Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Effects of Individualized Step Targets on Physical Activity in COPD. A Randomized Study
Authors Minakata Y ![]() , Sasaki S, Murakami Y
, Sasaki S, Murakami Y ![]() , Kawabe K, Ono H, Takahashi K
, Kawabe K, Ono H, Takahashi K ![]() , Asai K
, Asai K ![]() , Nakanishi M, Hirano T
, Nakanishi M, Hirano T ![]() , Matsunaga K
, Matsunaga K ![]()
Received 3 July 2025
Accepted for publication 11 December 2025
Published 25 December 2025 Volume 2025:20 Pages 4103—4114
DOI https://doi.org/10.2147/COPD.S550846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vanesa Bellou
Yoshiaki Minakata,1 Seigo Sasaki,1 Yusuke Murakami,1 Kazumi Kawabe,1 Hideya Ono,1 Koichiro Takahashi,2 Kazuhisa Asai,3 Masanori Nakanishi,4 Tsunahiko Hirano,5 Kazuto Matsunaga5
1Department of Respiratory Medicine, NHO Wakayama Hospital, Hidaka-gun, Wakayama, Japan; 2Division of Hematology, Respiratory Medicine and Oncology, Department of Internal Medicine, Faculty of Medicine, Saga University, Saga, Japan; 3Department of Respiratory Medicine, Graduate School of Medicine, Osaka Metropolitan University, Osaka, Japan; 4Third Department of Internal Medicine, Wakayama Medical University, Wakayama, Japan; 5Department of Respiratory Medicine and Infectious Disease, Graduate School of Medicine, Yamaguchi University, Ube, Yamaguchi, Japan
Correspondence: Yoshiaki Minakata, Department of Respiratory Medicine, NHO Wakayama Hospital, 1138 Wada, Mihama-cho, Hidaka-gun, Wakayama, 644-0044, Japan, Tel +81 738 22 3256, Fax +81 738 22 2126, Email [email protected]
Purpose: Improving physical activity (PA) is important in patients with chronic obstructive pulmonary disease (COPD). Goal setting can be a possible intervention to improve PA, but the increase in PA is not sustainable in the long term. We evaluated the effects of providing an individualized target step count, reflecting the disease condition of each patient, on PA and other factors, such as myokines, after six months in patients with COPD.
Patients and Methods: We performed a randomized parallel group, open-label study (INTAR-Step study) between the target provision (intervention) group and the usual care (control) group and investigated differences in the proportion of subjects who achieved the target as a primary outcome and differences in changes in PA parameters and myokines as secondary outcomes. This study was registered with UMIN-CTR (UMIN000046390, January 13, 2022).
Results: A total of 73 subjects were analyzed (intervention, n=38; control, n=35). The proportion of participants in the intervention group who achieved their target step count did not show a significant increase relative to the control group (p=0.157). However, the change in step count, and change in duration of activity at ≥ 3.0 metabolic equivalents were significantly increased in the intervention group. The Changes in the Growth differentiation factor-15 (GDF-15), fatty acid-binding protein-3, and Irisin levels also increased in the intervention group. Furthermore, GDF-15 levels were significantly higher in subjects with increased step counts than in those with decreased step counts.
Conclusion: Providing individualized step targets did not increase the proportion of subjects who achieved their targets, but it increased their step counts after six months. GDF-15 may be involved in the increase in the step count.
Plain Language Summary: Improving physical activity is important but achieving it is not easy. Providing patients with COPD with individualized target values of step count increased their step counts after six months. Growth differentiation factor-15 may be involved in the increase in the step count.
Keywords: accelerometer, behavior modification, goal setting, myokine, GDF-15
Introduction
Physical activity (PA) is decreased in patients with chronic obstructive pulmonary disease (COPD)1,2 and is an important factor in all-cause mortality.3–5 Therefore, increasing PA is recommended.6 The PA improvement rate tended to be higher in cases in which counseling and feedback were implemented in COPD.7 Exercise training did not improve PA, whereas it was significantly improved by behavioral modification interventions, with an effect size twice that of bronchodilator therapy.8
Providing pedometer and step count feedback could promote PA and could therefore be an effective intervention, but the effects lasted only four months.9 Several studies have attempted to provide target step count values for patients with COPD, in which the target value was set based on the current step count and adjusted weekly.10–12 They showed a significant increase in step count at three or four months, but not at six months.13 Furthermore, most participants felt that it was difficult to achieve their targets.14 The possible problems with these protocols are that the target values are decided based only on the current step count but not on disease conditions; even if patients do their best to reach their goals, they are expected to achieve even higher goals the following week, making it difficult for patients to maintain motivation for long periods of time. It is desirable that the target value reflects the disease condition and is fixed for a certain period so that the patient can feel a sense of goal achievement.
We previously established a reference equation for step count using PA-associated factors in patients with COPD.15 Furthermore, we developed a method to set a relatively easily attainable target step count value that reflects the calculated predicted value and current step count value.16 In a pilot study, we observed a significant increase in the percentage of subjects who achieved their target values (p=0.034) and a tendency to increase step count (p=0.06) after two months.16 However, its long-term effects have not been confirmed.
Myokine is a humoral factor (a cytokines) which is produced, expressed and released by contraction of muscle fibers and exerts autocrine, paracrine or endocrine effects.17,18 Exercise-induced myokines have anti-inflammatory effects and may alleviate disease pathology.19,20 A possible association between PA and myokines in COPD has been reported.21,22 Although it is not yet clear how myokines engage in PA, they may play some role in maintaining PA. Furthermore, the types of myokine changes associated with an increase in the step count in COPD remain unclear.
In this study, we performed a 6-month randomized parallel group, open-label study between a target step count provision group and the usual care group and investigated differences in the proportion of subjects who achieved target step counts and differences in changes in PA parameters and myokines between the two groups. Regarding the myokines that showed differences in change between the groups, we further investigated whether the degree of changes in myokines differed between subjects whose step counts increased and those whose step counts decreased.
Materials and Methods
Participants
Subjects aged > 40 years with stable COPD were recruited for this study. COPD was defined as a post-bronchodilator forced expiratory volume in one second (FEV1) / forced vital capacity (FVC) <0.7 based on the ATS/ERS recommendation method,23,24 and exclusion of other diseases. The exclusion criteria were as follows: 1) patients who required oxygenation during the daytime, 2) patients with clinically obvious bronchial asthma symptoms, 3) patients with an exacerbation within three months, 4) patients judged by a physician to have a significant reduction in PA due to a disease other than COPD, and 5) patients judged to be unsuitable for registration by the physician. Subjects were recruited from outpatients by physicians at five institutes, namely Osaka Metropolitan University, Saga University, Yamaguchi University, Wakayama Medical University, and NHO Wakayama Hospital, from June 2022 to January 2023. Written informed consent was obtained from all participants. This study was complied with the Declaration of Helsinki, approved by the ethics committee of NHO Wakayama Hospital (approval number: 03–06; approval date: October 26, 2021), and registered with UMIN-CTR (UMIN000046390, January 13, 2022).
Protocol
Participants were required 4 visits; visit 1, visit 2 (between four and twenty weeks after visit 1; week 0), visit 3 (twelve weeks after visit 2; week 12, permitted at weeks 8–19), and visit 4 (twenty-four weeks after visit 2; week 24, permitted at weeks 20–40). At visit 1, after obtaining informed consent, participants were required to measure subject demographics, post-bronchodilator spirometry, patient-reported outcome measures (PROs), serum myokines, body composition, chest computed tomography (CT), transdermal advanced glycation end-products (AGEs), and PA using an accelerometer with a recording of a diary for 2 weeks. At visit 2, participants were randomly assigned to either the intervention or control group and were encouraged to increase their step counts. At visit 3, participants were encouraged by their doctors to increase their step counts. At visit 4, participants were required to measure their demographics, PROs, body composition, serum myokines, transdermal AGEs and their PA using an accelerometer while recording a diary for 2 weeks. Subjects in the intervention group were educated and encouraged to increase their step counts and were provided with the target step count value and a pedometer. They were instructed to wear a pedometer (HJ-325; Omron Healthcare, Kyoto, Japan) on their waist from the time they woke up until the time they went to bed throughout the study period. Whereas subjects in the control group were educated and encouraged to increase their step counts (Figure 1). Encouragement to increase their step count was given individually to participants using written (Figure S1) and verbal instructions by the attending physician at visit 2 and visit 3.
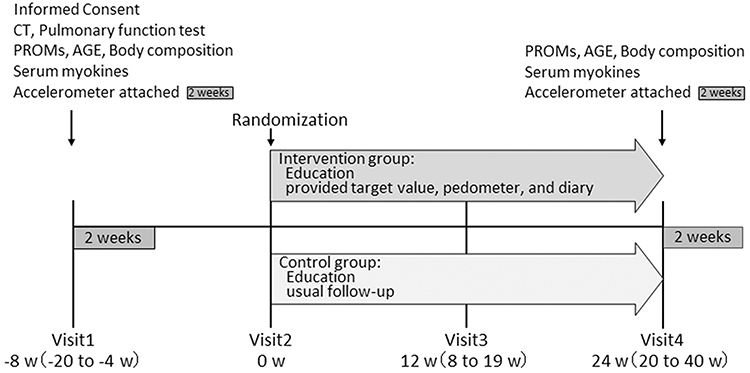 |
Figure 1 Protocol. |
Randomization
After confirming that participants meet the eligibility criteria and obtaining their consent, the attending physicians at each facility contacted the Wakayama Hospital Research Office to enroll participants. The Wakayama Hospital Office staff provided the participant identification number and randomized participants using the UMIN Internet Data and Information System for Clinical and Epidemiological Research, Cloud version (https://www.umin.ac.jp/indice/cloud.html). The UMIN Internet system generated the randomization sequence independently of the recruitment staff and stratified by the baseline step count and FEV1%pred. The allocation ratio between the intervention and control groups was 1:1. The allocation results were confirmed by the NHO Wakayama Hospital research office via the UMIN internet system and transmitted to each facility research office. The attending physicians at each facility then assigned participants to either the intervention or control group and informed the participants of their assignment at visit 2.
Outcomes
The primary outcome was the proportion of subjects achieving their target step count values after six months in the intervention group compared with the control group. The secondary outcomes were the following items in the intervention group compared with the control group: 1) the percentage of the actual step count value to the target value after six months, which was calculated as 100 × [step count at six months] / [target value]; 2) the change in step count values over six months; 3) the changes in other PA parameters including the duration of PA at ≥3.0 metabolic equivalents (METs), the duration of PA at ≥2.0 METs, the total activity calculated as the sum of METs values (at ≥3.0 METs) multiplied by hour, and the duration of PA at 1.0–1.5 METs after six months; and 4) the changes in parameters other than PA, including PROs, serum myokines, and body composition between baseline and six months. Furthermore, changes in other parameters that increased in the intervention group were compared between subjects whose step counts increased and those whose step counts decreased. Per-protocol analyses were performed to evaluate the changes in parameters between baseline and six months.
Accelerometer Measurement
Participants were required to wear a triaxial accelerometer (Active Style Pro HJA-750C; HJA: Omron Healthcare, Kyoto, Japan) on their waist from the time they woke up until the time they went to bed for two weeks at visit 1 and visit 4 (See Supplementary Information for details).
Setting Target Step Count Value
The target step count value was set based on our previous report.16 In brief, the target value was determined using both predicted and current step count values. The predicted value was calculated using the following reference equation: predicted step count value = (−0.079 × [age] −1.595 × [mMRC] +2.078 × [IC] + 18.149)3, where mMRC is the modified Medical Research Council dyspnea scale and, and IC is inspiratory capacity (L).15 This equation has been validated in the previous report.15 Ten ranges were established for each subject, ranging from 0.2 times the predicted value to 2 times the predicted value. Subsequently, the minimum number of steps above the applicable range containing the current measured value, was used as the target value (Figure S2).16 For example, when the predicted value was 4000 and the measured value was 2200, twice the predicted value became 8000, and the range was set at every 800 steps. The measured value is between 1600 and 2399; therefore, the target value is set as 2400 (minimum number above the applicable range). Target values were communicated to participants by the attending physician, both in writing and verbally.
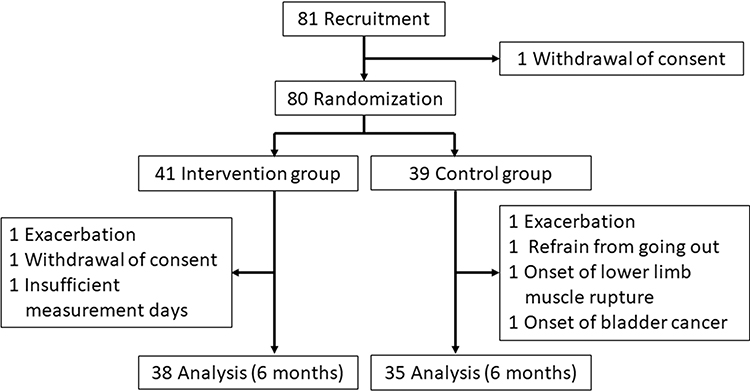 |
Figure 2 Flow diagram. |
PROs
The mMRC, COPD assessment test (CAT), PROs for dyspnea (PROMS-D),25 Kihon Checklist (KCL),26,27 and Japanese version of the Montreal Cognitive Assessment (MoCA-J)28 were employed.
Myokines
Fourteen myokines, including Apelin, Brain-derived neurotrophic factor (BDNF), erythropoietin (EPO), fatty acid-binding protein-3 (FABP-3), fibroblast growth factor-21 (FGF-21), Fractalkine/CX3CL1, Follistatin-like Protein 1 (FSTL-1), IL-6, IL-15, Leukemia Inhibitory Factor (LIF), myostatin/growth differentiation factor-8 (GDF-8), Oncostatin M, Osteocrin/Musclin, Osteonectin/Secreted protein acidic and rich in cysteine (SPARC), were measured using a Milliplex® human myokine magnetic bead panel, HMYOMAG-56K (Merck Inc., Darmstadt, Germany). Growth differentiation factor-15 (GDF-15) and the Irisin levels were measured using the GDF15 Human ELISA Kit Quantikine® (R&D Systems Inc., MN, USA) and the Irisin Canine/Human/Mouse/Rat EIA kit® (Phoenix Pharmaceuticals Inc., CA, USA), respectively.
Body Composition and AGEs Measurement
The skeletal muscle index (SMI) and phase angle (PhA) were determined by bioelectrical impedance analysis (BIA) using a body composition analyzer (InBody S10®, InBody Japan Inc., Tokyo, Japan). Measurements were performed in the morning, at least 2 hours after a meal, and in a seated position after resting for at least 5 minutes. SMI was calculated as the sum of the limb muscle mass (kg) divided by the square of height (m). The AGEs were transcutaneously measured using an AGE scanner AGE200® (Diagnoptics Technologies BV, Netherlands).
Sample Size Calculation
In our previous pilot study, the proportions of subjects who achieved their target values in the target step count provision and usual care groups were 68.8% and 31.8%, respectively.16 Assuming a 2-sided α- value of 0.05, and β-value of 0.20, the required number of participants in each group was 35; assuming a 10% dropout rate, the required number of participants in each group was 39.
Statistical Analysis
The normality of distribution was assessed using the D’Agostino & Pearson test, and the differences in characteristics between the intervention and control groups were assessed using the Mann–Whitney U-test, unpaired t-test, or Fisher’s exact test. The percentage of subjects who reached the target was compared between groups using Fisher’s exact test. Changes in the step count between baseline and six months were compared using the Wilcoxon signed-rank test. Changes in PA parameters and other parameters were compared between the groups using the Mann–Whitney U-test because most parameters showed non-normal distributions. Differences between groups were calculated using the Hodges-Lehmann estimator. Changes in myokines were compared between the increased and decreased step count groups using the Mann–Whitney U-test. All statistical analyses were performed using GraphPad Prism 9 software (GraphPad Software, San Diego, CA, USA). Statistical significance was set at P<0.05.
Results
Of the 81 subjects recruited, 80 were randomized, and 41 subjects were allocated to the intervention group and 39 to the control group (Figure 2). The study population included 76 male (95.0%) with a mean age of 74.3 years. The FEV1%pred, mMRC, CAT, and step count were 66.6±19.9%, 1.1±1.1, 9.4±6.3, and 4195±2578 steps, respectively (Table 1). There were no differences in any of the parameters between the intervention and control groups. The detailed comorbidities are shown in Table S1. Out of the 14 days of accelerometer measurements, the number of valid days in the intervention and control groups at baseline were 9.9±2.5 and 9.3±2.6 days, respectively, and those after six months were 10.4±3.0 and 10.5±2.5 days. Although the target values for the control group were not disclosed to the participants, the target step count values for the intervention and the control groups were 4134.9±2122.2 and 4680.8±2840.9, respectively.
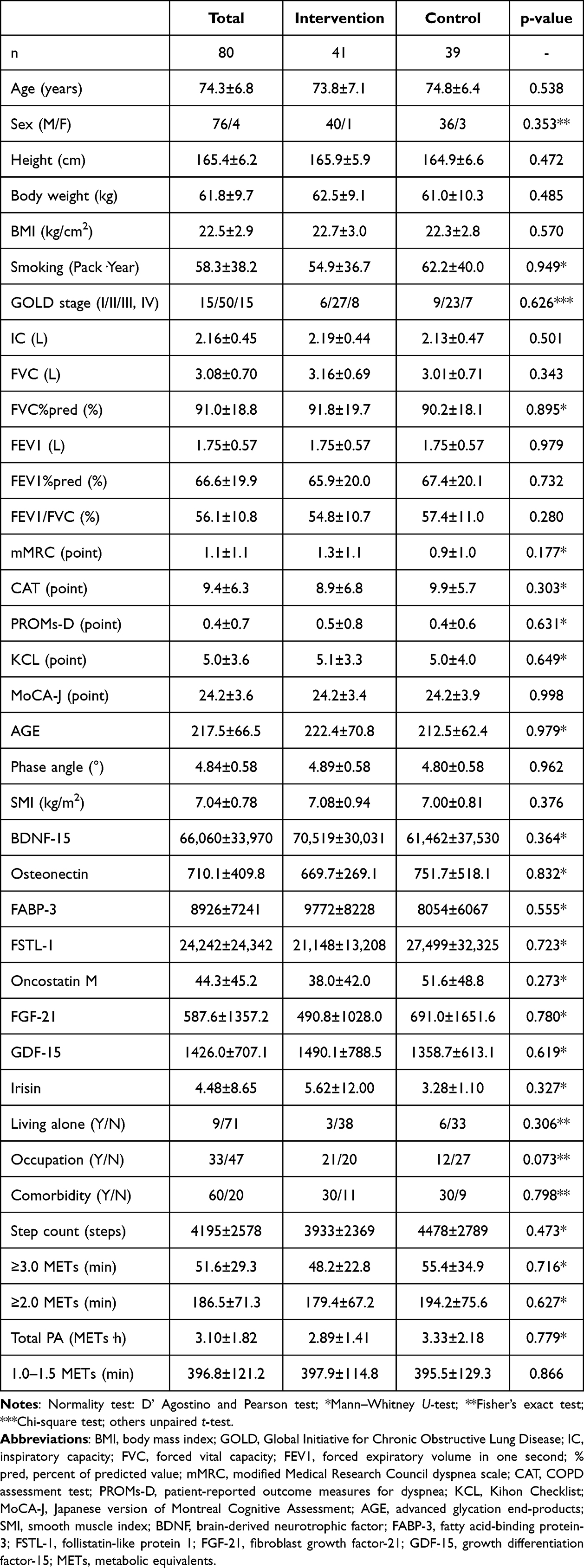 |
Table 1 Patient Characteristics |
Primary Outcome
The number of subjects who reached the target after six months was 20 of 38 (52.6%) in the intervention group and 12 of 35 (34.3%) in the control group, and the chi-square test showed that the difference between the 2 groups was not statistically significant (p=0.157; relative risk, 1.535; 95% CI, 0.904–2.706) (Table 2 and Figure S3).
 |
Table 2 Percentage of Subjects Who Reached Their Target Step Count |
Secondary Outcomes
The percentage of actual steps to the target value for each subject after six months was significantly higher in the intervention group than in the control group (p=0.014) (Table 3 and Figure S3). The step count taken in the intervention group increased significantly after six months compared with baseline (p=0.041), but no increase was observed in the control group (p=0.334) (Figure 3). The change in step count taken in the intervention group was significantly greater than that in the control group (p=0.039), and the median difference between the two groups was 639.7 (95% CI: 21.1 to 1060) steps (Table 3 and Figure S4). Among the other PA parameters, the change in duration of activity at ≥3.0 METs was significantly greater in the intervention group than in the control group (p=0.049), but the changes in other parameters were not (Table 3).
 |
Table 3 Changes in the Parameters of Physical Activity |
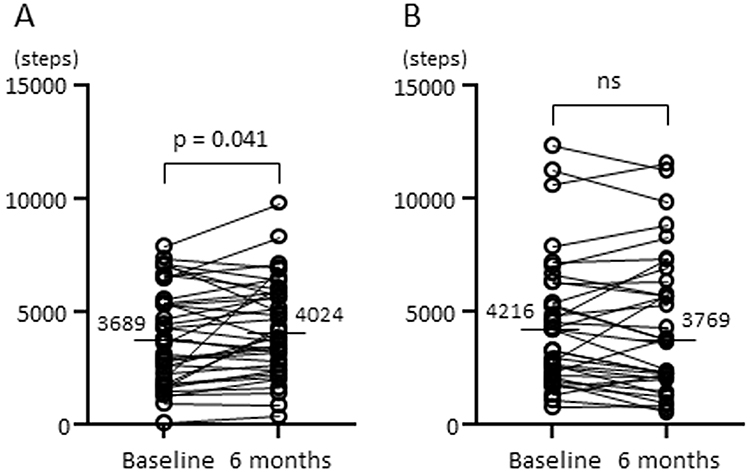 |
Figure 3 The step counts taken before and after the intervention. (A) Intervention group, (B) Control group. The horizontal lines and numbers indicate the median values. |
The changes in mMRC, CAT, PROMS-D, AGE, phase angle, and SMI did not differ markedly between the two study groups (Table 4). Among the 14 myokines measured with a myokine panel, only 6 myokines (BDNF-15, Osteonectin, FABP-3, FSTL-1, Oncostatin M, and FGF-21) were detected. The number of subjects in whom myokines were detected at both baseline and after six months by the myokines panel was 20, 19, 20, 13, 17, and 18, respectively. GDF-15 and Irisin, as measured by ELISA kits, were clearly detected in all subjects. The changes in the FABP-3, GDF-15, and Irisin levels after six months were significantly greater in the intervention group than in the control group (p=0.013, p=0.029, and p=0.028, respectively) (Table 4). Adverse events are shown in Table S2; none were related to the intervention.
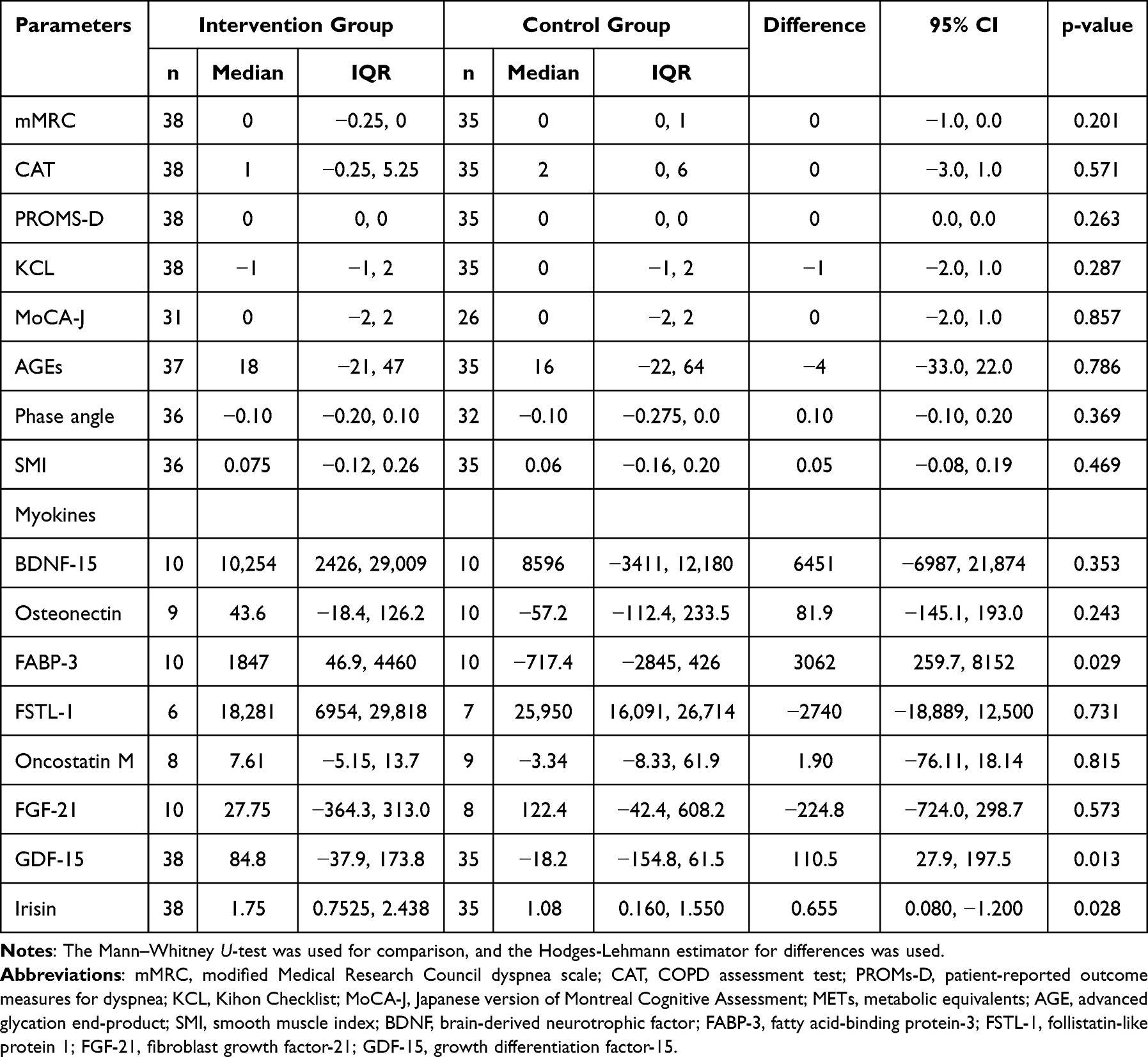 |
Table 4 Changes in Other Parameters |
When comparing the degree of change in these three myokines with increases or decreases in step count, the change in GDF-15 in subjects with an increase in step count (n=39) was significantly greater than that in subjects with a decrease in step count (n=34) (p=0.019). Changes in the other two myokines did not differ between the subjects with increased and decreased step counts. The baseline step count and GDF-15 levels did not differ between the subjects with increased and decreased step counts (Table S3).
Discussion
Providing the step count target value did not increase the proportion of subjects who achieved their target values, which was the primary outcome. However, it significantly increased the percentage of the actual step count value to the target value, the change in the step count, and the change in duration of PA at ≥3.0 METs after six months in comparison to the usual care. It also increased the changes in the FABP-3, GDF-15, and Irisin levels, among measurable myokines. Furthermore, the degree of change in GDF-15 level was significantly higher in subjects with increased step counts than in those with decreased step counts.
While setting the target value in the intervention group tended to increase the proportion of subjects who achieved their targets, the difference between the two groups was not statistically significant. However, the percentage of the actual step count to the target after six months was significantly greater in the intervention group than in the control group. The percentage of the actual step count to the target value means how close each subject is to achieving their goal. Therefore, current results showed that although this intervention did not significantly increase the number of subjects who achieved their goals, it did bring them closer to their respective goals. Half of the participants who were provided with target values reached their goals, which in turn meant that half of the participants needed additional approaches. Therefore, development of additional approaches that can induce motivation and behavior modification is required in the future.
Although it was a secondary outcome, the change in step count over six months in the intervention group was significantly greater than that in the control group. Furthermore, the median difference in the step count between the groups was 639.7, thereby exceeding the minimal clinically important difference.29 In previous reports in which the target value of the step count was provided to patients with COPD, the step count increased after three or four months10–12 but not at six months.13 The possible reasons for the positive results in the current study are as follows: 1) the target value was defined based on not only the current step count but also the predicted step count, which reflects individual disease conditions;15,16 and 2) the target value was fixed for six months; thus, by achieving their targets, participants may have felt a sense of accomplishment that maintained their motivation.
In addition to the step count, the change in the duration of PA at ≥3.0 METs was higher in the intervention group than in the control group, but the change in the duration of PA at ≥2.0 METs was not, which suggests that the target value could increase walking at moderate to vigorous intensity. In contrast, the change in duration of PA at 1.0–1.5 METs did not differ between the groups. When a target is set using step count as an indicator, there could be no obvious effect on sedentary time. As sedentary time is a risk factor for mortality in patients with COPD, independent of the duration of PA at ≥3.0 METs,30 additional new interventions may be needed to reduce sedentary time.
Of the eight measurable myokines, the changes in the GDF-15, BDNF-15, and Irisin levels were significantly greater in the intervention group than in the control group, although the changes in both SMI and phase angle were not markedly different between the groups. In particular, the change in GDF-15 values in subjects whose step count increased was significantly greater than that in subjects whose step count decreased. This change was thought to be due to an increase in their exercise habits.
GDF-15 is induced during tissue injury, inflammation, and oxidative stress,31 and is associated with senescence and energy metabolic disorders due to mitochondrial dysfunction.32,33 It is increased by long-term cell stress induced by several diseases, such as advanced cancer, chronic renal or cardiac failure, diabetes, or COPD,34 and this increase is a harmful response. However, it can also be temporarily increased by short-term cell stress such as exercise35 or pregnancy36 to restore homeostasis, presumably through a negative feedback mechanism; therefore, this increase is a beneficial response.34,37,38 According to the hypothesis of Breit et al, compared to this beneficial full feedback from exercise, partial feedback can occur when the patient has either obesity or diabetes (GDF-15 level of 800–3000 pg/mL), and no feedback can occur when the patient has either cancer or renal failure (GDF-15 level of 2000–10000 pg/mL).34
In the current study, the baseline level of GDF-15 was 1426±707 pg/mL, which is slightly higher than the normal range (GDF-15 level of 200–1200 pg/mL) and compatible with the previously reported levels in COPD.39–41 A feedback mechanism may be at work in patients with COPD, albeit only partially. Therefore, the increase in GDF-15 level after six months might have increased feedback as a beneficial adaptation. Although the direct mechanism underlying the effects of GDF-15 elevation induced by an increased step count is still unknown and requires further investigation, this change in GDF-15 might be a useful indicator for evaluating the effectiveness of exercise training for patients with COPD.
Although benefit of a web-based PA intervention for the patients with COPD with low self-efficacy has been reported,42 providing individualized step target and encouraging increased step count is a very simple intervention that may be useful in increasing PA in clinical settings. Further research is required to clarify the mechanisms and causal relationships between GDF-15 and PA changes.
The present study has several limitations. First, this study was conducted in a randomized but open-label manner because of the difficulty in providing target values using a blinded design. Although subjects in both groups were similarly encouraged to increase their step count to minimize influences other than providing target values, the presence of biases associated with an open-label approach cannot be excluded. Second, as we assessed differences in changes in PA and other parameters over six months between both groups, we performed a per-protocol rather than an intention-to-treat analysis. Therefore, we cannot exclude the possibility of overestimating the effect of the intervention or of bias. Third, the change in step count was one of the secondary outcomes but not the primary outcome. Therefore, the number of cases might not be sufficient to confirm the increasing effect of the step count by providing the target value. Further studies with larger numbers of participants are required to confirm the effects of providing the target value. Fourth, to exploratory evaluate the effect of providing target steps on other factors, changes in multiple factors including PA, PROs, and myokine parameters were set as secondary outcomes. Because the results of secondary outcomes could involve multiplicity of analysis, type 1 error could not be excluded. Fifth, the intervention was providing both target values and a pedometer but not target values alone. Therefore, it could not be denied that this positive effect might have been brought about by providing a pedometer. However, many previous studies have shown that patients who were given only a pedometer or only a target value were able to increase their step counts after three or four months, but these effects were not observed after six months.9–13 Considering these together, providing the individualized target values with a pedometer may be able to maintain the increasing subjects’ step counts over the long term. Sixth, the recruited subjects were older, with a higher proportion of men, and lower CAT scores than those observed in the COPD patient population in Western countries, which is characteristic of the Japanese COPD patient population.43 Further studies should examine whether compatible results are observed in subjects with different backgrounds. Seventh, the MoCA-J score of the recruited subjects was ≤25 points, indicating mild cognitive impairment. Cognitive impairment may put subjects at risk of difficulty remembering their target values or even remembering to increase their step count; therefore, this may have affected the results of the primary outcome. Eighth, most myokines were not detected by the myokines panel; therefore, we could not reach definitive results regarding the involvement of most myokines except GDF-15. It seems necessary to measure myokines using other methods that could measure smaller amounts. Nineth, we did not evaluate changes in the pulmonary function over six months. The relationship between changes in PA and changes in the pulmonary function should therefore be evaluated in future studies.
Conclusion
Providing individualized target step count values did not increase the proportion of subjects who achieved their target values but increased their step counts after six months. GDF-15 may be involved in this increase in step count.
Data Sharing Statement
The data that support the findings of this study are openly available in Dryad at https://doi.org/10.5061/dryad.v41ns1s6c.
Acknowledgments
We thank Brian Quinn, Managing Editor for Japan Medical Communication, for proofreading the manuscript. This study was funded by the Environmental Restoration and Conservation Agency, Japan.
Disclosure
Yoshiaki Minakata received lecture fees from Nippon Boehringer Ingelheim. Koichiro Takahashi received lecture fees from AstraZeneca, GlaxoSmithKline, Nippon Boehringer Ingelheim and Sanofi. Kazuhisa Asai received lecture fees from AstraZeneca, GlaxoSmithKline, Nippon Boehringer Ingelheim, Novartis Pharma and Sanofi. Tsunahiko Hirano received lecture fees from AstraZeneca, Sanofi, GlaxoSmithKline and Kyorin Pharmaceuticals. Kazuto Matsunaga received lecture fees from AstraZeneca, Sanofi, GlaxoSmithKline, Novartis Pharma, Kyorin Pharmaceutical and Nippon Boehringer Ingelheim. The authors report no other conflicts of interest in this work.
References
1. Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(9):972–977. doi:10.1164/rccm.200407-855OC
2. Minakata Y, Sugino A, Kanda M, et al. Reduced level of physical activity in Japanese patients with chronic obstructive pulmonary disease. Respir Investig. 2014;52(1):41–48. doi:10.1016/j.resinv.2013.06.0021
3. Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Anto JM. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax. 2006;61(9):772–778. doi:10.1136/thx.2006.060145
4. Waschki B, Kirsten A, Holz O, et al. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohort study. Chest. 2011;140(2):331–342. doi:10.1378/chest.10-2521
5. Garcia-Rio F, Rojo B, Casitas R, et al. Prognostic value of the objective measurement of daily physical activity in patients with COPD. Chest. 2012;142(2):338–346. doi:10.1378/chest.11-2014
6. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2025. Available from: www.goldcopd.org/2025-gold-report/.
7. Shioya T, Sato S, Iwakura M, et al. Improvement of physical activity in chronic obstructive pulmonary disease by pulmonary rehabilitation and pharmacological treatment. Respir Investig. 2018;56(4):292–306. doi:10.1016/j.resinv.2018.05.002
8. Megaritis D, Hume E, Chynkiamis N, et al. Effects of pharmacological and non-pharmacological interventions on physical activity outcomes in COPD: a systematic review and meta-analysis. ERJ Open Res. 2023;9(5):00409–2023. doi:10.1183/23120541.00409-2023
9. Armstrong M, Winnard A, Chynkiamis N, Boyle S, Burtin C, Vogiatzis I. Use of pedometers as a tool to promote daily physical activity levels in patients with COPD: a systematic review and meta-analysis. Eur Respir Rev. 2019;28(154):190039. doi:10.1183/16000617.0039-2019
10. Wan ES, Kantorowski A, Homsy D, et al. Promoting physical activity in COPD: insights from a randomized trial of a web-based intervention and pedometer use. Respir Med. 2017;130:102–110. doi:10.1016/j.rmed.2017.07.057
11. Moy ML, Collins RJ, Martinez CH, et al. An internet-mediated pedometer-based program improves health-related quality-of-life domains and daily step counts in COPD: a randomized controlled trial. Chest. 2015;148(1):128–137. doi:10.1378/chest.14-1466
12. Nolan CM, Maddocks M, Canavan JL, et al. Pedometer step count targets during pulmonary rehabilitation in chronic obstructive pulmonary disease. a randomized controlled trial. Am J Respir Crit Care Med. 2017;195(10):1344–1352. doi:10.1164/rccm.201607-1372OC
13. Moy ML, Martinez CH, Kadri R, et al. Long-term effects of an internet-mediated pedometer-based walking program for chronic obstructive pulmonary disease: randomized controlled trial. J Med Internet Res. 2016;18(8):e215. doi:10.2196/jmir.5622
14. Robinson SA, Wan ES, Shimada SL, Richardson CR, Moy ML. Age and attitudes towards an internet-mediated, pedometer-based physical activity intervention for chronic obstructive pulmonary disease: secondary analysis. JMIR Aging. 2020;3(2):e19527. doi:10.2196/19527
15. Nakanishi M, Minakata Y, Tanaka R, et al. Simple standard equation for daily step count in Japanese patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2019;14:1967–1977. doi:10.2147/copd.S218705
16. Sasaki S, Minakata Y, Azuma Y, Kaki T, Kawabe K, Ono H. Effects of individualized target setting on step count in Japanese patients with chronic obstructive pulmonary disease: a pilot study. Adv Respir Med. 2022;90(1):1–8. doi:10.5603/ARM.a2021.0080
17. Pedersen BK, Febbraio MA. Muscle as an endocrine organ: focus on muscle-derived interleukin-6. Physiol Rev. 2008;88(4):1379–1406. doi:10.1152/physrev.90100.2007
18. Raschke S, Eckardt K, Bjorklund Holven K, Jensen J, Eckel J. Identification and validation of novel contraction-regulated myokines released from primary human skeletal muscle cells. PLoS One. 2013;8(4):e62008. doi:10.1371/journal.pone.0062008
19. Pedersen BK. The diseasome of physical inactivity--and the role of myokines in muscle--fat cross talk. J Physiol. 2009;587(Pt 23):5559–5568. doi:10.1113/jphysiol.2009.179515
20. Fiuza-Luces C, Garatachea N, Berger NA, Lucia A. Exercise is the real polypill. Physiology. 2013;28(5):330–358. doi:10.1152/physiol.00019.2013
21. Ijiri N, Kanazawa H, Asai K, Watanabe T, Hirata K. Irisin, a newly discovered myokine, is a novel biomarker associated with physical activity in patients with chronic obstructive pulmonary disease. Respirology. 2015;20(4):612–617. doi:10.1111/resp.12513
22. Tanaka R, Sugiura H, Yamada M, et al. Physical inactivity is associated with decreased growth differentiation factor 11 in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2018;13:1333–1342. doi:10.2147/copd.S157035
23. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
24. Stanojevic S, Kaminsky DA, Miller MR, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J. 2022;60(1). doi:10.1183/13993003.01499-2021
25. Oishi K, Matsunaga K, Harada M, et al. A new dyspnea evaluation system focusing on patients’ perceptions of dyspnea and their living disabilities: the linkage between COPD and frailty. J Clin Med. 2020;9(11):3580. doi:10.3390/jcm9113580
26. Satake S, Senda K, Hong YJ, et al. Validity of the Kihon Checklist for assessing frailty status. Geriatr Gerontol Int. 2016;16(6):709–715. doi:10.1111/ggi.12543
27. Satake S, Shimokata H, Senda K, Kondo I, Toba K. Validity of total kihon checklist score for predicting the incidence of 3-year dependency and mortality in a community-dwelling older population. J Am Med Dir Assoc. 2017;18(6):552.e1–552.e6. doi:10.1016/j.jamda.2017.03.013
28. Fujiwara Y, Suzuki H, Yasunaga M, et al. Brief screening tool for mild cognitive impairment in older Japanese: validation of the Japanese version of the montreal cognitive assessment. Geriatr Gerontol Int. 2010;10(3):225–232. doi:10.1111/j.1447-0594.2010.00585.x
29. Demeyer H, Burtin C, Hornikx M, et al. The minimal important difference in physical activity in patients with COPD. PLoS One. 2016;11(4):e0154587. doi:10.1371/journal.pone.0154587
30. Furlanetto KC, Donaria L, Schneider LP, et al. Sedentary behavior is an independent predictor of mortality in subjects with COPD. Respir Care. 2017;62(5):579–587. doi:10.4187/respcare.05306
31. Unsicker K, Spittau B, Krieglstein K. The multiple facets of the TGF-β family cytokine growth/differentiation factor-15/macrophage inhibitory cytokine-1. Cytokine Growth Factor Rev. 2013;24(4):373–384. doi:10.1016/j.cytogfr.2013.05.003
32. Muñoz-Espín D, Serrano M. Cellular senescence: from physiology to pathology. Nat Rev Mol Cell Biol. 2014;15(7):482–496. doi:10.1038/nrm3823
33. Fujita Y, Taniguchi Y, Shinkai S, Tanaka M, Ito M. Secreted growth differentiation factor 15 as a potential biomarker for mitochondrial dysfunctions in aging and age-related disorders. Geriatr Gerontol Int. 2016;16 Suppl 1(S1):17–29. doi:10.1111/ggi.12724
34. Breit SN, Brown DA, Tsai VW. The GDF15-GFRAL pathway in health and metabolic disease: friend or foe? Annu Rev Physiol. 2021;10(83):127–151. doi:10.1146/annurev-physiol-022020-045449
35. Kleinert M, Clemmensen C, Sjøberg KA, et al. Exercise increases circulating GDF15 in humans. Mol Metab. 2018;9:187–191. doi:10.1016/j.molmet.2017.12.016
36. Andersson-Hall U, Svedin P, Mallard C, Blennow K, Zetterberg H, Holmäng A. Growth differentiation factor 15 increases in both cerebrospinal fluid and serum during pregnancy. PLoS One. 2021;16(5):e0248980. doi:10.1371/journal.pone.0248980
37. Wang D, Day EA, Townsend LK, Djordjevic D, Jørgensen SB, Steinberg GR. GDF15: emerging biology and therapeutic applications for obesity and cardiometabolic disease. Nat Rev Endocrinol. 2021;17(10):592–607. doi:10.1038/s41574-021-00529-7
38. Johann K, Kleinert M, Klaus S. The role of GDF15 as a myomitokine. Cells. 2021;10(11):2990. doi:10.3390/cells10112990
39. Patel MS, Lee J, Baz M, et al. Growth differentiation factor-15 is associated with muscle mass in chronic obstructive pulmonary disease and promotes muscle wasting in vivo. J Cachexia Sarcopenia Muscle. 2016;7(4):436–448. doi:10.1002/jcsm.12096
40. Husebø GR, Grønseth R, Lerner L, et al. Growth differentiation factor-15 is a predictor of important disease outcomes in patients with COPD. Eur Respir J. 2017;49(3):1601298. doi:10.1183/13993003.01298-2016
41. Hirano T, Doi K, Matsunaga K, et al. A novel role of growth differentiation factor (GDF)-15 in overlap with sedentary lifestyle and cognitive risk in COPD. J Clin Med. 2020;9(9):2737. doi:10.3390/jcm9092737
42. Robinson SA, Shimada SL, Quigley KS, Moy ML. A web-based physical activity intervention benefits persons with low self-efficacy in COPD: results from a randomized controlled trial. J Behav Med. 2019;42(6):1082–1090. doi:10.1007/s10865-019-00042-3
43. Ishii T, Nishimura M, Akimoto A, James MH, Jones P. Understanding low COPD exacerbation rates in Japan: a review and comparison with other countries. Int J Chron Obstruct Pulmon Dis. 2018;13:3459–3471. doi:10.2147/copd.S165187
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.