Back to Journals » Psychology Research and Behavior Management » Volume 16
Effects of Mindfulness on Obligatory Exercise During the Return of Injured Athletes to Sports: The Mediating Roles of Self-Criticism and Competitive State Anxiety
Authors Wu R ![]() , Jing L, Liu Y, Wang H, Xie L, Deng W
, Jing L, Liu Y, Wang H, Xie L, Deng W
Received 11 April 2023
Accepted for publication 28 May 2023
Published 12 June 2023 Volume 2023:16 Pages 2157—2171
DOI https://doi.org/10.2147/PRBM.S414709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Ruoshan Wu,1 Longjun Jing,1,2 Yang Liu,3 Huilin Wang,3,4 Lin Xie,5 Wu Deng6
1School of Physical Education, Hunan University of Science and Technology, Xiangtan, 411201, People’s Republic of China; 2China Athletics College, Beijing Sport University, Beijing, 100084, People’s Republic of China; 3School of Business, Hunan University of Science and Technology, Xiangtan, 411201, People’s Republic of China; 4Faculty of Economics, Chulalongkorn University, Bangkok, 10330, Thailand; 5School of Physical Fitness of Guangzhou Sport University, Guangzhou, 510000, People’s Republic of China; 6School of Physical Education, Shenzhen University, Shenzhen, 518000, People’s Republic of China
Correspondence: Huilin Wang, Email [email protected]
Purpose: Despite the Advances in sports training methods and medicine, they have not reduced the recurrence rate of athletes’ injuries significantly, and obligatory exercise may be an important reason for their re-injury. The purpose of this study was to investigate the effects of mindfulness on obligatory exercise behavior, self-criticism, and competitive state anxiety in athletes recovering from injury, and explain their interactions.
Patients and Methods: The study adopted the snowball and convenience sampling methods. From November to December 2022, a total of 265 high-level sports players in South China were selected, and ultimately, 208 valid data samples were obtained. Maximum likelihood estimation was used to analyze the data and test the hypotheses proposed using 5000 bootstrap samples to test the mediating effects of the structural equation model.
Results: The results demonstrated that there were positive correlations between self-criticism and obligatory exercise (standardized coefficients = 0.38, p < 0.001), as well as competitive state anxiety and self-criticism (standardized coefficients = 0.45, p < 0.001). Mindfulness and obligatory exercise were correlated negatively (standardized coefficients = − 0.31, p < 0.001), but there was no significant relation between competitive state anxiety and obligatory exercise (standardized coefficients = 0.05, p > 0.01). Self-criticism and competitive state anxiety mediated mindfulness’s positive effects on obligatory exercise in part (standardized indirect effect = − 0.16, p < 0.01), and this explanatory power was higher than in any previous study (R2 = 0.37).
Conclusion: The irrational beliefs in Activating events–Beliefs–Consequence (ABC) theory play an important role in explaining athletes’ obligatory exercise, and mindfulness has a positive effect on reducing obligatory exercise behavior.
Keywords: obligatory exercise, mindfulness, cognitive behavioral therapy, ABC theory, sports reinjury
Introduction
Research has shown that sports injuries are a serious problem among individuals who engage in long-term physical activity, particularly elite athletes, and plague their personal development.1 Johansson2 reported that athletes suffer a total injury rate of 3 per 1000 training hours. Dubravcic-Simunjak et al3 interviewed 469 skaters during four consecutive Junior World Figure Skating Championships and the Croatia Cup, and their results showed that 124 (26.4%) skaters reported that they suffered acute injuries and 207 (44.15%) skaters reported overuse syndrome. Galambos et al4 evaluated the sports injuries of 845 athletes from Queensland Academy of Sport, and found that approximately 67% of them were injured each year. Although the Advances in sports training methods and medicine have reduced athletes’ injury rate during training and accelerated their recovery from injuries to a certain extent, they do not reduce the recurrence rate of their old injuries significantly, particularly those that have attracted extensive attention from researchers. Further, athletes who are injured undergo a strengthening stage during recovery before they return to the field, during which they often have a high re-injury rate.5
In fact, obligatory exercise may be an important cause of athletes’ re-injury during the recovery period.6 Although coaching teams have been trying to reduce the re-injury rate by formulating more feasible training and recovery plans that protect the physical health of athletes objectively, it is worth noting that the athletes’ motivation dominates their behavior. Injured athletes who are about to return to sports may have a range of psychosocial issues related to sports injuries, which may affect their motivation to exercise and may lead to different strategies of action. For example, the fear of re-injury may lead some to adopt more conservative training strategies, although this is hindered to some extent. In this case, when athletes return to play, they tend not to re-injure themselves.7 Concerns about reaching pre-injury performance levels and being “behind” the competition often lead some athletes, particularly those with high self-esteem, to take more aggressive action strategies in which they will engage in obligatory exercise, and even while injured, will still force themselves to persist in strenuous activities, which is likely to be an important reason for their re-injury during the recovery period.8–10
However, few current studies have focused on athletes’ obligatory exercise behavior, and various obligatory exercise-related terms, such as exercise dependence,11 positive addiction,12 exercise addiction,13 and excessive exercise.14 Duncan et al’s15 research showed that compared with exercise addicts, exercise behavior itself and concentration are not significant features of obligatory exercise behavior, while stress, anxiety, guilt, and other sports-related emotions can predict obligatory exercise behavior better. Hall et al9 conducted a survey on the antecedents of long-distance runners’ compulsive sports behaviors. The survey results showed that 31% of compulsive sports behaviors are attributable to athletes’ goal orientation, perceptual ability, worry about mistakes, and high personal standards. Elements of high ability and perfectionism together explained 49% of the variance in women’s obligatory exercise behaviors. Studies have shown that excessive effort may be a common characteristic of some high-performance athletes, and may be an important reason for athletes’ compulsive sports behavior16 Although many studies have investigated the antecedents of obligatory exercise behavior, few have explored it from the perspective of intervention, ie, the way to reduce obligatory exercise behavior through effective intervention methods.
Cognitive Behavioral Therapy, based upon ABC theory, has advanced considerably since the 1970s, and become one of the more popular forms of psychotherapy.17 The ABC theory holds that activating events (A) and beliefs (B) trigger individual specific behaviors or emotions consequence (C) directly, and emotions can also affect beliefs (B) and behaviors (C). As an important means of cognitive behavioral therapy, mindfulness has attracted extensive attention from researchers in recent years. Its ability to regulate and improve individual attention and emotion provides a theoretical basis for the treatment of a series of clinical syndromes of mental illness, including generalized anxiety,18 post-traumatic stress disorder,19 addiction symptoms,20 eating disorders,21 etc. Based upon this, beliefs and emotions related to obligatory exercise may also be important antecedents of such behavior, and the study of mindfulness’s effect on reducing obligatory exercise can demonstrate its influence on these beliefs and emotions. Research has shown that self-criticism is a relatively stable personality trait that appears to contribute to maladaptation.22 Blatt and Homann’s23 research suggested that because of an overemphasis on achievement and self-worth, highly self-critical people often wish to maximize control over their environment to reduce their likelihood of failure. Research has shown that self-criticism is an important predictor of many psychological disorders, including anxiety,24 eating disorders,25 borderline personality disorder,26 and suicidality.27 Therefore, based upon the ABC theory, this study selected self-criticism as the belief dimension (B) of compulsive sports behavior, and anxiety related to competition (competitive state anxiety) as its emotional dimension. By exploring mindfulness, self-criticism, the relation between competitive state anxiety and obligatory exercise, this study attempted to identify a suitable treatment for obligatory exercise behavior to reduce athletes’ re-injury rate and help them return to competition.
This study had the following goals: (1) To investigate the interactions among mindfulness, self-criticism, competitive state anxiety, and obligatory exercise; (2) verify mindfulness’s influence on the three, and (3) explore the interaction mechanism among them to (4) provide suggestions to reduce athletes’ obligatory exercise behavior during the recovery period.
The contributions of this study are as follows: First, from a theoretical point of view, few previous studies have focused on the obligatory exercise behavior of athletes. This study focuses on the obligatory sports behavior of athletes during the recovery period by exploring the causes of athletes’ reinjury, and discusses them in more depth; second, based upon cognitive behavioral therapy, this study began from the perspective of improved intervention by exploring the relations among mindfulness, self-criticism, competitive state anxiety, and obligatory exercise behavior in an effort to verify mindfulness’s effect on obligatory exercise behavior. Identifying mindfulness’s positive influence provides theoretical support for using it to treat compulsive motor behavior, and expands the theoretical boundaries of cognitive behavioral therapy; third, ABC theory was the theoretical basis of this study, which explains self-criticism, competitive state anxiety, and the interaction relation among the three groups, provides theoretical support for the study of obligatory exercise behavior in other groups, and expands the theoretical boundary of the study of this behavior.
Literature Review
ABC Theory
American psychologist Ellis28 proposed the ABC theory on the basis of the stimulus-organism-response (SOR) theory. Ellis believed that activating events (A) did not trigger the individual’s behavior directly, as the SOR theory indicated. Instead, he proposed that the individual’s cognition and evaluation of an event, ie, beliefs (B) cause nervousness, anxiety, depression, and other specific emotional and behavioral consequences (C) directly. In the ABC theory, the relation between ABC is understood as a second-order problem, in that activating events (A) do not always trigger the consequence (C) through belief (B), external events do not always cause A, B and C can also exert a secondary influence on A, and C can influence B as well. Beliefs (B) are divided into rational beliefs (RB) and irrational beliefs (IB).29 RB are usually expressed in the form of preferences and rational derivatives, and IB are usually expressed in the form of absolute and irrational derivatives, eg, “I want to succeed, and if I fail, I will be nothing”. Woods and Ellis30 believed that cognitive evaluation related to IB is an important reason for unhealthy emotional and behavioral consequences (C). In addition, Lazarus31 indicated that on an individual level, goals, self-belief, and personal resources play an important role in shaping cognitive evaluation. The more individuals exhibit a high recognition of goals and high attention to self-belief, the more easily it leads to IB (B). Muran’s32 study showed that both cognitive distortions and IB are important causes of “neural fragility”. Therefore, in cognitive behavioral therapy based upon ABC theory, attempts to reduce IB and increase RB have become important ways to enhance individual emotional cognition and alleviate related mental illnesses. Based upon the ABC theory, this study explored the important factors that lead to athletes’ compulsive sports behavior during the recovery period, and at the same time, provided a theoretical basis for the treatment of such symptoms based upon cognitive behavioral therapy.
Mindfulness and Obligatory Exercise
In Rodgers et al’s33 study, obligatory exercise was defined as “… a compulsive behavioral pattern in which exercise dominates daily life at the expense of other symptoms”. Obligatory exercisers prioritize exercise over other commitments, exercise when they are physically unwell, and report increased guilt or negative emotions when they are unable to exercise.34 According to Bamber et al,35 people who exercise compulsively believe that activity is a key dimension that supports their self-definition. When the movement patterns become both rigid and inflexible, the individual’s dependence on activity may be greater, and they typically experience such withdrawal symptoms as anxiety, depression, and guilt if they stop exercising. Draeger et al6 described obligatory exercise as “athlete neurosis”, in which “compulsive” indicates that the patient’s motivation is no longer to improve performance, but to reduce or avoid emotional problems, such that when any arise, they may feel compelled to exercise. The premise of obligatory exercise behavior is that individuals have a high degree of recognition of their own goals. When individuals consider exercise goals a way to realize their self-worth and are gradually dominated by this view, they will often think repeatedly about whether they have the necessary resources. This in turn leads to increased anxiety and self-consciousness about adverse outcomes, and individuals are more likely to use maladaptive achievement strategies to avoid these outcomes.36 The multidimensional model of obligatory exercise that Mayer et al37 proposed argues that, in addition to this negative reinforcement for maintaining physical activity (ie avoiding anxiety, shame, and guilt), it may also be maintained through positive reinforcement (ie mood improvement).
An oft-cited definition of mindfulness is “… focusing attention in a specific way: consciously, in the present moment, and without judgment”.38 “Consciously” refers to being aware of the way attention is being directed, ie, the individual’s monitoring of thought processes, including the focus of attention,39,40 “… in the present moment” requires the individual to pay attention to what is happening now, including current body perception, negative emotions, painful thoughts, etc., in which the individual strives to free himself from the control of past experiences;41 “uncritical” refers to the individual’s experience of the present, having an attitude of openness and acceptance, accepting not being passive, but being able to take a bystander’s perspective, not criticizing or explaining, but simply witnessing it,42 eg, when an apple appears in the meditator’s mind, it is noticed for its shape, color, and smell, not only for its function as a food and commodity (Shapiro et al.43 Dividing the mechanism of mindfulness into three dimensions of attention, intention, and attitude, Shapiro et al proposed the concept of re-perception, and believed that re-perception in mindfulness can allow us to take a step back from anxiety and see clearly that it is simply an emotional state that is arising and will pass in time, and by developing the ability to observe emotional states such as anxiety and fear, we increase our “freedom” to cope with these states and are no longer dominated by such states. Brown and Ryan’s44 study demonstrated that individuals who score higher on mindfulness measures have a greater ability to self-regulate their emotions and behaviors.
In summary, Draeger et al6 described obligatory exercise as “athlete neurosis”. Although the specific cause of obligatory exercise is not yet clear, it is certain that it is not a health condition. Many negative emotions can affect an individuals’ mental state, and excessive attention to self-worth in sports leads to a certain extent to obligatory exercise behavior. As an important method of cognitive behavioral therapy, mindfulness can improve the regulation and control of individuals’ attention and emotion, which may enhance obligatory exercisers’ ability to resist negative emotions and change their self-defined value cognition.45,46 These factors may have a positive influence on reducing obligatory exercise behavior. Based upon this, this study proposes the following hypotheses:
Hypothesis 1 (H1): Mindfulness has a positive effect on reducing obligatory exercise.
Competitive State Anxiety, Self-Criticism, and Obligatory Exercise
Competitive state anxiety is defined as a state of momentary unease about a specific competitive situation that arises primarily from a perception of the importance of the situation and uncertainty of the outcome.47 This state of anxiety has three dimensions: cognitive anxiety; somatic anxiety, and self-confidence, and each has its own characteristics, antecedents, and consequences.48 Specifically, cognitive anxiety is the psychological component of anxiety attributable to negative expectations of success or a negative self-evaluation, while somatic anxiety is the physical and emotional component of anxiety that is related directly to autonomic arousal (eg, nervousness, sweating, etc.).49 Typically, cognitive anxiety precedes the onset of physical anxiety and is a longer-lasting response, while physical anxiety tends to peak rapidly at the beginning of the event.50 The degree of self-confidence can predict the development of cognitive anxiety and somatic anxiety.51 Studies have found that individual differences, such as trait anxiety,52 level of competition,53 Target orientation,54 and other factors55 influence competitive state anxiety.56 Tsopani et al showed that higher-performing athletes had lower average cognitive and somatic anxiety and higher average self-confidence than lower-performing athletes.
Self-criticism is described as a personal vulnerability characterized by an overemphasis on achievement and self-worth.57 Highly self-critical people tend to be extremely self-aware, as manifested by their overemphasis on self-worth and strong need for personal achievement. At the same time, in their continuous and severe self-criticism, they tend to focus their attention excessively and easily on their own mistakes in an effort to avoid failure, which makes it difficult for them to be satisfied with their successful performance.58 Whelton and Greenberg’s59 research showed that highly self-critical people are prone to negative emotions such as frustration, guilt, low self-esteem, and shame. Thompson and Zuroff60 divided self-criticism into two forms: comparative self-criticism and internalized self-criticism. Comparative self-criticism is characterized by evaluating oneself by comparison with others, while internalized self-criticism refers to a person’s self-perception, ie, the assessment of whether he can meet his own internal goals, expectations, and ideals. People who are highly self-critical are often perceived to have high personal standards, and their critique of their success also indicates that they tend to undervalue their successful experiences by raising their standards further. Dunkley et al’s22 research showed that there is a significant overlap between self-criticism and perfectionism, in that perfectionism has two dimensions, high standards and self-critical perfectionism, and while self-critical perfectionism is equivalent to self-criticism, it is not high personal standards per se that affect individuals adversely, but rather the self-critical aspect—perfectionist self-criticism—that appears to contribute to maladaptation.
Taken together, competitive state anxiety, self-criticism, and obligatory exercise appear to be highly correlated. First, studies have shown that individuals who are more self-critical generally have higher competitive anxiety,61 and although compared with the temporary emotional state of competitive state anxiety (C), self-criticism is a relatively stable personality trait (B), according to the ABC theory, the relation between B and C may be reversible, and competitive state anxiety (C) may also lead to greater self-criticism (B). Second, the individuals mentioned above engage in obligatory exercise behaviors to reduce or avoid emotional problems attributable to their inability to exercise, which shows that negative emotions are important predictors of obligatory exercise behaviors, so that competitive state anxiety, as a common withdrawal symptom among athletes, may be correlated highly with obligatory exercise behavior. Third, criticism is accompanied by high personal standards and full recognition of achievement goals. These factors may be important predictors of obligatory exercise behavior, so there may be a high positive correlation between the two. Based upon this, the following hypotheses are proposed:
Hypothesis 2 (H2): Competitive state anxiety has a negative influence on self-criticism. Hypothesis 3 (H3): Competitive state anxiety has a negative influence on obligatory exercise. Hypothesis 4 (H4): Self-criticism has a negative influence on obligatory exercise.
The Mediating Effects of Competitive State Anxiety and Self-Criticism
Studies have shown that athletes’ injury status has an important effect on individual emotions and behaviors. Kolt and Kirkby62 investigated the relation between gymnasts’ anxiety and injuries and found that those with serious injuries experienced more anxiety and fatigue, and reported greater cognitive anxiety. On the one hand, according to the ABC theory, an athlete’s injury is equivalent to an activating event (A), self-criticism is equivalent to belief (B), and competitive state anxiety and compulsive sports behavior are equivalent consequences (C), given that the assumption of the ABC sequence is established. According to the second-order relation between ABC in the theory, competitive state anxiety (C1) can also exert a secondary influence on obligatory exercise (C2) through the role of self-criticism (B), and the self-criticism between competitive state anxiety and obligatory exercise. On the other hand, cognitive behavioral therapy based upon ABC theory attempts to improve individuals’ emotional cognition by reducing IB and increasing RB, thereby achieving the goal of treating related neurological symptoms. According to the research on self-criticism and competitive state anxiety above, self-criticism actually embodies IB, and competitive state anxiety (C) affects IB indirectly through self-criticism. As an important means of cognitive behavioral therapy, mindfulness largely improves the individual’s emotional cognitive ability by reducing self-criticism and competitive state anxiety to achieve the purpose of treating obligatory exercise behavior. If the hypothesis above holds, self-criticism and competitive state anxiety serve as partial mediators between mindfulness and compulsive motor behavior. Based upon this, this study proposes the following hypotheses:
Hypothesis 5 (H5): Self-criticism mediates the relation between competitive state anxiety and obligatory exercise. Hypothesis 6 (H6): Self-criticism and competitive state anxiety mediate the relation between mindfulness and obligatory exercise in part.
Based on this, this study proposes a hypothetical model in Figure 1.
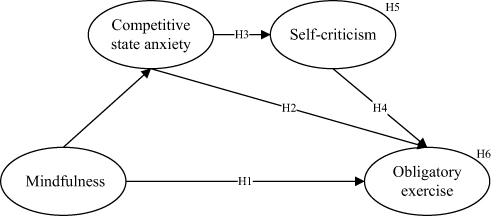 |
Figure 1 The hypothesized model. |
Method
Sample and Procedure
The study used snowball and convenience sampling methods to conduct a questionnaire survey of high-level injured athletes (ie, athletes at national level two and above) in Southwest China during their recovery period from November to December 2022. To ensure the data’s validity, the researchers contacted the coaches of high-level sports teams in various provinces in Southwest China in advance and distributed questionnaires to the team members after the coaches’ support was obtained. Prior to the start of the survey, we briefed participants on the purpose of the study and promised to keep the results strictly confidential and use only for academic research. On this basis, through the snowball method, team members who met the survey conditions also shared the questionnaire. Finally, to express their gratitude to all participants, the researchers gave participants small gifts (sports equipment such as sports socks and sports bracers) as feedback. As of the end of December, 300 questionnaires were distributed, and a total of 265 high-level athletes were recruited. After invalid questionnaires (eg, missing information and blank answers) were deleted, 208 valid questionnaires were obtained for a response rate of 69.3%.
Table 1 lists the demographic characteristics of the athletes surveyed. Nearly 70% of the respondents were between the ages of 18 and 23; 65.4% were men and 34.6% were women; 60.6% were second-level athletes, and ball sports was the main sports category (51.9%).
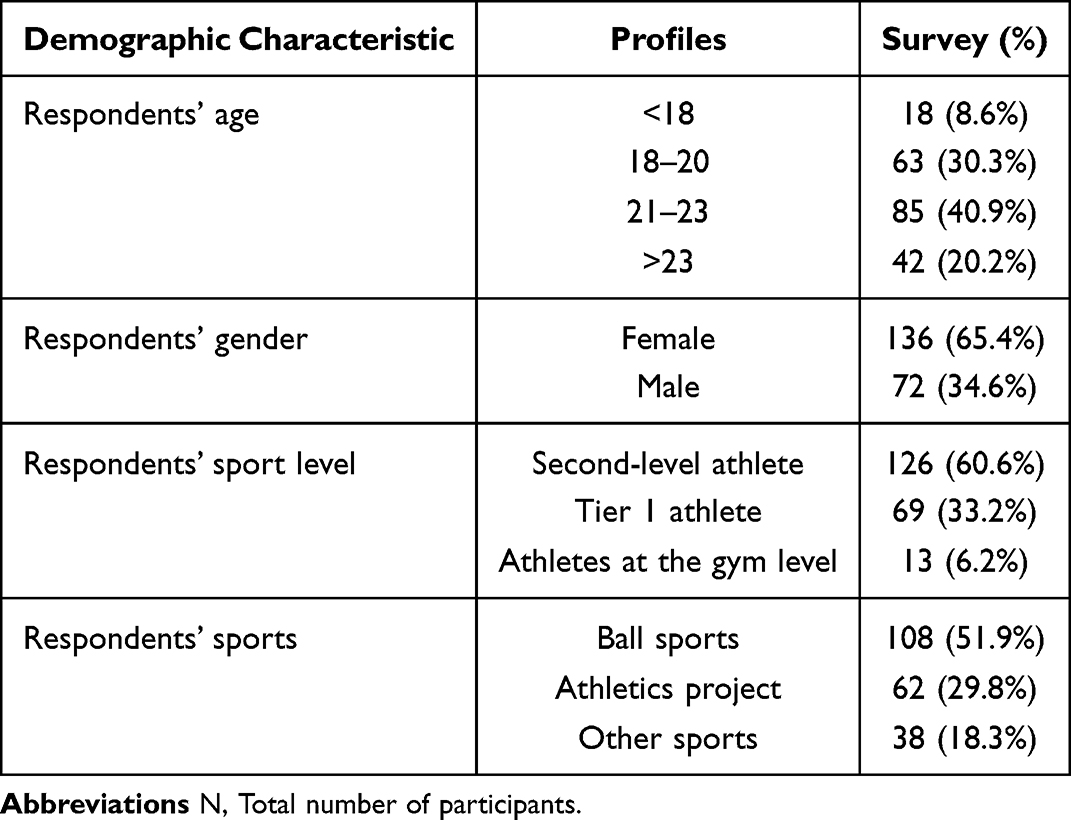 |
Table 1 Participants’ Profile (N = 208) |
Measures
Obligatory Exercise
This study used Steffen and Brehm’s63 meter table to measure obligatory exercise. This scale overcomes the previous limitations of measuring obligatory exercise using a single-dimension standard (eg, exercise frequency and strength training, etc.). Exercise-related emotions reflect the emotional consequences of missed exercise and obligatory exercise behavior is measured according to a person’s ideas about exercise. Duncan et al’s15 re-measurement of the scale indicated that the meter has good reliability. On this basis, combined with the need to measure individual psychological characteristics in this study, the six entries related to the two dimensions of exercise emotions and movement were finally selected to evaluate the athletes’ obligatory exercise.
Five Facet Mindfulness Questionnaire
The Five Facet Mindfulness Questionnaire was used to evaluate mindfulness in this study.64 The questionnaire is based upon observation, description, and conscious action without judging the internal experience, and evaluating the five dimensions of the internal experience without response Thompson and Zuroff.60
Self-Criticism Scale
The self-criticism scale was used to evaluate self-criticism in this study Cox et al.60 This scale assesses self-criticism from two dimensions: internalized self-criticism and comparative self-criticism.
Competitive State Anxiety Inventory-2 Revised
The competitive state anxiety list after revision 2 was used to evaluate competitive state anxiety in this study.48 The four scales were measured using a five-point Likert scale on which the responses ranged from 1 (Strongly Disagree) to 5 (Strongly Agree).
To ensure the study’s authenticity, the researchers referred to an adjustment of the table’s scale in reference to the specific research field and Chinese-specific cultural backgrounds. A pilot test was conducted to ensure the adjusted scale’s reliability.65 The researchers distributed 50 questionnaires to the Sports University’s high-level sports team using the convenience sampling method and obtained 45 valid questionnaires. The results showed that the Cronbach’s alpha coefficients were all greater than 0.80, indicating that the measurement instrument had good internal consistency.66
Data Analysis
The hypothetical model proposed by the Institute was verified with structural equation modelling (SEM) in AMOS v. 26.0. SEM is highly suitable to assess the potential variables in the measurement model and verify the relation between them.67 This study followed the two-step modelling method that Anderson and Garbing68 proposed. First, it tested the instrument’s reliability and validity, which was 0.84 and indicated that the instrument had good reliability and validity. Second, we adopted the maximum likelihood estimation method to verify that there was a significant relation between the independent variables (righteous thoughts, self-criticism, competitive state anxiety, and obligatory exercise). Third, we used 5000 bootstrap samples to test the indirect effects between mindfulness and obligatory exercise. Finally, we evaluated the validity of the model and measured the assumption model’s fit coefficient and path coefficient.
Results
Reliability and Validity
Reliability was measured with reference to Fornell and Larcker.66 As shown in Table 2, the Cronbach α coefficient of 0.84 and composite reliability (CR) coefficient of 0.84 was the minimum value of Cronbach’s α and composite reliability (CR) was the minimum value of all variables. Both values were higher than the minimum value of 0.80 that Hair et al69 recommended. Therefore, all variables demonstrated good reliability; the convergent validity was evaluated by the two indicators of factor loading and the average variance extracted (AVE). Table 2 shows that the minimum values of the factor loadings and AVE in all measurement items were 0.68 and 0.51, respectively, which are higher than the value of 0.5 that Fornell and Larcker69 recommended. Therefore, all variables had high convergent validity.
 |
Table 2 Reliability and Validity Tests |
Finally, the discriminant validity was verified by comparing the square root of the AVE and each variable’s correlation coefficients. Table 3 shows that the square root of each variable was higher than the correlation coefficient, which meets Fornell and Larcker’s69 requirements and demonstrates that the variables exhibited acceptable discriminant validity.
 |
Table 3 Discriminant Validity Test |
Common Method Variance
The study also considered the potential common method variance (CMV) issue and adopted two methods to test for it. On the one hand, the results of Harman’s Univar transport test showed that the percent of variance extracted from the University tests was 34.98%, which does not meet the conditions for the presence of CMV (ie, the percent of variance extracted from the University tests is higher than 50%), which indicates that there is no CMV.70 On the other hand, the study adopted Lindell and Whitney’s71 recommended CFA single-factor and dual-factor method as well to test for the potential presence of CMV in the study. The results showed that the single-factor model’s Chi-square value was 1188.9, with 190 degrees of freedom, and the Chi-square value of the multi-factor model was 229.5, with 183 degrees of freedom. The difference between the value of the two models and the degrees of freedom was 137.1, which is very significant, and proved that there was no CMV. Therefore, this study did not require CMV correction.
Structural Path Model
Referring to the test parameters used commonly in previous studies72 and Hair et al’s67 recommended values, the results showed that the data (χ2/df = 1.23, GFI = 0.91, NFI = 0.90, CFI = 0.98, TLI = 0.98, IFI=0.98, RMSEA = 0.03) fit the structural model well. The results of the model are shown in Figure 2. Positive correlations were found between mindfulness and obligatory exercise (standardized coefficients = −0.31, p < 0.001), competitive state anxiety and self-criticism (standardized coefficients = 0.45, p < 0.001), and self-criticism and obligatory exercise (standardized coefficients = 0.38, p < 0.001). All were statistically significant, and thus supported H1, H3, and H4. Of note, although competitive state anxiety was correlated positively with obligatory exercise (standardized coefficients = 0.05), it was not statistically significant (p >0.01) and therefore did not support H2. However, self-criticism appeared to mediate its effect on obligatory exercise.
 |
Figure 2 Path analysis results. ***p < 0.001, **p < 0.01. |
Mediation Test
This study followed Bollen and Stine’s73 recommendation to use the bootstrapping method to test the mediation effect. The 95% confidence interval results for the 5000 bootstrap samples are shown in Table 4. All Z values were greater than 1.96, and there was no zero value in the interval. This result indicated that there was a significant mediating effect between competitive state anxiety and obligatory exercise through self-criticism (standardized indirect effect = 0.18, p < 0.001), which supported H5. Further, there was a significant mediating effect between mindfulness and obligatory exercise through competitive state anxiety and self-criticism (standardized indirect effect = −0.16, p < 0.01), and thus, H6 was supported as well.
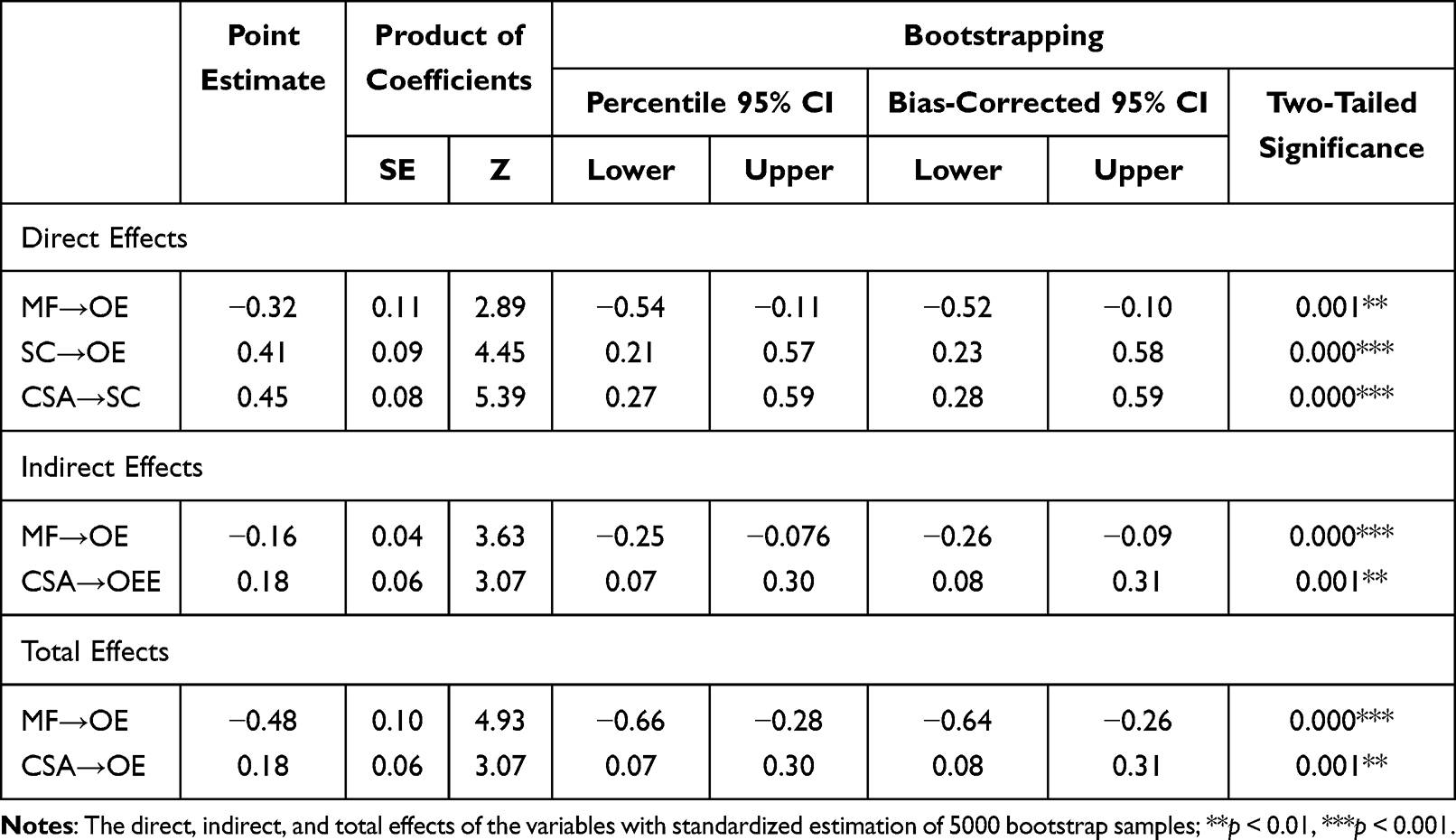 |
Table 4 Standardized Direct, Indirect, and Total Effects |
Discussion
The purpose of this investigation was to examine the relations among mindfulness, competitive state anxiety, self-criticism, and obligatory exercise in a sample of elite athletes. The theoretical hypotheses, H1, H3, H4, H5, and H6, were proposed before the results of the SEM and mediation test were performed. Positive thoughts through mindfulness achieved the purpose of reducing the athletes’ self-criticism and competitive state anxiety. However, it is worth noting that the results of the research did not support hypothesis H2, as there was no significant relation between competitive anxiety and obligatory exercise behavior. Instead, self-criticism mediated competitive anxiety’s effect on obligatory exercise completely. In fact, the obligatory exercise behavior mentioned above is described as a symptom of abstinence, in that the individual will engage in obligatory exercise to avoid the negative emotional effects of stopping exercise suddenly, but this does not mean that the negative emotions related to exercise will be able to change the cognitive evaluation (B) related to this incident directly. In this study, competitive state anxiety was defined as a specific negative emotional state related to sports competition. Both this and the obligatory exercise are consequence (C), while self-criticism is a more stable personality characteristic, in which criticism and the concept of perfectionism are similar and are (belief) B. According to ABC theory, the relation between ABC does not always follow A-B-C, but can be considered a second-order relation, A-B-C-A-B, in which C can affect B as well,28 and as H2 was not supported, it may be explained effectively, in that competitive state anxiety (C) in the C-B-C1 relation is followed by self-criticism (B) in obligatory exercise behavior.
In addition, the research results showed that these factors combined explained 37% of the variance in participants’ obligatory exercise behavior, which is higher than the 31% found in previous research,9 and thus needs to be explored further. Obligatory exercise is the general manifestation of athletes’ high degree of recognition of their goal, and efforts to support or strengthen their self-image through activities, so that performance achievements in the event become an important way to reflect their value, and when they realize that they are unable to compete, they feel a strong sense of loss of self. When there are advantages in the event, they often show a strong desire to control and even stabilize their position in the event through self-sacrifice.74 This has great similarities with self-criticism, which emphasizes the characteristics of achieving goals and self-worth. Self-criticism increases their excessive attention to, and evaluation of, achieving performance goals, which leads to obligatory exercise behavior. Studies have shown that self-criticism is similar to perfectionism, in that both are manifested as higher personal standards and excessive attention to their errors.22
It is worth noting that most of the current research on obligatory exercise focuses on individuals with eating disorders,37,75 and is less concerned about athletes.75,76 Although this is consistent with certain characteristics of obligatory exercise, the two still have highly different motivations. Studies have shown that excessive efforts may be the universal feature of some high-level athletes.16 When athletes recognize themselves and their current performance goals, they often have higher personal standards, and they also show excessive attention to errors. When athletes regard sports achievements as the only way to realize the value of life, they will focus great attention on their training. Once they encounter obstacles in training, they are prone to anxiety and have greater doubts about self-worth. In turn, obligatory exercise may compound their current unfavorable condition by causing re-injury.9 A common phenomenon among many athletes is that when their doctors or coaches tell them that they have suffered an injury and advise them to stop training, they still choose to continue to exercise vigorously; in fact, elite athletes are a special group. Unlike ordinary sports enthusiasts, exercise is not only their hobby; it is also their profession, and training occupies nearly all of their lives. At the same time, athletes are restricted by the sports ethics of “sacrifice”;
Real athletes must put their love competitions on anything else and allow other interests to obey the interests they are engaged in the interests of their movements, and athletes must pay for the competition.
Winning, surpassing or controlling others, pursuing excellence, and working hard to achieve first place mean everything to them.77 Under the influence of exercise ethics, athletes often manifest an excessive observance of rules, which are important reasons for their obligatory exercise.
This study found that compared with athletes in good physical condition, those who are recovering from an injury are more likely to engage in obligatory exercise. On the one hand, sports injuries are an emergency condition and exert negative emotional pressure on athletes. Some athletes with high self-esteem often try to take the initiative to eliminate this negative emotion through continued exercise. On the other hand, some athletes will not take the risk of ending their careers early to eliminate this negative emotion. Inaccurate judgment of their physical recovery or being too eager to return to the game results in a high incidence of compulsive sports behavior.78,79 Based upon this, it may help athletes who are recovering from injuries eliminate negative emotions through mindfulness exercises that will reduce their obligatory exercise.80 Mindfulness cultivates individuals’ ability to observe emotions other than their own (as the perceiver of emotions, not the parties involved), which increases their “degree of freedom” to cope with these states, improves their ability to control and regulate emotions and then alleviates the maladaptation related to this negative emotion promptly.81 At the same time, mindfulness’s positive effect on improving individuals’ cognitive ability also reduces their IB to a certain extent, which improves athletes’ mental health and reduces the incidence of their obligatory exercise behavior.
Theoretical Contributions and Practical Implications
This study makes the following contributions to obligatory exercise research. First, previous studies that have investigated obligatory exercise behaviors focused on individuals with other problems, such as eating disorders. Instead, this study focused on athletes during the recovery period because they are also a group that is more prone to obligatory exercise behaviors, and analyzed the antecedents of the two compulsive behaviors from the perspective of individual behavioral motivation. This provided a theoretical basis for future research on different groups’ obligatory exercise. Second, most of the previous studies on obligatory exercise have discussed personality traits, and given less attention to the influence of specific situational factors on obligatory exercise behavior. We explored the antecedents of athletes’ obligatory exercise during the recovery period jointly, and provided a theoretical basis to reduce the problem from the perspective of cognitive behavioral therapy by selecting the variable of mindfulness; third, the ABC theory informed this study and provided a theoretical basis to explain the interaction between the variables examined, in which competitive state anxiety (C) exerted an influence on obligatory exercise (C1) through self-criticism (B), and mindfulness had a positive influence on competitive state anxiety and self-criticism. In turn, this decreased athletes’ obligatory exercise behaviors, which further expanded the theoretical boundaries of cognitive behavioral therapy.
Studies have shown that obligatory exercise behavior has a high probability of causing re-injury in athletes, which is very likely to shorten their careers. In many cases, it is difficult for athletes to distinguish between overtraining and obligatory exercise effectively, which is an important cause of obligatory exercise behavior. The confusion between Functional Overreaching (FOR) and obligatory exercise is a big reason for this research situation, and successful training must involve moderate overload in order to maximize the body’s potential (this is called Functional Overreaching in training).76 Generally speaking, the premise of pursuing overtraining is to ensure scientific training. Overtraining is controllable and attempts to maximize the training benefits to ensure as much as possible that the athlete’s body is not damaged. On the other hand, the athlete’s motivation controls obligatory exercise to a greater extent, and many factors affect training motivation itself. Different athletes have different motivations to exercise, which makes this situation uncontrollable. Athletes rely on their subjective judgments to force themselves to exercise, which does not guarantee that the behavior is scientific, and thus, can easily cause sports injuries. The long offseason causes athletes who are recovering from injuries to face more emotional problems, and family, spectators, teammates, and coaches may all become sources of stress. These negative emotions prompt athletes to want to overcome their injuries urgently.79 However, this is precisely an important reason for their obligatory exercise behavior. However, mindfulness therapy based upon ABC theory appears to provide theoretical support for the ability to decrease athletes’ obligatory exercise behavior during the recovery period, as from the perspective of cognitive behavioral therapy, mindfulness therapy eliminates or reduces their compulsive behavior timely. Mindfulness relieves negative emotions, and thus achieves the purpose of preventing or reducing obligatory exercise behavior.
Limitations
This study has certain limitations that future research can examine, for example, the psychological mechanisms underlying the relation between various motivational states and obligatory exercise patterns. At the same time, longitudinal studies based upon mindfulness interventions can also be attempted, and the selection of research groups can be more extensive.
Conclusion
Overall, athletes’ obligatory exercise behavior while they are recovering from injury is an important cause of their re-injury. Cognitive behavioral therapy based upon ABC theory provides a theoretical basis to reduce obligatory exercise. This study verified the adverse effects of negative emotions on athletes’ obligatory exercise behavior, and explored mindfulness’s positive effect on reducing their obligatory exercise by eliminating or reducing the negative emotions associated with their injury, as well as the IB related to exercise. The results of the study showed that both self-criticism and competitive state anxiety were related closely to obligatory exercise behavior, but competitive state anxiety did not predict obligatory exercise significantly. Instead, self-criticism and competitive state anxiety mediated the effect in part.
Data Sharing Statement
The data can be made available on reasonable request from the corresponding author.
Institutional Review Board Statement
The study has obtained informed consent from all minor’s participants (under the age of 18) and their guardians and informed consent from all adult participants. The research project has received an approval on human research protection by the Ethics Committee of the School of physical Education, Hunan University of Science and Technology, which is in full compliance with international guidelines of human research protection such as Declaration of Helsinki, CLOMS Guidelines, and the Belmont Report. (No. ECSPEHUST 2022/0030).
Funding
This study was supported by the Hunan Provincial Social Science Committee (No. XSP21YBZ163) and the Scientific Research Fund of Hunan University of Science and Technology (No. E52203).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Maffulli N, Longo UG, Gougoulias N, Caine D, Denaro V. Sport injuries: a review of outcomes. Br Med Bull. 2011;97(1):47–80. doi:10.1093/bmb/ldq026
2. Johansson C. Injuries in elite orienteers. Am J Sports Med. 1986;14(5):410–415. doi:10.1177/036354658601400515
3. Dubravcic-Simunjak S, Pecina M, Kuipers H, Moran J, Haspl M. The incidence of injuries in elite junior figure skaters. Am J Sports Med. 2003;31(4):511–517. doi:10.1177/03635465030310040601
4. Galambos SA, Terry PC, Moyle GM, Locke SA. Psychological predictors of injury among elite athletes. Br J Sports Med. 2005;39(6):351. doi:10.1136/bjsm.2005.018440
5. Kvist J, Ek A, Sporrstedt K, Good L. Fear of re-injury: a hindrance for returning to sports after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2005;13(5):393–397. doi:10.1007/s00167-004-0591-8
6. Draeger J, Yates A, Crowell D. The Obligatory Exerciser. Phys Sportsmed. 2005;33(6):13–23. doi:10.3810/psm.2005.06.101
7. Christakou A, Stavrou NA, Psychountaki M, Zervas Y. Re-injury worry, confidence and attention as predictors of a sport re-injury during a competitive season. Res Sports Med. 2022;30(1):19–29. doi:10.1080/15438627.2020.1853542
8. Podlog L, Dimmock J, Miller J. A review of return to sport concerns following injury rehabilitation: practitioner strategies for enhancing recovery outcomes. Phys Ther Sport. 2011;12(1):36–42. doi:10.1016/j.ptsp.2010.07.005
9. Hall HK, Kerr AW, Kozub SA, Finnie SB. Motivational antecedents of obligatory exercise: the influence of achievement goals and multidimensional perfectionism. Psychol Sport Exerc. 2007;8(3):297–316. doi:10.1016/j.psychsport.2006.04.007
10. Lichtenstein MB, Hinze CJ, Emborg B, Thomsen F, Hemmingsen SD. Compulsive exercise: links, risks and challenges faced. Psychol Res Behav Manag. 2017;10:85–95. doi:10.2147/PRBM.S113093
11. Hausenblas HA, Downs DS. Exercise dependence: a systematic review. Psychol Sport Exerc. 2002;3(2):89–123. doi:10.1016/S1469-0292(00)00015-7
12. Ogilvie L, Carson J. Positive addiction recovery therapy: a pilot study. Adv Dual Diagn. 2022;15(4):196–207. doi:10.1108/ADD-06-2022-0018
13. Landolfi E. Exercise addiction. Sports Med. 2013;43(2):111–119. doi:10.1007/s40279-012-0013-x
14. Adams J, Kirkby RJ. Excessive Exercise as an Addiction: a Review. Addict Res Theory. 2002;10(5):415–437. doi:10.1080/1606635021000032366
15. Duncan LR, Hall CR, Fraser SN, Rodgers WM, Wilson PM, Loitz CC. Re-examining the Dimensions of Obligatory Exercise. Meas Phys Educ Exerc Sci. 2012;16(1):1–22. doi:10.1080/1091367X.2012.641442
16. Curran T, Hill AP, Jowett GE, Mallinson-Howard SH. The relationship between multidimensional perfectionism and passion in junior athletes. Int J Sport Psychol. 2014;45(4):369–384. doi:10.7352/IJSP2014.45.369
17. Butler AC, Chapman JE, Forman EM, Beck AT. The empirical status of cognitive-behavioral therapy: a review of meta-analyses. Clin Psychol Rev. 2006;26(1):17–31. doi:10.1016/j.cpr.2005.07.003
18. Roemer L, Orsillo SM. Expanding our conceptualization of and treatment for generalized anxiety disorder: integrating mindfulness/acceptance-based approaches with existing cognitive-behavioral models. Clin Psychol Sci Pract. 2002;9(1):54–58. doi:10.1093/clipsy.9.1.54
19. Wolfsdorf BA, Zlotnick C. Affect management in group therapy for women with posttraumatic stress disorder and histories of childhood sexual abuse. J Clin Psychol. 2001;57(2):169–181. doi:10.1002/1097-4679(200102)57:2<169::AID-JCLP4>3.0.CO;2-0
20. Garland EL, Roberts-Lewis A, Tronnier CD, Graves R, Kelley K. Mindfulness-Oriented Recovery Enhancement versus CBT for co-occurring substance dependence, traumatic stress, and psychiatric disorders: proximal outcomes from a pragmatic randomized trial. Behav Res Ther. 2016;77:7–16. doi:10.1016/j.brat.2015.11.012
21. Kristeller JL, Hallett CB. An exploratory study of a meditation-based intervention for binge eating disorder. J Health Psychol. 1999;4(3):357–363. doi:10.1177/135910539900400305
22. Dunkley DM, Zuroff DC, Blankstein KR. Specific perfectionism components versus self-criticism in predicting maladjustment. Pers Individ Dif. 2006;40(4):665–676. doi:10.1016/j.paid.2005.08.008
23. Blatt SJ, Homann E. Parent-child interaction in the etiology of dependent and self-critical depression. Clin Psychol Rev. 1992;12(1):47–91. doi:10.1016/0272-7358(92)90091-L
24. Cox BJ, Fleet C, Stein MB. Self-criticism and social phobia in the US national comorbidity survey. J Affect Disord. 2004;82(2):227–234. doi:10.1016/j.jad.2003.12.012
25. Dunkley DM, Grilo CM. Self-criticism, low self-esteem, depressive symptoms, and over-evaluation of shape and weight in binge eating disorder patients. Behav Res Ther. 2007;45(1):139–149. doi:10.1016/j.brat.2006.01.017
26. Kopala-Sibley DC, Zuroff DC, Russell JJ, Moskowitz DS, Paris J. Understanding heterogeneity in borderline personality disorder: differences in affective reactivity explained by the traits of dependency and self-criticism. J Abnorm Psychol. 2012;121(3):680–691. doi:10.1037/a0028513
27. Fazaa N, Page S. Personality style and impulsivity as determinants of suicidal subgroups. Arch Suicide Res. 2009;13(1):31–45. doi:10.1080/13811110802572122
28. Ellis A. An Operational Reformulation of Some of the Basic Principles of Psychoanalysis. University of Minnesota Press; 1956:131–135.
29. Ellis A. Expanding the ABCs of RET. J Rational Emot Ther. 1984;2(2):20–24. doi:10.1007/BF02281207
30. Woods PJ, Ellis A. Supervision in rational emotive behavior therapy. J Ration Emot Cogn Behav Ther. 1996;14(2):135–152. doi:10.1007/BF02238187
31. Lazarus RS. Stress and Emotion: A New Synthesis. Springer publishing company; 2006.
32. Muran JC. A reformulation of the ABC model in cognitive psychotherapies: implications for assessment and treatment. Clin Psychol Rev. 1991;11(4):399–418. doi:10.1016/0272-7358(91)90115-B
33. Rodgers WM, Hall CR, Blanchard CM, Munroe KJ. Prediction of obligatory exercise by exercise-related imagery. Psychol Addict Behav. 2001;15(2):152–154. doi:10.1037/0893-164X.15.2.152
34. Mond JM, Hay PJ, Rodgers B, Owen C. An update on the definition of “excessive exercise” in eating disorders research. Int J Eat Disord. 2006;39(2):147–153. doi:10.1002/eat.20214
35. Bamber DJ, Cockerill IM, Rodgers S, Carroll D. Diagnostic criteria for exercise dependence in women. Br J Sports Med. 2003;37(5):393. doi:10.1136/bjsm.37.5.393
36. Dweck CS. Self-Theories: Their Role in Motivation, Personality, and Development. Psychology press; 2000.
37. Meyer C, Taranis L, Goodwin H, Haycraft E. Compulsive exercise and eating disorders. Eur Eat Disord Rev. 2011;19(3):174–189. doi:10.1002/erv.1122
38. Reina CS, Kudesia RS. Wherever you go, there you become: how mindfulness arises in everyday situations. Organ Behav Hum Decis Process. 2020;159:78–96. doi:10.1016/j.obhdp.2019.11.008
39. Bishop SR, Lau M, Shapiro S, et al. Mindfulness: a proposed operational definition. Clin Psychol Sci Pract. 2004;11(3):230–241. doi:10.1093/clipsy.bph077
40. Teasdale JD. Metacognition, mindfulness and the modification of mood disorders. Clin Psychol Psychother. 1999;6(2):146–155. doi:10.1002/(SICI)1099-0879(199905)6:2<146::AID-CPP195>3.0.CO;2-E
41. Brown KW, Ryan RM, Creswell JD. Mindfulness: theoretical Foundations and Evidence for its Salutary Effects. Psychol Inq. 2007;18(4):211–237. doi:10.1080/10478400701598298
42. Creswell JD. Mindfulness Interventions. Annu Rev Psychol. 2017;68(1):491–516. doi:10.1146/annurev-psych-042716-051139
43. Shapiro SL, Carlson LE, Astin JA, Freedman B. Mechanisms of mindfulness. J Clin Psychol. 2006;62(3):373–386. doi:10.1002/jclp.20237
44. Brown KW, Ryan RM. The benefits of being present: mindfulness and its role in psychological well-being. J Pers Soc Psychol. 2003;84(4):822–848. doi:10.1037/0022-3514.84.4.822
45. Edenfield TM, Saeed SA. An update on mindfulness meditation as a self-help treatment for anxiety and depression. Psychol Res Behav Manag. 2012;131–141. doi:10.2147/PRBM.S34937
46. Chen J-H, Tsai P-H, Lin Y-C, Chen C-K, Chen C-Y. Mindfulness training enhances flow state and mental health among baseball players in Taiwan. Psychol Res Behav Manag. 2018;15–21. doi:10.2147/PRBM.S188734
47. Cupal DD. Psychological interventions in sport injury prevention and rehabilitation. J Appl Sport Psychol. 1998;10(1):103–123. doi:10.1080/10413209808406380
48. Cox RH, Martens MP, Russell WD. Measuring anxiety in athletics: the revised competitive state anxiety inventory–2. J Sport Exerc Psychol. 2003;25(4):519–533. doi:10.1123/jsep.25.4.519
49. Burton D. Do anxious swimmers swim slower? Reexamining the elusive anxiety-performance relationship. J Sport Exerc Psychol. 1988;10(1):45–61. doi:10.1123/jsep.10.1.45
50. Jones JG, Cale A. Relationships between multidimensional competitive state anxiety and cognitive and motor subcomponents of performance. J Sports Sci. 1989;7(3):229–240. doi:10.1080/02640418908729843
51. Jones G, Swain A. Intensity and Direction as Dimensions of Competitive State Anxiety and Relationships with Competitiveness. Percept Mot Skills. 1992;74(2):467–472. doi:10.2466/pms.1992.74.2.467
52. Crocker PRE, Alderman RB, Murray F, Smith R. Cognitive-affective stress management training with high performance youth volleyball players: effects on affect, cognition, and performance. J Sport Exerc Psychol. 1988;10(4):448–460. doi:10.1123/jsep.10.4.448
53. Hammermeister J, Burton D. Anxiety and the Ironman: investigating the antecedents and consequences of endurance athletes’ state anxiety. Sport Psychol. 1995;9(1):29–40. doi:10.1123/tsp.9.1.29
54. Ntoumanis N, Biddle S. The relationship between competitive anxiety, achievement goals, and motivational climates. Res Q Exerc Sport. 1998;69(2):176–187. doi:10.1080/02701367.1998.10607682
55. Beauchamp MR, Bray SR, Eys MA, Carron AV. The effect of role ambiguity on competitive state anxiety. J Sport Exerc Psychol. 2003;25(1):77–92. doi:10.1123/jsep.25.1.77
56. Tsopani D, Dallas G, Skordilis EK. Competitive state anxiety and performance in young female rhythmic gymnasts. Percept Mot Skills. 2011;112(2):549–560. doi:10.2466/05.09.20.PMS.112.2.549-560
57. Blatt SJ, Luyten P. A structural–developmental psychodynamic approach to psychopathology: two polarities of experience across the life span. Dev Psychopathol. 2009;21(3):793–814. doi:10.1017/S0954579409000431
58. Dunkley DM, Kyparissis A. What is DAS self-critical perfectionism really measuring? Relations with the five-factor model of personality and depressive symptoms. Pers Individ Dif. 2008;44(6):1295–1305. doi:10.1016/j.paid.2007.11.022
59. Whelton WJ, Greenberg LS. Emotion in self-criticism. Pers Individ Dif. 2005;38(7):1583–1595. doi:10.1016/j.paid.2004.09.024
60. Thompson R, Zuroff DC. The Levels of Self-Criticism Scale: comparative self-criticism and internalized self-criticism. Pers Individ Dif. 2004;36(2):419–430. doi:10.1016/S0191-8869(03)00106-5
61. Cunha M, Paiva MJ. Text anxiety in adolescents: the role of self-criticism and acceptance and mindfulness skills. Span J Psychol. 2012;15(2):533–543. doi:10.5209/rev_SJOP.2012.v15.n2.38864
62. Kolt GS, Kirkby RJ. Injury, anxiety, and mood in competitive gymnasts. Percept Mot Skills. 1994;78(3):955–962. doi:10.1177/003151259407800351
63. Steffen JJ, Brehm BJ. The Dimensions of Obligatory Exercise. Eat Disord. 1999;7(3):219–226. doi:10.1080/10640269908249287
64. Baer RA, Smith GT, Lykins E, et al. Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment. 2008;15(3):329–342. doi:10.1177/1073191107313003
65. Kimberlin CL, Winterstein AG. Validity and reliability of measurement instruments used in research. Am J Health Syst Pharm. 2008;65(23):2276–2284. doi:10.2146/ajhp070364
66. Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. 1981;18(1):39–50. doi:10.1177/002224378101800104
67. Hair JF, Sarstedt M, Ringle CM, Mena JA. An assessment of the use of partial least squares structural equation modeling in marketing research. J Acad Mark Sci. 2012;40:414–433. doi:10.1007/s11747-011-0261-6
68. Anderson JC, Gerbing DW. Structural equation modeling in practice: a review and recommended two-step approach. Psychol Bull. 1988;103(3):411. doi:10.1037/0033-2909.103.3.411
69. Hair JF, Sarstedt M, Pieper TM, Ringle CM. The use of partial least squares structural equation modeling in strategic management research: a review of past practices and recommendations for future applications. Long Range Plann. 2012;45(5):320–340. doi:10.1016/j.lrp.2012.09.008
70. Podsakoff PM, MacKenzie SB, Podsakoff NP. Sources of method bias in social science research and recommendations on how to control it. Annu Rev Psychol. 2012;63(1):539–569. doi:10.1146/annurev-psych-120710-100452
71. Lindell MK, Whitney DJ. Accounting for common method variance in cross-sectional research designs. J Appl Psychol. 2001;86(1):114–121. doi:10.1037/0021-9010.86.1.114
72. Jackson DL, Gillaspy JA, Purc-Stephenson R. Reporting practices in confirmatory factor analysis: an overview and some recommendations. Psychol Methods. 2009;14(1):6–23. doi:10.1037/a0014694
73. Bollen KA, Stine R. Direct and indirect effects: classical and bootstrap estimates of variability. Sociol Methodol. 1990;20:115–140. doi:10.2307/271084
74. O’Connor S, Moloney A, Beidler E, et al. Post-injury fear-avoidance and confidence in readiness to return to sport in Irish collegiate athletes. J Sports Sci. 2022;40(17):1973–1980. doi:10.1080/02640414.2022.2123519
75. Cook BJ, Hausenblas HA. The role of exercise dependence for the relationship between exercise behavior and eating pathology: mediator or moderator? J Health Psychol. 2008;13(4):495–502. doi:10.1177/1359105308088520
76. Meeusen R, Duclos M, Foster C, et al. Prevention, diagnosis and treatment of the overtraining syndrome: joint consensus statement of the European College of Sport Science (ECSS) and the American College of Sports Medicine (ACSM). Eur J Sport Sci. 2013;13(1):1–24. doi:10.1080/17461391.2012.730061
77. Hughes R, Coakley J. Positive deviance among athletes: the implications of overconformity to the sport ethic. Sociol Sport J. 1991;8(4):307–325. doi:10.1123/ssj.8.4.307
78. BulletinQuinn AM, Fallon BJ. The changes in psychological characteristics and reactions of elite athletes from injury onset until full recovery. J Appl Sport Psychol. 1999;11(2):210–229. doi:10.1080/10413209908404201
79. Conti C, Di Fronso S, Pivetti M, Robazza C, Podlog L, Bertollo M. Well-come back! Professional basketball players perceptions of psychosocial and behavioral factors influencing a return to pre-injury levels. Front Psychol. 2019;10(FEB). doi:10.3389/fpsyg.2019.00222
80. Bondár RZ, Robazza C, Di Fronso S, Bertollo M. Personality traits and psychobiosocial states among athletes: the mediating role of dispositional mindfulness. Sport Exerc Perform. 2022;11(4):397–411. doi:10.1037/spy0000300
81. Fronso S, Robazza C, Bondár RZ, Bertollo M. The effects of mindfulness-based strategies on perceived stress and psychobiosocial states in athletes and recreationally active people. IJERPH. 2022;19(12):1–12. doi:10.3390/ijerph19127152
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.