Back to Journals » Drug Design, Development and Therapy » Volume 19
Effects of Oliceridine Versus Sufentanil on Hemodynamic Stability in Elderly Hypertensive Patients During Laryngeal Mask Airway Anesthesia: A Randomized Controlled Trial
Authors Chen L ![]() , Xie K, Ji K, Long M, Zhang Y, He K
, Xie K, Ji K, Long M, Zhang Y, He K ![]()
Received 18 June 2025
Accepted for publication 10 October 2025
Published 22 October 2025 Volume 2025:19 Pages 9515—9522
DOI https://doi.org/10.2147/DDDT.S547901
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leonidas Panos
Lvlv Chen,1 Kangjie Xie,2 Kuiquan Ji,1 Mingbo Long,1 Yongguo Zhang,1 Kai He1
1Department of Anesthesiology, People’s Hospital of Qiannan, Duyun, 558000, People’s Republic of China; 2Department of Anesthesiology, First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 330300, People’s Republic of China
Correspondence: Yongguo Zhang, Department of Anesthesiology, People’s Hospital of Qiannan, Duyun, 558000, People’s Republic of China, Tel +86 18685405635, Email [email protected] Kai He, Department of Anesthesiology, People’s Hospital of Qiannan, Duyun, 558000, People’s Republic of China, Tel +86 18085408359, Email [email protected]
Purpose: To evaluate the efficacy and safety of low-dose oliceridine versus sufentanil in maintaining hemodynamic stability during laryngeal mask airway (LMA) general anesthesia in elderly hypertensive patients.
Patients and Methods: A prospective, double-blind, randomized controlled trial was conducted with 80 elderly hypertensive patients (aged ≥ 65 years, SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg). Participants were randomized into two groups: the oliceridine group (Group O, n = 40) and the sufentanil group (Group S, n = 40). Hemodynamic parameters (SBP, DBP, MAP, HR) were recorded at baseline, after drug administration, and post-LMA placement. Adverse events (eg, hypotension, hypertension, nausea/vomiting) were analyzed using Chi-square or Fisher’s exact tests.
Results: Compared with sufentanil, oliceridine significantly reduced the hemodynamic fluctuations after laryngeal mask insertion. Specifically, the variability of mean arterial pressure (MAP) decreased ((ΔMAP: − 4.8 ± 3.4 mmHg vs − 15.7 ± 10.5 mmHg, mean difference: 10.9mmHg, 95% CI: 7.4 to 14.3 mmHg, P = 0.000). Although there was no significant difference in intubation response rate between the two drugs (7.5% vs 10.0%, P = 0.236), oliceridine demonstrated better safety profile, with no occurrence of nausea or vomiting (0% vs 7.5%, P = 0.076).
Conclusion: Oliceridine may offer a safer alternative for hemodynamically fragile elderly patients during LMA anesthesia.
Keywords: elderly, hemodynamic stability, hypertension, laryngeal mask airway, oliceridine, randomized controlled trial
Introduction
Epidemiological studies indicate that as the population ages, more than 60% of individuals aged 60 and older are affected by hypertension.1 The pathophysiological mechanism is that arteriosclerosis weakens the buffering capacity of blood vessels, autonomic nerve dysfunction weakens the pressure reflex response; and endothelial dysfunction aggravates blood pressure fluctuations. These factors can substantially elevate the risk of perioperative complications in elderly patients, including myocardial ischemia2 and postoperative cognitive dysfunction.3 In essence, the conjunction of age-related declines in cardiovascular function and anesthesia-induced hemodynamic changes presents significant challenges for managing perioperative anesthesia in elderly hypertensive patients.2,4,5
A case-control study demonstrated that compared with tracheal intubation, laryngeal mask airway (LMA) in general anesthesia can reduce the stress response caused by tracheal intubation operation.6 Therefore, for patients who may have a strong reaction to intubation, such as those with hypertension, laryngeal mask general anesthesia is a relatively reasonable choice for most surgeries. However, its inhibitory effect on pharyngeal reflex is limited. Moreover, it may even aggravate sympathetic nerve activation during airway operation, leading to significant blood pressure fluctuations (in 38% of cases, systolic blood pressure [SBP] variation exceeded 20 mmHg).7 This clinical phenomenon reveals that for vulnerable patient groups such as elderly hypertensive patients, general anesthesia with LMA may require analgesic drugs that can stably control hemodynamic responses.
Conventional opioids such as sufentanil have shown significant efficacy in controlling nociceptive pain, but the therapeutic window in elderly patients is extremely limited. Multiple studies have confirmed that due to age-related factors, the activity of hepatic cytochrome P450 3A4 (CYP3A4) in adults over 65 years old decreases by 30% to 50%.8 Additionally, the autonomic compensatory function also weakens accordingly.9 This significantly increases the risk of dose-dependent hypotension (incidence rate of 30% to 45%),10 and respiratory depression (18% to 27%).11
Oliceridine (TRV130), an FDA-approved novel μ-opioid receptor (MOR) biased agonist since 2020 for acute pain management, demonstrates G protein-biased signaling. By preferentially activating G protein-coupled signaling over the β-arrestin pathway,12 it achieves analgesic efficacy comparable to morphine. Phase III drug studies suggest it reduces the risk of respiratory depression by 52%13 and the incidence of hypotension by 40%. Despite its pharmacological advantages, clinical adoption faces challenges including formulary access limitations and substantially higher acquisition costs (8-fold vs conventional opioids) in many healthcare systems.14 Recent pharmacokinetic models indicate that oliceridine has a context-sensitive half-life (CSHT) of 1.7 hours,15 which enables rapid titration - a key advantage for hemodynamically fragile patients. However, evidence regarding its application in laryngeal mask anesthesia in elderly hypertensive patients, particularly in terms of its interaction with the inherent vagal stimulation during supraglottic airway placement (eg, activation of the laryngopharyngeal reflex), remains scarce. This randomized controlled trial fills these gaps by systematically evaluating the hemodynamic stability characteristics of oliceridine vs sufentanil in this high-risk surgical setting.
Materials and Methods
Study Design
The present study was approved by the Ethics Committee of the People’s Hospital of Qiannan Prefecture and registered at https://www.chictr.org.cn/ (registration number: ChiCTR2500099243). The sample size was calculated using SPSS 26.0 software based on an anticipated mean MAP difference of 10 mmHg between groups, a significance level (α) of 0.05, a power (1-β) of 0.8, and an anticipated dropout rate of 20% for a two-sided test. From April 2025 to May 2025, 80 elderly hypertensive patients scheduled for ureteroscopic lithotripsy (URL) were randomly assigned into two groups: the Oliceridine group (Group O) and the Sufentanil group (Group S), with 40 cases in each group (Figure 1). Both participants and outcome assessors were blinded to group allocation.
 |
Figure 1 The study flowchart. |
Participants
- Inclusion Criteria: Age ≥65 years, diagnosed hypertension (SBP ≥140 mmHg/DBP ≥90 mmHg), ASA II–III.
- Exclusion Criteria: Severe organ dysfunction, opioid allergy.
Randomization and Blinding
Participants were stratified by ASA class (II vs III) and randomized 1:1 via computer-generated blocks (block size 4) to:
- Group O (Oliceridine): Induction with oliceridine 0.04 mg·kg−¹ (Jiangsu Enhua Humanwell Pharmaceuticals) diluted in 10 mL saline, administered over 2 minutes.
- Group S (Sufentanil): Induction with sufentanil 0.3 μg·kg−¹ (Yichang Humanwell Pharmaceuticals) diluted equivalently.
Anesthesia induction typically uses sufentanil at 0.3 μg/kg. The potency of oliceridine is approximately 5- to 10-fold that of morphine, and the potency of sufentanil is typically 500- to 1000-fold that of morphine (intravenous route). Based on potency conversion, a dose of oliceridine 0.04 mg/kg was determined.
All study drug solutions were prepared by an independent pharmacist using identical syringes. Patients, anesthesiologists, and outcome assessors were blinded to group allocation.
Anesthesia Protocol
- Induction: Propofol (Jiangsu Yingke Humanwell Pharmaceuticals) 1.5 mg/kg IV administered 90 seconds after study drug injection. LMA (LMA® Supreme™, size 3–5) was placed by senior anesthesiologists upon loss of eyelash reflex.
- Maintenance: Sevoflurane (1.0–1.5 MAC) was titrated to BIS 40–60. Neuromuscular blocking agents were avoided.
- Rescue: Ephedrine 6 mg IV for SBP <90 mmHg; nitroglycerin 0.5 μg/kg/min for SBP >160 mmHg.
Outcome Measures
- Primary: Hemodynamic parameters including systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), heart rate (HR), were recorded at baseline (T0), after drug administration (T1), and post-LMA placement (T2).
- Secondary: Adverse events (hypotension, hypertension, nausea/vomiting).
- Adverse events including nausea/vomiting were assessed by blinded anesthesiologists through:
- Direct observation during induction and recovery.
- Structured patient questioning at 15-min intervals for 2 hours postoperatively.
- Documentation of any emetic episodes or antiemetic requirements.
Statistical Analysis
Data analyzed were using SPSS 26.0 (SPSS Inc., Chicago, Illinois, USA). Continuous variables were assessed for normality using the Shapiro–Wilk test. Normally distributed data are presented as mean ± standard deviation (SD), while non-normally distributed data are summarized as median [interquartile range, IQR]. Categorical variables are reported as numbers (n) and percentages (%).
Continuous variables were compared using independent t-tests or repeated-measures analysis of variance (ANOVA). Mauchly’s test was employed to assess the sphericity assumption. If this assumption was violated, the Greenhouse-Geisser correction was applied to adjust the degrees of freedom. The equality of variances for between-group comparisons was verified using Levene’s test. If this assumption was violated, Welch’s t-test (for two groups) or Welch’s ANOVA with Games-Howell post-hoc tests (for multi-group comparisons) was used instead of the standard tests. Categorical variables were compared using Chi-square/Fisher’s exact tests.
A P value < 0.05 was deemed statistically significant. Data points exceeding ±3 standard deviations from the mean were reviewed for measurement error; none were excluded as all reflected valid clinical recordings.
Results
- There were no statistically significant differences in demographic characteristics, ASA classification, surgery time, or anesthesia time between the two groups. Figure 1 illustrates the study flowchart, and baseline characteristics are presented in Table 1.
- Compared to the sufentanil group (Group S), the oliceridine group (Group O) exhibited smaller hemodynamic fluctuations, indicating better maintenance of circulatory stability. Post-LMA placement, Group O showed smaller MAP fluctuations (ΔMAP: −4.8 ± 3.4 mmHg vs −15.7 ± 10.5 mmHg, Mean difference: 10.9mmHg, 95% CI: 7.4 to 14.3 mmHg, P = 0.000). Figure 2 illustrate the hemodynamic parameter comparisons.
- As shown in Table 2, there was no statistically significant difference in the intubation response between the oliceridine group (Group O) and the sufentanil group (Group S). However, oliceridine demonstrated a better safety profile, with no occurrence of nausea or vomiting (0% vs 7.5%, P = 0.076).
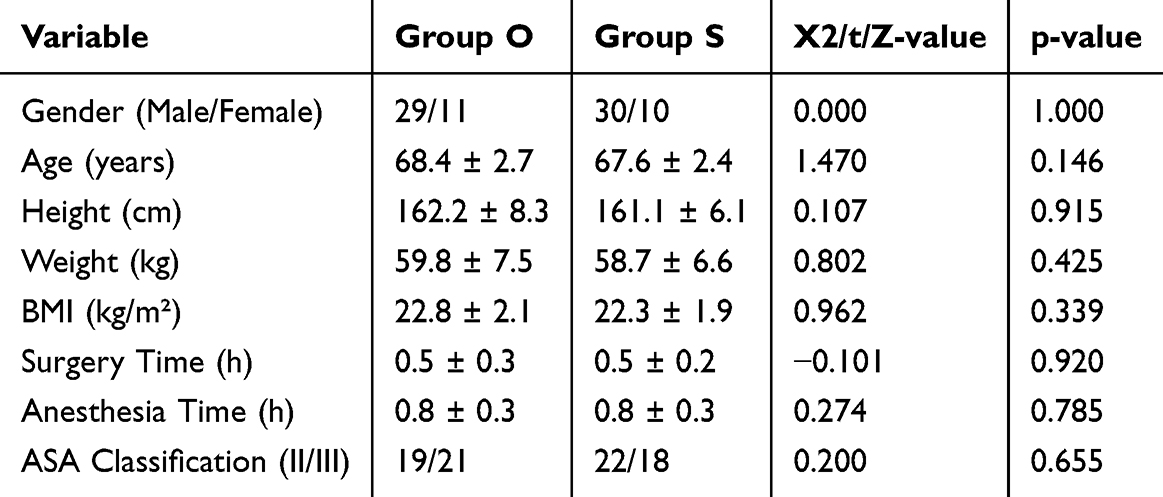 |
Table 1 Characteristics of the Study Population |
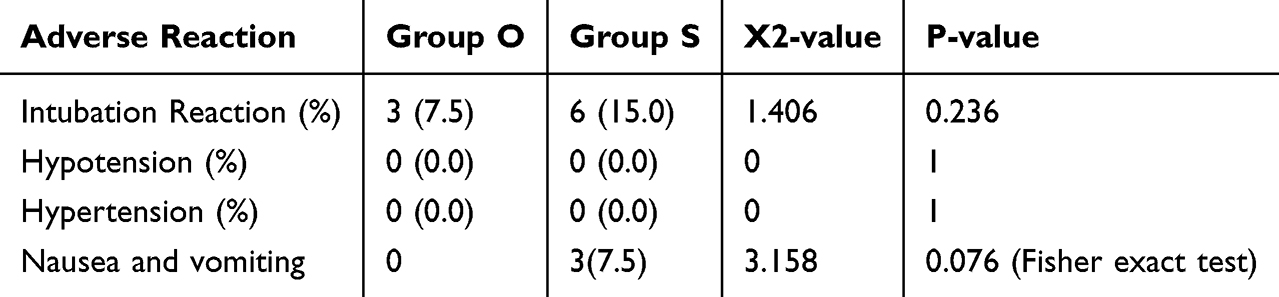 |
Table 2 Comparison of the Number of Cardiovascular Adverse Events During Anesthesia Induction (n=40) |
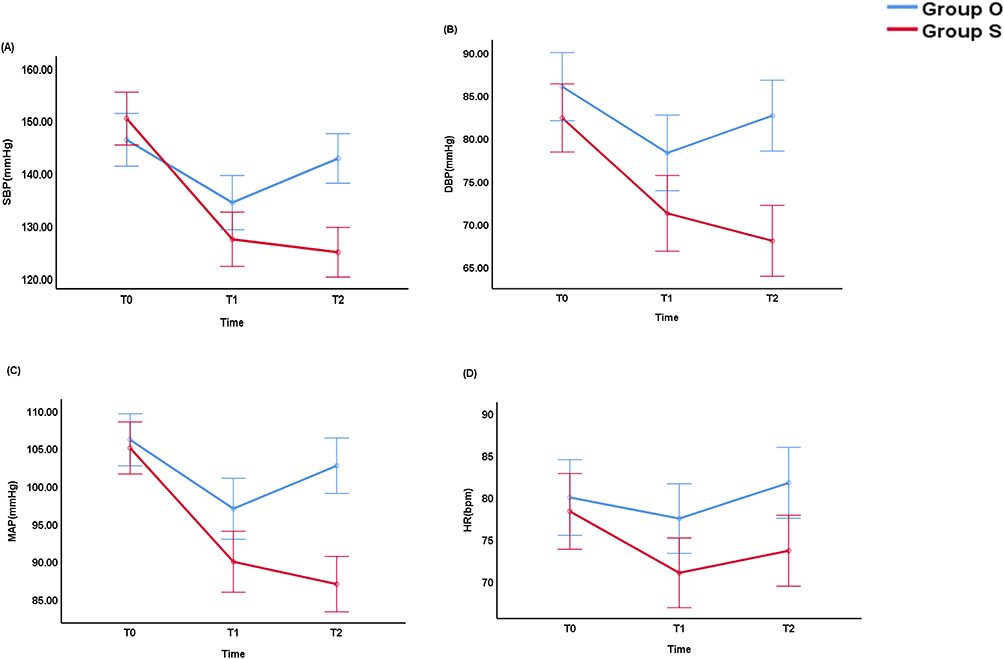 |
Figure 2 The hemodynamic parameter comparisons. (A) SBP Reduction at T2 (After Laryngeal Mask Insertion): Mean difference in ΔSBP (Group O - Group S): −15.2 mmHg (95% CI: −20.1 to −10.3), P = 0.000. (B) DBP Reduction At T1 (After Drug Administration): Mean difference in ΔDBP: −5.8 mmHg (95% CI: −10.6 to −1.0), P = 0.019. At T2 (After Laryngeal Mask Insertion): Mean difference in ΔDBP: −8.9 mmHg (95% CI: −13.5 to −4.3), P = 0.000. (C) MAP Reduction: At T1 (After Drug Administration): Mean difference in ΔMAP: −6.5 mmHg (95% CI: −11.0 to −2.0), P = 0.006. At T2 (After Laryngeal Mask Insertion): Mean difference in ΔMAP:10.9mmHg, 95% CI: 7.4 to 14.3 mmHg, P = 0.000. (D) HR Fluctuation Range (Absolute Change): At T1 (After Drug Administration): Mean difference in ΔHR: −3.2 bpm (95% CI: −6.2 to −0.2), P = 0.036. At T2 (After Laryngeal Mask Insertion): Mean difference in ΔHR: −4.1 bpm (95% CI: −7.4 to −0.8), P = 0.014. |
Discussion
Hemodynamic Stability
In this trial, we observed that oliceridine provided superior hemodynamic stability compared to sufentanil. It offers new insights into the pharmacological application of μ-opioid receptor (MOR) biased agonists in elderly hypertensive patients. The O group showed a smaller decrease in mean arterial pressure after laryngeal mask insertion, which is consistent with the mechanism that oliceridine preferentially activates G protein-coupled signaling, rather than the β-arrestin pathway. The observed MAP reduction (ΔMAP: −4.8 vs −15.7 mmHg) aligns with the threshold (>10 mmHg change) linked to increased myocardial injury risk in hypertensive elderly.7 Similarly, HR stability is clinically significant as intraoperative tachycardia >90 bpm correlates with 2.5-fold higher postoperative cardiac events.16 Oliceridine’s stable hemodynamic profile may thus directly mitigate perioperative cardiovascular complications. DeWire SM et al’s research indicates that traditional opioids like sufentanil recruit β-arrestin through vagal inhibition, intensifying sympathetic excitation and thereby impairing pressure reflex-mediated compensation during pain stimulation.17 In contrast, the G protein bias of oliceridine maintains autonomic tone, as evidenced by the weakened heart rate response in this trial. This finding aligns with Soergel et al’s results, which show that biased MOR agonists reduce catecholamine surges by 40% compared to traditional opioids during surgical stress.18
In addition, in this study, the reduction in SBP variability in the O group may be attributed to the unique regulatory effect of oliceridine on endothelial nitric oxide synthase (eNOS) activity. Unlike sufentanil, which inhibits eNOS through a β-arrestin-dependent pathway, oliceridine can maintain endothelium-dependent vasodilation, thereby effectively reducing perioperative blood pressure fluctuations.19 This mechanism is particularly important for elderly hypertensive patients, as age-related arteriosclerosis can increase pulse pressure variability by up to 35%.16
Clinical Implications of Time-Group Interactions
The diastolic blood pressure in group O gradually stabilized, indicating that oliceridine has excellent pharmacokinetic properties. The time for the plasma concentration of oliceridine to reach equilibrium with the concentration at the site of action (CSHT) was 1.7 hours, while that of sufentanil was 3.2 hours.20 Specifically, oliceridine achieved equilibrium between plasma and the site of action more rapidly (kₑ₀ was 0.24 min−¹, compared to 0.11 min−¹ for sufentanil),21 allowing for more precise dose adjustments during the dynamic phase of surgery. This pharmacokinetic advantage may explain the reduction of episodes of hypotension during the interval from induction to the start of surgery. This phase is critically significant. The study conducted by Mada S et al demonstrated that 68% of intraoperative hemodynamic instability events in elderly patients occur during this period.22
The time group interaction in heart rate variability further demonstrates oliceridine’s outstanding ability in dynamically regulating autonomic nerve responses. By maintaining the balance between the parasympathetic and sympathetic nerves, oliceridine can effectively reduce the risk of reflex tachycardia. Considering that a heart rate exceeding 90 beats per minute may increase the risk of postoperative myocardial injury in hypertensive patients,23 this characteristic is particularly important and deserves more attention.
Safety and Tolerability
According to the study by Melnikova I et al, traditional opioids activate DOR in the chemoreceptor trigger zone, increasing the risk of vomiting by 2.3 times, while biased agonists do not have this effect.24 Furthermore, Wilson-Poe AR and Moron JA’s research indicates that postoperative nausea and vomiting (PONV) can prolong the stay of elderly patients in the post-anesthesia care unit by 45 minutes and increase medical costs by approximately US $400 for each episode.16 Thus, the finding that oliceridine has a low incidence of nausea and vomiting is of great significance for clinical practice.
Limitations and Future Directions
While oliceridine demonstrates promising safety, its higher acquisition cost (8-fold vs sufentanil) and limited availability in resource-constrained settings warrant consideration for broader implementation. In our single-center study, we focused on ureteroscopy (a procedure that typically lasts 25 to 40 minutes). However, these results may not be applicable to long surgeries that require more than two hours of anesthesia. Considering that approximately 20% of Asian patients exhibit a CYP2D6 poor metabolizer phenotype, which could increase the AUC₀-∞ of oliceridine by 35%, there is still much to explore in the field of pharmacogenomics.22 Future studies that incorporate CYP2D6 genotyping will help to better optimize dosing for different ethnic groups. Additionally, as this study was conducted at a single center, it has certain limitations. To more comprehensively validate the research results, we recommend conducting multi-center studies to increase sample size and representativeness, thereby providing more reliable data.
Conclusion
Oliceridine’s G protein-biased agonism at the μ-opioid receptor (MOR) provides stable hemodynamic regulation in elderly hypertensive patients undergoing laryngeal mask general anesthesia, offering a new therapeutic option with opioids for these procedures.
Data Sharing Statement
All data generated in this study are available from Kai He (one of the corresponding authors) upon reasonable request. Supplementary material associated with this article can be found in the online version.
Ethical Approval
The study was approved by the Medical Ethics Committee of the People’s Hospital of Qiannan (Ethical approval (Number: 2025-qnzy-03), in accordance with the World Medical Association Declaration of Helsinki.
Consent
Written informed consent was obtained from all patients or their legal guardians prior to participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McEvoy JW, McCarthy CP, Bruno RM, et al. 2024 ESC Guidelines for the management of elevated blood pressure and hypertension. Eur Heart J. 2024;45(38):3912–4018. doi:10.1093/eurheartj/ehae178
2. Blumer V, Kanwar MK, Barnett CF, et al. Cardiogenic shock in older adults: a focus on age-associated risks and approach to management: a scientific statement from the American Heart Association. Circulation. 2024;149(14):e1051–65. doi:10.1161/CIR.0000000000001214
3. Theofilis P, Doumani G, Tsatsani GC, et al. The role of hypertension in cognitive dysfunction. J Clin Med. 2024;13(19). doi:10.3390/jcm13195979
4. Bergholz A, Grusser L, Khader W, et al. Personalized perioperative blood pressure management in patients having major non-cardiac surgery: a bicentric pilot randomized trial. J Clin Anesth. 2025;100:111687. doi:10.1016/j.jclinane.2024.111687
5. Fowler AJ, Abbott T, Prowle J, Pearse RM. Age of patients undergoing surgery. Brit J Surg. 2019;106(8):1012–1018. doi:10.1002/bjs.11148
6. Menna C, Fiorelli S, Massullo D, Ibrahim M, Rocco M, Rendina EA. Laryngeal mask versus endotracheal tube for airway management in tracheal surgery: a case-control matching analysis and review of the current literature. Interact Cardiov Th. 2021;33(3):426–433. doi:10.1093/icvts/ivab092
7. Soh MS, Park JS, Seo KW, et al. Visit-to-visit systolic blood pressure variability in patients with ST-elevation myocardial infarction predicts long-term cardiovascular outcomes. J Hum Hypertens. 2019;33(4):259–266. doi:10.1038/s41371-019-0176-0
8. Schnider TW, Minto CF, Gambus PL, et al. The influence of method of administration and covariates on the pharmacokinetics of propofol in adult volunteers. Anesthesiology. 1998;88(5):1170–1182. doi:10.1097/00000542-199805000-00006
9. Piantoni C, Carnevali L, Molla D, et al. Age-related changes in cardiac autonomic modulation and heart rate variability in mice. Front Neurosci-Switz. 2021;15:617698. doi:10.3389/fnins.2021.617698
10. Sanatkar M, Farhanchi A, Manouchehrian N, et al. Subarachnoid block with low dose of bupivacaine and sufentanil in patients with coronary artery disease. Arya Atheroscler. 2014;10(2):94–99.
11. Weerink M, Struys M, Hannivoort LN, Barends C, Absalom AR, Colin P. Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine. Clin Pharmacokinet. 2017;56(8):893–913. doi:10.1007/s40262-017-0507-7
12. Moss L, Hijma H, Demitrack M, et al. Neurocognitive effect of biased µ-Opioid receptor agonist oliceridine, a utility function analysis and comparison with morphine. Anesthesiology. 2023;139(6):746–756. doi:10.1097/ALN.0000000000004758
13. Viscusi ER, Skobieranda F, Soergel DG, Cook E, Burt DA, Singla N. APOLLO-1: a randomized placebo and active-controlled phase III study investigating oliceridine (TRV130), a G protein-biased ligand at the micro-opioid receptor, for management of moderate-to-severe acute pain following bunionectomy. J Pain Res. 2019;12:927–943. doi:10.2147/JPR.S171013
14. Bergese SD, Brzezinski M, Hammer GB, et al. ATHENA: a phase 3, open-label study of the safety and effectiveness of oliceridine (TRV130), A G-Protein Selective agonist at the micro-opioid receptor, in patients with moderate to severe acute pain requiring parenteral opioid therapy. J Pain Res. 2019;12:3113–3126. doi:10.2147/JPR.S217563
15. Fossler MJ, Sadler BM, Farrell C, et al. Oliceridine (TRV130), a Novel G protein-biased ligand at the mu-Opioid receptor, demonstrates a predictable relationship between plasma concentrations and pain relief. I: development of a pharmacokinetic/pharmacodynamic model. J Clin Pharmacol. 2018;58(6):750–761. doi:10.1002/jcph.1076
16. Wilson-Poe AR, Moron JA. The dynamic interaction between pain and opioid misuse. Brit J Pharmacol. 2018;175(14):2770–2777. doi:10.1111/bph.13873
17. DeWire SM, Yamashita DS, Rominger DH, et al. A G protein-biased ligand at the mu-opioid receptor is potently analgesic with reduced gastrointestinal and respiratory dysfunction compared with morphine. J Pharmacol Exp Ther. 2013;344(3):708–717. doi:10.1124/jpet.112.201616
18. Soergel DG, Subach RA, Burnham N, et al. Biased agonism of the mu-opioid receptor by TRV130 increases analgesia and reduces on-target adverse effects versus morphine: a randomized, double-blind, placebo-controlled, crossover study in healthy volunteers. Pain. 2014;155(9):1829–1835. doi:10.1016/j.pain.2014.06.011
19. Crowley RS, Riley AP, Alder AF, et al. Synthetic studies of neoclerodane diterpenes from salvia divinorum: design, synthesis, and evaluation of analogues with improved potency and G-protein activation bias at the mu-Opioid receptor. Acs Chem Neurosci. 2020;11(12):1781–1790. doi:10.1021/acschemneuro.0c00191
20. Kudla L, Przewlocki R. Influence of G protein-biased agonists of mu-opioid receptor on addiction-related behaviors. Pharmacol Rep. 2021;73(4):1033–1051. doi:10.1007/s43440-021-00251-1
21. Pedersen MF, Wrobel TM, Marcher-Rorsted E, et al. Biased agonism of clinically approved mu-opioid receptor agonists and TRV130 is not controlled by binding and signaling kinetics. Neuropharmacology. 2020;166:107718. doi:10.1016/j.neuropharm.2019.107718
22. Mada S, Gerak LR, Soyer A, et al. Behavioral effects of benzylideneoxymorphone (BOM), a low efficacy micro opioid receptor agonist and a delta opioid receptor antagonist. Psychopharmacology. 2020;237(12):3591–3602. doi:10.1007/s00213-020-05638-1
23. Wootten D, Christopoulos A, Marti-Solano M, Babu MM, Sexton PM. Mechanisms of signalling and biased agonism in G protein-coupled receptors. Nat Rev Mol Cell Bio. 2018;19(10):638–653. doi:10.1038/s41580-018-0049-3
24. Melnikova I. Pain market. Nat Rev Drug Discov. 2010;9(8):589–590. doi:10.1038/nrd3226
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.