Back to Journals » Drug Design, Development and Therapy » Volume 10
Effects of renal function on pharmacokinetics and pharmacodynamics of lesinurad in adult volunteers
Authors Gillen M, Valdez S, Zhou D, Kerr B, Lee CA, Shen Z
Received 17 August 2016
Accepted for publication 6 October 2016
Published 1 November 2016 Volume 2016:10 Pages 3555—3562
DOI https://doi.org/10.2147/DDDT.S119944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sukesh Voruganti
Michael Gillen,1 Shakti Valdez,2 Dongmei Zhou,2 Bradley Kerr,2 Caroline A Lee,2 Zancong Shen2
1AstraZeneca LP, Gaithersburg, MD, 2Ardea Biosciences, Inc., San Diego, CA, USA
Introduction: Lesinurad is a selective uric acid reabsorption inhibitor approved for the treatment of gout in combination with a xanthine oxidase inhibitor (XOI) in patients who have not achieved target serum uric acid (sUA) levels with an XOI alone. Most people with gout have chronic kidney disease. The pharmacokinetics, pharmacodynamics, and safety of lesinurad were assessed in subjects with impaired renal function.
Methods: Two Phase I, multicenter, open-label, single-dose studies enrolled subjects with normal renal function (estimated creatinine clearance [eCrCl] >90 mL/min; N=12) or mild (eCrCl 60–89 mL/min; N=8), moderate (eCrCl 30–59 mL/min; N=16), or severe (eCrCl <30 mL/min; N=6) renal impairment. Subjects were given a single oral lesinurad dose of 200 mg (N=24) or 400 mg (N=18). Blood and urine samples were analyzed for plasma lesinurad concentrations and serum and urine uric acid concentrations. Safety was assessed by adverse events and laboratory data.
Results: Mild, moderate, and severe renal impairment increased lesinurad plasma area under the plasma concentration–time curve by 34%, 54%–65%, and 102%, respectively. Lesinurad plasma Cmax was unaffected by renal function status. Lower renal clearance and urinary excretion of lesinurad were associated with the degree of renal impairment. The sUA-lowering effect of a single dose of lesinurad was similar between mild renal impairment and normal function, reduced in moderate impairment, and greatly diminished in severe impairment. Lesinurad increased urinary urate excretion in normal function and mild renal impairment; the increase was less with moderate or severe renal impairment. Lesinurad was well tolerated by all subjects.
Conclusion: Lesinurad exposure increased with decreasing renal function; however, the effects of lesinurad on sUA were attenuated in moderate to severe renal impairment.
Keywords: lesinurad, pharmacodynamics, pharmacokinetics, renal function, serum urate
Introduction
Gout is an inflammatory arthritis that results from high serum uric acid (sUA) levels, that is, hyperuricemia. In 80%–90% of patients, hyperuricemia results from inadequate excretion of uric acid.1,2 Hyperuricemia can lead to deposition of monosodium urate crystals in musculoskeletal structures, kidneys, and other tissues causing chronic inflammation, acute gout flares, and potentially chronic arthritis with joint damage and disfiguring tophi, kidney stones, and chronic kidney disease.
The recommendation for long-term management of gout is maintenance of sUA levels <6 mg/dL as a minimum and <5 mg/dL in cases of greater disease severity, using urate-lowering therapy (ULT).3 Allopurinol and febuxostat are xanthine oxidase inhibitors (XOIs) that block uric acid production and are recommended as first-line therapy for patients with gout.3–5 If the sUA target cannot be achieved with an XOI, treatment guidelines recommend combination therapy of an XOI with a uricosuric medication.3–5
Lesinurad 200 mg tablets have been approved by the United States Food and Drug Administration and by the European Medicines Agency for use in combination with an XOI for the chronic treatment of hyperuricemia associated with gout in patients who have not achieved target sUA levels with an XOI alone. Lesinurad inhibits the uric acid transporter URAT1 in the proximal tubules of the kidney,6 resulting in increased urinary excretion of uric acid and lower sUA.7,8 Seventy-one percent of patients with gout have chronic kidney disease.9
This report describes the pharmacokinetics (PK) and pharmacodynamics (PD) of a single dose of lesinurad in adult volunteers with various degrees of renal impairment. Results from this study helped determine inclusion/exclusion of patients with renal insufficiency to participate in the lesinurad Phase III clinical program.
Methods
The studies were designed and monitored in accordance with ethical principles of Good Clinical Practice as defined by the International Conference on Harmonisation and the Declaration of Helsinki. An institutional review board for each study site (Crescent City Institutional Review Board, New Orleans, LA, USA; Independent Institutional Review Board, Plantation, FL, USA; Schulman Associates Institutional Review Board, Durham, NC, USA) approved the protocol before trial commencement, and all subjects gave written informed consent.
Subjects
In the first study, both adult male and non-reproductive (post-menopausal or surgically sterile) female subjects, aged ≥18 years to ≤85 years, with body mass index (BMI) ≥18 kg/m2 and ≤40 kg/m2 and weight ≥50 kg, were eligible. Enrolled subjects were categorized as having mild or moderate renal impairment if their estimated creatinine clearance (eCrCl), determined by the Cockcroft–Gault formula at baseline, was 60–90 mL/min or 30 mL/min to <60 mL/min, respectively. Control subjects with eCrCl ≥90 mL/min were matched to those with renal impairment by age and BMI. Subjects who required dialysis for the treatment of renal disease were excluded. Subjects were not allowed to receive uricosuric medications (eg, probenecid and sulfinpyrazone) but could continue XOIs at the same dose throughout the study.
In the second study, male subjects, aged ≥18 years and ≤85 years, with BMI ≥18 kg/m2 and ≤40 kg/m2 and weight ≥50 kg, were eligible. Only male subjects were enrolled since gout is a disease that primarily occurs in males. Enrolled subjects were categorized as having moderate or severe impairment if their eCrCl at baseline was 30 mL/min to <60 mL/min or 15–30 mL/min, respectively. Control subjects with eCrCl ≥90 mL/min were matched to those with renal impairment by age, BMI, and CYP2C9 metabolizer phenotype. Poor metabolizer subjects with homozygous CYP2C9 polymorphism (eg, *2/*2 and *3/*3) or with compound heterozygous CYP2C9 polymorphisms (ie, both *1/*2 and *1/*3) and subjects who required dialysis for treatment of renal disease were excluded to ensure that comparisons of PK and PD between renal function categories were not confounded by an isolated poor metabolizer. Subjects receiving XOIs, including allopurinol and febuxostat, and those receiving uricosuric medications, including probenecid and sulfinpyrazone, and those indicated for the treatment of gout with hyperuricemia were excluded from the study.
Study design
Both studies were Phase I, multicenter, open-label, single-dose studies. Screening procedures to determine subject eligibility were performed within 21–28 days prior to dosing. Enrollment was in cohorts based on their eCrCl status. The normal renal function cohorts were enrolled after the other cohorts in order to match the baseline characteristics of age, gender, weight, and BMI to those subjects enrolled in the other cohorts. Subjects checked into the study center on Day −2 and stayed until the last study procedures had been completed 72 hours (Day 4) after dosing on Day 1. All subjects had a follow-up visit on Day 8±1.
A lesinurad 200 mg dose (first study) or 400 mg dose (second study) was administered to all subjects in the morning on Day 1 after an 8-hour fast; a snack was provided 1 hour after dosing.
PK assessment
Blood and urine samples, collected at pre-specified times, were analyzed for lesinurad concentrations by Ardea Biosciences, Inc. (San Diego, CA, USA). Plasma samples were prepared by protein precipitation and urine samples by dilution; both were quantified using high-performance liquid chromatography with tandem mass spectroscopy (LC MS/MS). Plasma protein binding of lesinurad was evaluated by adding [14C]lesinurad to plasma samples and measuring the unbound fraction by equilibrium dialysis.
PK parameters for lesinurad were calculated using non-compartmental analysis. Plasma PK parameters included maximum observed plasma concentration (Cmax), time to Cmax (Tmax), and area under the plasma concentration–time curve (AUC) from zero to infinity (AUC0–∞). Half-life (t1/2) was not reported; most individual values were considered unreliable as they were calculated over a time interval that was less than twice the calculated value. Despite the unreliable t1/2, AUC0–∞ was deemed reliable since <2% was extrapolated. AUC was calculated using the linear trapezoidal rule. The apparent oral clearance (CL/F) was also determined.
Urinary PK parameters included the amount of lesinurad excreted unchanged in urine over a time interval (Ae), the fraction of the lesinurad dose (% dose) excreted unchanged in urine following dosing (fe), and the renal clearance of lesinurad (CLR). Ae was calculated as concentration measured × volume, while CLR was calculated as Ae divided by plasma AUC over the same time interval. PK parameters were derived using WinNonlin Professional, version 5.2 (Pharsight Corporation, Mountain View, CA, USA).
PD assessment
Blood and urine samples were collected at specific times during the study for the measurement of serum and urinary concentrations of uric acid and creatinine. Urate in serum and urine samples was analyzed by a colorimetric and an enzymatic method in the first and second study, respectively. Serum creatinine concentrations were determined using an enzymatic method.
The PD parameters for uric acid in urine were determined using procedures (SAS Institute Inc., Cary, NC, USA). The amount of uric acid recovered in urine (AeUR) was calculated as the product of urine concentration of uric acid and urine volume. Renal clearance of uric acid (CLUR) was calculated as AeUR divided by plasma urate AUC over the same time interval, while the fractional excretion of uric acid (FEUA) was calculated as (CLUR/CrCl) ×100.
Safety assessment
Subjects were monitored throughout the study and any adverse events (AEs) or remedial actions were recorded in the subject’s clinical report form. The severity of an AE was assessed by the investigator according to Rheumatology Common Toxicity Criteria (RCTC) version 2.0. Blood and urine samples were collected for clinical laboratory evaluations at specific times during the study. Supine blood pressure, pulse rate, respiratory rate, and oral body temperature were also measured at specific times during the study. A physical examination was performed at Day −2 and at follow-up. Standard digital 12-lead electrocardiograms (ECGs) were recorded at specific times during the study to detect any immediate ECG effects. These ECGs were viewed by the investigator locally.
Statistical analyses
The PK population consisted of all subjects who received lesinurad and had evaluable PK data, while the PD population consisted of all subjects who received lesinurad and had evaluable PD data. The safety population consisted of all subjects who received lesinurad.
To assess the effect of renal impairment on the plasma and urine PK of lesinurad, the natural log-transformed PK parameters for mild, moderate, or severe renal impairment groups were compared against the normal renal function group. An estimate of the geometric mean ratios of the PK parameters with the corresponding 90% CIs was generated.
Descriptive statistics for PD and safety population data included N, arithmetic mean, minimum, maximum, and standard errors.
Results
Subject disposition and baseline characteristics
There were 24 subjects who entered and completed the first study and 18 subjects who entered and completed the second study. When subjects were categorized for renal function based on their baseline eCrCl, six subjects in the first study were classified as having normal renal function, eight having mild renal impairment, and ten having moderate renal impairment. In the second study, six subjects were classified as having normal renal function, six having moderate renal impairment, and six having severe renal impairment. The demographic characteristics of subjects are shown by renal function status and lesinurad dose in Table 1. Subjects given lesinurad 200 mg were generally older, had lower BMI, and were predominantly white compared with those given lesinurad 400 mg. Mean plasma protein binding of lesinurad ranged from 98.4% to 99.0% with no apparent differences between groups.
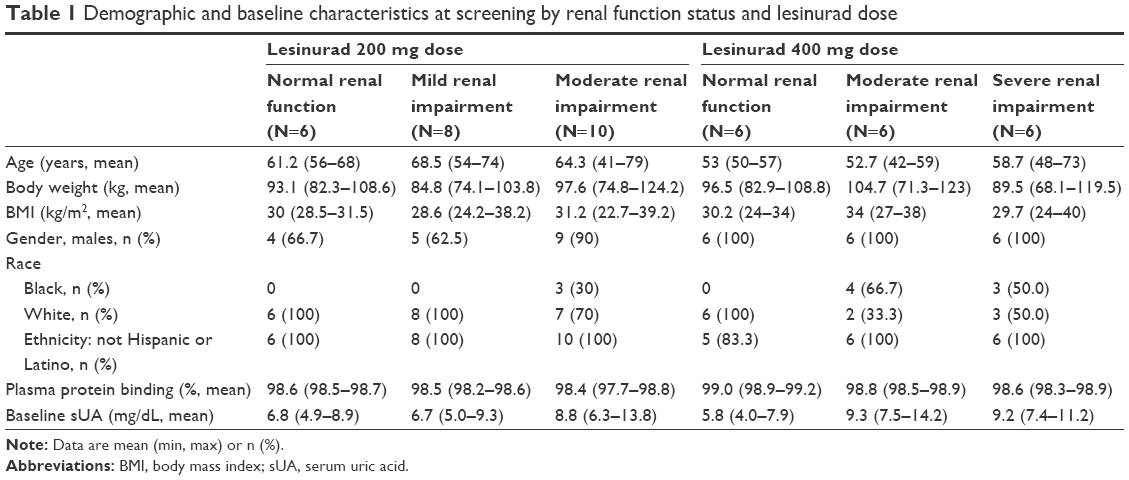 | Table 1 Demographic and baseline characteristics at screening by renal function status and lesinurad dose |
PK
The plasma concentration–time profiles of a single dose of lesinurad 200 or 400 mg in subjects with various degrees of renal function are shown in Figure 1, and a summary of plasma and urinary lesinurad PK parameters is presented in Table 2. Tmax was generally unchanged by renal function status. Cmax changed little with increasing renal insufficiency, while AUC0–∞ increased as renal function declined (Table 2). Compared with subjects with normal renal function, the geometric mean plasma Cmax increased by 41% following a lesinurad 200 mg dose in subjects with mild impairment; however, the 95% CIs largely overlapped between the two groups. Cmax was unchanged with moderate renal impairment following a lesinurad 200 mg dose and with moderate or severe renal impairment following a lesinurad 400 mg dose (Table 3). The geometric mean AUC0–∞ for the lesinurad 200 mg dose increased 34% with mild renal impairment and 65% with moderate renal impairment. For the lesinurad 400 mg dose, the increase was 54% and 102% with moderate and severe renal impairment, respectively.
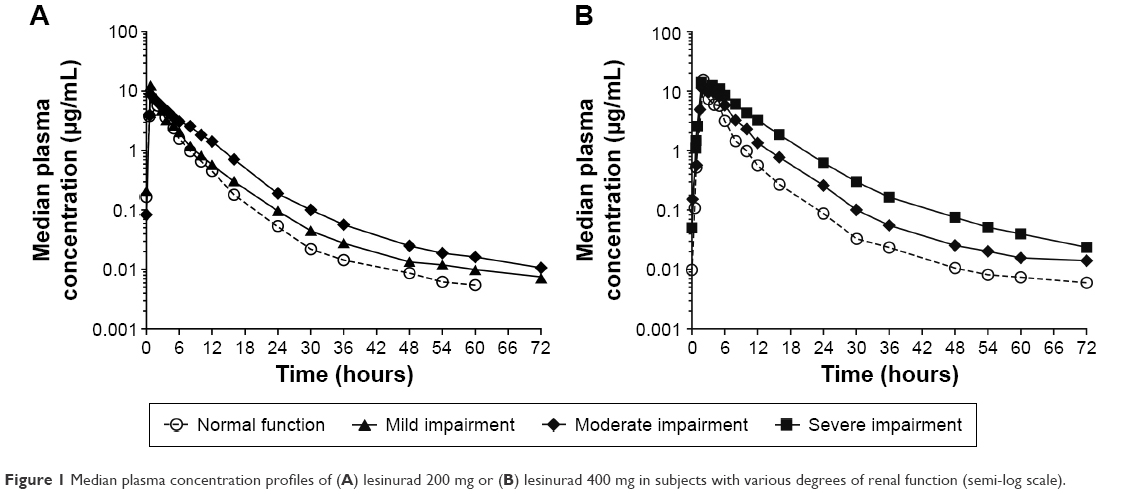 | Figure 1 Median plasma concentration profiles of (A) lesinurad 200 mg or (B) lesinurad 400 mg in subjects with various degrees of renal function (semi-log scale). |
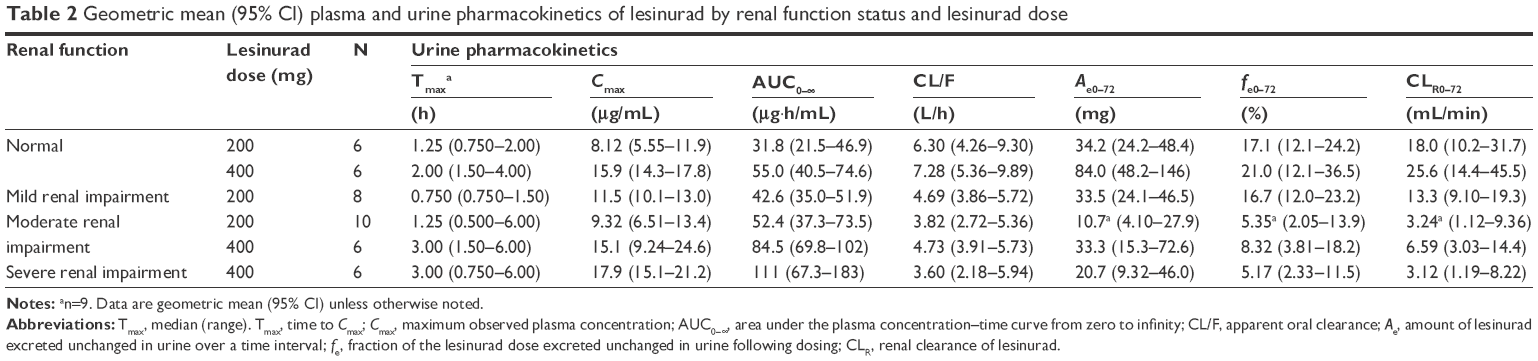 | Table 2 Geometric mean (95% CI) plasma and urine pharmacokinetics of lesinurad by renal function status and lesinurad dose |
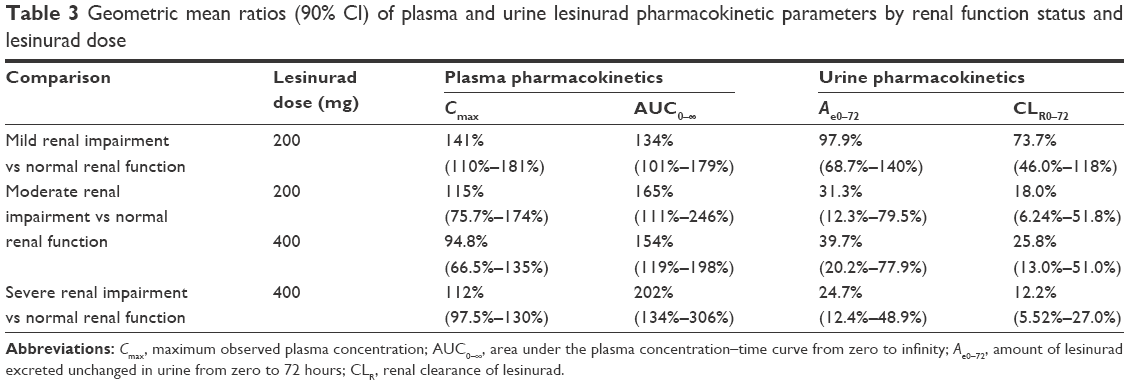 | Table 3 Geometric mean ratios (90% CI) of plasma and urine lesinurad pharmacokinetic parameters by renal function status and lesinurad dose |
The amount of the lesinurad 200 mg dose excreted in urine was unchanged with mild renal impairment, but decreased by 69% with moderate impairment. The decrease was 60% and 75% with moderate and severe renal impairment following a lesinurad 400 mg dose. Lesinurad renal clearance was reduced by 26% and 82% with mild and moderate renal impairment, respectively, following a lesinurad 200 mg dose and by 74% and 88% with moderate and severe impairment, respectively, following a lesinurad 400 mg dose (Table 3).
The relationship between the Cmax, AUC, total clearance, and renal clearance of lesinurad and creatinine clearance (CrCl) is shown in Figure 2. Compared with Cmax, AUC had a stronger upward trend as renal function declined, whereas total clearance and renal clearance both had downward trends with declining renal function.
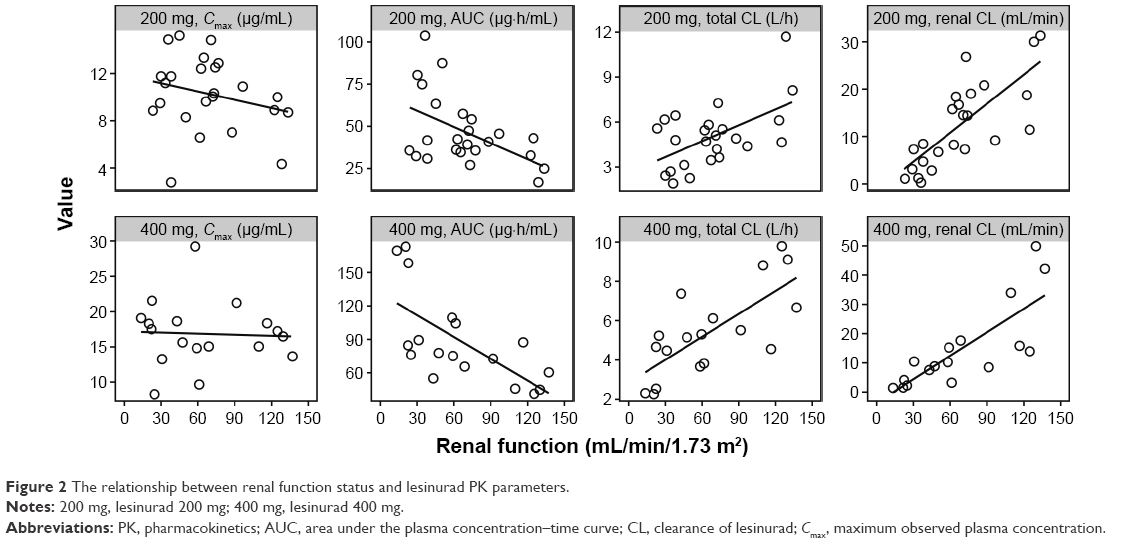 | Figure 2 The relationship between renal function status and lesinurad PK parameters. |
PD
Higher mean pre-dose sUA levels were observed for subjects with moderate and severe renal impairment (9.4 mg/dL and 9.1 mg/dL, respectively) compared with those with mild impairment or normal renal function (6–7 mg/dL). The changes from baseline sUA concentration–time profiles following a single dose of lesinurad 200 mg or 400 mg in subjects with various degrees of renal function are shown in Figure 3. With the 200 mg dose, sUA lowering was similar (maximum reduction ~22%) in mild impairment and with normal function, but the sUA lowering was attenuated in the moderate renal function group (maximum reduction ~8%). With the 400 mg dose, maximum sUA reduction was 28% in the normal renal function group, 17% in the moderate impairment group, and 6% with severe impairment.
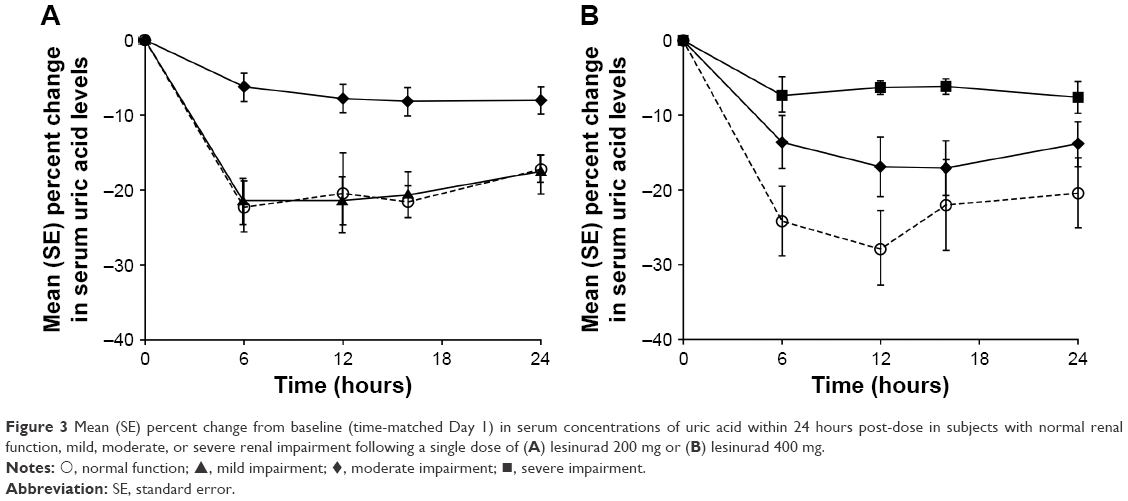 | Figure 3 Mean (SE) percent change from baseline (time-matched Day 1) in serum concentrations of uric acid within 24 hours post-dose in subjects with normal renal function, mild, moderate, or severe renal impairment following a single dose of (A) lesinurad 200 mg or (B) lesinurad 400 mg. |
PD parameters for urinary uric acid are summarized in Table 4. In the absence of any treatment, Ae and CLUR were lower with decreasing renal function status, while FEUA remained relatively constant. Treatment with lesinurad 200 mg or 400 mg increased mean Ae, CLUR, and FEUA regardless of renal function status, but the absolute values for Ae and CLUR decreased as renal function declined.
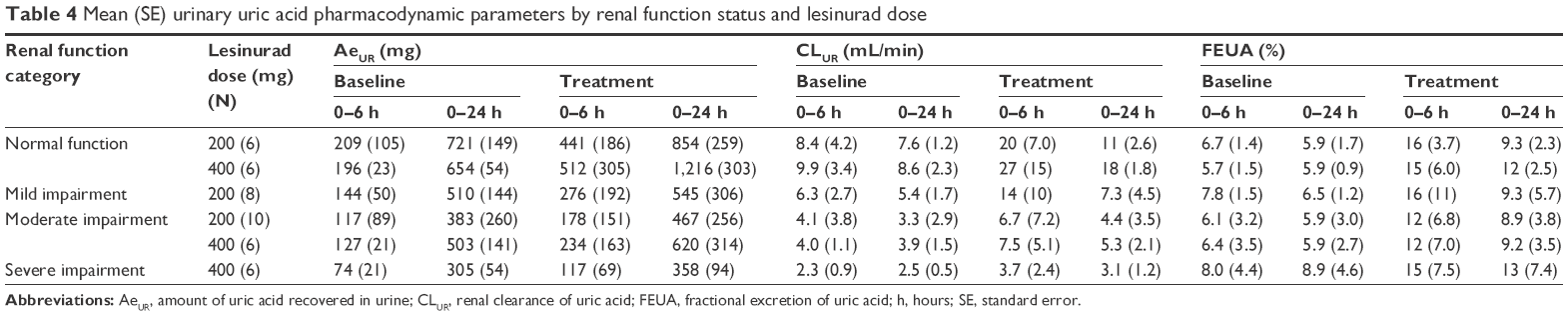 | Table 4 Mean (SE) urinary uric acid pharmacodynamic parameters by renal function status and lesinurad dose |
Safety
Lesinurad was well tolerated by all subjects, with few AEs reported. One moderate renal impairment subject, who had multiple comorbidities and co-medications, experienced Grade 1 (mild) acute renal failure 10 days after a 200 mg dose of lesinurad; the event resolved after ~3 days. At the time of this event, the subject also experienced Grade 3 (severe) hyperkalemia, which resolved after 2 days. The investigator considered that it was unlikely that the renal failure or the hyperkalemia was related to lesinurad and suggested an alternative etiology of concomitant administration of excess diuretics. Following a 400 mg dose, five treatment-emergent AEs were reported, all of which were reported by two subjects with moderate renal impairment. One subject reported musculoskeletal pain (left and right shoulders) and gouty arthritis, of which gouty arthritis was possibly related to lesinurad. The other subject reported arthralgia which was also rated as possibly related to lesinurad. Other than the expected decrease in sUA levels, no clinically significant changes in laboratory values were observed, except for one subject who experienced two episodes of hypoglycemia that were possibly related to lesinurad. There were no changes in mean serum creatinine following administration of a single dose of lesinurad. There were no clinically significant findings for vital signs, ECG, and physical examinations.
Discussion
Most patients with gout also have chronic kidney disease, therefore, it was important to assess the PK and PD of lesinurad to better understand its potential efficacy in people with different degrees of renal impairment. In this study, mild, moderate, and severe renal impairment increased lesinurad AUC by 34%, 54%–65%, and 102%, respectively. Lesinurad Cmax was not affected by renal impairment status at either the 200 mg or 400 mg dose. The lack of effect on Cmax is consistent with the mechanism of renal impairment status, where drug elimination is mostly affected, as demonstrated by the prolonged half-life of lesinurad. Urinary excretion of lesinurad was ~36%–66% lower with moderate renal impairment and ~81% lower in severe renal impairment compared with subjects with normal renal function. The increase in plasma AUC exposure of lesinurad is therefore consistent with reduced renal elimination due to renal impairment.
The site of URAT1 inhibition by lesinurad is in the apical membrane of the kidney proximal tubule and the most relevant concentration of lesinurad associated with the sUA lowering is likely the unbound concentration of lesinurad in the urinary lumen of the proximal tubule. The degree of sUA lowering was similar in mild renal impaired subjects compared with normal renal function, but although sUA lowering was attenuated in subjects with moderate renal impairment, it was considered to be adequate to study them in Phase III. However, sUA lowering was greatly diminished in subjects with severe renal impairment and these subjects were deemed not appropriate for enrollment in Phase III studies.
Uric acid is primarily eliminated by the kidney via filtration. As renal function declined, the amount of uric acid excreted in urine decreased along with CLR at baseline because of the decreased filtration of uric acid. Following administration of lesinurad, the amount of uric acid excreted increased as did CLR and FEUA due to inhibition of URAT1 but the effects were less than that observed in subjects with normal kidney function. Thus, a subject with greater renal insufficiency will have less uric acid available for reabsorption via URAT1, and the extent of inhibition by lesinurad is diminished.
Possible limitations of these studies were the almost exclusive inclusion of male subjects and that it was only a single-dose administration. However, safety and efficacy of lesinurad have been studied with long-term administration in subjects with normal, mild, and moderate renal impairment in Phase 3 studies, which also did include females with gout.10 Therefore, based on those data, the product was approved for use in mild and moderate impairment without any dose adjustment,11,12 although, in the US, lesinurad is not recommended for use in subjects with eCrCL <45 mL/min due to the limited amount of data in that population.
Conclusion
Lesinurad exposure increased with decreasing renal function; although sUA lowering in mild impairment was similar to normal kidney function, it was attenuated in moderate and severe renal impaired subjects. The effect of renal function and efficacy associated with lesinurad dosing from this investigation provided valuable inclusion/exclusion information for Phase 3 study design. Thus, Phase III studies did not enroll subjects with severe renal impairment and the treatment groups were balanced based on renal function (eCrCL).
Acknowledgments
Funding was provided by Ardea Biosciences/AstraZeneca. Editorial support was provided by Tom Claus, PhD, of PAREXEL and was funded by AstraZeneca. Ardea Biosciences is a member of the AstraZeneca group.
Disclosure
M Gillen is an employee of AstraZeneca. S Valdez, D Zhou, CA Lee, and Z Shen are employees of Ardea Biosciences, Inc. B Kerr is a paid consultant of Ardea Biosciences, Inc. The authors report no other conflicts of interest in this work.
References
Neogi T. Clinical practice. Gout. N Engl J Med. 2011;364(5):443–452. | ||
Terkeltaub R, Edwards NL. Gout: Diagnosis and Management of Gouty Arthritis and Hyperuricemia. 3rd ed. West Islip, NY: Professional Communications, Inc.; 2013. | ||
Khanna D, Fitzgerald JD, Khanna PP, et al. 2012 American College of Rheumatology guidelines for management of gout. Part 1: systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Arthritis Care Res (Hoboken). 2012;64(10):1431–1446. | ||
Richette P, Doherty M, Pascual E, et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheum Dis. Epub 2016 Jul 25. | ||
Zhang W, Doherty M, Bardin T, et al. EULAR evidence based recommendations for gout. Part II: management. Report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis. 2006;65(10):1312–1324. | ||
Bobulescu IA, Moe OW. Renal transport of uric acid: evolving concepts and uncertainties. Adv Chronic Kidney Dis. 2012;19(6):358–371. | ||
Fleischmann R, Kerr B, Yeh LT, et al. Pharmacodynamic, pharmacokinetic and tolerability evaluation of concomitant administration of lesinurad and febuxostat in gout patients with hyperuricaemia. Rheumatology (Oxford). 2014;53(12):2167–2174. | ||
Girardet J-L, Miner JN. Urate crystal deposition disease and gout – new therapies for an old problem. Annu Rep Med Chem. 2014;49:151–164. | ||
Zhu Y, Pandya BJ, Choi HK. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007–2008. Am J Med. 2012;125(7):679–687. | ||
Saag KG, Fitz-Patrick D, Kopicko J, et al. Lesinurad combined with allopurinol: randomized, double-blind, placebo-controlled study in gout subjects with inadequate response to standard of care allopurinol (a US-based study). Arthritis Rheumatol. Epub 2016, Aug 26. | ||
ZURAMPIC® (lesinurad) tablets [prescribing information]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2016. Available from: http://www.azpicentral.com/zurampic/zurampic.pdf. Accessed July 22, 2016. | ||
ZURAMPIC® (lesinurad) tablets [summary of product characteristics]. London, UK: AstraZeneca UK LTD; 2016. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/003932/WC500203066.pdf. Accessed July 22, 2016. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.