Back to Journals » Journal of Blood Medicine » Volume 16
Efficacy and Cost-Effectiveness of Low-Dose vs Standard Dose Prophylaxis for Hemophilia in Indonesia: A Systematic Review
Authors Romadhon PZ ![]() , Auliya K, Heryana MO
, Auliya K, Heryana MO ![]() , Erawati AA, Mahdi BA, Suryantoro SD
, Erawati AA, Mahdi BA, Suryantoro SD ![]() , Putri AE, Yusoff NM
, Putri AE, Yusoff NM
Received 12 December 2024
Accepted for publication 18 March 2025
Published 2 May 2025 Volume 2025:16 Pages 205—220
DOI https://doi.org/10.2147/JBM.S511906
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Pradana Zaky Romadhon,1,2 Kamila Auliya,2 Made Oka Heryana,2 Ajeng Ayu Erawati,2 Bagus Aulia Mahdi,3 Satriyo Dwi Suryantoro,1 Aditea Etnawati Putri,4 Narazah Mohd Yusoff5
1Doctoral Program of Medical Science, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia; 2Department of Internal Medicine, Airlangga University Hospital, Surabaya, Indonesia; 3Department of Internal Medicine, Muhammadiyah University, Surabaya, Indonesia; 4Department of Clinical Pathology, Universitas Airlangga Hospital, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia; 5Advanced Medical and Dental Institute, Universiti Sains Malaysia (USM), Kepala Batas, Penang, Malaysia
Correspondence: Pradana Zaky Romadhon, Doctoral Program of Medical Science, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia, 60115, Email [email protected]
Abstract: Studies on high-dose prophylaxis therapy using Factor VIII show promising decrease in the Annual Bleeding Rates (ABR) in hemophilia patients. However, the greater dose and frequency raise concerns on cost considerations and adherence of the patients, especially in several countries where resources are limited. Other data has proven that the low dose prophylaxis is also promising regarding the decrease of ABR. The purpose of this systematic review is to conduct a comprehensive analysis of the lower dosage formulation used for prophylaxis in hemophilia. A PubMed and Embase database search was performed based on articles that met the following criteria: written in English language and published within the last 10 years. Consequently, the following key terms were used in combination: ‘high dose’, ‘low dose’, ‘recombinant’, ‘prophylaxis’, and ‘hemophilia’ in different combinations. 19 articles were included for this review. 10 of the investigated papers demonstrated decrease in ABR, functional improvement of affected joints, alleviation of pain, and a better quality of life in hemophilia patients. Low dose prophylaxis has proven to significantly improve symptoms, lower ABR and preserve joint and bone health compared to episodic or on-demand treatment. Furthermore, low dose prophylaxis (LDP) was also observed to be cost-effective and more convenient in certain countries, especially in south-east Asia where resources are limited. Overall, low dose prophylaxis appears to be non-inferior in improving the overall Quality of Life in people with hemophilia, and therefore could be a beneficial alternative in countries of the south east Asian region.
Keywords: hemophilia, prophylaxis, South-East Asia, factor VIII
Introduction
Hemophilia is an X-linked inherited hematologic disorder characterized by the deficiency of Factor VIII (Hemophilia A) or Factor IX (Hemophilia B), the crucial proteins involved in the blood coagulation cascade. This deficiency leads to prolonged bleeding episodes, particularly in joints and muscles. Globally, hemophilia affects approximately 1 in 5000 male births for hemophilia A and 1 in 30,000 for hemophilia B, making it a rare disorder.1,2 By the end of 2018, there were 2098 haemophilia patients recorded based on data from the Indonesian Hemophilia Society, which is estimated to be only 10% of the total estimated number of patients (20,000–25,000 cases in total) suspected due to the inadequate screening. The management of haemophilia in Indonesia has been improving since the 1970‐1980s era, both in diagnosis and in treatment.1,2
In high-resource countries, early diagnosis and treatment options, including prophylaxis with clotting factor concentrates, have dramatically improved patient outcomes. Prophylactic therapy with FVIII is considered to be the optimal treatment for patients and is aimed at reducing the number of spontaneous hemorrhages as for improving overall quality of life in People with Hemophilia (PWH). In adults, prophylaxis is aimed at slowing the progression of joint deterioration and improving mobility, namely secondary prophylaxis. Previous studies have confirmed the efficacy of prophylaxis in children in preventing or delaying arthropathy, and early initiation of prophylaxis may have a protective effect against inhibitor development.3,4
The World Federation of Hemophilia (WFH) recommends that high- or intermediate-dose prophylaxis be started early for all severe haemophilia patients as the primary option, substantially reducing bleeds compared with on-demand treatment. On the other hand, low-dose prophylaxis was recommended for countries with limited resources. Recent studies investigated low-dose factor prevention as an alternative economically feasible approach.2,5 In Indonesia prophylaxis with standard dose is beyond affordability due to the high cost, availability of concentrate across all provinces and limited financial support from the government.2,5
The first low-dose prophylaxis (LDP) study in Indonesia by Chozie et al proved that low-dose prophylaxis significantly reduced bleeding episodes compared to on-demand therapy.1 In another study, long-term low-dose prophylaxis of children with severe haemophilia A reduced their joint damage and improved their quality of life (QOL) compared with on-demand treatment.1,6 A study about haemophilia patients in the Netherlands and Sweden found a more intensive and higher-dosed regimen may provide slightly improved outcomes at a significant cost increase.7
The aim of this literature study is to compare the effectiveness of FVIII prophylaxis for hemophilia A, based on the Annual Bleeding Rate (ABR), Annual Joint Bleeding Rate (AJBR), Functional Independence Score in Hemophilia (FISH) and other parameters defining overall quality of life in PWH. The purpose of this study is to give recommendations for deciding the best prophylaxis dose and method, based on availability and cost-effectiveness, that could be applied in South-East Asia, especially Indonesia.
Materials and Methods
Database Search and Article Selection
We conducted comprehensive literature study from PUBMED and Embase database, for the past 15 years, starting from 1 January 2009 to 1 October 2024. The following keywords are used with boolean operators; (Hemophilia) AND ((“Prophylaxis” AND “High Dose”) OR (“Prophylaxis” AND “Low Dose”) OR (“Prophylaxis” AND “Recombinant”)). All original articles are included in this study. All publications were examined against pre-set inclusion and exclusion criteria. For the selection process, Rayyan software was used to assist in the screening and selection of the studies.
Inclusion and Exclusion Criteria
Inclusion and Exclusion criteria were labeled in the application. The inclusion criteria are as follows: systematic review, meta-analysis, literature review, interventional and non-interventional studies, studies comparing two or more of the following; high-dose, low-dose, and recombinant therapy, multi-centered or single-centered studies. Exclusion criteria are as follows: conference abstracts, reviews, commentary, immune tolerance induction protocols using LDP, studies not mentioning specific dose of FVIII usage, on going studies, studies published in other languages.
Study Selection and Data Extraction
The study selection, method planning, and instruction provided by author 1 in the first step. Data extraction of all publications, screening, inclusion and exclusion processes were performed by author 2, 3 and 4, and being reviewed by author 5. Duplicates of publications were further screened. Any conflicts during the selection process were resolved by consensus or through arbitration by author 5. Study group and treatment are sorted using the following protocols: 1) Low dose efficacy compared to on-demand or episodic treatment, 2) Low dose efficacy compared to intermediate or higher dose prophylaxis. At the final step, the review and editing of the manuscript was directed by authors 1, 3 and 5. The following Figure 1 describes the flowchart of the process.
 |
Figure 1 Flowchart of the process. |
Results
We identified 1409 studies from the search output. After screening the titles, abstracts, removal of duplicates and non-English publications, 779 articles were assessed in full (Figure 1). Of these, 19 studies were included in the final review. Of these, ten compared LDP with episodic or on-demand treatment, seven examined the efficacy of recombinant Factor VIII (rFVIII) administered in low doses, while three studies directly compared LDP with intermediate- and high-dose regimens in reducing the annualized bleeding rate.
Of the selected articles, 10 studies were prospective cohorts of patients on LDP in Table 1. Studies of Low dose prophylaxis effectivity compared with on-demand or episodic treatment in hemophilia. Five of these studies were long-term studies extending beyond two years, while five had implemented dose/frequency escalation protocols based on clinical outcomes and PK parameters. Of these, four were randomized controlled trials. The most frequent LDP regimen used among the various studies was administration at 10–15 IU/kg body weight twice a week.
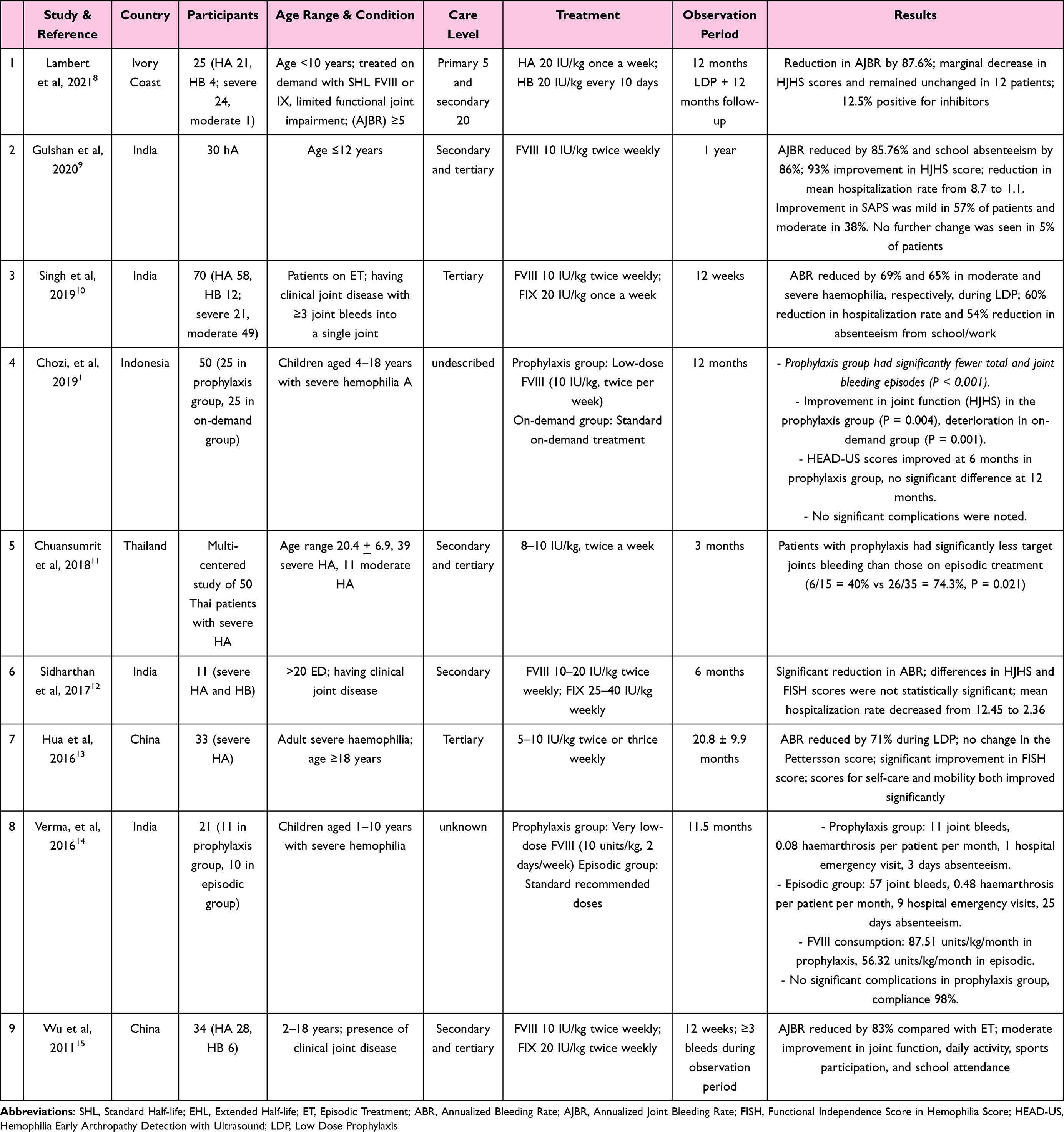 |
Table 1 Studies of Low Dose Prophylaxis Effectivity Compared with On-Demand or Episodic Treatment in Hemophilia |
Studies on efficacy of prophylaxis using recombinant Factor VIII regimens are summarized in Table 2 (Effectivity of Low Dose Prophylaxis using Recombinant Factor VIII). Patients treated with recombinant FVIII at various dosing and frequency schedules have demonstrated significant reductions in bleeding episodes. The studies also suggest a good safety profile, with no development of FVIII inhibitors and only a few adverse events reported. Table 3 (Low dose prophylaxis compared to intermediate or higher dose prophylaxis) presents data comparing low-dose and high-dose prophylaxis. They achieved an ABR of 5.0 for low-dose and 2.0 for high-dose prophylaxis, though the latter did not attain statistical significance.
 |
Table 2 Effectivity of Low Dose Prophylaxis Using Recombinant Factor VIII |
 |
Table 3 Low Dose Prophylaxis Compared to Intermediate or Higher Dose Prophylaxis |
We assessed the medical costs of hemophilia across several countries, including nations in South Asia, parts of Greater Asia, and some Western countries in Table 4: Cost comparison of hemophilia prophylaxis treatment across countries, to estimate the costs associated with low-dose compared to higher-dose treatment and to review government policies regarding hemophilia care, as detailed in Tables 4 and 5. Cost data were gathered from published studies specific to each country. Where data on certain costs were not available, we estimated them using data from the Report on the Annual Global Survey of Hemophilia in 2021, in which data on FVIII consumption by country are made available.25 In Table 5 (Government Health Policy supporting hemophilia prophylaxis therapy), different government policies across the countries listed in Table 4 are represented for the comparison and analysis of policies from different regions feasible.
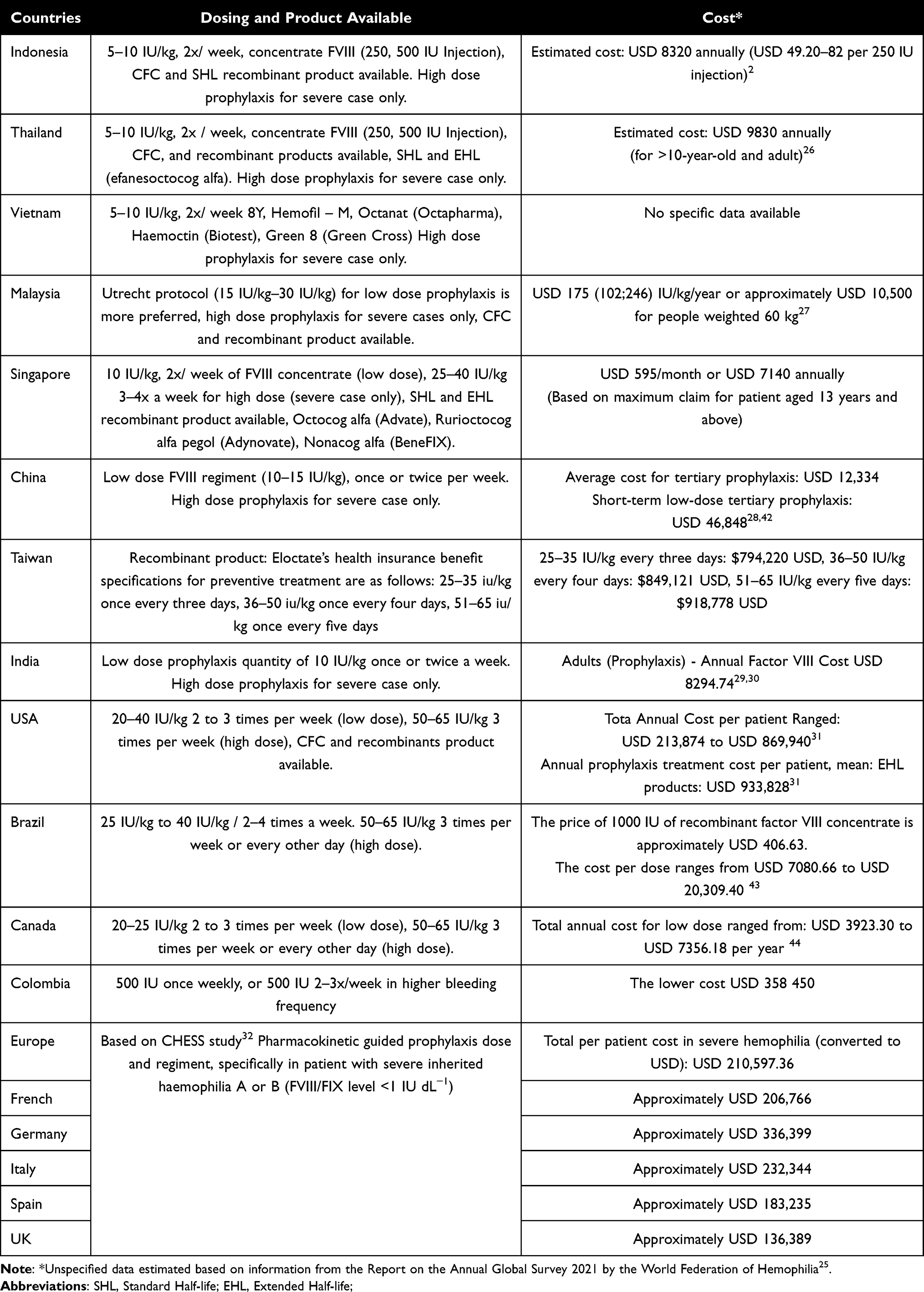 |
Table 4 Cost Comparison of Hemophilia Prophylaxis Treatment Across Countries |
 |
Table 5 Government Health Policy Supporting Hemophilia Prophylaxis Therapy |
Discussion
Low-Dose Prophylaxis Effectivity in Lowering ABR and AJBR in Hemophilia
Based on the literature review of 19 articles including systematic review, meta-analysis and multicentered observational studies, most of the study results describe that low-dose prophylaxis is non-inferior in improving ABR (Annualized Bleeding Rate), AJBR (Annualized Joint Bleeding Rate), FISH (Functional Independence Score in Hemophilia Score), and HEAD-US (Hemophilia Early Arthropathy Detection with Ultrasound) in PWH. As presented in Table 1, low-dose prophylaxis compared to on-demand/episodic prophylaxis has shown significant results. All studies in Table 1 conclude that low-dose prophylaxis has shown to significantly reduce ABR, 4 studies specifically describe improvement in AJBR.8,9,15,16 Three studies specifically presented improvement of the Hemophilia Joint Health Score (HJHS).1,8,9 One study conducted by Chozie et al presented an improvement in HEAD-US, and 2 studies showed improvement in FISH score in PWH receiving prophylaxis treatment.13
Low-dose prophylaxis in hemophilia has been shown to significantly reduce the frequency of bleeding episodes and improve joint outcomes compared with on-demand treatment. A study by Lambert et al (2021), including patients from the Ivory Coast, determined LDP associated with an AJBR reduction by 87.6% over a continuous period of 12 months.8 This study further reiterated that there were minor changes in HJHS; 12 patients did not deteriorate in joint health, and inhibitors developed in only 12.5% of the participants. A study by Gulshan et al (2020), conducted in India with hemophilia A patients discovered that infusions of 10 IU/kg twice a week cause a reduction of 85.76% in AJBR, whereas school absenteeism was reduced by 86%.9 The study also noted that the improvement in joint health was remarkable and increased the HJHS scores by 93%, drastically reducing hospitalization rates from 8.7 to 1.1 admissions per year.
A study conducted by Singh et al further concluded that the effectiveness of LDP in twice-weekly prophylaxis with 10 IU/kg of FVIII for patients with moderate-to-severe hemophilia led to a 69% reduction in ABR and a 65% reduction in AJBR, among other advantages over reductions in hospitalization rates and absence from school or work.10 In the much smaller study by Verma et al (2016) in India, children on very low-dose FVIII regimen of 10 IU/kg twice per week had significantly fewer joint bleeds, 0.08 haemarthrosis per patient per month, and less hospitalization compared to those on episodic therapy, 0.48 haemarthrosis per patient per month.14 The study also reported better compliance, 98%, in the LDP group, with no significant complications. Concisely, these data support the fact that the clinical benefit of LDP depends on an improvement in bleeding control and joint health in patients with hemophilia, while LDP may also be a viable option for on-demand treatments in reducing morbidity and improving the quality of life.8–10,14
A systematic review and meta-analysis study, conducted by Delgado-Flores et al, in Table 3, calculated the pooled statistic of 9 RCT studies of prophylaxis effectivities in lowering ABR and AJBR. It compared prophylaxis in all kinds of doses (low, intermediate, high) to on-demand and episodic treatment.24 There is a significant difference of ABR and AJBR rates in the two groups (p = 0.003, I2 = 82.9%). While there is no significant difference between the three sub-groups (Low vs Intermediate vs High dose) in lowering ABR and AJBR. These findings further enhanced the evidence that low dose is indeed non-inferior compared to high-dose prophylactic, especially when the goal is to lower ABR and AJBR.24
When using a recombinant factor (Table 2), it is more convenience to administer Low Dose prophylaxis, especially for Extended Half Life (EHL) products. It is suggested that low-dose prophylaxis with various recombinant factor VIII (rFVIII) products can provide significant clinical benefits in hemophilia A patients, showing the non-inferiority of lower dose prophylaxis compared to standard higher dose treatment. Mathias et al showed that 92.9% of bleeding episodes were markedly reduced in the population treated with simoctocog alfa treatment, and 92.3% were controlled with just 1 or 2 dose per week, showing effective bleeding control even at lower doses.17 Similarly, Choraria et al demonstrated the safety and efficacy of moroctocog alfa, while Wu et al reported a high hemostatic success rate of over 95% with turoctocog alfa, showing its effectiveness in both pediatric and adult patients.18
Valentino et al (2012) showed that prophylaxis cut annual bleeding rates (ABRs) by 60% compared to on-demand treatment (P<0.0001) where a third of clients on treatment did not have bleeding episodes.3 In comparison to Powell et al (2012), Manco-Johnson et al (2013) confirmed that rFVIII-FS prophylaxis virtually eliminated his patients’ bleeding episodes that required in-patient admission and also lowered his patients’ ABRs from 27.9 to zero when compared with on-demand treatment.21,22 These results are reinforcing that prophylaxis during treatment does not increase adverse events or FVIII inhibitors but rather improves the patient’s health by reducing bleeding episodes.
Low-Dose Prophylaxis in Comparison with Standard or Higher Dose Prophylaxis
Low-dose prophylaxis has demonstrated efficacy in reducing the annualized bleeding rate (ABR) in patients with severe hemophilia A, even when compared to higher-dose regimens. Multiple studies support the notion that LDP provides sufficient control of bleeding episodes, contributing to a reduction in joint damage and improvement in overall patient outcomes. For instance, Yang et al23 found that while high-dose prophylaxis (30–40 IU/kg, three times weekly) produced a numerically lower ABR (median: 2.0; range: 0–2.0) than low-dose prophylaxis (20–30 IU/kg, twice weekly), ABR (median: 5.0; range: 2.0–11.0), the difference was not statistically significant, suggesting that LDP can achieve comparable bleeding control. This result is consistent with evidence from the studies in Table 1, where patients on LDP experienced a clinically acceptable reduction in bleeding episodes, particularly in resource-limited settings where high-dose regimens may be impractical.9,10,14
Further evidence by Gringeri et al and Mathias et al also supports the effectiveness of prophylaxis, including lower-dose regimens, in reducing hemarthroses and preventing joint damage over time.17,20 Gringeri et al reported fewer joint bleeds in children receiving 25 IU/kg thrice a week, with no radiologic signs of arthropathy when early prophylaxis has been initiated, while Mathias et al demonstrated that simoctocog alfa prophylaxis achieved a success rate of 92.9% in treating bleeding episodes.20 Although higher-dose prophylaxis may show prominent advantage in ABR, the clinical impact of the LDP is quite significant and hence clinically effective as a viable non-inferior strategy for the patients. The same result of significant outcome comparing low-dose prophylaxis and on-demand prophylaxis also found in the study conducted by Chuansumrit et al (2019) shows that low-dose prophylaxis could significantly lower overall bleeding rate compared to on-demand treatment.11 This concluded that low-dose treatment, however, has a robust advantage in improving bleeding rate, musculoskeletal health, and overall quality of life in PWH.
Musculoskeletal Health Improvement in Low Dose Prophylaxis
Joint and bone health are important aspects of hemophilia management, aiming for the prevention of hemarthroses and long-term arthropathy. Chozi et al conducted a study comparing low dose and on-demand prophylaxis in children PWH.1 The result showed a significantly fewer total and joint bleeding rate episode (p<0.001), and improvement in all functions including, HJHS score (p=0.001) in the prophylactic group by 6 months of treatment compared to the on-demand group, and no significant complications were found. HEAD-US Score, however, showed no significant difference between the two groups.1 Sidhartan et al (2017) conducted the prophylaxis study in resource limited setting in India with the result of significant reduction in ABR; though differences in HJHS and FISH were not statistically significant. However, mean hospitalization rate decreased from 12.45 to 2.36.12
In a study by Gringeri et al, prophylactic treatment with recombinant factor VIII significantly reduced joint bleeds and the progression of joint damage compared to episodic therapy.20 Patients in the prophylaxis group exhibited fewer hemarthrosis (0.20 vs 0.52 per patient per month) and a lower percentage of radiological signs of arthropathy (29% vs 74%), demonstrating the efficacy of early intervention in preserving joint function. Moreover, in Valentino et al, a comparison between standard prophylaxis and PK-tailored prophylaxis revealed that both regimens resulted in a notable reduction in annual bleeding rates (ABRs), particularly in joint bleeds, further highlighting the importance of consistent factor replacement therapy for maintaining joint health.3
Newer imaging techniques include HEAD-US for early diagnosis of joint changes in hemophilia patients. HEAD-US, combined with clinical assessment, such as HJHS, thus enables clinicians to monitor subtle damage arising from progressive joint disease. Yang et al demonstrated that while prophylaxis with a low dose was effective, high-dose prophylaxis slightly fared better in terms of the outcome of preventing bleeding.37 Such studies using HEAD-US and HJHS applications underpin the need for early detection and individualized prophylaxis regimens to reduce joint damage in patients with hemophilia, especially given that low-dose prophylaxis has been considered adequate to prevent deterioration of the joints.
Annual Cost for Hemophilia Treatment in Different Countries
Cost of treatment for hemophilia using FVIII prophylaxis is quite different in different countries, which depends upon health policy, local production, importation, and various subsidies available in each country. In the low-income category of countries, the prices of FVIII concentrates like Octanate, Beriate, and Haemoctin might be high since their medicines are highly dependent on imports. A single 250 IU FVIII injection costs ranging USD 49.20–82 in Indonesia.2 In Thailand, Standard Half Life (SHL) FVIII concentrate of 34,500–55,500 IU (approximately 750–1000 IU/week) and SHL FIX concentrate of 23,000–24,000 IU (approximately 500 IU/week), intended for prophylaxis, are reimbursable annually.33,34 With lower product costs, however, many patients in these countries still cannot access higher dose prophylaxis; the main reasons include high prices and generally limited insurance coverage, especially in the cases of severe conditions.
On the other hand, countries like Malaysia and Singapore provide better government support for the treatment of hemophilia and hence have given better access to the patients. The annual treatment cost of FVIII in Malaysia reportedly could go as high as RM 4.5 million (approximately USD 1 million). Low dose prophylaxis is more preferred in practice with Utrecht protocol of 15–30 IU/kg, two to three times a week. The price per patient is approximately USD 175 (102;246) IU/kg/year or approximately USD 10,500 for people weighted 60 kg.27 The cost of the low dose prophylaxis is higher compared to on-demand treatment, however prophylactic therapy results in significantly less ABR and better joint health. In Singapore, there are subsidies from the Hemophilia Society of Singapore. A member is able to claim with the maximum of approximately USD 595 per month or approximately USD 7140 annually for those aged 13 years and above.36
Large-population countries indeed face special challenges in gaining appropriate access to FVIII prophylaxis. Tertiary prophylaxis in China can amount to as much as USD 12,334 per patient annually, amidst large disparities in coverage across various cities.28,38 India does report that 74% of people with hemophilia receive some kind of support either free or at low cost, but access to prophylaxis, especially low-dose, is challenging in this setting, particularly in rural areas.29,30 Most high-income countries such as the USA, Canada, and European countries have government programs that cover the majority of the costs for FVIII prophylaxis. In the USA, Medicaid pays the majority cost of this treatment for those of low incomes, while in Canada provincial health plans fund a significant proportion of treatment costs.31 In fact, Belgium currently offers high-dose options through its government-funded health insurance, with options up to 69 IU/kg/week available for the most severe cases.39
The huge cost and the availability contrast among countries bring into focus the difficulties that low- and middle-income countries face in offering sustainable care for hemophilia. While high-income countries have more access to treatment due to better government subsidies for treatment and insurance coverage, individuals in poorer countries often rely on humanitarian aid, charity, or cost-sharing mechanisms to afford the treatment they so desperately need. This wide disparity in treatment availability between countries, therefore, calls for more holistic policies and international cooperation to meet the needs of the disadvantaged regions regarding persons with hemophilia.
Cost-Effective Prophylaxis Treatment in Developing Countries
The management of hemophilia includes integrated care and primary care strategies to develop cost-effective treatment approaches, not only in developed countries but also in resource-limited settings. Key aspects of this care include treatment types, prevention of bleeding episodes, joint health maintenance, and quality of life improvement. Access to effective treatment remains a challenge in many nations, especially in countries where government policies do not adequately support hemophilia care. Socioeconomic factors, age, and the severity of hemophilia significantly impact treatment availability and accessibility. Although several countries have made significant advances in hemophilia management and insurance coverage, considerable disparities persist globally.1,2
Table 4 and 5 show studies comparing low-dose prophylaxis (LDP) and high-dose prophylaxis (HDP), highlighting outcome parameters from various countries, including available products and government coverage. Primary prophylaxis doses range from low-dose options (10–15 IU/kg) to high-dose regimens (25–40 IU/kg), with administration typically 2–3 times weekly. Secondary prophylaxis has been shown to effectively reduce bleeding episodes and improve quality of life compared to on-demand treatment. A study by the Hemophilia Society reported that LDP led to reductions in annualized bleeding rate (ABR), improvements in joint function, pain, and health-related quality of life (HRQoL) when compared to episodic treatment (ET). Developing countries may consider LDP as a first step before transitioning to a recombinant regiment.
A randomized study from Indonesia, using LDP (5–10 IU/kg twice weekly) with FVIII concentrates (eg, Octanate, Beriate, Haemoctin), showed a marked reduction in ABR and improved joint function, although insurance coverage was limited.1 The Hemophilia Society’s ASEAN consensus journal analysis recommended fixed doses (5–10 IU/kg twice weekly) supported by government health insurance, with IDP reporting zero bleeds at the end of treatment. In Singapore and under the Malmo protocol, HDP (25–40 IU/kg three times/week) and 50 IU/kg twice/week for hemophilia B showed efficacy in severe cases, with partial government coverage.25,36
Robust health systems and financial support mean that, in most European countries, as represented by the CHESS study, full coverage of prophylaxis treatment for hemophilia is possible.32 The high cost of treatment, especially EHL products, does not represent a barrier in these regions, with the annual prophylaxis cost ranging from 210,597 to 933,828 USD per patient. Such coverage is critical for ensuring that patients can receive consistent and effective prophylactic treatment for reducing bleeding episodes and long-term complications from hemophilia. This comprehensive prophylaxis coverage in high-income countries further illustrates how well the delivery of preventive care works and underlines the important role of government healthcare programs in supporting the financial accessibility of essential treatments.
On the contrary, middle to low-income countries like Indonesia, Thailand, and Malaysia have increasingly considered low-dose prophylaxis regimens as reasonable cost-effective alternatives. Low-dose prophylaxis remains quite within the budgets of governments, costing from USD 8320 to USD 28,988 annually.2,33,35 This means that even highly resource-constrained countries can still afford to make sure the health of their hemophilia patients is brought to the forefront of their agendas. With the institution of low-dose prophylaxis, governments can still attain a good level of reduction in bleeding episodes and enjoy an improved quality of life by the hemophilia patients.
Conclusion
The recognized standard dose of hemophilia prophylaxis ranges from 30 to 60 IU/kg of FVIII, administered 3 to 4 times a week, which makes it inconvenient for certain regions with limited resource. Cost and accessibility remain barriers in developing countries, especially in low- to middle-income countries where access to treatment is limited by high costs and inadequate support. Several researches have been conducted to study the efficacy of lower prophylaxis dose as the alternative to lower bleeding rates and improving quality of life of PWH. This review highlights that low-dose prophylaxis (LDP) is effective in reducing annualized bleeding rates (ABR) and annual joint bleeding rates (AJBR), making it a viable alternative to the standard dose, especially in resource limited countries. LDP is associated with notable reductions in bleeding episodes, without increased risks of thrombosis or FVIII Inhibitor formation. Early prophylaxis, using low dose FVIII, has been shown to significantly improve outcomes. However, continued advocacy for equitable healthcare policies and resources to support hemophilia management will be essential in addressing the global disparities in treatment access and outcomes. As the hemophilia community moves forward, strategies centered on LDP can provide a meaningful balance between clinical efficacy, cost-effectiveness, and improved quality of life for patients navigating the complexities of hemophilia. Overall, LDP is non-inferior to higher doses of prophylaxis in managing hemophilia and improving patient quality of life, particularly in settings where cost and accessibility are concerns.
Acknowledgments
We would like to extend our gratitude to our Alma mater, Airlangga University to provide support for our study process.
Funding
This study was funded by LPPM (Lembaga Penelitian dan Pengabdian Masyarakat, Institute of Research and Community Service) Airlangga University, under the scheme of PDU (Penelitian Dasar Unggulan, Leading Basic Research) Airlangga University 2024, with grand number; 4510/B/UN3.FK/PT.01.03/2024.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chozie NA, Primacakti F, Gatot D, Setiabudhy RD, Tulaar ABM, Prasetyo M. Comparison of the efficacy and safety of 12‐month low‐dose factor VIII tertiary prophylaxis vs on‐demand treatment in severe haemophilia A children. Haemophilia. 2019;25(4):633–639. doi:10.1111/hae.13770
2. Indonesia Ministry of Health. Keputusan Menteri Kesehatan Republik Indonesia Nomor HK.01.07/Menkes/243/2021 Tentang Pedoman Nasional Pelayanan Kedokteran Tata Laksana Hemofilia. Indonesia Ministry of Health. 2021.
3. Valentino LA, Mamonov V, Hellmann A, et al. A randomized comparison of two prophylaxis regimens and a paired comparison of on‐demand and prophylaxis treatments in hemophilia A management. J Thromb Haemost. 2012;10(3):359–367. doi:10.1111/j.1538-7836.2011.04611.x
4. Srivastava A, Santagostino E, Dougall A, et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia. 2020:26(S6):1–158. doi:10.1111/hae.14046.
5. Munawar Ali R, Abid M, Zafar S, et al. Management of severe hemophilia a: low-dose prophylaxis vs. on-demand treatment. Cureus. 2023;15:1. doi:10.7759/cureus.41410
6. Wu Y, Lu J, Zhou Y, et al. Long‐term joint outcomes of regular low‐dose prophylaxis in Chinese children with severe haemophilia A. Haemophilia. 2021;27(2):237–244. doi:10.1111/hae.14256
7. Fischer K, Steen Carlsson K, Petrini P, et al. Intermediate-dose versus high-dose prophylaxis for severe hemophilia: comparing outcome and costs since the 1970s. Blood. 2013;122(7):1129–1136. doi:10.1182/blood-2012-12-470898
8. Lambert C, Meité N, Sanogo I, Lobet S, Hermans C. Feasibility and outcomes of low‐dose and low‐frequency prophylaxis with recombinant extended half‐life products (Fc‐rFVIII and Fc‐rFIX) in Ivorian children with hemophilia: two‐year experience in the setting of World Federation of Haemophilia humanitarian aid programme. Haemophilia. 2021;27(1):33–40. doi:10.1111/hae.14216
9. Gulshan S, Mandal PK, Phukan A, et al. Is low dose a new dose to initiate hemophilia a prophylaxis? – a systematic study in Eastern India. Indian J Pediatr. 2020;87(5):345–352. doi:10.1007/s12098-019-03179-w
10. Singh A, Mehta S, Goyal LK, Mehta S, Sharma BS. Low dose prophylaxis vis-a-vis on-demand treatment strategies for hemophilia: a cost effective and disability attenuating approach. J Assoc Phys Ind. 2019;67(1):1.
11. Chuansumrit A, Sosothikul D, Natesirinilkul R, Lektrakul Y, Charoonruangrit U. Efficacy and safety of low‐dose prophylaxis of highly purified plasma‐derived factor VIII concentrate produced by the national blood centre, Thai Red Cross Society. Haemophilia. 2018;24(5). doi:10.1111/hae.13601
12. Sidharthan N, Sudevan R, Narayana Pillai V, et al. Low‐dose prophylaxis for children with haemophilia in a resource‐limited setting in south India—A clinical audit report. Haemophilia. 2017;23(4). doi:10.1111/hae.13272
13. Hua B, Lian X, Li K, Lee A, Poon MC, Zhao Y. Low-dose tertiary prophylactic therapy reduces total number of bleeds and improves the ability to perform activities of daily living in adults with severe haemophilia A. Blood Coagul Fibrinolysis. 2016;27(2):136–140. doi:10.1097/MBC.0000000000000389
14. Verma SP, Dutta TK, Mahadevan S, et al. A randomized study of very low‐dose factor VIII prophylaxis in severe haemophilia – a success story from a resource limited country. Haemophilia. 2016;22(3):342–348. doi:10.1111/hae.12838
15. Wu R, KH Luke, Poon MC, et al. Low dose secondary prophylaxis reduces joint bleeding in severe and moderate haemophilic children: a pilot study in China. Haemophilia. 2011;17(1):70–74. doi:10.1111/j.1365-2516.2010.02348.x
16. Tang L, Wu R, Sun J, et al. Short‐term low‐dose secondary prophylaxis for severe/moderate haemophilia A children is beneficial to reduce bleed and improve daily activity, but there are obstacle in its execution: a multi‐centre pilot study in China. Haemophilia. 2013;19(1):27–34. doi:10.1111/j.1365-2516.2012.02926.x
17. Mathias M, Abraham A, Belletrutti MJ, et al. Simoctocog alfa (Nuwiq®) in previously untreated patients with severe haemophilia A—Final efficacy and safety results from the NuProtectstudy. Eur J Haematol. 2023;111(4):544–552. doi:10.1111/ejh.14040
18. Choraria N, Rangarajan S, John MJ, et al. Moroctocog Alfa (AF-CC) for prophylaxis and treatment of bleeding episodes in previously treated patients with hemophilia A in India. Indian J Hematol Blood Transfusion. 2023;39(4):624–629. doi:10.1007/s12288-022-01587-1
19. Wu R, Sun J, Xu W, et al. Safety and efficacy of Turoctocog Alfa in the prevention and treatment of bleeding episodes in previously treated patients from china with severe hemophilia A: results from the guardian 7 trial. Ther Clin Risk Manag. 2020;16:567–578. doi:10.2147/TCRM.S243146
20. Gringeri A, Lundin B, Von Mackensen S, Mantovani L, Mannucci PM. A randomized clinical trial of prophylaxis in children with hemophilia A (the ESPRIT Study). J Thromb Haemost. 2011;9(4):700–710. doi:10.1111/j.1538-7836.2011.04214.x
21. Powell J, Martinowitz U, Windyga J, et al. Efficacy and safety of prophylaxis with once-weekly BAY 79–4980 compared with thrice-weekly rFVIII-FS in haemophilia A patients. Thromb Haemost. 2012;108(11):913–922. doi:10.1160/TH12-03-0188
22. Manco-Johnson MJ, Kempton CL, Reding MT, et al. Randomized, controlled, parallel-group trial of routine prophylaxis vs. on-demand treatment with sucrose-formulated recombinant factor VIII in adults with severe hemophilia A (SPINART). J Thromb Haemost. 2013;11(6):1119–1127. doi:10.1111/jth.12202
23. Yang R, Sun J, Zhao Y, et al. Efficacy and safety of prophylaxis with BAY 81‐8973 in Chinese patients with severe haemophilia A enrolled in the LEOPOLD II trial. Haemophilia. 2019;25(3). doi:10.1111/hae.13751
24. Delgado-Flores CJ, García-Gomero D, Salvador-Salvador S, Montes-Alvis J, Herrera-Cunti C, Taype-Rondan A. Effects of replacement therapies with clotting factors in patients with hemophilia: a systematic review and meta-analysis. PLoS One. 2022;17(1):e0262273. doi:10.1371/journal.pone.0262273
25. World Federation of Hemophilia. Report on the Annual Global Survey 2021 Is Published by the World Federation of Hemophilia.; 2022.
26. Baker JR, Riske B, Voutsis M, Cutter S, Presley R. Insurance, home therapy, and prophylaxis in U.S. youth with severe hemophilia. Am J Prev Med. 2011;41(6 Suppl 4):S338–45. doi:10.1016/j.amepre.2011.09.002.
27. Jamal M, Sathar J, Jamari J, Mohd Saffian S. A comparison of the incidence rate for joint bleeding and FVIII consumption between on-demand versus prophylaxis factor VIII replacement therapy and the direct cost of prophylaxis treatment in severe haemophilia A patients. Malaysian J Med Sci. 2023;30(1):129–136. doi:10.21315/mjms2023.30.1.11
28. Dou X, Poon M, Yang R. Haemophilia care in China: achievements in the past decade. Haemophilia. 2020;26(5):759–767. doi:10.1111/hae.14101
29. Seth T, Garg K, Mandal PK, et al. Cost-effectiveness analysis of low-dose prophylaxis versus on-demand treatment for moderate-to-severe hemophilia A in India. Hematology. 2023;28(1). doi:10.1080/16078454.2023.2277497
30. Sachdeva A, Gunasekaran V, Ramya H, Dass J, Kotwal J, Seth T. Consensus statement of the Indian academy of pediatrics in diagnosis and management of hemophilia. Ind pediatrics. 2018;55(1):582–590.
31. Chen Y, Cheng SJ, Thornhill T, Solari P, Sullivan SD. Health care costs and resource use of managing hemophilia A: a targeted literature review. J Manag Care Spec Pharm. 2023;29(6):647–658. doi:10.18553/jmcp.2023.29.6.647
32. O’Hara J, Hughes D, Camp C, Burke T, Carroll L, Diego DAG. The cost of severe haemophilia in Europe: the CHESS study. Orphanet J Rare Dis. 2017;12(1):106. doi:10.1186/s13023-017-0660-y
33. Moonla C, Sosothikul D, Pongtanakul B, et al. Practices and challenges for hemophilia management under resource constraints in Thailand. Orphanet J Rare Dis. 2023;18(1):110. doi:10.1186/s13023-023-02718-1
34. Mai NT. Hemophilia Care in Vietnam -. Ministry of Health National Institute of Hematology and Blood Transfusion.; 2019.
35. Malaysian Health Technology Assessment Section (MaHTAS). MDDM of HM. Clinical Practice Guidelines Management of Hemophilia. Ministry Health Malaysia. 2018.
36. Hemophilia Society of Singapore. Hemophilia Society of Singapore, Annual Report 2023/2024. Available from: https://haemophilia.org.sg/resources/publications/.
37. Yang R, Zhao Y, Wang X, et al. Safety and efficacy of Moroctocog Alfa (AF-CC) in Chinese patients with hemophilia A: results of two open-label studies. J Blood Med. 2020;11:439–448. doi:10.2147/JBM.S241605
38. Zhao H, Yang L, Long C, et al. Hemophilia care in China: review of care for 417 hemophilia patients from 11 treatment centers in Shanxi Province. Expert Rev Hematol. 2015;8(4):543–550. doi:10.1586/17474086.2015.1043263
39. Chowdary P, Ofori-Asenso R, Nissen F, et al. Disease burden, clinical outcomes, and quality of life in people with hemophilia A without inhibitors in Europe: analyses from CHESS II/CHESS PAEDs. TH Open. 2024;08(02):e181–e193. doi:10.1055/s-0044-1785524
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Gene Therapy and Hemophilia: Where Do We Go from Here?
Bolous NS, Bhatt N, Bhakta N, Neufeld EJ, Davidoff AM, Reiss UM
Journal of Blood Medicine 2022, 13:559-580
Published Date: 6 October 2022
Effectiveness of Prophylactic Coagulation Factor Replacement Therapy in Patients with Severe Hemophilia A in Taiwan – A Population-Based Study
Hsieh MHC, Chiou SS, Liao TC, Lai SJ, Lai ECC
Clinical Epidemiology 2022, 14:1501-1510
Published Date: 13 December 2022
Risk of Intracranial Hemorrhage in Persons with Hemophilia A in the United States: Real-World Retrospective Cohort Study Using the ATHNdataset
Hu J, Chandler M, Manuel CM, Caicedo J, Denne M, Ewenstein B, Mokdad AG, Xing S, Recht M
Journal of Blood Medicine 2024, 15:191-205
Published Date: 24 April 2024