Back to Journals » Drug Design, Development and Therapy » Volume 20
Effects of Ropivacaine-Based Thoracic Paravertebral Block versus Erector Spinae Plane Block on Quality of Recovery in Laparoscopic Colorectal Cancer Surgery: A Randomized Controlled Trial
Authors Shi S, Liang Y ![]() , Liu T, Wang J, Xu X, Cheng A, Wang H, Hu J
, Liu T, Wang J, Xu X, Cheng A, Wang H, Hu J ![]()
Received 12 November 2025
Accepted for publication 10 March 2026
Published 18 March 2026 Volume 2026:20 581084
DOI https://doi.org/10.2147/DDDT.S581084
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Georgios Panos
Shuaibo Shi,1 Yuhao Liang,1 Tao Liu,2 Junlong Wang,1 Xuanxuan Xu,1 Axue Cheng,1 Hui Wang,2 Jie Hu2
1Department of Anesthesiology, Luoyang Central Hospital Affiliated to Henan Medical University, Luoyang, People’s Republic of China; 2Department of Anesthesiology, Luoyang Central Hospital, Luoyang, People’s Republic of China
Correspondence: Jie Hu, Department of Anesthesiology, Luoyang Central Hospital, Luoyang, People’s Republic of China, Tel +86 137 2162 4858, Email [email protected]
Background: Colorectal cancer remains a leading cause of cancer-related mortality worldwide. Postoperative pain can impair recovery. Thoracic paravertebral block (TPVB) and erector spinae plane block (ESPB) are regional analgesic techniques that may enhance recovery, but their comparative efficacy in colorectal surgery is not well established. This study aimed to compare the effects of TPVB and ESPB on the quality of recovery in patients undergoing colorectal cancer surgery.
Methods: In this single-center, single-blind, randomized controlled trial, 87 patients scheduled for elective laparoscopic colorectal cancer surgery were initially enrolled and randomly assigned. Ultimately, 85 patients were included in the per-protocol analysis, distributed as follows: the bilateral TPVB (n = 29), the bilateral ESPB (n = 28), and the control (n = 28). Both blocks were performed at the T10 level using 20 mL of 0.375% ropivacaine per side. The primary outcome was the Quality of Recovery-15 (QoR-15) scores at 24 hours postoperatively. Secondary outcomes included pain scores, overall benefit of analgesia scores (OBAS), area under the curve (AUC) analyses for these scores and opioid consumption.
Results: Both TPVB and ESPB groups had higher QoR-15 scores at 24 hours compared to controls (TPVB: 122.03 ± 4.00, ESPB: 119.00 ± 3.09, Control: 109.79 ± 2.89; both P < 0.001). TPVB provided a statistically significant, yet clinically modest, improvement in recovery over ESPB at 24 hours (mean difference [MD] 3.03; 95% CI, 0.09 to 5.98; P = 0.036). However, QoR‑15 AUC over 72 hours did not differ between blocks (P = 0.12). Both blocks resulted in better OBAS throughout the first 48 hours (all P < 0.05). TPVB also demonstrated better early resting pain control at 6 hours (P = 0.012) but had a longer performance time than ESPB (P = 0.003). Both intervention groups reduced opioid consumption.
Conclusion: Both TPVB and ESPB improve recovery quality and analgesia after laparoscopic colorectal cancer surgery. Overall, the two block techniques provided comparable benefits for postoperative recovery and analgesia.
Trial Registration: ChiCTR2400089500.
Keywords: erector spinae plane block, paravertebral block, quality of recovery, enhanced recovery after surgery, colorectal cancer
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Ma has been published for this article.
Introduction
According to current statistical data, colorectal cancer has become the third leading cause of cancer-related mortality worldwide,1 with a 2% annual increase in incidence among non-elderly patients over the past decade.2 Surgical intervention remains the cornerstone of treatment. Laparoscopic surgery has gained widespread acceptance among gastrointestinal surgeons.3 However, acute postoperative pain following laparoscopic radical resection of colorectal cancer can significantly impact patients’ recovery quality.
The Enhanced Recovery After Surgery (ERAS) protocol has been strongly validated for its benefits in postoperative rehabilitation for patients undergoing colorectal cancer resection.4,5 Therefore, improving recovery quality, optimizing perioperative pain management, and effectively implementing the ERAS protocol have become major concerns for anesthesiologists. Based on the concept of multimodal analgesia, anesthesiologists often employ a variety of analgesic techniques to provide comprehensive postoperative pain relief.6
Epidural analgesia was once the standard analgesic strategy following colorectal surgery, providing comprehensive pain control. However, it is associated with potential serious adverse events. With advances in ultrasound-guided visualization, the technical barriers to performing thoracic paravertebral block (TPVB) have gradually diminished. This technique involves injecting local anesthetics into the paravertebral space (PVS), where the spread of the medication blocks the corresponding spinal and sympathetic nerves.7 As a result, TPVB not only effectively manages somatic pain but also modulates sympathetic activity, thereby reducing visceral pain. It has now been widely adopted for analgesia in various thoracic and abdominal surgeries.8,9 Some researchers10 have suggested further investigation into the application of TPVB in major abdominal surgery to evaluate its therapeutic efficacy.
The erector spinae plane block (ESPB) was first introduced by Forero et al11 in 2016. Its efficacy and safety have since been demonstrated in studies involving thoracic, abdominal, and even lumbar surgeries.12–16 The procedure involves injecting local anesthetic into the plane between the deep aspect of the erector spinae muscle and the transverse process to achieve blockade of the corresponding spinal segments.17–19 TPVB and ESPB differ in their anatomical basis, procedural complexity, and neuroregulatory effects. Evidence is therefore needed to compare their impact on patient-reported recovery outcomes to guide anesthesiologists in selecting the most appropriate block technique. While several studies have compared the effects of TPVB and ESPB on postoperative recovery, comparisons between these two regional techniques in the context of colorectal surgery remain scarce.
Herein, we conducted a single-blind, randomized, controlled trial to evaluate the impact of TPVB versus ESPB on recovery quality and analgesia in patients undergoing colorectal cancer surgery, with additional assessment of adverse events. This study aims to provide new insights into precise perioperative pain management strategies for colorectal cancer patients.
Materials and Methods
Study Design
This single-center, single-blind, randomized, controlled trial was approved by the Luoyang Central Hospital Medical Ethics Committee (LWLL-2024-08-29-02) on August 29, 2024. This study was conducted in accordance with the Declaration of Helsinki. All participants provided written informed consent at enrollment. The trial was registered in the Chinese Clinical Trial Registry (ChiCTR2400089500). Our clinical trial was registered before its initiation and prior to any patient enrollment, and the methods presented in the paper are identical to those described in the trial registration. The reporting complies with the 2025 version of the Consolidated Standards of Reporting Trials (CONSORT). This study was conducted from September 2024 to March 2025 at Luoyang Central Hospital.
Trial Participants
The inclusion criteria were as follows: age between 18 and 80 years; American Society of Anesthesiologists (ASA) physical status II–III; body mass index (BMI) between 18 and 32 kg/m2; and scheduled for elective laparoscopic radical colorectal cancer surgery. Exclusion criteria included: contraindications to regional blockade or related medications; spinal and chest wall deformities; severe respiratory and circulatory dysfunction or hepatic and renal abnormalities; chronic pain or long-term opioid use (>4 weeks); pregnancy or lactation; and inability to cooperate due to psychiatric disorders. The following cases were also excluded: perioperative major hemorrhage, cerebral infarction, or other serious accidents; postoperative intensive care unit (ICU) admission; reoperation within 3 days after surgery; conversion to laparotomy during surgery; and loss to follow-up.
Randomization and Blinding
Participants were assigned to three groups based on the intervention received: the Group TPVB, the Group ESPB, or the Group Control. Eligible participants were randomly allocated in a 1:1:1 ratio using computer-generated random numbers. To ensure strict allocation concealment, the group assignment for each participant was placed in sequentially numbered, opaque, sealed envelopes. On the day of surgery, the anesthesiologist who would perform the nerve block retrieved the corresponding envelope in sequential order only after the participant had been enrolled and had completed baseline assessments. The group allocation was blinded from both the responsible anesthesiologist and the outcome assessors. Participants in the intervention groups received either ESPB or TPVB, whereas those in the Group Control received general anesthesia alone and were aware of their group assignment.
Study Protocol
All participants strictly adhered to standard fasting guidelines. Before entering the operating room, participants were transferred to the anesthesia preparation room for nerve block. Standard monitoring, including electrocardiogram, non-invasive blood pressure, and pulse oximetry, was applied throughout the procedure. The nerve block was performed provided that vital signs remained stable. All invasive procedures were carried out by the same experienced anesthesiologist under strict aseptic conditions.
Both bilateral ultrasound-guided TPVB and ESPB were performed in the prone position using an in-plane technique. A low-frequency convex array transducer ultrasound probe (Wisonic Navi T ultrasound system, Wisonic Medical Technology Co., Ltd., Shenzhen, China) was utilized to visualize the anatomical structures. The ultrasound probe was initially placed transversely to identify the T12 rib and then moved cephalad to sequentially locate the ribs until the T10 level was identified. Sedative or analgesic drugs were not routinely administered during the performance of the nerve blocks. To ensure patient comfort during the procedure, prior to all nerve block procedures, local infiltration anesthesia was administered with 1–2 mL of 1% lidocaine to alleviate puncture-related discomfort.
For TPVB, a 22G block needle was advanced into the PVS. Correct needle tip position was confirmed by injecting 1–2 mL of normal saline. Subsequently, 20 mL of 0.375% ropivacaine (Guangdong Jiabo Pharmaceutical Co., Ltd., Guangdong, China) was injected into the PVS, with downward displacement of the pleura observed. The same procedure was repeated on the contralateral side.
For ESPB, the T10 transverse process was positioned midline in the parasagittal view. A 22G block needle was advanced toward the plane deep to the erector spinae muscle and superficial to the transverse process. After confirmation with normal saline, 20 mL of 0.375% ropivacaine was injected unilaterally. Elevation of the erector spinae muscle without intramuscular expansion was observed. The same procedure was repeated contralaterally (Figure S1).
Successful nerve block was defined as a reported difference in temperature sensation between the blocked dermatomal area and the contralateral region when assessed with an alcohol-soaked swab during the post-block period prior to anesthesia induction.
Anesthesia Procedures and Perioperative Management
All patients underwent general anesthesia. All patients received active or passive warming measures upon arrival in the operating room. Preoperatively, 500 mL of crystalloid fluid was administered for volume preloading. After preoxygenation, anesthesia was induced with midazolam (0.05 mg/kg), sufentanil (0.25–0.35 μg/kg), cisatracurium (0.15 mg/kg), and etomidate (0.3 mg/kg). Following neuromuscular blockade, an appropriately sized endotracheal tube was inserted. Invasive arterial pressure monitoring and right internal jugular venous access were established thereafter. Anesthesia was maintained with continuous infusions of propofol (3–6 mg·kg−1·h−1), remifentanil (0.1–0.2 μg·kg−1·min−1), and cisatracurium (0.1–0.2 mg·kg−1·h−1), supplemented with intermittent sevoflurane (0.5–3%) to maintain a Bispectral Index between 40 and 60. Ondansetron (4 mg) was administered intravenously for prophylaxis of postoperative nausea and vomiting (PONV). Thirty minutes before the end of surgery, neuromuscular blocking agents and inhalational anesthetics were discontinued, and sufentanil (5 μg) was administered for analgesic transition.
Postoperative analgesic management consisted of an opioid-based patient-controlled intravenous analgesia (PCIA) pump combined with scheduled intravenous administration of non-steroidal anti-inflammatory drugs (NSAIDs). The standard PCIA regimen consisted of sufentanil (100 μg), ondansetron (4 mg), and normal saline, with a total volume of 100 mL. No background infusion was programmed. The bolus dose was set at 2 mL per demand, with a lockout interval of 10 minutes. During preoperative education, patients were instructed to self-administer a bolus when they felt the need for analgesia. If the resting Numeric Rating Scale (NRS) score was ≥ 4, rescue analgesia was provided with intravenous morphine (1 mg). Intravenous flurbiprofen axetil (50 mg) was infused every 12 hours for analgesia.
Standard rescue protocols included: intravenous norepinephrine (4 μg) for intraoperative hypotension (mean arterial pressure < 65 mmHg), and atropine (0.5 mg) for bradycardia (heart rate < 50 beats per minute).20
Outcome Measurements
The primary outcome was the quality of recovery-15 (QoR-15) scores21 at 24 hours postoperatively. Secondary outcomes included QoR-15 scores at 48 and 72 hours after surgery; NRS at rest and during movement at 1, 6, 24, and 48 hours postoperatively; the Overall Benefit of Analgesia Score (OBAS) at 24, 48, and 72 hours; and the area under the curve (AUC) (1.1) for QoR-15, NRS, and OBAS scores over time. Perioperative opioid consumption, including intraoperative sufentanil and remifentanil, and postoperative sufentanil within 48 hours, calculated as morphine milligram equivalents (MME), was also recorded.
Other outcomes included changes in mean arterial pressure and heart rate immediately before and after skin incision; block performance time; length of hospital stay; time to first flatus; ambulation time; and the Systemic Immune-Inflammation Index (SII)22 on postoperative day 1. The incidence of chronic pain at 3 months after surgery was assessed using the S-LANSS score.23 Block-related adverse events (hypotension, hypothermia, bleeding, pneumothorax, intrathecal injection, and local anesthetic systemic toxicity) and the incidence of PONV were documented.
The SII is a composite biomarker derived from routine peripheral blood counts, calculated as SII = platelet count × neutrophil count / lymphocyte count, with units of (×109/L). It reflects the balance between pro-inflammatory and anti-inflammatory immune components, with elevated SII indicating a state of systemic inflammation and impaired immune surveillance. Numerous studies have demonstrated that SII can reflect the inflammatory status associated with colorectal tumors.24,25

where yi is the score at time point ti.
Statistical Analysis
Sample size calculation was performed using the PASS 15.0 program (NCSS, LLC., Kaysville, UT, USA), with the QoR-15 scores at 24 hours postoperatively designated as the primary outcome. Based on unpublished pilot data, the minimum detectable difference among the three groups was 8.8, with standard deviations (SD) of 6.28, 4.26, and 3.96, respectively. With a significance level of 0.05 and a power of 80%, a sample size of 26 participants per group was required. Accounting for a potential dropout rate of 10%, the final sample size was determined to be 29 patients per group.
Intention-to-treat (ITT) set was defined as all randomized patients, regardless of whether they received the assigned intervention (nerve block) or completed follow-up. Modified intention-to-treat (mITT) set was defined as all randomized patients who received at least one study intervention (nerve block). Per-protocol (PP) set was defined as patients who fully adhered to the study protocol, completed all key procedures, and provided data for the primary outcome.
The normality of continuous variables was assessed using the Shapiro–Wilk test. Homogeneity of variances was tested using Levene’s test. Normally continuous data were analyzed with one-way ANOVA and expressed as mean ± SD. Non-normally distributed continuous variables were analyzed using the Kruskal–Wallis H-test and reported as median (interquartile range [IQR]). Categorical variables were summarized as numbers (n, %) and compared using the χ2-test or Fisher’s exact test. For these variables, overall differences among the three groups were first evaluated. If a significant difference was detected, subsequent pairwise post-hoc comparisons were performed, and the resulting p-values were adjusted using the Bonferroni method to account for multiple testing (labeled as “Adj-P”).
For longitudinal analysis of repeated continuous measures, generalized estimating equations (GEE) were employed to provide robust parameter estimates. Detailed parameter settings for the GEE can be found in the supplementary material. For multiple comparisons in longitudinal data, a stratified correction strategy was adopted: within each time point, pairwise comparisons between groups were adjusted using the Bonferroni method (correction factor of 3). All p-values corrected by the Bonferroni method are labeled as “Adj-P”, where Adj-P < 0.05 indicates statistical significance; unlabeled p-values are unadjusted, where P < 0.05 was considered statistically significant.
To evaluate the potential impact of imbalanced baseline surgical type distribution on the main findings, surgical type was included as a covariate in the GEE model for sensitivity analyses of the primary outcome.
All primary and secondary efficacy analyses were based on the PP set. This approach was necessitated by the incomplete post-randomization outcome follow-up for patients who were excluded (due to ICU transfer or block failure), which precluded a complete strict ITT evaluation for the primary outcomes. In the per-protocol set, there were no missing values to handle. All statistical analyses were conducted using SPSS version 27.0 (IBM Corp., Chicago, IL, USA) and R version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria). Figures were generated with Origin 2021 (OriginLab Corporation, Northampton, MA, USA).
Results
Participants
Ninety-three patients were enrolled. After applying the exclusion criteria, 87 patients were randomized into three groups (n = 29 per group, ITT set). In the Group ESPB, one patient experienced block failure. One patient in the Group Control was transferred to the ICU due to major intraoperative hemorrhage. Consequently, complete post-randomization outcome follow-up (such as the 24-hour QoR-15 assessment) was not feasible for these two individuals. Because of this missing data, true ITT sensitivity analyses for the primary efficacy outcomes could not be performed, and these two subjects were excluded from the final efficacy evaluation. Although efficacy outcomes could not be evaluated for the entire randomized population, the baseline and intraoperative characteristics of the ITT and mITT analysis sets were analyzed and are pres ented in Table S1. Ultimately, 85 patients (PP set) completed the study (Figure 1). Baseline demographic and clinical characteristics were generally comparable across the groups with no statistically significant differences (Table 1). However, given a visible numerical variation in the types of surgery, this variable was accounted for in subsequent sensitivity analyses.
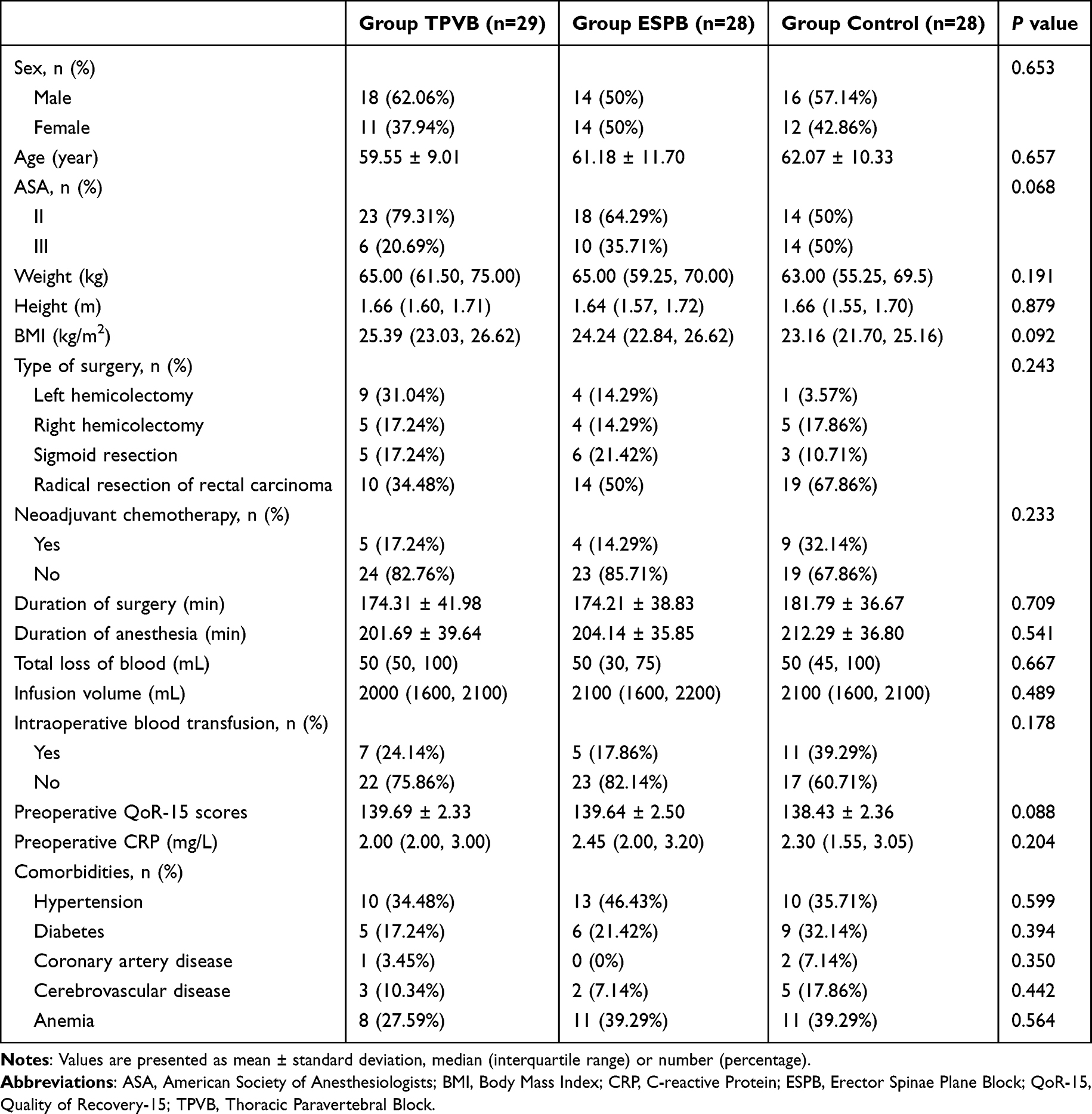 |
Table 1 Patient and Surgical Characteristics |
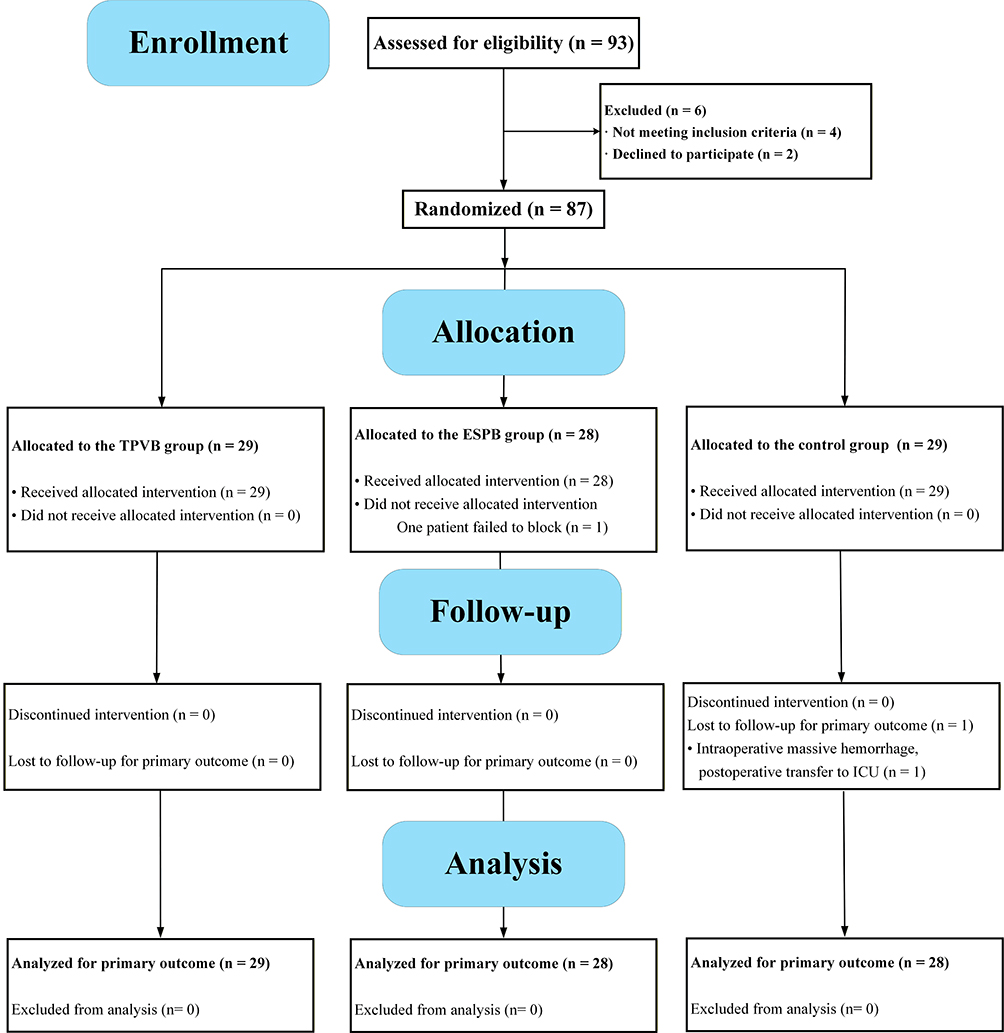 |
Figure 1 CONSORT diagram illustrating patient recruitment, allocation, follow-up, and analysis. Abbreviations: ESPB, Erector Spinae Plane Block; ICU, Intensive Care Unit; TPVB, Thoracic Paravertebral Block. |
Primary and Secondary Outcomes
At 24 and 48 hours postoperatively, the QoR-15 scores in the Group Control (109.79 ± 2.89 and 118.68 ± 2.71, respectively) were significantly lower than those in both the Group TPVB (122.03 ± 4.00 and 128.14 ± 3.64; Adj‐P < 0.001 for both) and the Group ESPB (119.00 ± 3.09 and 126.26 ± 2.61; Adj‐P < 0.001 for both). At the 24-hour assessment, the QoR-15 scores were significantly higher in the Group TPVB compared to the Group ESPB (mean difference [MD], 3.03; 95% confidence interval [CI], 0.09 to 5.98; Adj‐P = 0.036). However, no significant differences were observed among the three groups at 72 hours (Table S2 and Figure 2). The AUC for QoR-15 scores was significantly greater in both the TPVB and ESPB groups compared to the Group Control, although no statistically significant difference was detected between the TPVB and ESPB groups (P = 0.12) (Table 2).
 |
Table 2 The AUC of QoR-15, NRS and OBAS |
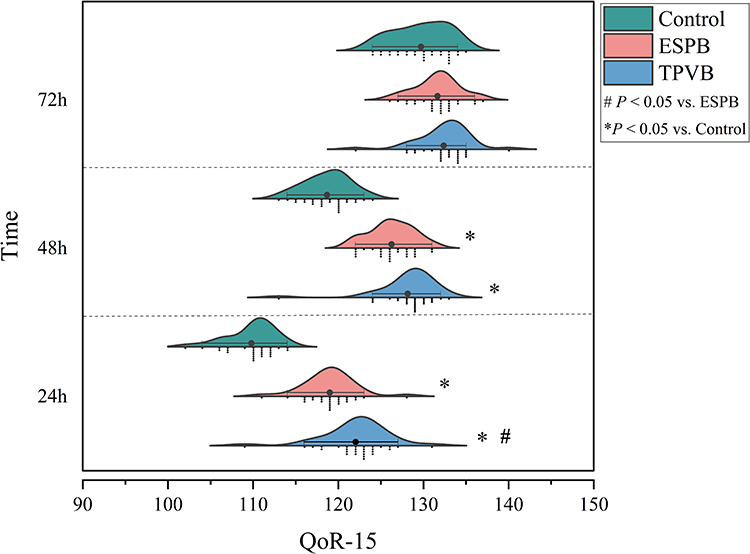 |
Figure 2 QoR-15 scores at 24, 48, and 72 hours postoperatively among the three groups. *: Significant difference compared with the Group Control (Adj‐P < 0.05); #: Significant difference compared with the Group ESPB (Adj‐P < 0.05). Abbreviations: TPVB, Thoracic Paravertebral Block; ESPB, Erector Spinae Plane Block; QoR-15, Quality of Recovery-15. |
At 1 hour postoperatively, the resting NRS score in the Group TPVB was significantly lower than that in the control group (MD, –0.64; 95% CI, –1.26 to –0.03; Adj‐P = 0.027). By 6 hours after surgery, pairwise comparisons of resting NRS scores showed statistically significant differences among all three groups (Table S2). For dynamic NRS scores, both the TPVB and ESPB groups demonstrated significantly lower values compared to the control group at 1 and 6 hours postoperatively (all Adj‐P < 0.001). At 24 hours, the dynamic NRS score remained significantly lower in the Group TPVB than in the Group Control (MD, –0.70; 95% CI, –1.38 to –0.02; Adj‐P = 0.032) (Figure 3). Additionally, significant differences in the OBAS were observed among all three groups at both 24 and 48 hours after surgery (Figure 4).
 |
Figure 3 NRS scores of the three patient groups at different time points after surgery. (A) NRS score at rest; (B) NRS score during movement. *: Significant difference compared with the Group Control (Adj‐P < 0.05); #: Significant difference compared with the Group ESPB (Adj‐P < 0.05). Abbreviations: ESPB, Erector Spinae Plane Block; NRS, Numerical Rating Scale; TPVB, Thoracic Paravertebral Block. |
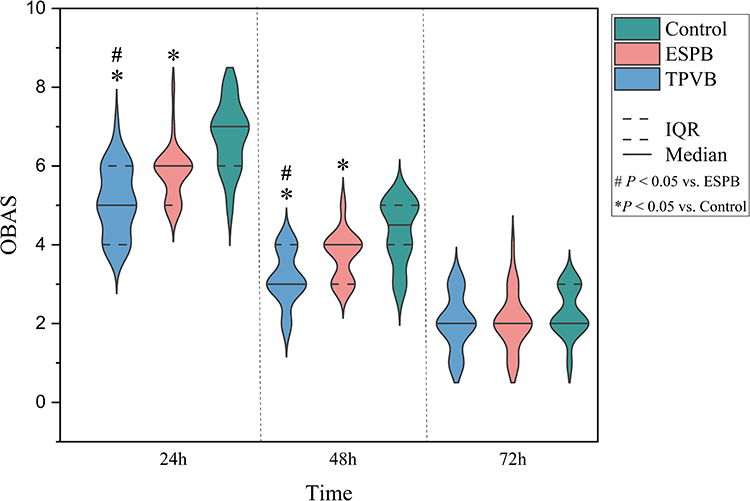 |
Figure 4 OBAS scores of the three patient groups at different time points after surgery. *: Significant difference compared with the Group Control (Adj‐P < 0.05); #: Significant difference compared with the Group ESPB (Adj‐P < 0.05). Abbreviations: ESPB, Erector Spinae Plane Block; IQR, Interquartile Range; OBAS, Overall Benefit of Analgesic Score; TPVB, Thoracic Paravertebral Block. |
The AUC values for both resting and dynamic NRS scores were significantly higher in the Group Control compared to the TPVB and ESPB groups. However, no statistically significant differences were observed between the TPVB and ESPB groups in either resting (MD, –0.73; 95% CI, –1.49 to 0.02; Adj‐P = 0.059) or dynamic (Adj‐P = 0.056) pain score AUC values. Similarly, there was no significant difference in the OBAS AUC values between the TPVB and ESPB groups (Table 2).
The perioperative opioid consumption, expressed as MME, was significantly higher in the Group Control compared to both the Group TPVB (MD, 32.94; 95% CI, 18.67 to 47.20; Adj‐P < 0.001) and the Group ESPB (MD, 22.95; 95% CI, 8.56 to 37.34; Adj‐P < 0.001). Furthermore, a significant difference was observed in postoperative sufentanil consumption within 48 hours among the three groups (P < 0.001). The changes in mean arterial pressure and heart rate before and after skin incision also differed significantly among the groups (both P < 0.001). The performance time of TPVB was longer than that of ESPB (P = 0.003). At 24 hours postoperatively, the SII was significantly lower in both the TPVB and ESPB groups compared to the Group Control (both Adj‐P < 0.001). Additionally, the SII in the Group TPVB was significantly lower than that in the Group ESPB (MD, –307.92; 95% CI, –586.40 to –29.44; Adj‐P = 0.025) (Table 3).
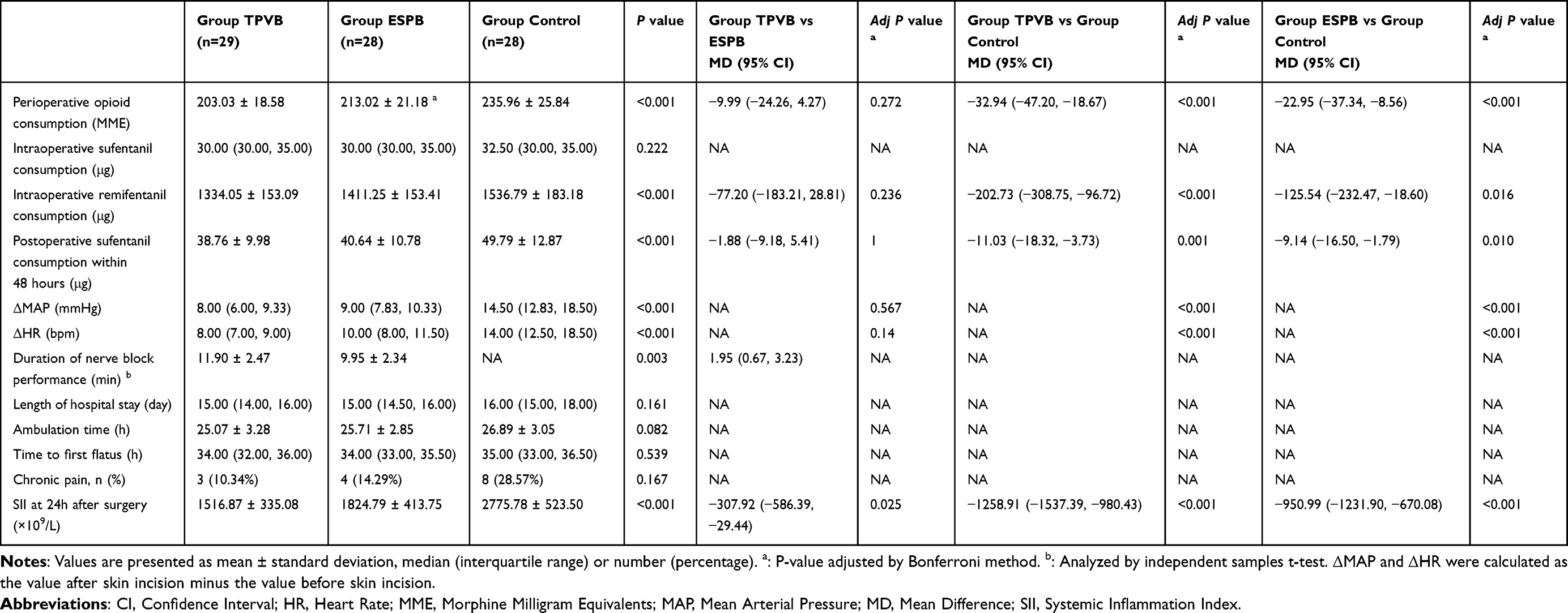 |
Table 3 Other Data |
There was a significant overall difference in the incidence of PONV among the three groups (Overall P = 0.026). Pairwise post-hoc comparisons revealed that the incidence of PONV was significantly lower in the Group TPVB (4 / 29 [13.79%]) compared to the Group Control (13 / 28 [46.43%]; Adj-P = 0.029). However, the incidence in the Group ESPB (8 / 28 [28.57%]) was not significantly different from that in the Group Control (Adj-P = 0.808) or the Group TPVB (Adj-P = 0.621). No significant differences were observed in other adverse events among the groups (Table S3).
Sensitivity Analysis
We treated the type of surgery as a covariate within a GEE model to re-evaluate the longitudinal QoR-15 scores, with all other model parameters identical to the primary analysis. The benefits of both TPVB and ESPB over the control group at 24 and 48 hours remained statistically significant after adjustment (Adj‐P < 0.001). Furthermore, the small, statistically significant difference in QoR-15 scores between the TPVB and ESPB groups at 24 hours remained detectable after adjustment (adjusted MD: 3.12; 95% CI: 0.05 to 6.20; Adj‐P = 0.042) (Table S4).
Discussion
This randomized controlled trial demonstrates that both TPVB and ESPB significantly enhance postoperative recovery quality at 24 hours in patients undergoing colorectal cancer surgery, with TPVB providing small, statistically significant but clinically modest early benefits. The study is also an exploratory exercise in moving from multimodal analgesia to precise multimodal analgesia.26
In this study, the QoR-15 scores, serving as a key patient-reported outcome measuring the quality of postoperative recovery, revealed two major findings: first, both TPVB and ESPB provided a clinically significant improvement in early recovery quality compared with general anesthesia alone; second, although the two regional techniques were largely equivalent in terms of the primary outcome, TPVB demonstrated a slight potential advantage in the early postoperative period.
First, both the TPVB and ESPB groups demonstrated significantly higher QoR-15 scores at 24 and 48 hours postoperatively compared to the Group Control, with the magnitude of improvement exceeding the minimal clinically important difference (MCID = 8 points).27 This finding supports the core value of incorporating either TPVB or ESPB into a multimodal analgesia strategy for achieving ERAS goals.5 By directly blocking nociceptive input, regional techniques not only provide superior analgesia but also mitigate surgical stress responses,28,29 thereby promoting overall recovery.
However, a more detailed analysis revealed that at the critical 24-hour postoperative time point, the QoR-15 scale in the TPVB group was significantly higher than that in the ESPB group (MD = 3.03, P = 0.036). The observed difference in primary outcome is less than half of the MCID of 8 points for the QoR-15 scale. Therefore, while statistically detectable, this difference is unlikely to represent a clinically meaningful advantage of TPVB over ESPB in terms of early recovery quality. Given the modest and clinically equivocal effect size, any mechanistic distinction between the blocks remains speculative. We cautiously speculate that this small difference may be attributable to an advantage of TPVB in sympathetic modulation. Perioperative autonomic regulation is increasingly recognized as a novel approach to improving recovery quality.30,31 However, given the modest effect size, the clinical importance of this mechanistic distinction remains uncertain. Nevertheless, by 48 hours post-surgery, the difference between the two groups was no longer statistically significant (P = 0.778), and there was no significant difference in the QoR-15 AUC values throughout the perioperative period (P = 0.12). This suggests that the overall recovery benefits of both techniques are largely equivalent over the entire perioperative period.
Bilateral TPVB or ESPB were performed at the T10 level based on the main spinal segmental distribution of nociceptive input from colorectal surgery. The nociceptive afferents from the colorectum travel through the hypogastric nerves, which play a key role in colorectal sensory transmission and serve as the primary pathway mediating colorectal pain. The neuronal cell bodies of these fibers are located in the thoracolumbar spinal ganglia, with their central projections entering the spinal cord segments from T2–T3 to L2–L3. Additionally, parasympathetic pathways transmit signals via the pelvic nerves,32 which are theoretically not directly targeted by TPVB. Local anesthetic administered at the T10 level takes advantage of its craniocaudal spread within the paravertebral space or fascial plane (a single injection of 20–25 mL typically covers 4–5 dermatomes33,34), thereby aiming to block as much of the afferent input from intraoperative visceral traction and the abdominal wall incision as possible.
Although our protocol incorporated the principles of multimodal analgesia—combining regional nerve blocks, scheduled NSAIDs, and opioid-based PCIA—the patient-controlled component remained centered on opioids. At 24 and 48 hours postoperatively, pain scores became comparable across the three groups, this finding consistent with studies by Yan et al35 and Zhao et al,18 likely attributable to the gradual wearing-off of local anesthetic effects. Although resting and dynamic pain scores converged after 48 hours, group differences in the OBAS persisted for a longer duration. As a composite endpoint, OBAS offers value beyond measuring pure pain intensity by integrating overall benefits and risk–benefit balance of an analgesic regimen, including analgesia quality, patient satisfaction, and opioid-related side effects.36 In the early postoperative period (24–48 hours), both the TPVB and ESPB groups showed significantly better OBAS scores than the Group Control (P < 0.001). Not only did these blocks provide superior analgesia, but the reduction in perioperative opioid requirements also lowered the incidence of PONV, the finding supported by Wang et al.37
Analysis of the AUC for QoR-15, NRS and OBAS indicated no statistically significant difference in the overall analgesic and recovery benefits between the TPVB and ESPB groups over the 72-hour postoperative period. This suggests that any early, minor advantages potentially offered by TPVB did not translate into a clinically relevant, sustained cumulative benefit. Therefore, the two techniques are equivalent in providing postoperative recovery and analgesic benefits. ESPB may hold unique practical appeal due to being quicker to perform. In this study, we observed that the SII at 24 hours postoperatively was lower in the TPVB group than in the ESPB group (MD: −307.92; 95% CI: −586.39 to −29.44; Adj-P = 0.025). The SII is a composite inflammatory marker, and it was measured at only a single postoperative time point in this study, precluding an assessment of the dynamic trajectory of the inflammatory response. A single marker cannot yet be considered to represent a clinically meaningful anti-inflammatory advantage. Therefore, we interpret this as a preliminary, mechanism-exploratory finding, suggesting that TPVB may differentially modulate the early surgical inflammatory response. However, this observation alone does not suffice to guide clinical decision-making.
The present study did not reveal significant differences in chronic pain among the three groups at 3 months postoperatively. The present study also observed one case of hypothermia (core temperature < 36 °C) in the Group TPVB despite comprehensive warming measures. The patient remained hemodynamically stable; this episode was likely attributable to vasodilation and increased heat loss following sympathetic blockade. Given the potential risks associated with hypothermia,38 future studies should consider focusing on thermal management in patients receiving major regional blocks.
This study has several limitations. First, we did not assess the actual dermatomal coverage of the nerve blocks, which may affect the precision of outcome interpretations. Nevertheless, hemodynamic changes during skin incision provided indirect evidence of blockade extent. We also acknowledge the limitations in our choice of the blockade level. The distal rectum and anal canal receive partial innervation from the sacral plexus, and the T10 level blocks employed in this study may not fully cover the pelvic nociceptive stimulation involved in low rectal surgery. Future studies could explore the effects of lumbar-level techniques, such as lumbar paravertebral block or erector spinae plane block, in colorectal surgical analgesia. Second, the sample size calculation was based on pilot data, and the observed intergroup differences in the primary outcome were smaller than anticipated; this may have resulted in insufficient statistical power to detect differences in secondary outcomes. Larger future studies are warranted to further delineate their comparative characteristics. Furthermore, an important methodological limitation is that our primary efficacy analyses were restricted to the PP population rather than a strict ITT population. Because post-randomization exclusions prevented complete outcome follow-up for these individuals, robust ITT sensitivity analyses could not be performed. Any post-randomization exclusion inherently introduces a potential risk of attrition bias. Consequently, this risk should be taken into consideration when interpreting the efficacy results of this trial. In addition, this study is that only preoperative CRP was measured, without assessing preoperative SII or postoperative CRP. Future studies should serially monitor both acute-phase proteins and cellular immune-inflammatory indices to more comprehensively delineate perioperative inflammatory and immunomodulatory trajectories. Finally, as a single-center, single-blind study conducted under specific inclusion and exclusion criteria, the generalizability of our findings may be limited.
Conclusions
In conclusion, this study confirms that in laparoscopic colorectal cancer surgery, both TPVB and ESPB are equally effective as core components of multimodal analgesia, significantly enhancing the quality of recovery, providing effective analgesia, and reducing opioid consumption. The overall benefits for postoperative recovery and analgesia are equivalent between the two block techniques. ESPB offers the technical advantages of being simpler to perform and requiring less time.
Abbreviations
ASA, American Society of Anesthesiologists; AUC, Area Under the Curve; BMI, Body Mass Index; CI, Confidence Interval; CONSORT, Consolidated Standards of Reporting Trials; CRP, C-reactive Protein; ERAS, Enhanced Recovery After Surgery; ESM, Erector Spinae Muscle; ESPB, Erector Spinae Plane Block; GEE, Generalized Estimating Equations; HR, Heart Rate; ICU, Intensive Care Unit; IQR, Interquartile Range; MAP, Mean Arterial Pressure; MCID, Minimal Clinically Important Difference; MD, Mean Difference; MME, Morphine Milligram Equivalents; NRS, Numeric Rating Scale; OBAS, Overall Benefit of Analgesia Score; PCIA, Patient-Controlled Intravenous Analgesia; PONV, Postoperative Nausea and Vomiting; PVS, Paravertebral Space; QoR-15, Quality of Recovery-15; SD, Standard Deviations; SII, Systemic Immune-Inflammation Index; TP, Transverse Process; TPVB, Thoracic Paravertebral Block.
Data Sharing Statement
The dataset generated and analysed during the current study is available from the corresponding author on reasonable request.
Informed Consent and Ethical Experimentation
The study involving humans was approved by the Medical Ethics Committee of Luoyang Central Hospital. The study was conducted in accordance with the local legislation and institutional requirements. Written informed consents for participation in this study were provided by the patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Health Commission of Henan Province [grant numbers 2023ZY3026].
Disclosure
The authors have no conflict of interest to disclose.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–15. doi:10.3322/caac.21834
2. Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233–254. doi:10.3322/caac.21772
3. Feng Q, Yuan W, Li T, et al. Robotic versus laparoscopic surgery for middle and low rectal cancer (REAL): short-term outcomes of a multicentre randomised controlled trial. Lancet Gastroenterol Hepatol. 2022;7(11):991–1004. doi:10.1016/S2468-1253(22)00248-5
4. Huang L, Zhang T, Wang K, Chang B, Fu D, Chen X. Postoperative multimodal analgesia strategy for enhanced recovery after surgery in elderly colorectal cancer patients. Pain Ther. 2024;13(4):745–766. doi:10.1007/s40122-024-00619-0
5. Gustafsson UO, Rockall TA, Wexner S, et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced recovery after surgery (ERAS) Society recommendations 2025. Surgery. 2025;184:109397. doi:10.1016/j.surg.2025.109397
6. Wick EC, Grant MC, Wu CL. Postoperative multimodal analgesia pain management with nonopioid analgesics and techniques: a review. JAMA Surg. 2017;152(7):691. doi:10.1001/jamasurg.2017.0898
7. Karmakar MK. Thoracic paravertebral block. Anesthesiology. 2001;95(3):771–780. doi:10.1097/00000542-200109000-00033
8. Melnikov AL, Bjoergo S, Kongsgaard UE. Thoracic paravertebral block versus transversus abdominis plane block in major gynecological surgery: a prospective, randomized, controlled, observer-blinded study. Local Reg Anesth. 2012;5:55–61. doi:10.2147/LRA.S35858
9. Zhang Q, Wu Y, An H, Feng Y. Postoperative recovery after breast cancer surgery: a randomised controlled trial of opioid-based versus opioid-free anaesthesia with thoracic paravertebral block. Eur J Anaesthesiol. 2023;40(8):552–559. doi:10.1097/EJA.0000000000001856
10. Madjdpour C, Chin KJ. Thoracic paravertebral blocks in abdominal surgery – a systematic review of randomized controlled trials. Br J Anaesth. 2016;117(3):297–308. doi:10.1093/bja/aew269
11. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–627. doi:10.1097/AAP.0000000000000451
12. Li Q, Zhang L, Zhou HM, Wu XW. Ultrasound-guided erector spinae plane block in elderly patients undergoing total hip arthroplasty: a triple-blind, randomized controlled trial. J Arthrop. 2025;40(4):999–1004. doi:10.1016/j.arth.2024.10.052
13. Oh SK, Lim BG, Won YJ, Lee DK, Kim SS. Analgesic efficacy of erector spinae plane block in lumbar spine surgery: a systematic review and meta-analysis. J Clin Anesth. 2022;78:110647. doi:10.1016/j.jclinane.2022.110647
14. Lin Z, Chen C, Xie S, Chen L, Yao Y, Qian B. Systemic lidocaine versus erector spinae plane block for improving quality of recovery after laparoscopic cholecystectomy: a randomized controlled trial. J Clin Anesth. 2024;97:111528. doi:10.1016/j.jclinane.2024.111528
15. Kekul O, Ustun YB, Kaya C, et al. Analgesic efficacy of the bilateral erector spinae plane block for colorectal surgery: a randomized controlled trial. J Anesth Analg Crit Care. 2022;2(1):43. doi:10.1186/s44158-022-00073-4
16. Aoyama Y, Sakura S, Tsuchiya R, Wittayapairoj A, Saito Y. Erector spinae plane block and paravertebral block for breast surgery: a retrospective propensity-matched noninferiority trial. J Pain Res. 2020;13:2367–2376. doi:10.2147/JPR.S265015
17. Zhu Y, Yang Y, Zhang Q, et al. Comparison of ultrasound-guided single-injection erector spinae plane block, retrolaminar block, and paravertebral block for postoperative analgesia in single-incision video-assisted thoracoscopic surgery: A 3-arm, double-blind, randomized controlled noninferiority trial. Clin J Pain. 2025;41(1):e1259. doi:10.1097/AJP.0000000000001259
18. Zhao H, Xin L, Feng Y. The effect of preoperative erector spinae plane vs. paravertebral blocks on patient-controlled oxycodone consumption after video-assisted thoracic surgery: a prospective randomized, blinded, non-inferiority study. J Clin Anesth. 2020;62:109737. doi:10.1016/j.jclinane.2020.109737
19. Mo X, Jiang T, Wang H, Zhang Y. Erector spinae plane block combined with serratus anterior plane block versus thoracic paravertebral block for postoperative analgesia and recovery after thoracoscopic surgery: a randomized controlled non-inferiority clinical trial. CURR MED SCI. 2023;43(3):615–622. doi:10.1007/s11596-023-2745-2
20. Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2019;140(8). doi:10.1161/CIR.0000000000000628
21. Bu XS, Zhang J, Zuo YX. Validation of the Chinese version of the quality of recovery-15 score and its comparison with the post-operative quality recovery scale. Patient. 2016;9(3):251–259. doi:10.1007/s40271-015-0148-6
22. Zhou S, Wang K, Yuan Q, et al. The role of sarcopenia in pre- and postoperative inflammation: implications of outcomes in patients with colorectal cancer. J Gastrointest Surg. 2024;28(11):1791–1798. doi:10.1016/j.gassur.2024.08.015
23. Koc R, Erdemoglu AK. Validity and reliability of the Turkish self-administered leeds assessment of neuropathic symptoms and signs (S-LANSS) questionnaire. Pain Med. 2010;11(7):1107–1114. doi:10.1111/j.1526-4637.2010.00837.x
24. Menyhart O, Fekete JT, Győrffy B. Inflammation and colorectal cancer: a meta-analysis of the prognostic significance of the Systemic Immune-Inflammation Index (SII) and the Systemic Inflammation Response Index (SIRI). Int J Mol Sci. 2024;25(15):8441. doi:10.3390/ijms25158441
25. Tan Y, Hu B, Li Q, Cao W. Prognostic value and clinicopathological significance of pre-and post-treatment systemic immune-inflammation index in colorectal cancer patients: a meta-analysis. World J Surg Onc. 2025;23(1):11. doi:10.1186/s12957-025-03662-z
26. Qi M, Xiao W, Yang S, et al. Pre-incisional preventive precise multimodal analgesia may enhance the rehabilitation process of acute postoperative pain following total laparoscopic hysterectomy: a randomized controlled trial. Pain Physician. 2023;26(3):E123–E131.
27. Kleif J, Waage J, Christensen KB, Gögenur I. Systematic review of the QoR-15 score, a patient- reported outcome measure measuring quality of recovery after surgery and anaesthesia. Br J Anaesth. 2018;120(1):28–36. doi:10.1016/j.bja.2017.11.013
28. Copik M, Bialka S, Daszkiewicz A, Misiolek H. Thoracic paravertebral block for postoperative pain management after renal surgery: a randomised controlled trial. Eur J Anaesthesiol. 2017;34(9):596–601. doi:10.1097/EJA.0000000000000673
29. Guran E, Kaplan O, Savlı S, Sonmez C, Dogan L, Unver S. Metabolomic profiling of erector spinae plane block for breast cancer surgery. Medicina. 2025;61(7):1294. doi:10.3390/medicina61071294
30. Yin ZY, Wang J, Wei P, et al. Impact of transcutaneous auricular vagus nerve stimulation on postoperative pain in patients undergoing perianal surgery: a randomized trial. Ann Med. 2025;57(1):2476045. doi:10.1080/07853890.2025.2476045
31. Yuan X, Tang Y, Xie X, et al. The effect of stellate ganglion block on postoperative recovery quality in peri-menopausal women undergoing gynecological laparoscopic surgery. Front Med Lausanne. 2025;12:1561512. doi:10.3389/fmed.2025.1561512
32. Cervero F. Neurophysiology of gastrointestinal pain. Baillieres Clin Gastroenterol. 1988;2(1):183–199. doi:10.1016/0950-3528(88)90027-9
33. Slinchenkova K, Lee K, Choudhury S, Sundarapandiyan D, Gritsenko K. A review of the paravertebral block: benefits and complications. Curr Pain Headache Rep. 2023;27(8):203–208. doi:10.1007/s11916-023-01118-1
34. Bonvicini D, Boscolo-Berto R, De Cassai A, et al. Anatomical basis of erector spinae plane block: a dissection and histotopographic pilot study. J Anesth. 2021;35(1):102–111. doi:10.1007/s00540-020-02881-w
35. Yan Z, Lin H, Yang Y, Yang J, Li X, Yao Y. Efficacy of ultrasound-guided thoracic paravertebral block on postoperative quality of recovery in patients undergoing percutaneous nephrolithotomy: a randomized double-blind placebo-controlled trial. J Pain Res. 2023;16:1301–1310. doi:10.2147/JPR.S405657
36. Lehmann N, Joshi GP, Dirkmann D, et al. Development and longitudinal validation of the overall benefit of analgesia score: a simple multi-dimensional quality assessment instrument. Br J Anaesth. 2010;105(4):511–518. doi:10.1093/bja/aeq186
37. Wang D, Liu Z, Zhang W, et al. Opioid-free anesthesia for quality of recovery score after surgery: a meta-analysis of randomized controlled trials. J Clin Anesth. 2025;103:111823. doi:10.1016/j.jclinane.2025.111823
38. Yoo JH, Sung TY, Oh CS. Cold temperatures, hot risks: perioperative hypothermia in geriatric patients - a narrative review. Anesth Pain Med. 2025;20(3):189–199. doi:10.17085/apm.25294
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.