")
Back to Journals » International Journal of Women's Health » Volume 15
Effects of the Severe Acute Respiratory Syndrome Coronavirus 2 Inactivated Vaccine on the Outcome of Frozen Embryo Transfers: A Large Scale Clinical Study
Authors Zhang XL, Chen YH, Zhang SP, Wu XQ, Wang XP
Received 8 February 2023
Accepted for publication 20 July 2023
Published 8 August 2023 Volume 2023:15 Pages 1305—1316
DOI https://doi.org/10.2147/IJWH.S407773
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Xue-Luo Zhang,* Yan-Hua Chen,* Si-Ping Zhang, Xue-Qing Wu, Xian-Ping Wang
The Reproductive Center, Children’s Hospital of Shanxi and Women Health Center of Shanxi, Shanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xian-Ping Wang, The Reproductive Center, Children’s Hospital of Shanxi and Women Health Center of Shanxi, 13 Xinmin North Street, Xinghualing District, Taiyuan, Shanxi, 030001, People’s Republic of China, Tel +86 13934500073, Email [email protected]
Background: Coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is a life-threatening infectious disease that has become a global pandemic.
Objective: This study aimed to explore the effects of SARS-CoV-2 inactivated vaccine on the outcome of frozen embryo transfer (FET).
Methods: We grouped patients who underwent FET between August 2021 and March 2022 based on their vaccination status, number of doses, and the interval between the last dose and the FET, and then compared the differences in pregnancy outcomes among the groups.
Results: There were 1084 vaccinated patients and 1228 non-vaccinated ones. There were significant differences in the live birth rate between the vaccination and non-vaccination groups (16.61% vs 28.26%), among the one-dose, two-dose, and three-dose groups (22.28% vs 19.51% vs 7.27%), and among the groups with interval ≤ 1 month, 1– 2 months, and ≥ 2 months (38.38% vs 27.27% vs 12.03%). There were significant differences in the persistent pregnancy rate between the vaccination and non-vaccination groups (22.88% vs 14.09%), among the one-dose, two-dose, and three-dose groups (14.51% vs 23.80% vs 38.18%), and among the groups with interval ≤ 1 month, 1– 2 months, and ≥ 2 months (1.01% vs 8.44% vs 28.16%). There were significant differences in the neonatal weight between the vaccination and non-vaccination groups [3805.50 (3746.00– 3863.50) vs 2970.00 (2500.00– 3400.00)]. There were significant differences in the premature birth rate among the one-dose, two-dose, and three-dose groups (23.26% vs 34.59% vs 100.00%), and among the groups with interval ≤ 1 month, 1– 2 months, and ≥ 2 months (15.79% vs 21.43% vs 37.00%).
Conclusion: Pregnancy outcomes were not affected by taking the SARS-CoV-2 inactivated vaccine before FET, the number of doses, and the interval between doses. These findings provide evidence supporting the safety of administering the SARS-CoV-2 inactivated vaccine during pregnancy, which can be used as a guide for vaccinating patients undergoing ART.
Keywords: COVID-19, frozen embryo transfer, pregnancy rate, vaccination
Introduction
Coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is one of the most threatening infectious diseases that mankind is facing in this century. On March 11, 2020, the World Health Organization (WHO) announced that COVID-19 had become a global pandemic,1 with more than 173 million confirmed cases, and 3.7 million deaths worldwide.2
Due to the population’s general susceptibility to SARS-CoV-2, universal vaccination is a matter of great urgency. China had got 90.63% of its total population vaccinated against COVID-19 by March 31, 2022.3–5 The latest consensus document released worldwide has no special restrictions on the vaccination of people of childbearing age for COVID-19.6,7 The inactivated vaccine has been proven safe for use in Chinese people over 18 years,8 and recipients of the inactivated vaccine in China also include those who are preparing for pregnancy or receiving treatment with assisted reproductive technology (ART).9 However, what remains unclear is whether vaccination against COVID-19 adversely affects a woman’s ability to conceive and what is its effect on the pregnancy outcome.
A comparison of obstetric outcomes of pregnant women receiving SARS-CoV-2 mRNA vaccines at different gestational weeks showed no evidence of association between increase in complications for pregnancy or childbirth, and the vaccination.10–13 Considering the uncertainty of COVID-19 vaccine on reproductive function and safety of offspring, there are only a handful of studies that have been conducted on the effects of vaccination on embryo quality and pregnancy outcomes of patients undergoing ART.
COVID-19 may affect female fertility by attacking ovarian tissue and granulosa cells and reducing ovarian function and oocyte quality. It may also damage endometrial epithelial cells and affect early embryo implantation.14,15 In the general population, COVID-19 may predispose to thrombosis in the venous and arterial circulation.16,17 COVID-19 may play an important role in pregnancy due to its prethrombotic state. Pregnant women with COVID-19 also exhibit a higher risk of intensive care unit admission, need for mechanical ventilation, maternal death, stillbirth, and other adverse outcomes compared to women of childbearing age who are not pregnant.18–20
Orvieto et al reported for the first time that SARS-CoV-2 mRNA vaccine had no effect on the quantity, quality, and ovarian reserve of eggs during the in vitro fertilization (IVF) cycle,21 as well as on the laboratory results or pregnancy rate during the IVF cycle.22 SARS-CoV-2 inactivated vaccine had no effect on the number of retrieved oocytes in fresh IVF, quality embryo implantation rate, and clinical pregnancy rate.22 A few studies have focused on the effects of COVID-19 vaccine on the pregnancy rate during the freezing cycle, but the sample size of such studies is limited.
This study intended to investigate the effects of SARS-CoV-2 inactivated vaccine on the outcome of frozen embryo transfer (FET) with a larger sample size.
Materials and Methods
Patients
We included participants who underwent FET between August 1, 2021 and March 10, 2022. We collected details pertaining to the dates of vaccination, and the names and manufacturers of SARS-CoV-2 inactivated vaccines received by participants and their spouses on the day of the embryo transfer procedure. To ensure the accuracy of information, we obtained information from relevant apps (eg, Alipay), and recorded it accurately. All patients were given SARS-CoV-2 inactivated vaccines (Beijing ConoVe Life Science Co., Ltd. or Beijing Institute of Biological Products Co., Ltd.). The entire vaccination process consisted of three doses, with 21 days between the first and the second doses, and at least six months between the second and the third doses. This study was approved by the Ethics Committee (Ethics No: IRB-KYYN-2021-002). All patients gave informed consent, and their information was kept confidential.
Inclusion criteria:23 We included patients whose age was between 20–40 years; the menstrual cycle was regular (24–35 days); the morphology of the uterine cavity was normal; there were transferrable frozen embryos or blastulas. Exclusion criteria:23 We excluded patients where one or both spouses had chromosome abnormalities; the uterine cavity was malformed; there was a history of endometrial tuberculosis; patients had adenomyosis or fibroid pressing on the uterine cavity; there were repeated instances of uterine dropsy; endometrial polyp; obvious hydrosalpinx; the thickness of endometrium was less than 8 mm; and repeated implantation failure (embryo transfer and implantation failed ≥ 3 times).
Grouping
Based on whether patients had received SARS-CoV-2 inactivated vaccines or not, they were divided into the vaccination group, and the non-vaccination group, respectively.24 Based on the number of doses they received, patients in the vaccination group were further divided into the one-dose group, the two-dose group, and the three-dose group.25 Based on the interval between the last dose of SARS-CoV-2 inactivated vaccine and the FET, they were further divided into the group with interval ≤ 1 month, the group with interval of 1–2 months, and the group with interval ≥ 2 months.22
Endometrium Preparation Schedule
The endometrial preparation was performed as previously described.26,27
Natural cycle: B-mode ultrasound monitoring was performed on day 10–12 after menstruation, and the follicle development was regularly monitored. When the diameter of the dominant follicle was ≥ 14 mm, the levels of luteinizing hormone (LH) was monitored. When the diameter of the follicle was more than 18 mm and the thickness of the endometrium was ≥ 8 mm, Human Chorionic Gonadotrophin HCG10000IU was intramuscularly injected to stimulate the LH peak and induce ovulation. Embryos were transferred on day 3–5 after the ovulation. From the ovulation day until 10 weeks of gestation, Dydrogesterone tablets (Abbott) were administered, 20 mg each time, and luteal support was administered twice a day.
Artificial cycle: From day 3 after menstruation, estrogen (Progynova) was given orally for 5 days, 2 mg/day; later, the dosage was increased to 4 mg/day, and it was given orally for 3 days. B-mode ultrasound monitoring was performed; if the thickness of the endometrium was < 7 mm, the dosage of estrogen was progressively increased by 2 mg, until the thickness of the endometrium was ≥ 8 mm. Dydrogesterone (Duphaston) was given, 20 mg each time, endometrium translation was performed twice a day; 3–5 days after oral administration of Dydrogesterone, embryos were transferred according to their conditions (embryos on day 3 or day 5). After the embryo transfer, we continued giving estrogen and dydrogesterone orally (same dose as before) until 10 weeks of gestation.
Downregulation artificial cycle: On day two of the menstruation cycle, we injected 3.75 mg of leuprorelin acetate microspheres sustained release. This was supplemented by estrogen (Progynova) after 28 days; the drug used was the same as that in the artificial cycle.
Ovulation induction cycle: On day 2 of menstruation, 50 mg of clomiphene citrate was given orally, twice a day, for 5 days. Later, the ovulation induction drugs were adjusted according to the follicle growth, until the diameter of the dominant follicle was ≥ 18 mm, and the thickness of endometrium was ≥ 8 mm, Then, HCG10000IU was intramuscularly injected to stimulate LH peak and induce ovulation. Embryos were transferred on day 3–5 after the ovulation. From the ovulation day until 10 weeks of gestation, 20 mg dydrogesterone tablets (Abbott) were administered twice a day, and luteal support was administered twice a day.
Study Definitions
In this study, we defined clinical pregnancy as gestational sacs and fetal cardiomotility that are visible in the transvaginal ultrasonography. Persistent pregnancy referred to pregnancy that lasted beyond 20 weeks. Premature birth referred to the birth of a baby between 28 weeks and 37 weeks gestational age. Embryo implantation rate = number of gestational sacs / number of transferred embryos × 100%; Clinical pregnancy rate = number of clinical pregnancy cycles / number of transfer cycles × 100%; Biochemical pregnancy rate = number of biochemical pregnancy cycles / number of transfer cycles × 100%; Abortion rate = number of abortion cycles less than 12 weeks / number of clinical pregnancy cycles × 100%; Ectopic pregnancy rate = number of ectopic pregnancy cycles / number of clinical pregnancy cycles × 100%; Live birth rate = number of live birth cycles / number of transfer cycles × 100%. Premature birth rate = number of women giving birth prematurely / total number of women in labor during the same period × 100%. Persistent pregnancy rate = number of persistent pregnancy cycles / number of transfer cycles × 100%.27,28
Statistical Analysis
We used SPSS 26.0 software for statistical processing and analysis. Categorical variables were compared using the Pearson chi-square test and expressed as numbers and percentages. Continuous variables were compared using the SK normality test. Those in normal distribution were analyzed using t-test or one-way Analysis of variance (ANOVA), and expressed by mean ± standard deviation (x±s). Data in non-normal distribution were analyzed using the Mann–Whitney U-test and expressed as median (lower quartile-upper quartile). P < 0.05 suggested statistically significant differences.
Results
General Characteristics of Participants
In this study, we included a total of 2312 patients who underwent FET between August 1, 2021 and March 10, 2022. The mean age of women was 32.39±3.79 years, and the mean thickness of the endometrium was (9.73±1.67) mm. Among them, 1084 were vaccinated, and 1228 were non-vaccinated. Among patients in the vaccination group, 193 had taken one dose, 836 had taken two doses, and 55 had taken three doses. Based on the interval between the last vaccine dose and FET, there were 99 patients in the group with interval ≤ 1 month, there were 154 in the group with interval of 1–2 months, and there were 831 patients in the group with interval ≥ 2 months.
Pregnancy Outcomes in the Vaccination and Non-Vaccination Groups
There were no significant differences between patients in the vaccination group and the non-vaccination group in terms of general characteristics such as age, body mass index (BMI), type of infertility, factors for infertility, transfer plan, the number of transferred embryos, and the level of transferred embryos. When we compared pregnancy outcomes, there were no significant differences between the two groups in factors such as the biochemical pregnancy rate, clinical pregnancy rate, implantation rate, abortion rate, ectopic pregnancy rate, and premature birth rate. However, the live birth rate in the non-vaccination group was significantly higher than that in the vaccination group, with statistically significant differences. The persistent pregnancy rate and the neonatal weight in the vaccination group were significantly higher than those in the non-vaccination group. Details are given in Table 1.
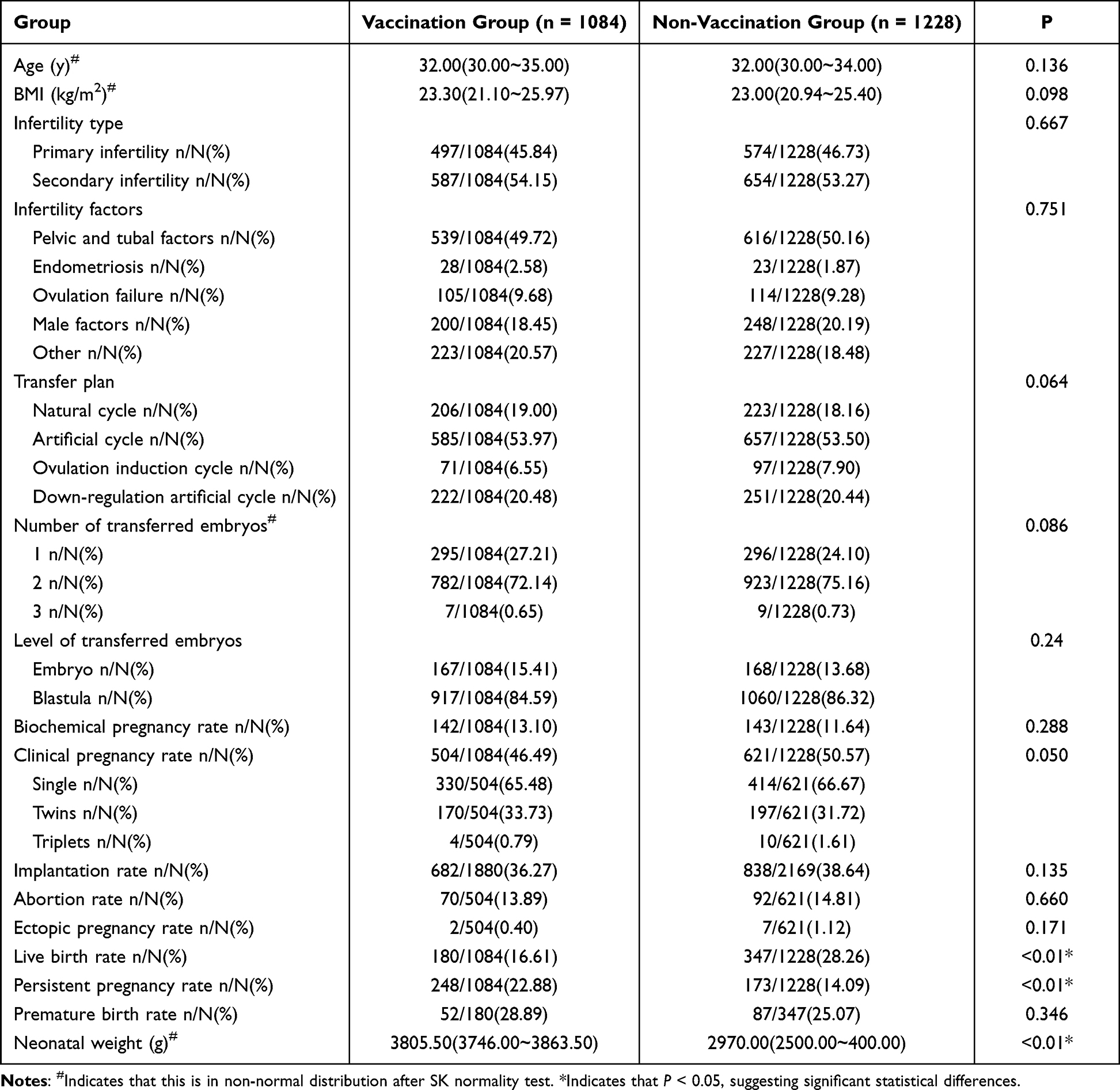 |
Table 1 Comparison of General Characteristics and Pregnancy Outcomes in Vaccinated and Non-Vaccinated Women Who Underwent FET |
Pregnancy Outcomes in the Vaccination Groups Receiving a Different Number of Doses
When we analyzed the general characteristics of patients in groups with different number of doses, we found that there were no significant differences in age, BMI, infertility type, transfer plan, and the number of transferred embryos among the one-dose group, the two-dose group, and the three-dose group, but there were statistically significant differences in the level of transferred embryos among the three groups. Comparison of pregnancy outcomes among the three groups showed no significant differences in the biochemical pregnancy rate, clinical pregnancy rate, embryo implantation rate, abortion rate, ectopic pregnancy rate, and neonatal weight among the three groups. However, the live birth rate in the one-dose group was significantly higher than that in the two-dose group, and the three-dose group, and the persistent pregnancy rate and the premature birth rate in the three-dose group were significantly higher than those in the one-dose group and the two-dose group, with statistically significant differences. Details are given in Table 2.
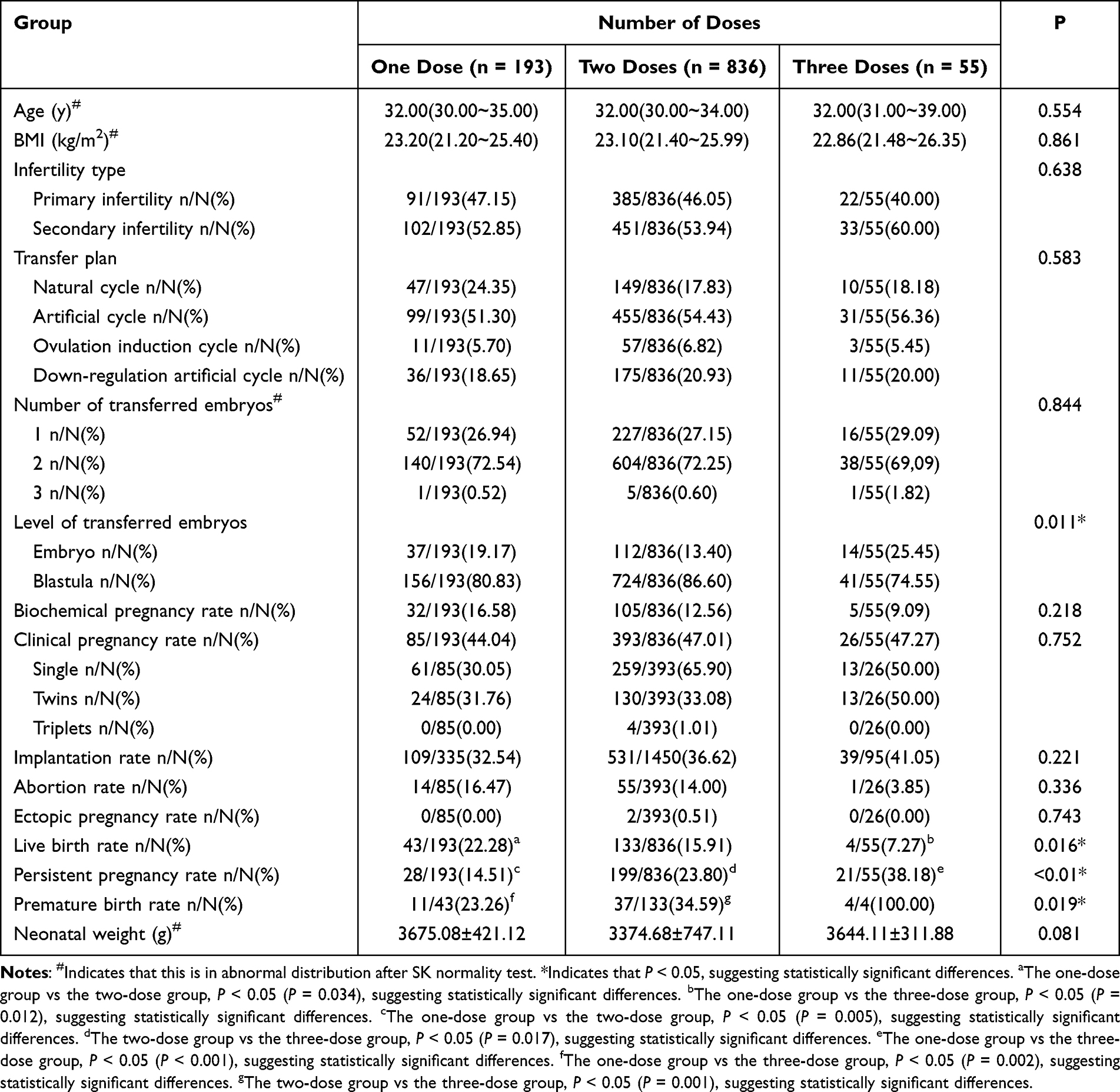 |
Table 2 Comparison of General Characteristics and Pregnancy Outcomes in FET Patients with Different Number of COVID-19 Vaccination Doses |
Pregnancy Outcomes in the Vaccination Groups with Different Intervals Between Last Vaccination Dose and FET
Comparison of general clinical characteristics of patients with different vaccination intervals indicated that there were no significant differences in the age, BMI, infertility type, transfer plan, the level of transferred embryos, and the number of transferred embryos among the group with interval ≤ 1 month, the group with interval of 1–2 months, and the group with interval ≥ 2 months. Analysis of the pregnancy outcomes of the three groups showed that there were no significant differences in the biochemical pregnancy rate, clinical pregnancy rate, embryo implantation rate, abortion rate, and neonatal weight among the three groups, but there were significant differences in the ectopic pregnancy rate. In addition, the live birth rate in the group with interval ≤ 1 month was significantly higher than that in the group with interval of 1–2 months, and the group with interval ≥ 2 months. The premature birth rate and persistent pregnancy rate were significantly lower than those in the group with interval in 1–2 months, and the group with interval ≥ 2 months. Details are given in Table 3.
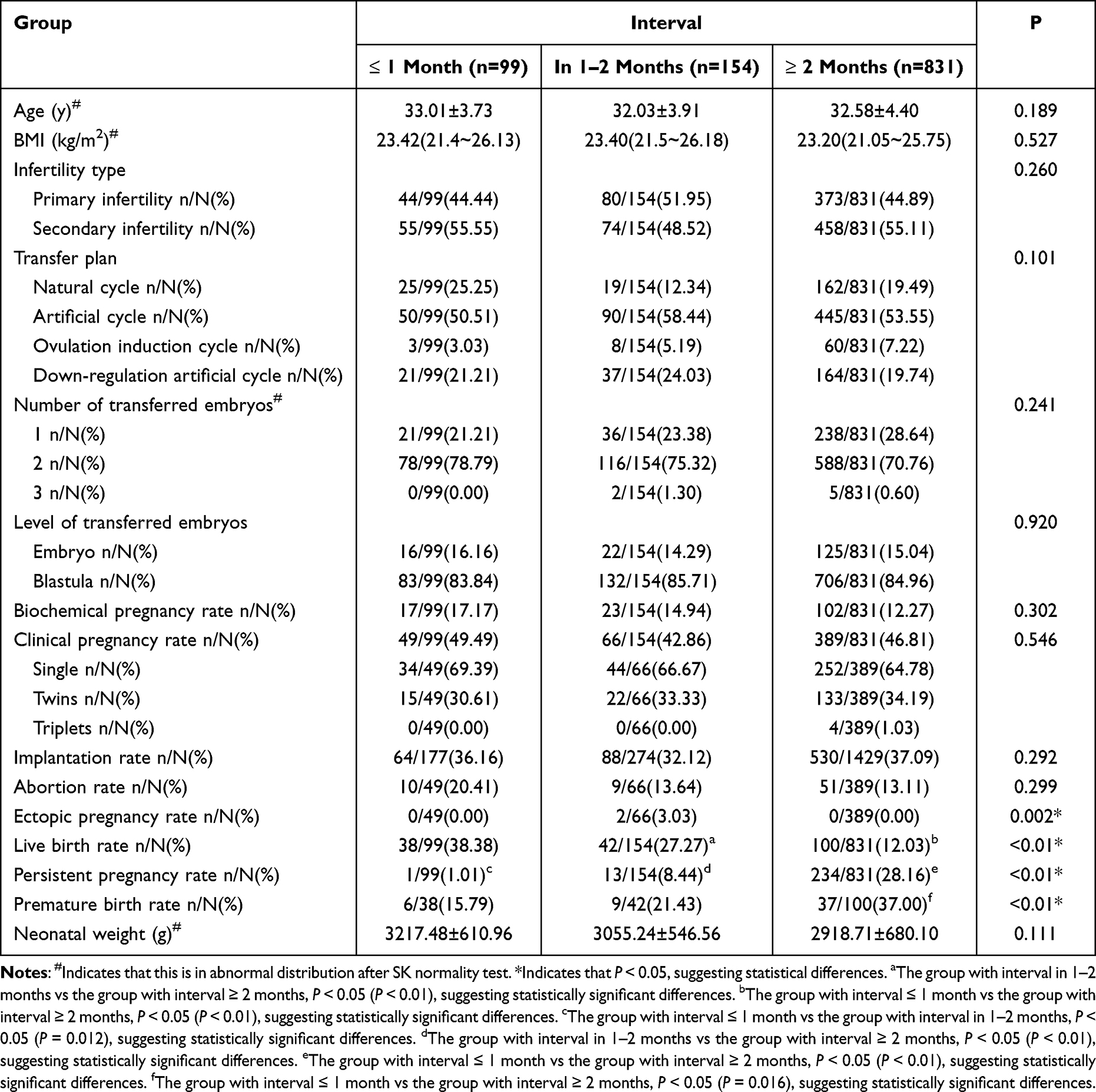 |
Table 3 Comparison of General Characteristics and Pregnancy Outcomes in Patients with Different Intervals Between the Last Dose of SARS-CoV-2 Inactivated Vaccine and the FET |
Discussion
This study is one of the few on the effects of SARS-CoV-2 inactivated vaccine on FET pregnancy outcomes. Our findings indicate that the vaccination status of patients before FET, the number of doses, and the intervals between last vaccine dose and FET had no impact on the clinical pregnancy rate, biochemical pregnancy rate, and abortion rate. This provides evidence support for the safety of vaccination for use in patients with infertility planning to undergo FET.
SARS-CoV-2 belongs to the subgenus Beta Coronavirus of Coronaviridae,29 with angiotensin converting enzyme 2 (ACE2) as the main receptor, while transmembrane protease serine 2 (TMPRSS2) is a serine protease activating the SARS-CoV-2 S protein.30 Therefore, ACE2 and TMPRSS2 are the portals through which viruses enter human cells and attack the immune system. Organs where ACE2 is positively expressed are considered to be at high risk for infection. There have been reports that ACE2 is widely expressed in syncytiotrophoblasts, cytotrophoblasts, and other cells in the ovary, uterus, and villi.31,32 This regulates follicular development and ovulation, and corpus luteum angiogenesis and degeneration by regulating angiotensin II (Ang II) and Ang-(1-7),33,34 so as to affect the growth of endometrium, thereby interfering with embryo implantation or leading to abortion.35
In a retrospective cohort study in Israel, 121 patients with infertility infected with SARS-CoV-2 were compared with 121 non-vaccinated/uninfected patients during the in vitro fertilization (IVF) cycle; the results showed that there were no significant differences in the mature oocyte rate, fertility rate, freezing per cycle, and clinical pregnancy rate, but the number of oocytes in those infected for more than 180 days significantly decreased.36 D6 embryos were relatively susceptible to SARS-CoV-2, and were at the highest potential risk of being infected with it during the peri-implantation embryo development.37 In a study on the effect of SARS-CoV-2 on male reproductive ability, spermatogonia, sustentacular cells, and mesenchymal cells in the testes had the highest concentration of ACE2 receptors. Spermatogonia with positive ACE2 showed significantly decreased functions in spermatoblast differentiation, spermic egg recognition, acrosomal reaction and other aspects,38 while the sperm count and mobility were significantly reduced in terms of semen parameters.39 These changes might be related to the rise of body temperature caused by COVID-19.40 Opinions differ on the presence of SARS-CoV-2 in semen, with most scholars holding negative views,41–44 but, nevertheless, some scholars have detected the genetic materials of SARS-CoV-2 in semen.40
It is speculated that SARS-CoV-2 may have adverse effects on pregnancy outcomes of women, given its effects on reproductive cells. There are reports of increase in the risk of maternal and neonatal mortality and morbidity due to SARS-CoV-2 infection.39 Compared to normal pregnant women, those with COVID-19 are at significantly higher risk of hospitalization, ICU occupancy, invasive ventilation support and premature birth,18,45,46 but also have a small risk of vertical mother-to-infant transmission.47–50 According to a comparison of 101 pregnant women who were COVID-19 positive with 938 non-infected pregnant women, infection with SARS-CoV-2 during the third trimester of pregnancy was an important risk factor for emergency cesarean delivery, premature rupture of membranes, premature birth, and low neonatal APGAR score.51 Factors such as inflammation, platelet activation, and endothelial dysfunction caused by SARS-CoV-2 infection may be the leading causes of fetal growth retardation and adverse pregnancy outcomes.52 However, other authors have endorsed a different view, finding that the risk of abortion does not increase in women infected with SARS-CoV-2.53
Safety and effectiveness of vaccines for use in pregnant and lactating women have been given precedence in the global COVID-19 vaccination program. The vaccination rate among patients with the desire to undergo ART to stimulate fertility is low due to limited evidence for the safety of COVID-19 vaccine on ovarian functions and assisted reproduction outcomes. In a small-size cohort study, Bentov et al compared hormonal levels of serum and follicular fluid in a COVID-19 infected group, a COVID-19 vaccinated group, and a control group, and found that the COVID-19 vaccine did not damage ovarian functions.54 In a retrospective cohort study that compared the natural pregnancy loss rate after six weeks of pregnancy, it was found that SARS-CoV-2 mRNA vaccination before or during pregnancy did not increase the natural pregnancy loss rate.55 SARS-CoV-2 mRNA vaccination during pregnancy was not associated with the increased complications of pregnancy or delivery, proving that the vaccine was safe and effective during pregnancy.13,53
In this study, we analyzed details of 1084 FET patients who received the SARS-CoV-2 inactivated vaccine, and 1228 FET patients who were not vaccinated against SARS-CoV-2. Our results showed that there were no significant differences between the two groups in pregnancy outcomes such as clinical pregnancy rate, biochemical pregnancy rate, abortion rate, and premature birth rate, which further proved the safety of SARS-CoV-2 inactivated vaccine. Although the neonatal weight in the vaccination group was significantly higher than that in the non-vaccination group, we did not investigate twin fetal weight and single fetal weight in this study. Hence, examining the effect of SARS-CoV-2 inactivated vaccine on neonatal weight needs additional analysis with further sub-grouping of patients.
At present, there is no evidence about whether the number of doses of SARS-CoV-2 inactivated vaccine has any effect on the pregnancy outcomes of FET patients. In this study, we analyzed patients who received one dose, two doses, and three doses of SARS-CoV-2 inactivated vaccines, and the results showed that despite the significant difference in the level of embryo transfer, there were no statistical differences in the pregnancy outcomes, such as implantation rate, clinical pregnancy rate, biochemical pregnancy rate, ectopic pregnancy rate, abortion rate, and neonatal weight, among the three groups. This suggests that the number of doses of SARS-CoV-2 inactivated vaccines had no effect on the clinical pregnancy outcomes of patients who underwent FET. However, it is important to note that there were significant differences in the ectopic pregnancy rate between groups. Furthermore, the live birth rate in the group with an interval of ≤ 1 month was significantly higher than that in the groups with intervals of 1–2 months and ≥ 2 months. Additionally, the rates of premature birth and persistent pregnancy were significantly lower in the group with an interval of ≤ 1 month compared to the groups with intervals of 1–2 months and ≥ 2 months.
There is no unanimous answer to the question of what is the optimal interval between vaccination and in vitro fertilization and embryo transfer (IVF-ET) for patients undergoing ART to stimulate fertility. According to the European Society of Human Reproduction and Embryology (ESHRE), it is safe to undergo IVF-ET treatment two months after vaccination,56 while the American Society for Reproductive Medicine (ASRM) suggests avoidance of egg retrieval or transfer within three days before and after vaccination.57
Chinese experts opine that fertility may be enhanced one month after vaccination.6 Huang et al22 divided patients with infertility into three groups according to the interval between the use of inactivated vaccine and fertility enhancement [≤ 1 month (n = 37), 1–2 months (n = 42), ≥ 2 months (n = 71)]. There were no significant differences in laboratory indicators and pregnancy outcomes among the three groups. Comparing semen parameters, they found that SARS-CoV-2 vaccination had no negative effect on IVF semen parameters, such as semen volume, sperm density, total sperm count, forward movement rate, and total movement rate.58 In terms of the IVF cycle, the vaccination status of the infertile couples had no significant effects on the ovarian reserve,59 quality of oocytes,54 quality of embryos, and pregnancy outcomes,22,60 and the vaccine type, and the interval between complete vaccination and transfer had no significant effects on the clinical pregnancy rate.23
However, SARS-CoV-2 mRNA vaccination may reduce the quality embryo rate of IVF patients.21 In a study that compared 264 FET cycles of patients infected with SARS-CoV-2 or receiving SARS-CoV-2 mRNA vaccine with 287 FET cycles of the control group, there were no significant differences in the implantation rate, clinical pregnancy rate, and persistent pregnancy rate between the two groups.61 In our study, there were no statistically significant differences in the implantation rate, clinical pregnancy rate, biochemical pregnancy rate, abortion rate, and neonatal weight among the group with interval ≤ 1 month, the group with interval of 1–2 months, and the group with interval ≥ 2 months, which further confirmed that the interval between SARS-CoV-2 inactivated vaccine and FET had no significant effect on the clinical pregnancy rate. This finding was similar to the conclusions from other studies.23,61
In this study, the live birth rate and persistent pregnancy rate were significantly different regardless of the groups, and such difference in our findings represent a contradictory trend. The contrasting results could be considered as related to the transfer and follow-up time of enrolled patients; that is, during the study period, the high live birth rate of a group is bound to reduce the number of patients with persistent pregnancy. Significant differences in ectopic pregnancy rates and preterm birth rates were observed among groups with varying vaccination intervals or different numbers of vaccinations. However, due to the limited sample size, further confirmation through large-scale data is required. It is important to note that existing evidence has shown no increased risk of miscarriage or decreased rates of sustained pregnancy or live birth associated with the COVID-19 vaccine in women of childbearing age.28 In addition, the administration of the COVID-19 vaccine in women undergoing assisted reproductive procedures has shown no significant impact on various outcomes, including laboratory indicators and clinical pregnancy outcomes such as miscarriage, live birth, and ongoing pregnancy rates.62 However, it is important to note that the existing evidence is limited, and further extensive population-based studies are necessary to comprehensively assess the efficacy and safety of the vaccine in women preparing for pregnancy or during pregnancy.
The present study has a notable strength in its large sample size. Our results provide compelling evidence that SARS-CoV-2 inactivated vaccines do not exert a significant impact on clinical pregnancy rate, biochemical pregnancy rate, and abortion rate. These findings reinforce the safety and efficacy of these vaccines in women undergoing assisted reproduction. They also serve to instill reassurance among healthcare providers and patients regarding the use of these vaccines in this population. This study also has a few limitations. We only included the SARS-CoV-2 inactivated vaccine in this study, and other types of vaccines were not included. The follow-up time was short, making it difficult to predict the long-term effect of SARS-CoV-2 inactivated vaccines on newborns. Additionally, we did not include the effect of vaccination status of the male partner on pregnancy outcomes. Lastly, as there was no statistically significant difference in age between the two groups within each subgroup in this study, we did not investigate the effect of age on pregnancy outcomes. However, we agree that age is an important factor and warrants further investigation. Taken together, further investigations including different types of vaccines, with longer follow-up time, and considering other factors, such as age and vaccination status of male partners are needed.
Conclusion
Our study demonstrated that the vaccination status of patients before FET, the number of doses, and the intervals between last vaccine dose and FET had no impact on the clinical pregnancy rate, biochemical pregnancy rate, and abortion rate. These findings suggest that the SARS-CoV-2 inactivated vaccine was safe for use during pregnancy, offering evidence for guiding the vaccination of patients undergoing ART.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
I confirm that I have read the Editorial Policy pages. This study was conducted with approval from the Ethics Committee of Children’s Hospital of Shanxi and Women Health Center of Shanxi. The approval number is IRB-KYYN-2021-002. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
The Research Fund of Children’s Hospital of Shanxi and Women Health Center of Shanxi (No: 2021030). Scientific research project of Shanxi Provincial Health Commission (No:2023XG040).
Disclosure
The authors declare that they have no competing interests.
References
1. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomedica. 2020;91(1):157.
2. World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available from: https://covid19.who.int.
3. National Health Commission of the People’s Republic of China. COVID-19 vaccination status. Available from: http://www.nhc.gov.cn/.
4. Yao CL, Wei WL, Zhang JQ, et al. Traditional Chinese medicines against COVID-19: a global overview. World J Tradit Chin Med. 2022;8(3):279–313. doi:10.4103/2311-8571.353502
5. Li MX, Yang YY, Liu Y, et al. Progress of traditional Chinese medicine treating COVID-19. World J Tradit Chin Med. 2021;7:167–183.
6. Expert Group for Beijing Human Assisted Reproductive Technology Center For Quality Control and Improvement. COVID-19 vaccination strategy for planning pregnancy and assisted reproductive technology treatment: expert recommendations. Chin J Reprod Contracep. 2021;41:296–299. In Chinese.
7. European Society of Human Reproduction and Embryology (ESHRE). COVID-19 vaccination and assisted reproduction [EB/OL]; 2021. Available from: https://www.eshre.eu/Home/COVID19WG.
8. Jara A, Undurraga EA, Gonzalez C, et al. Effectiveness of an inactivated SARS-CoV-2 vaccine in Chile. N Engl J Med. 2021;385(10):875–884. doi:10.1056/NEJMoa2107715
9. Bureau of Disease Control Prevention, National Health Commission of the People’s Republic of China. Technical guidelines for new coronavirus vaccination (First Edition). Chin J Viral Dis. 2021;11:161–162. In Chinese.
10. Moderna. Frequently asked questions: what is known about the safety of the vaccine for special populations (Children, Pregnant Women, Elderly People)? Available from: https://www.modernatx.com/covid19vaccine-eua/providers/faq#patientvaccination.
11. Rubin R. Pregnant people’s paradox-excluded from vaccine trials despite having a higher risk of COVID-19 complications. JAMA. 2021;325(11):1027–1028. doi:10.1001/jama.2021.2264
12. National Center for Immunization & Respiratory Diseases. COVID-19 vaccine safety update Advisory Committee on Immunization Practices (ACIP); 2021.
13. Theiler RN, Wick M, Mehta R, et al. Pregnancy and birth outcomes after SARS-CoV-2 vaccination in pregnancy. Am J Obstet Gynecol MFM. 2021;3(6):100467. doi:10.1016/j.ajogmf.2021.100467
14. Barreta MH, Gasperin BG, Ferreira R, et al. The components of the angiotensin-(1-7) system are differentially expressed during follicular wave in cattle. J Renin Angiotensin Aldosterone Syst. 2013;16(2):275–283. doi:10.1177/1470320313491996
15. Reis FM, Bouissou DR, Pereira VM, Camargos AF, Dos Reis AM, Santos A. Angiotensin-(1-7), its receptor Mas, and the angiotensin-converting enzyme type 2 are expressed in the human ovary. Fertil Steril. 2011;95(1):176–181. doi:10.1016/j.fertnstert.2010.06.060
16. Bikdeli B, Madhavan MV, Jimenez D, et al. COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up. J Am Coll Cardiol. 2020;75(23):2950–2973. doi:10.1016/j.jacc.2020.04.031
17. Connors JM, Levy JH. Thromboinflflammation and the hypercoagulability of COVID-19 [published online ahead of print, 2020 Apr 17]. J Thromb Haemost. 2020. doi:10.1111/jth.14849
18. Allotey J, Stallings E, Bonet M, et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ. 2020;370:m3320. doi:10.1136/bmj.m3320
19. Chmielewska B, Barratt I, Townsend R, et al. Effects of the COVID-19 pandemic on maternal and perinatal outcomes: a systematic review and meta-analysis. Lancet Glob Health. 2021;9(6):e759–e772. doi:10.1016/S2214-109X(21)00079-6
20. Wei SQ, Bilodeau-Bertrand M, Liu S, Auger N. The impact of COVID-19 on pregnancy outcomes: a systematic review and meta-analysis. CMAJ. 2021;193(16):E540–E548. doi:10.1503/cmaj.202604
21. Orvieto R, Noach-Hirsh M, Segev-Zahav A, et al. Does mRNA SARS-CoV-2 vaccine influence patients’ performance during IVF-ET cycle? Reprod Biol Endocrinol. 2021;19(1):69. doi:10.1186/s12958-021-00757-6
22. Huang J, Xia L, Lin J, et al. No effect of inactivated SARS-CoV-2 vaccination on in vitro fertilization outcomes: a propensity score-matched study. J Inflamm Res. 2022;15:839–849. doi:10.2147/JIR.S347729
23. Dong M, Wu S, Zhang X, et A. Effects of COVID-19 vaccination status, vaccine type, and vaccination interval on IVF pregnancy outcomes in infertile couples. J Assist Reprod Genet. 2022;39(8):1849–1859. doi:10.1007/s10815-022-02543-8
24. Wu Y, Cao M, Lin Y, et al. Inactivated COVID-19 vaccination does not affect in vitro fertilization outcomes in women. Hum Reprod. 2022;37(9):2054–2062. doi:10.1093/humrep/deac160
25. Jacobs E, Summers K, Sparks A, Mejia R. Fresh embryo transfer cycle characteristics and outcomes following in vitro fertilization via intracytoplasmic sperm injection among patients with and without COVID-19 vaccination. JAMA Netw Open. 2022;5(4):e228625. doi:10.1001/jamanetworkopen.2022.8625
26. Li C, He YC, Xu JJ, et A. Perinatal outcomes of neonates born from different endometrial preparation protocols after frozen embryo transfer: a retrospective cohort study. BMC Pregnancy Childbirth. 2021;21(1):341. doi:10.1186/s12884-021-03791-9
27. Cao M, Wu Y, Lin Y, et al. Inactivated Covid-19 vaccine did not undermine live birth and neonatal outcomes of women with frozen-thawed embryo transfer. Hum Reprod. 2022;37(12):2942–2951. doi:10.1093/humrep/deac220
28. Rimmer MP, Teh JJ, Mackenzie SC, Al Wattar BH. The risk of miscarriage following COVID-19 vaccination: a systematic review and meta-analysis. Hum Reprod. 2023;38(5):840–852. doi:10.1093/humrep/dead036
29. International Committee on Taxonomy of Viruses (ICTV) [Internet]; 2021. Available from: https://ictv.global/taxonomy/.
30. Hoffmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181(2):271–80.e8. doi:10.1016/j.cell.2020.02.052
31. Pringle KG, Tadros MA, Callister RJ, Lumbers ER. The expression and localization of the human placental prorenin/renin-angiotensin system throughout pregnancy: roles in trophoblast invasion and angiogenesis? Placenta. 2011;32(12):956–962. doi:10.1016/j.placenta.2011.09.020
32. Li M, Chen L, Zhang J, et al. The SARS-CoV-2 receptor ACE2 expression of maternal-fetal interface and fetal organs by single-cell transcriptome study. PLoS One. 2020;15(4):e0230295. doi:10.1371/journal.pone.0230295
33. Pereira VM, Reis FM, Santos RAS, et al. Gonadotropin stimulation increases the expression of angiotensin-(1--7) and MAS receptor in the rat ovary. Reprod Sci. 2009;16(12):1165–1174. doi:10.1177/1933719109343309
34. Jing Y, Run-Qian L, Hao-Ran W, et al. Potential influence of COVID-19/ACE2 on the female reproductive system. Mol Hum Reprod. 2020;26:367–373. doi:10.1093/molehr/gaaa030
35. Li R, Yin T, Fang F, et al. Potential risks of SARS-CoV-2 infection on reproductive health. Reprod Biomed Online. 2020;41(1):89–95. doi:10.1016/j.rbmo.2020.04.018
36. Youngster M, Avraham S, Yaakov O, et al. IVF under COVID-19: treatment outcomes of fresh ART cycles. Hum Reprod. 2022;37(5):947–953. doi:10.1093/humrep/deac043
37. Chen W, Yuan P, Yang M, et al. SARS-CoV-2 entry factors: ACE2 and TMPRSS2 are expressed in peri-implantation embryos and the maternal-fetal interface. Engineering. 2020;6(10):1162–1169. doi:10.1016/j.eng.2020.07.013
38. Wang Z, Xu X. scRNA-seq profiling of human testes reveals the presence of the ACE2 receptor, a target for SARSCoV-2 infection in spermatogonia, Leydig and Sertoli cells. Cells. 2020;9(4):920. doi:10.3390/cells9040920
39. Holtmann N, Edimiris P, Andree M, et al. Assessment of SARS-CoV-2 in human semen-A cohort study. Fertil Steril. 2020;114(2):233–238. doi:10.1016/j.fertnstert.2020.05.028
40. Arneiro Gomes PR, Rodrigues da Rocha MD, da Rocha Coelho FA, et al. Alterations of the male and female reproductive systems induced by COVID-19. Wien Klin Wochenschr. 2021;133(17–18):966–972. doi:10.1007/s00508-021-01875-2
41. Omolaoye TS, Adeniji AA, Maya WDC, du Plessis SS. SARS-COV-2 (COVID-19) and male fertility: where are we? Reprod Toxicol. 2021;99:65–70. doi:10.1016/j.reprotox.2020.11.012
42. Song C, Wang Y, Li W, et al. Absence of 2019 novel coronavirus in semen and testes of COVID-19 patients. Biol Reprod. 2020;103(1):4–6. doi:10.1093/biolre/ioaa050
43. Paoli D, Pallotti F, Colangelo S, et al. Study of SARSCoV-2 in semen and urine samples of a volunteer with positive naso-pharyngeal swab. J Endocrinol Invest. 2020;43(12):1819–1822. doi:10.1007/s40618-020-01261-1
44. Ning J, Li W, Ruan Y, Cheng F, et al. Effects of 2019 novel coronavirus on male reproductive system: a retrospective study. Preprints; 2020.
45. Galang RR, Newton SM, Woodworth KR, et al. Risk factors for illness severity among pregnant women with confirmed SARS-CoV-2 infection—Surveillance for Emerging Threats to Mothers and Babies Network, 22 state, local, and territorial health departments, March 29, 2020-March 5, 2021. Clin Infect Dis. 2021;73(Supplement_1):S17–S23. doi:10.1093/cid/ciab432
46. Mullins E, Hudak ML, Banerjee J, et al. Pregnancy and neonatal outcomes of COVID −19: coreporting of common outcomes from PAN-COVID and AAP-SONPM registries. Ultrasound Obs Gynecol. 2021;57(4):573–581. doi:10.1002/uog.23619
47. Dumitriu D, Emeruwa UN, Hanft E, et al. Outcomes of neonates born to mothers with severe acute respiratory syndrome Coronavirus 2 infection at a large medical center in New York City. JAMA Pediatr. 2021;175(2):157–167. doi:10.1001/jamapediatrics.2020.4298
48. Gross R, Conzelmann C, Muller JA, et al. Detection of SARS-CoV-2 in human breastmilk. Lancet. 2020;395(10239):1757–1758. doi:10.1016/S0140-6736(20)31181-8
49. Kotlyar AM, Grechukhina O, Chen A, et al. Vertical transmission of coronavirus disease 2019: a systematic review and meta-analysis. Am J Obstet Gynecol. 2021;224(1):35–53. doi:10.1016/j.ajog.2020.07.049
50. Centeno-Tablante E, Medina-Rivera M, Finkelstein JL, et al. Transmission of SARS-CoV-2 through breast milk and breastfeeding: a living systematic review. Ann N Y Acad Sci. 2021;1484(1):32–54. doi:10.1111/nyas.14477
51. Timircan M, Bratosin F, Vidican I, et al. Exploring pregnancy outcomes associated with SARS-CoV-2 infection. Medicina. 2021;57(8):796. doi:10.3390/medicina57080796
52. Kazemi SN, Hajikhani B, Didar H, et al. COVID-19 and cause of pregnancy loss during the pandemic: a systematic review. PLoS One. 2021;16(8):e0255994. doi:10.1371/journal.pone.0255994
53. Di Mascio D, Buca D, Berghella V, et al. Counseling in maternal-fetal medicine: SARS-CoV-2 infection in pregnancy. Ultrasound Obstet Gynecol. 2021;57(5):687–697. doi:10.1002/uog.23628
54. Bentov Y, Beharier O, Moav-Zafrir A, et al. Ovarian follicular function is not altered by SARS-CoV-2 infection or BNT162b2 mRNA COVID-19 vaccination. Hum Reprod. 2021;36(9):2506–2513. doi:10.1093/humrep/deab182
55. Zauche LH, Wallace B, Smoots AN, et al.; CDC v-safe Covid-19 Pregnancy Registry Team. Receipt of mRNA Covid-19 vaccines and risk of spontaneous abortion. N Engl J Med. 2021;385(16):1533–1535. doi:10.1056/NEJMc2113891
56. ESHRE COVID-19 Working Group. ESHRE statement on COVID-19 vaccination and medically assisted reproduction. Available from: https://www.eshre.eu/Europe/Position-tatements/COVID19/vaccination.
57. Coronavirus/COVID-19 Task Force of the American Society for Reproductive Medicine. ASRM patient management and clinical recommendations during the (coronavirus COVID-19) pandemic: update no. 13—variants, vaccines, and vaccination; February 22, 2021. Available from: https://www.asrm.org/globalassets/asrm/asrm-content/news-and-publications/covid-19/covidtaskforceupdate13.pdf.
58. Barda S, Laskov I, Grisaru D, et al. The impact of COVID-19 vaccine on sperm quality. Int J Gynaecol Obstet. 2022;158(1):116–120. doi:10.1002/ijgo.14135
59. Odeh-Natour R, Shapira M, Estrada D, et al. Does mRNA SARS-CoV-2 vaccine in the follicular fluid impact follicle and oocyte performance in IVF treatments? Am J Reprod Immunol. 2022;87(5):e13530. doi:10.1111/aji.13530
60. Aharon D, Lederman M, Ghofranian A, et al. In vitro fertilization and early pregnancy outcomes after coronavirus disease 2019 (COVID-19) vaccination. Obstet Gynecol. 2022;139(4):490–497. doi:10.1097/AOG.0000000000004713
61. Aizer A, Noach-Hirsh M, Dratviman-Storobinsky O, et al. The effect of coronavirus disease 2019 immunity on frozen-thawed embryo transfer cycles outcome. Fertil Steril. 2022;117(5):974–979. doi:10.1016/j.fertnstert.2022.01.009
62. Huang J, Fang Z, Liu Y, et al. Effect of female coronavirus disease 2019 vaccination on assisted reproductive outcomes: a systematic review and meta-analysis. Fertil Steril. 2023;119(5):772–783. doi:10.1016/j.fertnstert.2023.01.024
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.