Back to Journals » Journal of Pain Research » Volume 18
Efficacy and Safety Comparison of Ulinastatin versus Flurbiprofen Axetil for Preemptive Analgesia in Reducing Opioid Burden After Total Knee Arthroplasty: A Randomized Controlled Trial [Response to Letter]
Received 13 December 2025
Accepted for publication 19 December 2025
Published 31 December 2025 Volume 2025:18 Pages 7195—7197
Di Wang,1 Yan Li1,2
1College of Anesthesiology, Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 2Tianjin Jizhou People’s Hospital, Fifth Teaching Hospital of Tianjin University of TCM, Jizhou District, Tianjin, People’s Republic of China
Correspondence: Yan Li, School of Anesthesiology, Shanxi Medical University, No. 56 Xinjian South Road, Yingze District, Taiyuan, Shanxi, 030001, People’s Republic of China, Email [email protected]
View the original paper by Ms Wang and colleagues
This is in response to the Letter to the Editor
Dear Editorial Team
Thank you for the opportunity to respond to the Letter to the Editor by Wu M and Ye Y regarding our manuscript titled
Efficacy and Safety Comparison of Ulinastatin Versus Flurbiprofen Axetil for Preemptive Analgesia in Reducing Opioid Burden After Total Knee Arthroplasty: A Randomized Controlled Trial published in the Journal of Pain Research.
We have carefully reviewed the comments and appreciate the thoughtful feedback provided by the readers. Below, we have prepared a point-by-point response to address the concerns raised.
Response to the Letter
Dose Selection and Correction of Ulinastatin (UTI) Dosage Error
We fully acknowledge the comment regarding the reported UTI dosage. The value “30 IU” was indeed an error; the correct dosage is 300,000 IU. This inaccuracy resulted from a unit conversion oversight during manuscript preparation (omission of the term “万” [ten-thousand]). We sincerely apologize for this error and will correct it promptly in the final revised manuscript.
- Rationale for Dose Selection: The single preoperative dose of 300,000 IU was selected based on established clinical practice and pharmacological studies. Multiple references indicate that the commonly used clinical dosage of UTI ranges between 100,000 and 500,000 IU (or 10,000 U/kg).1–4 Furthermore, preclinical studies using a rat incisional pain model demonstrated that a single preoperative dose within this range effectively reduced postoperative mechanical hypersensitivity.5 Our own pilot data confirmed that this dosage offered an optimal balance between efficacy and safety.
- Future Refinement: We agree with the suggestion to include multiple dosing groups (eg, 100,000 IU, 300,000 IU, 500,000 IU) in future trials to identify the optimal regimen. Additionally, incorporating pharmacokinetic data (eg, plasma concentration-time curves) would further substantiate dose justification.
Imbalance in Stroke History After Randomization
We acknowledge the observed imbalance in stroke history between the flurbiprofen axetil (FA) group (20%) and the control group (2%). Although the trial was double-blinded and randomized, this discrepancy could potentially confound secondary outcomes such as delirium incidence. Below we provide a point-by-point response:
- Stringent Exclusion Criteria: Our protocol explicitly excluded patients with “uncontrolled major depression (PHQ-9 ≥20) or cognitive impairment (MMSE ≤24).” This effectively precluded enrollment of individuals with recent (within 6 months) or symptomatic stroke that could contribute to cognitive sequelae.
- Context from Overall Baseline Data: The overall prevalence of stroke history in the study cohort was 12.2%. Although the FA group showed a higher rate (20%), this difference was not statistically significant compared to the UTI group. Given that our exclusion criteria minimized the inclusion of patients with stroke likely to affect cognitive outcomes, we believe this imbalance did not materially alter the conclusion that UTI reduces postoperative delirium.
- Supporting Outcome Data: The incidence of delirium was significantly lower in the UTI group (4.1%) than in both the control (30.0%, p = 0.001) and FA (18.0%, p = 0.028) groups, whereas no significant difference was observed between FA and control (p = 0.160).
- Adoption of Reviewer’s Suggestion: We fully agree that further stratified analysis is necessary to ensure robustness. Accordingly, we have performed a post hoc stratification based on stroke history (see Table 1).
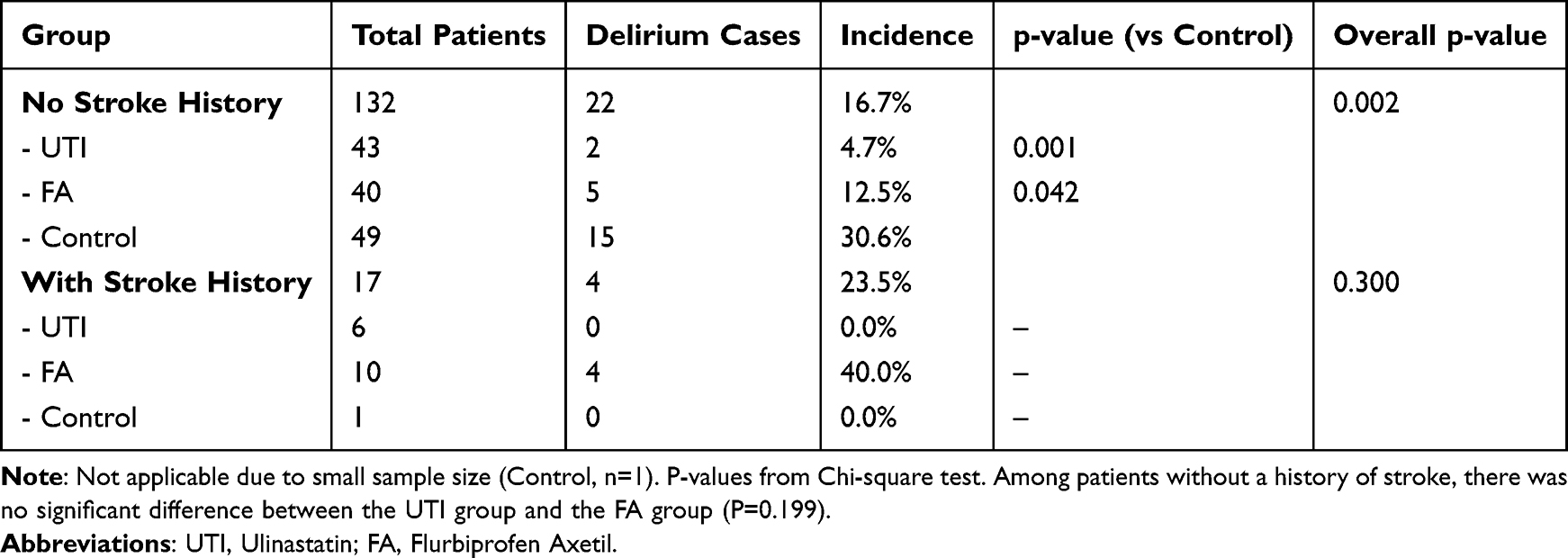 |
Table 1 Comparison of the Incidence of Postoperative Delirium Among Groups After Stratification by Stroke History |
To further assess the influence of stroke history imbalance, we conducted the following supplementary analyses:
In patients without a history of stroke (most patients), the result is clear: the UTI group significantly reduced delirium compared to both the FA and Control group. In the very small group of patients with a history of stroke, the sample size is too small (especially the control group, n=1) to draw any reliable conclusions. The data here is inconclusive.
Conclusion: The finding that Ulinastatin (UTI) reduces the incidence of delirium is robust and is based on the analysis of the larger, clinically relevant subgroup of patients without a prior history of stroke. The observed baseline imbalance does not alter this main conclusion. Even when accounting for the potential confounding effect of stroke history through stratified analysis, the core conclusion—that UTI significantly lowers the risk of postoperative delirium—remains valid.
Limitations in Analgesia Assessment
We appreciate the comment regarding the potential “ceiling effect” of VAS scores, which may have limited their ability to reflect true differences in pain experience.
- Supplementary explanation of the research conclusion: The primary endpoint of this study was morphine consumption rather than VAS score. Therefore, the conclusion that “the analgesic effect of the UTI group was not inferior to that of the control group” was mainly based on the morphine sparing effect. The absence of difference in VAS scores may result from the active adjustment of the standardized PCIA protocol (target VAS ≤30 mm), rather than the ineffectiveness of analgesia.
- Future Refinement: We agree that future trials should incorporate additional measures such as frequency of breakthrough pain, number of PCIA attempts/effective deliveries, and patient-reported outcomes (eg, QoR-15). Although these were not systematically recorded in this study, we will explicitly address this limitation in the Discussion.
Thank you again for these insightful comments, which have greatly enhanced the rigor of our research and the clarity of our report. We believe our responses clarify the concerns raised and hope they contribute to a constructive discussion around our findings. Thank you again for facilitating this scholarly exchange.
Disclosure
The authors declare no conflicts of interest in this communication.
References
1. Abraham P, Rodriques J, Moulick N, et al. Efficacy and safety of intravenous ulinastatin versus placebo along with standard supportive care in subjects with mild or severe acute pancreatitis. J Assoc Physicians India. 2013;61(8):535–538.
2. Chen F, Xu Y, Wang Z. Ulinastatin combined with somatostatin enhances disease control and modulates serum inflammatory factors in patients with severe pancreatitis. Am J Transl Res. 2023;15(9):5797–5807.
3. Wang SQ, Jiao W, Zhang J, et al. Ulinastatin in the treatment of severe acute pancreatitis: a single-center randomized controlled trial. World J Clin Cases. 2023;11(19):4601–4611.
4. Nawan A, Wu Z, Jiang B, Wang G, Zhang W, Feng Y. Effect of combination of multiple anti-inflammatory drugs strategy on postoperative delirium among older patients undergoing Hip fracture surgery: a pilot randomized controlled trial. BMC Med. 2025;23(1):108. doi:10.1186/s12916-025-03946-x
5. Guo ZB, Tang L, Wang LP, et al. The analgesic effects of ulinastatin either as a single agent or in combination with sufentanil: a novel therapeutic potential for postoperative pain. Eur J Pharmacol. 2021;907:174267. doi:10.1016/j.ejphar.2021.174267
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.