Back to Journals » Journal of Pain Research » Volume 15
Effects of Unilateral Intermediate Cervical Plexus Block on the Diaphragmatic Function in Patients Undergoing Unilateral Thyroidectomy: A Randomized Controlled Study
Authors Han C, Shao P, Li H ![]() , Shi R, Wang Y
, Shi R, Wang Y ![]()
Received 14 May 2022
Accepted for publication 30 August 2022
Published 7 September 2022 Volume 2022:15 Pages 2663—2672
DOI https://doi.org/10.2147/JPR.S374739
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Jinlei Li
Chao Han,1,2 Peiqi Shao,1 Huili Li,1 Rong Shi,1 Yun Wang1
1Department of Anesthesiology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Anesthesiology, Beijing Longfu Hospital, Beijing, People’s Republic of China
Correspondence: Yun Wang, Department of Anesthesiology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China, Email [email protected]
Background and Purpose: Although unilateral intermediate cervical plexus block (ICPB) can be used for perioperative analgesia in neck surgery, its effect on diaphragm function remains controversial. This prospective study aimed to examine whether unilateral ICPB with different concentrations of ropivacaine resulted in the diaphragmatic dysfunction in unilateral thyroidectomy.
Methods: A total of 54 patients scheduled to undergo unilateral thyroidectomy under general anesthesia were randomly allocated to receive either 10 mL of 0.3% (Group L) or 0.5% (Group H) ropivacaine for ICPB. General anesthesia was then administered for surgery. The diaphragm thickness and diaphragmatic excursion were measured at three different times: before the ICPB, at 40 min and 4 h after the block. The primary outcome was the incidence of diaphragmatic dysfunction of the block side at 40 min and 4 h after ICPB. Secondary outcomes included the maximum pain score within 24 h after the surgery, rescue analgesics within 24 h after the surgery, and time to first ambulation.
Results: The incidence of diaphragmatic dysfunction on the block side of Group H was higher than that of Group L at 40 min after block (58% vs 29%, P = 0.01). However, the incidence of diaphragmatic dysfunction was comparable between Group H and Group L (65% vs 46%) at 4 h after block placement. Within 24 h after the operation, the maximum VAS pain score of Group H was significantly lower than Group L (P = 0.04), and fewer patients in Group H required rescue analgesics (P < 0.01).
Conclusion: The ICPB with different concentrations of ropivacaine can induce the ipsilateral diaphragmatic dysfunction. The high concentration of ropivacaine results in higher incidence of diaphragmatic dysfunction at 40 min, but comparable incidence at 4 h after block compared with lower concentration of ropivacaine.
Chinese Clinical Trial Registry: ChiCTR2000029348.
Keywords: intermediate cervical plexus block, regional block, diaphragmatic dysfunction, ultrasound
Introduction
The intermediate cervical plexus is the area where the deep cervical plexus penetrates the prevertebral fascia and branches deep to the sternocleidomastoid muscle to migrate to the superficial cervical plexus.1 Intermediate cervical plexus block (ICPB) was named by Telford and Stoneham in 2004.2 Ultrasound-guided ICPB targets the space between the investing fascia and prevertebral fascia at the C4 level. Local anesthetics (LAs) injected in this space can block the superficial cervical plexus which includes the great auricular nerve (GAN), the lesser occipital nerve (LON), the transverse cervical nerve (TCN), and the supraclavicular nerve (SCN).3 The ultrasound-guided ICPB can reduce intra- and postoperative pain in patients undergoing thyroidectomy.4
The phrenic nerve is on the surface of the anterior scalene muscle and beneath the prevertebral fascia and the phrenic nerve block could result in diaphragmatic dysfunction. Nevertheless, it is still controversial whether LAs can penetrate the prevertebral fascia and then block the phrenic nerve following the ICPB. These conflicting results were derived from cadaveric dissection.5,6 Previous clinical studies have used the presence of Horner syndrome, dyspnea and atelectasis to predict whether LAs could penetrate the prevertebral fascia after ICPB; however, these methods had drawbacks such as low sensitivity and thus the result is unreliable.7–9 At present, the diaphragm ultrasound has been used to identify the changes in diaphragm function after ICPB.10,11 It is noteworthy that the concentration of LAs used and the diagnostic criteria for diaphragmatic dysfunction were different among different studies on the effect of ICPB on diaphragm function, leading to conflicting conclusions. In this study, two different concentrations of ropivacaine were used for ultrasound-guided ICPB, diaphragm ultrasound was used to assess the diaphragmatic excursions and diaphragm thickness, and a more comprehensive diagnostic criteria for diaphragmatic dysfunction was used to evaluate whether the phrenic nerve was affected.12 We hypothesized that the lower concentration of ropivacaine may decrease the incidence of diaphragmatic dysfunction. The primary outcome was the incidence of diaphragmatic dysfunction at 40 min and 4 h after the block. The results of the current study will provide a theoretical foundation for the clinical safety of ICPB.
Methods
Ethics
Ethical approval for this study (Ethics approval number: 2019-K-370) was provided by the Ethical Committee of Beijing Chaoyang Hospital affiliated to Capital Medical University (Chairperson Prof. Yong Chen) on 6 January 2020. It was registered as a clinical trial on the Chinese Clinical Trial Registry (http://www.chictr.org.cn/edit.aspx?pid=48648&htm=4) with the registration number of ChiCTR2000029348 on 25 January, 2020. Written informed consent was obtained from all participants. The study was conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT) statement and Helsinki declaration.
Subjects
Fifty-four patients who underwent unilateral thyroidectomy were enrolled between February 17, 2020, and March 31, 2021 at Beijing Chaoyang Hospital (Figure 1). The study included patients aged 18–75 years with ASA I-III status. Exclusion criteria included diaphragmatic dysfunction showed by diaphragm ultrasound before the block, severe respiratory diseases, severe cardiovascular and cerebrovascular diseases, including heart failure, COPD (chronic obstructive pulmonary diseases), asthma, pulmonary heart disease and hemiplegia after stroke. Patients who had a fever before the surgical day (≥37.3°C) were not enrolled. Patients with Alzheimer’s disease history, mental diseases, long-term use of psychotropic drugs were also excluded. Electronic laryngoscope was used to evaluate the activity of the vocal cords. Patients with vocal cords diseases and Horner syndrome were excluded.
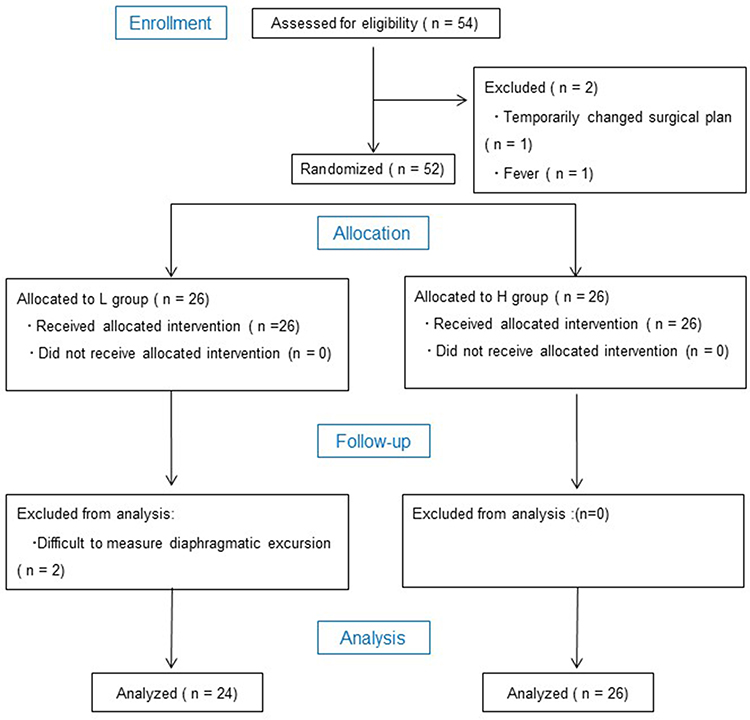 |
Figure 1 Consort flow chart showing patient progress. |
Study Intervention
Participating subjects were randomized on the day of surgery to either the 0.3% ropivacaine group (Group L) or the 0.5% ropivacaine group (Group H), using a computer-generated randomization table. Assignments were concealed in a sealed opaque envelope. A research assistant who did not play any other role in the study prepared one 10-mL syringe according to appropriate specifications. Each syringe had 10 mL of 0.5% or 0.3% ropivacaine tagged with the randomization number of the patient. The anesthesiologists, patients, and follow-up staff nurses were all blinded to the concentrations of ropivacaine.
Diaphragmatic Ultrasound, Block Procedure and Anesthesia Management
Intravenous access was established as soon as the patient arrived in the operating room, and electrocardiogram, noninvasive blood pressure as well as pulse oximeter were routinely monitored. Pulse oxygen saturation was all recorded without oxygen inhalation. The first diaphragm ultrasound was performed before the ICPB, and the bilateral diaphragm thickness, diaphragm thickening fraction (DTF) and diaphragmatic excursions during quiet and deep breathing were recorded. The skilled anesthesiologists (CH, PS, and HL) performed all ultrasonographic examinations and everyone had the experience of diaphragm ultrasound examination in more than 50 patients.
The patient was kept in the supine position. Diaphragm thickness and DTF were measured with a high-resolution linear array probe (5~12 MHz, Navi, Wisonic, Shenzhen, China). The probe was placed at the midaxillary line at the level of the seventh and eighth intercostal space, with the marking point of the probe towards cephalad. The probe should be perpendicular to the zone of apposition of the diaphragm. Diaphragm which appeared as hypoechoic structure between two hyperechoic lines could be found in B-mode (Figure 2A). The diaphragm thickness can be measured as the distance between pleura and peritoneum at the end of maximal inspiration and maximal expiration. The measurement was repeated three times and the average value was taken. DTF was calculated using the following formula: (thickness at end-inspiration − thickness at end-expiration)/thickness at end-expiration.12,13
 |
Figure 2 Diaphragmatic ultrasound and intermediate cervical plexus block. (A), Ultrasound measurement of the diaphragm thickness. The schematic diagram in the upper left corner illustrates the position of the transducer. Using a linear probe, the diaphragm is seen between two hyperechoic lines at the level of the seventh and eighth intercostal spaces and midaxillary line. The superficial line refers to the pleura, and the deeper one corresponds to the peritoneum. (B), Ultrasonography of the intermediate cervical plexus block. The puncture needle is advanced with the posterior-anterior direction into the interfascial space between the investing fascia and the prevertebral fascia at the C4 level. (C), The right diaphragmatic movement during deep breathing was scanned through the liver window in B-mode. The probe was placed at the subcostal area in the anterior axillary line as shown in the image in the upper left corner. (d), The left diaphragm movement during quiet breathing was measured through the splenic window in B-mode. The probe position illustrated in the diagram in the upper left corner is the same as on the right. (E) The right diaphragmatic excursion was measured in M-mode during deep breathing. (F), The left diaphragmatic excursion was measured in M-mode during quiet breathing. Abbreviations: CA, carotid artery; SCM, sternocleidomastoid muscle; TP, transverse process. R, right; L, left. |
The patients’ position remained unchanged and the diaphragmatic excursions were assessed by M-mode ultrasonography. The convex array probe (2–5 MHz) was placed at the subcostal area in the anterior axillary line, below the bilateral costal margin of the eighth and ninth ribs. The probe was directed medially, cephalad and dorsally to make the ultrasound beam reach the posterior third of diaphragm perpendicularly. The probe then scanned along the long axis of the intercostal spaces, using the liver as the acoustic window on the right side and the spleen as the acoustic window on the left side (Figure 2C and D). The M-mode sampling line was positioned perpendicularly to the diaphragm and the diaphragmatic excursions could be measured during quiet and deep breathing. The perpendicular distance between the most caudal point of this line during inspiration and the most cephalic point during expiration represents the diaphragmatic excursion (Figure 2E and F).12,13 Each measurement was repeated three times and the average value was calculated.
Both groups received ultrasound-guided ICPB with different concentrations of ropivacaine. The skilled anesthesiologists (CH, PS, HL) performed the blocks to ensure the correct position of needle tip and every anesthesiologist had the experience of successfully performing the ICPBs in more than 50 cases. With the patient’s head slightly rotating to the opposite side in the supine position, the linear array probe was placed on the lower neck for cross-sectional scanning to identify the C7 transverse process. Then, the probe slid cranially to position the C4 transverse process. The needle (22 gauge, 50-mm needle, B.Braun, Melsungen, Germany) was inserted in a postero-anterior direction using an in-plane technique, and 10 mL of 0.3% or 0.5% ropivacaine (Astra Zeneca, London, UK) was injected into the interfascial space between the investing fascia and the prevertebral fascia at the C4 level and just deep to the sternocleidomastoid muscle (Figure 2B). Cold sensation in the distribution of the superficial cervical plexus was assessed to determine the effect of ICPB at 40 min after the block. Sensory blockade was assessed in distributions innervated by LON (post-auricular), GAN (ear lobe), TCN (mid-level of the neck), SCN (clavicle) with the ice. The block was successful when the cold sensation in the area innervated by the four superficial branches decreased or disappeared. At 40 min after ICPB, the bilateral DTF and diaphragmatic excursions were assessed by ultrasound. The pulse oxygen saturation without oxygen inhalation, the incidence of hoarseness and Horner syndrome were also recorded.
All patients then received standard general anesthesia (GA) for surgery. GA was induced with 0.02 mg/kg midazolam (Nhwa Pharma, Jiangsu, China), 0.3–0.4 μg/kg sufentanil (Yichang Renfu Pharma, Yichang, China) and 1.5–2.0 mg/kg propofol (Fresenius Kabi AB, Uppsala, Sweden). Intubation was facilitated by 0.8 mg/kg rocuronium (Xianju Pharma, Xianju, China). A neural integrity monitoring (NIM) endotracheal tube (Medtronic, Minneapolis, Minnesota, USA) was used for intraoperative recurrent laryngeal nerve (RLN) monitoring. Anesthesia was maintained with 4–12 mg/kg/h propofol (Fresenius Kabi AB, Uppsala, Sweden) and 0.1–0.6μg/kg/min remifentanil (Yichang Renfu Pharma, Yichang, China). No additional muscle relaxant was administered after anesthesia induction. Train of four stimulation (TOF) was used to monitor muscle relaxant effect. The depth of anesthesia was adjusted according to the hemodynamic response and bispectral index (BIS). No muscle relaxant antagonists were used during the surgery, and the endotracheal tube was removed after T4/T1≥0.9 under TOF monitoring.
Postoperative Diaphragmatic Ultrasound, Pain Management and Assessment of Outcomes
All patients returned to the ward after the surgery. The bilateral DTF and diaphragmatic excursions were assessed at 4 h after ICPB. To exclude drug effects of GA technique on postoperative diaphragm function, the diaphragmatic motion of contralateral side was measured. The pulse oxygen saturation without oxygen inhalation were recorded at the same time. A 10 cm visual analogue scale (VAS) was used to measure subjective pain intensity rated from 0 (no pain) to 10 (worst pain). For patients with a VAS pain score of ≥4, intravenous flurbiprofen (50 mg; Beijing Taide Pharma, Beijing, China) was administered as rescue analgesics. The maximum VAS score, the number of patients requiring rescue analgesics within 24 h after the surgery, and the time to first ambulation after surgery were followed up.
The primary outcome was the incidence of diaphragmatic dysfunction of the block side at 40 min and 4 h after ICPB. According to the diagnostic criteria, DTF <20%, diaphragmatic tidal excursion <9 mm in females, diaphragmatic tidal excursion <10 mm in males, diaphragmatic excursion during deep breathing <37 mm in females, diaphragmatic excursion during deep breathing <47 mm in males were abnormal.12 Meeting any of the diagnostic criteria was defined as diaphragmatic dysfunction.14,15
The amount of intraoperative general anesthetics, complications related to the ICPB, oxygen saturation at 40 min and 4 h after the block without oxygen inhalation, the maximum VAS score within 24 h after the surgery, rescue analgesics within 24 h after the surgery, and time to first ambulation were all analyzed as the secondary outcomes.
Sample Size and Statistical Analysis
The sample size was calculated according to the data of a pilot study. The primary outcome was the incidence of diaphragmatic dysfunction, which was 30% in group L, and 60% in group H in the preliminary study at 40 min after ICPB. Hence, a total sample size of 42 (21 in each group) was sufficient to detect a power of 90% and a significance level of 5%. By taking into account patients lost to follow-up, the sample size was further increased to 54 patients.
SPSS 23.0 (IBM Corp, Armonk, New York, USA) was used for statistical analysis. Continuous variables with normal distribution are presented as means and standard deviations, and non-normal variables are reported as median (interquartile range), and categorical data are labeled as number and frequency. Statistical significance of differences between two groups with respect to categorical variables were analyzed with χ2 test. Continuous normally distributed variables were analyzed by analysis of variance (ANOVA), non-normally distributed continuous variables by the Mann–Whitney U-test. P < 0.05 were considered statistically significant.
Results
Fifty-four patients were included in this study, and four patients were excluded in the study. One case was excluded due to the surgical plan change. One case was excluded due to the fever which was found on the morning of surgical day. Two cases had difficulty measuring left diaphragmatic excursions. Our study included the remaining 50 cases, including 24 cases in group L and 26 cases in group H. Baseline characteristic and intraoperative details were not significantly different between the two groups (Table 1). No abnormalities of diaphragm function were noted before ICPB. At 40 min after the ICPB, all patients reported that cold sensation in the intermediate cervical plexus cutaneous innervation area decreased or disappeared.
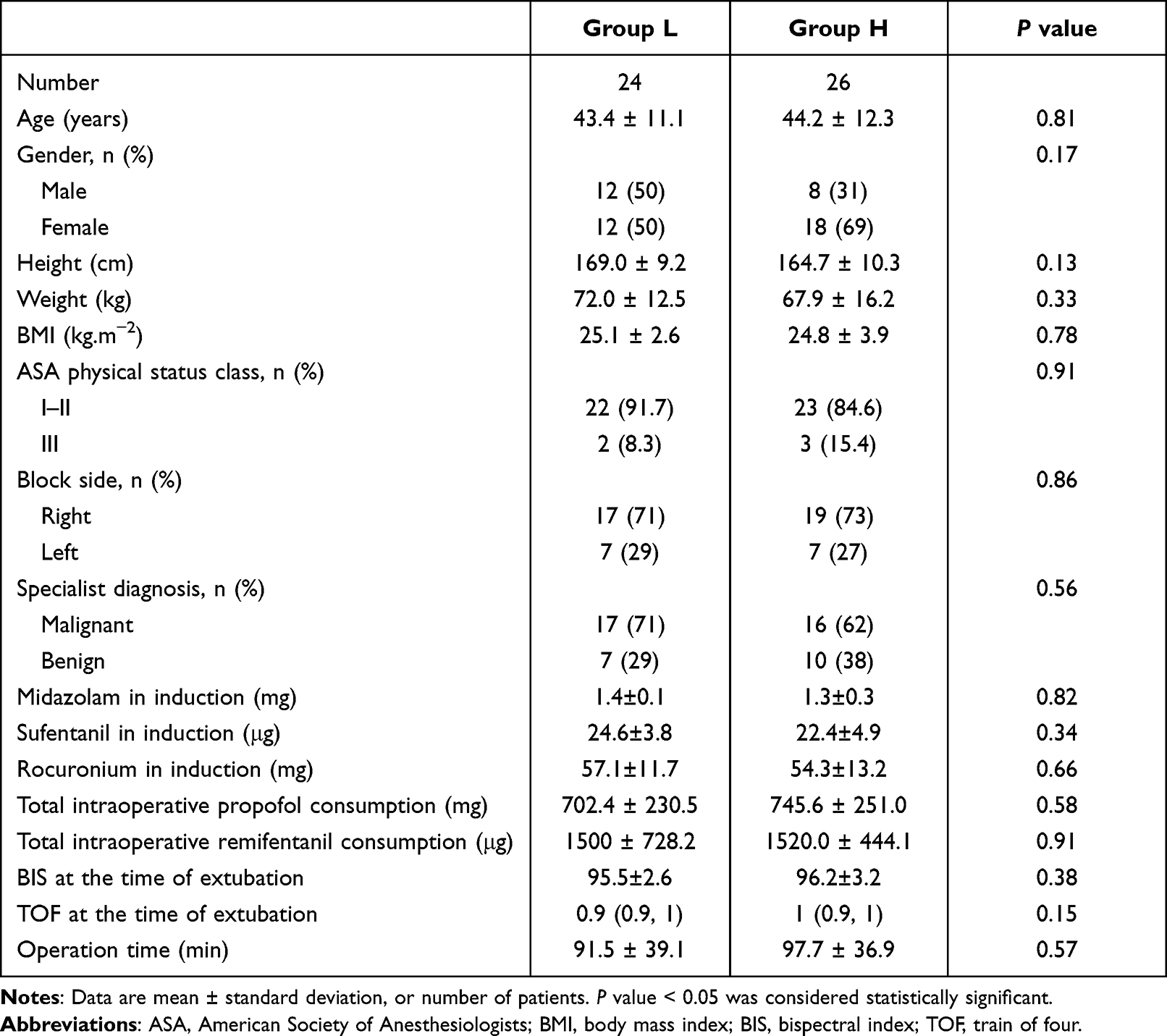 |
Table 1 Demographic Data and Intraoperative Details |
Primary Outcome Measurements
The incidence of diaphragmatic dysfunction was compared between the two groups at 40 min and 4 h after ICPB, respectively. Group H had a higher incidence of diaphragmatic dysfunction than group L at 40 min after the block (58% vs 29%, P = 0.04). At 4 h after ICPB, the incidence of diaphragmatic dysfunction in group H was comparable to that in group L (65% vs 46%, P = 0.13) (Table 2). In the subgroup analysis, it was found that at 40 min after the block, the incidence of abnormal diaphragmatic excursion during deep breathing was higher in the group H than in the L group (54% vs 21%, P = 0.02). At 4 h after ICPB, the incidence of abnormal DTF in group H was higher than that in group L (46% vs 13%, P = 0.04) (Table 2).
 |
Table 2 Incidence of Diaphragmatic Dysfunction of Group H and L After ICPB |
Three evaluation indices (DTF, diaphragmatic tidal excursion, diaphragmatic excursion during deep breathing) were employed to evaluate the bilateral diaphragmatic dysfunction. For the ipsilateral ultrasound examinations, the three indices of group L and group H decreased significantly at 40 min or 4h after block, compared with those before block (P < 0.05) (Figure 3). For the contralateral ultrasound examinations, there were no significant differences in the three indices in Group L and Group H at 40 min or 4 h after block, in comparison to those before block (P > 0.05) (Figure 4).
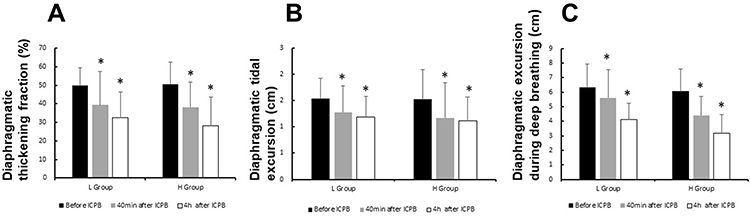 |
Figure 3 Comparisons of diaphragm function indices on the block side at different timepoints. The diaphragm thickening fraction (A), diaphragmatic tidal excursion (B) and diaphragmatic excursion during deep breathing (C) of group L and group H decreased significantly at 40 min or 4h after block, compared with those before block (P <0.05). *P <0.05, compared with the baseline before block. |
 |
Figure 4 Comparisons of diaphragmatic function indices on the contralateral side at different time-points. The diaphragm thickening fraction (A), diaphragmatic tidal excursion (B) and diaphragmatic excursion during deep breathing (C) at 40 min or 4 h after block in Group L and Group H had no difference with those before block (P > 0.05). |
Secondary Outcome Measurements
There was no significant difference in the incidence of Horner syndrome and hoarseness between the two groups at 40 minutes after ICPB (P > 0.05). The pulse oxygen saturation was in the normal range in both groups at 40 min and 4 h after the block, with no significant difference between the two groups (P > 0.05). The maximum VAS score within 24 hours after the surgery in group H was significantly lower than that in group L (P = 0.04). There was no difference in the time to the first ambulation between two groups (P > 0.05). Fewer patients in group H required rescue analgesics within 24 h after block placement compared with group L (P = 0.01). Rescue analgesics was required when VAS ≥ 4. (Table 3).
 |
Table 3 Secondary Outcome Parameters |
Discussion
This is a prospective, randomized, controlled study. Different concentrations of ropivacaine could induce significant diaphragmatic dysfunctions on the block side at 40 min and 4 h after unilateral ICPB, while the contralateral side was unaffected. Additionally, the high concentration of ropivacaine results in higher incidence of diaphragmatic dysfunction at 40 min, but comparable incidence at 4 h after block compared with lower concentration of ropivacaine.
Diaphragmatic ultrasonography as a new non-invasively tool for diagnosis of diaphragmatic paralysis or dysfunction has been recommended in guidelines.15,16 In this study, we assessed comprehensively the DTF, diaphragmatic tidal excursion and diaphragmatic excursion during deep breathing to define diaphragmatic dysfunction. Our results showed that ICPB could result in diaphragmatic dysfunction.14 However, Kim et al and Opperer et al argued that ICPB did not lead to diaphragmatic dysfunction in their studies.10,11 The contradictory results between these studies may be caused by the different diagnostic criteria of diaphragmatic dysfunction. Both Kim HY and Opperer M defined diaphragmatic dysfunction depending on the difference of diaphragm movement compared with baseline level. Nevertheless, we diagnosed diaphragmatic dysfunction based on the abnormal value of each indicator and used more comprehensive indicators representing diaphragmatic function, which can increase the diagnostic sensitivity.17 According to our criteria, substantial patients in both groups were diagnosed with diaphragmatic dysfunction with at least one impaired diaphragm function. DTF is a little-noticed indicator in previous literatures. However, at 4h after the block in our study, the incidence of abnormal DTF in group H was significantly higher than that in group L. This may explain the reason of high incidence of diaphragmatic dysfunction in our study.
Diaphragmatic dysfunction after ICPB is due to LAs penetrating the prevertebral fascia and then blocking the phrenic nerve. The permeability of prevertebral fascia to LAs is still controversial. In this study, at 40 min after the block, the incidence of diaphragmatic dysfunction in group H was higher than that in group L, especially for the abnormal diaphragmatic movement during deep breathing, indicating that 0.5% ropivacaine could penetrate the prevertebral fascia more quickly. At 4h after block, there was no significant difference in the incidence of diaphragm dysfunction between the two groups, illustrating that low concentration of ropivacaine can slowly penetrate the prevertebral fascia, but there was still a significant difference in the incidence of DTF between the two groups. These phenomena confirmed that LAs could penetrate the prevertebral fascia and variable different concentrations of ropivacaine had different effects on diaphragmatic function. Several studies using 0.5% or higher concentrations of ropivacaine also suggest that the prevertebral fascia can be permeated.8,9,18–20 There are also clinical studies suggesting that the prevertebral fascia is impermeable, and these studies have lower concentrations of LAs.4,7,21,22
So far, there was no study involving long-term observation of diaphragmatic excursion more than 1h after ICPB. In this study, the observation time of diaphragm movement was extended to 4h after ICPB, which also explained the higher incidence of diaphragmatic dysfunction in our study. All indicators of diaphragmatic function on the block side decreased significantly and tended to worsen with time extension. The patient could fully comply with the diaphragmatic function and pain score examination at 4h after the surgery. In the current study, the contralateral diaphragmatic function was not significantly influenced compared with the baseline. In current study, patients with unilateral diaphragmatic dysfunction did not experience dyspnea or a severe decrease in blood oxygen saturation, possibly because of the compensation of auxiliary muscles involved in respiratory movement, suggesting that unilateral ICPB with 10 mL of ropivacaine at 0.5% or lower concentration is safe. LAs was not injected directly around the phrenic nerve in ICPB, causing only mild to moderate phrenic palsy, and no contralateral diaphragmatic compensatory effect was observed. Considering the high incidence of unilateral diaphragmatic dysfunction in this study, bilateral ICPB should be treated with caution and should be performed under close monitoring in elderly patients or patients with poor lung function.
A small number of patients in each group developed Horner syndrome at 40 min after the block. In this study, the incidence of Horner syndrome was assessed at 40 min after the block, considering that the sympathetic trunk block usually lasted a short time and resolved within 90 min.23 The sign of Horner syndrome might be missed if complications were evaluated at 4 hours after the block. Horner syndrome is a complication caused by blockade of the sympathetic chain. The sympathetic chain was located beneath the prevertebral fascia and on the surface of the longus colli muscle, the occurrence of Horner syndrome after the ICPB indicated that the prevertebral fascia is permeable to LAs in some studies.8,18,24 However, Horner syndrome was not observed in some other studies, which might be related to the use of lower concentrations of LAs.4,10,21,25,26 Furthermore, the sympathetic chain was located on the surface of the longus colli muscle, a bit far from the LAs injection points. It was difficult to produce a sustained blocking effect if there were no enough volume of LAs penetrating the prevertebral fascia.23 The lesser volume of LAs using in this study might explain that while the incidence of diaphragmatic dysfunction increased in the group H, there was no corresponding increase in complications. In this study, it was found that a small number of patients in both groups complained about hoarseness after 40 minutes of the block. Some studies also reported the occurrence of hoarseness in ICPB.8,18,19,24 They found that when the volume of LAs exceeded 10 mL or the LAs was in a higher concentration in ICPB, the drug would diffuse and deposit around the carotid sheath, resulting in the block of RLN, superior laryngeal nerve and vagus nerve. The incidence of hoarseness was assessed at 40 minutes after the block (before surgery) in this study. In order to prepare for intraoperative RLN monitoring, it is necessary to rule out hoarseness caused by ICPB before surgery. Additionally, at 4 h after ICPB, the patient underwent surgery and GA with endotracheal intubation, which could result in hoarseness due to vocal cord edema and RLN injury, potentially increasing the incidence of hoarseness. The surgical manipulation of the unilateral thyroidectomy would not affect the spread of LAs too, since the LAs deposit area was far away from the surgical area.
There was no significant difference in the amount of propofol and remifentanil during GA between the two groups, and the effect of GA on the diaphragmatic motion of both groups was similar. In this study, the patients in group H did not require rescue analgesics within 24 h after the block, and they had better postoperative analgesia than those in Group L. Although the proportion of patients in group H ambulating earlier after surgery was higher than that in group L, there was no statistical significance. Kim et al used a lower concentration of 0.25% ropivacaine in studies of ICPB, they observed the postoperative analgesia effect completely subsided at only 3 h after the surgery.25,26 and there was no difference in the amount of rescue analgesics between the ICPB and control group.25
The present study is subject to several limitations. First, patients with respiratory diseases were excluded from this study. Although the data showed that unilateral ICPB is safe in normal patients, it would be inappropriate to extend the result to patients with respiratory diseases. Second, we used a compound outcome to assess diaphragmatic dysfunction in this study, which has a high sensitivity to detect diaphragmatic dysfunction due to monitoring of three indicators representing different functions of the diaphragm. However, the blood oxygen saturation of patients with diaphragmatic dysfunction did not significantly decrease, and we did not observe the effect of diaphragmatic dysfunction on other respiratory indicators such as partial pressure of carbon dioxide. Third, the relatively small sample size may limit the ability to identify rare adverse events.
Conclusions
Different concentrations of LAs for ICPB can induce the diaphragmatic dysfunctions on the block side, while the contralateral side is unaffected. Additionally, the high concentration of ropivacaine results in higher incidence of diaphragmatic dysfunction at 40 min, but comparable incidence at 4 h after block compared with lower concentration of ropivacaine. Additionally, unilateral ICPB does not seem to reduce oxygen saturation in the setting of no oxygen inhalation.
Data Sharing Statement
We all agree to share all the data about this article. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Armbruster W, Eichholz R, Notheisen T. Sonoanatomy of the “Cervical Nerves Pathway”. Recommendations for ultrasound-guided regional anaesthesia for carotid endarterectomy. Ultraschall Med. 2013;34(S 01):S 01. doi:10.1055/s-0033-1355096
2. Telford RJ, Stoneham MD. Correct nomenclature of superficial cervical plexus blocks. Br J Anaesth. 2004;92(5):775. doi:10.1093/bja/aeh550
3. Choquet O, Dadure C, Capdevila X. Ultrasound-guided deep or intermediate cervical plexus block: the target should be the posterior cervical space. Anesth Analg. 2010;111(6):1563–1564. doi:10.1213/ANE.0b013e3181f1d48f
4. Senapathi TGA, Widnyana IMG, Aribawa IGNM, et al. Ultrasound-guided bilateral superficial cervical plexus block is more effective than landmark technique for reducing pain from thyroidectomy. J Pain Res. 2017;10:1619–1622. doi:10.2147/JPR.S138222
5. Pandit JJ, Dutta D, Morris JF. Spread of injectate with superficial cervical plexus block in humans: an anatomical study. Br J Anaesth. 2003;91(5):733–735. doi:10.1093/bja/aeg250
6. Seidel R, Schulze M, Zukowski K, Wree A. Ultrasound-guided intermediate cervical plexus block. Anatomical study. Der Anaesthesist. 2015;64(6):446–450. doi:10.1007/s00101-015-0018-6
7. Colegrave N, Mascitti P, Zannis K, et al. Ultrasound-guided intermediate cervical plexus block for transcarotid transcatheter aortic valve replacement. J Cardiothorac Vasc Anesth. 2021;35(6):1747–1750. doi:10.1053/j.jvca.2020.08.053
8. Leblanc I, Chterev V, Rekik M, et al. Safety and efficiency of ultrasound-guided intermediate cervical plexus block for carotid surgery. Anaesth Crit Care Pain Med. 2016;35(2):109–114. doi:10.1016/j.accpm.2015.08.004
9. Merdad M, Crawford M, Gordon K, Papsin B. Unexplained fever after bilateral superficial cervical block in children undergoing cochlear implantation: an observational study. Can J Anaesth. 2012;59(1):28–33. doi:10.1007/s12630-011-9607-2
10. Kim HY, Soh EY, Lee J, et al. Incidence of hemi-diaphragmatic paresis after ultrasound-guided intermediate cervical plexus block: a prospective observational study. J Anesth. 2020;34(4):483–490. doi:10.1007/s00540-020-02770-2
11. Opperer M, Kaufmann R, Meissnitzer M, et al. Depth of cervical plexus block and phrenic nerve blockade: a randomized trial. Reg Anesth Pain Med. 2022;47(4):205–211. doi:10.1136/rapm-2021-102851
12. Sferrazza Papa GF, Pellegrino GM, Di Marco F, et al. A review of the ultrasound assessment of diaphragmatic function in clinical practice. Respiration. 2016;91(5):403–411. doi:10.1159/000446518
13. Matamis D, Soilemezi E, Tsagourias M, et al. Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med. 2013;39(5):801–810. doi:10.1007/s00134-013-2823-1
14. Vetrugno L, Guadagnin GM, Barbariol F, Langiano N, Zangrillo A, Bove T. Ultrasound imaging for diaphragm dysfunction: a narrative literature review. J Cardiothorac Vasc Anesth. 2019;33(9):2525–2536. doi:10.1053/j.jvca.2019.01.003
15. Boussuges A, Brégeon F, Blanc P, Gil J-M, Poirette L. Characteristics of the paralysed diaphragm studied by M-mode ultrasonography. Clin Physiol Funct Imaging. 2019;39(2):143–149. doi:10.1111/cpf.12549
16. Robba C, Wong A, Poole D, et al. Basic ultrasound head-to-toe skills for intensivists in the general and neuro intensive care unit population: consensus and expert recommendations of the European Society of Intensive Care Medicine. Intensive Care Med. 2021;47(12):1347–1367. doi:10.1007/s00134-021-06486-z
17. Kang RA, Chung YH, Ko JS, Yang MK, Choi DH. Reduced hemidiaphragmatic paresis with a “Corner Pocket” technique for supraclavicular brachial plexus block: single-center, observer-blinded, randomized controlled trial. Reg Anesth Pain Med. 2018;43(7):720–724. doi:10.1097/AAP.0000000000000795
18. Martusevicius R, Swiatek F, Joergensen LG, Nielsen HB. Ultrasound-guided locoregional anaesthesia for carotid endarterectomy: a prospective observational study. Eur J Vasc Endovasc Surg. 2012;44(1):27–30. doi:10.1016/j.ejvs.2012.04.008
19. Koköfer A, Nawratil J, Felder TK, Stundner O, Mader N, Gerner P. Ropivacaine 0.375% vs. 0.75% with prilocaine for intermediate cervical plexus block for carotid endarterectomy: a randomised trial. Eur J Anaesthesiol. 2015;32(11):781–789. doi:10.1097/EJA.0000000000000243
20. Pandit JJ, Satya-Krishna R, Gration P. Superficial or deep cervical plexus block for carotid endarterectomy: a systematic review of complications. Br J Anaesth. 2007;99(2):159–169. doi:10.1093/bja/aem160
21. Tran DQH, Dugani S, Finlayson RJ. A randomized comparison between ultrasound-guided and landmark-based superficial cervical plexus block. Reg Anesth Pain Med. 2010;35(6):539–543. doi:10.1097/AAP.0b013e3181faa11c
22. Bhoi D, Bhatia R, Mohan VK, Thakar A, Kalagara R, Sikka K. Efficacy of ultrasound-guided intermediate cervical plexus block by anterior route for perioperative analgesia in robotic thyroidectomy by retroauricular approach: a case series. AA Pract. 2021;15(8):e01501. doi:10.1213/XAA.0000000000001501
23. Flores S, Riguzzi C, Herring AA, Nagdev A. Horner’s syndrome after superficial cervical plexus block. West J Emerg Med. 2015;16(3):428–431. doi:10.5811/westjem.2015.2.25336
24. Calderon AL, Zetlaoui P, Benatir F, et al. Ultrasound-guided intermediate cervical plexus block for carotid endarterectomy using a new anterior approach: a two-centre prospective observational study. Anaesthesia. 2015;70(4):445–451. doi:10.1111/anae.12960
25. Kim J-S, Joe HB, Park MC, Ahn H, Lee SY, Chae YJ. Postoperative analgesic effect of ultrasound-guided intermediate cervical plexus block on unipolar sternocleidomastoid release with myectomy in pediatric patients with congenital muscular torticollis: a prospective, randomized controlled trial. Reg Anesth Pain Med. 2018;43(6):634–640. doi:10.1097/AAP.0000000000000797
26. Kim J-S, Lee J, Soh E-Y, et al. Analgesic effects of ultrasound-guided serratus-intercostal plane block and ultrasound-guided intermediate cervical plexus block after single-incision transaxillary robotic thyroidectomy: a prospective, randomized, controlled trial. Reg Anesth Pain Med. 2016;41(5):584–588. doi:10.1097/AAP.0000000000000430
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.