Back to Journals » Therapeutics and Clinical Risk Management » Volume 17
Effects of Scleral Contact Lenses for Keratoconus Management on Visual Quality and Intraocular Pressure
Authors Formisano M ![]() , Franzone F
, Franzone F ![]() , Alisi L
, Alisi L ![]() , Pistella S, Spadea L
, Pistella S, Spadea L ![]()
Received 26 November 2020
Accepted for publication 15 January 2021
Published 25 January 2021 Volume 2021:17 Pages 79—85
DOI https://doi.org/10.2147/TCRM.S293425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Martina Formisano, Federica Franzone, Ludovico Alisi, Santino Pistella, Leopoldo Spadea
Eye Clinic, Department of Sense Organs, University of Rome Sapienza, Policlinico Umberto I, Rome, Italy
Correspondence: Leopoldo Spadea
Eye Clinic, Policlinico Umberto 1, “Sapienza” University of Rome, Via Benozzo Gozzoli 34, Rome 00142, Italy
Tel +039 06 519 3220
Fax +39 06 8865 7818
Email [email protected]
Purpose: To evaluate the visual acuity level achieved by scleral contact lens (CL) fitting in patients affected by keratoconus and to evaluate possible intraocular pressure (IOP) changes during the scleral CL wear using a transpalpebral tonometer.
Methods: In a prospective case series a comparison was made between visual acuity obtained with glasses, RGP and 16.8mm diameter scleral CL in 30 consecutive patients affected by keratoconus. IOP was tested during scleral CL wear by transpalpebral Diaton Tonometer (DT) and also by Goldmann Applanation Tonometer (GAT) before and after scleral CL wear.
Results: The mean logMAR visual acuity improved from 0.2± 0.25SD with glasses and 0.1± 0.02SD with RGP, to − 0.002± 0.041SD when using the scleral CL (p< 0.05). The mean IOP value before scleral CL wear was 12.93mmHg± 2.20SD when measured with GAT and 7.85mmHg± 2.27SD when measured with DT. During scleral CL wear, IOP was assessed through DT, with a mean value of 8.86mmHg± 2.36SD; values were stable after 8 hours of scleral CL use. Immediately after scleral CL removal, the mean IOP measured with GAT was 12.85mmHg ± 2.40SD and the mean IOP measured with DT was 7.66mmHg± 1.88SD. Therefore, during scleral CL wear, it was evidenced a small but statistically significant increase of the mean IOP value (1.01mmHg; p< 0.01), with a reversion to values prior to application when scleral CL was removed.
Conclusion: Scleral CLs remarkably improved visual acuity in keratoconus patients when compared to glasses or RGP contact lenses. Even if it was evidenced a small increase of the mean IOP value during their wear, it may not be significant in otherwise healthy eyes. Statistical analysis demonstrated good agreement between GAT and DT but their numerical values presented a constant gap, that should be taken into account when there is a need to relate the DT values to the reference ones.
Keywords: keratoconus, higher-order aberrations, IOP, scleral contact lens
Introduction
Keratoconus is a non-inflammatory corneal disease that causes a gradual and progressive corneal ectasia. The disease typically involves both eyes.1 In keratoconus, all cornea layers, particularly the stroma, are characterized by a disruption in the arrangement of collagen fibrils, alterations in proteoglycans expression, and unstable interconnectivity of collagen lamellae, with varying degrees of severity.2 Changes in stromal biomechanics result in paracentral steepening of the cornea, apical thinning, and conic shaping of the cornea.3 The displaced optic zone leads to irregular astigmatism, significant coma aberration, and a remarkable reduction in the quality of vision.4
Traditional sphero-cylindrical spectacles do not provide significant visual improvement in keratoconus patients, due to higher-order aberrations (HOAs) typical of the keratoconic cornea. Consequently, when a high number of HOAs appear in keratoconus patients, rigid gas permeable (RGP; corneal, corneoscleral, and scleral) contact lenses are suggested as soon as they create a more regular refractive surface.4 However, corneal RGP lenses may not be suitable for advanced corneal irregularity and can be associated with corneal scarring at the point of contact between the lens and cornea.5
Piggyback contact lenses, intended as rigid gas-permeable lenses that are fitted over soft contact lenses, are suggested for people who cannot tolerate rigid gas permeable lenses, but they are more expensive and have complex maintenance and storage.6
Scleral lenses are large-diameter rigid gas-permeable lenses, which vault over the cornea and limbal area and rest on the conjunctival tissue overlying the sclera, which provides a major comfort during their use. The mid-peripheral and peripheral parts of the lenses are customizable to improve stabilization. Even if scleral CLs share the same composition as RGP contact lenses, the entrapment of a thick layer of fluid beneath the scleral contact lens alters the relationship between the cornea and the lens, and also provide relief in case of dry eye.7
Scleral CLs can have different diameters but generally, inferior diameter scleral CLs (previously referred to as mini-scleral CL) have easier handling8 and are more proximal to structures involved in the aqueous humour outflow than larger diameter lenses.6
The indication for surgery is usually due to contact lenses intolerance or a limitation of the best spectacles or contact lenses-corrected visual acuity.9 Nonetheless, high levels of aberrations may not be eliminated with surgery, and have been reported in keratoconus patients treated with intrastromal corneal ring segments, cross-linking, radial keratotomy and lamellar or penetrating keratoplasty.10,11 Contact lenses also may be needed after surgical intervention for keratoconus to address the HOAs still present.
In this study, we evaluated the effects of a 16.8mm diameter scleral CL wear in keratoconus eyes in terms of visual acuity and intraocular pressure, the latter measured through a transpalpebral tonometer.
Methods
The present study was designed as a prospective case series. The study was approved by the ethical board of the Sapienza University of Rome, Umberto I Hospital, and was conducted in accordance with the tenets of the Declaration of Helsinki. Written informed consent was obtained by all the patients. The patients attended a dedicated keratoconus department in our university hospital (Policlinico Umberto I, Rome) for 1-year (from June 1st, 2018 to June 1st, 2019). The study included 60 eyes of 30 consecutive patients (9 females and 21 males) with a mean age of 38.4±11.8 years (range 26–62ys). All the patients were affected by different grades of keratoconus in both eyes and they were visually unsatisfied after correction with traditional spectacles or corneal RGP (Table 1). We classified keratoconus using Krumeich classification: keratometric measurements <48 D were graded as “stage 1” keratoconus, measurements <53D were graded as “stage 2” keratoconus, measurements >53 D were classed as “stage 3” keratoconus, and measurements >55D were graded as the ultimate stage, “stage 4”.12 Subjects were free of any systemic or concomitant ocular disease. They were not known as being at risk for glaucoma and had no familial history for this pathology, and they had no previous eye surgeries. Subjects who were contact lens wearers were instructed to stop wearing contact lens at least ten days before the evaluation day. Objective and subjective refraction was conducted with trial frame lenses under standardized room and chart illumination conditions by one of the authors (MF). The distance corrected visual acuity (DCVA) was measured using an ETDRS chart and given as a logarithm of minutes of arc resolution (logMAR). Baseline findings for anterior central and posterior corneal curvature, corneal pachymetry, iridocorneal angle, as well as anterior chamber depth and volume, using different maps were taken with Precisio 2 tomographer (iVIS Technologies, Taranto, Italy). IOP values before scleral CL wear were assessed by both GAT (Haag-Streit AT900, USA) and DT (BICOM Inc, Long Beach, NY, USA), to have comparable measurements before and after the contact lenses wear.13
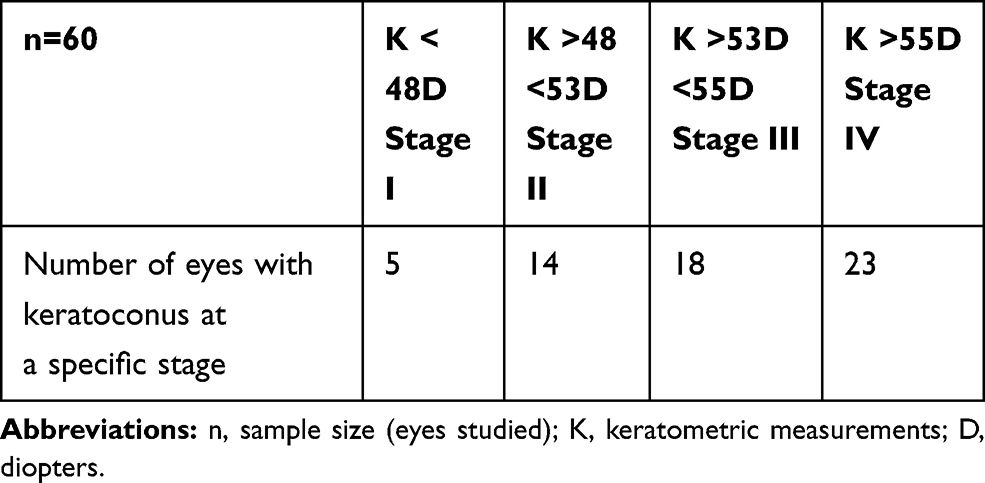 |
Table 1 Eyes Divided in 4 Groups Based on Krumeich Classification |
Then, a customized scleral contact lens (Medlac 16.8mm diameter; MedLac, Avellino, Italy) was prescribed to the 30 enrolled subjects. These Medlac lenses were chosen because of their ease of use given by their intermediate diameter, which is essential for patients requiring daily usage. Moreover, these lenses allowed us to maintain a safety distance of 2mm between the corneal limbus and the lens landing zone, to avoid a possible compression of the angle structures.
Patients with a corneal diameter greater than 12.30mm or less than 11.80mm have been excluded since the manufacturer indicates the 16.80mm diameter suitable for medium-sized horizontal visible iris diameter (HIVD). The 16.8mm overall diameter scleral CL not fenestrated were used for this study made by Tisilfocon A, with DK of 180, and a flexure modulus of 1341Mpa. Lenses were manufactured with 220μm center thickness. The landing zone angle was assessed through AS-OCT. It ranged from 48º to 52º. The landing zone angle was established to avoid edge compression or impeachment in the conjunctiva tissue and to avoid excessive edge lift to the sclera portion. An experienced examiner (BS) performed all fitting following the manufacturer’s guide. Subjects with a difference between HIVD and vertical visible iris diameter (VVID) of more than 0.5mm, were fitted with scleral LC Conica Evolution design, with an elliptical-shaped corneal chamber; allowing to control the distance between the lens landing and the limbus in each sector. Scleral CLs were inserted with preservative-free saline and sodium fluorescein and then assessed using a slit-lamp biomicroscope. The relationship between the central lens and the cornea was evaluated, checking that the lens was without air bubbles. Lenses with smaller or larger back optic zone radii of curvature were tested progressively until the highest point of the cornea (apex) showed a light feather apical clearance (Figure 1). Once centering was achieved, the settling of the lens on the conjunctiva was observed to avoid over-pressure on the conjunctival vessels, a settling of the scleral portion on the conjunctiva was considered normal within a range of 100–150μm, evaluated by the anterior segment module of Spectralis OCT (Heidelberg engineering Inc, USA). This procedure was followed by a final slit-lamp examination to assess ocular health (Figure 2). Lissamine Green stain was used to check any signs of conjunctival distress during lens wear as well as after the lens removal.
 |
Figure 1 Slit-lamp examination of a patient’s eye fitting a scleral lens (Medlac 16.8mm diameter). It’s visible a thin tear layer between the posterior lens surface and the corneal apex. |
 |
Figure 2 Scleral lenses were inserted with preservative-free saline and sodium fluorescein, which helped the analysis of the tear allocation under the lens. The colored tear layer is homogeneous and air-bubbles free. |
The intraocular pressure (IOP) during scleral CL wear was evaluated through the DT at baseline and 8 hours after. Comfort and visual acuity with the scleral CL were documented. The scleral lenses were then carefully removed by using a small plunger to avoid inducing excessive pressure on the ocular surface during the process.14 Then, just after lens removal, we measured again the IOP with both GAT and DT.
The Diaton tonometer has a U-shaped tip designed to adapt to the eyelid and obtain IOP measurements through a freely moving rod inside the tonometer, which falls freely onto the elastic surface of the eyeball through the eyelid. Thus, the instrument measures the resistance of the eyelid, the conjunctiva, and sclera through the backward acceleration after interaction with the sclera via the eyelid and converts it to an estimate of intraocular pressure. The Diaton automatically displays the average measurement of up to 6 readings. The measurements in our study were taken with the examiner and the patient facing the same direction. During the DT, the patients were sitting with their heads reclined, looking at an index finger to obtain primary gaze fixation. The upper eyelid was retracted so that the lid margin was 1mm above the superior limbus and the tonometer’s tip was placed perpendicularly onto the tarsal plate, at about 2mm behind the superior lid margin, careful to avoid placing the tonometer above the scleral lens when applied. When the tip of the tonometer touched the eyelid correctly, the measurement was noted automatically. The tonometer is tilted back from vertical to reset the scale for each of the two following measurements after which the average of the three was displayed digitally on the screen. In this study, all DT measures were made by the same experienced observer to reduce the variability in the measurement process.15,16
Statistical analysis with Student’s t-test for paired data was performed to investigate the effect on IOP of scleral CL repeating the measurement before, during and after the application. Bland-Altman method was repeatedly employed to evaluate the level of agreement between DT and GAT before scleral CL wearing, and after their removal (95% limits of agreement was calculated as mean difference±1.96SD). All analyses were performed averaging measurement obtained in both eyes.
Results
The mean logMAR visual acuity improved from 0.2±0.25SD with glasses and 0.1±0.02SD with RGP to −0.002±0.041SD in all the eyes wearing scleral CL (p<0.05). All the patients found the scleral CL to be comfortable with a mean daily wear time of more than 6 hours. Average IOP values before, during, and after scleral CL wear are listed in Table 2. The high p-value shows that there is not a significant difference in IOP before lens wearing and after their removal for both GAT (p=0.45) and DT (p=0.31).
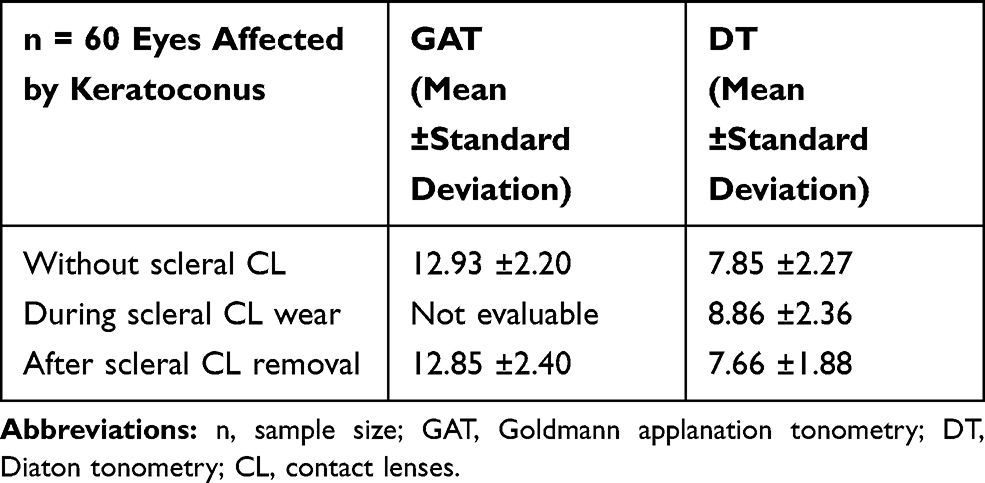 |
Table 2 Average IOP Obtained with GAT and DT Before, During and After Scleral CL Wear. Results are Expressed in Millimeters of Mercury Along with the Standard Deviation Value |
t-test performed on DT results before and during the lens wearing showed a significant increase in IOP (p-value <0.01). Similar results were obtained when comparing IOP measured with DT during and after lens removal (p-value <0.01). These results indicate that scleral CLs induce a small but statistically significant DT increase in IOP. Using the Bland-Altman method, the upper and lower limits of agreement between DT and GAT were found to be +7.8 and +2.5, respectively, before contact lens wearing. Upper and lower limits of agreement between DT and GAT were found to be +8.4 and +1.8, after lens removal (Figure 3).
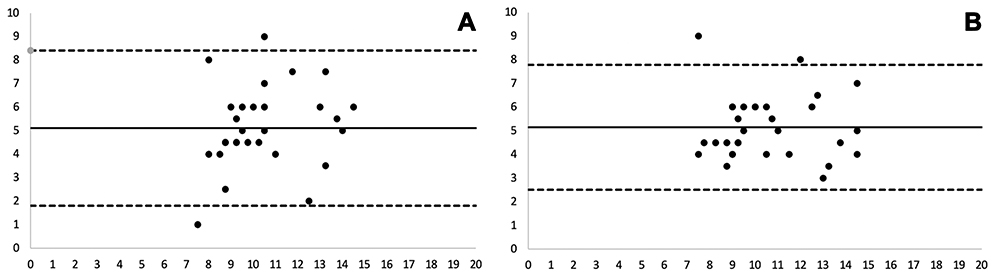 |
Figure 3 Bland-Altman plot on Diaton tonometry vs Goldmann tonometry, before the scleral lens application (A) and after their removal (B). Dotted black lines show upper limits of agreement (ULOA) and lower limits of agreement (LLOA). Continuous black line shows mean difference. (A) mean: +5.15, ULOA: +7.8, LLOA: +2.5; (B) mean: +5.10, ULOA: +8.4 LLOA: +1.8. Diff: difference. Results are shown in mmHg. |
Discussion
The efficiency of scleral lenses in correcting aberrations due to keratoconus is well demonstrated by many studies.6,8,17–19 In this study, our patients achieved a significantly better visual acuity with scleral CL when compared with spectacles or RGP contact lenses, providing an additional non-surgical option for the treatment of the pathology.
Besides, comfort was one of the primary advantages of scleral CL. Indeed, all the patients experienced relief from dryness and were able of tolerating at least a scleral CL wear of 6 hours daily. Scleral CLs regularized the corneal surface by vaulting the irregular keratoconic cornea with their surface and the tear reservoir underlying the lens. Differently, RGP contact lenses do not create a tear reservoir which vaults the cornea and their contact with the cornea, could compromise visual acuity and contact lenses tolerance.5
IOP changes in these patients wearing scleral CL were also investigated. Unlike soft lenses, scleral CL compress and settle into conjunctival tissue. During each blink, the pressure from the lid may press the lens farther into the conjunctiva.20 In general, large-diameter scleral lenses (≥18.0mm in diameter) have relatively wide haptics or landing zones (up to 2mm wide), with a broader distribution of the lens-bearing force on the eye. Thus, large-diameter scleral lenses may be less likely to compress any structures within or adjacent to the anterior chamber angle. However, small-diameter scleral lenses (14.0 to 16.5mm in diameter) generally have limited haptic widths and diameters, and they contact the conjunctiva closer to the limbus than do the larger lenses. The concentration of the bearing surface over a smaller area close to the limbus may presumably compress structures responsible for aqueous humor outflow as the Schlemm canal, the collector channels, or the episcleral veins and consequently increase intraocular pressure.20 Nonetheless, it is hypothesized that the functional diameter and the chord where the lens lands on the conjunctiva, are more important than the overall lens diameter.2 Compression of the structures of the anterior chamber angle could be indirectly related to signs of tight-fitting in the periphery such as blanching of the conjunctival blood vessels, conjunctival flush and marked suction between the lens and the conjunctival tissue that is difficult to break on lens removal.22 Ideally, well-fitted scleral lenses, which do not create excessively tight bearing zones as they settle, should not significantly elevate IOP.23 Apart from the degree of lens fit tightness, any IOP elevation associated with scleral fittings appears to be linked to individual patient characteristics. For example, eyes with reduced scleral thickness and/or rigidity appear likely to be more easily applanated at zones of tight scleral lens bearing.16 Anyway, eyes that are susceptible to baropathic diseases such as glaucoma, axial myopia, and corneal thinning diseases, such as keratoconus, could have pathological adverse events due to scleral CLs induced elevation of IOP.22 In literature, there are many studies regarding the relationship between scleral lens wear and IOP but results and methods range widely. Indeed, some studies conducted on lenses with a diameter between 15mm and 18mm, did not find a significant rise in IOP during the SLs wear using a pneumotonometer20 or after the scleral CLs wear, using GAT, a Tonopen, or a non-contact tonometer.24–26 Differently, other authors found a rise in IOP (average of 5mmHg) following scleral lens removal (diameter between 14.6mm and 18mm) using GAT, DT, or Icare tonometer and during scleral CLs wear using DT or a rebound tonometer.21,27–29
Authors who found an IOP elevation consequently to scleral CL application supposed that such findings might be a consequence of increased susceptibility to scleral lens-induced IOP elevation due to having thinner scleral tissue. Indeed, a thinner sclera would be easier to applanate or indent by bearing areas of scleral lenses. Tight fittings might also explain such effects. Any rise in IOP may also depend on aqueous drainage facility, which might be restricted in some individuals. In addition, aqueous drainage may be compromised by lenses with bearing areas at the limbus.20
In the present study, we found a small (1.01mmHg) but statistically significant increase of the IOP measured with DT during the scleral CL wearing. We decided to use DT because, even if GAT represents the gold standard in the IOP measurement, it does allow IOP measurement while wearing scleral contact lenses, and measuring IOP after lens removal can only be indirectly relevant to lens-in situ IOP.30 The Diaton tonometer is a handheld device capable of measuring IOP through the upper eyelid, avoiding corneal contact.31 However, the transpalpebral tonometer is a novel and still not well-standardized technique to measure IOP in eyes wearing scleral CL. For the Diaton, the manufacturer describes a possible error of ±2mmHg for eyes with IOP between 5 and 20mmHg, and an error of 10% of the current IOP for IOP between 20 and 60mmHg.21,26 Even if there was good agreement between DT and GAT, we found that DT usually gives a lower IOP value (about 5mmHg) compared to GAT results. From a clinical perspective, the differences are significant; indeed, it is not possible to relate values obtained with DT to reference values. Other studies reported poor agreement between DT and GAT,32 under or overestimation of the IOP,33 and a significant influence of the positioning on the IOP measurement with the DT.34 A moderate correlation between AT and DT was found when used on a normal eye in a study35 and when corrected for central corneal thickness in another study.31
Conclusions
Scleral CLs could be successfully used to treat corneal diseases such as keratoconus. They give a valid alternative to surgery with quality of vision and comfort superior to other actual devices. Even if 16.8mm diameter scleral CLs have easier handling than larger diameter scleral CLs, their landing zone is closer to structures involved in the aqueous humor outflow. We demonstrated that well-fitted scleral CLs, checked by AS-OCT and biomicroscopic examination, do not usually cause any signs of distress on the eye, rendering unlikely a compression of the structures of the anterior chamber angle.
The IOP values acquisition during scleral CL wear has been possible thanks to a new transpalpebral tonometer. Even if the methodic is new and still not standardized, its parallel use to GAT before and after scleral CL use allowed a better interpretation of the results. Statistical analysis showed good agreement between the two instruments but a constant numeric difference between values obtained with GAT and DT. This should be considered when relating DT values to reference ones.
The DT showed a small but significant (1.01mmHg; p<0.01) raise of the IOP during scleral CL wear. We believe that this small raise is unlikely to cause any glaucomatous damage in the eyes otherwise normal. Moreover, changes in the DT position should be occurred trying to avoid contact with the part of the superior lid overlying the scleral CL. Finally, it is recommendable for a proper selection and follow-up of the patients during the use of the scleral CLs. More studies with a wider casuistry are also needed.
Acknowledgment
Presented in part at the “International Summit of Specialty Contact Lenses (ISSCL)”, Rome (Italy) 8–10 November 2019.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chang HY, Chodosh J. The genetics of keratoconus. Semin Ophthalmol. 2013;28(5–6):275–280. doi:10.3109/08820538.2013.825295
2. Alkanaan A, Barsotti R, Kirat O, Khna A, Almubrad T, Akhtar S. Collagen fibrils and proteoglycans of peripheral and central stroma of the keratoconus cornea - Ultrastructure and 3D transmission electron tomography. Sci Rep. 2019;9:1–11. doi:10.1038/s41598-019-56529-1
3. Jinabhai AN. Customised aberration-controlling corrections for keratoconic patients using contact lenses. Clin Exp Optom. 2020;103(1):31–43. doi:10.1111/cxo.12937
4. Montalt JC, Porcar E, España-Gregori E, Peris-Martínez C. Corneal biomechanical parameters with corneoscleral contact lenses in post-laser in situ keratomileusis eyes. Eye Contact Lens. 2018;44(Suppl 2):S65–9. doi:10.1097/ICL.0000000000000420
5. Weissman B, Chun MW, Barnhart LA. Corneal abrasion associated with contact lens correction of keratoconus–a retrospective study. Optom Vis Sci. 1994;71(11):677–681. doi:10.1097/00006324-199411000-00001
6. Sengor T, Kurna SA, Aki S, Özkurt Y. High Dk piggyback contact lens system for contact lens-intolerant keratoconus patients. Clin Ophthalmol. 2011;5:331–335. doi:10.2147/OPTH.S16727
7. Walker MK, Schornack MM, Vincent SJ. Anatomical and physiological considerations in scleral lens wear: conjunctiva and sclera. Cont Lens Anterior Eye. 2020;
8. Michaud L, Lipson M, Kramer E, Walker M. The official guide to scleral lens terminology. Cont Lens Anterior Eye. 2019.
9. Koppen C, Kreps EO, Anthonissen L, Van Hoey M, Dhubhghaill SN, Vermeulen L. Scleral lenses reduce the need for corneal transplants in severe keratoconus. Am J Ophthalmol. 2018;185:43–44. doi:10.1016/j.ajo.2017.10.022
10. Kumar M, Shetty R, Dutta D, Rao HL, Jayadev C, Atchison DA. Effects of a semi-scleral contact lens on refraction and higher order aberrations. Cont Lens Anterior Eye. 2019;42(6):670–674. doi:10.1016/j.clae.2019.06.002
11. Spadea L, Gizzi R, Evangelista Conocchia N, Urbano S. Optical pachymetry-guided custom excimer laser-assisted lamellar keratoplasty for the surgical treatment of keratoconus. J Cataract Refract Surg. 2012;38(9):1559–1567. doi:10.1016/j.jcrs.2012.05.029
12. Krumeich JH, Daniel J, Knulle A. Live-epikeratophakia for keratoconus. J Cataract Refract Surg. 1998;24:456–463. doi:10.1016/S0886-3350(98)80284-8
13. Cacho I, Sanchez-Naves J, Batres L, Pintor J, Carracedo G. Comparison of intraocular pressure before and after laser in situ keratomileusis refractive surgery measured with perkins tonometry, noncontact tonometry, and transpalpebral tonometry. J Ophthalmol. 2015;2015:683895. doi:10.1155/2015/683895
14. Khan JA, LaGreca BA. Tono-pen estimation of intraocular pressure through bandage contact lenses. Am J Ophthalmol. 1989;108(4):422–425. doi:10.1016/S0002-9394(14)73310-0
15. Sandner D, Bohm A, Kostov S, Pillunat L. Measurement of the intraocular pressure with the “transpalpebral tonometer” TGDc-01 in comparison with applanation tonometry. Graefes Arch Clin Exp Ophthalmol. 2005;243:563–569. doi:10.1007/s00417-004-1037-1
16. Troost A, Yun SH, Specht K, Krummenauer F, Schwenn O. Transpalpebral tonometry: reliability and comparison with Goldmann applanation tonometry and palpation in healthy volunteers. Br J Ophthalmol. 2005;89:280–283. doi:10.1136/bjo.2004.050211
17. Kim S, Lee JS, Park YK, et al. Fitting miniscleral contact lenses in Korean patients with keratoconus. Clin Exp Optom. 2017;100(4):375–379. doi:10.1111/cxo.12424
18. Montalt JC, Porcar E, España-Gregori E, Peris-Martínez C. Visual quality with corneoscleral contact lenses for keratoconus management. Cont Lens Anterior Eye. 2018;41(4):351–356. doi:10.1016/j.clae.2018.01.002
19. Sabesan R, Johns L, Tomashevskaya O, Jacobs DS, Rosenthal P, Yoon G. Wavefront-guided scleral lens prosthetic device for keratoconus. Optom Vis Sci. 2013;90(4):314–323. doi:10.1097/OPX.0b013e318288d19c
20. Nau CB, Schornack MM, McLaren JW, Sit AJ. Intraocular pressure after 2 hours of small- diameter scleral lens wear. Eye Contact Lens. 2015;42:350–353. doi:10.1097/ICL.0000000000000214
21. Michaud L, Samaha D, Giasson CJ. Intra-ocular pressure variation associated with the wear of scleral lenses of different diameters. Contact Lens Anterior Eye. 2019;42(1):104–110. doi:10.1016/j.clae.2018.07.004
22. McMonnies CW. A hypothesis that scleral contact lenses could elevate intraocular pressure. Clin Experiment Optom. 2016;99(6):594–596. doi:10.1111/cxo.12368
23. McMonnies CW, Boneham GC. Experimentally-increased intraocular pressure, using digital forces. Eye Cont Lens. 2007;33:124–129. doi:10.1097/01.icl.0000247637.71618.26
24. Shahnazi KC, Isozaki VL, Chiu GB. Effect of scleral lens wear on central corneal thickness and intraocular pressure in patients with ocular surface disease. Eye Contact Lens. 2019. doi:10.1097/ICL.0000000000000670
25. Kramer EG, Vincent SJ. Intraocular pressure changes in neophyte scleral lens wearers: a prospective study. Cont Lens Anterior Eye. 2020;43:SS1367–9. doi:10.1016/j.clae.2020.05.010
26. Vincent SJ, Alonso-Caneiro D, Collins MJ. Evidence on scleral contact lenses and intraocular pressure. Clin Exp Optom. 2017;100(1):87–88. doi:10.1111/cxo.12448
27. Aitseabomo AP, Wong-Powell J, Miller W, Farshid A. Effect of scleral lens wear on intraocular pressure. Invest Ophthalmol Vis Sci. 2018;3(1):e1–e9.
28. Turpin S, Antoniuk K, Caroline P, Kojima R, Kinoshita B, Lampa M, Does IOP increase during scleral lens wear?
29. Cheung SY, Collins MJ, Vincent SJ. The impact of short-term fenestrated scleral lens wear on intraocular pressure. Cont Lens Anterior Eye. 2020;43:SS1367. doi:10.1016/j.clae.2020.02.003
30. McMonnies CW. Re: evidence on scleral contact lenses and intraocular pressure. Clin Exp Optom. 2017;100(2):200. doi:10.1111/cxo.12505
31. Toker MI, Vural A, Erdogan H, Topalkara A, Arici MK. Central corneal thickness and Diaton transpalpebral tonometry. Graefes Arch Clin Exp Ophthalmol. 2008;246(6):881–889. doi:10.1007/s00417-008-0769-8
32. Wisse RPL, Peeters N, Imhof SM, van der Lelij A. Comparison of Diaton transpalpebral tonometer with applanation tonometry in keratoconus. Int J Ophthalmol. 2016;9(3):395–398. doi:10.18240/ijo.2016.03.12
33. Li Y, Shi J, Duan X, Fan F. Transpalpebral measurement of intraocular pressure using the Diaton tonometer versus standard Goldmann applanation tonometry. Graefes Arch Clin Exp Ophthalmol. 2010;248:1765–1770. doi:10.1007/s00417-009-1243-y
34. Doherty MD, Carrim ZI, O’Neill DP. Diaton tonometry: an assessment of validity and preference against Goldmann tonometry. Clin Exp Ophthalmol. 2012;40(4):e171–e5. doi:10.1111/j.1442-9071.2011.02636.x
35. Bali SJ, Bhartiya S, Sobti A, Dada T, Panda A. Comparative evaluation of Diaton and Goldmann applanation tonometers. Ophthalmologica. 2012;228(1):42–46. doi:10.1159/000336047
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.