Back to Journals » Journal of Pain Research » Volume 19
Effects of Lung-Protective Ventilation on Cerebral Oxygenation During One-Lung Ventilation in Neonates
Authors Lv L, Zhang WZ, Zhang HP, Wei YW, Duan JW, Ren JM
Received 7 August 2025
Accepted for publication 23 January 2026
Published 16 February 2026 Volume 2026:19 559083
DOI https://doi.org/10.2147/JPR.S559083
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Helen Koechlin
Lei Lv,1 Wei-Zhi Zhang,1 Hong-Peng Zhang,1 Yun-Wei Wei,1 Jin-Wei Duan,1 Jun-Ming Ren2
1Department of Anesthesiology, Shanxi Provincial Children’s Hospital, Taiyuan, Shanxi, 030013, People’s Republic of China; 2Department of Anesthesiology, Shanxi Provincial People’s Hospital, Taiyuan, Shanxi, 030012, People’s Republic of China
Correspondence: Jun-Ming Ren, Department of Anesthesiology, Shanxi Provincial People’s Hospital, Taiyuan, Shanxi, 030012, People’s Republic of China, Tel +86 03514960423, Email [email protected]
Objective: This study aimed to investigate the effects of different lung ventilation strategies on cerebral oxygen saturation (rSO2) during one-lung ventilation (OLV) in neonates.
Methods: A total of 50 neonates scheduled for elective OLV between October 2022 and April 2024 were enrolled and randomly assigned to either the control group (Group C) or the study group (Group S). In Group S, the respiratory rate was adjusted to maintain end-tidal carbon dioxide (PETCO2) levels between 45– 55 mmHg at 30 minutes of OLV (T3) and subsequently restored to normal levels (35– 45 mmHg) at 45 minutes of OLV (T4). Lung recruitment maneuvers were applied. In Group C, PETCO2 was maintained within the normal range throughout the procedure. Oxygen saturation (SpO2) and rSO2, along with additional physiological parameters, were recorded at five time points: before OLV (T1), 15 minutes after OLV initiation (T2), T3, T4, and 60 minutes after OLV initiation (T5). Arterial blood samples were collected for blood gas analysis.
Results: In both groups, rSO2 levels significantly decreased during OLV compared to baseline (T1) (p < 0.05). However, at T3, rSO2 was significantly higher in Group S compared to Group C. Comparisons within the group indicated that rSO2 in Group S at T3 was significantly higher than at T5. Lung compliance was superior in Group S compared to Group C at T5. Furthermore, lung compliance in both groups decreased at T2 when compared to T1 (p < 0.05).
Conclusion: Despite maintaining SpO2 within the normal range, rSO2 declined during OLV in neonates. The application of permissive hypercapnia during OLV improved rSO2 within a certain range. Routine perioperative monitoring of rSO2 in neonates undergoing OLV may facilitate early detection of cerebral oxygenation changes, contributing to neuroprotection.
Keywords: cerebral oxygen saturation, hypercapnia, lung protected ventilation, lung recruitment, neonates, one lung ventilation
Introduction
With the rapid advancement of endoscopic technology, minimally invasive surgical techniques in thoracic and cardiac surgery have been widely adopted, facilitating the management of complex and technically demanding procedures.1 These surgical advancements are closely linked to the continuous refinement of anesthesia techniques and concepts. Several studies have reported varying degrees of cerebral oxygenation disturbances during one-lung ventilation (OLV).2–4 This imbalance is particularly pronounced in the growing population of pediatric patients undergoing major surgical interventions, as cerebral autoregulation may be compromised due to multiple contributing factors.4
Although routine intraoperative monitoring often indicates stable oxygen saturation (SpO2) levels, indicating that SpO2 monitoring alone may be insufficient for assessing cerebral oxygenation and perfusion in key target organs such as the brain.5 In contrast, rSO2 monitoring provides a non-invasive, real-time, and dynamic assessment of cerebral oxygenation, enabling the early identification and intervention of disruptions in cerebral oxygen supply-demand equilibrium. By facilitating timely adjustments, this technology contributes to maintaining cerebral oxygen homeostasis and has been widely implemented in various surgical settings.6,7 However, the specific patterns, clinical significance, and management strategies of rSO2 during OLV in neonatal patients are not completely understood and warrant further investigation.
The Lung-Protective Ventilation Strategy (LPVS) is a perioperative respiratory support strategy designed to prevent alveolar overdistension and collapse, promote the recruitment of atelectatic alveoli, minimize ventilator-induced lung injury, and reduce the incidence of perioperative pulmonary complications. When implemented appropriately, LPVS has the potential to decrease perioperative mortality while ensuring adequate oxygenation and ventilation. This strategy incorporates a range of respiratory management techniques, including the use of lower tidal volumes (VT, 6–8 mL/kg), reduced minute ventilation, optimized positive end-expiratory pressure (PEEP), lung recruitment, permissive hypercapnia (PHC), and low-concentration oxygen inhalation.8 Collectively, these measures mitigate mechanical stress-related lung injury, such as pressure-volume, and have been increasingly recognized as an effective protective ventilation strategy.9
This study aimed to evaluate the effects of LPVS on lung compliance, arterial oxygenation, hemodynamics, blood gas parameters, and rSO2 at multiple perioperative time points in neonates undergoing OLV. Additionally, postoperative complications were assessed to further investigate the impact of LPVS on decreased cerebral oxygen saturation (rSO2) during OLV.
Materials and Methods
Pediatric patients of all sexes who required elective thoracic surgery with OLV between October 2022 and April 2024 were included in the study. The types of surgery include congenital diaphragmatic hernia and congenital esophageal atresia.
Study Participants
Inclusion Criteria
1) Neonates aged from birth to 5 days, with no sex restriction. 2) Classified as American Society of Anesthesiologists (ASA) class I to III. 3) No history of severe cardiac, pulmonary, or cerebral comorbidities. 4) Scheduled for thoracic surgery requiring OLV with an expected surgical duration exceeding 30 minutes.
Exclusion Criteria
1) Pediatric patients older than 5 days. 2) Presence of severe cardiac, pulmonary, or cerebral diseases, including malignant arrhythmias, acute lung injury, acute respiratory distress syndrome, as well as children with respiratory failure caused by various reasons before the operation. 3) Diagnosis of acute respiratory failure due to various etiologies. 4) Children who had severe lung damage or respiratory distress syndrome and required tracheal intubation and ventilator support before the operation. 5) Presence of progressive neuromuscular disorders. 6) Diagnosis of sepsis or septic shock. 7) Presence of contraindications for lung recruitment, such as severe pulmonary arterial hypertension or intracranial hypertension. 8) Presence of traumatic or burn scars on the forehead that could interfere with rSO2 monitoring.
Withdrawal Criteria
1) Pediatric patients undergoing OLV for less than 30 minutes. 2) Pediatric patients who experienced severe intraoperative allergic reactions. 3) Pediatric patients who developed severe intraoperative cardiovascular or cerebrovascular events. 4) Cases with intraoperative blood loss exceeding 60mL. 5) Surgical procedures with a duration exceeding 5 hours.
Participant Grouping
Patients were randomly assigned to two groups using the random number table method. In Group C (control group), volume-control ventilation was applied. During two-lung ventilation (TLV), the ventilator settings included a tidal volume (VT) of 8 mL/kg, a PEEP of 5 cmH2O, and a fraction of inspired oxygen (FiO2) of 80%. During OLV, the VT was set at 6 mL/kg with a PEEP of 5 cmH2O. The respiratory rate (RR) was adjusted to maintain a PETCO2 level within the range of 35–45 mmHg. Following surgery, suctioning and sustained lung inflation were performed.
In Group S (study group), volume-control ventilation was used. The ventilator settings for TLV included a VT of 8 mL/kg, PEEP of 5 cmH2O, and FiO2 of 80%. During OLV, the VT was set at 6 mL/kg with a PEEP of 5 cmH2O. The RR was adjusted to maintain PETCO2 levels between 45–55 mmHg at time point T3 and returned to the normal range (35–45 mmHg) after T4. Lung recruitment maneuvers (RM) were implemented, consisting of three breaths (10 seconds per breath) with an inspiratory pressure of 30 cmH2O and a PEEP of 5 cmH2O, administered every 30 minutes.
Anesthetic Management
Preoperative Preparation
The surgical team directly engaged with the family of the patient to obtain a comprehensive history, including the current disease, prior surgical and anesthetic history, laboratory test results, and relevant ancillary examinations. Particular attention was given to cardiopulmonary, neurological, hepatic, and renal function, as these factors could influence surgical outcomes. The family was provided with detailed data regarding the significant anesthetic considerations, potential risks, and study objectives to ensure informed participation and cooperation. Written informed consent was obtained from all the patients’ parents or legal guardians before proceeding with the study.
On the day of surgery, preoperative anesthesia preparation included readying the anesthetic equipment, anesthetic agents, and patient-specific considerations. Upon the arrival of the patient in the operating room, a three-way verification process involving the surgeon, anesthesiologist, and circulating nurse was conducted to confirm patient identification before proceeding. Routine intraoperative monitoring included heart rate (HR), blood pressure (BP), SpO2, and electrocardiogram (ECG). Peripheral venous access was secured, followed by femoral artery puncture and catheterization for continuous arterial pressure monitoring after zero calibration. The necessity for central venous pressure (CVP) monitoring was determined based on the specific surgical procedure. Additionally, nasopharyngeal temperature was continuously monitored using a temperature probe throughout the procedure.
Designated personnel were responsible for monitoring and recording rSO2. After skin preparation, the sensor electrode patch was applied and subjected to a light-impermeable process to minimize interference from external light sources, ensuring accurate measurements.
Anesthesia Induction
Intravenous induction was performed using propofol at a dose of 2 mg/kg, succinylcholine at 2 mg/kg, and sufentanil at 0.2 µg/kg. OLV was performed using single-chamber bronchial intubation. Under video laryngoscopy, the glottic aperture was visualized and a cuffed endotracheal tube (size 3.0 #) was inserted. Following repositioning to the left-lateral decubitus position, the tube was advanced into the left mainstem bronchus under direct guidance of a flexible fiberoptic bronchoscope (diameter 2.2 mm). The depth of the tube was adjusted based on fiberbronchoscope to confirm proper placement. Once the correct positioning was verified, the endotracheal tube was secured with adhesive tape. Following successful intubation, the anesthetic ventilator was connected to initiate mechanical ventilation.
Anesthesia Maintenance
Anesthesia was maintained with inhaled sevoflurane (2–3%) supplemented by intermittent boluses of cisatracurium besylate and sufentanil as clinically indicated. Dopamine was administered to maintain mean arterial pressure (MAP) within 20% of baseline values. Bradycardia (defined as heart rate <60 beats/min) was treated with atropine boluses when required.
Anesthetic Recovery
Once the surgical procedure was performed and transition to TLV had occurred, the surgical lung and lung RM were suctioned. The patients were transferred back to the ICU with the endotracheal tube for further postoperative care.
Intraoperative Ventilation Management
Volume-targeted ventilation was selected, with TLV settings configured as follows: VT of 8 mL/kg, RR of 30 breaths per minute, an inspiratory-to-expiratory (I:E) ratio of 1:2, PEEP of 5 cmH2O, and a FiO2 of 80%. OLV was initiated prior to the commencement of surgery, with settings including a VT of 6 mL/kg, PEEP of 5 cmH2O, and an I:E ratio of 1:2. The RR was adjusted to maintain PETCO2 levels while ensuring that peak airway pressure remained below 30 cmH2O.
If a decrease in oxygen saturation (SpO2) below 80% occurred during the procedure, the following emergency interventions were implemented: 1) Verification of endotracheal tube positioning. 2) Assessment of airway pressures. 3) Evaluation of blood volume adequacy. 4) Adjustment of ventilatory parameters, including an increase in inspired oxygen concentration, modification of VT. 5) If necessary, resumption of TLV and termination of data collection for the affected case.
If necessary, the tracheal tube will be withdrawn to the main airway and OLV will be changed to double lung ventilation. These children will be removed from the rental.
This study utilized the INVOS 5100B device for measurement. This device employs continuous wave spectroscopy technology, using two near-infrared wavelengths of 730 and 805 nanometers to detect the ratio of oxyhemoglobin to total hemoglobin. The final result is presented in percentage form, representing the cerebral oxygen saturation value. It is safe and effective for newborns.
Anesthesia Observation Indicators
General Characteristics of the Participants
The patient’s age, sex, height, weight, ASA classification, duration of anesthesia, duration of surgery, duration of OLV, intraoperative blood loss, urine output, total volume of fluid administered, and the number of cases requiring intraoperative blood transfusion or vasoactive drug interventions were recorded and documented.
Data Collection Time Points
T1: before OLV.
T2: OLV 15 minutes.
T3: OLV 30 minutes.
T4: OLV 45 minutes.
T5: OLV 60 minutes.
Observation Indicators
1) The surgical duration, anesthesia duration, OLV duration, and intraoperative fluid balance were recorded for each pediatric patient. 2) Intraoperative parameters, including MAP, HR, RR, SpO2, plateau pressure, peak inspiratory pressure, static compliance (Cs), blood gas analysis, and rSO2 at various time points, were documented. 3) Peripheral venous blood of 2 mL was collected from the children before surgery and 6h after surgery, and the serum was separated by centrifugation at 3000 r/min for 10 min. The serum brain hemoglobin was detected by enzyme-linked immunosorbent assay. 4) After surgery, mechanical ventilation continued in the same mode. Chest X-ray was taken and recorded 2h after surgery to record whether pneumothorax occurred or not, and the time from the end of operation to the withdrawal of ventilator and the postoperative hospital stay were recorded.
Statistical Analysis
All the data collected in this study were analyzed using SPSS 20.0 software. Normally distributed measurement data were expressed as mean±standard deviation (SD), and the comparisons were examined by Student-t test and ANOVA test. The categorical data were expressed as n (%), and the differences between the two groups were examined by chi-square analysis or Fisher’s exact test. P<0.05 was considered statistically significant.
Results
General Data of Patients
A total of 50 patients were enrolled in the study, with 25 patients assigned to each group. However, in Group C, two cases had an OLV duration of less than 30 minutes, one case experienced an allergic reaction, and one case exhibited a decline in SpO2 below 80% during surgery. As a result, 21 patients were included in the final statistical analysis. Similarly, in Group S, two cases had an OLV duration of less than 30 minutes, and two cases were lost to follow-up, leading to the inclusion of 21 patients in the final analysis (Figure 1).
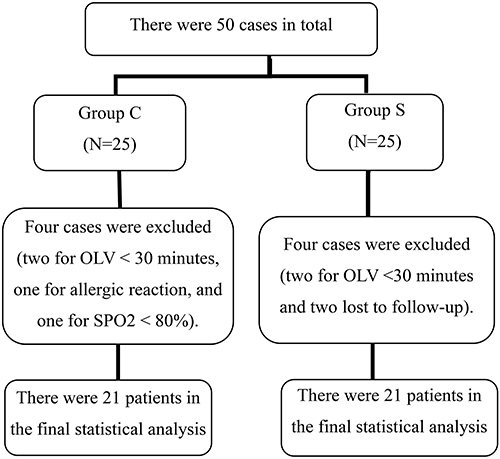 |
Figure 1 The study flow diagram depicts the movement of participants through each step of the randomized experiment. |
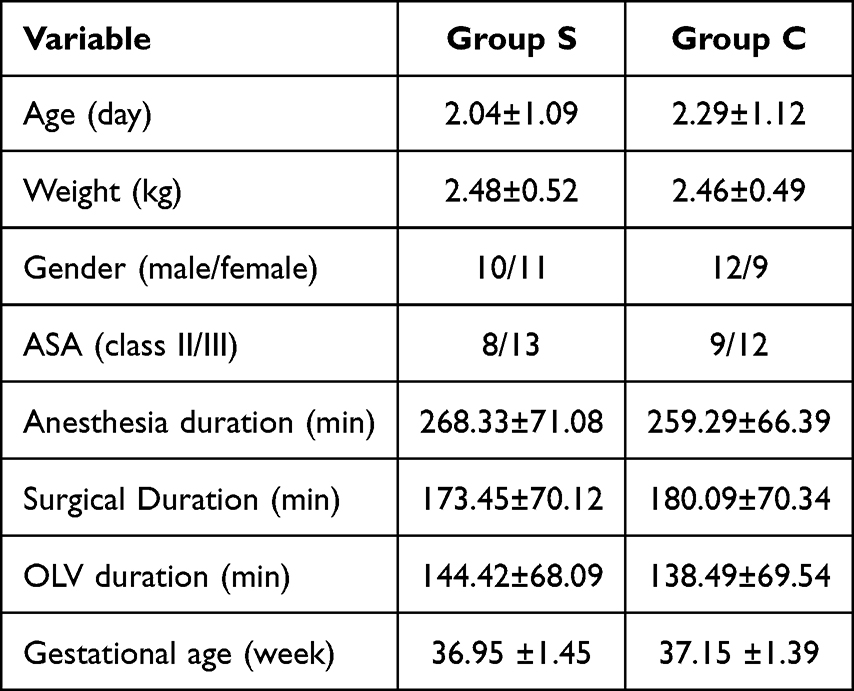
No statistically significant differences were observed between the two groups concerning general patient characteristics, including age, height, weight, sex, and ASA classification, as detailed in Table 1.
 |

Hemodynamic and Lung Compliance Changes
Despite the administration of dopamine to prevent significant reductions in MAP, patients in the study group exhibited lower MAP than those in the control group, which was attributed to the implementation of lung RM.
With respect to lung compliance, both groups experienced a decline in Cs upon transitioning from TLV to OLV (p = 0.005). However, in Group S, Cs improved at T5 following the application of RM and was significantly higher than that observed in the control group, demonstrating a statistically significant difference (p = 0.018). Detailed results are presented in Table 2 and Figure 2.
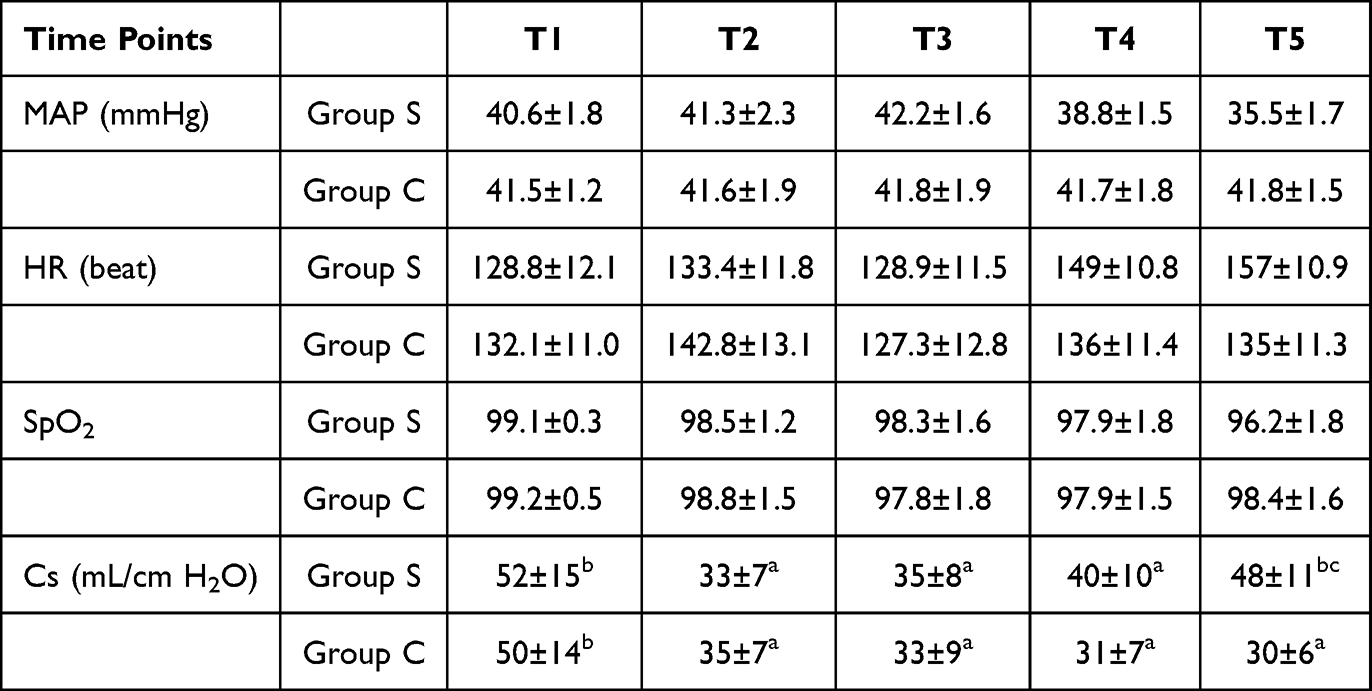 |
Table 2 Changes in MAP, HR, SpO2, and Lung Compliance at Various Time Points (n=21, |

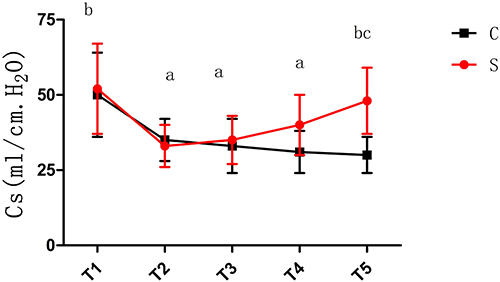 |
Figure 2 Depicts a comparison of Cs between the two patient groups.ap < 0.05 compared with T1; bp < 0.05 compared with T3; cp < 0.05 compared with Group C. |
Comparison of Arterial Blood Gas Analysis and Changes in rSO2
Intra-Group Comparisons: Compared to TLV at T1, a significant decrease in rSO2 was observed during OLV in both groups (p = 0.003). In Group S, as PaCO2 increased, PaO2, PaO2/FiO2 ratio, and rSO2 demonstrated relative improvements at T3, with statistically significant differences (p = 0.037). Following the application of lung RM, PaO2 and the PaO2/FiO2 ratio in Group S improved at T5, with statistically significant differences (p = 0.033), while rSO2 exhibited the most pronounced increase at T3, revealing a statistically significant difference (p = 0.007).
Inter-Group Comparisons: At T3, rSO2 in Group S was significantly higher than that in Group C (p = 0.006). Additionally, PaO2 and the PaO2/FiO2 ratio in Group S were significantly higher than those in Group C at both T3 and T5 (p = 0.015). Detailed results are presented in Table 3 and Figure 3.
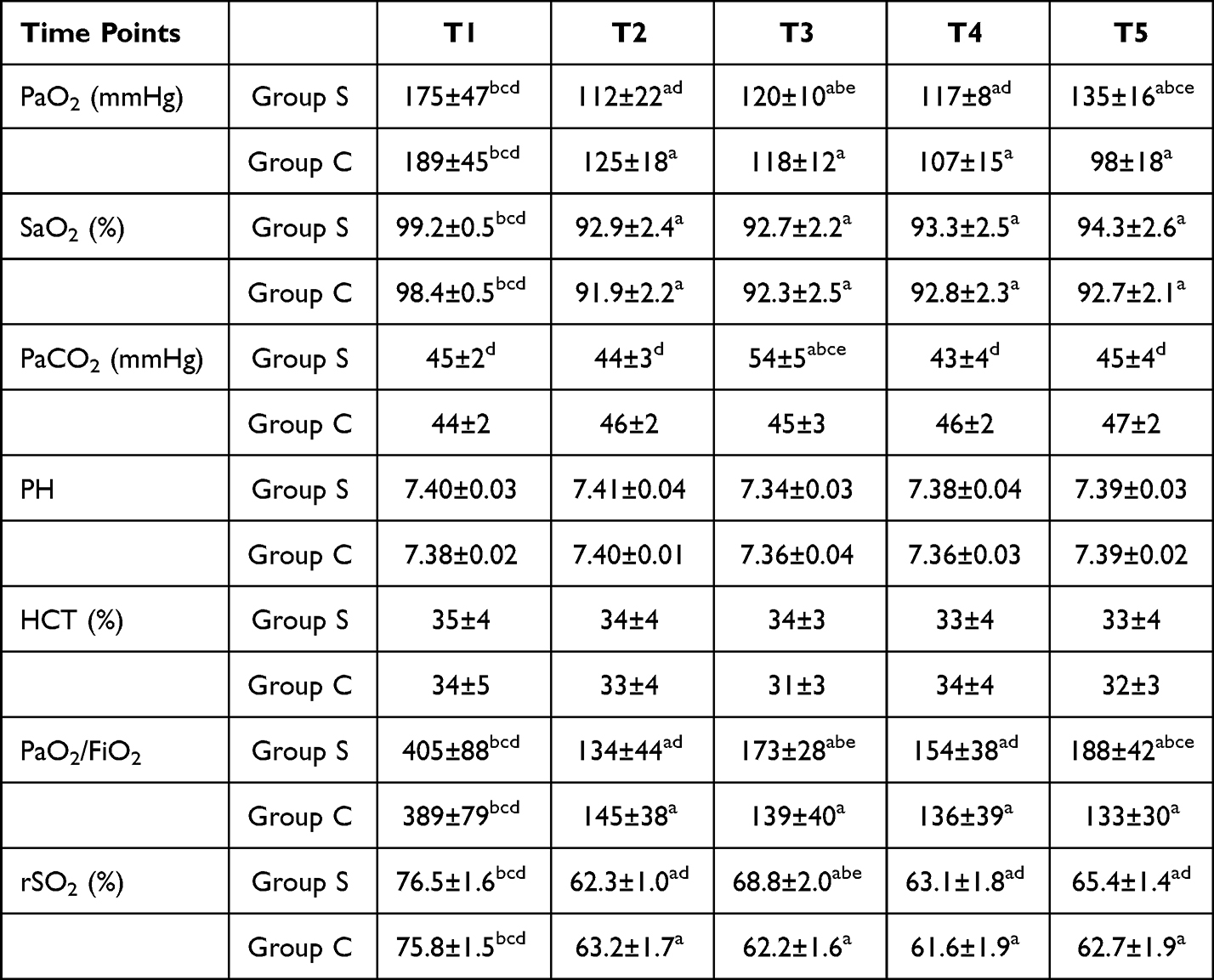 |
Table 3 Arterial Blood Gas Analysis Results and Changes in Cerebral Oxygen Saturation at Different Time Points (n=21, |

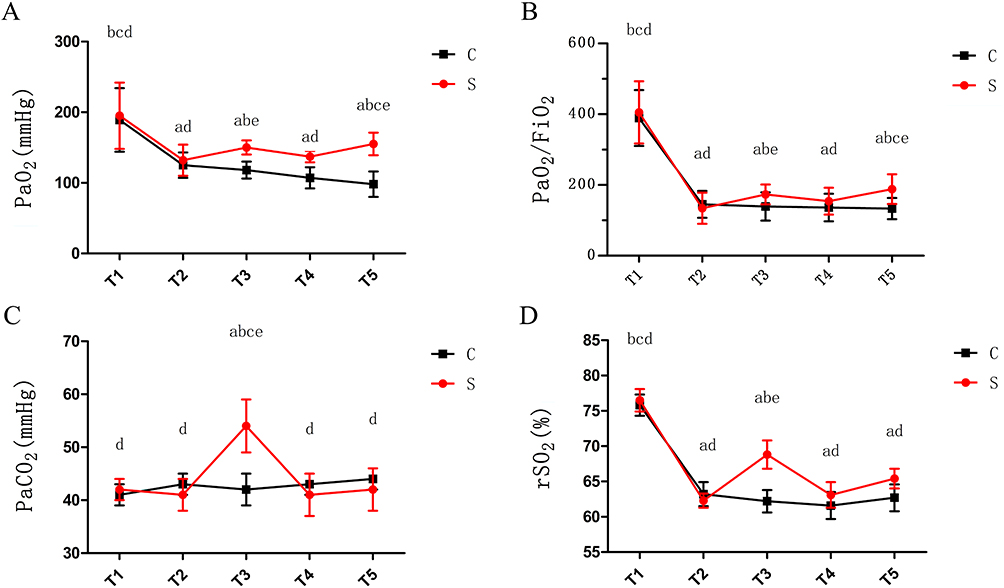 |
Figure 3 Comparison of PaO2 (A) PaO2/FiO2 (B) PaCO2 (C) and rSO2 (D) levels in the two patient groups. ap<0.05 compared with T1; bp<0.05 compared with T2; cp<0.05 compared with T4; dp<0.05 compared with T3; ep < 0.05 compared with Group C. |
The results of this study showed that there was no significant difference in the incidence of postoperative pneumothorax, time to extubation after surgery and length of stay between the two groups (p=0.020). The serum brain hemoglobin content was significantly lower in group S than in Group C 6 hours after surgery. Detailed results are presented in Table 4.
 |
Table 4 Comparison of Postoperative Pneumothorax Incidence, Hospital Stay Duration, Duration of Postoperative Mechanical Ventilation, and Serum Brain Hemoglobin Between the Two Groups |
Discussion
Perioperative rSO2 Monitoring
The INVOS 5100B is a non-invasive monitoring device based on near-infrared spectroscopy (NIRS) technology. It reflects the balance between cerebral oxygen supply and demand by detecting the ratio of oxygenated to deoxygenated hemoglobin in brain tissue. Its clinical applicability in neonates has been investigated. The INVOS 5100B can be used with different sensor models for adults, children, and neonates. Neonatal-specific sensors are designed with adapted light intensity and penetration depth to accommodate the unique physiological characteristics of newborns, featuring a more miniaturized and flexible design. rScO2 values measured with neonatal sensors are typically higher than those obtained with adult sensors (by up to 10%), but this difference is not constant and is smaller near thresholds indicative of cerebral hypoxia.10–12 It is important to note, however, that the calibration algorithms for this and most commercial NIRS devices were primarily developed and validated in adult populations. Applying these algorithms to neonates, despite using dedicated sensors, may introduce an inherent calibration bias. This potential bias is an important consideration when interpreting absolute rSO2 values.
A previous study have found that an increased depth and duration of desaturation below the 50% saturation threshold in the first 24 hours after cardiac surgery are associated with longer PICU and hospital stays and with longer duration of mechanical ventilation.13 These reductions are more frequently observed in pediatric patients undergoing major surgical procedures. Therefore, perioperative monitoring of rSO2 is essential not only for the early detection of changes in cerebral oxygenation but also for evaluating the effectiveness of intervention strategies, making it particularly relevant for pediatric patients undergoing OLV.
In this study, up to 28% of neonates experienced a decrease in rSO2 exceeding 20% from baseline during OLV. Notably, a decline in rSO2 was observed even in patients whose SpO2 remained within the normal range. Several factors may contribute to this phenomenon: (1) dysregulation of the ventilation/perfusion (V/Q) ratio due to OLV; (2) the impact of body positioning, general anesthesia, and thoracotomy on the V/Q ratio; and (3) the physiological characteristics of pediatric patients, including the incomplete development of organ and systemic functions, which increase the susceptibility to imbalances in cerebral oxygen supply and demand. When a reduction in rSO2 occurs,14 there may be a heightened incidence of postoperative agitation and behavioral changes, necessitating careful perioperative management and monitoring.
Perioperative monitoring of rSO2 is an advanced approach that provides real-time, non-invasive, and highly sensitive assessment of the balance between cerebral oxygen supply and demand. Unlike traditional monitoring methods, rSO2 measurement is user-friendly and remains unaffected by pulsatile blood flow. However, several factors can influence its accuracy, including the overall condition, inspired oxygen concentration, blood pressure, pH value, PaO2, PaCO2, body temperature, cranial bone density, probe positioning and spacing, as well as skin pigmentation of the patient.
Despite these limitations, the findings of this study indicate that perioperative monitoring of rSO2 trends enables the early detection of cerebral oxygenation changes, facilitates timely intervention, and reduces the incidence of postoperative complications. This approach holds significant value in protecting brain function and mitigating the risk of central nervous system complications in neonates undergoing OLV.
Lpvs
LPVS primarily consists of low VT ventilation, PEEP ventilation on the ventilated lung, continuous positive airway pressure (CPAP) ventilation on the non-ventilated lung, lung RM, and PHC. The management of the airway during OLV presents considerable challenges, as maintaining adequate ventilation often necessitates the use of higher VT, which can lead to alveolar overdistension and exacerbate ventilator-induced lung injury. Numerous studies support the implementation of LPVS in the perioperative management of OLV, demonstrating benefits that extend into the postoperative recovery period.15–18 In clinical practice, low VT ventilation, PEEP, and RM are commonly used to achieve lung-protective effects. Low VT ventilation, when compared to high VT mechanical ventilation, has been revealed to significantly reduce ventilator-associated lung injury.19 Findings from a study by Güldner et al indicate that low VT ventilation during OLV contributes to maintaining cerebral oxygen balance, potentially due to a reduction in mean intrathoracic pressure, which in turn enhances cerebral venous return.15 The VT was set at 8 mL/kg during two-lung ventilation (TLV) and 6 mL/kg during OLV for both study groups based on these considerations.
The selection of an appropriate PEEP level for the ventilated lung during surgery remains a subject of debate. Excessively high PEEP levels can increase pulmonary resistance and have been associated with a higher risk of postoperative pulmonary complications.20 Experimental studies propose that a PEEP level of 5–10 cm H2O is more effective in improving oxygenation compared to higher PEEP levels, potentially because this range enhances lung volume while at the same time improving lung compliance and reducing intrapulmonary shunting.21 Although various methods have been proposed for titrating PEEP levels, further research is needed to establish the most effective approach for selecting an optimal PEEP level in clinical practice. The primary criterion for determining the optimal PEEP level is its ability to sustain lung recruitment while preventing alveolar overdistension.22 RM and PEEP should be used as lung-protective strategies rather than solely as measures to improve oxygenation.15
In this study, a PEEP level of 5 cm H2O was combined with RM to mitigate atelectasis and counteract reductions in functional residual capacity, thereby optimizing oxygenation.
RM serves as a simple, cost-effective, and bedside-implementable protective intervention for lung ventilation. This technique involves the application of appropriate airway pressures to temporarily increase transpulmonary pressures, facilitating the reopening of collapsed alveoli. Once alveolar recruitment is achieved, improvements in pulmonary mechanics and gas exchange can be observed. However, the process of alveolar reopening may result in transient vascular compression, potentially leading to effects similar to alveolar overdistension, which may limit the expected improvement in gas exchange.23
Conventional sustained inflation, a commonly used RM technique, aims to maintain alveolar expansion but is often associated with respiratory and cardiovascular side effects. Additionally, the effectiveness of RM may be influenced by several factors, including the severity of lung injury, transpulmonary pressure, patient positioning, and cardiac preload. Theoretically, RM combined with PEEP should be initiated following the induction of general anesthesia and applied whenever a decline in blood oxygenation occurs during anesthesia maintenance. This approach allows for the maintenance of adequate oxygenation while minimizing the fraction of inspired oxygen, thereby promoting the re-expansion of collapsed alveoli and improving oxygenation.24
A study by Anup et al demonstrated that RM provided significant benefits in patients with moderate to severe acute respiratory distress syndrome (ARDS) by facilitating alveolar re-expansion.25 Furthermore, investigations have examined the application of RM in non-ARDS populations.26,27
Despite hemodynamic stabilization with vasoactive agents in the present study, a reduction in MAP was observed following RM, emphasizing the importance of close hemodynamic monitoring during its application. The findings indicated that, compared to Group C, lung compliance significantly improved in Group S after RM, with notable increases in PaO2 and the PaO2/FiO2 ratio. These results indicate that RM during OLV contributes to enhanced lung compliance and improved oxygenation to a certain extent.
PHC is a ventilation strategy used in situations where reducing ventilatory pressures while maintaining adequate gas exchange is not feasible. This approach allows for a moderate increase in PaCO2 and a certain degree of acidemia to minimize the risk of ventilator-induced lung injury associated with excessive VT. A study by Kregenow et al demonstrated the feasibility of moderate hypercapnia as a protective measure against lung injury in clinical practice.28 In recent years, the implementation of LPVS in patients with ARDS, acute lung injury, and other pulmonary conditions has revealed that hypercapnia exerts lung-protective effects, primarily by reducing lung injury. These benefits are believed to result from the anti-inflammatory properties of hypercapnia and its role in preserving the ventilation/perfusion (V/Q) ratio, thereby significantly decreasing the incidence of lung injury.29,30
As the mechanisms underlying the lung-protective effects of hypercapnia have been progressively elucidated, increasing attention has been directed toward its potential protective effects on other vital organs, including the heart, lungs, liver, gastrointestinal tract, and brain. The brain, in particular, is highly susceptible to ischemia and hypoxia-induced injury, such as oxidative stress-related damage. Research finding PHC applied to congenital diaphragm in newborns Mechanical ventilation for hernia, can reduce mortality, reduce extracorporeal membrane oxygenation The utilization rate of the contract, and do not extend the length of hospital stay.31 Studies have shown that PHC has protective and anti-inflammatory effects on a variety of organs, including the lungs, heart muscle, and nervous system.32
In addition to its effects on cerebral perfusion, hypercapnia influences cardiovascular function. Acute hypercapnia directly inhibits the contractility of cardiac and vascular smooth muscle, while indirectly increasing myocardial contractility and heart rate by stimulating sympathetic nervous system activation.33 Consequently, hemodynamic responses cannot be reliably predicted based solely on hypercapnia. Regarding its role in improving oxygenation, hypercapnia, despite being a potent cerebral vasodilator, also enhances the hypoxic pulmonary vasoconstriction response, leading to a reduction in intrapulmonary shunting and subsequent improvement in oxygenation.33
In the present study, PETCO2 in Group S was maintained within the range of 45–55 mmHg at T3 through adjustments in respiratory parameters, with arterial blood gas analysis indicating PaCO2 levels between 49–59 mmHg. Changes in PETCO2 correlated with changes in PaCO2 to some extent, likely due to the exclusion of patients with severe hypoxemia. After the implementation of hypercapnia, a significant improvement in the PaO2/FiO2 ratio was observed, consistent with findings from previous studies. The increase in rSO2 may be attributed to PaCO2 elevation, which induces cerebral vasodilation, thereby enhancing cerebral blood flow and improving cerebral perfusion. Blood lactate levels can help us understand the perfusion status of the entire body’s tissues. This study mainly uses a non-invasive cerebral oxygen saturation monitor to observe cerebral oxygen metabolism. It is possible that cerebrospinal fluid lactate is a better indicator of cerebral perfusion than blood lactate. However, whether it is measuring central venous oxygen saturation by drawing blood from the internal jugular vein, calculating oxygen extraction rate, or measuring cerebrospinal fluid lactate, none of these methods are as safe, convenient, or likely to be widely adopted in clinical practice as cerebral oxygen saturation monitoring in neonatal surgeries.
Peripheral blood brain hemoglobin has a certain predictive value in neonatal hypoxic-ischemic brain injury, Hypoxic-ischemic brain injury can induce upregulation of brain hemoglobin expression in tissue cells. The results of this study show that LVPS was implement during the operation can reduce the expression of serum brain hemoglobin.
In summary, the implementation of LPVS plays a key role in maintaining perioperative ventilation and oxygenation in neonates undergoing OLV. Lung RM contributes to improved lung compliance, while PHC provides a distinct advantage in optimizing the balance between cerebral oxygen supply and demand.
Limitations and Shortcomings of This Study
This study has several limitations. First, postoperative agitation and behavioral changes were not observed or compared between the two groups, limiting the assessment of potential neurological effects. Second, the INVOS 5100B employs sensors and algorithms primarily validated in adults, potentially introducing calibration bias, and significant discrepancies can exist in absolute readings across different NIRS sensors. These technical limitations, combined with our limited sample size (n=21 per group), constrain the generalizability of the findings. Therefore, we focused on rSO2 trends rather than absolute values, integrating these with SpO2, heart rate, blood pressure, and blood gas analysis for comprehensive clinical judgment. Third, patients with severe comorbidities involving key organs were excluded, which may have introduced the possibility of false-negative results. Addressing these limitations requires further research, including multicenter studies with larger sample sizes, validation of neonate-specific NIRS protocols, investigation into calibration corrections across different commercial sensors, and the inclusion of additional observational parameters to generate more comprehensive and clinically meaningful data.
Conclusion
During neonatal OLV, a reduction in rSO2 may occur even when SpO2 remains within the normal range. Routine perioperative monitoring of rSO2 during neonatal OLV enables early detection of cerebral oxygenation changes, providing valuable guidance for perioperative neuroprotection strategies. PHC can improve rSO2 within a specific range in neonates undergoing OLV.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of the Shanxi Provincial Children’s Hospital (No.IRB-KYYN-2023-010). Written informed consent was obtained from all the patients’ parents or legal guardians.
Acknowledgments
We thank the library of Hebei General Hospital for providing literature search service.
Funding
No external funding received to conduct this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Lazar JF, Hwalek AE. A review of robotic thoracic surgery adoption and future innovations. Thorac Surg Clin. 2023;33(1):1–12. doi:10.1016/j.thorsurg.2022.07.010
2. Tang L, Kazan R, Taddei R, Zaouter C, Cyr S, Hemmerling TM. Reduced cerebral oxygen saturation during thoracic surgery predicts early postoperative cognitive dysfunction. Br J Anaesth. 2012;108(4):623–629. doi:10.1093/bja/aer501
3. Yoshitani K, Kawaguchi M, Tatsumi K, Kitaguchi K, Furuya H. A comparison of the INVOS 4100 and the NIRO 300 near-infrared spectrophotometers. Anesth Analg. 2002;94(3):586–590. doi:10.1097/00000539-200203000-00020
4. Tran NN, Tran M, Lopez J, et al. Near-infrared spectroscopy: clinical use in high-risk neonates. 2021;40;2:73–79. doi:10.1891/0730-0832/11-T-678
5. Hemmerling TM, Bluteau MC, Kazan R, Bracco D. Significant decrease of cerebral oxygen saturation during single-lung ventilation measured using absolute oximetry. Br J Anaesth. 2008;101(6):870–875. doi:10.1093/bja/aen275
6. Murkin JM, Adams SJ, Novick RJ, et al. Monitoring brain oxygen saturation during coronary bypass surgery: a randomized, prospective study. Anesth Analg. 2007;104(1):51–58. doi:10.1213/01.ane.0000246814.29362.f4
7. Slater JP, Guarino T, Stack J, et al. Cerebral oxygen desaturation predicts cognitive decline and longer hospital stay after cardiac surgery. Ann Thorac Surg. 2009;87(1):36–44. doi:10.1016/j.athoracsur.2008.08.070
8. Huang D, Zhou S, Yu Z, et al. Lung protective ventilation strategy to reduce postoperative pulmonary complications (PPCs) in patients undergoing robot-assisted laparoscopic radical cystectomy for bladder cancer: a randomized double blinded clinical trial. J Clin Anesth. 2021;71:110156. doi:10.1016/j.jclinane.2020.110156
9. Verbrugge SJ, Lachmann B, Kesecioglu J. Lung protective ventilatory strategies in acute lung injury and acute respiratory distress syndrome: from experimental findings to clinical application. Clin Physiol Funct Imaging. 2007;27(2):67–90. doi:10.1111/j.1475-097X.2007.00722.x
10. Dix LM, van Bel F, Baerts W, Lemmers PM. Comparing near-infrared spectroscopy devices and their sensors for monitoring regional cerebral oxygen saturation in the neonate. Pediatr Res. 2013;74(5):557–563. doi:10.1038/pr.2013.133
11. Alderliesten T, Dix L, Baerts W, et al. Reference values of regional cerebral oxygen saturation during the first 3 days of life in preterm neonates. Pediatr Res. 2016;79(1–1):55–64. doi:10.1038/pr.2015.186
12. Variane GFT, Dahlen A, Noh CY, et al. Cerebral oxygen saturation in neonates: a bedside comparison between neonatal and adult NIRS sensors. Pediatr Res. 2023;94(5):1810–1816. doi:10.1038/s41390-023-02705-z
13. Flechet M, Güiza F, Vlasselaers D, et al. Near-Infrared cerebral oximetry to predict outcome after pediatric cardiac surgery: a prospective observational study. Pediatr Crit Care Med. 2018;19(5):433–441. doi:10.1097/PCC.0000000000001495
14. Caicedo A, De Smet D, Vanderhaegen J, et al. Impaired cerebral autoregulation using near-infrared spectroscopy and its relation to clinical outcomes in premature infants. Adv Exp Med Biol. 2011;701:233–239. doi:10.1007/978-1-4419-7756-4_31
15. Güldner A, Kiss T, Serpa Neto A, et al. Intraoperative protective mechanical ventilation for prevention of postoperative pulmonary complications: a comprehensive review of the role of tidal volume, positive end-expiratory pressure, and lung recruitment maneuvers. Anesthesiology. 2015;123(3):692–713. doi:10.1097/ALN.0000000000000754
16. Severgnini P, Selmo G, Lanza C, et al. Protective mechanical ventilation during general anesthesia for open abdominal surgery improves postoperative pulmonary function. Anesthesiology. 2013;118(6):1307–1321. doi:10.1097/ALN.0b013e31829102de
17. Michelet P, D’Journo XB, Roch A, et al. Protective ventilation influences systemic inflammation after esophagectomy: a randomized controlled study. Anesthesiology. 2006;105(5):911–919. doi:10.1097/00000542-200611000-00011
18. Zupancich E, Paparella D, Turani F, et al. Mechanical ventilation affects inflammatory mediators in patients undergoing cardiopulmonary bypass for cardiac surgery: a randomized clinical trial. J Thorac Cardiovasc Surg. 2005;130(2):378–383. doi:10.1016/j.jtcvs.2004.11.061
19. Gajic O, Dara SI, Mendez JL, et al. Ventilator-associated lung injury in patients without acute lung injury at the onset of mechanical ventilation. Crit Care Med. 2004;32(9):1817–1824. doi:10.1097/01.ccm.0000133019.52531.30
20. Neto AS, Hemmes SN, Barbas CS, et al. Association between driving pressure and development of postoperative pulmonary complications in patients undergoing mechanical ventilation for general anaesthesia: a meta-analysis of individual patient data [published correction appears in lancet respir med. 2016;4(6):e34. doi:10.1016/S2213-2600(16)30026-1
21. Retamal J, Bugedo G, Larsson A, Bruhn A. High PEEP levels are associated with overdistension and tidal recruitment/derecruitment in ARDS patients. Acta Anaesthesiol Scand. 2015;59(9):1161–1169. doi:10.1111/aas.12563
22. Schultz MJ, Haitsma JJ, Slutsky AS, Gajic O. What tidal volumes should be used in patients without acute lung injury? Anesthesiology. 2007;106(6):1226–1231. doi:10.1097/01.anes.0000267607.25011.e8
23. Rocco PR, Pelosi P, de Abreu MG. Pros and cons of recruitment maneuvers in acute lung injury and acute respiratory distress syndrome. Expert Rev Respir Med. 2010;4(4):479–489. doi:10.1586/ers.10.43
24. Hartland BL, Newell TJ, Damico N. Alveolar recruitment maneuvers under general anesthesia: a systematic review of the literature. Respir Care. 2015;60(4):609–620. doi:10.4187/respcare.03488
25. Das A, Haque M, Chikhani M, et al. Hemodynamic effects of lung recruitment maneuvers in acute respiratory distress syndrome. BMC Pulm Med. 2017;17(1):34. doi:10.1186/s12890-017-0369-7
26. Almarakbi WA, Fawzi HM, Alhashemi JA. Effects of four intraoperative ventilatory strategies on respiratory compliance and gas exchange during laparoscopic gastric banding in obese patients. Br J Anaesth. 2009;102(6):862–868. doi:10.1093/bja/aep084
27. Aretha D, Fligou F, Kiekkas P, et al. Safety and effectiveness of alveolar recruitment maneuvers and positive end-expiratory pressure during general anesthesia for cesarean section: a prospective, randomized trial. Int J Obstet Anesth. 2017;30:30–38. doi:10.1016/j.ijoa.2016.12.004
28. Kregenow DA, Rubenfeld GD, Hudson LD, Swenson ER. Hypercapnic acidosis and mortality in acute lung injury. Crit Care Med. 2006;34(1):1–7. doi:10.1097/01.ccm.0000194533.75481.03
29. Gao W, Liu DD, Li D, Cui GX. Effect of therapeutic hypercapnia on inflammatory responses to one-lung ventilation in lobectomy patients. Anesthesiology. 2015;122(6):1235–1252. doi:10.1097/ALN.0000000000000627
30. Sinclair SE, Kregenow DA, Starr I, et al. Therapeutic hypercapnia and ventilation-perfusion matching in acute lung injury: low minute ventilation vs inspired CO2. Chest. 2006;130(1):85–92. doi:10.1378/chest.130.1.85
31. Guidry CA, Hranjec T, Rodgers BM, et al. Permissive hypercapnia in the management of congenital diaphragmatic hernia: our institutional experience. J Am Coll Surg. 2012;214(4):640–645,647.e1. doi:10.1016/j.jamcollsurg.2011.12.036
32. Curley G, Contreras MM, Nichol AD, et al. Hypercapnia and acidosis in sepsis: a double-edged sword? Anesthesiology. 2010;112(2):462–472. doi:10.1097/ALN.0b013e3181ca361f
33. Kregenow DA, Swenson ER. The lung and carbon dioxide: implications for permissive and therapeutic hypercapnia. Eur Respir J. 2002;20(1):6–11. doi:10.1183/09031936.02.00400802
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.