Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Effects of Ultra-Long-Acting Insulin Compared to Long-Acting Insulin on Diabetic Ketoacidosis Incidence in Type 1 Diabetes Mellitus Patients
Authors Alsofiani WA ![]() , Alessa BH, Alsabaan F, Althemery AU
, Alessa BH, Alsabaan F, Althemery AU ![]() , Ghith AM, Alfaifi AA
, Ghith AM, Alfaifi AA ![]()
Received 15 December 2021
Accepted for publication 16 February 2022
Published 5 March 2022 Volume 2022:15 Pages 733—739
DOI https://doi.org/10.2147/DMSO.S351155
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Wafa A Alsofiani,1 Bandar H Alessa,2 Fahad Alsabaan,3 Abdullah U Althemery,4 Aliah M Ghith,3 Abdullah A Alfaifi4
1Family Medicine and Diabetes Center, Prince Mansour Hospital, Taif, Saudi Arabia; 2Family Medicine Department, National Guard Hospital, Jeddah, Saudi Arabia; 3Endocrinology and Diabetes Department, Security Forces Hospital, Riyadh, Saudi Arabia; 4Department of Clinical Pharmacy, Prince Sattam bin Abdulaziz University, Al-Kharj, Saudi Arabia
Correspondence: Abdullah A Alfaifi, Clinical Pharmacy Department, Prince Sattam Bin Abdulaziz University, P.O. Box 173, Al-Kharj, Riyadh, 11942, Kingdom Of Saudi Arabia, Tel +966 11 588 6058, Fax + 966 11 588 8888, Email [email protected]
Purpose: This research was intended to explore the effects of new-generation basal insulin (degludec U100 And glargine U300) versus long-acting basal insulin (glargine U100, detemir) on the incidence of diabetic ketoacidosis episodes and diabetes treatment measures.
Patients and methods: This is a cross-sectional, retrospective medical record analysis. The study population included adults with type 1 diabetes mellitus (DM) who were on the hospital records in 2020. Data were collected from 221 eligible participants through review of electronic medical records. Each record was scanned for basal insulin type, total daily insulin dose, diabetic ketoacidosis (DKA) occurrences, and glycated hemoglobin A1C (HbA1c) levels. Data were collected from 6 months before to 6 months after the initiation of ultra-long-acting insulin. Statistical analysis was conducted using R version 3.5.2. The normality of distribution for each independent variable was verified using Shapiro–Wilk tests. The independent paired t-test was used to compare insulin therapy measures between the two insulin regimens. The main outcome measures were the incidence of DKA episodes and clinical outcomes associated with diabetes.
Results: The HbA1c did not change significantly before and after ultra-long-acting insulin therapy was initiated (9.9 vs 9.8, respectively; P > 0.05). Insulin total daily doses were significantly higher after shifting to ultra-long-acting insulin. Sub-analysis showed higher total daily insulin doses in glargine U300 users compared with degludec U100 users (P =0.0021). However, basal insulin doses did not change after treatment with ultra-long-acting insulin. No statistically significant difference in DKA occurrences was found before and after the start of ultra-long-acting insulin treatment.
Conclusion: The frequency of DKA episodes was not affected by changing the treatment to ultra-long-acting insulin. Moreover, the results suggest that insulin dosage and types are not the only cause of uncontrolled diabetes. Additional efforts should be made to cover all factors affecting diabetes complication control.
Keywords: diabetic ketoacidosis, insulin therapy, diabetic outcomes, long-acting therapy
Introduction
Diabetes mellitus (DM) is a disease characterized by high levels of blood glucose that occurs due to a deficiency in insulin action, production, or both. Type 1 DM usually occurs due to the damage of insulin‐producing ß‐cells in the pancreatic islets leading to insulin deficiency. The destruction of ß‐cells in the pancreatic islets could be attributed to immune mediated effects or idiopathic causes.1 Type 1 DM patients need life‐long insulin for survival. In addition to glycemic control, self-management and education can aid in averting or decreasing acute as well as chronic complications of diabetes.2
Diabetic ketoacidosis (DKA) is a common, life-threatening but preventable acute complication of type 1 diabetes.3 A total or relative insulin insufficiency and an upsurge in hormones such as glucagon, catecholamines, cortisol, and growth hormone may increase the chances of DKA.4 Globally, the currently reported morbidity and mortality associated with DKA is low compared to that in the past due to development of medical services and advancements is the treatment methods. Nevertheless, an increase in admissions due to DKA has been reported over the years.5
A common factor for reducing DKA occurrence is adherence to insulin regimen.6 Moreover, long-acting insulin plays a significant role in preventing DKA because of its pharmacokinetic properties.7 Both insulin glargine and insulin degludec are basal insulin analogues. As insulin synthesis has progressed, the half-life of ultra-long-acting insulin has increased, which might help decrease DKA episodes.8
Several methods have been used to improve the pharmacodynamic and pharmacokinetic profiles for basal insulin preparations. A higher concentration of insulin with post-injection precipitation is required to ensure a longer half-life and duration of action for insulin glargine U300 compared to that for glargine U100 (32 and 19 hours, respectively).9 On the other hand, insulin degludec has a longer half-life and duration of action (reaching up to 42 hours) as a result of multihexamer formation and albumin binding.10
One of the factors that may decrease DKA episodes is an adequate insulin dosage. Accordingly, a multicenter randomized controlled trial was conducted to assess the efficacy and safety of degludec compared to that of detemir.11 Children and adolescents (1–17 years old) with type 1 diabetes and who were treated with degludec had substantially decreased rates of hyperglycemia with ketosis as a secondary outcome, compared with those treated with detemir. The results of this study suggested that this reduction may be attributed to the ultra-long and flat pharmacokinetic profile of degludec.
The effectiveness of glargine U300 in patients with type 1 diabetes was assessed in a multicenter, retrospective, observational study conducted in the UK among 298 participants who used glargine U300 for 6 months. Four participants (1%) had a DKA episode requiring emergency Department visit or Hospitalization in the 6 months prior to the initiation of glargine U300, whereas six participants (2%) had DKA in the 6 months after initiation. However, no statistically significant differences were found in the frequency of DKA episodes between pre and post basal insulin initiation. Furthermore, none of these participants discontinued glargine U300 despite documented DKA episodes 6 months post initiation.12 The primary objective of our study was to assess the effects of ultra-long-acting insulin, in comparison to long-acting insulin, on the incidence of diabetic ketoacidosis (DKA) episodes among patients with type 1 DM. The secondary objective was to determine the differences in diabetes treatment indicators between the different insulin regimen types including hemoglobin A1C (HbA1c) and daily dose measures.
Methods
This study is a retrospective, observational study conducted among patients with type 1 diabetes who had appointments at the diabetes care clinic of the Security Forces Hospital, Riyadh, Saudi Arabia, from March 1, 2020, to June 31, 2020. The study was conducted following the Declaration of Helsinki and was approved by the Security Forces Hospital ethical committee before data collection or analysis, with approval number (H-01-R-069). The study was conducted using a purposive sample of patients who met the inclusion and exclusion criteria, and written informed consent was obtained from all participants in the study. Moreover, all data collected from the medical records were anonymized before analysis to maintain participants confidentiality. All patients diagnosed as type 1 DM confirmed by low c-peptide level and positive antibodies (either positive glutamic acid decarboxylase antibody or islet cell antibody or both) for more than 2 years were included in the study. Usage of both long-acting and ultra-long-acting basal insulin was considered as an inclusion criterion.
In this study, long-acting insulin was defined as an insulin that Clinically demonstrated glucose-lowering action exceeding that of intermediate-acting insulin of 16 hours and reaching up to 24 hours after subcutaneous injection in individuals with DM; this definition was met by glargine U100 and detemir. Ultra-long-acting insulin was defined as insulin with a clinical glucose lowering effect of more than 24 hours after subcutaneous injection in patients with DM.13 This included glargine U300 and degludec. The exclusion criteria were as follows: pregnant women, non-adherence with medication refill, periodic laboratory investigations or follow up appointments in a clinic; use of systemic steroids, end-stage renal disease, patients who used pre-mixed insulin, or who used an insulin pump before or during the study period, and patients who received more than two types of basal insulin during the period of the study.
Sociodemographic and clinical data were retrieved from the electronic medical records. All selected participants had regular clinic visits with at least one HbA1C reading before and after changing to ultra-long-acting basal insulin; the post readings were taken from the patients only after 6 months of initiating ultra-long-acting insulin therapy. The data collection was performed retrospectively from all patients who met the study criteria. These data included demographic data, duration of diabetes and other co-morbidities, as well as insulin type and dosage before and after starting ultra-long-acting basal insulin. Body mass index, HbA1C, and details of DKA occurrence were also included. The data about the DKA episodes were obtained from the patient records, which documented number of episodes, causes, severity, and length of hospital stay. If the DKA events had occurred outside the diabetes care clinic of the Security Forces Hospital, the patients were asked to provide this information.
Participants’ medical records were scanned for any emergency visits or admissions related to DKA 6 months before and 6 months after starting ultra-long-acting insulin. The DKA incidence criteria included any confirmed DKA as a discharge diagnosis. The diagnosis of DKA was made based on serum glucose level > 250 mg/dL, venous pH level < 7.30, serum bicarbonate level < 18, anion gap > 10, and positive ketonemia or ketonuria test. Euglycemic DKA was included if glucose level was normal or near normal at presentation, in the presence of other DKA diagnosis criteria.4 Moreover, patients were asked if they had visited their primary doctor or emergency Department because of DKA and this was recorded as well.
Statistical analysis was conducted using R version 3.5.2. The normality of distribution for each independent variable was verified using Shapiro–Wilk test. The independent paired t-test was used to compare insulin therapy measures between the two insulin regimens. In each case, the null hypothesis stated that there is no difference between mean diabetic outcomes, and the alternative hypothesis asserted that mean diabetic outcomes were affected by changing the patient’s insulin treatment. Cochran’s Q test was used to test the marginal probability of a positive occurrence of diabetic ketoacidosis before and after the longer insulin regimen.14 A P value of less than 0.05 was adopted for statistical significance.
Results
A total of 221 patients met the criteria for this study. An analysis of the individual sociodemographic and clinical characteristics revealed that most patients were female and relatively young (Table 1). In addition, the patients had comorbid conditions such as dyslipidemia, hypothyroidism, and diabetic nephropathy. ACEI (angiotensin-converting enzyme inhibitors) were the most frequently used medication after insulin therapy, followed by levothyroxine.
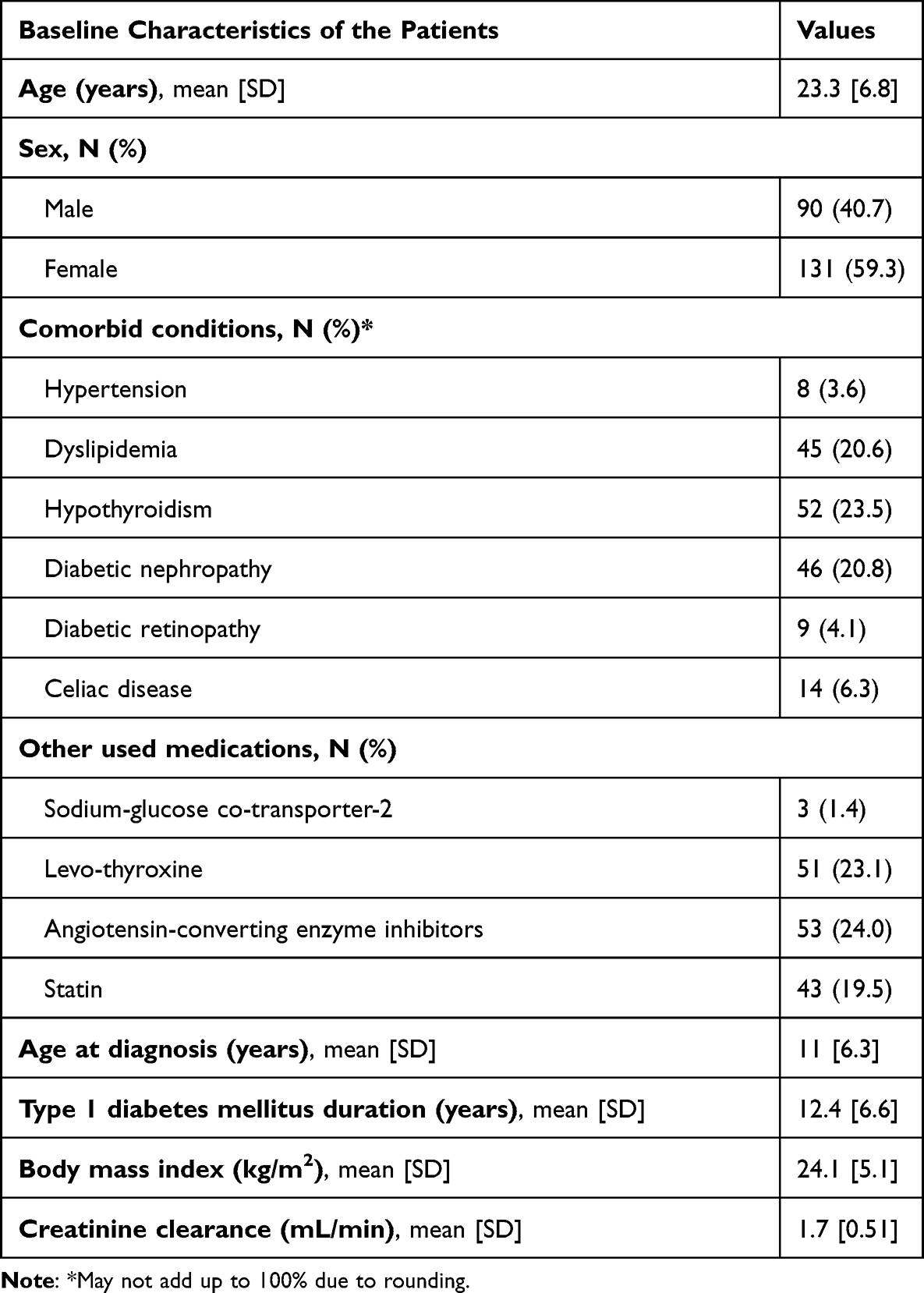 |
Table 1 Sociodemographic and Clinical Characteristics of the Study Participants |
The HbA1c level did not change significantly before and after starting the ultra-long-acting insulin therapy (9.9 vs 9.8, respectively; P >0.05). However, there was a significant increase in the total daily dose of insulin when the patients changed to the ultra-long-acting basal insulin therapy (Table 2). The average of the total daily dose of insulin therapy increased upon switching, from 76.6 to 79.3 units, with a P value of 0.0265. Nevertheless, the average basal insulin therapy doses did not show significant difference. The sub-analysis of changes in total daily insulin doses (both degludec U100 and glargine U300) showed a significant increase in the total daily dosage of insulin in the patients’ group that received glargine U300. However, degludec users showed a lesser change in the total daily dose, as shown in Table 3.
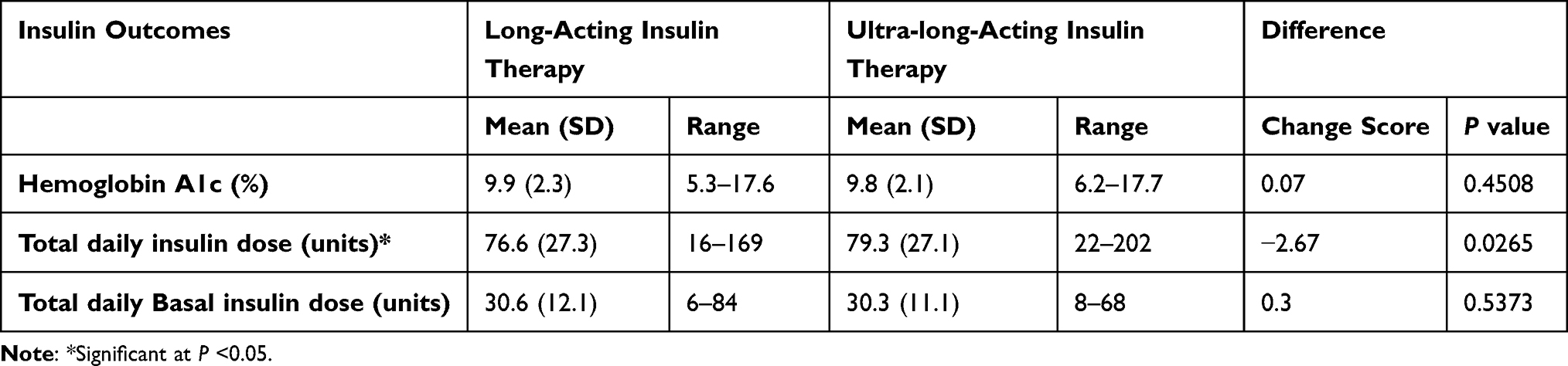 |
Table 2 Measures of Diabetes Clinical Outcomes |
 |
Table 3 Total Daily Dose Variation (Sub-Analysis for Both Basal Insulin Types: Glargine U300 and Degludec U100) |
Table 4 shows the one-way frequency charts and provides the marginal response for each insulin therapy. Subjects had fewer episodes of DKA when they were on long-acting insulin compared with ultra-long-acting insulin. Cochran’s Q test was used to display measures of agreement to identify whether DKA occurred as a result of switching to ultra-long-acting insulin therapy; it did not indicate any differences among the two proportions, χ2(1) = 0.052, P =0.8185. Moreover, sub-analysis of DKA occurrence among degludec and glargine U300 users showed no statistically significant differences as shown in Table 5. However, the frequency of DKA was lower when insulin therapy was changed from long-acting insulin therapy to degludec as compared to glargine U300.
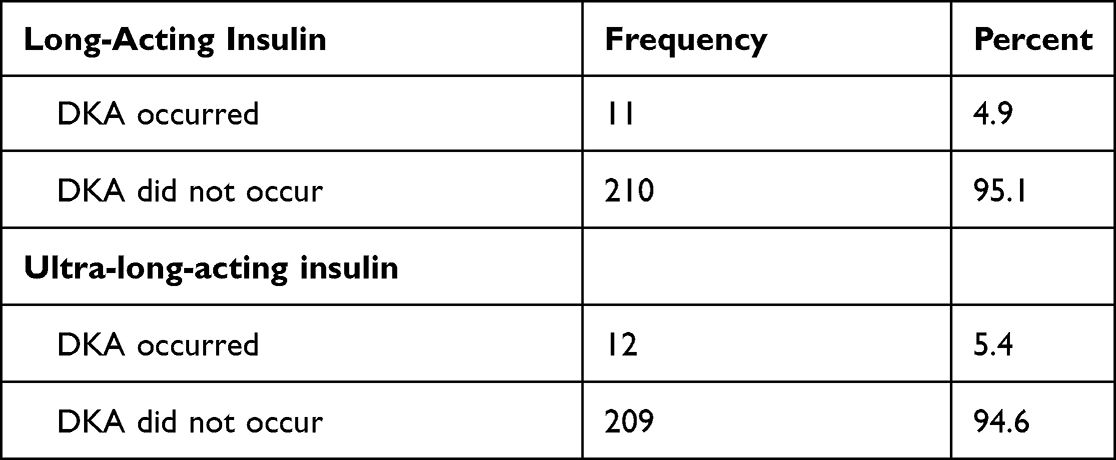 |
Table 4 The Marginal Response of Diabetic Ketoacidosis (DKA) |
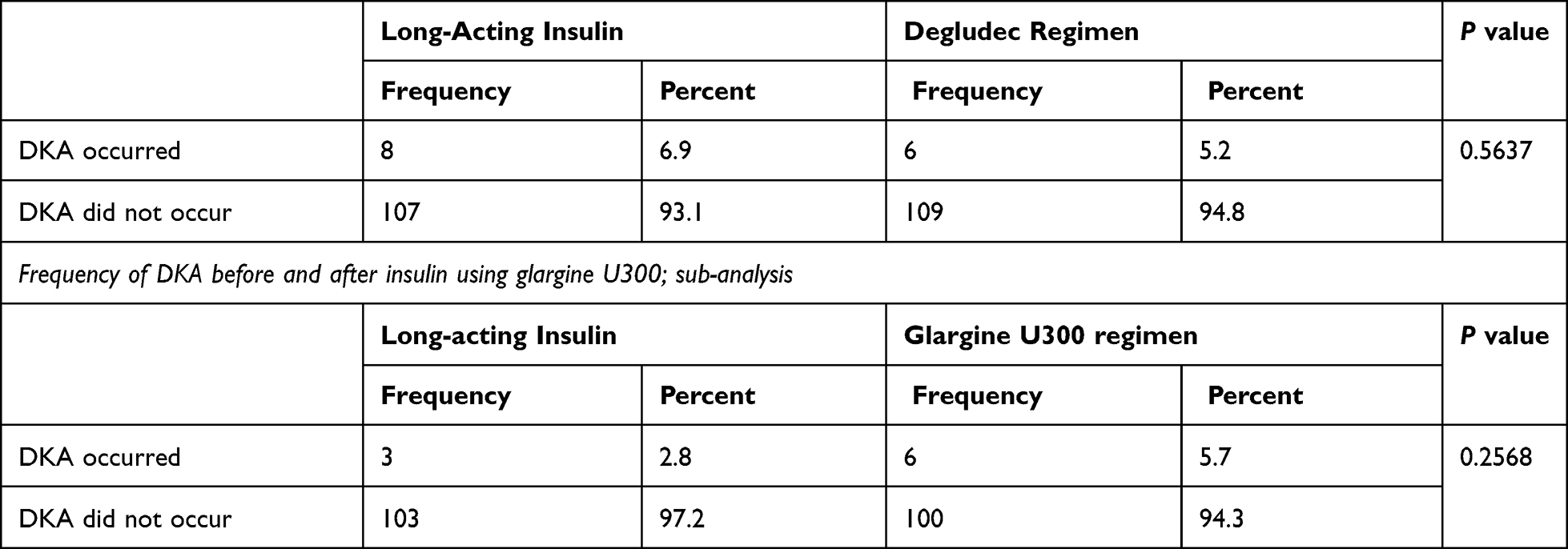 |
Table 5 Frequency of Diabetic Ketoacidosis (DKA) Before and After Using Insulin Degludec U100 or Glargine U300; Sub-Analysis |
Discussion
This study aimed to investigate the safety/efficacy profile of ultra-long-acting insulin in the provision of usual care. The study subjects were relatively young, more than half were female and suffered from multiple chronic conditions, such as dyslipidemia and hypothyroidism. A direct connection between hypothyroidism and DM has been established in literature.15 More than 24% of the study subjects had diabetic nephropathy, which might explain the high use of ACEI.
This study is the first to evaluate DKA occurrences as the primary outcome. The results did not show any statistically significant difference between before and after the initiation of ultra-long-acting basal insulin. In addition, the sub-analysis of DKA occurrence among insulin degludec and insulin glargine U300 users showed no statistically significant differences. Small and nonsignificant differences in the number of DKA episodes were noted in the medical literature. However, that study mainly investigated the effects of insulin glargine U300 on HbA1c change, whereas DKA occurrences were studied as a secondary endpoint.12
A previous randomized, controlled, open-label, multiNational trial was conducted to compare the efficacy and safety of insulin degludec and insulin detemir in children with type 1 diabetes.11 Two DKA episodes were reported in the insulin degludec group. However, the ketosis rate (ketone more than 1.5 mmol/L) was lower with degludec. A similar result was obtained in our study, as we observed fewer episodes of DKA among the study participants. This may indicate that the rate of DKA episodes might be influenced by the type of insulin used.
Total daily insulin dose showed no significant difference between pre and post insulin degludec treatment. This result is inconsistent with a previously reported study that showed a 30% reduction in the dose of insulin degludec among patients who shifted to degludec.11 However, the design and patient characteristics of that study were different from the present study.
Interestingly, the patients who shifted to insulin glargine U300 had a statistically significant increase in total daily insulin dose by over 4 units. However, the basal daily dose itself did not change after starting insulin glargine U300. A possible explanation for such an increase is the reassessment of the appropriate daily dose by the physician in patients with diabetes when switching to ultra-long-acting basal insulin. An observational study conducted among type 1 diabetes patients to assess diabetes control level after shifting to insulin glargine U300 showed nonsignificant differences in both total and basal insulin doses before and after changing basal insulin.12
A secondary endpoint included in this study was the change in HbA1c before and after ultra-long-acting basal insulin initiation. The HbA1c levels at both the time points indicated uncontrolled diabetes in the participants. This might be explained by factors other than just insulin type and preparations, such as adherence to the management plan, diabetic education, follow-up frequency, availability of diabetes management technology, and previous medical conditions including co-morbidities and complications.
The present study is not without limitations. The study data was based on medical records and was conducted in a single healthcare facility, which may hinder the generalizability of the study to the general diabetic population. Moreover, patient interviews were only conducted if the data were missing, and the data collection was performed during the COVID-19 pandemic. Some patients were lost to follow-up and had to be excluded. Prospective studies are needed for a deeper exploration of the effects of basal insulin on blood glucose control, and the impact of this on DKA occurrence in patients with type 1 diabetes.
Conclusion
The frequency of DKA episodes was not affected by changing the treatment to ultra-long-acting basal insulin in this study. Thus, the causes and prevention of DKA should be further explored. Prospective studies may help improve the assessment of basal insulin in the control of diabetes, which will reflect on the rate of general complications such as DKA. A minor increase in total daily insulin doses after shifting to ultra-long-acting basal insulin was noted especially with insulin glargine U300. However, daily basal insulin doses did not change. Uncontrolled mean HbA1c after shifting to ultra-long-acting basal insulin may suggest that insulin dosage and types are not the only cause of uncontrolled diabetes. Further studies should cover all factors affecting diabetes control.
Acknowledgement
The authors would like to thank the Deanship of Scientific Research at Prince Sattam Bin Abdulaziz University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2013;36(Supplement_1):S67–S74. doi:10.2337/dc13-S067
2. O’Keeffe DT, Maraka S, Rizza RA. HbA1c in the evaluation of diabetes mellitus. JAMA. 2016;315(6):605–606.
3. Desai D, Mehta D, Mathias P, Menon G, Schubart UK. Health care utilization and burden of diabetic ketoacidosis in the US over the past decade: a nationwide analysis. Diabetes Care. 2018;41(8):1631–1638.
4. Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009;32(7):1335–1343.
5. Zhong VW, Juhaeri J, Mayer-Davis EJ. Trends in hospital admission for diabetic ketoacidosis in adults with type 1 and type 2 diabetes in England, 1998–2013: a retrospective cohort study. Diabetes Care. 2018;41(9):1870–1877.
6. Flores M, Amir M, Ahmed R, et al. Causes of diabetic ketoacidosis among adults with type 1 diabetes mellitus: insulin pump users and non-users. BMJ Open Diabetes Res Care. 2020;8(2):e001329.
7. Barski L, Brandstaetter E, Sagy I, Jotkowitz A. Basal insulin for the management of diabetic ketoacidosis. Eur J Intern Med. 2018;47:14–16.
8. Woo VC. A review of the clinical efficacy and safety of insulin degludec and glargine 300 U/mL in the treatment of diabetes mellitus. Clin Ther. 2017;39(8S2):S12–S33.
9. Heise T, Kaplan K, Haahr HL. Day-to-day and within-day variability in glucose-lowering effect between insulin degludec and insulin glargine (100 U/mL and 300 U/mL): a comparison across studies. J Diabetes Sci Technol. 2018;12(2):356–363.
10. Heise T, Mathieu C. Impact of the mode of protraction of basal insulin therapies on their pharmacokinetic and pharmacodynamic properties and resulting clinical outcomes. Diabetes Obes Metab. 2017;19(1):3–12.
11. Thalange N, Deeb L, Iotova V, et al. Insulin degludec in combination with bolus insulin aspart is safe and effective in children and adolescents with type 1 diabetes. Pediatr Diabetes. 2015;16(3):164–176.
12. Pang T, Bain SC, Black RNA, et al. A multicentre, UK, retrospective, observational study to assess the effectiveness of insulin glargine 300 units/mL in treating people with type 1 diabetes mellitus in routine clinical practice (SPARTA). Diabet Med. 2019;36(1):110–119.
13. Ooi CP, Ting TH, Lye MS. Ultra‐long-acting insulin versus long-acting insulin for type 1 diabetes mellitus. Cochrane Database Syst Rev. 2018;2018(7):CD011102.
14. Seeger P, Gabrielsson A. Applicability of the Cochran Q test and the F test for statistical analysis of dichotomous data for dependent samples. Psychol Bull. 1968;69(4):269–277.
15. Joffe BI, Distiller LA. Diabetes mellitus and hypothyroidism: strange bedfellows or mutual companions? World J Diabetes. 2014;5(6):901–904.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.