with uveitis, steroid-induced glaucoma, and exfoliation glaucoma, respectively. Lines indicate intraocular pressure (scale on the left axis), and bars indicate medication score (scale on the right axis). Statistical significance is denoted as follows: *P < 0.05, **P < 0.01, ***P < 0.001. Pre = preoperative; 12M = 12 months after surgery. |
Kaplan–Meier Survival Analysis
The cumulative survival, non-failure (surgical success) rates based on criterion A were 92.3%, 74.4%, 71.8%, and 60.3% at 1, 3, 6, and 12 months, respectively (Figure 4a). According to criterion B, the survival rates declined to 66.7% and 55.4% at 3 and 12 months, respectively (Figure 4b). Under criterion C, the survival rates were 61.5% and 50.1% at 3 and 12 months, respectively (Figure 4c). No statistically significant differences in survival were observed between groups under any criterion. As an additional glaucoma surgery, a total of four eyes underwent filtration procedures: one case each of SIG and inflammatory glaucoma, and two cases of XFG.
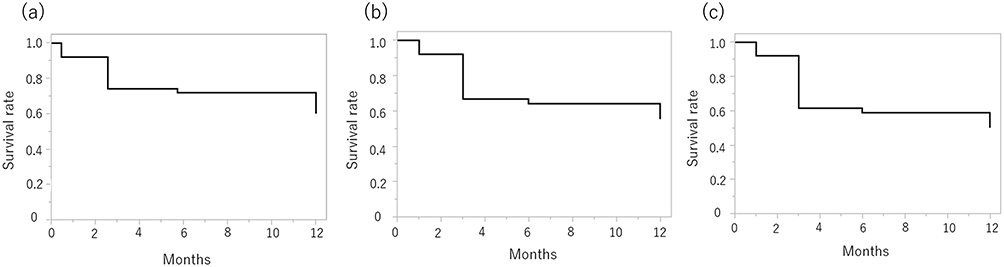 |
Figure 4 (a–c) Kaplan–Meier survival analysis based on different intraocular pressure (IOP) control criteria. The horizontal axis indicates time (months), and the vertical axis shows the cumulative survival probability. (a) Criterion A – defined as IOP ≤ 21 mmHg and/or ≥ 20% reduction from preoperative IOP with glaucoma medications. (b) Criterion B – defined as IOP ≤ 18 mmHg and/or ≥ 20% reduction from preoperative IOP with glaucoma medications. (c) Criterion C – defined as IOP ≤ 15 mmHg and/or ≥ 20% reduction from preoperative IOP with glaucoma medications. |
Cox Proportional Hazards Analysis
Table 4 presents the results of univariate and multivariate Cox regression analyses for criteria A, B, and C. Under criteria B and C, older age and pseudophakic status were associated with improved IOP control. In the multivariate model, age demonstrated a hazard ratio (HR) of 0.98 (95% confidence interval [CI] 0.94–1.16), whereas pseudophakia (compared to phakia) exhibited an HR of 0.36 (95% CI 0.11–1.18), indicating a potential confounding effect.
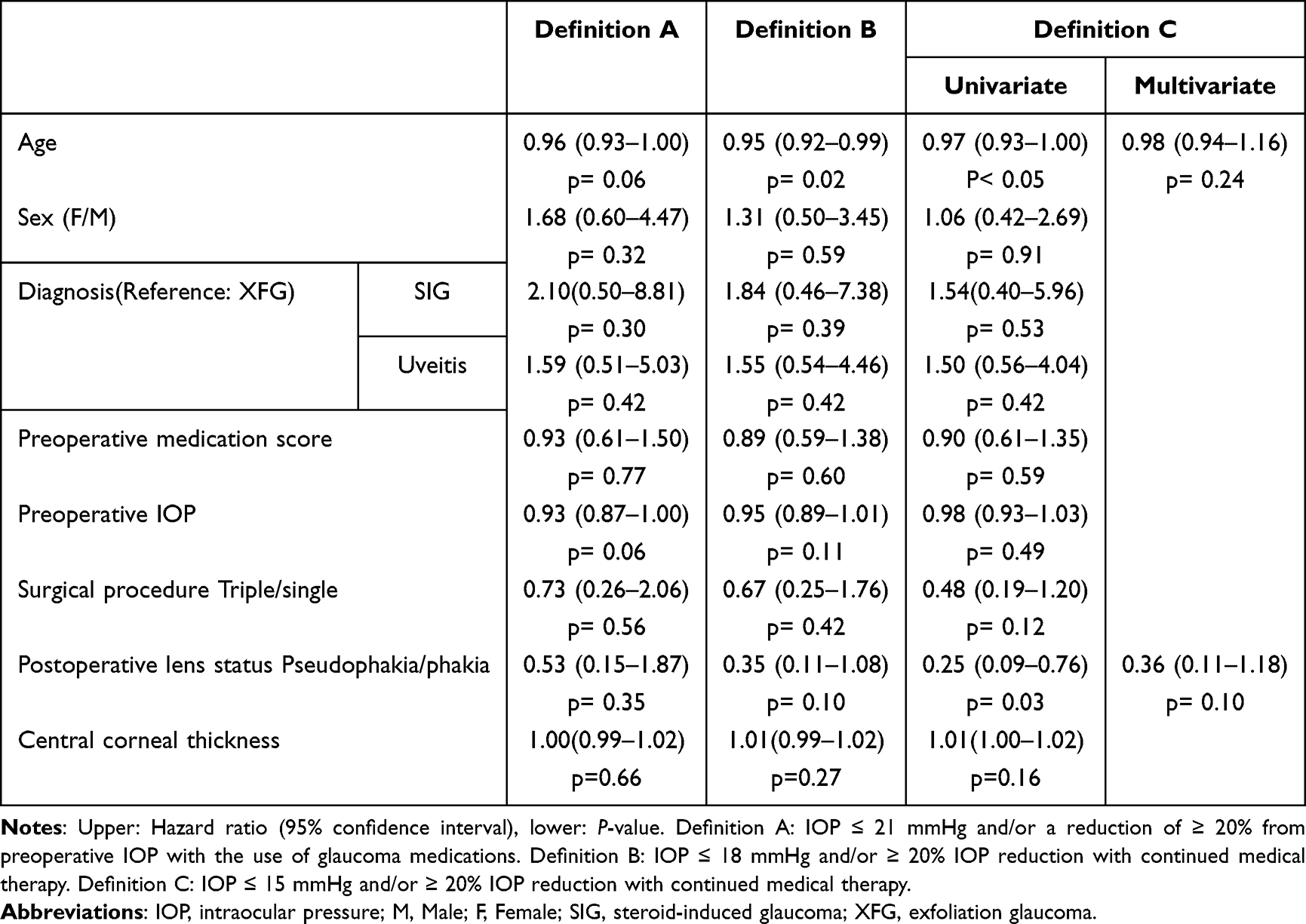 |
Table 4 Results of Cox’s Proportional Hazard Model Analysis of Postoperative IOP Control After Surgery |
Postoperative Complications
Postoperative complications are summarized in Table 5. The most common adverse event was anterior chamber hemorrhage (14 eyes out of 39 eyes, 35.9%). Transient IOP spikes were observed in seven eyes, with one requiring subsequent filtration surgery. In addition, one patient with sarcoidosis developed iritis at 2 months postoperatively, which resolved with topical betamethasone 0.1%.
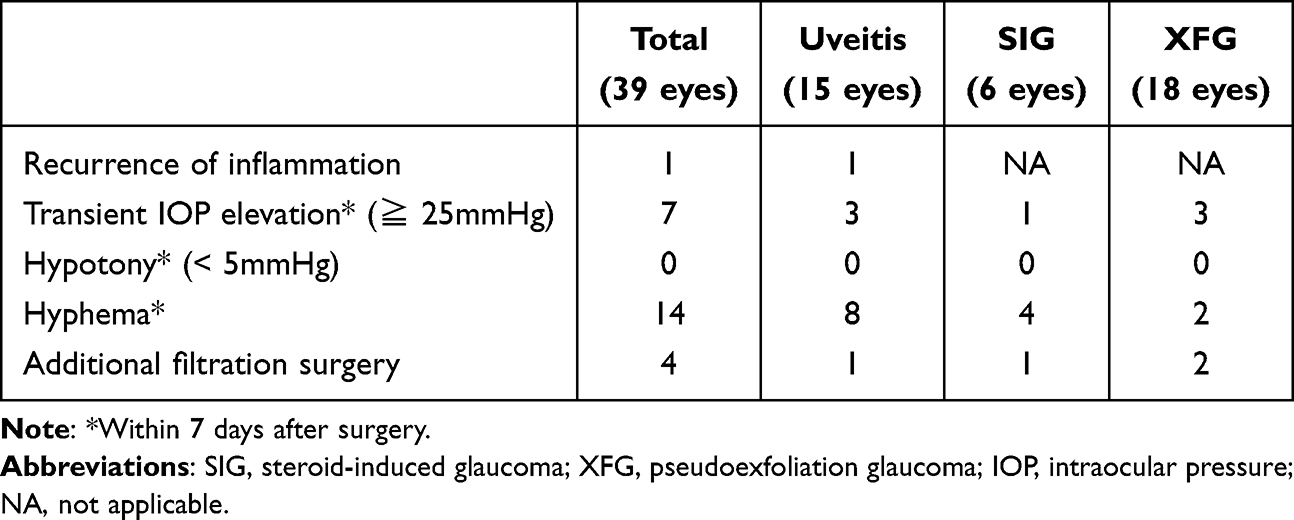 |
Table 5 Complications and Additional Procedure After Surgery |
Discussion
We evaluated the postoperative outcomes of initial ab interno trabeculotomy using the microhook technique in 39 eyes diagnosed with XFG, uveitic glaucoma, and SIG. Over a 12-month follow-up period, the mean IOP decreased significantly from 25.4 ± 9.3 mmHg preoperatively to 14.9 ± 5.5 mmHg postoperatively. Four eyes required additional glaucoma surgery. The 12-month success rate, defined as an IOP reduction of ≥ 20%, an IOP < 22 mmHg, and no more than one glaucoma medication, was 60.3%.
Although the heterogeneity of underlying diseases and variability in follow-up durations complicate direct comparisons, our findings differ from those reported in previous studies. Okeke et al reported success rates of 94% for triple ablation and 79% for single ablation MIGS procedures in a large cohort (n = 658).4 Similarly, Dang et al reported an 86% success rate in SIG,20 and Swamy et al reported a 91% success rate in uveitic glaucoma.21 Sotani et al reported a 67% success rate using the hook technique in uveitic glaucoma,22 whereas Kawaii et al23 and Kitahara et al24 reported success rates of 83% and 100%, respectively, in amyloidosis. The relatively lower success rate in our study may be attributable to the inclusion of heterogeneous glaucoma subtypes, particularly XFG, which is associated with increased post-trabecular outflow resistance. However, the mean postoperative IOP of 14.9 ± 5.5 mmHg in our cohort was consistent with previously reported values, which ranged from 13.8 ± 3.9 to 16.7 ± 4.6 mmHg.21,24 These findings emphasize the practicality and effectiveness of MIGS, particularly for patients with moderate target IOPs or those for whom filtration surgery is contraindicated or undesirable. In addition, subgroup analysis showed a significant reduction in glaucoma medication burden in eyes with preoperative IOP < 20 mmHg, whereas IOP reduction was not statistically significant. These results indicate potential benefits of MIGS even in cases with lower baseline IOP.
Comparative analyses of MIGS efficacy between SG, such as SIG, XFG, and primary open-angle glaucoma (POAG), have yielded heterogeneous and sometimes conflicting findings. Dang et al reported that Trabectome ab interno trabeculotomy resulted in a significantly greater IOP reduction in SIG compared to POAG, indicating that pathophysiological differences in outflow resistance may influence surgical outcomes.20 Similarly, Okeke et al, in a large cohort study, observed higher surgical success rates in XFG than in POAG, potentially due to more pronounced TM dysfunction and the accumulation of exfoliative material in XFG, which may enhance the efficacy of MIGS.4
Conversely, other investigations have reported contrasting findings. Sakai et al observed significantly lower 1-year survival rates following MIGS in SG compared to POAG,25 suggesting that the complex and multifactorial nature of SG, including inflammatory components in uveitic glaucoma and steroid responsiveness, may undermine long-term surgical efficacy. In addition, Kuusniemi et al and Murata et al found no statistically significant differences in success rates among POAG, XFG, SG, and uveitic glaucoma cohorts;26,27 these findings imply that factors such as patient selection, surgical technique, and perioperative management may play a more critical role in determining outcomes than the glaucoma subtype itself.
Several prognostic factors influencing MIGS outcomes in SG have been reported. While combined cataract surgery has been associated with favorable results, factors such as White race (relative to Hispanic, Asian, and African American patients) and prolonged preoperative use of glaucoma medications have been identified as negative predictors.4,28 Although a study found no significant association between age or baseline IOP and surgical survival,23 other reports have indicated that older age and concurrent cataract surgery are favorable prognostic factors.27,29 In our study, neither combined cataract surgery nor the SG subtype significantly affected surgical survival. However, under stricter IOP control criteria, older age and pseudophakia were associated with improved outcomes, consistent with previous findings.
It is well established that the efficacy of MIGS diminishes over time, and from a long-term perspective, IOP control in younger patients may be more challenging compared to elderly patients. In the present study, the proportion of XFG, which is more common in older individuals, was relatively high. This may have contributed to an overestimation of the surgical effectiveness. Furthermore, age-related accumulation of extracellular matrix components is known to increase aqueous outflow resistance, with various regions of the trabecular meshwork contributing equally to this resistance.30 Therefore, the observed IOP-lowering effect of trabecular meshwork incision using a microhook may have been more pronounced in elderly eyes. In pseudophakic eyes, the IOP-lowering effect of cataract surgery31 may act synergistically with MIGS procedures, further enhancing the overall prognosis. However, the inclusion of heterogeneous SG subtypes and the limited sample size may have reduced the statistical power of our analyses.
The choice between MIGS and trabeculectomy remains clinically important, especially in advanced cases or eyes with very high IOP. Although MIGS is less invasive and less predictable, our findings suggest it may still be a reasonable treatment option in selected patients.
Our study has several limitations. It was retrospective with a relatively short 12-month follow-up, and some patients discontinued or transferred care, though most had well-controlled IOP at their last visits, suggesting our results may underestimate surgical success. The sample size was small, particularly in the SIG group, reflecting diagnostic challenges in distinguishing it from inflammatory glaucoma. In addition, the MIGS procedure assessed was limited to microhook trabeculotomy, so the findings may not extend to device-based MIGS such as iStent or Hydrus. Nevertheless, the microhook technique avoids device-related occlusion and may offer specific advantages in these cases. This method is gaining international acceptance,32 and the present study may contribute to the growing body of evidence supporting its clinical utility. Also, the absence of POAG cases precluded evaluation of the specific postoperative characteristics of uveitic glaucoma, SIG, and XFG in comparison with POAG. Previous reports of microhook trabeculotomy in secondary glaucoma generally focused on a single disease entity. In this study, we examined three common types—uveitic, steroid-induced, and exfoliation glaucoma—where IOP elevation is mainly due to increased resistance in the conventional outflow pathway. Microhook trabeculotomy achieved significant pressure reduction across these conditions. Although the sample size, particularly for steroid-induced glaucoma, was small, our findings suggest applicability to a broader spectrum of secondary glaucoma. Further large-scale studies are needed to confirm these results and identify disease-specific predictors.
Conclusion
Microhook trabeculotomy for SG demonstrated consistent IOP reduction and a decrease in the number of glaucoma medications required over 1 year, suggesting that it may serve as a viable surgical option. Improved IOP control is particularly anticipated in elderly patients and those with an intraocular lens.
Funding
This work was partially supported by a clinical trial grant (Y.A.) from Takeda Development Center Americas, Inc.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kesav N, Palestine AG, Kahook MY, et al. Current management of uveitis-associated ocular hypertension and glaucoma. Surv Ophthalmol. 2020;65(4):397–407. doi:10.1016/j.survophthal.2019.12.003
2. Roberti G, Oddone F, Agnifili L, et al. Steroid-induced glaucoma: epidemiology, pathophysiology, and clinical management. Surv Ophthalmol. 2020;65(4):458–472. doi:10.1016/j.survophthal.2020.01.002
3. Pose-Bazarra S, López-Valladares MJ, López-de-Ullibarri I, et al. Surgical and laser interventions for pseudoexfoliation glaucoma systematic review of randomized controlled trials. Eye. 2021;35(6):1551–1561. doi:10.1038/s41433-021-01424-1
4. Okeke CO, Miller-Ellis E, Rojas M. Trabectome success factors. Medicine. 2017;96(24):e7061. doi:10.1097/MD.0000000000007061
5. Buffault J, Labbé A, Hamard P, et al. The trabecular meshwork: structure, function and clinical implications. A review of the literature. J Fr Ophtalmol. 2020;43(7):e217–e30. doi:10.1016/j.jfo.2020.05.002
6. Zhang X, Wang B, Liu R, et al. The effectiveness of AGV, Ex-PRESS, or trabeculectomy in the treatment of primary and secondary glaucoma: a systematic review and network meta-analysis. Ann Palliat Med. 2022;11(1):321–331. doi:10.21037/apm-21-3968
7. European glaucoma society terminology and guidelines for glaucoma. 4th Edition - chapter 3: treatment principles and options supported by the EGS foundation: part 1: foreword; introduction; glossary; chapter 3 treatment principles and options. Br J Ophthalmol. 2017;101(6):130–195. doi:10.1136/bjophthalmol-2016-EGSguideline.003
8. Lee SY, Kim YH, Kim KE, et al. Comparison of surgical outcomes between trabeculectomy with mitomycin C and Ahmed valve implantation with mitomycin c in eyes with uveitic glaucoma. J Clin Med. 2022;11.
9. Li F, Tang G, Zhang H, et al. The effects of trabeculectomy on pseudoexfoliation glaucoma and primary open-angle glaucoma. J Ophthalmol. 2020;2020:1723691. doi:10.1155/2020/1723691
10. Senthil S, Rao HL, Ali MH, et al. Long-term outcomes and risk factors for failure of glaucoma filtering surgery in eyes with vernal keratoconjunctivitis and steroid-induced glaucoma. Indian J Ophthalmol. 2022;70(3):820–825. doi:10.4103/ijo.IJO_1897_21
11. Chihara E, Hamanaka T. Historical and contemporary debates in schlemm’s canal-based MIGS. J Clin Med. 2024;13.
12. Paik B, Chua CH, Yip LW, et al. Outcomes and complications of minimally invasive glaucoma surgeries (MIGS) in primary angle closure and primary angle closure glaucoma: a systematic review and meta-analysis. Clin Ophthalmol. 2025;19:483–506. doi:10.2147/OPTH.S505856
13. Fellman RL, Mattox C, Singh K, et al. American glaucoma society position paper: microinvasive glaucoma surgery. Ophthalmol Glaucoma. 2020;3(1):1–6. doi:10.1016/j.ogla.2019.12.003
14. Lavia C, Dallorto L, Maule M, et al. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: a systematic review and meta-analysis. PLoS One. 2017;12(8):e0183142. doi:10.1371/journal.pone.0183142
15. Tanito M, Matsuo M. Ab-interno trabeculotomy-related glaucoma surgeries. Taiwan J Ophthalmol. 2019;9(2):67–71. doi:10.4103/tjo.tjo_38_19
16. Iwao K, Inatani M, Tanihara H. Success rates of trabeculotomy for steroid-induced glaucoma: a comparative, multicenter, retrospective cohort study. Am J Ophthalmol. 2011;151(6):1047–56.e1. doi:10.1016/j.ajo.2010.11.028
17. Chen RI, Purgert R, Eisengart J. Gonioscopy-assisted transluminal trabeculotomy and goniotomy, with or without concomitant cataract extraction, in steroid-induced and uveitic glaucoma: 24-month outcomes. J Glaucoma. 2023;32(6):501–510. doi:10.1097/IJG.0000000000002183
18. Gedde SJ, Vinod K, Bowden EC, et al. Special commentary: reporting clinical endpoints in studies of minimally invasive glaucoma surgery. Ophthalmology. 2025;132(2):141–153. doi:10.1016/j.ophtha.2024.07.030
19. Mathew DJ, McKay BR, Basilious A, et al. Adherence to world glaucoma association guidelines for surgical trials in the era of microinvasive glaucoma surgeries. Ophthalmol Glaucoma. 2019;2(2):78–85. doi:10.1016/j.ogla.2019.01.007
20. Dang Y, Kaplowitz K, Parikh HA, et al. Steroid-induced glaucoma treated with trabecular ablation in a matched comparison with primary open-angle glaucoma. Clin Exp Ophthalmol. 2016;44(9):783–788. doi:10.1111/ceo.12796
21. Swamy R, Francis BA, Akil H, et al. Clinical results of ab interno trabeculotomy using the trabectome in patients with uveitic glaucoma. Clin Exp Ophthalmol. 2020;48(1):31–36. doi:10.1111/ceo.13639
22. Sotani N, Kusuhara S, Matsumiya W, et al. Outcomes of microhook ab interno trabeculotomy in consecutive 36 eyes with uveitic glaucoma. J Clin Med. 2022;11(13):3768. doi:10.3390/jcm11133768
23. Kawaji T, Sato T. Suture trabeculotomy ab interno for secondary glaucoma in Japanese patients with Val30Met hereditary transthyretin amyloidosis. Sci Rep. 2022;12(1):19330. doi:10.1038/s41598-022-23150-8
24. Kitahara J, Kakihara S, Hirano T, et al. Microhook ab interno trabeculotomy for secondary glaucoma in patients with hereditary transthyretin amyloidosis. Japan J Ophthalmol. 2023;67(1):84–90. doi:10.1007/s10384-022-00966-5
25. Sakai D, Fujihara M, Yokota S, et al. One-year outcomes and predictable factors for microhook ab interno trabeculotomy. Int J Ophthalmol. 2022;15(4):598–603. doi:10.18240/ijo.2022.04.12
26. Kuusniemi AM, Lindbohm N, Allinen P, et al. Ab interno trabeculotomy: key prognostic factors. J Glaucoma. 2020;29(3):211–216. doi:10.1097/IJG.0000000000001432
27. Murata N, Takahashi E, Saruwatari J, et al. Outcomes and risk factors for ab interno trabeculotomy with a Kahook Dual Blade. Graefes Arch Clin Exp Ophthalmol. 2023;261(2):503–511. doi:10.1007/s00417-022-05799-z
28. Okuda M, Mori S, Takano F, et al. Association of the prolonged use of anti-glaucoma medications with the surgical failure of ab interno microhook trabeculotomy. Acta Ophthalmol. 2022;100(6):e1209–e15. doi:10.1111/aos.15090
29. Kaplowitz K, Bussel II, Honkanen R, et al. Review and meta-analysis of ab-interno trabeculectomy outcomes. Br J Ophthalmol. 2016;100(5):594–600. doi:10.1136/bjophthalmol-2015-307131
30. Miyazaki M, Segawa K, Urakawa Y. Age-related changes in the trabecular meshwork of the normal human eye. Japan J Ophthalmol. 1987;31(4):558–569.
31. Mansberger SL, Gordon MO, Jampel H, et al. Reduction in intraocular pressure after cataract extraction: the ocular hypertension treatment study. Ophthalmology. 2012;119(9):1826–1831. doi:10.1016/j.ophtha.2012.02.050
32. Maheshwari D, Grover DS, Ramakrishnan R, et al. Early outcomes of combined phacoemulsification and ab interno tanito microhook trabeculotomy in open-angle glaucoma. Ophthalmol Glaucoma. 2024;7(2):123–130. doi:10.1016/j.ogla.2023.10.007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors and Management of Intraocular Pressure Elevation After Vitrectomy Combined with Silicone Oil Tamponade
Ge L, Su N, Fan W, Yuan S
International Journal of General Medicine 2024, 17:447-456
Published Date: 3 February 2024
Intraocular Pressure and Cup-to-Disc Ratio Asymmetry in Diagnosing Iris Melanoma
Kong AW, Au A, Song W, Oh AJ, McCannel TA
Clinical Ophthalmology 2024, 18:2907-2915
Published Date: 16 October 2024