Back to Journals » Drug Design, Development and Therapy » Volume 16
Effects of Dexmedetomidine Administered Through Different Routes on Kidney Tissue in Rats with Spinal Cord Ischaemia–Reperfusion Injury
Authors Şengel N, Köksal Z ![]() , Dursun AD
, Dursun AD ![]() , Kurtipek Ö, Sezen ŞC
, Kurtipek Ö, Sezen ŞC ![]() , Arslan M
, Arslan M ![]() , Kavutçu M
, Kavutçu M
Received 14 February 2022
Accepted for publication 2 July 2022
Published 13 July 2022 Volume 2022:16 Pages 2229—2239
DOI https://doi.org/10.2147/DDDT.S361618
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Necmiye Şengel,1 Zeynep Köksal,2 Ali Doğan Dursun,3 Ömer Kurtipek,2 Şaban Cem Sezen,4 Mustafa Arslan,2 Mustafa Kavutçu5
1Department of Oral and Maxillofacial Surgery, Gazi University Faculty of Dentistry, Ankara, Turkey; 2Department of Anesthesiology and Reanimation, Gazi University Faculty of Medicine, Ankara, Turkey; 3Department of Physiology, Atılım University Faculty of Medicine, Ankara, Turkey; 4Department of Histology and Embryology, Kırıkkale University Faculty of Medicine, Kırıkkale, Turkey; 5Department of Medical Biochemistry, Gazi University Faculty of Medicine, Ankara, Turkey
Correspondence: Mustafa Arslan, Gazi University, Medical Faculty, Department of Anesthesiology and Reanimation, Ankara, 06510, Turkey, Tel +90 533 422 85 77, Email [email protected]
Background: Ischaemia–reperfusion (IR) injury, which can be encountered during surgical procedures involving the abdominal aorta, is a complex process that affects distant organs, such as the heart, liver, kidney, and lungs, as well as the lower extremities. In this study, we aimed to contribute to the limited literature by investigating the protective effect of dexmedetomidine, which was administered through different routes, on kidney tissue in rats with spinal cord IR injury.
Methods: A total of 30 rats were randomly divided into five groups: control (C group), IR (IR group), IR-intraperitoneal dexmedetomidine (IRIPD group), IR-intrathecal dexmedetomidine (IRITD group), and IR-intravenous dexmedetomidine (IRIVD group). The spinal cord IR model was established. Dexmedetomidine was administered at doses of 100 μg/kg intraperitoneally, 3 μg/kg intrathecally, and 9 μg/kg intravenously. Histopathologic parameters in kidney tissue samples taken at the end of the reperfusion period and biochemical parameters in serum were evaluated.
Results: When examined histopathologically, tubular dilatation was found to be significantly reduced in the IRIVD, IRITD, and IRIPD groups compared with the IR group (p = 0.012, all). Vascular vacuolization and hypertrophy were significantly decreased in the IRIVD, IRITD, and IRIPD groups compared with the IR group (p = 0.006, all). Tubular cell degeneration and necrosis were significantly reduced in the IRIVD, IRITD, and IRIPD groups compared with the IR group (p = 0.008, p = 0.08, and p = 0.030, respectively). Lymphocyte infiltration was significantly decreased in the IRIVD and IRITD groups compared with the IR group (p = 0.006 and p = 0.06, respectively).
Conclusion: It was observed that dexmedetomidine administered by different routes improved the damage caused by IR in kidney histopathology. We think that the renoprotective effects of dexmedetomidine administered intravenously and intrathecally before IR in rats are greater.
Keywords: dexmedetomidine, ischaemia–reperfusion, intrathecal, intravenous, rat
Introduction
Spinal cord ischaemia–reperfusion (IR) injury is a condition that can be encountered during spine, spinal cord, and thoracoabdominal aorta surgeries.1,2 Damage due to ischaemia during surgery is aggravated by reperfusion, and delayed death of tissue cells may occur. When the spinal cord is subjected to ischemic injury, the vascularity in the tissue is impaired and the blood–spinal cord barrier (BSCB) is compromised. The BSCB is an important structure that provides the integrity of the central nervous system, which is an important physiologic and metabolic structure between microvascular structures, such as the blood–brain barrier and the surrounding tissues.3
Spinal cord IR injury can lead to damage by the disruption of the BSCB and by the proinflammatory mediators reaching the kidney tissue, where microcapillary structures are dense, through the circulation.4 In the clinic, no specific treatment is available other than supportive treatment to alleviate acute kidney injury (AKI) or accelerate its recovery.
Dexmedetomidine, a new, highly selective α-2 receptor agonist, has taken its place in the clinic due to its short elimination half-life, non-addictive metabolites, and dose-dependent sedative, anxiolytic, analgesic, and anti-sympathomimetic properties.5,6 Many studies have reported that continuous infusion of dexmedetomidine reduces renal IR injury in patients and rats.7,8
This study, in rats with spinal cord IR injury, aimed to contribute to the literature by assuming that dexmedetomidine, which is applied through different routes of administration in kidney tissue, may have a protective effect.
Methods
The study was started after obtaining approval from the Gazi University Animal Experiments Local Ethics Committee (Approval No.: G.Ü.E.T-20.047). The animal studies were carried out in line with the Guide for the Care and Use of Laboratory Animals (National Institutes of Health, 1986). A total of 30 adult male Wistar albino rats (aged 10–12 weeks) weighing 250–325 g were obtained from Gazi University Laboratory Animal Breeding and Experimental Research Center (GUDAM).
All rats were illuminated between 8:00 and 20:00. They were housed in separate cages in a room with 25 ± 2°C and 55 ± 5% absolute humidity. Free access to feed and water was allowed before and after the experiments. The rats were anesthetized with intramuscular 100 mg/kg ketamine (Ketalar 1 mL: 50 mg, Pfizer, Istanbul, Turkey) and provided with a body temperature of 36 ± 0.1°C using a heating pad. The rats were randomized into five groups, with six animals in each group using the closed-envelope method (Figure 1).
 |
Figure 1 The rats were randomized into five groups. |
The IR model in which the abdominal aorta was clamped was used to generate the experimental IR. The abdomen was dissected with a vertical incision, and the abdominal aorta was not clamped in the control group (C group, n = 6).
The vertical incision was opened and the aortic clamp time was 30 minutes, followed by an ischemic period, and a 2-hour reperfusion period was performed after the clamp was opened in the ischaemia–reperfusion group (IR group, n = 6).
After the vertical incision, 30 minutes before the IR procedure, intraperitoneal dexmedetomidine hydrochloride 100 µg/kg (Sedodamid 100 µg/2 mL, Koçak Farma®, Turkey) was administered in the IR-intraperitoneal dexmedetomidine group (IRIPD group, n = 6).
Intrathecal dexmedetomidine hydrochloride 3 µg/kg was administered using the same surgical procedure in the IR-intrathecal dexmedetomidine group (IRITD group, n = 6) as in the IRIPD group. During the intrathecal application, when the subarachnoid area was entered with a microsyringe between the L5 and L6 vertebrae of the rat and a sudden slight movement of the tail was observed, the drug was administered in 30 seconds, and the needle was withdrawn after waiting for 15 seconds.
Intravenous dexmedetomidine hydrochloride 9 µg/kg was administered through the tail vein, using the same surgical procedure in the IR-intravenous dexmedetomidine group (IRIVD group, n = 6) as in the IRITD group.
To prevent hypovolemia, an isotonic saline solution was administered hourly (3 mL/kg, i.p.). The abdomen was covered with a moist sterile pad during the reperfusion period.
Previous studies were considered when deciding on dexmedetomidine doses.9,10
For the IR model, the abdomen was dissected under anaesthesia, the abdominal aorta was clamped using a haemostasis clamp for 30 minutes, and then the clamp was removed and the abdominal aorta was reperfused for 2 hours. The rats were sacrificed using the intracardiac blood collection method under deep anaesthesia. Kidney tissue samples were collected and kept in 10% formalin solution and serum samples at –80°C, and biochemical and histopathologic tests were performed.
Histopathologic Analysis
Renal tissues were sliced and immersed in 10% buffered neutral formalin and embedded in paraffin for 24 hours. Also, 4-μm tissue sections taken from paraffin blocks were mounted on slides for staining with haematoxylin and eosin (H&E). The samples were examined histopathologically under light microscopy. The scoring of each tissue sample represented the mean score of 10 different fields.
Renal injury was evaluated by determining glomerular vacuolization (GV), tubular dilation (TD), vascular vacuolization and hypertrophy (VVH), tubular cell degeneration and necrosis (THDN), Bowman space dilation (BSD), tubular hyaline cylinders (THC), lymphocyte infiltration (LI), and tubular cell shedding (TCS) as follows: 0, no change; +1, minimal change; +2, medium; and +3, severe.11,12
Biochemical Analysis
Oxidative Parameters
The renal tissue was first washed with cold deionized water to discard blood contamination and then homogenized in a homogenizer. Measurements of cell content require an initial preparation of the tissues. The preparation procedure may involve grinding the tissue in a ground-glass tissue blender using a rotor driven by a simple electric motor. The homogenizer, a tissue blender similar to the typical kitchen blender, is used to emulsify and pulverize the tissue (Heidolph Instruments GMBH & CO KGDiax 900 Germany) at 1000 U for about 3 min. After centrifugation at 10,000 g for about 60 min, the upper clear layer was removed. Superoxide dismutase (SOD) activity was measured using Durak et al’s method.13 The SOD activity method is based on the measurement of the absorbance increase at 560 nm due to the reduction of nitro blue tetrazolium (NBT) to a diformazan precipitate (NBTH2). One unit of SOD activity was defined as the enzyme protein amount causing 50% inhibition in the NBTH2 reduction rate, and results were expressed in U/mg protein. For the measurement of malondialdehyde (MDA) levels, the thiobarbituric acid (TBA) reactive substance assay was performed using Van Ye et al’s method.14 The reaction with TBA at 90–100°C was used to determine the MDA level because MDA or similar substances react with TBA and produce a pink pigment with an absorption maximum of 532 nm. To ensure protein precipitation, the sample at room temperature was mixed with cold 20% (wt/vol) trichloroacetic acid, and the precipitate was then centrifuged for 10 min at 3000 rpm and room temperature to form a pellet. An aliquot of the supernatant was then placed into an equal volume of 0.6% (wt/vol) TBA in a boiling water bath for 30 min. Following cooling, sample and blank absorbance were read at 532 nm, and the results were expressed as nmol/mg protein, based on a graph where 1,1,3,3-tetra methoxy propane was used as the MDA standard. The sample protein amount was determined using the Lowry method, and BSA was used as the standard protein.15
Homogenization of Tissues
The renal tissue collected in the Eppendorf tube was frozen immediately in liquid nitrogen and stored at –80° C in a deep freezer until the time of the total antioxidant status (TAS), total oxidant status (TOS), and oxidative stress index (OSI) analyses. The procedures were performed very quickly so that the tissues would not thaw. First, pieces (80–100 mg) were cut with 22 lancets (PLUSMED®) from the renal tissues and weighed on a precision scale. The weighed tissue was smashed in a porcelain bowl in the presence of liquid nitrogen, and the powdered tissue was immediately transferred to a homogenization tube (099C S3, Glas-Col). A KCl solution (140 mM) was added per gram of tissue to achieve a 1/10 (w/v) dilution. To avoid increasing the temperature, the homogenization tube was placed in a flake-ice-filled glass beaker. A Glas-Col (K5424®) homogenizer was used at a speed of 50 rpm for 2 min to complete the process (pestle, 099C S21G, Glas-Col). Homogenates were transferred to 1.5-mL Eppendorf tubes and centrifuged at 3000 rpm for 10 minutes (NF 048, NUVE). The supernatants obtained were transferred to new Eppendorf tubes.
Measurements of TAS/TOS
TAS Measurement
The TAS test kit (RelAssay Diagnostic®, Turkey) was used according to the manufacturer’s instructions to measure the TAS levels. In brief, 30 μL of the sample was mixed with 500 μL of measurement buffer (reagent 1) in an Eppendorf tube, and 2 μL of that mixture was used to measure the absorbance at 660 nm (A1) (NanoDrop® ONE, Thermo Scientific). Then, 75 μL of coloured 2,2-azino-bis-3-ethylbenzothiazoline-6-sulfonic acid (ABTS) (reagent 2) was added to the mixture, and incubation was performed at 37 °C for 5 min (ST 30, NUVE). The A2 measurement was evaluated at an absorbance of 660 nm. Trolox Eq solution at a concentration of 1 mmol/L was used instead of samples to obtain the standard values. A1 and A2 measurements were performed three times for each sample, and the average values were calculated. The absorbance change (ΔAbs) was calculated by subtracting the first absorbance value (A1) from the second absorbance value (A2). The TAS level was calculated using the formula given in the kit and expressed as mmol Trolox Eq/L.

TOS Measurement
The TOS test kit (RelAssay Diagnostic®, Turkey) was used according to the manufacturer’s instructions to measure the TOS levels. In brief, 75 μL of the sample was mixed with 500 μL of measurement buffer (reagent 1) in an Eppendorf tube, and 2 μL of that mixture was used to measure the absorbance at 530 nm (A1) (NanoDrop® ONE, Thermo Scientific). Then, 25 μL of pro-chromogenic solution (reagent 2) was added to the mixture, and incubation was performed at 37°C for 5 min (ST 30, NUVE). The A2 measurement was evaluated at an absorbance of 530 nm. A standard solution containing 10 μmol/L of hydrogen peroxide (H2O2) equivalent/litre given in the kit was used for the standard measurement. A1 and A2 measurements were performed three times for each sample, and the average values were calculated. The absorbance change (ΔAbs) was calculated by subtracting the first absorbance value (A1) from the second absorbance value (A2). The TOS level was calculated using the formula given in the kit and expressed as mmol H2O2 Eq/L.

Oxidative Stress Index
The OSI, which is shown as an indicator of oxidative stress, is expressed as the ratio of TOS to TAS levels. When calculating the OSI of the samples, TAS levels were multiplied by 100 to equalize the TOS levels and the units [20]. The results were expressed as arbitrary units (AU).

Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS, Chicago, IL, USA) 20.0 program. The Shapiro–Wilk test and Q–Q plot test were used to assess data distribution. The results were analysed using the Kruskal–Wallis test, with a Bonferroni-adjusted Mann–Whitney U post hoc test. The results were expressed as the mean ± standard deviation (SD) and median (25–75%). A value of p < 0.05 was considered statistically significant.
Results
When examined histopathologically, there was significantly more tubular dilatation in the IR group than in the C group (p = 0.003). Tubular dilatation was significantly decreased in the IRIVD, IRITD, and IRIPD groups compared with the IR group (p = 0.012, all). There was significantly more vascular vacuolization and hypertrophy in the IR group than in the C group (p = 0.001). Vascular vacuolization and hypertrophy were significantly decreased in the IRIVD, IRITD, and IRIPD groups compared with the IR group (p = 0.006, all). There was significantly more tubular cell degeneration and necrosis in the IR group than in the C group (p = 0.008). Tubular cell degeneration and necrosis were significantly decreased in the IRIVD, IRITD, and IRIPD groups compared with the IR group (p = 0.008, p = 0.08, and p = 0.030, respectively). Lymphocyte infiltration was significantly greater in the IR group than in the C group (p = 0.001). Lymphocyte infiltration was significantly decreased in the IRIVD and IRITD groups compared with the IR group (p = 0.006 and p = 0.06, respectively) (Table 1, Figures 2–6).
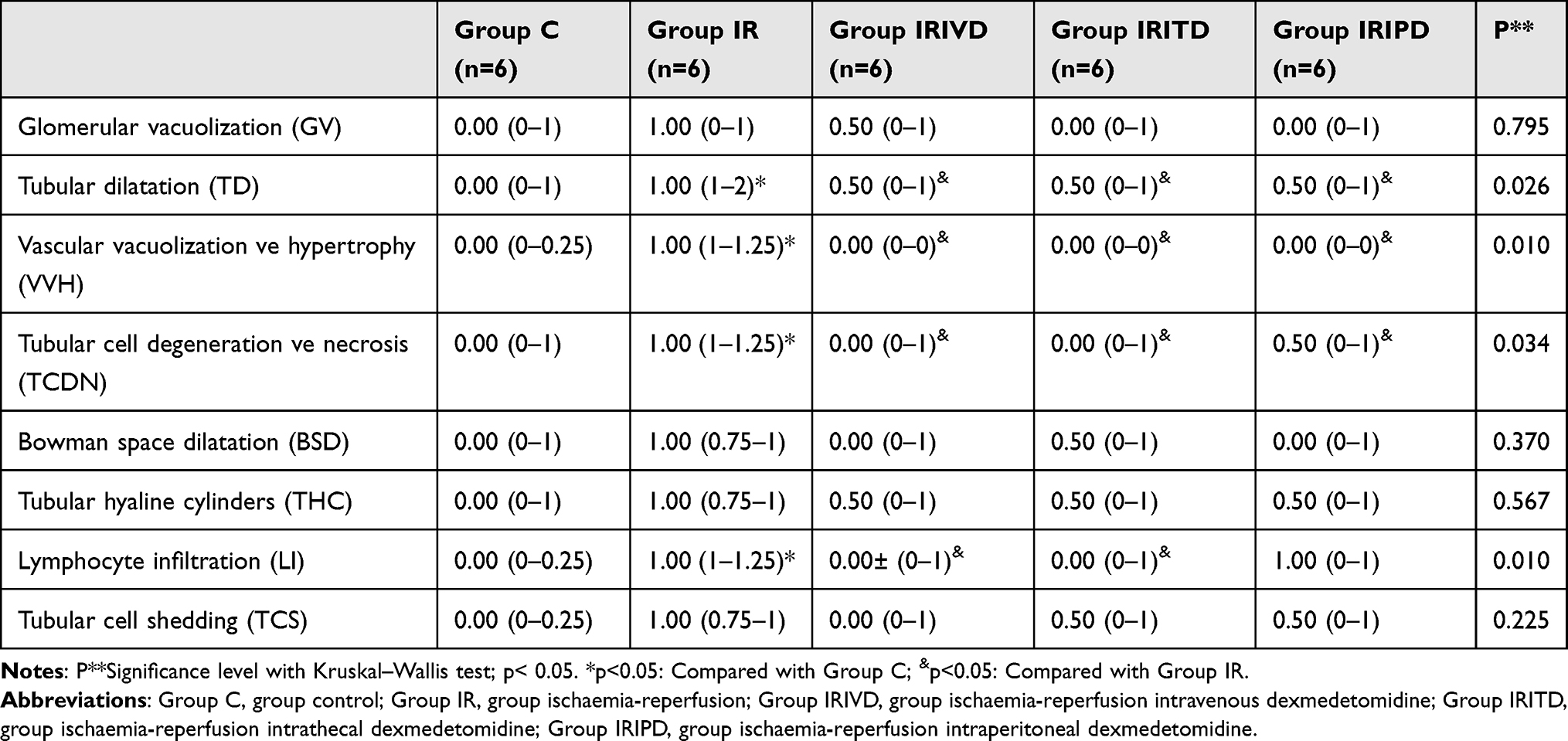 |
Table 1 Renal Tissue Histopathological Findings [Median (25%-75%)] |
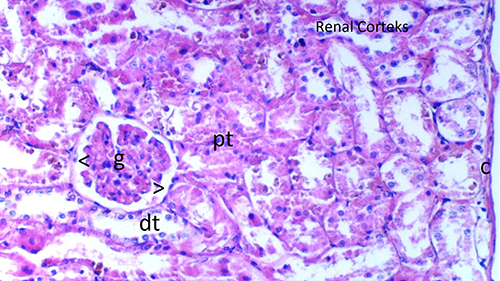 |
Figure 2 Normal kidney tissue, Group C, H&Ex100. Abbreviations: g, glomerulus; dt, distal tubule; pt, proximal tubule; C, cortex; ^, Bowman space; RC, renal cortex. Note: Image shows histopathologic analysis of kidney samples. |
 |
Figure 3 Group IR, H&Ex100. Abbreviations: g, glomerulus; dt, distal tubule; pt, proximal tubule; m, macula densa; inf, inflammation; conj, congestion; ↓, dilated tubule. |
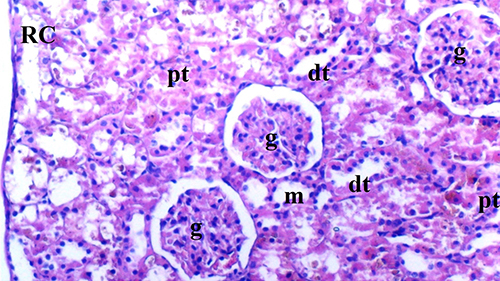 |
Figure 4 Group IRIVD, H&Ex100. Abbreviations: g, glomerulus; dt, distal tubule; pt, proximal tubule; RC, renal cortex; m, macula densa. |
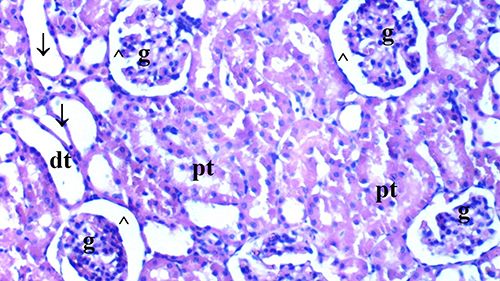 |
Figure 5 Group IRITD, H&Ex100. Abbreviations: g, glomerulus; dt, distal tubule; pt, proximal tubule; ^, Bowman space; ↓, dilated tubule. |
 |
Figure 6 Group IRIPD group, H&Ex100. Abbreviations: g, glomerulus; dt, distal tubule; pt, proximal tubule; RC, renal cortex; ↓, dilated tubule. |
Biochemical Results
TAS levels showed statistically significant differences in all groups (p = 0.001). TAS levels in the IR group were significantly lower than in the C group (p < 0.0001). TAS levels in the IR group were significantly higher than in the IRIVD, IRITD, and IRIPD groups (p = 0.001, p = 0.001, and p = 0.009, respectively) (Table 2).
 |
Table 2 Rat Kidney Tissue Oxidant Status Parameters [Mean ± SD] |
Similar to TAS levels, TOS levels were statistically significantly different in all groups (p < 0.0001). TOS levels were significantly higher in the IR group than in the C and IRIPD groups (p < 0.0001 and p = 0.032, respectively). TOS levels in the IRIVD, IRITD, and IRIPD groups were significantly lower than in the IR group (p < 0.0001, p < 0.0001, and p = 0.005, respectively) (Table 2).
OSI showed statistically significant differences in all groups (p < 0.0001). OSI in the IR and IRIPD groups were significantly higher than in the C group (p < 0.0001 and p = 0.022, respectively). OSI in the IR group was significantly higher than in the IRIVD, IRITD, and IRIPD groups (p < 0.0001, all) (Table 2).
The MDA levels were significantly higher in the IR group than in the C group (p < 0.0001) and were significantly lower in in the IRIVD, IRITD, and IRIPD groups than in the C group (p < 0.0001, p < 0.0001, and p = 0.001, respectively). SOD activity was significantly lower in the IR group than in the C group (p < 0.001) and significantly higher in the IRIVD, IRITD, and IRIPD groups than in the IR group (p < 0.0001, p < 0.0001, and p = 0.007, respectively) (Table 2).
Discussion
AKI due to spinal cord IR injury is a complication that can develop after major vascular surgeries, such as thoracoabdominal aortic surgery, causing negative outcomes as well as high costs and long-term treatment.16 Serious complications such as this cause impaired blood flow in the aorta, decreased oxygen and nutrient delivery to the tissue, accumulation of intracellular sodium, hydrogen, and calcium ions, and tissue acidosis, which leads to mitochondrial membrane depolarization and adenosine triphosphate (ATP) depletion.17
With reperfusion, the release of free radicals and proinflammatory cytokines occurs due to the development of mitochondrial failure in kidney tissue. In ischemic conditions, mitochondria switch from aerobic to anaerobic metabolism, ATP production decreases, and acid accumulation occurs in the tissue. With a decrease in ATP production, sodium increases inside the cell, and potassium increases outside the cell, which initiates cell depolarization. The compensatory increase in intracellular calcium causes proteolytic enzyme activation, which leads to apoptosis and necrosis, and enzymatic activities, such as ATP-based phosphorylation, are also affected.18
During surgery, the body is exposed to surgical stress in which inflammatory, endocrine, metabolic, and immunologic mediators are activated, and when IR is added during surgery, exaggerated reactive oxygen radical formation occurs.19 In normal tissue physiology, the scavenging of reactive oxygen radicals can be achieved by various enzymatic mechanisms. It has been shown that reperfusion of ischemic tissue may lead to an excessive increase in reactive oxygen species and that this oxidative burst may mediate IR injury, and it has been reported that it may be accompanied by serious cellular events such as lipid peroxidation.20
Major contributors to the damage caused by IR include the production of reactive oxygen radicals, the release of proinflammatory cytokines that exacerbate inflammation and tissue damage, and the activation of immune cells that cause cell death via apoptosis or necrosis.21 As the oxidative stress level and the severity of the inflammatory process increase in the tissue subjected to IR, they may cause inflammatory activation both in that tissue and in distant organs that have not been exposed to ischaemia, and the process may lead to multiorgan failure.22,23 Previous studies have also shown that IR causes an increase in inflammatory mediators in local and distant organs.24 These cytokines can induce tubular epithelial cell necrosis and renal tubular atrophy and eventually lead to IR injury–induced AKI.25–27
The balance between pathogenic mechanisms [eg prolonged ischaemia, cell death, and the production of proinflammatory mediators such as tumour necrosis factor (TNF)-α] and protective mechanisms (eg the production of extracellular adenosine, haem oxygenase, leukotrienes) determines the outcome of AKI that develops as a result of IR injury.28
In most studies with spinal cord IR models, a reperfusion period is applied after a 30-minute ischaemia period in the aorta.29 In the renal IR model in rats, functional impairment in renal functions develops during the reperfusion period, which lasts approximately 6–24 hours.30 In our study, we preferred to apply a 30-minute ischaemia period followed by a 2-hour reperfusion period.
TAS and TOS can provide accurate information by enabling the measurement of unknown markers in the serum,31,32 MDA is a useful indirect indicator that can show free radical–related damage,33,34 and SOD is an important antioxidant.35 TOS, TAS, OSI, MDA, and SOD were used to determine the oxidant–antioxidant level in our study. SOD and TAS levels were found to be significantly higher in the IRIVD, IRITD, and IRIPD groups than in the IR group. TOS levels were found to be significantly lower in the IRIVD, IRITD, and IRIPD groups than in the IR group, whereas they were found to be significantly higher in the IRIPD group than in the C group. OSI, which is shown as an indicator of oxidative stress, in the IR group was significantly higher than in the IRIVD, IRITD, and IRIPD groups. MDA levels were found to be significantly lower in the IRIVD, IRITD, and IRIPD groups than in the IR group. Based on the findings of this study, it is clear that dexmedetomidine treatment protects against oxidative stress, and dexmedetomidine can achieve an anti-inflammatory effect by inhibiting the expressions of inflammatory factors in renal tissue and can inhibit the process of oxidative stress damage.
Therapeutic approaches to preventing or treating AKI are limited, so preventive approaches are important.36 The protective effects of dexmedetomidine have been demonstrated in preclinical studies in a wide variety of organ systems, and it has been stated that this feature may be due to its anaesthetic effect and its anti-inflammatory and anti-apoptotic properties.37–40
The effects of dexmedetomidine have been explained by various mechanisms. It acts on the locus caeruleus and reduces the central sympathetic outflow and surgical stress response by stimulating presynaptic a2-adrenoceptors, which prevent the release of noradrenaline in the sympathetic synapses.41 It decreases the genetic expression of proinflammatory mediators, such as interleukin 1β (IL-1β), IL-6, and TNF-α, and the expression of TNF-α and IL-6 by inhibiting toll-like receptor 4 (TLR-4), which initiates an innate immune response, after being activated by endogenous ligands secreted from necrotic cells due to injury, and by down-regulating the activity of nuclear transcription factor B (NFκB) and mitogen-activated protein kinase (MAPK).42 It increases the expression of anti-inflammatory IL-10 by decreasing the phosphorylation of Janus kinase 2 (JAK2) and the signal transducer and activator of transcription (STAT)-3.43
The anti-inflammatory and anti-apoptotic effects of dexmedetomidine also improve histopathological results. In the study by Kuzgun et al, it was observed that the proximal tubule and total cell damage scores were improved in the groups that received intraperitoneal dexmedetomidine (100 μg/kg) before the renal IR model in rats in which diabetes mellitus was induced using streptozotocin.10
In another study examining the effects of dexmedetomidine on IR-induced kidney damage, intraperitoneal dexmedetomidine (25 µg/kg) was injected 30 minutes before IR in one group. It was found that focal renal haemorrhage, focal tubular necrosis, neutrophil infiltration, and vacuolar degeneration in renal tubular epithelial cells were significantly lower than in the IR group.34
In this study, the effect of dexmedetomidine administered by different routes before spinal IR injury on kidney tissue was examined histopathologically. Histologic damage, including TD, VVH, and THDN, was found to be less in the dexmedetomidine groups than in the IR group. Lymphocyte infiltration was found to be decreased in the IRIVD and IRITD groups. Lymphocyte infiltration also decreased in the IRIPD group, but no significant difference was found when compared with the IR group.
The anti-inflammatory activity of dexmedetomidine may change in a dose-dependent manner. Xu et al reported that intraperitoneal 25 μg/kg, 50 μg/kg, and 100 μg/kg dexmedetomidine decreased IR injury in a dose-dependent manner on kidney and myocardial tissue, by reducing the inflammatory effect, in rats in which IR injury was created.44
In light of studies in the literature, considering that dexmedetomidine administered by different means might have an anti-inflammatory effect, it was desired to contribute to the limited literature with this study. However, the study had some limitations. One was the inability to apply a longer reperfusion time, such as 24 hours, to detect variations in biochemical and histopathologic parameters. As stated in the literature, dexmedetomidine decreases the genetic expression of proinflammatory mediators.42 Therefore, we did not measure inflammatory and apoptotic markers by ELISA or by immunohistochemistry. Another was the failure to provide haemodynamic monitoring in the experimental model.
Conclusions
In sum, dexmedetomidine, a selective α-2 adrenergic receptor agonist, had kidney protective effects because renal oedema and inflammatory response decreased significantly when it was administered 30 minutes before an IR procedure in rats with spinal cord IR injury. Furthermore, it was observed that dexmedetomidine had renal protective effects because it improved histopathological results and decreased oxidative stress and lipid peroxidation markers in the groups in which it was used. It was seen that this effect was greater with the intravenous and intrathecal administration of dexmedetomidine.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Auerbach JD, Kean K, Milby AH, et al. Delayed postoperative neurologic deficits in spinal deformity surgery. Spine. 2016;41(3):E131–E138. doi:10.1097/BRS.0000000000001194
2. Bell MT, Puskas F, Smith PD, et al. Attenuation of spinal cord ischemia-reperfusion injury by specific α-2a receptor activation with dexmedetomidine. J Vasc Surg. 2012;56(5):1398–1402. doi:10.1016/j.jvs.2012.04.012
3. Fang B, Li X-Q, Bi B, et al. Dexmedetomidine attenuates blood-spinal cord barrier disruption induced by spinal cord ischemia reperfusion injury in rats. Cell Physiol Biochem. 2015;36(1):373–383. doi:10.1159/000430107
4. Liu M, Liang Y, Chigurupati S, et al. Acute kidney injury leads to inflammation and functional changes in the brain. J Am Soc Nephrol. 2008;19:1360–1370. doi:10.1681/ASN.2007080901
5. Tang C, Huang X, Kang F, et al. Intranasal dexmedetomidine on stress hormones, inflammatory markers, and postoperative analgesia after functional endoscopic sinus surgery. Mediators Inflamm. 2015;2015:939431. doi:10.1155/2015/939431
6. Tang C, Xia Z. Dexmedetomidine in perioperative acute pain management: a non-opioid adjuvant analgesic. J Pain Res. 2017;10:1899–1904. doi:10.2147/JPR.S139387
7. Balcı C, Akan M, Boztaş N, et al. Protective effects of dexmedetomidine and remote ischemic preconditioning on renal ischemia reperfusion injury in rats. Ulus Travma Acil Cerrahi Derg. 2017;23(4):279–286. doi:10.5505/tjtes.2016.49103
8. Liu Y, Sheng B, Wang S, Lu F, Zhen J, Chen W. Dexmedetomidine prevents acute kidney injury after adult cardiac surgery: a meta-analysis of randomized controlled trials. BMC Anesthesiol. 2018;18(1):7. doi:10.1186/s12871-018-0472-1
9. Ma D, Hossain M, Rajakumaraswamy N, et al. Dexmedetomidine produces its neuroprotective effect via the alpha 2A-adrenoceptor subtype. Eur J Pharmacol. 2004;502:87–97. doi:10.1016/j.ejphar.2004.08.044
10. Kuzgun Ö, Özkardeşler S, Özbilgin Ş, et al. Effects of dexmedetomidine on renal ischaemia reperfusion injury in streptozotocin-induced diabetic rats. Turk J Anaesthesiol Reanim. 2018;46(6):462–469. doi:10.5152/TJAR.2018.62592
11. Bostan H, Kalkan Y, Tomak Y, et al. Reversal of rocuronium-induced neuromuscular block with sugammadex and resulting histopathological effects in rat kidneys. Ren Fail. 2011;33(10):1019–1024. doi:10.3109/0886022X.2011.618972
12. Erbatur ME, Sezen ŞC, Bayraktar AC, Arslan M, Kavutçu M, Aydın ME. Effects of dexmedetomidine on renal tissue after lower limb ischemia reperfusion injury in streptozotocin induced diabetic rats. Libyan J Med. 2017;12(1):1270021. doi:10.1080/19932820.2017.1270021
13. Durak I, Canbolat O, Kavutcu M, Ozturk HS, Yurtarslani Z. Activities of total, cytoplasmic, and mitochondrial superoxide dismutase enzymes in sera and pleural fluids from patients with lung cancer. J Clin Lab Anal. 1996;10(1):17–20. doi:10.1002/(SICI)1098-2825(1996)10:1<17::AID-JCLA4>3.0.CO;2-I
14. Van Ye TM, Roza AM, Pieper GM, Henderson J, Johnson JP, Adams MB. Inhibition of intestinal lipid peroxidation does not minimize morphological damage. J Surg Res. 1993;55:553–558. doi:10.1006/jsre.1993.1183
15. Lowry O, Rosenbraugh N, Farr L, Randall R. Protein measurement with folin phenol reagent. J Biol Chem. 1951;182:265–275. doi:10.1016/S0021-9258(19)52451-6
16. Wan IY, Angelini GD, Bryan AJ, Ryder I, Underwood MJ. Prevention of spinal cord ischaemia during descending thoracic and thoracoabdominal aortic surgery. Eur J Cardiothorac Surg. 2001;19:203–213. doi:10.1016/S1010-7940(00)00646-1
17. Hausenloy DJ, Yellon DM. Myocardial ischemia-reperfusion injury: a neglected therapeutic target. J Clin Invest. 2013;123:92–100. doi:10.1172/JCI62874
18. Yan HF, Tuo QZ, Yin QZ, Lei P. The pathological role of ferroptosis in ischemia/reperfusion-related injury. Zool Res. 2020;41(3):220–230. doi:10.24272/j.issn.2095-8137.2020.042
19. Misthos P, Katsaragakis S, Theodorou D, et al. The degree of oxidative stress is associated with majör adverse effects after lung resection: a prospective study. Eur J Cardiothorac Surg. 2006;29:591–595. doi:10.1016/j.ejcts.2005.12.027
20. Farmer EE, Mueller MJ. ROS-mediated lipid peroxidation and RES-activated signaling. Annu Rev Plant Biol. 2013;64:429–450. doi:10.1146/annurev-arplant-050312-120132
21. Klune JR, Tsung A. Molecular biology of liver ischemia/reperfusion injury: established mechanisms and recent advancements. Surg Clin North Am. 2001;90:665–677. doi:10.1016/j.suc.2010.04.003
22. Park SW, Kim M, Brown KM, D’Agati VD, Lee HT. Paneth cell-derived interleukin-17A causes multiorgan dysfunction after hepatic ischemia and reperfusion injury. Hepatology. 2011;53(5):1662–1675. doi:10.1002/hep.24253
23. Nishikata R, Kato N, Hiraiwa K. Oxidative stress may be involved in distant organ failure in tourniquet shock model mice. Leg Med. 2014;16(2):70–75. doi:10.1016/j.legalmed.2013.11.004
24. Gu J, Sun P, Zhao H, et al. Dexmedetomidine provides renoprotection against ischemia-reperfusion injury in mice. Crit Care. 2011;15(3):R153. doi:10.1186/cc10283
25. Fröhlich GM, Meier P, White SK, Yellon DM, Hausenloy DJ. Myocardial reperfusion injury: looking beyond primary PCI. Eur Heart J. 2013;34(23):1714–1722. doi:10.1093/eurheartj/eht090
26. Heusch G, Gersh BJ. The pathophysiology of acute myocardial infarction and strategies of protection beyond reperfusion: a continual challenge. Eur Heart J. 2017;38(11):774–784. doi:10.1093/eurheartj/ehw224
27. Tang C, Hu Y, Gao J, et al. Dexmedetomidine pretreatment attenuates myocardial ischemia reperfusion induced acute kidney injury and endoplasmic reticulum stress in human and rat. Life Sci. 2020;257:118004. doi:10.1016/j.lfs.2020.118004
28. Bonventre JV, Yang L. Cellular pathophysiology of ischemic acute kidney injury. J Clin Invest. 2011;121(11):4210–4221. doi:10.1172/JCI45161
29. An M, Zhang T, Deni W, Hou L, Jin K, Jin K. Dexmedetomidine inhibits microglial activation through SNHG14/HMGB1 pathway in spinal cord ischemia-reperfusion injury mice. Int J Neurosci. 2022;132(1):77–88. doi:10.1080/00207454.2020.1835901
30. Singh AP, Junemann A, Muthuraman A, et al. Animal models of acute renal failure. Pharmacol Rep. 2012;64(1):31–44. doi:10.1016/S1734-1140(12)70728-4
31. Erel O. A novel automated method to measure total antioxidant response against potent free radical reactions. Clin Biochem. 2004;37(2):112–119. doi:10.1016/j.clinbiochem.2003.10.014
32. Erel O. A new automated colorimetric method for measuring total oxidant status. Clin Biochem. 2005;38(12):1103–1111. doi:10.1016/j.clinbiochem.2005.08.008
33. Halder T, Upadhyaya G, Basak C, Das A, Chakraborty C, Ray S. Dehydrins impart protection against oxidative stress in transgenic tobacco plants. Front Plant Sci. 2018;14(9):136. doi:10.3389/fpls.2018.00136
34. Bao N, Dai D. Dexmedetomidine protects against ischemia and reperfusion-induced kidney injury in rats. Mediators Inflamm. 2020;2020:2120971. doi:10.1155/2020/2120971
35. Yaribeygi H, Mohammadi MT, Sahebkar A. PPAR-α agonist improves hyperglycemia-induced oxidative stress in pancreatic cells by potentiating antioxidant defense system. Drug Res. 2018;68(6):355–360. doi:10.1055/s-0043-121143
36. Kumar AB, Suneja M, Riou B. Cardiopulmonary bypass-associated acute kidney injury. Anesthesiology. 2011;114(4):964–970. doi:10.1097/ALN.0b013e318210f86a
37. Kocoglu H, Karaaslan K, Gonca E, Bozdogan O, Gulcu N. Preconditionin effects of dexmedetomidine on myocardial ischemia/reperfusion injury in rats. Curr Ther Res Clin Exp. 2008;69(2):150–158. doi:10.1016/j.curtheres.2008.04.003
38. Kocoglu H, Ozturk H, Ozturk H, Yilmaz F, Gulcu N. Effect of dexmedetomidine on ischemia-reperfusion injury in rat kidney: a histopathologic study. Ren Fail. 2009;31(1):70–74. doi:10.1080/08860220802546487
39. Yu X, Chi X, Wu S, et al. Dexmedetomidine pretreatment attenuates kidney injury and oxidative stress during orthotopic autologous liver transplantation in rats. Oxid Med Cell Longev. 2016;2016:4675817. doi:10.1155/2016/4675817
40. Bell MT, Puskas F, Bennett DT, et al. Dexmedetomidine, an α-2a adrenergic agonist, promotes ischemic tolerance in a murine model of spinal cord ischemia-reperfusion. J Thorac Cardiovasc Surg. 2014;147(1):500–506. doi:10.1016/j.jtcvs.2013.07.043
41. Carollo DS, Nossaman BD, Ramadhyani U. Dexmedetomidine: a review of clinical applications. Curr Opin Anaesthesiol. 2008;21(4):457–461. doi:10.1097/ACO.0b013e328305e3ef
42. Lai YC, Tsai PS, Huang CJ. Effects of dexmedetomidine on regulating endotoxin-induced up-regulation of inflammatory molecules in murine macrophages. J Surg Res. 2009;154(2):212–219. doi:10.1016/j.jss.2008.07.010
43. Si YN, Bao HG, Zhang Y, et al. Renoprotective effects and mechanism of dexmedetomidine on renal ischemia/reperfusion injury in rats. J Clin Anesthesiol. 2013;29:261–264.
44. Xu Z, Wang D, Zhou Z, et al. Dexmedetomidine attenuates renal and myocardial ischemia/reperfusion injury in a dose-dependent manner by inhibiting inflammatory response. Ann Clin Lab Sci. 2019;49(1):31–35.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.