Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Efficacy and Safety Analysis of Transarterial Chemoembolization Combined with Sintilimab Plus Bevacizumab Biosimilar in the Treatment of Unresectable Hepatocellular Carcinoma
Authors Qin H, Jiang K ![]() , Liu C
, Liu C ![]() , Lin H
, Lin H ![]() , Xia J, Ya H, Gu J, Suo L, Li B, Deng X, Wang D, Huang X, Li S
, Xia J, Ya H, Gu J, Suo L, Li B, Deng X, Wang D, Huang X, Li S
Received 5 May 2025
Accepted for publication 15 August 2025
Published 27 August 2025 Volume 2025:12 Pages 1943—1955
DOI https://doi.org/10.2147/JHC.S536381
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hop Tran Cao
Huixia Qin,1,* Kaiwen Jiang,2,* Chengyuan Liu,2,* Hesheng Lin,2,* Jing Xia,2,* Houxiang Ya,2 Jing Gu,2 Liya Suo,2 Bo Li,2 Xin Deng,2 Dejie Wang,3 Xiaowang Huang,3 Shuqun Li2
1Interventional Center, The First Affiliated Hospital of Guilin Medical University, Guilin, Guangxi, 450001, People’s Republic of China; 2Department of Hepatobiliary Pancreatic Surgery, The First Affiliated Hospital of Guilin Medical University, Guilin, Guangxi, 541001, People’s Republic of China; 3Department of Hepatobiliary and Pancreatic Surgery, the Affiliated Cangnan Hospital of Wenzhou Medical University, Wenzhou, Zhejiang Province, 325800, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuqun Li, Email [email protected] Xiaowang Huang, Email [email protected]
Background: Transarterial chemoembolization (TACE) remains a cornerstone for unresectable hepatocellular carcinoma (uHCC) but is limited by tumor progression. Combining TACE with systemic therapies may enhance efficacy. Notably, sintilimab combined with bevacizumab biosimilar has shown synergistic effects in tumor control and has been incorporated into the first-line treatment regimen in China. This study evaluates the therapeutic efficacy and safety of TACE combined with sintilimab and bevacizumab biosimilar in patients with uHCC.
Methods: This retrospective cohort study analyzed 76 uHCC patients who received TACE plus sintilimab-bevacizumab biosimilar at the First Affiliated Hospital of Guilin Medical University between September 2020 and March 2024, with follow-up continuing until March 31, 2025. The primary outcomes, overall survival (OS) and progression-free survival (PFS), were evaluated through Kaplan-Meier survival analysis. Independent risk factors for OS and PFS were evaluated using both univariate and multivariate analyses. Secondary outcomes comprised objective response rate (ORR), disease control rate (DCR), and treatment-related adverse events (tr-AEs).
Results: The study cohort comprised 76 patients meeting predefined eligibility criteria, achieving median OS of 23.2 months and median PFS of 14.5 months. Tumor response was assessed per mRECIST criteria, demonstrating an ORR of 59.2% and DCR of 81.6%. Multivariable analysis confirmed the modified albumin-bilirubin (mALBI) grade 3, alpha-fetoprotein (AFP) level, and macrovascular invasion as independent risk factors for OS and PFS (all P< 0.05). All tr-AEs were manageable, with no fatal events reported.
Conclusion: TACE combined with sintilimab and bevacizumab biosimilar demonstrated favorable efficacy and manageable safety in patients with uHCC.
Keywords: unresectable hepatocellular carcinoma, sintilimab, bevacizumab biosimilar, transarterial chemoembolization
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common cancer globally and continues to be the third most significant cause of cancer deaths. Among malignancies, HCC stands out as one of the few cancers with both rising incidence and increasing mortality rates globally.1–3 Unfortunately, a significant proportion of HCC cases are identified only after the disease has progressed to advanced stages, where surgical intervention is no longer deemed feasible, resulting in unresectable HCC (uHCC) and ultimately leading to unfavorable clinical outcomes.2 Given these challenges, exploring innovative and effective treatment strategies is crucial for enhancing patient outcomes and extending survival in those with uHCC.
Systemic therapy has profoundly transformed the therapeutic landscape for uHCC.4–6 In the evolution of systemic therapy, combination regimens, particularly those integrating immune checkpoint inhibitors with anti-angiogenic agents, exemplified by the atezolizumab-bevacizumab regimen and the durvalumab-tremelimumab regimen, have become established as first-line standard treatment strategies in individuals with uHCC.7 Results from the ORIENT-32 study, a multicenter clinical trial based in China, revealed that the combination of sintilimab, with a bevacizumab biosimilar significantly surpassed sorafenib alone in clinical outcomes among patients with uHCC.8 Supported by the robust findings from the ORIENT-32 trial, the combination of sintilimab with bevacizumab biosimilar has been granted regulatory approval by China’s National Medical Products Administration (NMPA) to serve as a first-line treatment option in uHCC.
Transarterial chemoembolization (TACE), which is the most frequently utilized locoregional treatment for uHCC, can be effectively combined with systemic therapy to achieve improved survival outcomes.9–11 However, the combination of TACE with sintilimab and bevacizumab biosimilar in the management of uHCC remains underexplored. This single-center, retrospective study was conducted to assess the safety profile and preliminary antitumor efficacy of the regimen comprising TACE, sintilimab, and bevacizumab biosimilar among individuals diagnosed with uHCC.
Materials and Methods
Study Population
Unresectable hepatocellular carcinoma can be categorized into two types. One type refers to surgical unresectability, which arises from factors such as poor general health, inadequate liver function, or insufficient residual liver volume, rendering patients unable to tolerate the trauma of surgery. The second type involves oncological or biological unresectability, a more controversial category, where tumors may technically be resectable, but post-surgical outcomes are unlikely to offer any better efficacy than non-surgical treatments.12 This study included patients diagnosed with uHCC and treated with TACE combined with sintilimab plus bevacizumab biosimilar at the First Affiliated Hospital of Guilin Medical University between September 2020 and March 2024, with follow-up continuing until March 31, 2025 for survival outcome assessment. This retrospective study was conducted in accordance with the ethical principles established by the Declaration of Helsinki (1975). Ethical approval for this retrospective analysis was granted by the Ethics Committee of the First Affiliated Hospital of Guilin Medical University, and written informed consent was obtained from each participant prior to inclusion.
All patients underwent baseline contrast-enhanced CT or MRI prior to treatment initiation to assess tumor characteristics, macrovascular invasion (MVI), extrahepatic metastasis, and the presence of liver cirrhosis. Imaging assessments were independently reviewed by two radiologists with over 15 years of experience. MVI was defined radiologically as the presence of intraluminal filling defects adjacent to the primary tumor within the portal vein, hepatic vein, or inferior vena cava (IVC), accompanied by arterial-phase enhancement and washout appearance in the portal or delayed phase. Extrahepatic metastasis was determined based on baseline imaging findings and referred to confirmed metastatic lesions outside the liver, including pulmonary nodules, bone lesions, or distant lymphadenopathy. Liver cirrhosis was diagnosed through a comprehensive evaluation combining clinical history, laboratory parameters, and characteristic imaging features, such as a nodular liver surface, splenomegaly, and radiological signs of portal hypertension (eg, ascites or varices). Liver biopsy was not routinely performed for confirmation.
Inclusion criteria were as follows: (1) age ≥18 years old; (2) diagnosis of HCC confirmed by histologic or cytologic analysis or clinical feature according to the American Association for the Study of Liver Diseases (AASLD) guideline;13 (3) staging as B or C based on the Barcelona Clinic Liver Cancer (BCLC) classification system; (4) unable to perform radical resection; (5) received no previous locoregional or systemic therapy; (6) at least one measurable target lesion according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST); (7) Eastern Cooperative Oncology Group Performance Status (ECOG-PS) score of 0–1; (8) Child-Pugh class A/B. Exclusion criteria included the following: (1) risk of bleeding, coagulation dysfunction, or current thrombolytic therapy; or the presence of severe esophagogastric varices detected on gastrointestinal endoscopy; (2) had central nervous system metastasis; (3) had a major surgery within 1 month; (4) combined with other malignant tumors; (5) multiple organ dysfunction syndrome; (6) incomplete medical information, and loss of follow-up.
TACE Procedures
The TACE was performed by interventional radiologists who have over 15 years of clinical experience. After the femoral artery was punctured using a modified Seldinger’s technique, a 5F catheter was inserted into the celiac trunk and superior mesenteric artery for arteriography. Then a 2.7-F microcatheter was inserted to identify tumor-feeding arteries and portal vein anatomy. Based on the angiography results, oxaliplatin (75 mg/m2) and raltitrexed (3 mg/m2) or 5-fluorouracil (750 mg/m2) were injected into tumor arteries via microcatheter. Then, the iodized oil (10–20 mL, Lipiodol Ultra-Fluid) mixed with epirubicin (30–50 mg/m2) was used to embolize tumor-feeding arteries. Ultimately, the tumor-feeding arteries were embolized using absorbable gelatin sponge particles and polyvinyl alcohol (PVA) microspheres, until complete arterial flow stasis was achieved. The number of TACE procedures was determined individually by the treating physician based on the patient’s clinical condition, tumor burden, and radiological response. In general, patients received 1 to 3 sessions of TACE during the course of treatment.
Systemic Therapy
Intravenous therapy with sintilimab (200 mg) and bevacizumab biosimilar IBI305 (15 mg/kg) commenced starting 3 days after TACE, with both agents administered on a 3-week cycle. If treatment-related adverse events (tr-AEs) necessitated the interruption or discontinuation of either sintilimab or bevacizumab biosimilar, patients were allowed to continue with the other agent as monotherapy. The decision to interrupt either sintilimab or bevacizumab biosimilar was made based on the type of the adverse event, the known safety profiles of each agent, and clinical judgment.
Follow-up
The initial follow-up was conducted 24 days after the TACE procedure, with subsequent follow-ups conducted every 3 weeks thereafter. During each follow-up, patients underwent serological testing, which included routine blood tests, liver function tests, renal function tests, coagulation function tests, alpha-fetoprotein (AFP) levels. Imaging assessments, including chest CT, abdominal contrast-enhanced CT or MRI, were scheduled every 2 months following the TACE procedure. Follow-up was maintained through March 31, 2025, in alignment with the survival data cutoff.
Efficacy and Safety Assessment
The primary outcomes were overall survival (OS) and progression-free survival (PFS): OS was defined as the time from the date of the initial TACE procedure to death from any cause or the last follow-up.14 PFS was defined as the time from the date of the initial TACE procedure to the first documented radiological progression (based on mRECIST criteria), death from any cause, or the last follow-up, whichever occurred first. A 25% increase in intrahepatic tumor size compared to the baseline, transient deterioration of liver function to Child-Pugh class C, presence of macrovascular invasion, or the occurrence of extrahepatic metastasis were considered tumor progression.9 Secondary outcomes were objective response rate (ORR), disease control rate (DCR), and tr-AEs. Complete response (CR) was defined as the disappearance of all arterial-enhancing target lesions. Partial response (PR) was defined as a reduction of more than 30% in the total diameter of the arterial-enhancing target lesions from the baseline. Disease progression (PD) was defined as an increase of more than 20% in the size of the longest diameter of the arterial-enhancing target lesions from the baseline or appearance of new lesions. Stable disease (SD) was defined as neither a decrease in lesion size by more than 30% nor an increase by more than 20% compared to baseline. The ORR was defined as the percentage of patients achieving a CR or PR. The DCR was defined as the percentage of patients with CR, PR, or SD. Tumor response was evaluated according to mRECIST criteria. Tr-AEs were evaluated based on the National Cancer Institute Common Terminology Criteria for Adverse Events ver.5.0.
Statistical Analyses
The Kaplan-Meier method was utilized to estimate PFS and OS. Univariate Cox regression analysis was performed to explore potential risk factors. Only variables with a P-value < 0.05 in the univariate analysis were included in the multivariate Cox regression model, and this selection criterion was strictly and consistently applied. For categorical variables such as modified albumin-bilirubin (mALBI) grade, comparisons in the multivariate model were made using grade 1 as the reference group. p<0.05 was considered statistically significant. All statistical analyses were performed using R version 4.4.3.
Results
Baseline Characteristics
In total, 104 patients with uHCC who received a combination of sintilimab, bevacizumab biosimilar, and TACE were enrolled between September 2020 and March 2024. Following the application of predefined exclusion criteria, 28 individuals were excluded from the study cohort, and the final analysis involved 76 participants. Of the 76 included patients, there were 67 males (88.2%) and 9 females (11.8%), and most patients were <65 years old. 57 patients (75.0%) had an ECOG-PS score of 0. Child-Pugh class A was identified in 64 patients (84.2%). In addition, the BCLC stages B and C accounted for 21.1% and 78.9%, respectively. The mALBI grade 1, 2, and 3 accounted for 31.6%, 46.0%, and 22.4%, respectively. 40 patients (52.6%) had an AFP level of <400 ng/mL. 64 patients (84.2%) had a DCP level of <400 mAU/mL. 41 patients (53.9%) had macrovascular invasion, while 35 patients (46.1%) did not. Table 1 presents the clinical baseline characteristics of the included patients, while Figure 1 illustrates the detailed patient enrollment process.
 |
Table 1 Baseline Characteristics of the Patients |
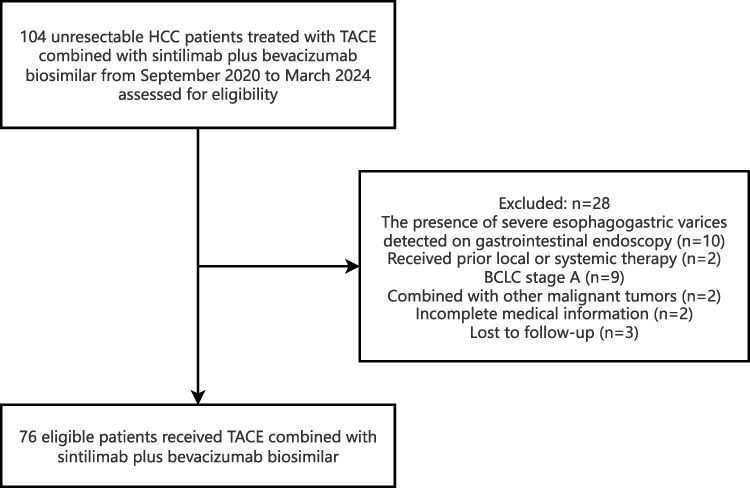 |
Figure 1 Flow diagram of study population enrolled in this study. |
Efficacy Outcomes
As of the data cutoff on March 31, 2025, the median OS (mOS) was 23.2 months (95% CI 14.7-not reached) (Figure 2A), with a median PFS (mPFS) of 14.5 months (95% CI 11.6–23.9) (Figure 2B). Based on mRECIST, the treatment responses were categorized as follows: CR in 6 patients (7.9%), PR in 39 patients (51.3%), SD in 17 patients (22.4%), and PD in 14 patients (18.4%). The ORR was calculated as 59.2%, and the DCR reached 81.6%. Comprehensive details of these outcomes are presented in Table 2. The change in tumor size was illustrated in Figure 3.
 |
Table 2 Tumor Response According to mRECIST Criteria |
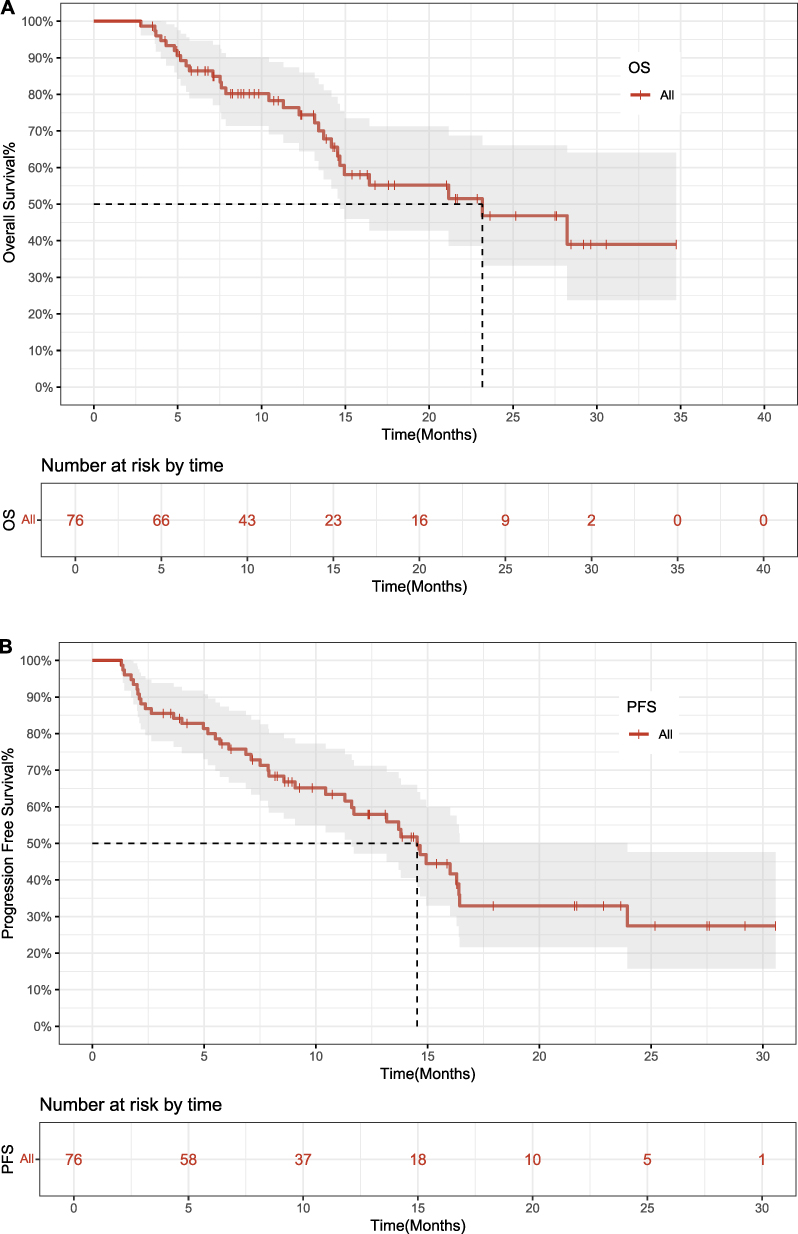 |
Figure 2 (A) Kaplan-Meier survival curves of overall survival. (B) Kaplan-Meier survival curves of progression-free survival. |
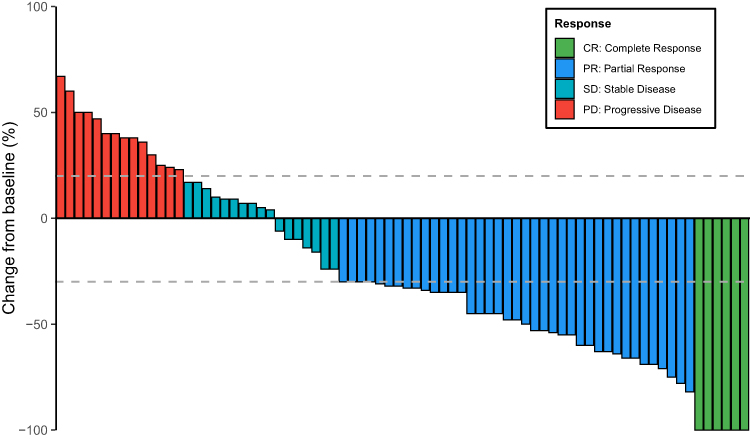 |
Figure 3 Waterfall plot for changes in size of target lesions. |
Cox Regression Analysis
Table 3 presents the independent risk factors related to OS. In the univariate analysis, the mALBI grade, AFP level, tumor size, macrovascular invasion, and extrahepatic metastasis emerged as significant risk factors of OS. Further multivariate analysis identified the mALBI grade 3 [hazard ratio (HR) = 8.31; 95% CI, 2.00–34.54; P = 0.004], AFP level (HR = 3.95; 95% CI, 1.20–13.02; P = 0.024), and macrovascular invasion (HR = 3.13; 95% CI, 1.02–9.67; P = 0.047) as independent risk factors for OS.
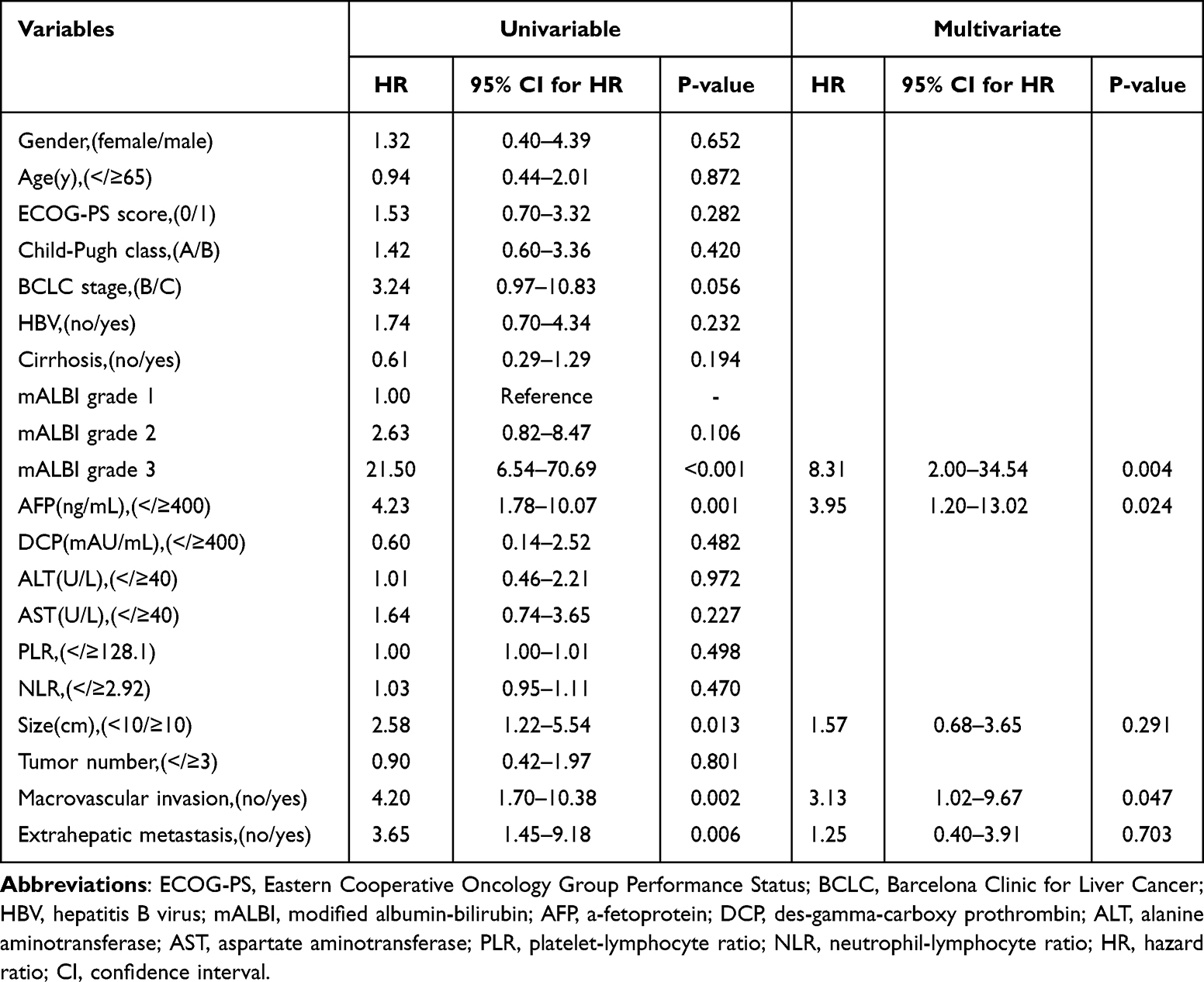 |
Table 3 Results of the Univariable and Multivariate Analysis of OS |
Table 4 presents the independent risk factors related to PFS. In the univariate analysis, HBV, the mALBI grade, AFP level, macrovascular invasion, and extrahepatic metastasis emerged as significant risk factors of PFS. Further multivariate analysis identified the mALBI grade 3 (HR = 4.64; 95% CI, 1.51–14.26; P = 0.007), AFP level (HR = 3.39; 95% CI, 1.38–8.31; P = 0.008), and macrovascular invasion (HR = 2.55; 95% CI, 1.12–5.80; P = 0.026) as independent risk factors for PFS.
 |
Table 4 Results of the Univariable and Multivariate Analysis of PFS |
Safety Outcomes
A total of 71 patients (93.42%) experienced tr-AEs of any grade. Among the tr-AEs, the most frequently observed were hypertension (35.53%), decreased appetite (28.95%), fatigue (26.32%), abdominal pain (25.00%), nausea (23.68%), diarrhea (22.37%), elevated ALT/AST (22.37%), and proteinuria (21.05%). 17 patients (22.37%) encountered grade ≥3 tr-AEs, with hypertension as the most common. Among the 76 patients, 3 patients (3.95%) experienced grade ≥3 tr-AEs that led to temporary discontinuation of sintilimab, while bevacizumab biosimilar was continued as monotherapy. These events included elevated total bilirubin (n = 1), diarrhea (n = 1), and decreased platelet count (n = 1). In contrast, 4 patients (5.26%) required temporary discontinuation of bevacizumab biosimilar due to grade ≥3 tr-AEs—specifically hypertension (n = 2) and proteinuria (n = 2)—while continuing treatment with sintilimab alone. All tr-AEs were successfully managed, with no fatalities attributed to the treatment. Table 5 provides a detailed listing of adverse events, irrespective of their causality.
 |
Table 5 Treated Related Adverse Events Observed in Enrolled Patients |
Discussion
This study evaluated the antitumor efficacy and safety profile of TACE, sintilimab, and bevacizumab biosimilar for individuals with uHCC. In our previous publication, we demonstrated that the combination of TACE with lenvatinib and a PD-1 inhibitor yielded promising therapeutic outcomes.15 However, it is important to note that the regimen of lenvatinib plus PD-1 inhibitor is not currently considered a first-line treatment option. In contrast, the combination of sintilimab and a bevacizumab biosimilar has been recommended as a first-line therapy in the Chinese clinical guidelines. Based on this, we aimed to further explore the efficacy and safety of integrating TACE with this guideline-endorsed systemic regimen, in an effort to offer novel practical insights for current clinical management.
Our results showed that patients with uHCC had an ORR of 59.2% and a DCR of 81.6% by the mRECIST. The mOS was 23.2 months (95%Cl 14.7-not reached), and the mPFS was 14.5 months (95%Cl 11.6–23.9). Among the patients, 6 (7.9%) achieved a CR, while 39 (51.3%) demonstrated a PR. Additionally, 17 cases (22.4%) exhibited SD, and 14 patients (18.4%) experienced PD. The incidence rate of tr-AEs was 93.42%, with a 22.37% incidence rate of tr-AEs graded as 3 or higher. Temporary discontinuation of either agent due to grade ≥3 tr-AEs occurred in 7 patients (9.21%). Among them, 3 patients paused sintilimab while continuing bevacizumab biosimilar, and 4 patients paused bevacizumab biosimilar while maintaining sintilimab therapy. All tr-AEs were manageable through temporary discontinuation of the suspected agent, continuation of monotherapy, and symptomatic treatment. No treatment-related deaths have occurred. Consequently, these results suggest that TACE combined with sintilimab plus bevacizumab biosimilar may provide satisfactory efficacy and survival benefits for uHCC patients.
Conventional TACE monotherapy for uHCC typically yields ORR of 25–30%, with mPFS of 3–7 months and mOS spanning 10–16 months.16–18 In contrast, combination therapies demonstrate significantly superior efficacy. Many previous studies have demonstrated that the combination of ICIs with targeted therapies is markedly effective. Updated findings from the IMbrave150 trial revealed a 5.8-month prolongation in mOS with atezolizumab-bevacizumab combination versus sorafenib monotherapy, while tr-AEs maintained comparable severity gradients to established safety benchmarks.19 The ORIENT-32 trial aimed to determine the therapeutic outcomes of sintilimab and a bevacizumab biosimilar combination in individuals with uHCC. The study documented a mPFS of 4.6 months, although the mOS remained undetermined. According to the mRECIST, the ORR was 25%, while the DCR reached 74%.8 In addition, increasing evidence suggests that the combination of TACE with systemic therapy can significantly enhance therapeutic efficacy. In the Phase 3 LEAP-012 trial evaluating TACE combined with lenvatinib plus pembrolizumab versus dual placebo in unresectable non-metastatic HCC, the combination significantly prolonged mPFS versus dual placebo to 14.6 months (95% CI 12.6–16.7) per RECIST v1.1 (HR 0.66, 95% CI 0.51–0.84; p=0.0002) and 14.5 months (95% CI 12.2–16.8) by mRECIST (HR 0.64, 95% CI 0.50–0.83). The ORR reached 47% (95% CI 40–53) per RECIST v1.1 and 71% (95% CI 65–77) by mRECIST, while OS data remained immature with favorable 24-month rates (75% vs 69%; HR 0.80, 95% CI 0.57–1.11).20 In a retrospective cohort study by Wang, Zhao et al, the combination of TACE, PD-1 inhibitors, and lenvatinib achieved a mOS of 20.5 months and a mPFS of 12.1 months following propensity score matching. These outcomes were significantly superior to those observed in the group receiving PD-1 inhibitors combined with lenvatinib alone.21 The multicenter observational investigation by Shen et al demonstrated compelling clinical outcomes in advanced HCC management, revealing an ORR of 54.3% (95% CI 51.2–57.4) per mRECIST criteria following combination therapy with atezolizumab-bevacizumab and TACE. With a median follow-up duration of 18.7 months (IQR 15.3–22.1), the therapeutic regimen achieved mOS of 15.9 months (95% CI 14.5–17.2) and mPFS of 9.1 months (95% CI 7.4–10.8).22 Collectively, triple-modality regimens exhibit statistically significant superiority in therapeutic outcomes relative to dual-agent or monotherapeutic approaches.
Besides, our results have demonstrated favorable mPFS and mOS for patients treated with TACE combined with sintilimab plus bevacizumab biosimilar. Similar therapeutic patterns have been consistently observed in other trials investigating combined immune checkpoint inhibitors, anti-angiogenic agents, and locoregional therapies for uHCC.23–25 The combination therapy of TACE, PD-1 inhibitors, and vascular endothelial growth factor (VEGF) inhibitor carries inherent bleeding risks. Consequently, patients with endoscopically confirmed severe esophagogastric varices were excluded from the cohort. No treatment-emergent gastrointestinal hemorrhagic events or grade ≥3 tr-AEs were observed during follow-up, suggesting that this stringent exclusion criterion may underlie the manageable safety profile of the triple-modality regimen. We believe that the high effectiveness and improved survival in this study may be caused by the synergistic effect of TACE and sintilimab, bevacizumab biosimilar. TACE is an effective local therapeutic regimen that leads to extensive local necrosis of the tumor, which may subsequently trigger an anti-cancer immune response that may be further enhanced by PD-1 inhibitors.26,27 However, TACE causes tissue hypoxia leading to elevated VEGF, which may induce intra-tumor angiogenesis.26 In contrast, PD-1 inhibitors plus anti-VEGF can counteract hypoxia-induced angiogenesis after TACE, normalize tumor vascularization, and modulate the tumor immune microenvironment to enhance the therapeutic effect of TACE in HCC.28,29 Therefore, the use of TACE and sintilimab in combination with bevacizumab biosimilar may produce synergistic antitumor activity, reduce tumor burden, and contribute to the improvement of clinical prognosis in patients with uHCC.
Additionally, our univariate and multivariate analysis results indicate that the mALBI grade 3, the AFP level, and the presence of macrovascular invasion are independent risk factors influencing OS and PFS. Although age and gender are generally considered important independent prognostic factors in uHCC, their inclusion in the multivariate Cox regression analysis yielded P-values greater than 0.05, suggesting no statistically significant association in our cohort. These findings suggest that improving liver function reserve (as reflected by the mALBI grade), reducing AFP levels, and preventing macrovascular invasion may contribute to better patient prognosis.
Despite its contributions, this research has certain limitations. A primary limitation is its retrospective design, which was confined to a single center and may introduce inherent biases. Secondly, the population included in our study consisted exclusively of Chinese patients with liver cancer, predominantly those with hepatitis B-induced liver cancer. These findings may not be fully applicable to liver cancer patients with alcoholic hepatitis from other countries, suggesting the need to conduct similar research involving more varied populations across different geographic regions. Moreover, due to the lack of a control group, the assessment of the regimen’s relative efficacy relies on indirect comparisons with outcomes reported for other combination strategies. Prospective investigations incorporating randomized or matched controlled designs will be essential to confirm these findings. Lastly, the sample size of our study is limited. Consequently, to derive more generalizable results, a multicenter randomized clinical trial is required to validate our findings.
Conclusion
In conclusion, our findings suggest that, after excluding cases with severe esophagogastric varices, the combination therapy involving TACE, sintilimab, and bevacizumab biosimilar demonstrates favorable efficacy and a well-controlled safety profile in patients with uHCC. Therefore, the TACE combined with sintilimab plus bevacizumab biosimilar regimen has the potential to introduce an innovative treatment strategy for the patients with uHCC.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
Ethical approval for this observational study was obtained from the Ethics Committee of the First Affiliated Hospital of Guilin Medical University. The study was conducted in accordance with the Declaration of Helsinki (1975). All participants provided written informed consent before enrollment.
Consent to Participate
Written informed consent was obtained from all participants prior to treatment, following a thorough explanation of the study objectives, potential risks, and benefits. The consent process included specific authorization for access to medical records and the collection and analysis of clinical data. Particular attention was paid to maintaining patient confidentiality and data security throughout the study.
Acknowledgments
We extend our sincere gratitude to all participants and researchers whose invaluable contributions were instrumental in the successful completion of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Guangxi Medical and Health Key discipline construction project, Guangxi medical and healthcare appropriate technology development and promotion and application projects (grant number: S2022132), Guangxi Natural Science Foundation (grant number: 2022JJA140009, 2025GXNSFHA069049), Self-financed scientific research projects of Guangxi Autonomous Region Health and Wellness Commission (Z-C20230840).
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA a Cancer J Clinicians. 2024;74:229–263. doi:10.3322/caac.21834
2. Singal AG, Kanwal F, Llovet JM. Global trends in hepatocellular carcinoma epidemiology: implications for screening, prevention and therapy. Nat Rev Clin Oncol. 2023;20(12):864–884. doi:10.1038/s41571-023-00825-3
3. Rumgay H, Ferlay J, De Martel C, et al. Global, regional and national burden of primary liver cancer by subtype. Eur J Cancer. 2022;161:108–118. doi:10.1016/j.ejca.2021.11.023
4. Llovet JM, Montal R, Sia D, Finn RS. Molecular therapies and precision medicine for hepatocellular carcinoma. Nat Rev Clin Oncol. 2018;15(10):599–616. doi:10.1038/s41571-018-0073-4
5. Llovet JM, Castet F, Heikenwalder M, et al. Immunotherapies for hepatocellular carcinoma. Nat Rev Clin Oncol. 2022;19(3):151–172. doi:10.1038/s41571-021-00573-2
6. Rizzo A, Ricci AD. PD-L1, TMB, and other potential predictors of response to immunotherapy for hepatocellular carcinoma: how can they assist drug clinical trials? Expert Opin Invest Drugs. 2022;31(4):415–423. doi:10.1080/13543784.2021.1972969
7. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
8. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, Phase 2–3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
9. Kudo M, Ueshima K, Ikeda M, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut. 2020;69(8):1492–1501. doi:10.1136/gutjnl-2019-318934
10. Cao F, Yang Y, Si T, et al. The efficacy of TACE combined with lenvatinib plus sintilimab in unresectable hepatocellular carcinoma: a multicenter retrospective study. Front Oncol. 2021;11:783480. doi:10.3389/fonc.2021.783480
11. Peng Z, Fan W, Zhu B, et al. Lenvatinib combined with transarterial chemoembolization as first-line treatment for advanced hepatocellular carcinoma: a phase III, randomized clinical trial (LAUNCH). JCO. 2023;41(1):117–127. doi:10.1200/JCO.22.00392
12. Sun H-C, Zhou J, Wang Z, et al. Alliance of Liver Cancer Conversion Therapy, Committee of Liver Cancer of the Chinese Anti-Cancer Association. Chinese expert consensus on conversion therapy for hepatocellular carcinoma (2021 edition). Hepatobiliary Surg Nutr. 2022;11(2):227–252. doi:10.21037/hbsn-21-328
13. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
14. Yang Y, Chen Y, Ye F, et al. Late recurrence of hepatocellular carcinoma after radiofrequency ablation: a multicenter study of risk factors, patterns, and survival. Eur Radiol. 2021;31(5):3053–3064. doi:10.1007/s00330-020-07460-x
15. Jin M, Jiang ZQ, Qin JH, et al. Efficacy and safety of lenvatinib plus programmed death-1 inhibitors with or without transarterial chemoembolization in the treatment of unresectable hepatocellular carcinoma. J Hepatocell Carcinoma. 2024;11:2309–2320. doi:10.2147/JHC.S485047
16. Qu S, Zhang X, Wu Y, et al. Efficacy and safety of TACE combined with lenvatinib plus PD-1 inhibitors compared with TACE alone for unresectable hepatocellular carcinoma patients: a prospective cohort study. Front Oncol. 2022;12:874473. doi:10.3389/fonc.2022.874473
17. Tang Z, Bai T, Wei T, et al. TACE combined lenvatinib plus camrelizumab versus TACE alone in efficacy and safety for unresectable hepatocellular carcinoma: a propensity score-matching study. BMC Cancer. 2024;24(1):717. doi:10.1186/s12885-024-12484-3
18. Zong Z, Tang R, Li M, et al. Department of Infectious and Liver Disease, The Second Hospital of Nanjing, Affiliated to Nanjing University of Chinese Medicine, Nanjing, China. Efficiency and stability of transarterial chemoembolization combined with or without lenvatinib for unresectable hepatocellular carcinoma. Turk J Gastroenterol. 2024;35(3):212–222. doi:10.5152/tjg.2024.23071
19. Cheng A-L, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76(4):862–873. doi:10.1016/j.jhep.2021.11.030
20. Kudo M, Ren Z, Guo Y, et al. Transarterial chemoembolisation combined with lenvatinib plus pembrolizumab versus dual placebo for unresectable, non-metastatic hepatocellular carcinoma (LEAP-012): a multicentre, randomised, double-blind, phase 3 study. Lancet. 2025;405(10474):203–215. doi:10.1016/S0140-6736(24)02575-3
21. Wang J, Zhao M, Han G, et al. Transarterial chemoembolization combined with PD-1 inhibitors plus lenvatinib showed improved efficacy for treatment of unresectable hepatocellular carcinoma compared with PD-1 inhibitors plus lenvatinib. Technol Cancer Res Treat. 2023;22:15330338231166765. doi:10.1177/15330338231166765
22. Shen X, Zhang J-X, Liu J, et al. Efficacy of atezolizumab plus bevacizumab combined with transarterial chemoembolization for unresectable hepatocellular carcinoma: a real-world study. J Hepatocellular Carcinoma. 2024;11:1993–2003. doi:10.2147/JHC.S478604
23. Mei J, Tang Y-H, Wei W, et al. Hepatic arterial infusion chemotherapy combined with PD-1 inhibitors plus lenvatinib versus PD-1 inhibitors plus lenvatinib for advanced hepatocellular carcinoma. Front Oncol. 2021;11:618206. doi:10.3389/fonc.2021.618206
24. Xuexian Z, Ruidong W, Yuhan D, et al. Safety and efficacy of DEB-TACE in combination with lenvatinib and camrelizumab for the treatment of unresectable hepatocellular carcinoma (uHCC): a two-centre retrospective study. Front Immunol. 2024;15:1422784. doi:10.3389/fimmu.2024.1422784
25. Zhao Y, Wen S, Xue Y, et al. Transarterial chemoembolization combined with lenvatinib plus tislelizumab for unresectable hepatocellular carcinoma: a multicenter cohort study. Front Immunol. 2024;15:1449663. doi:10.3389/fimmu.2024.1449663
26. Chang Y, Jeong SW, Young Jang J, Jae Kim Y. Recent updates of transarterial chemoembolilzation in hepatocellular carcinoma. IJMS. 2020;21(21):8165. doi:10.3390/ijms21218165
27. Cheu JW, Wong CC. Mechanistic rationales guiding combination hepatocellular carcinoma therapies involving immune checkpoint inhibitors. Hepatology. 2021;74(4):2264–2276. doi:10.1002/hep.31840
28. Kudo M. A new era in systemic therapy for hepatocellular carcinoma: atezolizumab plus bevacizumab combination therapy. Liver Cancer. 2020;9(2):119–137. doi:10.1159/000505189
29. LAPEYRE-PROST A, TERME M, PERNOT S, et al. Immunomodulatory activity of VEGF in cancer. Int Rev Cell Mol Biol. 2017;330:295–342. doi:10.1016/bs.ircmb.2016.09.007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Retrospective Analysis of Conversion Therapy with Lenvatinib, Sintilimab, and Arterially-Directed Therapy in Patients with Initially Unresectable Hepatocellular Carcinoma
Gan L, Lang M, Tian X, Ren S, Li G, Liu Y, Han R, Zhu K, Li H, Wu Q, Cui Y, Zhang W, Fang F, Li Q, Song T
Journal of Hepatocellular Carcinoma 2023, 10:673-686
Published Date: 22 April 2023