Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Effects of Lithium Combined with Second-Generation Antipsychotics for the Treatment of Manic Episodes in Patients with Bipolar Disorder: A Naturalistic Study in China
Authors Liu Y, Liang J, Xia Q, Zhou X, Xie X ![]()
Received 7 July 2020
Accepted for publication 8 October 2020
Published 4 November 2020 Volume 2020:16 Pages 2623—2632
DOI https://doi.org/10.2147/NDT.S270596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Yu-Ping Ning
Yang Liu,1,2,* Jun Liang,2,* Qingrong Xia,2 Xin Zhou,1 Xuefeng Xie1
1Department of Basic and Clinical Pharmacology, Anhui Institute of Innovative Drugs, School of Pharmacy, Anhui Medical University, Hefei 230032, Anhui, People’s Republic of China; 2Department of Pharmacy, Hefei Fourth People’s Hospital, Hefei 230000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuefeng Xie
Department of Basic and Clinical Pharmacology, Anhui Institute of Innovative Drugs, School of Pharmacy, Anhui Medical University, 81 Meishan Road, Hefei 230032, Anhui, People’s Republic of China
Tel/Fax +86 551 65172137
Email [email protected]
Objective: To explore the therapeutic effects of lithium combined with second-generation antipsychotics (SGAs) of quetiapine, clozapine, olanzapine, and risperidone for the treatment of manic episodes in patients with bipolar disorder (BD) to guide the selection of medications.
Methods: We examined the case data of patients with BD who experienced manic episodes and were hospitalized in a Class 3A Psychiatric Hospital in Anhui Province from January 2015 to October 2019. The enrolled patients were rated using the Bech–Rafaelsen Mania Rating Scale (BRMS) before and after treatment, and relevant adverse effects were monitored.
Results: Analysis of the collected case data of 182 patients showed significant differences in the BRMS scores on admission and at discharge of patients treated with lithium combined with each SGA. The chi-square test showed no obvious difference in the final therapeutic effects of lithium combined with each of the four SGAs (χ2 = 7.365, P = 0.146). However, there were differences in the incidence of adverse effects (χ2 = 10.604, P = 0.014) and remission rate after 2 weeks of treatment (χ2 = 10.174, P = 0.017). Logistic regression analysis revealed that the incidence of adverse effects was related to the length of stay in hospital and clozapine treatment. The remission rate after 2 weeks was associated with the length of stay in hospital, clozapine treatment, and age of onset.
Conclusion: Lithium combined with SGAs (quetiapine, clozapine, olanzapine, and risperidone) effectively improves the manic symptoms of patients with BD who experience manic episodes. Lithium combined with quetiapine for the treatment of bipolar manic episode has advantages with respect to the speed of effective and incidence of adverse effects.
Keywords: bipolar mania, atypical antipsychotic, mood stabilizers, remission rate
Introduction
Bipolar disorder (BD) is a recurrent mental illness characterized by fluctuations in mood and energy in affected patients.1 BD carries a heavy social burden and its estimated lifetime prevalence is 1–2% of the global population.2 Clinical manifestations include repeated episodes of mania and depression, which seriously impair personal life and result in unstable work performance, tense marital relationships, and increased incidence of psychosocial issues.3,4 BD has also been recognized as the primary cause of premature death due to comorbidities, such as suicide, diabetes, and cardiovascular diseases.5
Lithium is the most widely used and effective agent for the treatment of BD and has been the first-line treatment for over 70 years.6 Its mechanisms of action are complex and effects are multifaceted.7 Similar to the monovalent cation sodium (Na+), lithium under in vitro conditions replaces Na+ to produce a single action potential in a neuron.8 However, lithium carries a high risk of adverse effects due to its narrow therapeutic window. Therefore, lithium treatment alone may not be the most effective option for the treatment of manic episodes in patients with BD.9 The combined use of mood stabilizers (MSs), lithium/valproate, and antipsychotics (APs) has been the most common choice for the treatment of bipolar manic episodes.10 Considering the likelihood of adverse effects resulting from the use of first-generation APs, second-generation antipsychotics (SGAs) were gradually introduced for the treatment of BD. SGAs are antagonists at both serotonin 5-HT2 and dopamine D2 receptors, and its antipsychotic effects are thought to stem from interactions at these receptors.11 Case-controlled studies have been conducted to determine the effectiveness and safety of SGAs, such as olanzapine, risperidone, and quetiapine.12–14 Despite a relatively low implementation worldwide,15 clozapine has been listed as the second-line drug for manic episodes in the Guidelines for the Prevention and Treatment of Bipolar Disorder in China (Second Edition) and is one of the most commonly used drugs in clinical settings.16
The length of stay in hospital for patients with BD ranges from 18 to 31 days in Europe,17,18 and from 9 to 14 days in the United States.19 A study indicated that patients with bipolar manic episodes did not experience manic symptom improvements at the end of the second week of treatment in hospital and were not likely to show any further improvement in the fourth week of treatment.20 Therefore, the first 14 days after admission have the greatest impact on treatment success. Recent studies have reported that the therapeutic course of BD depends on a number of factors, including sex, psychotic symptoms, age, age of onset, and treatment regimen.2,21–25
Randomized controlled trials (RCTs) are the gold standard for evaluating treatment efficacy. However, the outcomes of RCTs sometimes lack clinical utility and do not address real-world effectiveness.26 On the other hand, naturalistic studies are pragmatic, with no active intervention, and outcomes are generally those used in clinical practice.27
This study aimed to explore the differences in efficacy of lithium combined with SGAs quetiapine, olanzapine, risperidone, and clozapine, which are widely used in China for the treatment of manic episodes in patients with BD without intervention measures, and to evaluate the incidence of the adverse effects of combined drugs so as to provide a reference for clinical and rational drug use.
Materials and Methods
Ethical Statement
This study (Project No. 20182D06) was approved by the Ethics Committee of the Fourth People’s Hospital of Hefei. The institutional review board waived the requirement for informed consent owing to the retrospective nature of the study and because we did not use any patient identifying information. We have kept patient information confidential. The treatment complies with the Helsinki Declaration, and the protection and treatment of patient data in research comply with the Helsinki Declaration.
Evaluation Scale
All patients were assessed using the Bech–Rafaelsen Mania Rating Scale (BRMS), a popular evaluation scale widely used in clinical evaluation in China. The BRMS scale comprises 11 items that are divided into 5 grades of 0–4, where 0 implies no such symptoms or a grade similar to the normal level of the patient; 1, mild; 2, moderate; 3, more serious; and 4, very serious. Each item is individually rated and a final score is calculated. Total BRMS scores of 0–5 indicate no manic symptoms; 6–10, definite manic symptoms; and >22, severe manic symptoms. Research indicates that BRMS and YMRS are quite consistent, both compared mania scales revealed satisfactory indices of reliability and validity.28,29 Bech-Rafaelsen Mania Scale has been used extensively in trials that have assessed the efficacy of treatments for bipolar disorder.30 In this study, all patients were rated using BRMS by two experienced doctors on admission. The tests were repeated 2 weeks after treatment and again at discharge.
Subjects
This study investigated the records of 1782 in-patients with BD aged 18–65 years who were admitted to Anhui Mental Health Center from January 2015 to October 2019. Psychiatric diagnosis was based on the International Classification of Diseases 10th Revision (ICD-10). In this study, two clinicians made the diagnosis of bipolar manic episodes on the basis of standard structured clinical interviews (F31.0, Bipolar affective disorder, current episode hypomanic; F31.1, Bipolar affective disorder, current episode manic without psychotic symptoms; and F31.2, Bipolar affective disorder, current episode manic with psychotic symptoms). Patients were treated with one of the four treatment regimens, with each comprising lithium combined with one of the following SGAs: olanzapine, risperidone, clozapine, and quetiapine. Treatment lasted more than 2 weeks. All patients had initial BRMS scores of 10. No other APs or MSs were administered during this period. The exclusion criteria were patients with comorbidities of major mental diseases, such as organic mental disorders or serious medical diseases, those with a history of drug abuse, those who had recently taken other psychoactive drugs, and pregnant and lactating women. The case records of the last admission were used for patients who had been admitted to the hospital several times during the study period.
Efficacy Analysis and Predictors
The case data of 182 eligible patients were included in this study for further analysis. The BRMS scores of patients receiving lithium combined with different SGAs on admission and at discharge were compared to determine whether various combined treatment regimens can effectively alleviate the symptoms of patients with BD and manic episodes. Remission of manic symptoms was defined as a reduction of ≥50% in the BRMS score compared with the baseline BRMS score at admission. Furthermore, the difference in remission rate was assessed in patients with different treatment regimens. If there was a difference in the remission rate, the factors influencing this difference were further analyzed. The factors included sex, educational background, psychotic features, age, and age of onset. The study also observed the incidence of adverse effects in patients. The common adverse effects of lithium and SGAs include consistency, increase in transient life enzymes, hyperprolactinemia, heart rate abnormalities, and EPS.
Statistical Analysis
The SPSS 23.0 statistical analysis software (SPSS, Chicago, IL) was used to analyze the data. The Kolmogorov–Smirnov test was used to test whether the data followed a normal distribution. Analysis of variance was used for data conforming to normal distribution, and the Wilcoxon signed-rank test was used for data not following normal distribution. The chi-square (χ2) test was used to compare the ranked data, and P < 0.05 indicated statistical significance. Additional post hoc pairwise comparison with significance corrected using the Bonferroni method for multiple hypothesis testing considered the results statistically significant at a level of 0.05/6 = 0.008. Univariate logistic regression analysis was performed to explore the potential factors related to the remission rates after 2 weeks and adverse effects. Statistically significant factors (P < 0.05) obtained from the first step were used for forward multivariate logistic analysis to identify the definite risk factors after adjusting for other covariates.
Results
Patient Demographics
The participant selection process is shown in Figure 1. In total, 182 eligible patients were enrolled, including 88 in the lithium + quetiapine group, 43 in the lithium + clozapine group, 31 in the lithium + olanzapine group, and 20 in the lithium + risperidone group. There were no significant differences in employment status, psychotic features, years of education, age of onset among the different treatment groups. However, there were significant differences in age (F = 3.305, P = 0.022), sex (χ2 = 8.774, P = 0.032), and marital status (χ2 = 8.420, P = 0.038) (Table 1). On the other hand, there were no significant differences in sex and marital status of patients among the four groups via post hoc pairwise comparison with the significance corrected using the Bonferroni method.
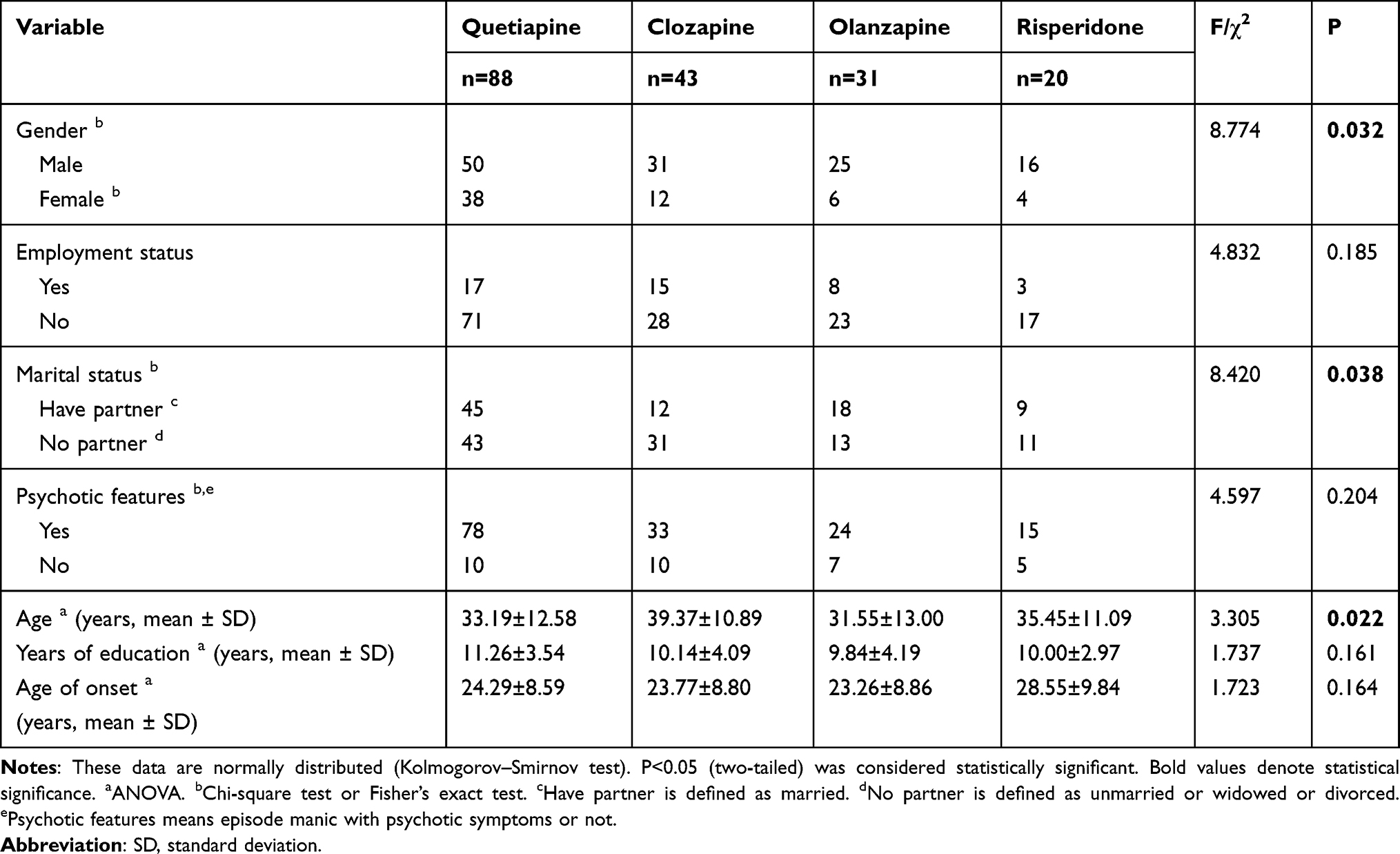 |
Table 1 Basic Socio-Demographic and Clinical Characteristics of the Study Sample |
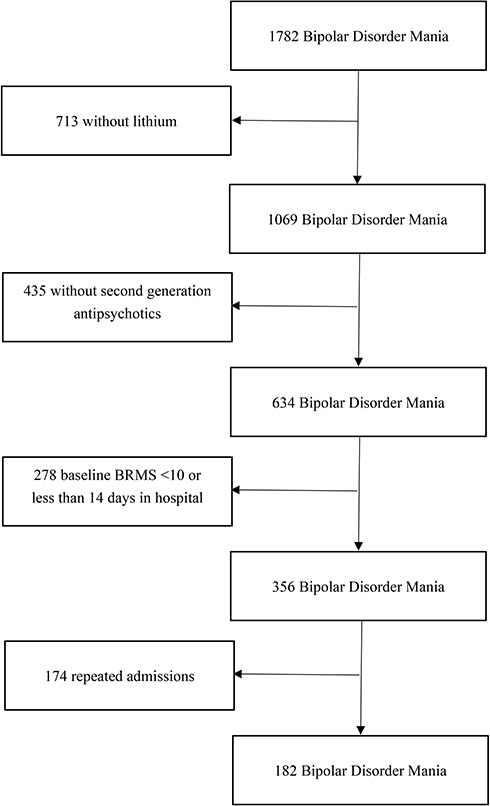 |
Figure 1 Selection of patients for analysis based on retrospective chart review. |
Comparison of Treatment Effects on Manic Symptoms
The mean daily dosages of lithium among the four groups (lithium + quetiapine, lithium + clozapine, lithium + olanzapine, lithium + risperidone) were 0.95 ± 0.20g, 0.99 ± 0.25g, 0.91 ± 0.19g, 0.92 ± 0.32g, and the mean daily dosages of SGAs were 397.46 ± 135.92mg, 133.78 ± 81.71mg, 10.54 ± 4.86mg, 3.16 ± 1.15mg, respectively. There was no significant difference in the baseline scores of BRMS at admission among the different treatment groups (H = 5.990, P = 0.112). However, statistical difference was observed among the different treatment regimens with respect to BRMS scores after 2 weeks of treatment (H = 7.718, P = 0.052). Furthermore, significant difference was observed in the remission rate after 2 weeks of treatment with different drugs (χ2 = 10.174, P = 0.017). Post hoc pairwise comparison with the significance corrected using the Bonferroni method revealed that the effective rate of the quetiapine group was significantly higher than that of the clozapine and risperidone groups after 2 weeks of treatment (P < 0.05). However, there was no significant difference in the remission rates at discharge (χ2 = 7.365, P = 0.146). Significant difference was observed in the rates of adverse effects (χ2 = 10.604, P = 0.014). Post-hoc pairwise comparison with the significance corrected using the Bonferroni method revealed that the incidence of adverse effects was significantly lower in the quetiapine group than in the clozapine and risperidone groups (Table 2).
 |
Table 2 Therapeutic Effect Among the Four Groups |
Adverse Effects of Patients with Mania
The incidence of adverse effects was the lowest in the lithium + quetiapine group and mainly comprised constipation, liver injury, and heart rate abnormalities. During the study period, no other serious adverse effects were observed, and no adverse effect-related drug withdrawal was reported in the enrolled patients (Table 3).
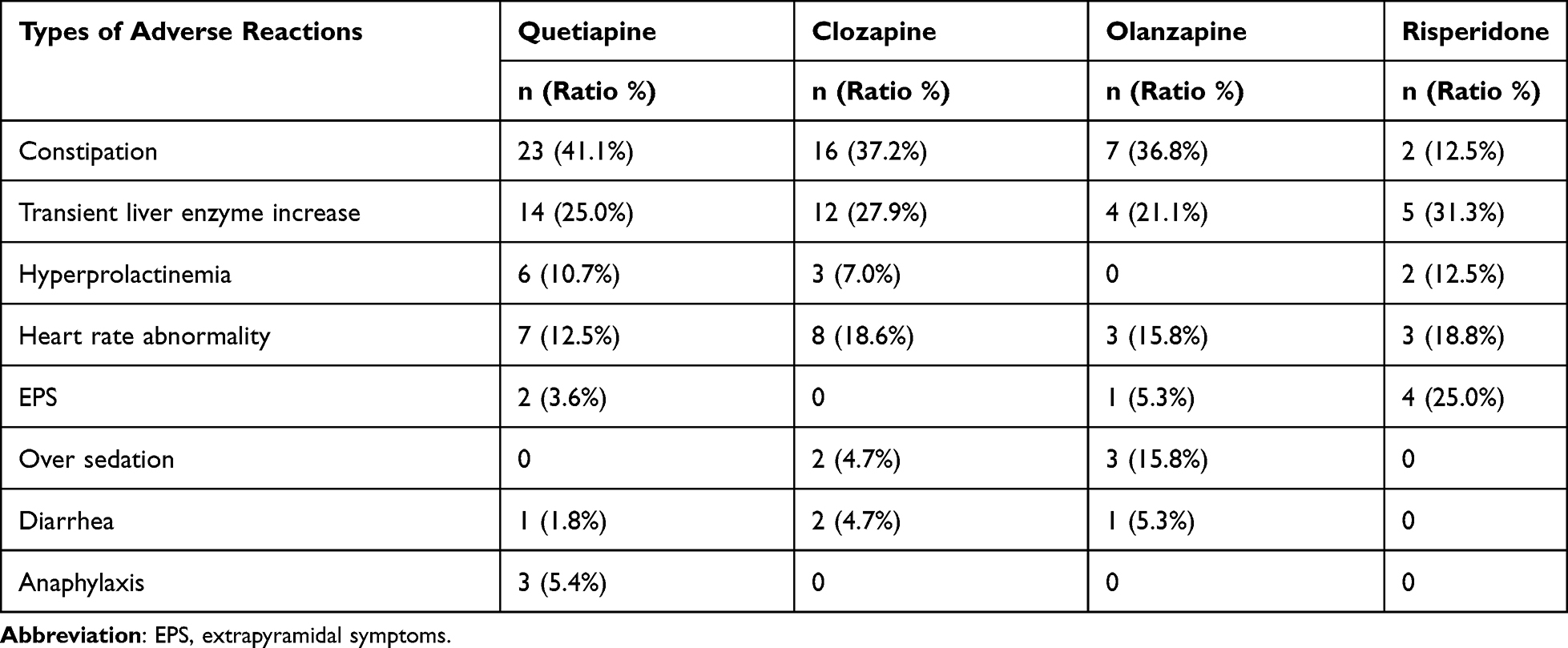 |
Table 3 Adverse Reactions Among the Four Groups |
Logistic Regression Analysis of Adverse Effects
Demographic and therapeutic factors were included in univariate logistic regression analysis, which indicated that adverse effects in patients with BD after 2 weeks of treatment were related to the treatment regimen, years of education, age of onset, and length of stay in hospital (Table 4). Furthermore, multivariate logistic regression analysis involving relevant variables revealed that the type of combined SGA and length of stay in hospital influenced adverse effects after 2 weeks of treatment.
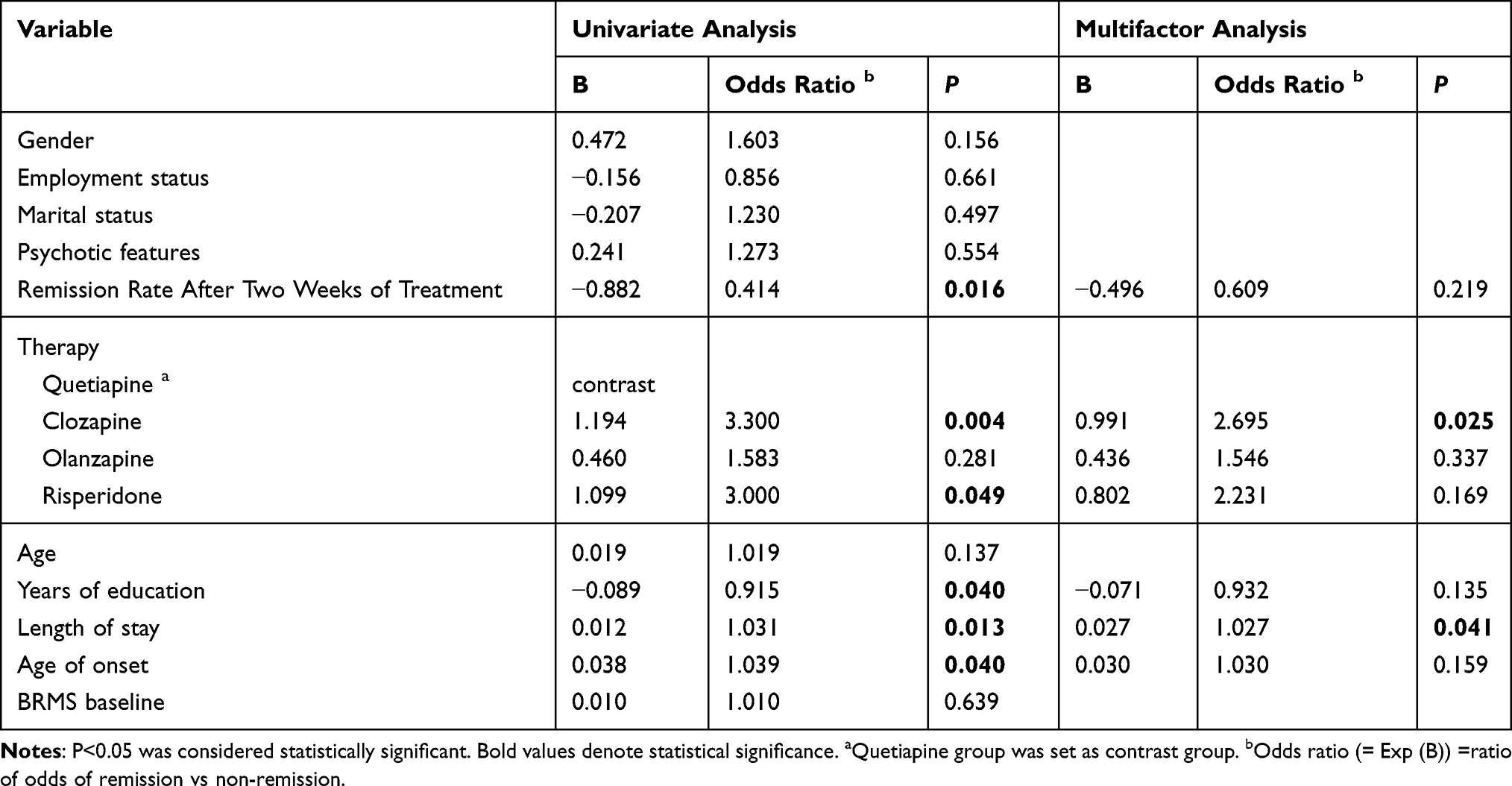 |
Table 4 Potential Predictors of Adverse Events Identified by Logistic Analysis |
Logistic Regression Analysis of the Remission Rates After 2 Weeks
Univariate logistic regression analysis including demographic and therapeutic factors indicated that the remission rates of manic episodes in patients with BD after 2 weeks of treatment were related to the treatment regimen, adverse effects, age of onset, and length of stay in hospital (Table 5). Multivariate logistic regression analysis of the relevant variables indicated that the type of combined SGA, age of onset, and length of stay in hospital influenced remission rates after 2 weeks of treatment.
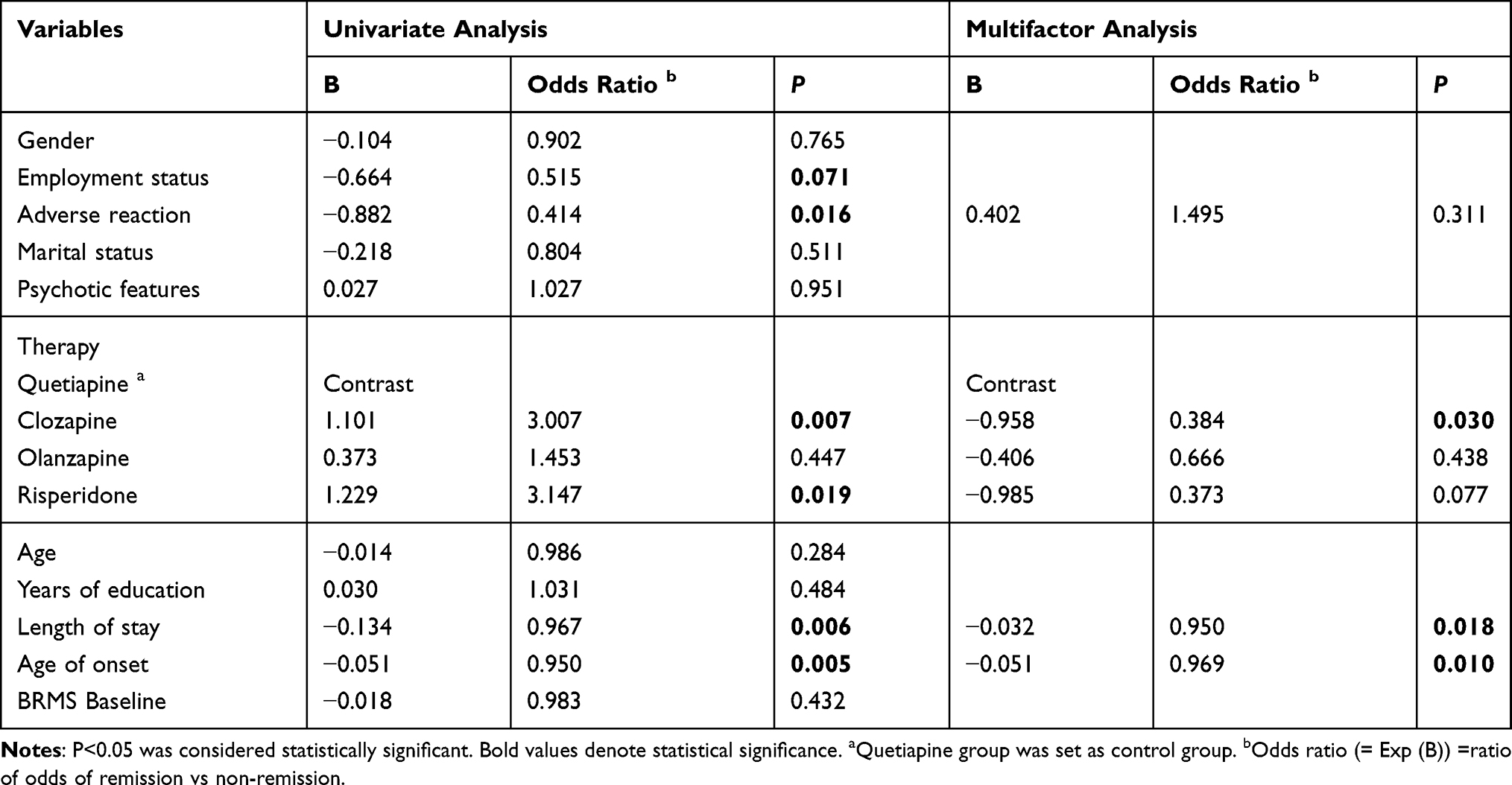 |
Table 5 Potential Predictors of Remission Rate After Two Weeks of Treatment Identified by Logistic Analysis |
Discussion
All Combinations Were Effective
At present, lithium or SGAs alone are considered effective for the treatment of manic episodes in patients with BD.31–34 In this study, we demonstrated that lithium combined with SGAs had significant therapeutic effects on manic episodes in patients with BD and could effectively alleviate manic symptoms. After treatment with the combination of lithium and one of four different SGAs (quetiapine, clozapine, olanzapine, and risperidone), the patients’ BRMS scores were significantly lower than their baseline BRMS scores on admission, and their manic symptoms were significantly improved. There was no significant difference in the remission rates of patients receiving different treatment combinations (χ2 = 7.365, P = 0.146), suggesting similar final therapeutic outcomes for the different treatment regimens. Therefore, to establish treatment guidelines, attention should be paid to the incidence of adverse effects and the speed of action of different drugs in the treatment process.
Differences in Remission Rate After Two Weeks Treatment
This study found that after 2 weeks of treatment with lithium combined with one of four SGAs, there were significant differences in the remission rates of manic symptoms among the different treatment regimens (P = 0.017). In a previous study involving 30 adolescents with manic episodes, the rate of decline in YMRS scores of the lithium + quetiapine group was significantly higher than that of the lithium + risperidone group after 2 weeks of treatment; however, there was no obvious differences between the two treatment regimens at the end of treatment.35 Clozapine treatment is widespread in China, and in a previous study involving 84 patients with mania in China who were treated with either the combination of lithium + quetiapine (n = 42) or lithium + clozapine (n = 42), the BRMS scores of the lithium + quetiapine group were significantly lower than those of lithium + clozapine group after 1 week of treatment. However, no difference was observed between the two groups after 4 weeks of treatment.36 In our study, the mean remission rate of patients treated with lithium + quetiapine was 80.7% after 2 weeks of treatment, whereas that of lithium + clozapine and lithium + risperidone was 58.1% and 55.0%, respectively. These results suggest that although lithium combined with SGAs can effectively alleviate manic symptoms in patients with acute mania, there may be a difference in the speed of their action. Similarly, further regression analysis revealed that the remission rates of patients after 2 weeks of treatment were associated with the age of onset (OR = 0.969, P = 0.010), length of stay in hospital (OR = 0.950, P = 0.018), and clozapine treatment (OR = 0.384, P = 0.030, with quetiapine as the control). At present, it is commonly accepted that patients with BD who have a younger age of onset have poor prognosis,37 because the age at the beginning of the first emotional episode determines the degree of brain structural changes and cognitive impairment. This finding suggests that it is more difficult to treat early-onset BD than late-onset BD. However, in this study, we found that patients who are young at initial onset experienced higher remission rates. SGAs have been shown to have an unsatisfactory therapeutic effect on the treatment course of manic episodes in older patients with BD,38 suggesting that lithium combined with SGAs is less effective for the treatment of patients with older age of onset. Therefore, lithium combined with SGAs should be indicated with caution for the treatment of manic episodes in patients with BD with older age of onset, and further research into its use in these patients is warranted. Meanwhile, there was a significant correlation between the length of stay in hospital and the remission rate after 2 weeks of treatment, indicating that the length of stay in hospital in in-patients with improved manic symptoms was shorter after 2 weeks of treatment. Therefore, rapid relief of manic symptoms of in-patients with BD resulted in shortened hospitalization period, improved utilization of hospital medical resources, and reduced economic burden. A higher 2-week remission rate is of great significance in improving medical efficiency and treatment rates of hospitals, particularly in countries where medical resources are relatively scarce.
Differences in the Incidence of Adverse Effects
The primary adverse effects of lithium combined with SGAs are constipation, abnormal heart rate, liver injury, increased prolactin, excessive sedation, and extrapyramidal reactions. Considering that APs may have a distinct sedative effect, only excessive (rather than mild or moderate) sedation was considered an adverse effect for the purpose of this study. Although no serious adverse effects were observed in this study, there were 110 cases with less severe adverse effects. The total incidence of adverse effects was 60.44%, among the four groups, lithium + quetiapine group has the lowest incidence of adverse effects (50.0%) while the clozapine + lithium group has the highest incidence of adverse effects (76.7%). In a study evaluating the safety and effectiveness of clozapine + lithium in 44 in-patients, the effective rate of the combined regimen was 84% and the incidence of adverse effects was 64%, comprising mainly transient and mild adverse effects.39 Olanzapine is considered the most effective SGA for the treatment of acute manic episodes.33 In this study, however, we found no significant difference between treatments with lithium + olanzapine and lithium + quetiapine in terms of efficacy and incidence of adverse effects. Current research supports the efficacy of risperidone in significantly improving manic symptoms in patients with acute mania; however, it is accompanied by a relatively higher incidence of adverse effects, particularly extrapyramidal reactions.40 In this study, the incidence of extrapyramidal reactions was as high as 25% in patients receiving lithium + risperidone treatment. Additional analysis revealed that patients exhibited good tolerance to lithium + quetiapine for the treatment of acute manic episodes, and there was no significant difference in the incidence of extrapyramidal reactions compared with placebo treatment.41 Our study found that the incidence of adverse effects of the lithium + quetiapine group was lower than that of the other three groups. Subsequent regression analysis revealed that the incidence of adverse effects was related to the treatment regimen and length of stay in hospital. Compared with quetiapine, clozapine had a higher risk of inducing adverse effects (OR = 2.695, P = 0.025). Current research generally shows that in the treatment of psychosis, quetiapine has fewer and milder adverse effects (sedation, extrapyramidal reactions, and weight gain) than clozapine.42 Therefore, clozapine is rarely used for the treatment of mental illness in Europe and America, and there are only a few studies on the treatment of acute mania by lithium + clozapine, most of which have been conducted in China. In fact, one Chinese study involving 60 patients who underwent 6 weeks of treatment found no difference in the efficacy of lithium + quetiapine versus lithium + clozapine for the treatment of manic episodes, and a higher incidence of adverse effects to clozapine.43 In this study, the incidence of adverse effects was associated with the length of stay in hospital (OR = 1.027, P = 0.041). Similarly, current research indicates that the incidence of adverse effects may prolong the length of stay of patients in hospital and may also increase treatment cost.44,45 It should be noted that while there is generally a high incidence of adverse effects during the use of psychiatric drugs, the application of treatment regimens with lower incidence of adverse effects will not only reduce the incidence of adverse effects but also treatment costs.
Treatment with Clozapine
Clozapine may cause neutropenia and even death of patients; therefore, clozapine treatment is less popular in European and American countries.46,47 As a result, only few studies have reported on the use of clozapine for the treatment of BD. In China, however, clozapine is listed as the second-line drug recommended in the Guidelines for the Prevention and Treatment of Bipolar Disorder in China (Second Edition).16 Current studies confirm that clozapine has a significant effect on the treatment of treatment-resistant BD better than other SGAs used for the treatment of treatment-resistant bipolar disorder.31 These studies confirm the status and significance of clozapine for the treatment of BD. However, in our study, we observed that clozapine combined with lithium had the lowest remission rates of manic states and higher incidence of adverse effects in the second week of treatment. It has been reported in the past that changing from clozapine to another AP may increase the risk of recurrence in patients with BD.48 Therefore, careful consideration is required when using clozapine combined with lithium despite its recommendation as the second-line drug in relevant Guidelines in China, although clozapine is effective in the treatment of treatment-resistant BD. Specifically, once it has been used for the treatment of manic episodes in patients with BD, changing clozapine to another SGA due to poor efficacy may increase the risk of recurrence of mania.
This study has some limitations that deserve attention. First, the patients enrolled in this study were from the same hospital and the sample size was relatively small. Second, because this was a retrospective study, some information might have been lost in clinical records, which may limit the presentation of results. Third, no attention was paid to the sedative effect of benzodiazepines on manic symptoms, and some patients treated with lithium combined with SGAs may have simultaneously received benzodiazepines. Fourth, BRMS scores were the only rating standards for patients in this study. BRMS is widely used in China, whereas YMRS has a wider application in the rest of the world. Notwithstanding, the reliability of BRMS has been demonstrated by the current research, and it is recommended in the Guidelines for the Prevention and Treatment of Bipolar Disorder in China (Second Edition). Fifth, this study emphasized the scores of Mania Assessment Scale without considering evaluation of the Clinical Global Impression-Bipolar Version Scale, Positive and Negative Syndrome Scale. The lack of evaluation using the “clinimetrics” method can be considered one of the limitations of this study.49,50 Furthermore, patients diagnosed as F31.6 (bipolar affective disorder, current episode mixed) in ICD-10 were not included in this study. Sixth, ideally the manic symptoms of patients should be monitored against the scale once every 2 weeks; however, considering the duration of hospitalization of most patients, and in view of the retrospective design of this study and clinical considerations of patients treatment costs, our data were obtained only from BRMS scores of tests taken on admission, 2 weeks after treatment, and at the end of the treatment. More accurate results to clarify the therapeutic outcomes of lithium combined with SGAs could be obtained if the period of evaluation is shortened, sample size is increased, and a larger variety of scales are used.
Conclusions
Our results indicate that lithium combined with SGAs (quetiapine, clozapine, olanzapine or risperidone) effectively improves the symptoms of manic episodes in patients with BD. There are differences in the speed of action and the incidence of adverse effects among different treatment regimens for acute mania. Lithium combined with quetiapine for the treatment of bipolar manic episode has advantages with respect to the speed of effective and the incidence of adverse effects.
Acknowledgments
This work was supported by Hefei Applied Medicine Research Project (No. hwk2018zc017). The authors would like to thank all participants for their involvement.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. These authors contributed equally to this article: Yang Liu and Jun Liang.
Disclosure
The authors have no conflicts of interest.
References
1. Baldessarini RJ, Tondo L, Vazquez GH, et al. Age at onset versus family history and clinical outcomes in 1665 international bipolar-I disorder patients. World Psychiatry. 2012;11(1):40–46. doi:10.1016/j.wpsyc.2012.01.006
2. Geddes JR, Miklowitz DJ. Treatment of bipolar disorder. Lancet. 2013;381(9878):1672–1682. doi:10.1016/S0140-6736(13)60857-0
3. Peters AT, Peckham AD, Stange JP, et al. Correlates of real world executive dysfunction in bipolar I disorder. J Psychiatr Res. 2014;53:87–93.
4. Depp CA, Mausbach BT, Bowie C, et al. Determinants of occupational and residential functioning in bipolar disorder. J Affect Disord. 2012;136(3):812–818. doi:10.1016/j.jad.2011.09.035
5. Chen J, Chen H, Feng J, et al. Association between hyperuricemia and metabolic syndrome in patients suffering from bipolar disorder. BMC Psychiatry. 2018;18(1):390.
6. López-Muñoz F, Shen WW, D’Ocon P, et al. A history of the pharmacological treatment of bipolar disorder. Int J Mol Sci. 2018;19(7):2143.
7. Malhi GS, Tanious M, Das P, et al. The science and practice of lithium therapy. Aust N Z J Psychiatry. 2012;46(3):192–211.
8. Oruch R, Elderbi MA, Khattab HA, et al. Lithium: a review of pharmacology, clinical uses, and toxicity. Eur J Pharmacol. 2014;740:464–473.
9. Goodwin FK. Rationale for long-term treatment of bipolar disorder and evidence for long-term lithium treatment. J Clin Psychiatry. 2002;63(Suppl 10):5–12.
10. Scherk H, Pajonk FG, Leucht S. Second-generation antipsychotic agents in the treatment of acute mania: a systematic review and meta-analysis of randomized controlled trials. Arch Gen Psychiatry. 2007;64(4):442–455. doi:10.1001/archpsyc.64.4.442
11. Harrison-Read PE. Antimanic potency of typical neuroleptic drugs and affinity for dopamine D2 and serotonin 5-HT2A receptors-a new analysis of data from the archives and implications for improved antimanic treatments. J Psychopharmacol. 2009;23(8):899–907. doi:10.1177/0269881108094349
12. Xu L, Lu Y, Yang Y, et al. Olanzapine-valproate combination versus olanzapine or valproate monotherapy in the treatment of bipolar I mania: a randomized controlled study in a Chinese population group. Neuropsychiatr Dis Treat. 2015;11:1265–1271.
13. Rendell JM, Gijsman HJ, Bauer MS, et al. Risperidone alone or in combination for acute mania. Cochrane Database Syst Rev. 2006;1(1):CD004043.
14. Suttajit S, Srisurapanont M, Maneeton N, Maneeton B. Quetiapine for acute bipolar depression: a systematic review and meta-analysis. Drug Des Devel Ther. 2014;8:827–838. doi:10.2147/DDDT.S63779
15. Wilkowska A, Cubała WJ. Clozapine as transformative treatment in bipolar patients. Neuropsychiatr Dis Treat. 2019;15:2901–2905. doi:10.2147/NDT.S227196
16. Wang ZW, Ma YT, Chen J, et al. The Chinese guidelines for the prevention and treatment of bipolar disorders: evidence-based choices. Chin J Psychiatry. 2017;50(2):96–100.
17. Osby U, Tiainen A, Backlund L, et al. Psychiatric admissions and hospitalization costs in bipolar disorder in Sweden. J Affect Disord. 2009;115(3):315–322.
18. Gonzalez-Pinto AM, Dardennes R, de Zélicourt M, et al. In-patient care costs of patients with bipolar I disorder: a comparison between two European centers. J Affect Disord. 2010;121(1–2):152–155.
19. Begley CE, Annegers JF, Swann AC, et al. The lifetime cost of bipolar disorder in the US: an estimate for new cases in 1998. Pharmacoeconomics. 2001;19(5 Pt 1):483–495. doi:10.2165/00019053-200119050-00004
20. Li DJ, Lin CH, Lu MJ. Early improvement predicts treatment outcomes for patients with acute mania: a naturalistic study in Taiwan. J Clin Psychopharmacol. 2017;37(4):435–440.
21. Bauer M, Pfennig A. Epidemiology of bipolar disorders. Epilepsia. 2005;46(Suppl 4):8–13.
22. Duffy A, Malhi GS, Grof P. Do the trajectories of bipolar disorder and schizophrenia follow a universal staging model? Can J Psychiatry. 2017;62(2):115–122.
23. Li DJ, Lin CH, Chen FC. Factors affecting time to remission for inpatients with bipolar mania - a naturalistic Taiwanese study. J Affect Disord. 2018;232:73–78.
24. Lichtenstein P, Yip BH, Björk C, et al. Common genetic determinants of schizophrenia and bipolar disorder in Swedish families: a population-based study. Lancet. 2009;373(9659):234–239. doi:10.1016/S0140-6736(09)60072-6
25. Kora K, Saylan M, Akkaya C, et al. Predictive factors for time to remission and recurrence in patients treated for acute mania: health outcomes of manic episodes (HOME) study. Prim Care Companion J Clin Psychiatry. 2008;10(2):114–119.
26. Fagiolini A, Rocca P, De Giorgi S, et al. Clinical trial methodology to assess the efficacy/effectiveness of long-acting antipsychotics: randomized controlled trials vs naturalistic studies. Psychiatry Res. 2017;247:257–264. doi:10.1016/j.psychres.2016.11.044
27. Leichsenring F. Randomized controlled versus naturalistic studies: a new research agenda. Bull Menninger Clin. 2004;68(2):137–151. doi:10.1521/bumc.68.2.137.35952
28. Shansis FM, Reche M, Capp E. Evaluating response to mood stabilizers in patients with mixed depression: a study of agreement between three different mania rating scales and a depression rating scale. J Affect Disord. 2016;197:1–7. doi:10.1016/j.jad.2016.02.064
29. Wciórka J, Schaeffer E, Switaj P, et al. Bech-Rafaelsen Mania Scale and Young Mania Rating Scale–comparison of psychometric properties of the two instruments for rating a manic syndrome. Psychiatr Pol. 2011;45(1):61–78.
30. Bech P. The Bech-rafaelsen Mania Scale in clinical trials of therapies for bipolar disorder: a 20-year review of its use as an outcome measure. CNS Drugs. 2002;16(1):47–63. doi:10.2165/00023210-200216010-00004
31. Delgado A, Velosa J, Zhang J, et al. Clozapine in bipolar disorder: a systematic review and meta-analysis. J Psychiatr Res. 2020;125:21–27. doi:10.1016/j.jpsychires.2020.02.026
32. Perlis RH, Welge JA, Vornik LA, et al. Atypical antipsychotics in the treatment of mania: a meta-analysis of randomized, placebo-controlled trials. J Clin Psychiatry. 2006;67(4):509–516. doi:10.4088/JCP.v67n0401
33. Cipriani A, Barbui C, Salanti G, et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis. Lancet. 2011;378(9799):1306–1315.
34. Tarr GP, Glue P, Herbison P. Comparative efficacy and acceptability of mood stabilizer and second generation antipsychotic monotherapy for acute mania–a systematic review and meta-analysis. J Affect Disord. 2011;134(1–3):14–19.
35. Habibi N, Dodangi N, Nazeri A. Comparison of the effect of lithium plus quetiapine with lithium plus risperidone in children and adolescents with bipolar I disorder: a randomized clinical trial. Med J Islam Repub Iran. 2017;31:16.
36. Yue HW, Fang M, Ma LM. Clinical efficacy of quetiapine and clozapine combined with lithium carbonate in the treatment of mania. J Med Forum. 2016;37(6):150–151.
37. Zhang L, Yang HC, Xu XF, et al. Demographic and clinical differences between early- and late-onset bipolar disorders in a multicenter study in China. Psychiatry Res. 2016;246:688–691. doi:10.1016/j.psychres.2016.10.063
38. Oostervink F, Nolen WA, Kok RM. Two years’ outcome of acute mania in bipolar disorder: different effects of age and age of onset. Int J Geriatr Psychiatry. 2015;30(2):201–209.
39. Bender S, Linka T, Wolstein J, et al. Safety and efficacy of combined clozapine-lithium pharmacotherapy. Int J Neuropsychopharmacol. 2004;7(1):59–63. doi:10.1017/S1461145703003870
40. Komossa K, Rummel-Kluge C, Schwarz S, et al. Risperidone versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst Rev. 2011;1(1):CD006626.
41. Adler CM, Fleck DE, Brecher M, Strakowski SM. Safety and tolerability of quetiapine in the treatment of acute mania in bipolar disorder. J Affect Disord. 2007;100(Suppl 1):S15–22.
42. Asmal L, Flegar SJ, Wang J, et al. Quetiapine versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst Rev. 2013;11(11):CD006625.
43. Ying YF, Xu SQ, Liu XX, et al. Clinical controlled study on quetiapine and clozapine combined with lithium in patients with mania. Chin Pharm J. 2007;42:877–878.
44. Qing-ping S, Xiao-dong J, Feng D, et al. Consequences, measurement, and evaluation of the costs associated with adverse drug reactions among hospitalized patients in China. BMC Health Serv Res. 2014;14:73.
45. Liao PJ, Mao CT, Chen TL, et al. Factors associated with adverse drug reaction occurrence and prognosis, and their economic impacts in older inpatients in Taiwan: a nested case-control study. BMJ Open. 2019;9(5):e026771.
46. Li XB, Tang YL, Wang CY, de Leon J. Clozapine for treatment-resistant bipolar disorder: a systematic review. Bipolar Disord. 2015;17(3):235–247.
47. Goodwin GM, Haddad PM, Ferrier IN, et al. Evidence-based guidelines for treating bipolar disorder: revised third edition recommendations from the British association for psychopharmacology. J Psychopharmacol. 2016;30(6):495–553.
48. Ifteni P, Teodorescu A, Moga MA, et al. Switching bipolar disorder patients treated with clozapine to another antipsychotic medication: a mirror image study. Neuropsychiatr Dis Treat. 2017;13:201–204. doi:10.2147/NDT.S122367
49. Fleck MP, Carrozzino D, Fava GA. The challenge of measurement in psychiatry: the lifetime accomplishments of Per Bech (1942–2018). Braz J Psychiatry. 2019;41(5):369–372.
50. Fava GA, Carrozzino D, Lindberg L, et al. The clinimetric approach to psychological assessment: a tribute to Per Bech, MD (1942–2018). Psychother Psychosom. 2018;87(6):321–326.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.