Back to Journals » Drug Design, Development and Therapy » Volume 19
Efficacy and Long-Term Outcomes of Tacrolimus versus Cyclophosphamide and Mycophenolate Mofetil in the Management of Pediatric IgA Vasculitis Nephritis: A Cohort Study in Single-Center
Authors Han Y, Yang F, Zhou L, Yang J, Yang Y, Wang Y, Qiu L, Zhang Y, Zhou J
Received 24 March 2025
Accepted for publication 17 July 2025
Published 29 July 2025 Volume 2025:19 Pages 6413—6422
DOI https://doi.org/10.2147/DDDT.S528565
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Yanxinli Han,* Fengjie Yang,* Lanqi Zhou, Jing Yang, Yuan Yang, Yi Wang, Liru Qiu, Yu Zhang, Jianhua Zhou
Department of Pediatrics, Tongji Hospital, Tongji Medical College, Huazhong University of Science & Technology, Wuhan, Hubei Province, 430030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianhua Zhou, Department of Pediatrics, Tongji Hospital, Tongji Medical College, Huazhong University of Science & Technology, Wuhan, Hubei Province, 430030, People’s Republic of China, Tel +86 027 83662684, Email [email protected]
Purpose: IgA vasculitis nephritis (IgAVN) is one of the most common secondary glomerulonephritis in children. Although guidelines have reached a consensus about the effectiveness of cyclophosphamide (CYC) in IgAVN, the recommendations regarding the use of tacrolimus (TAC) and mycophenolate mofetil (MMF) are still inconsistent. Studies have demonstrated that TAC is safe and effective in IgAVN. However, the impact of immunosuppressive agents on the long-term outcome remains ambiguous. Therefore, the objective of this study is to compare the effectiveness and long-term outcome of TAC, CYC, and MMF in combination with glucocorticoid in pediatric IgAVN.
Patients and Methods: A retrospective analysis was conducted on children with grade II–V IgAVN by renal biopsy at Tongji Hospital from November 2011 to October 2021. The collected clinical, pathological, treatment and follow-up data were analyzed.
Results: A total of 422 patients were eligible. Among them, 108 patients received glucocorticoid in combination with oral TAC, 143 with intravenous CYC, and 171 with oral MMF. The complete remission rate (CR) of TAC (25.9%/44.3%) was significantly higher than that of CYC (16.1%/36.4%) at 3 and 6 months. Additionally, mean absolute decrease in urine protein at 1, 3, and 6 months were significantly higher in TAC than that in CYC and MMF groups. Compared to CYC, TAC and MMF groups had significantly lower overall incidence of adverse events (60.2%, 65.7% vs 84.4%). Moreover, TAC and MMF group had a more favorable renal prognosis (grade A and B) and a significantly lower recurrence rate (17.9%, 23.9% vs 41.8%) than CYC.
Conclusion: This study reveals that TAC can rapidly and effectively reduce proteinuria and achieve renal complete remission with fewer adverse effects. Moreover, TAC and MMF are more favourable for renal prognosis.
Keywords: IgAVN, immunosuppressive agents, renal remission, tacrolimus, cyclophosphamide, mycophenolate mofetil, long-term outcome
Introduction
IgA vasculitis nephritis (IgAVN) is caused by allergic purpura (HSP) representing a form of kidney glomerulus injury that is triggered by immune dysregulation. It has been documented that renal involvement occurs in a significant proportion of individuals with HSP, ranging from 30% to 80%.1 Notably, among those with IgAVN, approximately 20% develop nephritis or nephrotic syndrome, which corresponds to roughly 7% of the entire HSP patient population.2 The involvement of the kidney and the degree of severity play a crucial role in predicting the long-term prognosis of IgAVN.3 In recent years, long-term follow-up cohorts have revealed that 10%~20% of children with moderate to severe proteinuria may eventually progress to end-stage renal disease (ESKD).4,5 Therefore, effective treatment for children with severe renal involvement can improve the prognosis.
The guidelines recommend the routine use of glucocorticoids for IgAVN patients with severe clinical symptoms and pathological damage. However, the domestic and international treatment guidelines for IgAVN are still debatable. The 2021 KDIGO guideline suggests the application of glucocorticoid in children with mild or moderate IgAVN. Cyclophosphamide (CYC) is merely recommended for children presenting with nephrotic syndrome and/or rapidly deteriorating renal function.6 The 2016 Chinese evidence-based guideline for IgAVN provides detailed guidance according to clinical and pathological grading. For children presenting with non-nephrotic proteinuria or pathological grade IIb or IIIa, it is advisable to contemplate the active utilization of immunosuppressive agents. For children with nephrotic-level proteinuria, nephrotic syndrome, acute nephritis syndrome, or pathological grade IIIb, IV, in addition to glucocorticoid combined with CYC treatment, other immunosuppressive treatment options, including cyclosporine A and mycophenolate mofetil (MMF), are also recommended.7 There is currently no standardized specific treatment regimen. Therefore, this study retrospectively compared the efficacy and safety of tacrolimus (TAC), CYC or MMF combined with glucocorticoids therapy in children with IgAVN in our department, so as to provide a more optimal choice for the treatment of IgAVN.
Materials and Methods
Patients
This single-center retrospective study included 422 pediatric patients with grade II, III, IV, and V who were treated with glucocorticoids and combined with either CYC, MMF or TAC from November 2011 to October 2021. All patients were under 18 years old and were hospitalized at the Pediatric Department of Tongji Hospital. In particular, they were composed of 13 cases of grade II, 315 cases of grade III, 77 cases of grade IV and 17 cases of grade V according to the International Study of Kidney Disease in Children (ISKDC) classification. The diagnosis was determined according to the evidence-based guidelines for diagnosis and treatment of IgAVN formulated by the Subspecialty Group of Nephrology, Society of Pediatrics, Chinese Medical Association in 2016.7 Patients were excluded if they had not undergone renal biopsy, had incomplete clinical data, had other immune diseases, or were allergic to immunosuppressive agents.
The study was approved by the Ethics Committee of Tongji Hospital and was conducted in accordance with the tenets of the Declaration of Helsinki.
Data Collection, Treatment, and Definition in Evaluation and Follow Up
All patients were regularly evaluated during treatment. Responses were assessed at 1, 3, 6 and 12 months of induction treatment. The demographic, clinical, pathological and followed-up data were collected and analyzed at the time of diagnosis, at the end of 1-month, 3-month 6-month and 12-month treatment.
Patients were subsequently monitored during their final clinic visit, with follow-up assessments encompassing urine routine, renal function, and 24-hour urinary protein. Prognosis was determined in accordance with Counahan’s grading criteria.8 The prognosis was categorized into 4 grades: grade A (complete remission) with no hematuria, proteinuria, and normal renal function; Grade B (mild abnormal urine) with only microscopic hematuria and/or mild proteinuria (<1 g/24 h), and normal renal function; Grade C (active kidney disease) with proteinuria ≥ 1 g/24 h and eGFR ≥ 60 mL/(min·1.73 m2); Grade D (renal insufficiency) with eGFR < 60 mL/(min·1.73 m2) or death. It is considered that the prognosis of grade A and B is favorable, while that of grade C and D is unfavorable.
Renal parameters were defined as followed: eGFR was calculated by using the modified Schwartz formula.9 Renal pathology was classified according to the criteria of the International Study of Kidney Disease in Children (ISKDC) classification.8 The complete remission (CR) was defined as proteinuria amount < 0.15g/24h, normalization of urinary red blood cell count and normal eGFR. Partial remission (PR) was defined as a 50% reduction or more in proteinuria and normal or stable eGFR.10 And the total remission (TR) was the sum of CR and PR.
Statistical Analyses
Normality tests such as Shapiro–Wilk test and Q-Q plot were combined to determine whether continuous variables were normally distributed. Continuous variables of non-normal distribution were expressed as median (interquartile range), and continuous variables of normal distribution were expressed as mean ± standard deviation (SD). Mann–Whitney U-test or Kruskal–Wallis test was used to compare differences in medians, and Dunn’s test with Bonferroni correction was used as a post hoc test for multiple comparisons when Kruskal–Wallis test showed significant difference. t-test or analysis of variance (ANOVA) were applied to evaluate the difference of means, and Tukey’s test was used for pairwise comparisons as a post hoc test when ANOVA analysis indicated overall differences. Categorical variables were presented as numbers and percentages and were compared by Pearson’s chi-squared tests or Fisher’s exact tests. Logistic regression analysis was used to adjust for confounding factors on renal remission. Kaplan–Meier survival curves and the Log rank test were applied to compare recurrence-free probability among three induction treatments. Statistical significance was assumed for p < 0.05.
Results
Clinical Features at Biopsy of Patients with Different Histopathological Grades
A total of 422 eligible patients with IgAVN were included in this study, comprising 13 cases of grade II, 315 cases of grade III, 77 cases of grade IV, and 17 cases of grade V. Among these, grade III was the most prevalent, accounting for 74.6% of the total cases, while grade II, grade IV, and grade V constituted 3%, 18.2%, and 4.0%, respectively. As illustrated in Table 1, the baseline levels of hematuria, 24-hour urine protein (24hUP), and urinary albumin-to-creatinine ratio (UACR) were significantly higher in patients with grade IV and grade V compared to those with grade II and grade III. Conversely, the levels of serum albumin (ALB), estimated glomerular filtration rate (eGFR), serum creatinine (Scr), and 25-Hydroxyvitamin D were significantly lower in grade IV and grade V patients than in grade II and grade III patients. Despite these biochemical differences, there were no significant differences in clinical presentations among different histopathological grades.
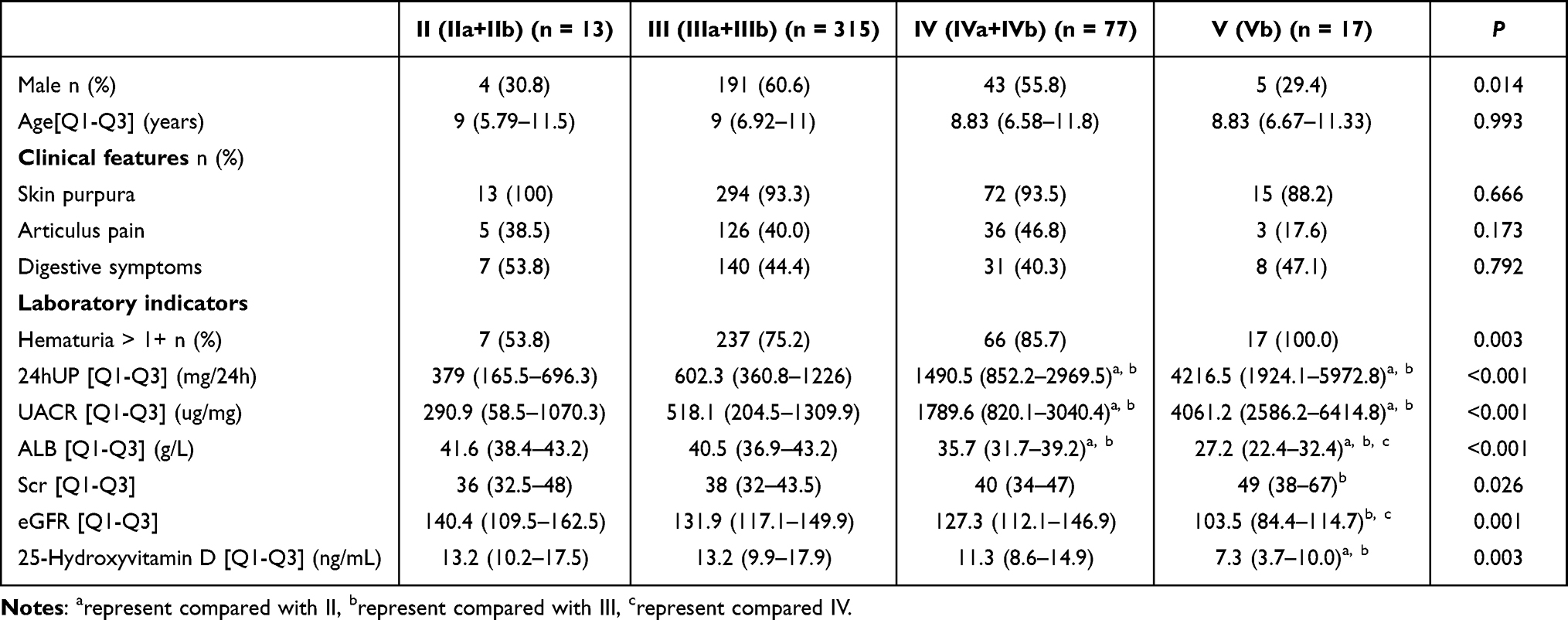 |
Table 1 Clinical Features of Patients at Biopsy with Different Histopathological Subtypes |
Clinical Features at Baseline in CYC, MMF and TAC Groups
The baseline clinical data of IgAVN patients were compared among CYC, TAC and MMF groups (Table 2). The baseline levels of 24hUP and UACR were significantly higher in TAC group than those in the CYC and MMF groups. However, the levels of ALB were significantly lower in TAC and CYC groups than in MMF group. CYC and MMF were more frequently used for patients with grade III compared to TAC, while TAC was more commonly used for patients with grade IV and grade V compared to MMF (p < 0.001).
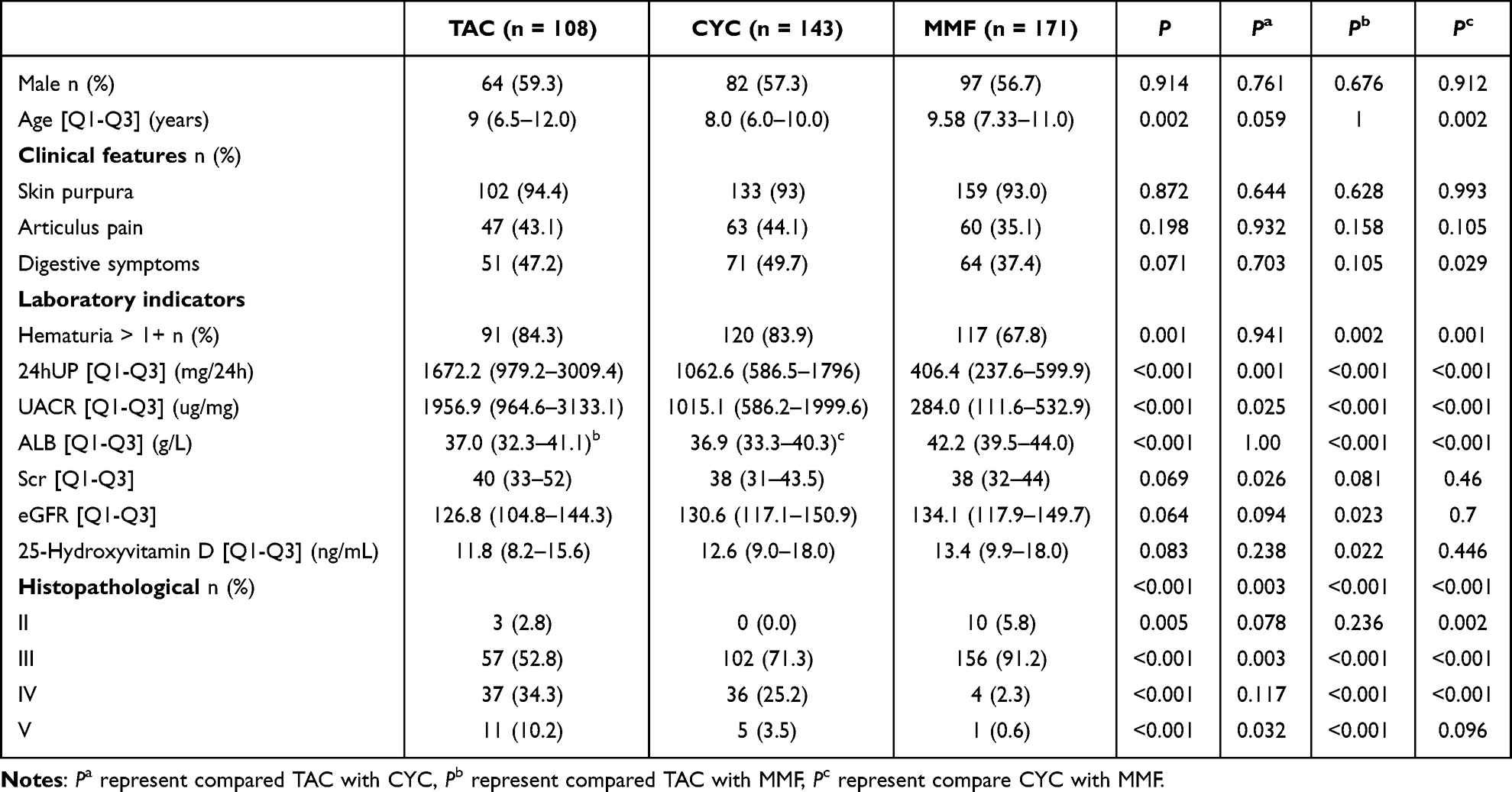 |
Table 2 Clinical Features of HSPN Patients at Baseline with Treatment of CYC, MMF and TAC |
The Renal Responses to TAC, CYC and MMF Treatment at the End of 1, 3, 6 and 12 Months
At the end of 1, 3, 6 and 12-month treatment, complete remission (CR) rate of TAC was higher than CYC (3.7% vs 2.8%, 25.9% vs 16.1%, 44.4% vs 36.4%, 63% vs 61.5%). After adjusting for confounding factors proteinuria, hematuria, and pathological grade, TAC was 1.73 times (95% CI: 1.19–2.53) more likely to improve remission than CYC at 3 months (p = 0.004). Moreover, TAC was 1.46 times than CYC at 6 months (95% CI: 1.02–2.09) (p = 0.037) (Table 3). Although there was a trend towards higher CR in MMF group compared to CYC at 1,3, 6 and 12 months (16.4% vs 2.8%, 35.7% vs 16.1%, 56.7% vs 36.4%, 73.7% vs 61.5%), MMF did not show obvious advantage on remission than CYC after adjusting for confounding factors (Table 3) (Figure 1).
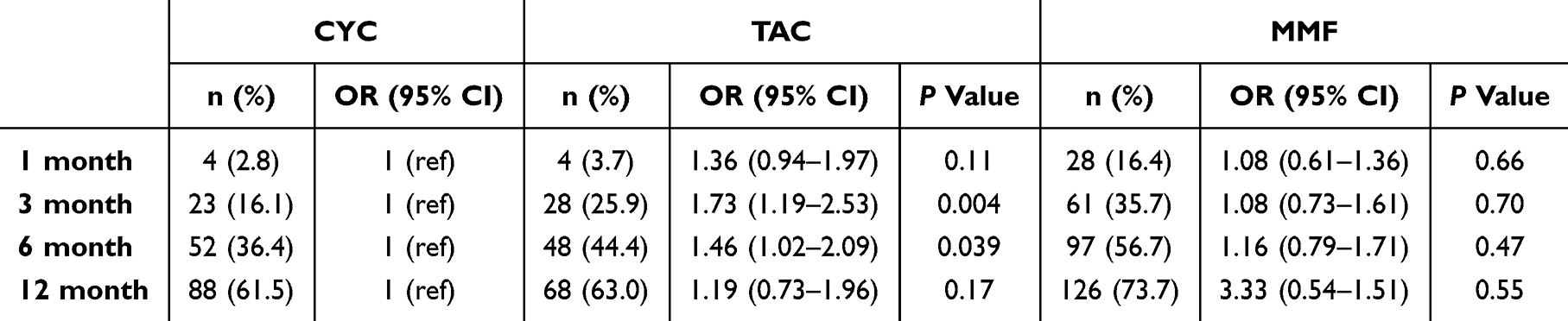 |
Table 3 Complete Remission After 1, 3, 6 and 12 Month of Induction Therapy |
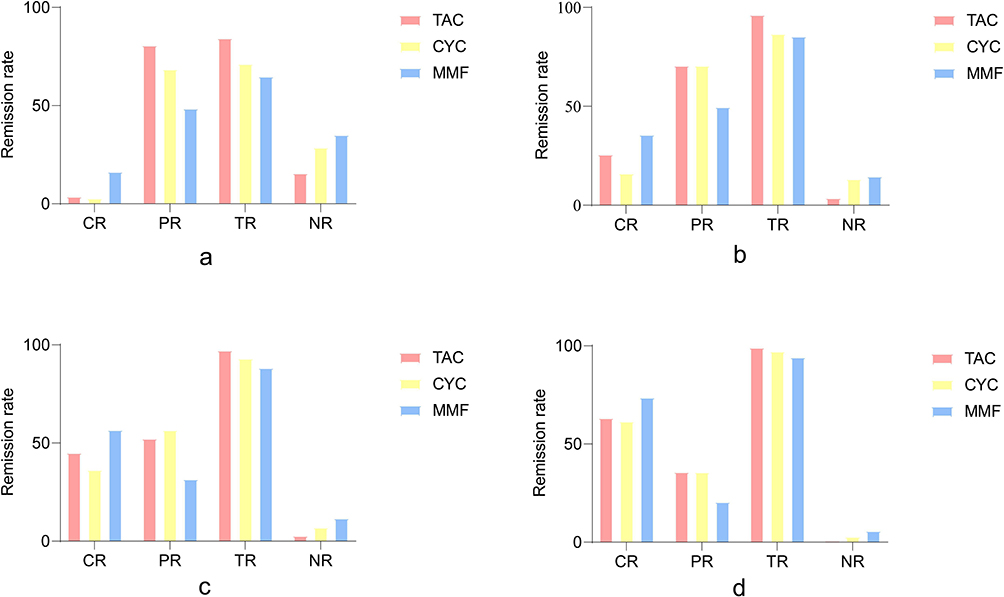 |
Figure 1 Renal remission at 1 month (a), 3 month (b), 6 month (c) and 12 month (d). Abbreviations: CR, complete remission; PR, partial remission; TR, total remission; NR, non remission. |
In addition, the mean absolute change of UACR from baseline in TAC group was significantly higher than that in CYC and MMF groups (p < 0.001). Moreover, the mean percentage change of UACR from baseline was also higher in TAC group than that in MMF group with significant difference (Figure 2).
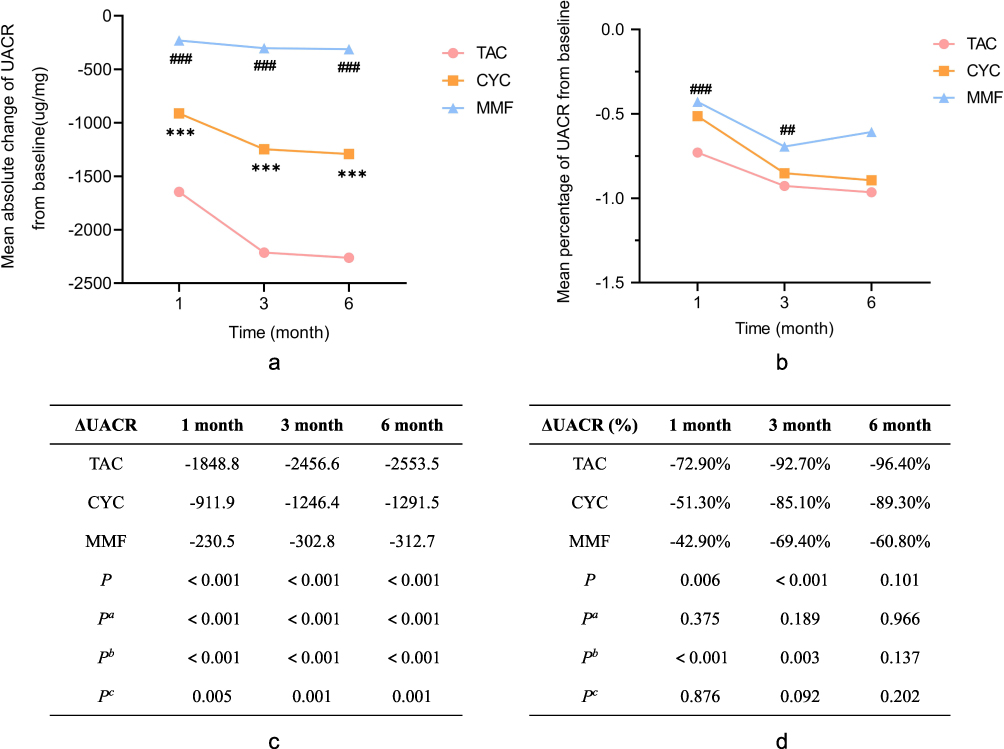 |
Figure 2 Mean absolute change (a, c) and mean percentage change (b, d) in UACR from baseline after treatment of CYC, MMF and TAC. * represent compared TAC with CYC, # represent compared TAC with MMF. *** and ### represent P < 0.001; ## represent P < 0.01. Pa represent compared TAC with CYC, Pb represent compared TAC with MMF, Pc represent compare CYC with MMF. |
The Side Effects of CYC, TAC and MMF on Treated IgAVN Patients
The overall incidence of adverse effects was both significantly lower in TAC group and MMF group compared to CYC group (60.2%, 65.7% vs 84.4%, p < 0.001). And the rates of leukopenia, gastrointestinal reaction and infection were significantly lower in TAC group and MMF group than those in CYC group (2.8% and 3.6% vs 9.2%, 0.0% and 1.8% vs 19.9%, 60.2% and 63.3% vs 81.6%) (p < 0.05). There was a trend towards lower incidence of side effects in TAC than MMF with no significant difference (Table 4).
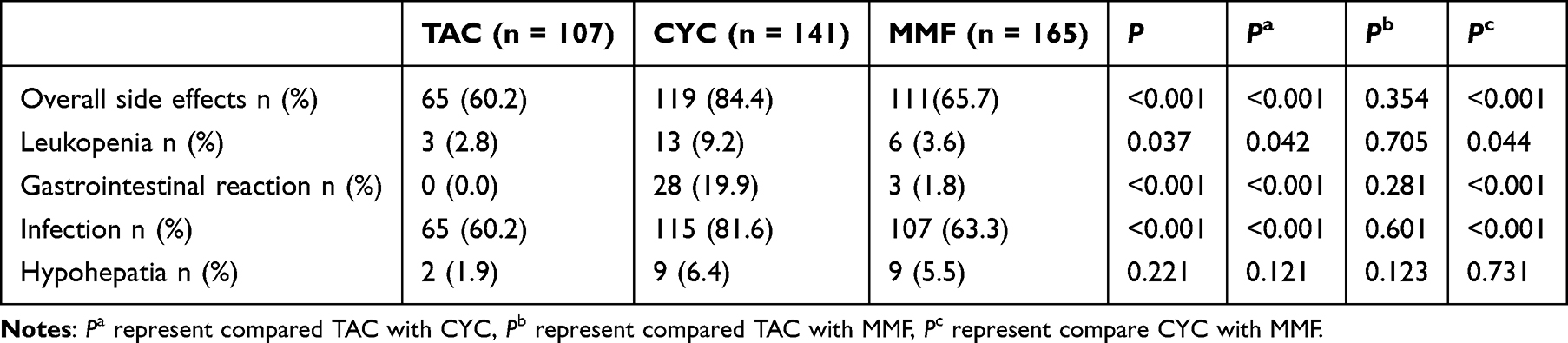 |
Table 4 The Side Effect of Patients with Different Induction Treatment |
The Long-Term Outcomes of IgAVN Patients with Different Treatment
Four hundred and ten IgAVN patients were followed up for 12~134 months in this study, with a median follow-up time of 43 months. Three hundred and thirteen (76.3%) patients were graded into class A, 93 (22.7%) into class B with mild abnormal urine and 4 (1%) into class C with active kidney disease. No class D with renal insufficiency was found in this study. The rate of class A in TAC group (85.8%) was significantly higher than that in CYC group (66.7%) (p = 0.001), and the rate of class B in TAC group (13.2%) was lower than that in CYC group (32.6%) (p < 0.001), but there was no significant difference in class A and class B between TAC group and MMF group. Class C was rare in all three groups without statistically significant difference (Table 5).
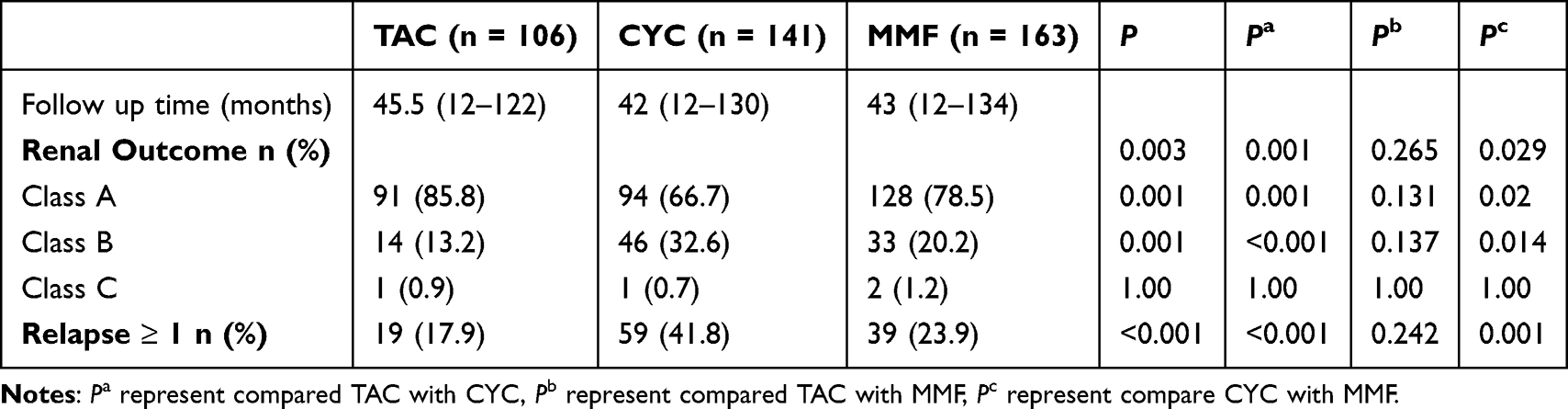 |
Table 5 The Long-Term Outcomes of Patients with Different Responses to Induction Treatment |
In addition, a total of 117 patients (28.5%) experienced at least one relapse during the course of the disease. The probability of no recurrence curves of different induction treatment with TAC, CYC and MMF are shown in Figure 3, and a significant difference was found among three treatments (p = 0.017). The proportion of recurrence in TAC group (17.9%) was significantly lower than that in CYC group (41.8%), but there was no significant difference between TAC group and MMF group (Table 5).
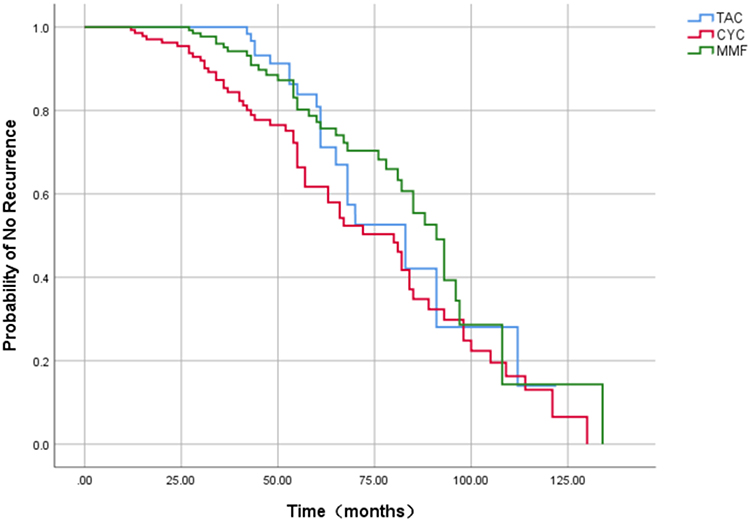 |
Figure 3 Recurrence-free probability analysis K-M curves of the time from diagnosis to last follow-up in patients with different treatment of TAC (Blue), CYC (Red), MMF (Green). |
Discussion
IgAVN is one of the most common secondary kidney diseases in children. While the majority of patients can achieve remission following active treatment, 1% to 7% of patients may still progress to ESKD.11 Some studies have identified that nephrotic syndrome and severe proteinuria in IgAVN as significant risk factors for ESKD.12 Therefore, actively controlling proteinuria is crucial in the management of IgAVN. TAC or CsA (calcineurin inhibitor) has been shown to rapidly reduce urinary protein and achieve remission not only in immune glomerulonephritis but also hereditary podocytopathy.13–15 Although CNIs are not routinely recommended, Chan et al still support the individualized use of TAC according to clinical symptoms and pathological type.16 Therefore, TAC combined with glucocorticoids is preferred for IgAVN children with higher levels of proteinuria and more severe pathological grades in our center.
The effect of treatment in achieving remission is crucial to prevent renal progression. A combination of glucocorticoids and CYC, which has demonstrated relative effectiveness, is more likely to be utilized.17 However, it had been reported that some patients did not achieve remission following treatment with glucocorticoids combined with CYC.18 Additionally, due to the significant side effects of CYC, various treatment regimens have been developed, such as glucocorticoids combined with other immunosuppressants including MMF, and TAC, all of which have also achieved significant efficacy.19 A meta-analysis has reported that MMF has better efficiency and safety compared with CYC.20 In a retrospective study, TAC has been shown to be an effective treatment option for IgAVN who are refractory to CYC or combined with MMF.21 But in the study conducted by Rohner et al, no significant advantage of TAC or MMF or CYC in the efficacy and prognosis of IgAVN was found.22 There are still insufficient studies to compare the efficacy and safety of TAC, CYC and MMF in the treatment of pediatric IgAVN. Therefore, our center has been more proactive in using intensive immunosuppressive therapy for IgAVN in acute lesions, and comparing the efficacy of TAC (a kind of calcineurin inhibitors), MMF and CYC. In this retrospective study, although the CR rate of TAC was higher than CYC at 3 and 6 months, TAC was primarily used in IgAVN patients with higher levels of proteinuria and more severe pathological types, which may bias the conclusions. Therefore, we adjusted for confounding factors and again confirmed that TAC resulted in greater response than CYC. Furthermore, MMF did not show a significant inferiority to CYC in achieving remission. Moreover, TAC demonstrated superior efficacy to CYC in terms of achieving a more rapid and greater extent of reduction in proteinuria.
Several studies have reported that adverse effects of TAC therapy are infrequent and minimal in patients with IgAVN.21,23 Xu et al have demonstrated that MMF has a lower incidence of adverse effects such as gastrointestinal reaction, liver function injury, myelosuppression, alopecia compared with CYC.20 In this study, we found that TAC and MMF showed lower rates of leukopenia, gastrointestinal reactions and infections, as well as a lower overall incidence of adverse effects compared with CYC. These findings suggest that TAC and MMF are relatively safer for the treatment of IgAVN. Notably, although not statistically significant, TAC was associated with a lower incidence of leukopenia, gastrointestinal reactions, infection, and hypohepatia compared with MMF. This may indicate that TAC has fewer side effects and is more secure. However, additional data are required for further support.
Deng et al reported that nearly 97.8% of children with IgAVN had a favorable prognosis, with no cases of renal insufficiency observed during the follow-up period in their cohort.24 In another cohort study, 7.9% of patients with IgAVN progressed to ESKD, and it was found that clinicopathological presentation rather than different therapeutic regimens was a risk predictor for poor outcome.25 Moreover, a prognostic study showed no evidence to support any specific immunosuppressive therapy over others.22 Surprisingly, none of the IgAVN patients in our study had progressed to ESKD during long-term follow-up. Moreover, our study demonstrated that TAC was superior to CYC in achieving more complete renal remission.
There are many factors that influence renal remission and relapse in IgAVN, yet studies on the recurrence of IgAVN are relatively rare. In a cohort study of Japanese children with IgAVN, 16% experienced at least one relapse following combination therapy.26 Zhang et al showed the long-term safety and efficacy of TAC in IgAVN in a randomized controlled trial, and they also found that TAC could significantly reduce the recurrence rate.27 In a retrospective study, an analysis of risk factors for recurrence showed that age range, pathological grade, and treatment were effective predictors of recurrence. Moreover, it was found that MMF or MMF in combination with TAC significantly reduced the recurrence rate.28 In our study, we reported 28.5% patients experienced at least one relapse, which was higher than previously reported. Although we did not perform an analysis of risk factors for recurrence, time-to-recurrence analysis showed that different treatment regimens affected the probability of renal recurrence. Moreover, our study indicated that TAC and MMF combined with glucocorticoid therapy had significantly lower recurrence rates compared to CYC, suggesting that TAC not only provides rapid remission but may also provide long-term renal stability.
Of course, there are several limitations inherent in this study. Firstly, it should be noted that this study is a retrospective analysis, which is subject to numerous biases and confounding factors. For example, this study is a single center study, which may hinder the broad generalization of the conclusions. Therefore, our findings need to be validated through large-scale prospective comparative studies that can better control for these biases. Furthermore, our study showed differences in baseline proteinuria between different treatment, which may have biased the results. Therefore, we performed logistic regression to adjust for confounding factors, which is more reliable for our conclusions. Secondly, although the effects of various treatment regimens on long-term prognosis were compared, no bias correction was carried out, and further validation is requisite.
Conclusion
In summary, we conducted a retrospective study to summarize the efficacy and safety of TAC, CYC and MMF in the treatment of pediatric IgAVN. TAC combined with glucocorticoid therapy can be considered for the induction treatment of IgAVN with higher proteinuria level and severe pathological grades, which can rapidly and effectively reduce the level of urine protein and achieve renal remission. Moreover, TAC can significantly improve renal prognosis and reduce the recurrence rate, making it an effective and safe treatment option for pediatric IgAVN.
Abbreviations
IgAVN, IgA vasculitic nephritis; CYC, cyclophosphamide; TAC, Tacrolimus; MMF, mycophenolate mofetil; ESKD, End-stage kidney disease; CR, Complete remission.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Declarations
The study was approved by the Human Ethics Committee of Tongji Hospital and was conducted in accordance with the tenets of the Declaration of Helsinki.
Consent to Participate
This study was a retrospective study, and therefore the waiver of informed consent had been approved by the ethics committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (Registry number TJ-IRB202404037).
Statement of Data Confidentiality
All authors and ethics committee ensure data confidentiality.
Acknowledgment
The authors thank all patients and their families for participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work for this study was supported by the National Key Scientific Research and Development Program of China (No.2022YFC2705102, No.2022YFC2705103), the Key Scientific Research and Development Program of Hubei Province (No.2022BCA047), Natural Science Foundation of Hubei Province (No.2021CFB073) and Chen Xiaoping Science and Technology Development Foundation of Hubei (CXPJJH121002-202154).
Disclosure
The authors have no competing interests to disclose in this work.
References
1. Kaku Y, Nohara K, Honda S. Renal involvement in Henoch-Schonlein purpura: a multivariate analysis of prognostic factors. Kidney Int. 1998;53(6):1755–1759. doi:10.1046/j.1523-1755.1998.00915.x
2. Chen J, Mao J. Henoch-Schönlein purpura nephritis in children: incidence, pathogenesis and management. World J Pediatrics. 2015;11(1):29–34. doi:10.1007/s12519-014-0534-5
3. Lu S, Liu D, Xiao J, et al. Comparison between adults and children with Henoch–Schönlein purpura nephritis. Pediatric Nephrol. 2015;30(5):791–796. doi:10.1007/s00467-014-3016-z
4. Wakaki H, Ishikura K, Hataya H, et al. Henoch-Schönlein purpura nephritis with nephrotic state in children: predictors of poor outcomes. Pediatric Nephrol. 2011;26(6):921–925. doi:10.1007/s00467-011-1827-8
5. Chartapisak W, Opastiraku SL, Willis NS, et al. Prevention and treatment of renal disease in Henoch-Schönlein purpura: a systematic review. Arch Dis Childhood. 2009;94(2):132–137. doi:10.1136/adc.2008.141820
6. Rovin BH, Adler SG, Barratt J, et al. KDIGO 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int. 2021;100(4S):S1–S276. doi:10.1016/j.kint.2021.05.021
7. Subspecialty Group Of Renal Diseases T S O P. Evidence-based guideline for diagnosis and treatment of Henoch-Schonlein purpura nephritis (2016). Zhonghua Er Ke Za Zhi. 2017;55(9):647–651. doi:10.3760/cma.j.issn.0578-1310.2017.09.003
8. Counahan R, Winterborn MH, White RH, et al. Prognosis of Henoch-Schonlein nephritis in children. BMJ. 1977;2(6078):11–14. doi:10.1136/bmj.2.6078.11
9. Schwartz GJ, Munoz A, Schneider MF, et al. New equations to estimate GFR in children with CKD. J Am Soc Nephrol. 2009;20(3):629–637. doi:10.1681/ASN.2008030287
10. Ren P, Han F, Chen L, et al. The combination of mycophenolate mofetil with corticosteroids induces remission of Henoch-Schonlein purpura nephritis. Am J Nephrol. 2012;36(3):271–277. doi:10.1159/000341914
11. Soylemezoglu O, Ozkaya O, Ozen S, et al. Henoch-Schonlein nephritis: a nationwide study. Nephron Clin Pract. 2009;112(3):c199–c204. doi:10.1159/000218109
12. Coppo R, Andrulli S, Amore A, et al. Predictors of outcome in Henoch-Schonlein nephritis in children and adults. Am J Kidney Dis. 2006;47(6):993–1003. doi:10.1053/j.ajkd.2006.02.178
13. Zhang Q, Shi S, Zhu L, et al. Tacrolimus Improves the Proteinuria Remission in Patients with Refractory IgA Nephropathy. Am J Nephrol. 2012;35(4):312–320. doi:10.1159/000337175
14. Grossman OK, Schretlen CF, Nield LS. Concordant nephrotic syndrome in twins with PAX2 and MYO1E mutations. Clin Nephrol Case Stud. 2022;10:37–41. doi:10.5414/CNCS110799
15. Park JM, Won SC, Shin JI, et al. Cyclosporin A therapy for Henoch-Schonlein nephritis with nephrotic-range proteinuria. Pediatr Nephrol. 2011;26(3):411–417. doi:10.1007/s00467-010-1723-7
16. Lee MH, Chan EY, Ma AL. Timely and individualized use of immunosuppression is associated with favourable outcomes in paediatric IgA vasculitis nephritis. Pediatr Nephrol. 2022;37(4):913–914. doi:10.1007/s00467-021-05405-0
17. Sestan M, Jelusic M. Diagnostic and management strategies of IgA vasculitis nephritis/Henoch-Schonlein Purpura nephritis in pediatric patients: current perspectives. Pediatric Health Med Ther. 2023;14:89–98. doi:10.2147/PHMT.S379862
18. Tarshish P, Bernstein J, Edelmann JCM. Henoch-Schönlein purpura nephritis: course of disease and efficacy of cyclophosphamide. Pediatric Nephrol. 2004;19(1):51–56. doi:10.1007/s00467-003-1315-x
19. Kawasaki Y. The pathogenesis and treatment of pediatric Henoch–Schönlein purpura nephritis. Clin Exp Nephrol. 2011;15(5):648–657. doi:10.1007/s10157-011-0478-1
20. Wang D, Liu T, Lu J, et al. Efficacy and safety of mycophenolate mofetil versus cyclophosphamide therapy for Henoch schonlein purpura nephritis in children: a meta-analysis. Medicine. 2024;103(30):e39059. doi:10.1097/MD.0000000000039059
21. Gan Y, Chen J, Wang M, et al. The efficacy and safety of tacrolimus in treating refractory IgA vasculitis nephritis: a single-center retrospective study on 16 cases. Clin Kidney J. 2024;17(5):sfae115. doi:10.1093/ckj/sfae115
22. Rohner K, Marlais M, Ahn YH, et al. Outcome of immunosuppression in children with IgA vasculitis-related nephritis. Nephrol Dial Transplant. 2024;39(8):1299–1309. doi:10.1093/ndt/gfae009
23. Zhang D, Hao G, Li C, et al. Off-label use of tacrolimus in children with Henoch-Schönlein purpura nephritis: a pilot study. Arch Dis Childhood. 2018;103(8):772–775. doi:10.1136/archdischild-2017-313788
24. Lv Y, Fu R, Peng XJ, et al. Comparative study on clinicopathological features and prognosis of IgA vasculitis nephritis and IgA nephropathy in children. Bmc Pediatr. 2023;23(1):423. doi:10.1186/s12887-023-04243-3
25. Tan J, Tang Y, Xu Y, et al. The clinicopathological characteristics of Henoch-Schönlein Purpura nephritis with presentation of nephrotic syndrome. Kidney Blood Pressure Res. 2019;44(4):754–764. doi:10.1159/000501459
26. Nagai S, Horinouchi T, Ninchoji T, et al. Long-term outcome of combination therapy with corticosteroids, mizoribine and RAS inhibitors as initial therapy for severe childhood IgA vasculitis with nephritis. Pediatr Nephrol. 2023;38(12):4023–4031. doi:10.1007/s00467-023-06052-3
27. Zhang H, Li X, Xu H, et al. Effect and safety evaluation of tacrolimus and tripterygium glycosides combined therapy in treatment of Henoch–Schönlein purpura nephritis. Int J Urology. 2021;28(11):1157–1163. doi:10.1111/iju.14665
28. Mukanhaire L, Ren X, Liu G, et al. Recurrence of Henoch Schoenlein Purpura nephritis in children: a retrospective study. Heliyon. 2023;9(11):e22501. doi:10.1016/j.heliyon.2023.e22501
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
How to Choose Treatment Regimens for Idiopathic Membranous Nephropathy Patients with PLA2R-Negative: A Single-Center Retrospective Cohort Study
Zhou Z, Zou Y, Ke B, Shen W
ImmunoTargets and Therapy 2025, 14:515-522
Published Date: 6 May 2025