Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Effects of Two Types of Moderate- and High-Intensity Interval Training on Serum Salusin-α and Salusin-β Levels and Lipid Profile in Women with Overweight/Obesity
Authors Nazari M ![]() , Minasian V
, Minasian V ![]() , Hovsepian S
, Hovsepian S
Received 26 February 2020
Accepted for publication 7 April 2020
Published 24 April 2020 Volume 2020:13 Pages 1385—1390
DOI https://doi.org/10.2147/DMSO.S248476
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Maryam Nazari,1 Vazgen Minasian,1 Silva Hovsepian2
1Department of Exercise Physiology, Faculty of Sport Sciences, University of Isfahan, Isfahan, Iran; 2Imam Hossein Children’s Hospital, Isfahan University of Medical Sciences, Isfahan, Iran
Correspondence: Vazgen Minasian Email [email protected]
Objective: The current study aimed to compare the effects of two modes of moderate- and high-intensity interval training on serum Salusin-α and Salusin-β and lipid profile in women with overweight/obesity.
Subjects and Methods: A number of forty females were assigned to each of (1) Control (BMI= 30.2 ± 2.8 kg/m2, n=14), (2) Moderate-intensity (BMI= 31.2 ± 3.3 kg/m2, n=13) and (3) High-intensity interval training (BMI=30.9± 3.4 kg/m2, n=13) groups. The subjects of experimental groups participated in the selected interval trainings for eight weeks. The first blood sampling was performed within 48 hours prior to the first training session and the second samples were obtained 48 hours after the last training session.
Results: The findings revealed that there were significant increases in Salusin-α (36% vs. 3%; p = 0.001) and high-density lipoprotein levels (7% vs. 5%; P = 0.039), while significant reductions in the levels of Triglyceride (− 8% vs. − 9%; p= 0.012) and total cholesterol (− 1% vs. − 8%; P =0.01) levels of moderate- and high-intensity interval training groups, respectively. Also, there were insignificant changes in Salusin-β (− 7% vs. − 5%; P = 0.108), low-density lipoproteins (− 3% vs. − 11%; P =0.046) and very-low-density lipoprotein (− 10% vs. − 8%; P = 0.056) compared to control group. There were only significant differences between Salusin-α and high-density lipoprotein levels of training groups (P< 0.05).
Conclusion: It is suggested that, although improvements in lipid profile was nearly similar for two training modes, moderate intensity interval training was more effective to prevent and control atherosclerosis.
Keywords: exercise, lipid profile, obesity, Salusin-α, Salusin-β
Introduction
Due to lifestyle changes such as inactivity and malnutrition, increasing obesity is a social-medical problem in developed and developing countries.1 Obesity increases the risk of metabolic diseases such as type 2 diabetes, hypertension, dyslipidemias and cardiovascular disease, which prevents healthy aging.1 Since, dyslipidemia may affect atherosclerosis and these are associated with cardiovascular diseases (CHD), hence, high levels of low-density lipoprotein increase the risk of cardiovascular disease and high levels of high-density lipoprotein are considered as a protective factor.2,3 Interestingly, dyslipidemia is one of the most important causes of the progression of atherosclerosis.4
Salusins belong to a new class of peptides discovered by Shichiri et al.5 Two peptides consisting of 28 and 20 amino acids are called Salusin-α and Salusin-β, respectively.6 Salusins are peptides that considered to be biosynthesized from preprosalusin, an alternative-splicing product of the torsion dystonia-related gene (TOR2A), after frameshift reading and digestion at dibasic amino acids. Salusins are expressed and synthesized ubiquitously within human tissues, including the vasculature, the central nervous system, the kidney, and also Salusin-α is present in human plasma and urine.5 The accumulation of cholesterol esters as lipid droplets within macrophages and the formation of foam cells lead to the production of atherosclerotic plaques that play an important role in the development and occurrence of atherosclerosis.7 Both Salusin-α and Salusin-β are produced from one peptide called Prosalusin; however, they have different effects on acetyl-CoA acetyltransferase (ACAT1) expression. Although each Salusin probably binds to its own junction at the cell surface, specific receptors for each Salusin have not yet been identified.8
Watanabe et al6 showed that Salusin-α suppresses the formation of foam cells by downregulation of ACAT1, but Salusin-β increases the foam cell formation by upregulation of ACAT1. This findings indicated that Salusin α may prevent atherosclerosis, whereas Salusin-β acts as a potential proatherogenic agent, and it is concluded that the serum levels of Salusin-α were significantly lower in patients with coronary artery disease than in those without coronary artery disease. In contrast, serum levels of Salusin-β were significantly higher in patients with coronary artery disease,9 also, it seems that Salusin β can act as a ligand surrogate or substituent, but the precise receptor for Salusins has not yet been identified as a natural ligand.10 Additionally, it was shown very recently that, there was no significant difference in the Salusin-α and Salusin-β levels between obese and healthy children. However, a negative correlation was found between Salusin-α and diastolic blood pressure.11 The sedentary lifestyle is closely linked to obesity and many biomarkers that underlie atherosclerosis, such as decreased high-density lipoproteins and increased low-density lipoproteins and triglycerides. Therefore, regular physical activity can induce metabolic adaptations, resulting in improved lipid profile and reduced cardiovascular disease.12 The review of literatures suggest that the amount of positive changes in lipid profile has been investigated and quantified among endurance athletes or following endurance and resistance training and there are little studies examining impacts of different training methods and comparing different training intensities. Paoli et al, in a study showed that after 12 weeks of high intensity circuit exercise, the levels of triglyceride, low-density lipoprotein and total cholesterol were significantly decreased and the levels of high-density lipoprotein was increased, and high intensity exercises caused more changes in the indices associated with lipid profile.13 In another study, Wong et al examined the effect of combination of aerobic and resistance training on lipid profile among children with obesity, and reported that following exercise intervention, plasma triglyceride levels in children with obesity were significantly reduced.14 Although, several studies have investigated the effect of Salusin injections as a medicinal compound, whereas the impact of exercise training on serum levels of Salusins, and especially in women with obesity is unclear in the literature. However, in a study by Grzegorzewska et al, a significant increase in serum levels of Salusin-α was observed with changing diet and inactive lifestyle among dialysis patients.15
High intensity interval training (HIIT) has been shown to increase aerobic fitness more effectively than continuous moderate intensity training (CMIT), therefore suggesting that it would confer greater cardioprotective benefits, improve abdominal and subcutaneous fat loss, fat oxidation, appetite regulation and aerobic capacity.16 Therefore, given the lack of a clear picture on the impact of MIIT and HIIT exercises on Salusins and lipid profile for individuals with overweight and obesity who are always being exposed to cardiovascular disease, this study aimed to compare the effects of 8 weeks of HIIT and MIIT and without exercise upon Salusin α, Salusin β and lipid profile of women with overweight/obesity. It has been also hypothesized that gains induced by HIIT would be greater than MIIT.
Subjects and Methods
Subjects
This is a quasi-experimental study. A number of 40 women (age 25–35 years) with overweight/obesity volunteered to participate in the study. The subjects were divided into three matched group according to measurement of Body mass index (BMI). (Control; BMI= 30.2 ± 2.8 kg/m2, n=14, MIIT; BMI= 31.2 ± 3.3 kg/m2, n=13 and HIIT (BMI= 30.9 ± 3.4 kg/m2, n=13). Subjects were first asked to complete the General Health and Wellness Questionnaire and signed a written informed consent to confirm their voluntary participation in the study. The committee of research ethics of University of Isfahan was also licensed for this research under number IR.UI.REC.1396.059 with adherence to Helsinki ethical principles. Inactive people included those who had not participated in any regular training during the last year. Exclusion criteria included smoking, arthritis, immune disorders, taking medications that affect immune function, recent surgery, infection and any other chronic disorders.
One week before the beginning of the study, the intervening variables of weight, body fat percentage and maximum rate of oxygen consumption were measure on the subjects. Further, prior to the start of the eight-week training period, the training protocol was piloted on the volunteers to ensure their ability to execute the training program. For this study, Jackson and Pollock test were used to measure fat percentage of subjects using caliper17 and Astrand cycle test18 was used to estimate the peak oxygen consumption (VO2peak). The maximal heart rate of each subject was also calculated using the formula (Age −220).
The initial blood sampling was performed 48 hours prior to the first training session to determine basal levels of Salusin-α, Salusin-β, High-density lipoproteins (HDL), Low-density lipoproteins (LDL), Very low-density lipoproteins (VLDL), Total cholesterol and Triglycerides. The HIIT and MIIT experimental groups performed the training protocol for 8 weeks (3 sessions per week) using Stationary bicycles. During the period of eight weeks of training, the subject’s nutritional control was out of the reach for the researcher; however, the subjects were asked to consume low-fat and light meals at nights before blood sampling to minimize the impact of the last meal (At least 12 hours fasting before blood sampling) on lipid profile. 48 hours after the completion of eight-week training, the second blood sampling was performed on the subjects in both groups. Similar tests were performed on the control group to more accurately examine the effects of the independent variable. Blood samples were taken from the subjects’ anterior vein in sitting position. The samples were centrifuged and stored at −80°C in the freezer for subsequent stages. Serum concentrations of Salusin-α and Salusin-β were measured using the Eastbiopharm (H)-96 Test kit. The most important limitations of the study were the possible effects of the menstrual cycle, hormonal changes, daily activities and diet on outcomes, that precise control of these factors was not possible.
The training protocol consisted of 2-minute sets with 30 seconds of pedaling and 30 seconds of rest. Three minutes of active rest (50% of maximal heart rate) was considered between each set. The training intensity for the MIIT and HIIT groups consist of 75–80% and 90–95% maximal heart rate (HRmax), respectively. Table 1. Provides the summary of training protocol.
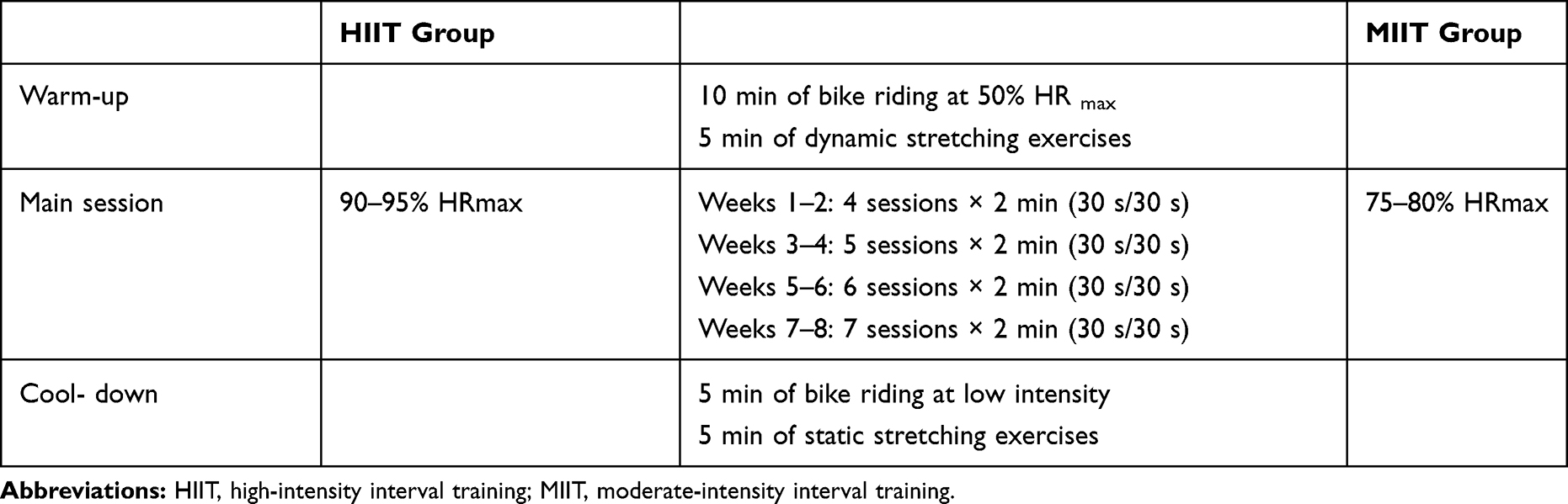 |
Table 1 Summary of the Training Programs |
Statistical Analysis
The mean and standard deviation values of measured variables calculated by descriptive statistics. Shapiro–Wilk test was used to check the normality of data, while analysis of covariance (ANCOVA) statistics was used to compare the between group changes in serum levels of factors being studied. SPSS software version 21 (IBM, New York, USA) was applied for data analysis. The significance level of P ≤ 0.05 was considered for testing research hypotheses.
Results
The mean age of participants was 28 ± 3.3y. Forty women with overweight/obesity and body mass index of control: (BMI= 30.2 ± 2.8 kg/m2), MIIT: (BMI= 31.2 ± 3.3 kg/m2) and HIIT (BMI= 30.9 ± 3.4 kg/m2), engaged in the 8-week exercise interventions. Participant characteristics in pre and post interventions are listed in Table 2.
 |
Table 2 Descriptive and Physiological Characteristics of Subjects (Mean ±SD) |
The results of ANCOVA by adjusting pre-test as covariate variable showed significant increases in levels of Salusin-α (F2,40=65.889, Ƞ2=0.785, P=0.001), HDL (F2,40=3.549, Ƞ2=0.165, P=0.039), and significant decreases in total cholesterol (F2,40=5.202, P = 0.010, Ƞ2 = 0.224) and triglyceride levels (F2,40=5.058, P = 0.012, Ƞ2= 0.219) for both training groups compared to the control group. But, there was no significant changes in serum levels of Salusin β (F2, 40=0.812, P = 0.452, Ƞ2= 0.043), LDL (F2, 40 =2.366, P=0.108, Ƞ2= 0.116), VLDL (F2, 40 =3.12, P = 0.056, Ƞ2= 0.148).
There were significant reductions across time from pre- to post-intervention in both training groups in Salusin-β (MIIT= −7%, vs HIIT= −5%), Triglyceride (MIIT= −8% vs HIIT= −9%) and VLDL (MIIT= −10%, HIIT= −8%) levels respectively. In contrary, Salusin-α (MIIT= 36% vs HIIT= 3%) and HDL levels (MIIT= 7% vs HIIT= 5%) were increased across time from pre- to post-intervention in both MIIT and HIIT groups, respectively (P<0.05) (Table 3).
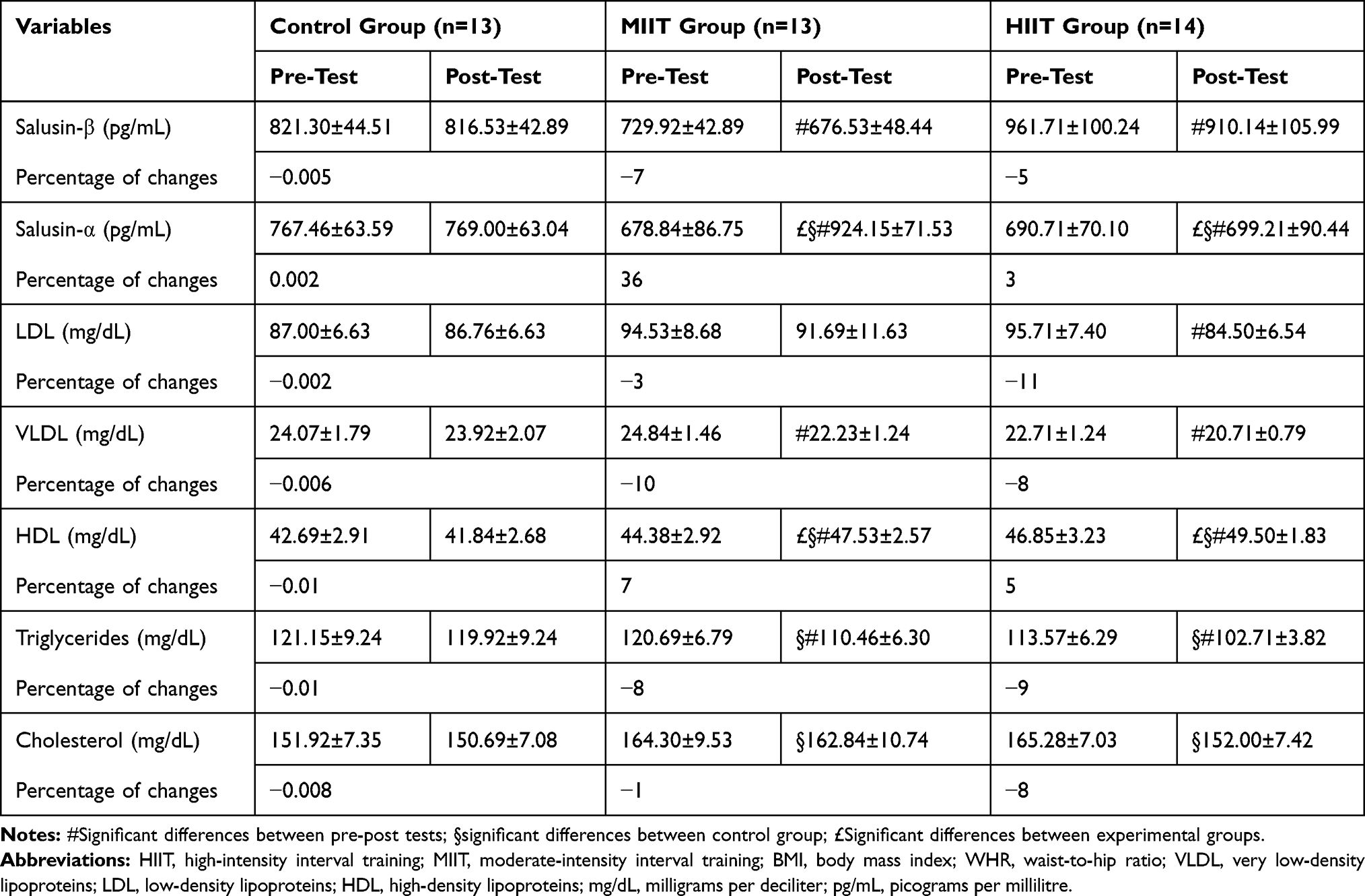 |
Table 3 Variables Measured in Pre- and Post-Test (Mean± SD) |
Discussion
Salusins, which are endogenously secreted from the hypothalamopituitary axis, vascular endothelium, and kidneys, play roles in atherogenesis and the regulation of hemostasis. However, they have opposing effects on atherosclerosis. Salusin-β is a precursor of atherosclerosis, while Salusin-α has a protective effect against atherosclerosis.7
The results reveal insignificant reductions in Salusin β levels and significant increases in Salusin α in the MIIT and HIIT groups, respectively. In this regard, previous studies have shown that there is no study available on the effect of exercise training on serum levels of Salusin α and Salusin β. Only a single study performed by Grzegorzewska (2014) showed that in patients dialyzed, lifestyle changes (reduced dietary fat + increased physical activity) and increased the levels of high-density lipoproteins and Salusin-α.15 The results of this study are in line with the results the Grzegorzewska on changes in levels of Salusin-α, but there were differences in mode and intensity of exercises.
However, some concomitant changes in Salusin-α and improvement in lipid profile observed through the present study confirm the results of some laboratory studies. One study has found that mice with apolipoprotein E (ApoE) deficiency showed a significant increase in the incidence of atherosclerotic lesions in the aorta and macrophage infiltration after 4 and 8 weeks injections Salusin β, but no changes was obtained in total cholesterol.19 In contrast, 4 and 8 weeks injections of Salusin-α significantly decreased aortic atherosclerosis which is the product of reduced formation of macrophage foam cells, and there were also positive changes in lipid profile, with a significant increase in serum levels of high-density lipoproteins and a decrease in total cholesterol levels.19
The results of this study showed positive effects on lipid profile among both the MIIT and HIIT groups. However, for some factors such as cholesterol, the percentage of positive changes was more frequent for the HIIT group. As in some recent studies, Racil et al investigated the impact of high-intensity interval training vs. moderate-intensity interval training on lipid profile in women with obesity. Subjects were trained in two groups: the HIIT group with an intensity of 110–100% VO2peak and the MIIT group with an intensity of 70–80% VO2 peak. After 12 weeks of training, both training groups showed positive changes in levels of low-density lipoproteins and high-density lipoproteins. Triglyceride and cholesterol levels were significantly decreased only in the HIIT group.20 In this regard, Heidari et al investigated the impact of HIIT on changes in lipid profile among males with obesity. After 12 weeks of HIIT exercise intervention with an intensity of 80–90% HR max, the results of lipid profile did not improve significantly.21 On the other hand, Whyte et al examined effects of two weeks of sprint interval training (SIT) on lipid profile and health-related factors among overweight and sedentary men. They reported that although SIT improved some variables associated with lipid profile, these changes were not significant, and they emphasized on a sufficient training time to make changes in lipid profile.22 Previous studies have shown the role of regular physical activities o metabolic adaptations and lipid profile improvement;13 but there is still no consensus on determining the best training intensity to improve lipid profile. It should be noted that intensity and duration of trainings are important determinants. Regarding to the importance of training intensity, Okura et al examined the impact of walking (a low intensity exercise) and aerobic exercises (70–85% maximal oxygen uptake) and found that training intensity was the key factors affecting the improvement of lipid profile.23 These results demonstrated that moderate intensity interval exercises may have beneficial effects on lipid profile and some new introduced biomarkers of atherosclerosis in women with overweight/obesity. Furthermore, based on the nature of HIIT exercise, this training mode in spite of its time saving benefit, the adherence in obese individuals are extremely difficult and requires more motivation. Therefore, it is recommended that future studies investigate the effects of various exercise training with different intensities on Salusins and other related biomarkers in order to obtain more information in this regard.
Conclusion
In sum, we concluded that Salusin-α as a protective biomarker against atherosclerosis and the regulation of haemostasis were more pronounced in response to medium intensity interval training. In contrast, Salusin-β as a precursor of atherosclerosis and lipid profile of subjects probably were more influenced by high intensity interval training. Therefore, both exercise training modes are useful to prevention of atherosclerosis. However, due to restricted findings on the impact of various exercise training on Salusins levels, no definitive conclusion can be obtained. Moreover, because of positive changes found through the current study, we suggest moderate intensity interval training to prevention or management of atherosclerosis.
Ethical Approval
This study was carried out in accordance with the ethical code of working with human subjects under IR.UI.REC. 1396.059 code of the University of Isfahan.
Acknowledgment
This study was supported by the vice dean for research and technology of the University of Isfahan for doctoral students. Therefore, it is my duty to express my gratitude for his unconditional support.
Funding
This work was supported by the vice dean for research and technology of the University of Isfahan for doctoral students.
Disclosure
The authors declare that they have no conflicts of interest regarding this work.
References
1. Handschin C, Spiegelman BM. The role of exercise and PGC1α in inflammation and chronic disease. Nature. 2008;454(7203):463–469. doi:10.1038/nature07206
2. Ingelsson E, Schaefer EJ, Contois JH, et al. Clinical utility of different lipid measures for prediction of coronary heart disease in men and women. JAMA. 2007;298(7):776–785. doi:10.1001/jama.298.7.776
3. Lichtenstein L, Kersten S. Modulation of plasma TG lipolysis by angiopoietin-like proteins and GPIHBP1. Biochim Biophys Acta Mol Cell Biol Lipids. 2010;1801(4):415–420.
4. Shoji T, Abe T, Matsuo H, et al. Chronic kidney disease, dyslipidemia, and atherosclerosis. J Atheroscler Thromb. 2012;19(4):299–315. doi:10.5551/jat.10454
5. Shichiri M, Ishimaru S, Ota T, Nishikawa T, Isogai T, Hirata Y. Salusins: newly identified bioactive peptides with hemodynamic and mitogenic activities. Nat Med. 2003;9(9):1166–1172. doi:10.1038/nm913
6. Watanabe T, Nishio K, Kanome T, et al. Impact of salusin-α and-β on human macrophage foam cell formation and coronary atherosclerosis. Circulation. 2008;117(5):638–648. doi:10.1161/CIRCULATIONAHA.107.712539
7. Yu X-H, Fu Y-C, Zhang D-W, Yin K, Tang C-K. Foam cells in atherosclerosis. Clin Chim Acta. 2013;424:245–252. doi:10.1016/j.cca.2013.06.006
8. Wang Z, Takahashi T, Saito Y, et al. Salusin β is a surrogate ligand of the mas-like G protein-coupled receptor MrgA1. Eur J Pharmacol. 2006;539(3):145–150. doi:10.1016/j.ejphar.2006.03.064
9. Sato K, Watanabe R, Itoh F, Shichiri M, Watanabe T. Salusins: potential use as a biomarker for atherosclerotic cardiovascular diseases. Int J Hypertens. 2013;2013:1–8. doi:10.1155/2013/965140
10. Niepolski L, Grzegorzewska AE. Salusins and adropin: new peptides potentially involved in lipid metabolism and atherosclerosis. Adv Med Sci. 2016;61(2):282–287. doi:10.1016/j.advms.2016.03.007
11. Dervişoğlu P, Elmas B, Kösecik M, İşgüven SP, Büyükavc M, Mehmet KM. Salusin-α levels are negatively correlated with diastolic blood pressure in children with obesity. Cardiol Young. 2019;29(10):1225–1229. doi:10.1017/S1047951119001173
12. Durstine JL, Grandjean PW, Davis PG, Ferguson MA, Alderson NL, DuBose KD. Blood lipid and lipoprotein adaptations to exercise. Sports Med. 2001;31(15):1033–1062. doi:10.2165/00007256-200131150-00002
13. Paoli A, Pacelli QF, Moro T, et al. Effects of high-intensity circuit training, low-intensity circuit training and endurance training on blood pressure and lipoproteins in middle-aged overweight men. Lipids Health Dis. 2013;12(1):131. doi:10.1186/1476-511X-12-131
14. Wong PC, Chia M, Tsou IY, et al. Effects of a 12-week exercise training programme on aerobic fitness, body composition, blood lipids and C-reactive protein in adolescents with obesity. Ann Acad Med Singapore. 2008;37(4):286–293.
15. Grzegorzewska AE, Niepolski L, Sikora J, Janków M, Jagodzinski PP, Sowinska A. Effect of lifestyle changes and atorvastatin administration on dyslipidemia in hemodialysis patients: a prospective study. Pol Arch Med Wewn. 2014;124:443–451. doi:10.20452/pamw.2401
16. De Souza DC, Matos DC, Victor AF, et al. Effects of high-intensity interval and moderate-intensity continuous exercise on inflammatory, leptin, IgA, and lipid peroxidation responses in obese males. Front Physiol. 2018;9:567–570. doi:10.3389/fphys.2018.00567
17. Roger E, Thomas R. Kinanthropometry and Exercise Physiology Laboratory Manual: Tests, Procedures and Data: Volume Two: Physiology. Routledge; 2013.
18. Ekblom‐Bak E, Björkman F, Hellenius ML, Ekblom B. A new submaximal cycle ergometer test for prediction of VO2max. Scand J Med Sci Sports. 2014;24(2):319–326. doi:10.1111/sms.12014
19. Nagashima M, Watanabe T, Shiraishi Y, et al. Chronic infusion of salusin-α and-β exerts opposite effects on atherosclerotic lesion development in apolipoprotein E-deficient mice. Atherosclerosis. 2010;212(1):70–77. doi:10.1016/j.atherosclerosis.2010.04.027
20. Racil G, Ben Ounis O, Hammouda O, et al. Effects of high vs. moderate exercise intensity during interval training on lipids and adiponectin levels in obese young females. Eur J Appl Physiol. 2013;113(10):2531–2540. doi:10.1007/s00421-013-2689-5
21. Heydari M, Freund J, Boutcher SH. The effect of high-intensity intermittent exercise on body composition of overweight young males. J Obes. 2012;2012:1–8. doi:10.1155/2012/480467
22. Whyte LJ, Gill JM, Cathcart AJ. Effect of 2 weeks of sprint interval training on health-related outcomes in sedentary overweight/obese men. Metabolism. 2010;59(10):1421–1428. doi:10.1016/j.metabol.2010.01.002
23. Okura T, Nakata Y, Tanaka K. Effects of exercise intensity on physical fitness and risk factors for coronary heart disease. Obesity. 2003;11(9):1131–1139. doi:10.1038/oby.2003.154
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.