Back to Journals » Journal of Pain Research » Volume 14
Effects of Different Local Analgesic Techniques on Postoperative Quality of Life and Pain in Patients Undergoing Total Hip Arthroplasty Under General Anesthesia: A Randomized Controlled Trial
Authors Yang R ![]() , Liu RH
, Liu RH ![]() , Xu JN
, Xu JN ![]() , Xu GH, Jin XB, Xiao R
, Xu GH, Jin XB, Xiao R ![]() , Mei B
, Mei B
Received 27 October 2020
Accepted for publication 30 December 2020
Published 24 February 2021 Volume 2021:14 Pages 527—536
DOI https://doi.org/10.2147/JPR.S289018
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert B. Raffa
Rui Yang,1 Rui-hong Liu,1 Jia-nan Xu,1 Guang-hong Xu,1,2 Xiao-bin Jin,1 Rui Xiao,1 Bin Mei1
1Department of Anesthesiology, First Affiliated Hospital, Anhui Medical University, Hefei, Anhui, 230022, People’s Republic of China; 2Department of Neurology, First Affiliated Hospital, Anhui Medical University, Hefei, Anhui, 230022, People’s Republic of China
Correspondence: Guang-hong Xu
Department of Anesthesiology, First Affiliated Hospital, Anhui Medical University, 218 Jixi Road, Hefei, Anhui, 230022, People’s Republic of China
Tel +86-551-62922344
Fax +86 551 62923704
Email [email protected]
Background: Both lumbosacral plexus block (LSPB) and local infiltration analgesia (LIA) can provide postoperative analgesia for patients undergoing total hip arthroplasty (THA). The current study aimed to compare the differences between LSPB and LIA on postoperative pain and quality of life (QoL) in THA patients.
Methods: A total of 117 patients aged 40– 80 years, ASA I-III, were prospectively randomized into two groups: a general anesthesia plus LSPB (Group LSPB) and a general anesthesia plus LIA (Group LIA). Pain intensity and opioid consumption were recorded Within 72 hours after surgery. QoL was measured by EQ-5D and EQ-VAS questionnaires, and the incidence of postoperative pain was measured as part of the EQ-5D on day 1, day 3, day 7, and month 1, month 3, and month 6 after surgery.
Results: EQ-5D scores: Mobility, Self-Care, Usual Activities, Pain/Discomfort, and Anxiety/Depression were higher in Group LSPB versus Group LIA throughout six-month follow-ups (p = 0.039). The pain intensity was lower in Group LSPB than in Group LIA 0– 12 h after surgery (2.41 vs 2.79, p = 0.01), but was higher in Group LSPB than in Group LIA 12– 24 h (2.59 vs 2.05, p = 0.02) and 24– 48 h (2.18 vs 1.73, p = 0.02) after surgery. There were no differences in opioid consumption between the groups during the first 72 postoperative hours. In the first month after surgery, more patients in Group LSPB than in Group LIA had no pain (52 vs 40, p = 0.04).
Conclusion: Both LSPB and LIA can provide satisfactory postoperative analgesia. The LSPB is better than LIA for long-term QoL in THA patients undergoing general anesthesia.
Clinical Trial Registration Number: The Chinese Clinical Trial Registry (ChiCTR-INR-17012545).
Keywords: total hip arthroplasty, lumbosacral plexus block, local infiltration analgesia, postoperative pain, quality of life
Introduction
Total hip arthroplasty (THA) is the most common procedure used to relieve pain, improve joint function and quality of life (QoL) in patients with hip arthropathy.1 More than one million THA procedures are performed annually in the United States, and that number is projected to increase substantially in the coming decades.2 Such a high number of surgical patients warrants greater concern for long-term QoL after surgery, including postoperative and perioperative pain.
In recent years, with the development of ultrasound visualization technology, lumbosacral plexus block (LSPB) is widely used for THA because it reduces the use of opioids, reduces the occurrence of acute pain, promotes early mobilization, and shortens the length of the hospital stay.3,4 However, the LSPB can also lead to several complications such as hematoma or local anesthetic systemic toxicity or accidental neuraxial injections or spread.5,6 Ultrasound guidance was reported to decrease the incidence of these complications.7 Local infiltration analgesia (LIA) is a new analgesic method for patients undergoing THA. Kuchalik et al showed that LIA could alleviate postoperative pain and reduce opioid consumption.8 However, the effect of LSPB on long-term QoL and postoperative pain for patients undergoing THA compared with LIA remains unknown. In this prospective, randomized, single-blind controlled trial, we investigated the long-term QoL of LSPB versus LIA. Besides, the numeric rating scale (NRS) for pain, opioid consumption, and incidence of postoperative nausea and vomiting (PONV) were recorded during the first 72 postoperative hours.
Patients and Methods
The trial was registered before patient enrollment at the Chinese Clinical Trail Registry (ChiCTR-INR-17012545). Ethical approval for this study was provided by the Ethical Committee of our hospital (PJ2018-07-17). All patients provided written consent to participate in this study.
A total of 167 patients undergo elective THA, aged 40–80 years, ASA I-III were screened, and 117 patients completed the study; the Consolidated Standards of Reporting Trials (CONSORT) diagram is shown (Figure 1). The patients eligible for the study were American Society of Anesthesiologists physical class < 4. Exclusion criteria were contraindications to LSPB, such as coagulopathy, infection at the puncture site, preoperative cognitive impairment, a mental or language barrier, regular opioid, alcohol, or drug abuse, and any condition that the investigator determined would adversely affect the study. A computer-generated allocation program randomly assigned the patients to Group LSPB and Group LIA. Group assignments were concealed in opaque envelopes until after consent had been obtained. The postoperative observers were blind to the group allocations.
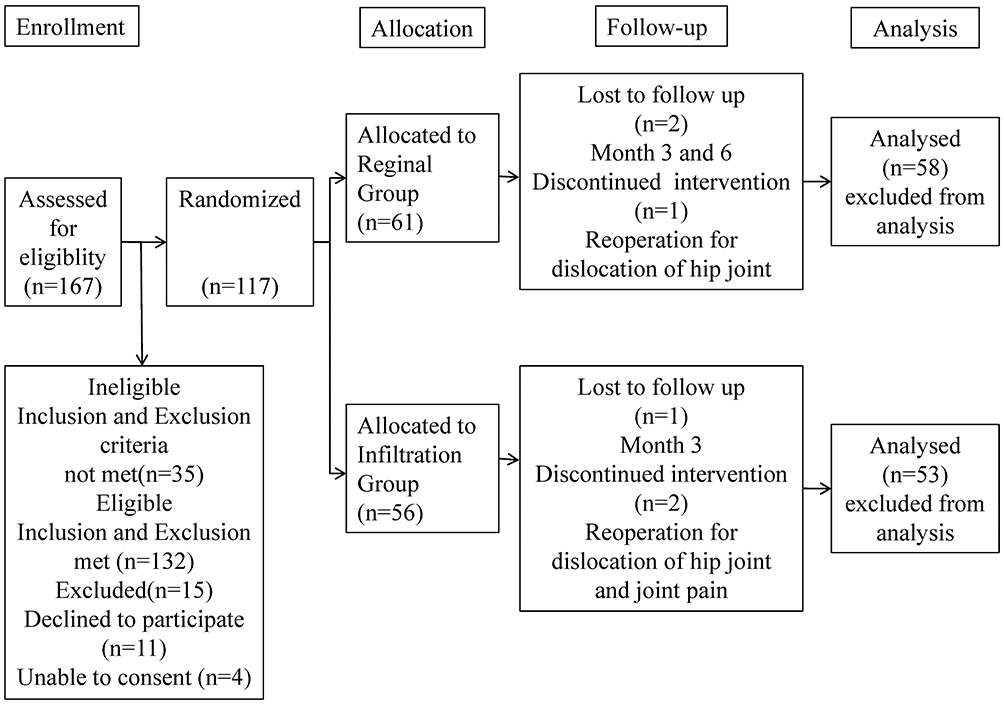 |
Figure 1 The CONSORT flowchart. |
Study Protocol
Once the patients were transferred to the operation room, they were infused venously with 5 mL/kg Lactated Ringer’s Solution, and oxygen was administered immediately at 4 L/min using a face mask. Standard monitoring included continuous oxygen saturation, pulse oximetry, five-lead ECG, and non-invasive arterial blood pressure measurements at 5 min intervals. In addition, bispectral index monitoring (BIS; Vista, Aspect Medical System Inc., USA) was used to adjust the depth of anesthesia. The target BIS value was set at 40–60. Patients were randomly divided into Group LSPB and Group LIA.
Group LSPB patients received LSPB before the induction of General anesthesia (GA). The patient maintained a lateral position such that the surgical limb was uppermost. An intravenous sufentanil bolus (5–10 μg) was given to decrease anxiety and discomfort while keeping in touch with the patient during the LSPB procedure. Both nerve stimulator and ultrasound were used to ensure the accuracy of blocking and avoid nerve injury. A 2–5 MHz curved array transducer (M-Turbo, FUJIFILM Sonosite Inc., USA), an electrically isolated 12-cm 22G needle (Stimuplex D, B. Braun Medical Inc., Germany), and a nerve stimulator (Stimuplex HNS 12, B. Braun Medical Inc., Germany) were used for the LSPB procedure. As described previously for the lumbar plexus block,9 the ultrasound transducer was placed adjacent to the spine longitudinally at the second to third lumbar level (Supplementary Material Figure 1). The needle was inserted continuously using the in-plane technique until the lumbar plexus was stimulated. As for the sacral plexus block,10 the transducer was aligned between the posterior superior iliac spine and the midpoint of the line connecting the posterior superior iliac spine and the greater trochanter (Supplementary Material Figure 2). A continuous high-echo image was visible by ultrasound, and the sacral plexus was identified as the elliptical structure between the sacrum and the iliac bone. The needle was inserted in a similar manner. Stimulation was initially assessed at an intensity of 1.5 mA for 50 μs with a frequency of 2 Hz. The lumbar plexus was identified with the motor response of the femoral quadriceps muscle. The sacral plexus was identified with the motor responses of the gluteus maximus and gastrocnemius. The intensity of the current was gradually reduced while observing the motor response, and the final position of the needle was based on the best response to stimulation, which was between 0.5–0.35 mA, to provide a valid block and to avoid nerve injury. As a deep nerve block, a test dose of 2 mL of 0.5% ropivacaine was injected, when the test dose was observed spreading around the nerve plexus on ultrasound and the twitch disappeared. The remaining drugs were injected in 5 mL aliquots with repeated aspiration, 25mL and 15mL 0.5% ropivacaine were administrated for lumbar plexus and sacral plexus block, respectively. The block procedure was performed by an anesthesiologist with over five years of experience with regional anesthesia. The effectiveness of the block was checked by an assistant at 10 minutes after block procedure completion. A diminished or absent sensation of the pinprick test was considered as block success. Patients with failed nerve block received GA and withdrew from the study. All blocks were successful for the patients in Groups LSPB.
General anesthesia was a total intravenous technique with propofol and remifentanil. After the administration of propofol (1.5–2.5 mg/kg), sufentanil (0.3–0.5 μg/kg), and cis-atracurium (0.15–0.2 mg/kg) during anesthesia induction, a laryngeal mask airway was inserted after 3min. The lungs were ventilated and were adjusted to keep the end-tidal CO2 between 35–45 mmHg. In Group LIA, Propofol (target-controlled infusion: 1.0–4 μg/mL) and remifentanil were used to maintain anesthesia. In Group LSPB, propofol (target-controlled infusion: 1.0–4 μg/mL) was used to maintain anesthesia. In both groups, the propofol infusion rates were adjusted according to the target BIS range. An increase in MAP and/or HR 20% above preinduction baseline values for at least 1 min was considered inadequate analgesia and was treated with an infusion of sufentanil by bolus (5–10ug). If symptoms were not relieved, remifentanil infusion was initiated in Group LSPB and increased in Group LIA (max 0.35 μg.kg- 1.min-1)
Before the closure of the posterior soft-tissue flap, Group LIA patients received the LIA block by the surgeon. A total volume of 40 mL of 0.5% ropivacaine was infiltrated.11 Half of the ropivacaine was carefully and evenly infiltrated into the periosteum of the femoral neck, the hip capsule, and the trochanteric bursa at multiple points in the area. Care was taken to avoid infiltration of the soft tissue surrounding the sciatic nerve. The remaining ropivacaine was infiltrated into the surface tissue of the iliotibial fascia and subcutaneous fat similarly.
Predefined complications were managed according to the study protocol: for hypotension (systolic blood pressure < 90 mmHg, or 20% less than the baseline), an intravenous bolus of 3–6 mg of ephedrine was given, and the infusion rate of the Lactated Ringer’s Solution was increased; for bradycardia (heart rate < 50 beats per minute), an intravenous bolus of 0.2–0.5 mg of atropine was given. Propofol and remifentanil infusion were discontinued at the end of the operation. Flurbiprofen axetil (50 mg) was given intravenously before incisions and the end of surgery, and sufentanil (5–10 μg) was given at the end of surgery in two groups. Azastron (10 mg) was infused intravenously to prevent PONV.
After the surgery, patients recovered in the post-anesthesia care unit. When the NRS score was > 3, the pain was treated with IV flurbiprofen axetil (50mg). If NRS remained ≥ 3 at 5 minutes after receiving flurbiprofen axetil. Then sufentanil 0.1 μg/kg was given intravenous for a maximum dose of 10 μg. During this period, a blind observer monitored the patient for signs of respiratory depression and evaluated the patient’s NRS every ten minutes. Once the patients were transferred to the orthopedic ward, patients routinely received a standard postoperative regimen of celecoxib 100–200 mg and tramadol 50–100 mg every 12h for three days. A single rescue dose of tramadol (50–100mg) or oxycodone (5–10 mg) was used in the ward.
Outcome Measures
Our primary outcome measures were QoL scores, which were assessed using the EQ-5D. The EQ-5D questionnaire is a generic instrument for describing and evaluating health based on a descriptive system that defines health in terms of five dimensions: Mobility, Self-Care, Usual Activities, Pain/Discomfort, and Anxiety/Depression.12 Each dimension has three response categories: no problems (score of 1), some problems (score of 2), and extreme problems (score of 3). Researchers usually add a “global” score to describe health outcomes, which is determined by the time trade-off method. The utility values for EQ-5D health states are determined using the time trade-off method from the general population, this study was conducted in China, and Chinese utility values for EQ-5D has been established.13 Patients also rate their current overall health status on the day of the interview using a vertical visual analog scale (EQ-VAS) in which 0 is the worst score and 100 is the best score. The EQ-5D and EQ-VAS scores were measured two days before surgery and 1, 3, and 7 days post-surgery (DPS) and at 1, 3, and 6 months post-surgery (MPS).
Secondary outcome measures were the NRS score, the cumulative consumption of postoperative oral morphine equivalents,14 and the incidence of PONV in the first 72 h postoperatively. The consumption of intraoperative general anesthetics, the length of hospital stay, the incidence of postoperative delirium (POD), postoperative cognitive dysfunction (POCD), and postoperative pain were also recorded. POD was assessed in the first three DPS by the Confusion Assessment Method. POCD was assessed 1, 3, and 7 DPS and 1, 3, and 6 MPS using the Postoperative Quality of Recovery Scale.15 The incidence of postoperative pain was assessed as part of the EQ-5D up to 6 MPS.
Effect size (ES) was calculated as the difference between the mean scores for chosen time intervals divided by the standard deviation of the score for the previous (or former) time interval.16 This method allowed for a direct comparison of the extent of change determined by two instruments by standardizing the change measured by an instrument. A large ES value indicates a large change.
Baseline data and data from the in-patient stay were collected face-to-face, whereas measurements after hospital discharge were collected via phone. Baseline was defined as the first set of recorded data after participant consent.
Statistical Analysis
We assumed the pre-operation to 6-months post-operation intra-patient survey correlation to be 0.60 (moderate correlation) and cross-sectional EQ-5D scores to have a standard deviation of 0.15, which was calculated from a pilot study of 30 patients randomized to the LSPB or LIA group. A minimally clinical important difference (MCID) is defined as a change or difference in the outcome measure that would be perceived as essential and beneficial by the clinician or the patient.17 The MCID for the EQ-5D was reported to be 0.074.18 A sample size of 49 patients in each group provided 85% power with a two-sided α of 5% to detect a 0.074 point difference in the mean scores between two groups at any time points. We adopted a conservative approach and increased the sample size to 55 per group in case of potential missing visits.
Continuous variables were expressed as mean and variance and analyzed using an independent samples t-test if conformed to the normal distribution, otherwise expressed as median and range, and analyzed with Mann–Whitney U-tests. Categorical variables expressed as percentages or numbers and analyzed by Pearson’s Chi-square tests or Fisher’s exact test. Two-way ANOVA repeated measures were implemented to test the differences in the EQ-5D and EQ-VAS scores between the groups. The significance level for all statistical tests was set at P < 0.05. All statistical analyses were done using SPSS version 16.
Results
From October 2019 to August 2020, of the 167 patients who were screened for the study, 50 of the patients were excluded; 35 failed to meet the inclusion criteria, 11 refused to participate, 4 were unable to consent. In Group LSPB, 2 patients were lost to follow-up at 3 and 6 MPS. In Group LIA, 1 patient was lost to follow up at 3 MPS, 1 patient underwent hip revision surgery. One patient in Group LSPB and the third patient in Group LIA underwent surgery for dislocation of the hip prosthesis. A total of 111 patients were included in the final analysis (Figure 1). Baseline characteristics did not differ between the groups (Table 1).
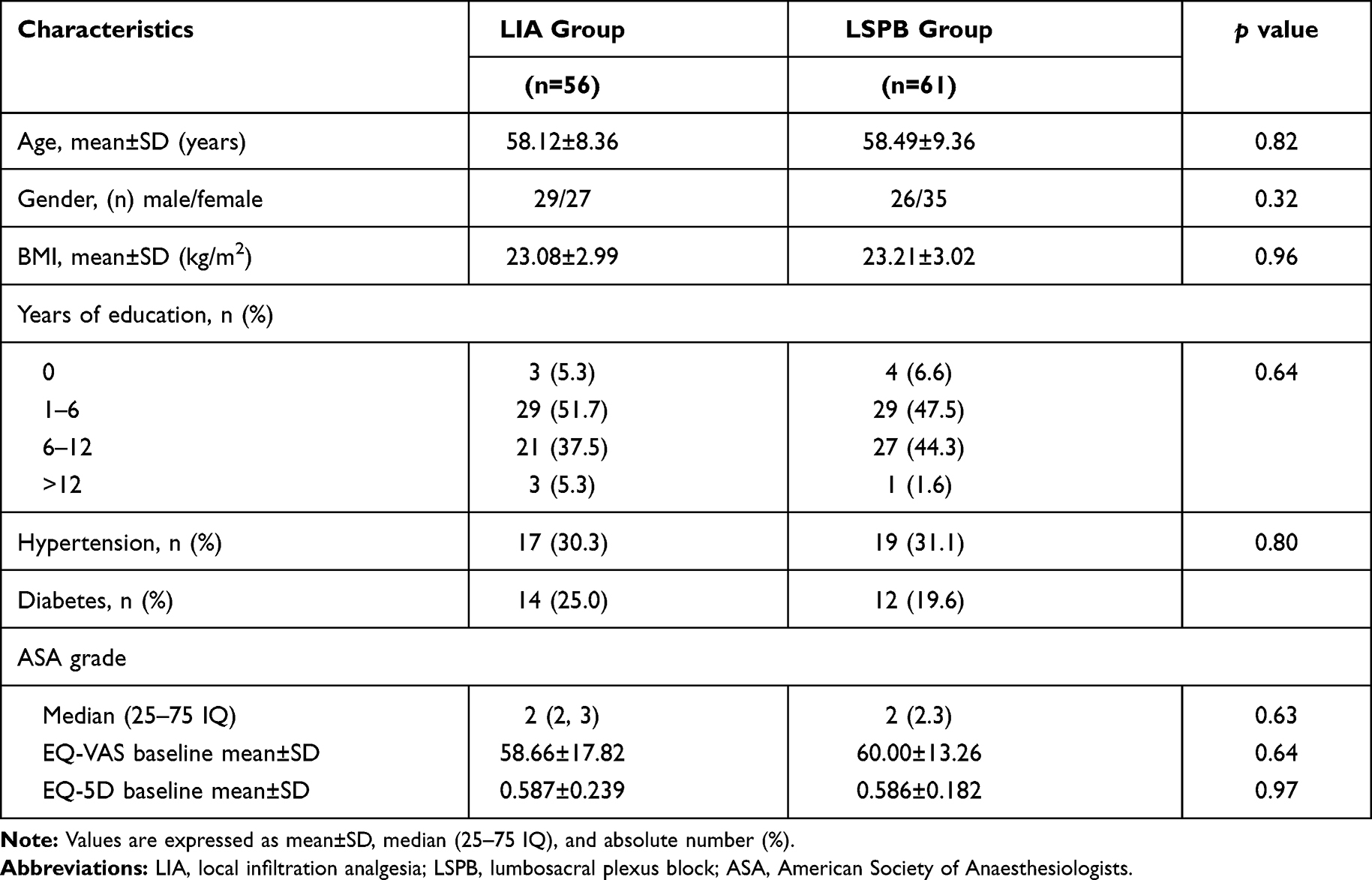 |
Table 1 Preoperative Data for Two Anesthetic Groups |
Health-Related QoL
During the postoperative follow-ups, the EQ-5D scores continuously increased in both groups. The EQ-5D scores peaked at the last assessment (6 months), with values of 0.882 and 0.950 for the LIA and LSPB groups, respectively. Generally, the EQ-5D scores were higher for Group LSPB than Group LIA (p = 0.039; Table 2). Similarly, the EQ-VAS scores increased at all follow-ups and peaked at the last assessment (6 months) with values of 77.4 and 85.7 for the LIA and LSPB groups, respectively. Generally, the EQ-VAS score was higher for Group LSPB than Group LIA (p = 0.047; Table 2).
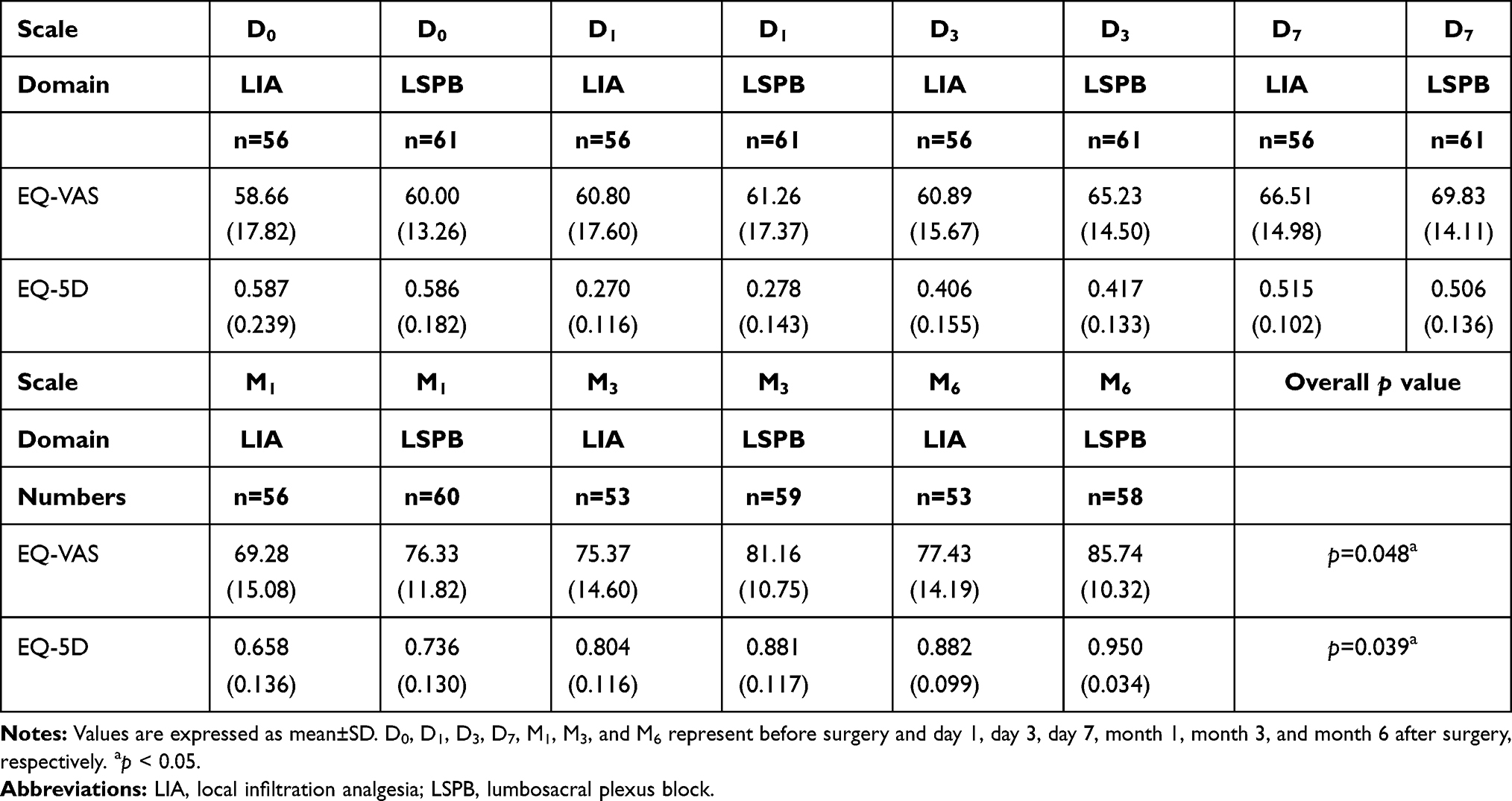 |
Table 2 The EQ-VAS and EQ-5D Score Changes Over Time |
The ES calculations showed that changes in EQ-5D scores were greatest between day 7 and month 1 in both groups. Similarly, changes in EQ-VAS scores were greatest between day 7 and month 1 in Group LSPB and between month 1 and month 3 in Group LIA. (Table 3)
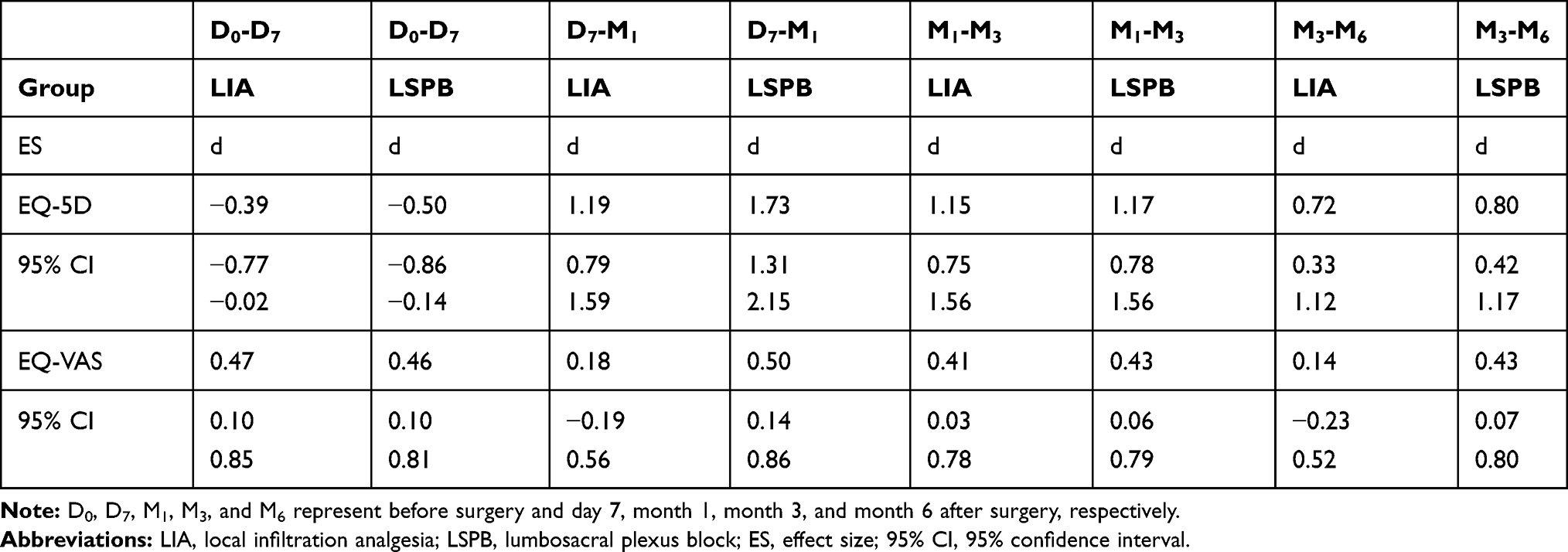 |
Table 3 ES of Changes in Health-Related QoL Scores for Patients at Different Time Intervals |
The Pain/Discomfort parts of the EQ-5D questionnaire were calculated separately to discover differences between the groups (Table 4). There was no difference in pain/discomfort between the groups except at 1 DPS and MPS. In Group LSPB more patients had severe problems than in Group LIA at 1 DPS (18 vs 12, p = 0.01). More patients at 1 MPS in Group LSPB had no problems than in Group LIA (52 vs 40, p = 0.04).
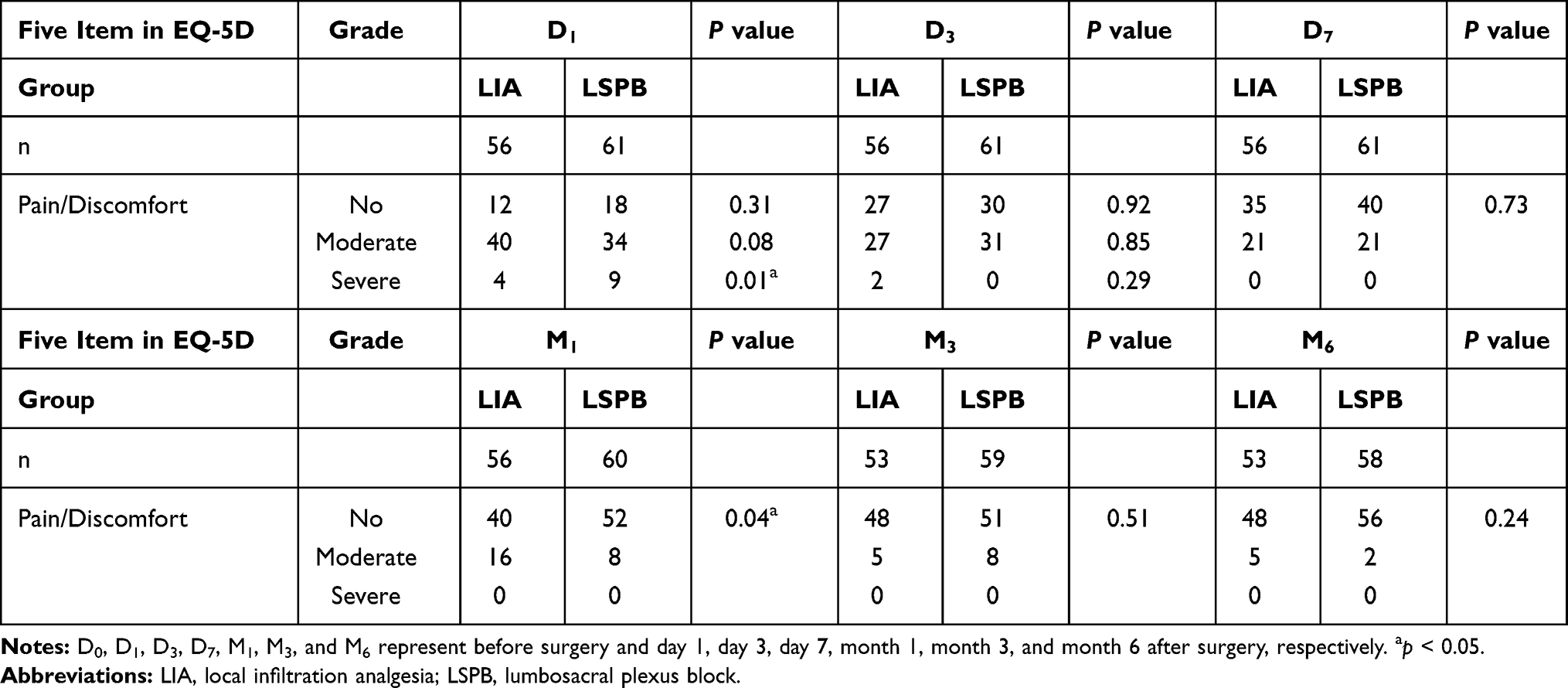 |
Table 4 The Mobility and Pain/Discomfort Dimensions of the EQ-5D Were Analyzed for the Two Groups |
Differences were found in postoperative pain scores between the two groups. The pain intensity was lower in Group LSPB than in Group LIA 0–12 h after surgery (2.41 vs 2.79, p = 0.01), but was higher in Group LSPB than in Group LIA 12–24 h (2.59 vs 2.05, p = 0.02) and 24–48 h (2.18 vs 1.73, p = 0.02) after surgery. (Table 5)
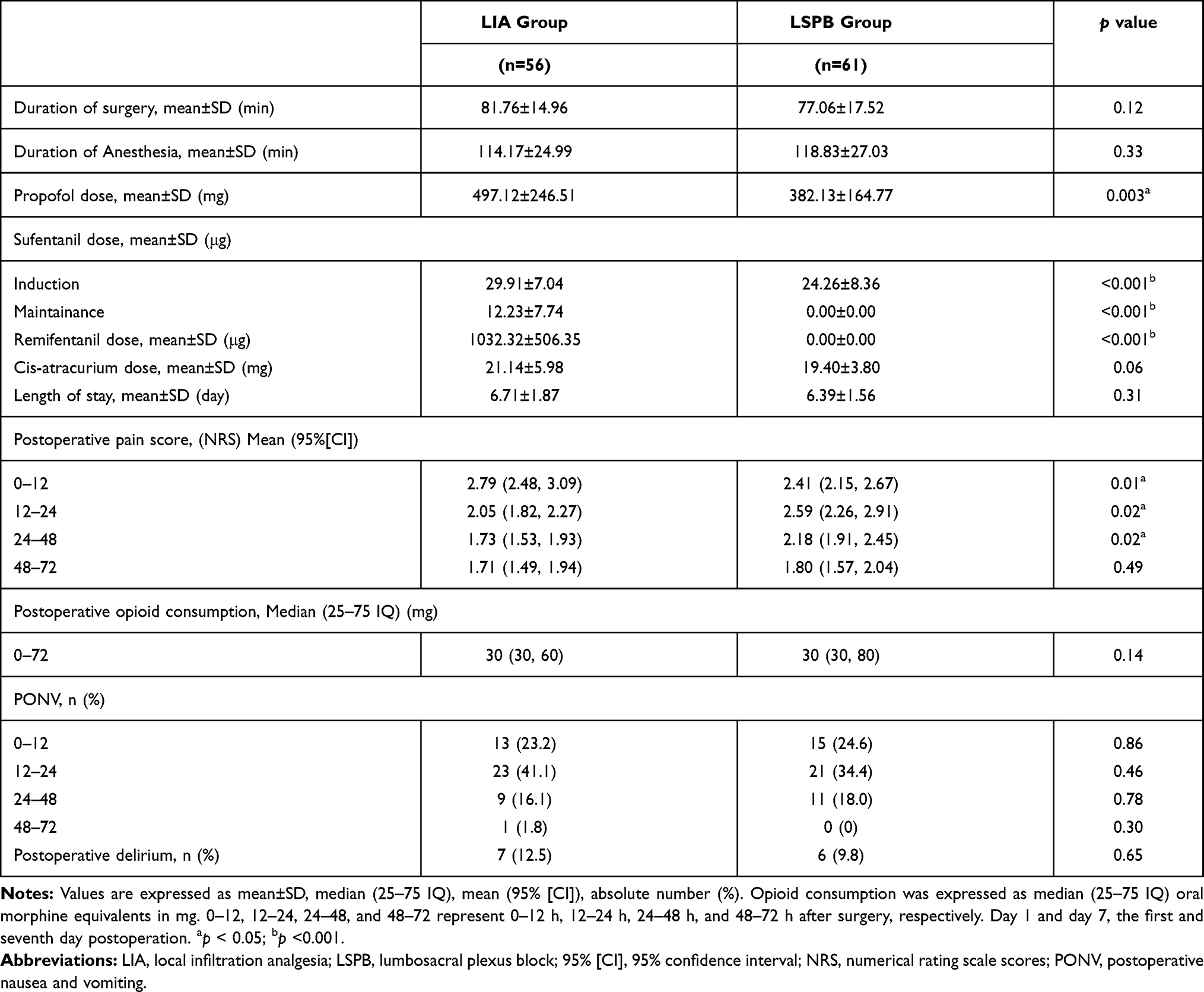 |
Table 5 Intraoperative and Postoperative Data for the Two Groups During Hospitalization |
Discussion
In this study, we found that patients who received LSPB preoperatively were associated with higher QoL scores during the six-month follow-ups, especially at 1 MPS. Fewer patients in Group LSPB than in Group LIA reported pain at 1 MPS.
Our results showed that Group LSPB patients had lower NRS scores than Group LIA patients within 12 h postoperatively. However, the NRS scores were higher for patients in Group LSPB than in Group LIA during the 12–24 h and 24–48 h postoperatively. One possible factor contributing to these findings may be that the LSPB produces excellent postoperative analgesia after surgery. When LSPB analgesia gradually wears off over time, the patient’s pain increased from painless state to painful state. The patients easily felt that the pain was suddenly appeared and aggravated with analgesia gradually wears off over time in group LSPB. So some patients might be more likely to rate it as “pain increased” and to feel that such pain is “not normal”.19
As we know, nerve block prevents the noxious stimuli from the wound to reach and to sensitize the central nervous system (central sensitization). Central sensitization plays a significant role in the occurrence of postoperative chronic pain. Musculoskeletal trauma from surgery causes local and systemic inflammatory reactions. Tissue injury and local inflammation induce hyperalgesia to subsequent noxious stimuli. Nerve block also modulates the inflammatory responses to reduce the incidence of hyperalgesia.20 Our results also showed that LSPB could effectively inhibit noxious stimulation in group LSPB, and only propofol, no extra sufentanil or remifentanil, was needed during the maintenance of anesthesia. NRS scores were lower for patients in Group LSPB than in Group LIA 12 h postoperatively, and fewer patients in Group LSPB than in Group LIA reported postoperative pain at 1 MPS. Patients received LSPB to provide complete intraoperative analgesia, the occurrence of central sensitization during surgery was minimized.21 However, patients received LIA near the end of surgery, which might be unable to effectively block central nociceptive input or prevent sensitization. Thus the incidence of postoperative chronic pain was higher in Group LIA than in group LSPB at 1MPS.
The overall EQ-5D scores were higher in Group LSPB, which meant that health in terms of five dimensions: Mobility, Self-Care, Usual Activities, Pain/Discomfort, Anxiety/Depression were higher in Group LSPB than in Group LIA. The MCID for the EQ-5D was reported to be 0.074,14 thus, the QoL of patients in Group LSPB was higher than that in Group LIA at 1 and 3 MPS, and it had clinical significance. Pain is one of the significant recovery predictors for THA patients.22 Lower incidence of postoperative pain for Group LSPB explains the greater improvement of QoL in Group LSPB at 1MPS. A study that compared LIA with femoral nerve block for THA patients showed that LIA was superior in reducing pain intensity and analgesic consumption than the femoral nerve block and no differences were observed in the QoL at 6 MPS.8 In this study, unlike in our study, all of the patients received spinal anesthesia and the analgesic effect of femoral nerve block was not as good as that of LSPB. Moreover, patients in Group LIA were administered a second local infiltration 23 h after the first injection. Group LIA patients received two injections with larger doses of local anesthetic, and the opioid sparing effect of nerve block during surgery was less detectable.
Lin et al showed that patients systematically self-rated their health lower using the EQ-VAS compared to the EQ-5D index.23 In our study, the P value of EQ-VAS (P=0.047) is close to 0.05, which may not reach significance after multiplicity adjustment, but EQ-VAS is only used as a supplement to EQ-5D. The ES calculations showed the peak ES value for the EQ-VAS was delayed when compared with the peak ES value for the EQ-5D in Group LIA, whereas in Group LSPB, the peak ES values for the EQ-VAS and EQ-5D occurred simultaneously. The EQ-VAS captured information on how patients feel about their health before and after surgery, and the EQ-5D questionnaire covered only five dimensions: Mobility, Self-Care, Usual Activities, Pain/Discomfort, and Anxiety/Depression. Cognitive impairment occurs frequently and affects patient QoL after THA. The incidence of POD and POCD was comparable between the groups at all follow-ups. Thus the differences between the EQ-VAS and EQ-5D could not be attributed to cognitive impairment. As an essential complement to the EQ-5D index, the EQ-VAS results indicated that patients must report relatively larger improvements in QoL (according to the EQ-5D Index) to rate their general health status (EQ-VAS) as improved. Patients in Group LSPB achieved a greater improvement in health (larger EQ-5D ES value) between day 7–month 1 after surgery, resulting in an earlier ES peak in EQ-VAS scores compared with Group LIA.
A potential limitation of the current study was the power of our study is only 85%, which may not be strong enough to detect the difference in the quality of life between the two groups. Second, our research shows that LSPB is better than LIA in improving the quality of life of patients after THA. However, there are still some factors that affect the quality of life of patients after surgery that are not included in our study, so we should carefully interpret our results. Third, our evaluation of patients was limited to 6 MPS. A longer follow-up is needed to observe the differences between the groups. Because population aging, younger age at surgery, and increased life expectancy, it is necessary to evaluate long-term QoLs after operations.
Conclusion
For patients undergoing THA under GA, within 72 h postoperatively, LIA can provide an analgesic effect no less than LSPB. The LSPB reduces the incidence of postoperative pain at 1 MPS, and improves the postoperative QoL, especially at 1 MPS.
Implication Statement
This article is an original work, has not been published before and is not being considered for publication elsewhere in its final form either in printed or electronic form.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request in five years.
Ethical Adherence
Ethical approval was provided by the Ethical Committee Anhui Medical University, Hefei, Anhui, China. All patients provided informed consent and all procedures were conducted according to the Declaration of Helsinki.
Acknowledgments
This research was supported by the National Nature Science Foundation of China (Grant No. 81870837) and the natural science research project of Anhui institution of higher learning, Anhui Provincial Education Department, China, No. KJ2018A0189. The funders had no role in the design, execution, and writing up of the study.
Author Contributions
Rui Yang: Conceptualization, Methodology, Software, Writing, Reviewing and Editing. Rui-hong Liu: Conceptualization, Writing Original Draft, Data Curation. Jia-nan Xu: Conceptualization, Resources, Writing Original draft. Guang-hong Xu: Conceptualization, Methodology, Supervision, Project administration, Writing, Reviewing and Editing. Xiao-bin Jin: Formal analysis, Validation, Project administration Writing Original Draft. Rui Xiao: Conceptualization, Investigation, Visualization, Writing Original Draft. Bin Mei: Conceptualization, Project administration, Investigation, Writing Original Draft.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the National Nature Science Foundation of China (Grant No. 81870837) and the natural science research project of Anhui institution of higher learning, Anhui Provincial Education Department, China, No. KJ2018A0189.
Disclosure
None of the authors have any conflicts of interest.
References
1. Koutras C, Antoniou SA, Talias MA, et al. Impact of total hip resurfacing arthroplasty on health-related quality of life measures: a systematic review and meta-analysis. J Arthroplasty. 2015;30(11):1938–1952. doi:10.1016/j.arth.2015.05.014
2. Sloan M, Premkumar A, Sheth NP. Projected volume of primary total joint arthroplasty in the U.S. 2014 to 2030. J Bone Joint Surg Am. 2018;100(17):1455–1460. doi:10.2106/JBJS.17.01617
3. de Visme V, Picart F, Le Jouan R, et al. Combined lumbar and sacral plexus block compared with plain bupivacaine spinal anesthesia for hip fractures in the elderly. Reg Anesth Pain Med. 2000;25(2):158–162. doi:10.1097/00115550-200003000-00005
4. Guay J, Parker MJ, Griffiths R, et al. Peripheral nerve blocks for hip fractures: a cochrane review. Anesth Analg. 2018;126(5):1695–1704. doi:10.1213/ANE.0000000000002489
5. Gadsden JC, Lindenmuth DM, Hadzic A, et al. Lumbar plexus block using high-pressure injection leads to contralateral and epidural spread. Anesthesiology. 2008;109(4):683–688. doi:10.1097/ALN.0b013e31818631a7
6. Aveline C, Bonnet F. Delayed retroperitoneal haematoma after failed lumbar plexus block. Br J Anaesth. 2004;93(4):589–591. doi:10.1093/bja/aeh242
7. Marhofer P, Harrop-Griffiths W, Willschke H, et al. Fifteen years of ultrasound guidance in regional anaesthesia: part 2-recent developments in block techniques. Br J Anaesth. 2010;104(6):673–683. doi:10.1093/bja/aeq086
8. Kuchálik J, Magnuson A, Lundin A, et al. Local infiltration analgesia or femoral nerve block for postoperative pain management in patients undergoing total hip arthroplasty. A randomized, double-blind study. Scand J Pain. 2017;16(1):223–230. doi:10.1016/j.sjpain.2017.05.002
9. Karmakar MK, Li JW, Kwok WH, et al. Sonoanatomy relevant for lumbar plexus block in volunteers correlated with cross-sectional anatomic and magnetic resonance images. Reg Anesth Pain Med. 2013;38(5):391–397. doi:10.1097/AAP.0b013e31829e52cc
10. Bendtsen TF, Lönnqvist PA, Jepsen KV, et al. Preliminary results of a new ultrasound-guided approach to block the sacral plexus: the parasacral parallel shift. Br J Anaesth. 2011;107(2):278–280. doi:10.1093/bja/aer216
11. Johnson RL, Amundson AW, Abdel MP, et al. Continuous posterior lumbar plexus nerve block versus periarticular injection with ropivacaine or liposomal bupivacaine for total hip arthroplasty: a three-arm randomized clinical trial. J Bone Joint Surg Am. 2017;99(21):1836–1845. doi:10.2106/JBJS.16.01305
12. Janssen MF, Szende A, Cabases J, et al. Population norms for the EQ-5D-3L: a cross-country analysis of population surveys for 20 countries. Eur J Health Econ. 2019;20(2):205–216. doi:10.1007/s10198-018-0955-5
13. Liu GG, Wu H, Li M, et al. Chinese time trade-off values for EQ-5D health states. Value Health. Value Health. 2014;17(5):597–604. doi:10.1016/j.jval.2014.05.007
14. Nielsen S, Degenhardt L, Hoban B, et al. A synthesis of oral morphine equivalents (OME) for opioid utilisation studies. Pharmacoepidemiol Drug Saf. 2016;25(6):733–737. doi:10.1002/pds.3945
15. Royse CF, Newman S, Williams Z, et al. A human volunteer study to identify variability in performance in the cognitive domain of the postoperative quality of recovery scale. Anesthesiology. 2013;119(3):576–581. doi:10.1097/ALN.0b013e318299f72b
16. Kazis LE, Anderson JJ, Meenan RF. Effect sizes for interpreting changes in health status. Med Care. 1989;27(3Suppl):S178–S89. doi:10.1097/00005650-198903001-00015
17. Guyatt GH, Osoba D, Wu AW, et al.; Clinical Significance Consensus Meeting Group. Methods to explain the clinical significance of health status measures. Mayo Clin Proc. 2002;77(4):371–383. doi:10.4065/77.4.371.
18. Walters SJ, Brazier JE. Comparison of the minimally important difference for two health state utility measures: EQ-5D and SF-6D. Qual Life Res. 2005;14(6):1523–1532. doi:10.1007/s11136-004-7713-0
19. Sunderland S, Yarnold CH, Head SJ, et al. Regional versus general anesthesia and the incidence of unplanned health care resource utilization for postoperative pain after wrist fracture surgery: results from a retrospective quality improvement project. Reg Anesth Pain Med. 2016;41(1):22–27. doi:10.1097/AAP.0000000000000325
20. Carvalho B, Aleshi P, Horstman DJ, et al. Effect of a preemptive femoral nerve block on cytokine release and hyperalgesia in experimentally inflamed skin of human volunteers. Reg Anesth Pain Med. 2010;35(6):514–519. doi:10.1097/AAP.0b013e3181faa107
21. Rivat C, Bollag L, Richebé P. Mechanisms of regional anaesthesia protection against hyperalgesia and pain chronicization. Curr Opin Anaesthesiol. 2013;26(5):621–625. doi:10.1097/01.aco.0000432511.08070.de
22. McHugh GA, Campbell M, Luker KA. Predictors of outcomes of recovery following total hip replacement surgery: a prospective study. Bone Joint Res. 2013;2(11):248–254. doi:10.1302/2046-3758.211.2000206
23. Lin FJ, Samp J, Munoz A, et al. Evaluating change using patient-reported outcome measures in knee replacement: the complementary nature of the EQ-5D index and VAS scores. Eur J Health Econ. 2014;15(5):489–496. doi:10.1007/s10198-013-0489-9
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.