Back to Journals » Journal of Pain Research » Volume 19
Effects of External Oblique Intercostal Plane Block and Subcostal Transversus Abdominis Plane Block on Postoperative Pulmonary Functions After Laparoscopic Cholecystectomy: A Prospective Observational Study
Authors Gürbüz Z, Köksal İncegül BG, Baytar Ç ![]() , Baytar MS, Bollucuoğlu K, Okyay RD, Tomruk Erdem A, Kurada G
, Baytar MS, Bollucuoğlu K, Okyay RD, Tomruk Erdem A, Kurada G ![]() , Pişkin Ö, Ayoğlu H
, Pişkin Ö, Ayoğlu H
Received 1 April 2026
Accepted for publication 28 May 2026
Published 3 June 2026 Volume 2026:19 613785
DOI https://doi.org/10.2147/JPR.S613785
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Karina Gritsenko
Zeynep Gürbüz,1 Bengü Gülhan Köksal İncegül,2 Çağdaş Baytar,2 Merve Sena Baytar,2 Keziban Bollucuoğlu,2 Rahşan Dilek Okyay,2 Ayşegül Tomruk Erdem,3 Gizem Kurada,2 Özcan Pişkin,2 Hilal Ayoğlu2
1Department of Anesthesiology and Reanimation, Lüleburgaz State Hospital, Kırklareli, Türkiye; 2Department of Anesthesiology and Reanimation, Zonguldak Bülent Ecevit University Medicine Faculty, Zonguldak, Türkiye; 3Department of Chest Diseases, Zonguldak Bülent Ecevit University Medicine Faculty, Zonguldak, Türkiye
Correspondence: Bengü Gülhan Köksal İncegül, Department of Anesthesiology and Reanimation, Faculty of Medicine, Zonguldak Bülent Ecevit University, Esenköy- Kozlu, Zonguldak, 67630, Turkey, Tel +90 530 558 30 76, Fax +90 372 257 21 40, Email [email protected]
Background: We aimed to investigate the effects of the external oblique intercostal plane block (EOIPB) and subcostal transversus abdominis plane (TAP) block on postoperative pulmonary function in patients undergoing laparoscopic cholecystectomy. The primary outcome was spirometric pulmonary function test (PFT) results. Secondary outcomes included postoperative pain scores, opioid consumption, and postoperative recovery assessed using the Quality of Recovery (QoR)-15 questionnaire.
Methods: A total of 102 patients aged 18– 65 years with ASA physical status I–III who underwent elective laparoscopic cholecystectomy were included in this prospective observational study. According to the perioperative analgesia technique applied, patients were evaluated in three groups: Group Subcostal (n=34), Group EOIPB (n=34), and Group Control (n=34). After losses to follow-up, 90 patients were included in the final analysis. Preoperative and postoperative spirometric PFTs, postoperative pain scores, opioid consumption, and QoR-15 scores were recorded and compared among groups.
Results: Postoperative reductions in FVC, FEV1, predicted FEV1, and PEF values were observed in all groups but were significantly more pronounced in the Control group. At postoperative hour 1, pulmonary function parameters were significantly lower in the Control group compared with both block groups (p < 0.05). Predicted FEV1 at postoperative hour 1 was significantly higher in the EOIPB group than in Subcostal group (p = 0.003). Postoperative pain scores and opioid consumption were significantly lower in both block groups compared with the Control group (p < 0.05), whereas QoR-15 scores were significantly higher (p < 0.05). No significant differences were observed between the two block groups for most postoperative outcomes.
Conclusion: Both EOIPB and subcostal TAP block were associated with attenuated decline in postoperative pulmonary function, reduced opioid consumption, and improved early postoperative recovery after laparoscopic cholecystectomy.
Keywords: external oblique intercostal plane block, subcostal transversus abdominis plane block, postoperative pulmonary dysfunction, opioid consumption, quality of recovery
Introduction
Major abdominal surgeries may lead to early postoperative respiratory dysfunction by impairing respiratory muscle activity.1 Following abdominal surgery, patients typically exhibit a respiratory pattern resembling a “restrictive syndrome”, characterized by reductions in tidal volume, vital capacity, and functional residual capacity. The underlying mechanisms include muscle incision, reflex diaphragmatic inhibition, and pain.2 Reflex diaphragmatic inhibition refers to partial paralysis of the diaphragm and is considered one of the most important contributors to postoperative respiratory dysfunction. Postoperative respiratory dysfunction is more severe after upper abdominal surgeries, such as laparoscopic cholecystectomy, compared with lower abdominal procedures and may persist for up to 10 days after surgery. Consequently, the incidence of respiratory complications including atelectasis, pneumonia, tracheobronchial infection, respiratory failure, and prolonged hospital stay increases.3 Effective pain control improves diaphragmatic movement and respiratory function and helps prevent postoperative respiratory complications.1
Pain following laparoscopic cholecystectomy consists of both parietal and visceral components.4 Visceral pain results from tissue injury caused by gallbladder dissection and stretching of nerve endings within the peritoneal cavity, whereas parietal pain arises from incisional trauma at the port entry sites.5 In addition, postoperative shoulder pain may occur due to irritation and stretching of the phrenic nerve by carbon dioxide during pneumoperitoneum. This acute postoperative pain is typically moderate to severe in intensity. It peaks within the first few hours after surgery and generally decreases within 2–3 days. However, numerous factors influence pain severity, including the extent of surgical trauma, anesthetic management, and the patient’s physiological and psychological status. Therefore, the optimal strategy for pain management is a multimodal analgesic approach.6 The addition of regional anesthesia techniques to pain management reduces the surgical stress response, decreases opioid consumption, facilitates pain control, and improves postoperative patient satisfaction.7
The somatic sensation of the upper abdominal wall is derived from the anterior and lateral cutaneous branches of the lower intercostal nerves (T6–T10). The subcostal transversus abdominis plane (TAP) block targets the upper abdominal dermatomes (T6–T9) and is therefore suitable for incisions in the supraumbilical region. By blocking the anterior cutaneous branches of the intercostal nerves, it primarily provides sensory blockade in the midline region of the abdomen.7–9
The external oblique intercostal plane block (EOIPB) is a regional anesthesia technique that provides cutaneous analgesia to the anterolateral upper abdomen by blocking the anterior and lateral cutaneous branches of the intercostal nerves between T6 and T9/10.10
We aimed to investigate the effects of the EOIPB and the subcostal TAP block on postoperative pulmonary function in patients undergoing laparoscopic cholecystectomy. The primary outcome was to compare spirometric PFT results. Secondary outcomes were the comparison of postoperative pain scores at rest and during movement, total opioid consumption, and assessing the functional recovery via Quality of Recovery (QoR)-15 on postoperative day 1. Although both EOIPB and subcostal TAP block have been investigated for postoperative analgesia, comparative data regarding their effects on postoperative pulmonary function after laparoscopic cholecystectomy remain limited. Therefore, we hypothesized that both regional anesthesia techniques would be associated with improved postoperative pulmonary function and reduced opioid consumption compared with conventional analgesia.
Methods
Study Design
This prospective observational study was conducted between December 2023 and October 2024 after obtaining approval from the Clinical Research Ethics Committee of Zonguldak Bülent Ecevit University Hospital (meeting date: 18 August 2023/10; protocol number: 2023/ 04–3; ClinicalTrials.gov identifier: NCT06144307). The study aimed to prospectively evaluate postoperative pulmonary outcomes among patients receiving different perioperative analgesia approaches routinely used in clinical practice. All patients were informed about the study, and both written and verbal informed consent were obtained. The study was conducted in accordance with the STROBE guidelines.
Study Population
A total of 102 patients aged 18–65 years, classified as American Society of Anesthesiologists physical status (ASA PS) I–III and scheduled for elective laparoscopic cholecystectomy under general anesthesia, were included in the study.
Exclusion criteria included refusal to participate, ASA PS IV–V, allergy to local anesthetics; presence of coagulopathy; infection at the planned block site; chronic analgesic use; spirometric values below 50% of predicted values in preoperative measurements; known diaphragmatic paralysis; presence of dementia or confusion; any respiratory disease; congestive heart failure; unstable hypertension; severe cardiac, renal, hepatic, or hematologic disease; history of thoracoabdominal surgery; respiratory tract infection within the previous month; history of smoking; inability to cooperate; psychiatric illness; or body mass index (BMI) > 30 kg/m2 and conversion to open surgery. Smokers and patients with a BMI >30 kg/m2 were excluded because these factors are independent predictors of postoperative pulmonary complications and could confound spirometric outcomes. Patients with pre-existing pulmonary disease were excluded to ensure a homogeneous study population and to allow isolated evaluation of the regional anesthesia technique on postoperative pulmonary function.
Group Allocation and Blinding
Patients were categorized into three groups according to the perioperative analgesia technique applied during clinical management, ensuring an equal number of participants in each group. The anesthesiologist responsible for postoperative assessments and data collection, as well as ward nurses, were blinded to group categorization throughout the study period. Patients were not informed about the analgesia technique group during postoperative outcome assessments. No sham block procedure was performed in the control group because of ethical concerns regarding an invasive placebo intervention.
Preoperative Procedures
After obtaining written and verbal informed consent, all patients were provided with detailed information in the premedication room regarding the Numeric Rating Scale (NRS), the intravenous patient-controlled analgesia (IV PCA) device, and the maneuvers required during PFT. Following the recording of demographic data, patients were placed in a seated position for measurement of pulmonary function. Pulmonary function was assessed using a portable spirometer (CONTEC SP10 Digital Spirometer, CONTEC, Hebei, China) in accordance with the American Thoracic Society guidelines. After entering the patients’ sex, age, height, weight, and smoking status into the device, a disposable mouthpiece with a filter was attached. A nose clip was applied to prevent nasal airflow. After positioning the mouthpiece between the patients’ lips and allowing 4–5 normal breaths, patients were instructed to take a deep and forceful inspiration. Subsequently, without delay, patients were instructed to perform a rapid and forceful expiration lasting at least 6 seconds. The test was completed by instructing the patients to take a deep inspiration again. During this procedure, the device recorded forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), the FEV1/FVC ratio, peak expiratory flow (PEF), and predicted FEV1 values. The best result of three consecutive measurements was recorded for analysis.
Anesthesia and Analgesia Management
All patients were taken to the operating room, and in addition to routine monitoring, train-of-four monitoring (TOF; TOF-Watch SX), bispectral index (BIS), and Pleth Variability Index (PVI; Masimo Radical-7™ Pulse CO-Oximeter®) monitoring were applied. All patients received standardized general anesthesia. Anesthesia was induced with 1 mg/kg lidocaine, 2–3 mg/kg propofol, 1 µg/kg fentanyl, and 0.6 mg/kg rocuronium. Following endotracheal intubation, oxygenation was maintained with a 50:50 air–oxygen mixture. Mechanical ventilation was adjusted to a tidal volume of 6–8 mL/kg, PEEP 5–10 cmH2O, and a respiratory rate adjusted to maintain EtCO2 between 35 and 45 mmHg.
After endotracheal intubation, patients were assigned to their respective groups, and the block was performed before the surgical incision. In the Group Subcostal, patients were placed in the supine position, and standard sterile preparation was performed. A linear ultrasound probe (Esaote MyLab X7, Italy) was positioned inferior to the xiphoid process. The rectus abdominis muscles were identified bilaterally, with the linea alba located centrally. The probe was then moved laterally along the costal margin in a slightly oblique orientation until the transversus abdominis muscle was visualized beneath the rectus abdominis muscle. Using an in-plane technique, a 22-gauge, 80-mm block needle (BRAUN Stimuplex® Ultra 360®, Germany) was advanced from anteromedial to posterolateral to reach the fascial plane between the rectus abdominis and transversus abdominis muscles. After negative aspiration, correct needle placement was confirmed with 1 mL of normal saline, followed by injection of 20 mL of 0.25% bupivacaine solution. The spread of the solution along the fascial plane was visualized in real time on ultrasound (Figure 1). The procedure was performed bilaterally.
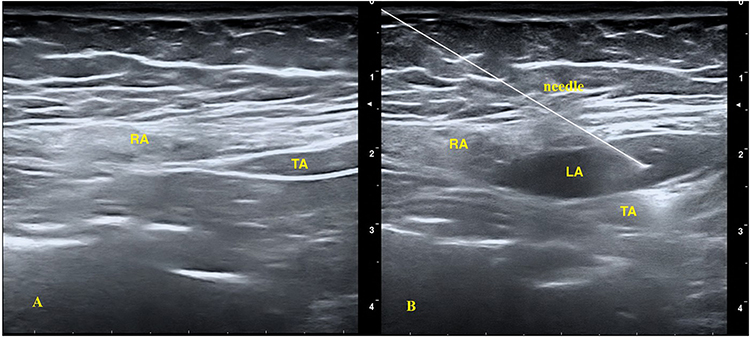 |
Figure 1 Ultrasound image of subcostal transversus abdominis plane block. (A) Pre-injection view of the target plane. (B) Post-injection spread of local anesthetic within the interfascial plane. Abbreviations: RA, rectus abdominis muscle; TA, transversus abdominis muscle; LA, local anesthetic. |
In the Group EOIPB, after standard sterile preparation in the supine position, a linear ultrasound probe (Esaote MyLab X7, Italy) was placed in a sagittal orientation at the level of the sixth and seventh ribs, lateral to the midclavicular line. After slight rotation of the probe, the intercostal muscle between the sixth and seventh ribs and the overlying external oblique muscle were identified. Using an in-plane technique, a 22-gauge, 50-mm block needle (BRAUN Stimuplex® Ultra 360®, Germany) was advanced from superior to inferior to reach the fascial plane beneath the external oblique muscle. Following negative aspiration, correct needle placement was confirmed with 1 mL of normal saline, and 20 mL of 0.25% bupivacaine solution was injected. The spread of the solution along the fascial plane was visualized in real time on ultrasound (Figure 2). The procedure was performed bilaterally. After completion of the block, the patient was handed over to the surgical team.
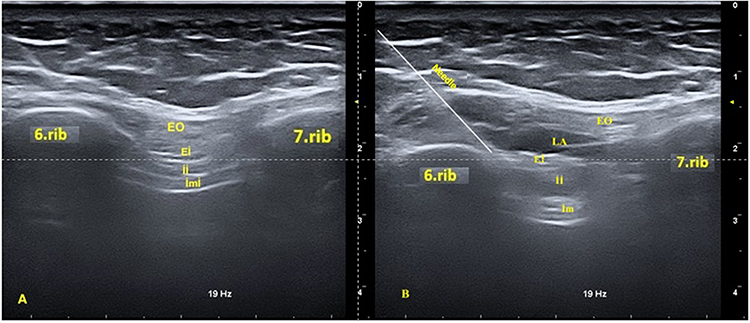 |
Figure 2 Ultrasound image of external oblique intercostal plane block technique. (A) Pre-injection view of the target plane. (B) Post-injection spread of local anesthetic within the interfascial plane. Abbreviations: EO, external oblique muscle; EI, external intercostal muscle; II, internal intercostal muscle; IMI, innermost intercostal muscle; LA, local anesthetic. |
Anesthesia maintenance was provided with sevoflurane with a BIS between 40 and 60 during surgery. Remifentanil infusion was administered at a rate of 0.05–0.2 µg/kg/min, adjusted to allow no more than a 20% change from baseline mean arterial pressure. Intraoperative fluid therapy was maintained at a PVI of 14% to 16%. Hemodynamic parameters were recorded at certain intervals during the intraoperative period. In cases of a greater than 20% decrease in baseline heart rate or blood pressure, 0.01 mg/kg intravenous atropine and 5 mg intravenous ephedrine were administered, respectively. Thirty minutes before the end of surgery, all groups received 1 g paracetamol, 100 mg tramadol, and 10 mg metoclopramide intravenously. Remifentanil infusion was stopped with the final suture, and the total amount of remifentanil consumed was recorded. Neuromuscular blockade was reversed with 2–4 mg/kg sugammadex. Patients were extubated when the TOF ratio exceeded 0.9 and subsequently transferred to the recovery unit. The time from anesthesia induction to extubation was defined as “anesthesia duration”, the time from incision to placement of the final suture as “surgical duration”, and the time from the final suture to extubation as “extubation time”.
Surgical Technique
All surgeries were performed by a single surgeon using the same technique (IT). Following a 1-cm supraumbilical incision and establishment of pneumoperitoneum, a 10-mm trocar was inserted, and the intra-abdominal cavity was accessed using a camera. A 10-mm trocar was placed through a 1-cm subxiphoid incision, and two 5-mm trocars were inserted through 0.5-cm incisions along the right anterior axillary and midclavicular lines. After identification and dissection of the cystic artery and cystic duct, cholecystectomy was completed, and the gallbladder was removed from the abdominal cavity using an endobag. Following hemostasis, the peritoneal cavity was irrigated with normal saline. A Jackson drain was placed in the operative bed, and the abdomen was desufflated. After removal of all trocars, the fascia, subcutaneous tissue, and skin were closed at the umbilical trocar site, whereas only the subcutaneous tissue and skin were closed at the remaining trocar sites.
Postoperative Procedures
Patients who were transferred to and monitored in the post-anesthesia care unit (PACU) were connected to an IV PCA device. The PCA device was programmed to deliver tramadol at a concentration of 3 mg/mL without basal infusion, with a bolus dose of 10 mg, a lockout interval of 20 minutes, and a 4-hour limit of 100 mg. The time of admission to the PACU was defined as postoperative hour 0. Pain scores at rest and during movement (coughing) were assessed using the NRS, and sedation levels were evaluated using the Ramsay Sedation Scale (RSS) at 20 minutes in the PACU. Patients with an NRS score ≥ 4 at 20 minutes received 25 µg fentanyl as rescue analgesia. Pain was reassessed every 15 minutes, and fentanyl administration was repeated if the NRS score remained ≥ 4. The use of rescue analgesia and the total amount administered were recorded until discharge from the PACU. The presence of nausea and vomiting was evaluated using a Likert scale (0: none, 1: mild, 2: moderate, 3: severe nausea, 4: vomiting). If the score was ≥ 3, 4 mg ondansetron was administered and documented. Patients with a modified Aldrete score ≥ 9 were transferred to the ward.
In the ward, spirometric PFTs were performed at postoperative hours 1, 6, and 24. For each time point, the best value of three consecutive measurements was selected and recorded. FVC, FEV1, the FEV1/FVC ratio, PEF, and predicted FEV1 values were documented.
Paracetamol 1 g every 8 hours and dexketoprofen 50 mg every 12 hours were administered. Pain scores at rest and during movement were recorded at postoperative hours 1, 2, 6, 12, and 24 using the NRS. At each assessment, RSS scores and the presence of nausea and vomiting (according to the Likert scale) were also documented. If the NRS score was ≥ 4 despite administration of paracetamol, dexketoprofen, and tramadol via IV PCA, intravenous pethidine 0.25 mg/kg was planned as rescue analgesia. The PCA device was discontinued at postoperative hour 24. Cumulative tramadol consumption was recorded at postoperative hours 1, 2, 6, 12, and 24. The total amount of rescue analgesic administered was also documented. At postoperative hour 24, patients completed the QoR-15 questionnaire, and the results were recorded. The validated Turkish version of the QoR-15 questionnaire was used for postoperative recovery assessment.11 Other postoperative complications were also documented.
Statistical Analysis
The estimated sample size was calculated prior to study initiation using GPower software. The calculation was based on pilot data obtained from 10 patients in each group prior to initiation of the main study, and these patients were not included in the final analysis. Postoperative FEV1 values, defined as the primary outcome of the study, were used for sample size estimation. Because postoperative opioid consumption and recovery parameters were also considered clinically relevant secondary outcomes, supplementary analyses were additionally performed. Among these variables, postoperative opioid consumption required the largest sample size (29 patients per group). Therefore, the final sample size was determined according to this most conservative estimate. Considering possible losses to follow-up, 102 patients were enrolled in the study.
Data were analyzed using SPSS version 27.0. Descriptive statistics were presented as mean ± standard deviation (SD), median, and minimum–maximum (min–max) for quantitative variables, and as frequency and percentage for categorical variables. The normality of quantitative variables within groups was assessed using the Kolmogorov–Smirnov test. Normally distributed continuous variables were compared across the three groups using one-way ANOVA; when a statistically significant overall difference was identified, pairwise comparisons were conducted using the Tukey post hoc test. For variables that did not meet the assumption of normality, the Kruskal–Wallis test was employed, followed by Dunn’s test with Bonferroni correction for pairwise comparisons when the overall test reached significance. Categorical variables were analyzed using the chi-square test. All analyses were evaluated at a 95% confidence interval (CI), and p < 0.05 was considered statistically significant.
Results
A total of 109 patients scheduled to undergo laparoscopic cholecystectomy were assessed for eligibility, of whom 102 were included in the study. Three patients declined participation, and four were excluded due to inability to comply with spirometry. In the Group Control, four patients refused postoperative spirometry, and in both the Group Subcostal and Group EOIPB, technical problems with the PCA devices occurred in four patients each. Therefore, 90 patients were included in the final statistical analysis (Figure 3). No significant differences were found among the groups regarding demographic and clinical characteristics or operative durations (p>0.05) (Table 1). Intraoperative remifentanil consumption was significantly higher in the Group Control (573.33 ± 369.00 µg) compared with the block groups (p < 0.05). However, no significant difference was observed between the Group EOIPB (371.67 ± 281.86 µg) and the Group Subcostal (316.17 ± 196.42 µg; p = 0.578). Intraoperative hemodynamic parameters, BIS, EtCO2, and PVI values did not differ significantly among the groups.
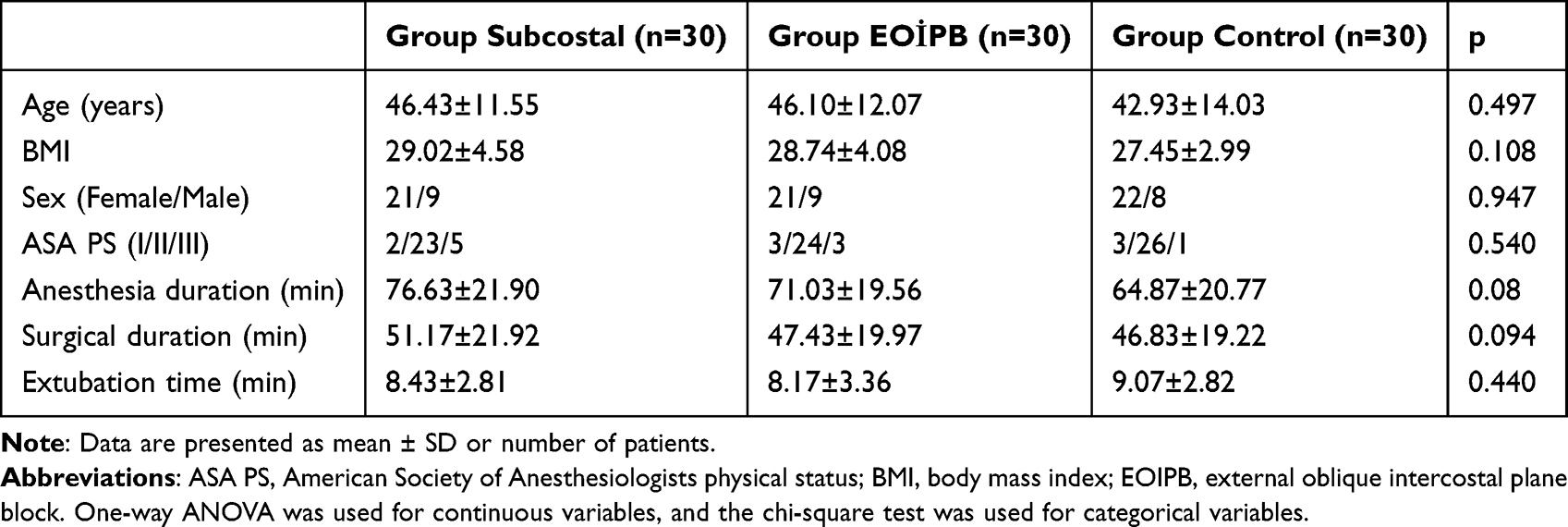 |
Table 1 Demographic and Clinical Characteristics of the Patients and Operative Durations |
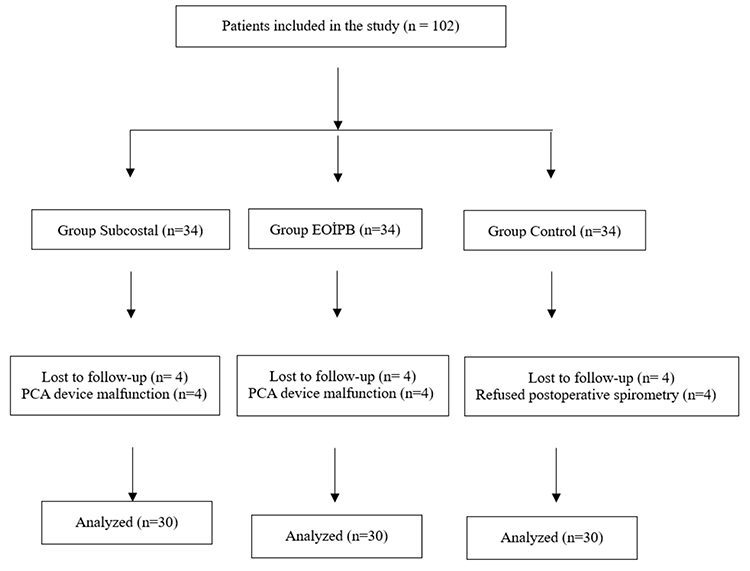 |
Figure 3 Flow Diagram. |
When RSS scores at 20 minutes in the PACU were compared, no statistically significant differences were observed among the groups (Group Control: 1 [1–3], Group Subcostal: 2 [1–3], Group EOIPB: 2 [1–3]; p > 0.05). In the PACU, pain scores at rest and during movement were significantly higher in the Group Control compared with the block groups (Group Control, rest NRS: 5 [2–8], dynamic NRS: 6 [3–9]; Group EOIPB, rest NRS: 3 [0–7], dynamic NRS: 3 [0–7]; Group Subcostal, rest NRS: 3 [0–7], dynamic NRS: 4 [1–8]; p < 0.001). No significant difference was observed between the Group EOIPB and Group Subcostal (p > 0.05). Fentanyl was administered in the PACU to 19 patients in the Group Control, 10 patients in the Group Subcostal, and 7 patients in the Group EOIPB. The amount of fentanyl consumed in the PACU was significantly higher in the Group Control compared with the block groups (Group Control: 37.5 [0–75] µg; Group Subcostal: 0 [0–50] µg; Group EOIPB: 0 [0–75] µg; p < 0.05), with no significant difference between the Group EOIPB and Group Subcostal (p = 0.390). Vital parameters in the PACU were similar among all groups (p > 0.05). No complications occurred in the PACU.
Analysis of spirometric PFT results demonstrated no significant differences among the groups in preoperative FVC, FEV1, FEV1/FVC ratio, PEF, or predicted FEV1 values (Table 2). Similarly, no statistically significant differences were observed among the groups in FEV1/FVC values at postoperative hours 1, 6, and 24. At postoperative hour 1, FVC, FEV1, predicted FEV1, and PEF values were significantly lower in the Control group compared with the Group Subcostal and Group EOIPB (Table 2). At postoperative hour 6, predicted FEV1 and PEF values remained significantly lower in the Group Control than in the block groups. Across all postoperative time points, the reduction in FVC, FEV1, predicted FEV1, and PEF values relative to preoperative measurements was greater in the Group Control compared with the Group Subcostal and Group EOIPB. At postoperative hour 1, the predicted FEV1 value was significantly higher in the Group EOIPB than in the Group Subcostal. However, no significant differences were observed between the two block groups in predicted FEV1 or other pulmonary function parameters at the remaining postoperative time points.
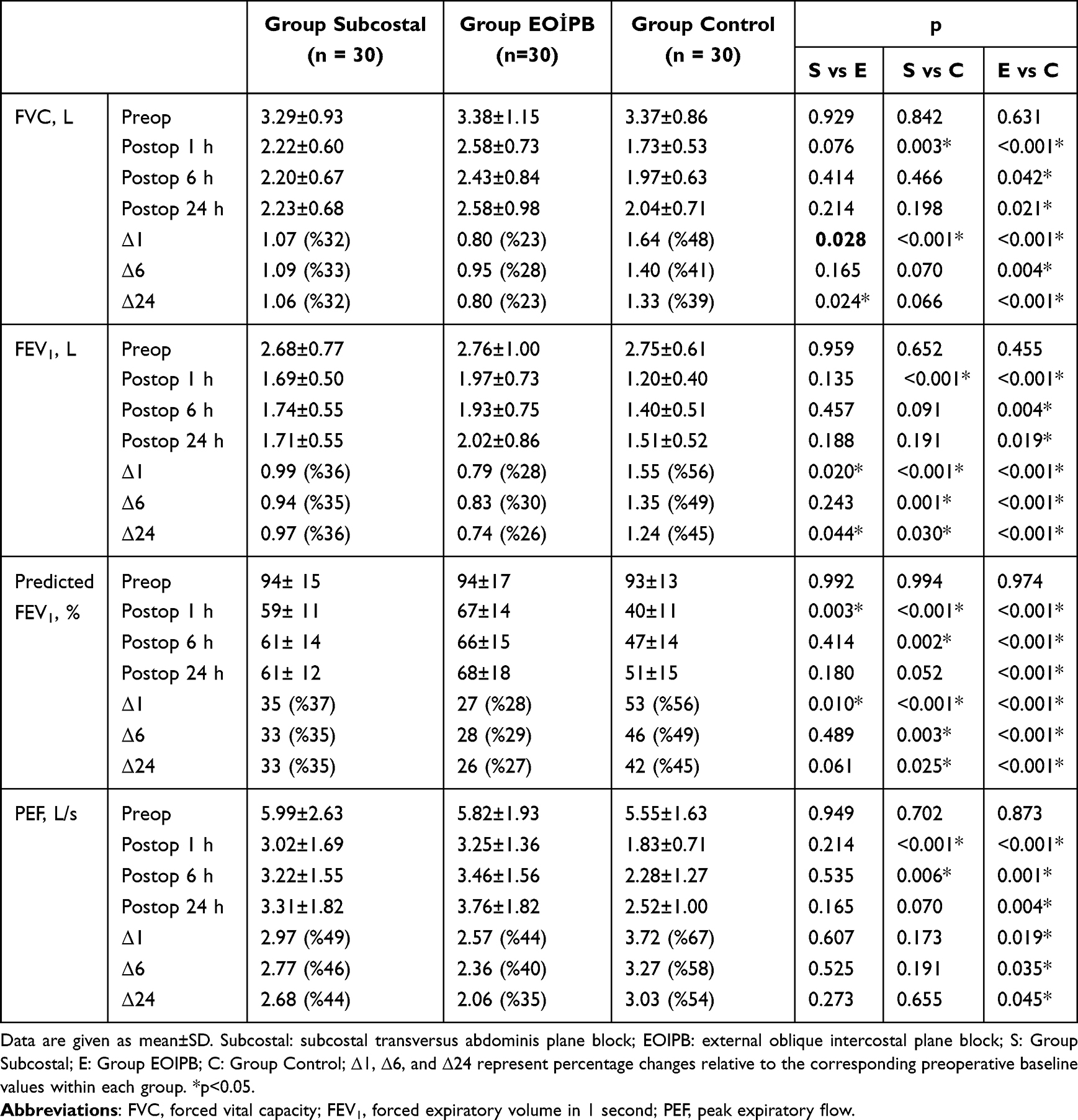 |
Table 2 Comparison of Spirometric Pulmonary Function Test Results Among the Groups |
When cumulative postoperative tramadol consumption was compared among the groups at 0–1, 0–2, 0–6, 0–12, and 0–24 hours, tramadol use was significantly lower in both the Group Subcostal and Group EOIPB compared with the Group Control at all time intervals (p < 0.05). During the first postoperative hour (0–1 h), tramadol consumption was significantly lower in the Group EOIPB than in the Group Subcostal (p = 0.036) (Table 3).
 |
Table 3 Comparison of Cumulative Postoperative Tramadol Consumption (Mg) |
Postoperative NRS scores at rest were significantly higher in the Group Control compared with the block groups, with no statistically significant difference between the Group Subcostal and Group EOIPB. Dynamic NRS scores at postoperative 20 minutes and at 1, 2, 6, and 12 hours were significantly higher in the Group Control compared with both the Group Subcostal and Group EOIPB. At postoperative hour 24, dynamic NRS scores were significantly lower in the Group Subcostal compared with the Group Control, whereas no significant difference was observed between the Group EOIPB and Group Control. No statistically significant differences in dynamic NRS scores were observed between the Group Subcostal and Group EOIPB at any time point (Table 4).
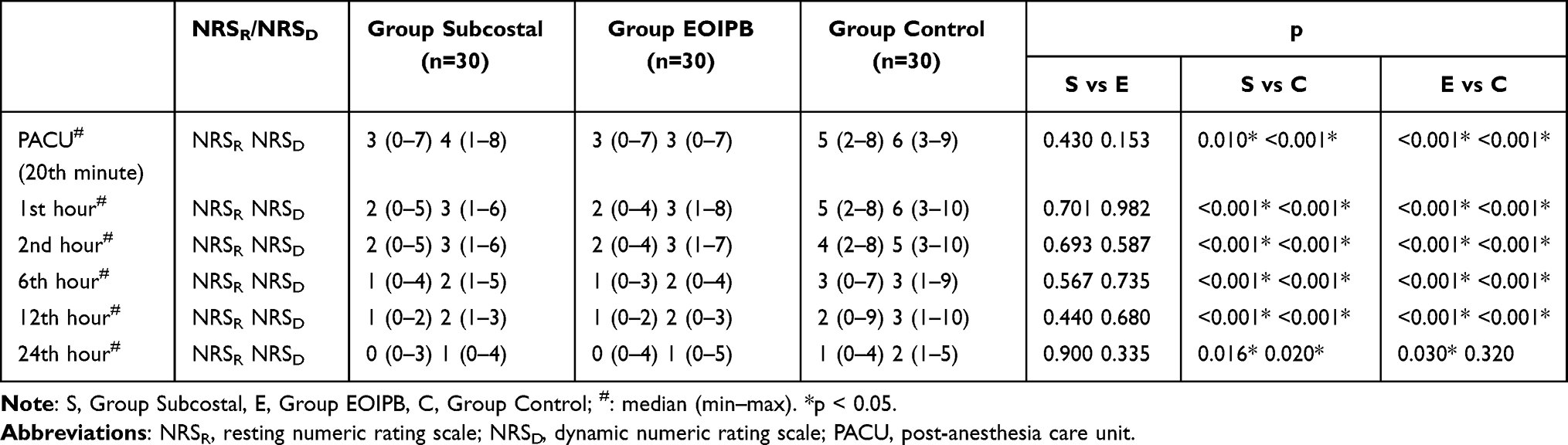 |
Table 4 Comparison of the Numerical Rating Scale (NRS) Pain Scores |
At postoperative hour 24, total QoR-15 scores were significantly lower in the Group Control compared with the Group Subcostal and Group EOIPB. Among the QoR-15 subdomains, pain, physical comfort, physical independence, and emotional state scores were significantly lower in the Group Control than in the Group Subcostal and Group EOIPB. No significant differences were observed among the groups in the psychological support subdomain. No statistically significant differences were found between the Group Subcostal and Group EOIPB in any of the QoR-15 subdomain scores (Table 5).
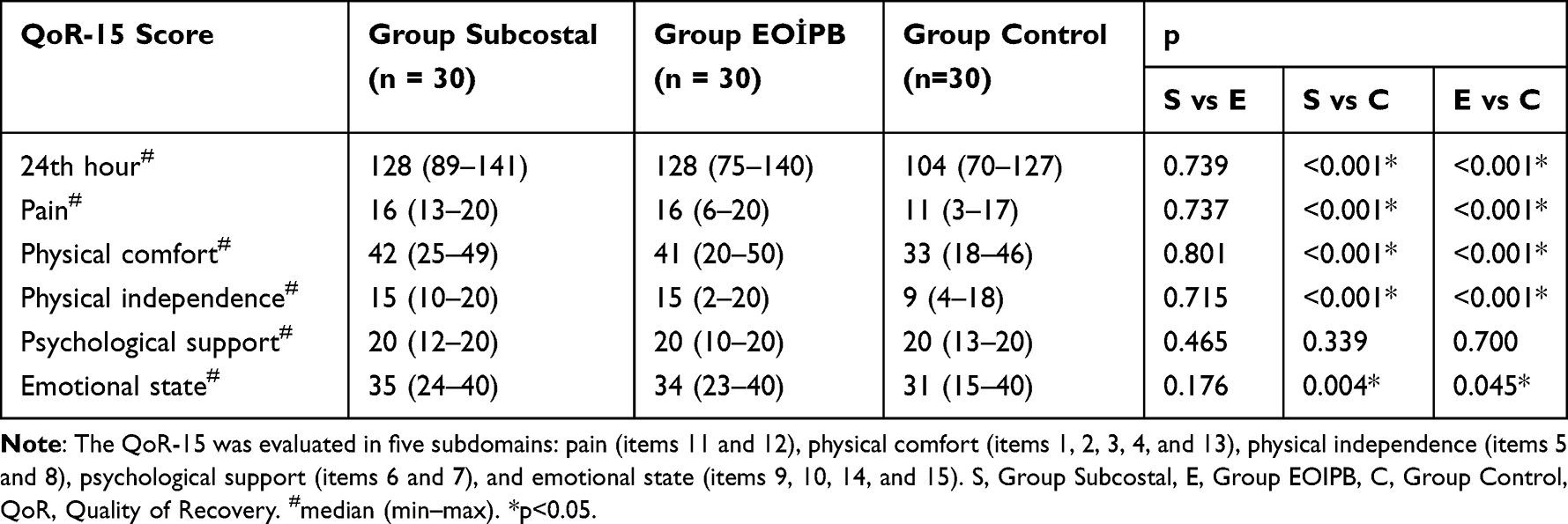 |
Table 5 Quality of Recovery-15 Scores Between the Groups |
No statistically significant differences were observed among the groups in RSS scores at any time point (Table 6). Based on nausea and vomiting data recorded during the 24-hour follow-up, 5 patients in the Group Subcostal, 3 patients in the Group EOIPB, and 9 patients in the Group Control had a Likert scale score ≥ 3 and required ondansetron administration. There was no statistically significant difference among the groups (p > 0.05). No block-related complications, including local anesthetic systemic toxicity, pneumothorax, or hematoma formation, were observed in any patient. No other postoperative complications occurred within the 24-hour follow-up period. When rescue analgesic requirements were compared at 24 hours, pethidine consumption was significantly lower in the Group Subcostal (n = 3) and Group EOIPB (n = 2) compared with the Group Control (n = 20; p < 0.001). No significant difference was observed between the Group Subcostal and Group EOIPB (p = 1.000).
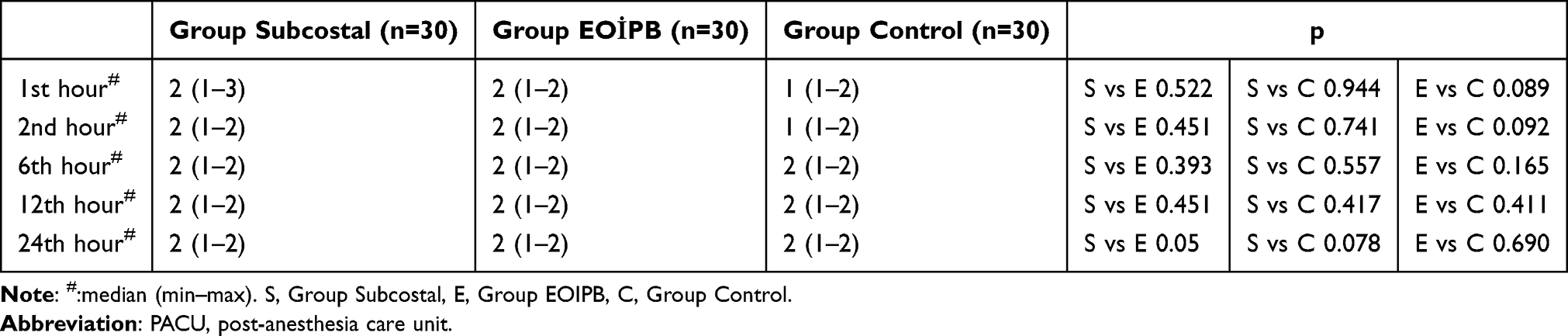 |
Table 6 Ramsay Sedation Scale (RSS) Scores |
Discussion
In this study, we investigated the effects of the EOIPB and the subcostal TAP block on postoperative pulmonary function in patients undergoing laparoscopic cholecystectomy. Compared with the Group Control, postoperative spirometric PFT results were less impaired in both the Group Subcostal and Group EOIPB. The significant improvements in FEV1 and FVC observed in the Group EOIPB compared with the Group Control persisted for up to 24 hours postoperatively. Predicted FEV1 values remained higher in both block groups for up to 24 hours compared with the Group Control. Similarly, PEF values were higher up to 24 hours in the Group EOIPB and up to 6 hours in the Group Subcostal compared with the Group Control. Opioid consumption was lower in both block groups than in the Group Control, whereas postoperative QoR-15 scores were higher. In addition, both resting and dynamic NRS pain scores were lower in the block groups compared with the Group Control. No significant differences were observed between the Group EOIPB and Group Subcostal.
After upper abdominal surgery, expiration is markedly impaired due to both muscle incision and postoperative pain, resulting in the development of a restrictive respiratory pattern.1,12 In restrictive disorders, FEV1 and FVC typically decrease to approximately 40–50% below preoperative values, whereas the FEV1/FVC ratio generally remains unchanged.13,14 Rademaker et al15 reported a 30–45% reduction in FEV1 and FVC at postoperative hours 2 and 24 following laparoscopic cholecystectomy. Similarly, Keus et al16 and Staehr-Rye et al17 observed a 18–20% decrease in FEV1 and FVC at 24 hours after laparoscopic cholecystectomy. In our study, the Group Control demonstrated a 39–56% reduction in FEV1 and FVC values at postoperative hour 24. The finding that the FEV1/FVC ratio remained above 70% at all time points indicates the absence of obstructive pulmonary dysfunction in our patient population.
Optimal pain control is one of the critical factors in reducing postoperative pulmonary complications.18 In a study including 58 patients undergoing laparoscopic cholecystectomy, FEV1 and FVC values at postoperative hour 1 were reported to be significantly higher in the TAP block group compared with the control group.19 In our study, reductions in FEV1 and FVC values in the Group Control ranged from 45–56% and 39–48%, respectively. In contrast, decreases in FEV1 and FVC were 26–30% and 23–28% in the Group EOIPB, and 35–36% and 32–33% in the Group Subcostal, respectively. These findings indicate that FEV1 and FVC values were preserved by approximately 10–20% in the block groups compared with the Group Control. Compared with the Group Control, FEV1 and FVC values remained significantly higher for up to 24 hours postoperatively in the Group EOIPB, whereas in the Group Subcostal, a statistically significant difference was observed only at postoperative hour 1. Although not statistically significant, the magnitude of reduction in FEV1 and FVC over 24 hours was consistently lower in the Group Subcostal compared with the Group Control. These findings suggest that both block techniques contribute to the development of a less pronounced restrictive respiratory pattern. Although no statistically significant difference was observed between the two blocks, we noted that the beneficial effects of EOIPB on pulmonary function appeared to persist for a longer duration.
Peak expiratory flow (PEF) represents the highest flow rate achieved at the beginning of forced expiration and reflects the strength of the expiratory muscles.20 The rectus abdominis, external oblique, internal oblique, and transversus abdominis muscles contribute to respiration to varying degrees and are primarily active during forced expiration. Following abdominal surgery, expiration is markedly impaired due to both muscle incision and postoperative pain.21 Hendolin et al22 demonstrated that PEF decreased by 55% in patients receiving general anesthesia alone after laparoscopic cholecystectomy, whereas the reduction was limited to 20% in patients receiving thoracic epidural analgesia. In our study, PEF values in the Group EOIPB remained higher than those in the Group Control for up to 24 hours postoperatively, while in the Group Subcostal, higher PEF values were observed up to 6 hours compared with the Group Control. Furthermore, the reduction in PEF at postoperative hours 1, 6, and 24 was less pronounced in the block groups. These findings suggest that effective analgesia provided by EOIPB and subcostal TAP block enabled patients to use their expiratory (abdominal) muscles more effectively in the postoperative period. However, because no significant differences in PEF values were observed between the block groups over 24 hours, neither technique appears to be superior to the other in this regard.
The severity of restrictive respiratory dysfunction is recommended to be determined based on FEV1 values. Predicted FEV1 is an effort-dependent parameter, and postoperative pain may significantly limit patient effort. A predicted FEV1 value > 70% indicates mild restriction, 60–69% moderate restriction, 50–59% moderately severe restriction, 35–49% severe restriction, and < 35% very severe restriction.13 In our study, at postoperative hour 1, severe restriction was observed in the Group Control, whereas restriction was moderately severe in the Group Subcostal and moderate in the Group EOIPB. At postoperative hour 1, predicted FEV1 values were significantly higher in the Group EOIPB than in the Group Subcostal, and the reduction in predicted FEV1 was less pronounced in the Group EOIPB. At postoperative hour 6, moderate restriction was observed in both the Group Subcostal and Group EOIPB, while severe restriction persisted in the Group Control. At postoperative hour 24, moderate restriction continued in both block groups, whereas the Group Control demonstrated moderately severe restriction, with a significant difference between the Group Control and Group EOIPB. Throughout the first 24 postoperative hours, the reduction in predicted FEV1 was less pronounced in the block groups compared with the Group Control. These findings suggest that both EOIPB and subcostal TAP block reduce the severity of restrictive dysfunction for up to 24 hours following laparoscopic cholecystectomy. Moreover, the higher predicted FEV1 values observed in the EOIPB group at postoperative hour 1 suggest a less pronounced restrictive pattern during the early postoperative period. As no universally accepted MCID for postoperative spirometric parameters after laparoscopic cholecystectomy has been established, clinical relevance was interpreted based on the severity grading of restrictive dysfunction according to predicted FEV1 values per the Turkish Thoracic Society consensus report. The observed shift from severe restriction in the Group Control to moderate restriction in the block groups at postoperative hour 1 is considered clinically meaningful.
In laparoscopic cholecystectomy, the primary source of pain (50–70%) originates from the incision sites. Other contributors include pneumoperitoneum (20–30%) and gallbladder removal (10–20%).23 Bisgaard et al24 reported that somatic pain arising from incision sites is more prominent than visceral pain. Because pain following laparoscopic cholecystectomy is multifactorial, postoperative pain management should adopt a multimodal approach. Although opioids remain an important component of postoperative analgesia, their use is associated with several adverse effects, including nausea, vomiting, sedation, constipation, respiratory depression, and opioid-induced hyperalgesia.25,26 Therefore, reducing opioid requirements is an important goal of multimodal analgesia. In the present study, both EOIPB and subcostal TAP block significantly reduced postoperative tramadol consumption during the first 24 hours compared with the control group. Apart from lower tramadol consumption in the EOIPB group during the first postoperative hour, no significant differences were observed between the two block techniques. These findings indicate that both regional anesthesia techniques provided a comparable opioid-sparing effect.
In a study by Gerbershagen et al27 using NRS scores, a tolerable pain threshold was defined as an NRS score ≤ 4, whereas an NRS score ≥ 5 indicated the need for rescue analgesia. In a review by Soliz et al,28 the subcostal TAP block was reported to provide effective analgesia in major abdominal surgery. Similarly, Emile et al29 demonstrated that the subcostal TAP block significantly reduced postoperative pain after laparoscopic cholecystectomy, whereas Amin et al30 reported that EOIPB and subcostal TAP block provided comparable analgesia in supraumbilical surgery. Consistent with these findings, patients receiving either subcostal TAP block or EOIPB in our study maintained median resting and dynamic NRS scores ≤ 4 throughout the postoperative period, indicating effective analgesia for up to 24 hours. Both block groups demonstrated significantly lower pain scores than the control group, whereas no significant differences were observed between the two regional anesthesia techniques. Although a statistically significant difference was identified between the Subcostal and Control groups in dynamic NRS scores at postoperative hour 24, median NRS values remained within the clinically acceptable range in both groups. The lower opioid consumption observed in both block groups was consistent with the improved postoperative pain scores. Taken together, these findings suggest that both EOIPB and subcostal TAP block provide effective postoperative analgesia following laparoscopic cholecystectomy.
Emergence agitation (EA) is defined as the presence of agitation, confusion, disorientation, or aggressive behavior during the early phase of recovery from general anesthesia.31 It may result in harm to both patients and healthcare personnel and can increase hospital costs. Abdominal surgery and postoperative pain are recognized risk factors for EA. Card et al32 reported that increasing perioperative opioid doses are associated with a higher risk of delirium. Tolchard et al33 demonstrated that the subcostal TAP block reduces opioid consumption in the PACU and shortens the time to discharge from the PACU. In our study, when sedation and agitation levels were assessed using the RSS, no statistically significant differences were observed among the groups at any time point. However, in the Group Control where opioid consumption was significantly higher than in the block groups the median RSS value in the PACU was 1. The median RSS value also remained 1 at postoperative hours 1 and 2 in the Group Control. In contrast, the median RSS value was 2 in the block groups at all follow-up time points, including in the PACU. These findings suggest that patients in the Group Control were awake but restless and potentially agitated during the first two postoperative hours, whereas patients in the block groups were awake and calm. This observation was consistent with the NRS pain scores. Furthermore, the fact that median RSS values ranged between 1 and 2 in all groups at all postoperative time points indicates that postoperative assessments were performed while patients were awake and at comparable levels of sedation.
The QoR-15 questionnaire is a widely used, internationally validated, patient-centered measure of postoperative recovery. Korkusuz et al34 reported higher QoR-15 scores in patients who received bilateral EOIPB after laparoscopic cholecystectomy. In our study, higher total QoR-15 scores, as well as higher scores in the pain, physical comfort, physical independence, and emotional state subdomains, were observed in the Group EOIPB and Group Subcostal compared with the Group Control. These findings suggest that both EOIPB and subcostal TAP block may enhance recovery following laparoscopic cholecystectomy. The pain subdomain of the QoR-15 questionnaire is based on the severity of pain experienced during the preceding 24 hours. In our study, higher pain subdomain scores at postoperative hour 24 in the Group EOIPB and Group Subcostal compared with the Group Control indicate that patients receiving these blocks experienced less pain during the first 24 postoperative hours. This improvement in pain control may have positively influenced the other subdomains, thereby contributing to the overall enhancement of postoperative recovery observed in the Group EOIPB and Group Subcostal.
Limitations
This study has several limitations. First, pulmonary function was not evaluated beyond the first 24 postoperative hours. Given that respiratory dysfunction following upper abdominal surgery may persist for up to 10 days, the time required for pulmonary function to return to baseline values in our patient population was not assessed. Second, because the blocks were performed under general anesthesia, dermatomal sensory assessment could not be conducted. However, all blocks were performed under ultrasound guidance, and correct spread of the local anesthetic within the intended fascial plane was confirmed. Third, the time to first analgesic request was not recorded. Fourth, the efficacy of the blocks was not evaluated in patients with chronic pulmonary disease, particularly those with COPD, and therefore remains uncertain in this population. Furthermore, the exclusion of smokers and patients with a BMI >30 kg/m2, although intended to minimize confounding factors and ensure a more homogeneous study population, may limit the generalizability of our findings to these patient populations. Finally, the long-term effects of the blocks on quality of recovery were not evaluated. The time required for QoR-15 scores to return to baseline values was also not assessed. In addition, no sham block procedure was performed in the control group because of ethical concerns regarding an invasive placebo intervention. Therefore, subjective postoperative outcomes such as NRS pain scores and QoR-15 assessments may have been influenced by expectation bias. Furthermore, blinding of the anesthesiologist performing the block procedures was not feasible because of the nature of the intervention.
Conclusion
In this study, both ultrasound-guided subcostal TAP block and EOIPB were associated with improved postoperative pulmonary function, reduced opioid consumption, and enhanced early postoperative recovery following laparoscopic cholecystectomy. Both techniques were effective and safe for postoperative pain control and may therefore be considered as components of a multimodal analgesia regimen in this patient population.
Data Sharing Statement
Data is provided within the manuscript.
Ethics Approval and Consent to Participate
The study was performed in accordance with the declaration of Helsinki. Ethical approval from the Ethics Committee of the Zonguldak Bülent Ecevit University was obtained prior to initiation of the study (Protocol number: 2023/ 04-3). The patients were provided with a detailed explanation of the preoperative procedure, and verbal and written informed consent was obtained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare no competing interests.
References
1. Beaussier M, Genty T, Lescot T, Aissou M. Influence of pain on postoperative ventilatory disturbances: management and expected benefits. Ann Fr Anesth Reanim. 2014;33(9):484–14. doi:10.1016/j.annfar.2014.07.005
2. Do Nascimento Junior P, Módolo NS, Andrade S, Guimarães MM, Braz LG, El Dib R. Incentive spirometry for prevention of postoperative pulmonary complications in upper abdominal surgery. Cochrane Database Syst Rev. 2014;2014(2):CD006058. doi:10.1002/14651858.CD006058.pub3
3. Erice F, Fox GS, Salib YM, Romano E, Meakins JL, Magder SA. Diaphragmatic function before and after laparoscopic cholecystectomy. Anesthesiology. 1993;79(5):966–975. doi:10.1097/00000542-199311000-00015
4. Joris J, Thiry E, Paris P, Weerts J, Lamy M. Pain after laparoscopic cholecystectomy: characteristics and effect of intraperitoneal bupivacaine. Anesth Analg. 1995;81(2):379–384. doi:10.1097/00000539-199508000-00029
5. Basak F, Hasbahceci M, Sisik A, et al. Glisson’s capsule cauterisation is associated with increased postoperative pain after laparoscopic cholecystectomy: a prospective case-control study. Ann R Coll Surg Engl. 2017;99(6):485–489. doi:10.1308/rcsann.2017.0068
6. Jiang B, Ye S. Pharmacotherapeutic pain management in patients undergoing laparoscopic cholecystectomy: a review. Adv Clin Exp Med. 2022;31(9):1023–1033. doi:10.17219/acem/151995
7. Abdelhamid BM, Khaled D, Mansour MA, Hassan MM. Comparison between the ultrasound-guided erector spinae block and the subcostal approach to the transversus abdominis plane block in obese patients undergoing sleeve gastrectomy: a randomized controlled trial. Minerva Anestesiol. 2020;86(8):816–826. doi:10.23736/S0375-9393.20.14064-1
8. Rozen WM, Tran TMN, Ashton MW, Barrington MJ, Ivanusic JJ, Taylor GI. Refining the course of the thoracolumbar nerves: a new understanding of the innervation of the anterior abdominal wall. Clin Anat. 2008;21(4):325–333. doi:10.1002/ca.20621
9. Tsai HC, Yoshida T, Chuang TY, et al. Transversus abdominis plane block: an updated review of anatomy and techniques. Biomed Res Int. 2017;2017:8284363. doi:10.1155/2017/8284363
10. Hamilton DL, Manickam BP. Is a thoracic fascial plane block the answer to upper abdominal wall analgesia? Reg Anesth Pain Med. 2018;43(8):891–892. doi:10.1097/AAP.0000000000000838
11. Selvi O, Azizoglu M, Temel G, et al. Translation and validation of the Turkish version of the quality of postoperative recovery score QoR-15: a multi-centred cohort study. Turk J Anaesthesiol Reanim. 2022;50(6):443–448. doi:10.5152/TJAR.2022.21417
12. Kleif J, Waage J, Christensen KB, Gögenur I. Systematic review of the QoR-15 score, a patient-reported outcome measure measuring quality of recovery after surgery and anaesthesia. Br J Anaesth. 2018;120(1):28–36. doi:10.1016/j.bja.2017.11.013
13. Ulubay G, Dilektaşlı AG, Börekçi Ş, et al. Turkish Thoracic Society consensus report: interpretation of spirometry. Turk Thorac J. 2019;20(1):69–89. doi:10.5152/TurkThoracJ.2018.180175
14. Siafakas NM, Mitrouska I, Bouros D, Georgopoulos D. Surgery and the respiratory muscles. Thorax. 1999;54(5):458–465. doi:10.1136/thx.54.5.458
15. Rademaker BM, Ringers J, Odoom JA, De Wit LT, Kalkman CJ, Oosting J. Pulmonary function and stress response after laparoscopic cholecystectomy: comparison with subcostal incision and influence of thoracic epidural analgesia. Anesth Analg. 1992;75(3):381–385. doi:10.1213/00000539-199209000-00011
16. Keus F, Ahmed Ali U, Noordergraaf GJ, Roukema JA, Gooszen HG, Van Laarhoven CJHM. Laparoscopic vs small incision cholecystectomy: implications for pulmonary function and pain. A randomized clinical trial. Acta Anaesthesiol Scand. 2008;52(3):363–373. doi:10.1111/j.1399-6576.2007.01488.x
17. Staehr-Rye AK, Rasmussen LS, Rosenberg J, et al. Minimal impairment in pulmonary function following laparoscopic surgery. Acta Anaesthesiol Scand. 2014;58(2):198–205. doi:10.1111/aas.12254
18. Warner DO, Weiskopf R. Preventing postoperative pulmonary complications: the role of the anesthesiologist. Anesthesiology. 2000;92(5):1467–1472. doi:10.1097/00000542-200005000-00037
19. Lee SY, Ryu CG, Koo YH, et al. The effect of ultrasound-guided transversus abdominis plane block on pulmonary function in patients undergoing laparoscopic cholecystectomy: a prospective randomized study. Surg Endosc. 2022;36(10):7334–7342. doi:10.1007/s00464-022-09131-y
20. Gold WM, Koth LL. Pulmonary function testing. In: Broaddus VC, Mason RJ, Ernst JD, editors. Murray and Nadel’s Textbook of Respiratory Medicine.
21. Abe T, Kusuhara N, Yoshimura N, Tomita T, Easton PA. Differential respiratory activity of four abdominal muscles in humans. J Appl Physiol. 1996;80(4):1379–1389. doi:10.1152/jappl.1996.80.4.1379
22. Hendolin H, Lahtinen J, Länsimies E, Tuppurainen T, Partanen K. The effect of thoracic epidural analgesia on respiratory function after cholecystectomy. Acta Anaesthesiol Scand. 1987;31(7):645–651. doi:10.1111/j.1399-6576.1987.tb02637.x
23. Mitra S, Khandelwal P, Roberts K, Kumar S, Vadivelu N. Pain relief in laparoscopic cholecystectomy: a review of the current options. Pain Pract. 2012;12(6):485–496. doi:10.1111/j.1533-2500.2011.00513.x
24. Bisgaard T, Klarskov B, Rosenberg J, Kehlet H. Characteristics and prediction of early pain after laparoscopic cholecystectomy. Pain. 2001;90(3):261–269. doi:10.1016/S0304-3959(00)00406-1
25. Benyamin R, Trescot AM, Datta S, et al. Opioid complications and side effects. Pain Physician. 2008;11(2 Suppl):S105–S120. doi:10.36076/ppj.2008/11/S105
26. Colvin LA, Bull F, Hales TG. Perioperative opioid analgesia — when is enough too much? A review of opioid-induced tolerance and hyperalgesia. Lancet. 2019;393(10180):1558–1568. doi:10.1016/S0140-6736(19)30430-1
27. Gerbershagen HJ, Rothaug J, Kalkman CJ, Meissner W. Determination of moderate-to-severe postoperative pain on the numeric rating scale: a cut-off point analysis applying four different methods. Br J Anaesth. 2011;107(4):619–626. doi:10.1093/bja/aer195
28. Soliz JM, Lipski I, Hancher-Hodges S, Speer BB, Popat K. Subcostal transverse abdominis plane block for acute pain management: a review. Anesth Pain Med. 2017;7(5):e12923. doi:10.5812/aapm.12923
29. Emile SH, Elfeki H, Elbahrawy K, Sakr A, Shalaby M. Ultrasound-guided versus laparoscopic-guided subcostal transversus abdominis plane (TAP) block versus no TAP block in laparoscopic cholecystectomy: a randomized double-blind controlled trial. Int J Surg. 2022;101:106628. doi:10.1016/j.ijsu.2022.106639
30. Amin S, Khedr A, Elhadad M. External oblique intercostal plane block versus subcostal transversus abdominis plane block for pain control in supraumbilical surgeries: a randomised controlled clinical trial. South Afr J Anaesth Analg. 2024;30(1):22–28. doi:10.36303/SAJAA.3134
31. Vlajkovic GP, Sindjelic RP. Emergence delirium in children: many questions, few answers. Anesth Analg. 2007;104(1):84–91. doi:10.1213/01.ane.0000250914.91881.a8
32. Card E, Pandharipande P, Tomes C, et al. Emergence from general anaesthesia and evolution of delirium signs in the post-anaesthesia care unit. Br J Anaesth. 2015;115(3):411–417. doi:10.1093/bja/aeu442
33. Tolchard S, Davies R, Martindale S. Efficacy of the subcostal transversus abdominis plane block in laparoscopic cholecystectomy: comparison with conventional port-site infiltration. J Anaesthesiol Clin Pharmacol. 2012;28(3):339–343. doi:10.4103/0970-9185.98331
34. Korkusuz M, Basaran B, Et T, Bilge A, Yarimoglu R, Yildirim H. Bilateral external oblique intercostal plane block (EOIPB) in patients undergoing laparoscopic cholecystectomy. Saudi Med J. 2023;44(10):1037–1046. doi:10.15537/smj.2023.44.10.20230350
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.