")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Effects of Daily Mean Temperature on Daily Hospital Admissions for Coronary Artery Disease: A Retrospective Study
Authors Wang R, Lin Y, Chen M, Wang W , Chen Y, Qiu X, Miao X
Received 12 October 2023
Accepted for publication 20 January 2024
Published 31 January 2024 Volume 2024:17 Pages 269—277
DOI https://doi.org/10.2147/RMHP.S444451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Rehua Wang,1,2,* Yongjun Lin,3,* Mao Chen,4 Wei Wang,5 Yongli Chen,6 Xiaoxia Qiu,7 Xing Miao1,2
1Department of Cardiology, Fujian Provincial Hospital, Fuzhou, 350001, People’s Republic of China; 2Department of Cardiology, Shengli Clinical Medical College of Fujian Medical University, Fuzhou, 350001, People’s Republic of China; 3Department of General Medicine, the First Hospital of Quanzhou Affiliated to Fujian Medical University, Quanzhou, 362000, People’s Republic of China; 4Department of Scientific Research, Fujian Provincial Hospital, Fuzhou, 350001, People’s Republic of China; 5Department of Psychiatry, Fuzhou Neuro-Psychiatric Hospital Affiliated to Fujian Medical University, Fuzhou, 350008, People’s Republic of China; 6Department of Cardiology, Fujian Provincial Hospital South Branch, Fuzhou, 350028, People’s Republic of China; 7Department of Cardiology, Fujian Medical University Union Hospital, Fuzhou, 350001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xing Miao, Department of Cardiology, Fujian Provincial Hospital, Shengli Clinical Medical College of Fujian Medical University, No. 134 East Street, Gulou District, Fuzhou, 350001, People’s Republic of China, Tel +86 13763810443, Email [email protected]
Purpose: Temperature changes unfavorably impact on cardiovascular disease. However, the association between temperature changes and coronary artery disease (CAD) is not well documented. This study aimed to explore the association between daily mean temperature and daily CAD hospital admissions on the southeast coast of China (Fuzhou City).
Methods: A total of 1883 CAD patients who underwent percutaneous coronary intervention between 2017 and 2019 were obtained. The severity of CAD was evaluated by the Gensini score. Distributed lag non-linear model (DLNM) combined with a quasi-Poisson regression model was used to examine the delayed effect between daily mean temperature and daily CAD hospital admissions. Stratified analyses were performed by Gensini score and severity of lesions. The relative risk (RR) with a 95% confidence interval (CI) was used to assess the relationship.
Results: Extreme cold (8°C) (RR=0.49, 95% CI: 0.25– 0.99) and moderate cold (10°C) (RR=0.56, 95% CI: 0.31– 0.99) daily mean temperature with a lag of 0– 20 days were correlated with lower risk of daily CAD hospital admissions. Moderate heat (30°C) (RR=1.80, 95% CI: 1.01– 3.20) and extreme heat (32°C) (RR=2.02, 95% CI: 1.01– 4.04) daily mean temperature with a lag of 0– 20 days related to a higher risk of daily CAD hospital admissions. Similar results were observed for daily mean temperature with a lag of 0– 25 days. Stratified analysis showed the lagged effect of daily mean temperature (lag 0, 0– 5, 0– 15, 0– 20, and 0– 25 days) on the daily CAD hospital admissions was observed only in patients with a Gensini score ≤ 39 (tertile 1).
Conclusion: Cold temperatures may have a protective effect on daily CAD hospital admissions in the Fuzhou area, whereas hot temperatures can have an adverse effect.
Keywords: temperature, coronary artery disease, gensini score, daily admissions, lag effect
Introduction
Coronary artery disease (CAD), which mainly includes angina pectoris, ST-segment elevation myocardial infarction, and non-ST-segment elevation myocardial infarction, is one of the major cardiovascular diseases affecting the global population.1 Epidemiological studies of cardiovascular diseases have shown that the prevalence of CAD varies widely by geographic location, race, and sex.2 Lifestyle, environmental, and genetic factors are associated with the development of CAD,3 with modifiable risk factors such as environment and lifestyle attracting research attention. Several studies of the association between migration and cardiovascular diseases suggested that migration to a new environment can significantly affect the risk of morbidity and mortality from CAD.4,5 A study of Finnish twins found that the incidence of CAD was substantially lower in Finnish immigrants who moved to Sweden than in identical twins who had always lived in Finland.6 These studies suggested that modifiable environmental factors may play an important role in the development of CAD.
Climate and environmental pollution are two risk factors for atherothrombosis, and they affect individuals through population effect.7–9 Extreme temperature conditions (hot and cold temperatures) have been reported to be associated with the occurrence of cardiovascular diseases, while atmospheric pressure and relative humidity have a lesser effect on the cardiovascular system.10,11 Redfors et al showed that extreme temperatures were related to larger infarct size and smaller left ventricular ejection fraction in patients with ST-segment elevation myocardial infarction.12 Hensel et al reported that even in moderate climatic conditions, low temperatures can still lead to an increased frequency of CAD, especially below 10 °C.13 A time-series analysis study based on major cities across China found that the mortality risk and burden from main cardiopulmonary diseases was more pronounced in temperate monsoon and subtropical monsoon climatic zones.14 Previous studies on ambient temperature and cardiovascular disease in China were mainly in the northwest and inland areas (representing different climates), while there were fewer studies on the southeastern coastal areas of China.15–17 The association between ambient temperature and CAD risk under different climatic conditions needs to be further explored. We hypothesized that the subtropical monsoon climate along the southeast coast of China would affect the risk of hospitalization for patients with CAD.
Therefore, this study aimed to determine the impact of daily mean temperature on the daily CAD hospital admissions, in Fuzhou, southeast coast of China.
Methods
Study Area
Fuzhou is the capital of Fujian Province, China. It is located on the southeast coast of China, with a geographical location of 119.28 E and 26.08 N. Fuzhou is a typical subtropical monsoon climate with abundant sunshine, abundant rainfall, and suitable temperature, with an annual average temperature of 20–25 °C. January-February, the coldest month, has an average temperature of 6–10 °C, while July-August, the hottest month, has an average temperature of 33–37 °C.
Study Design and Data Collection
Admission data of patients with CAD were obtained from the Fujian Provincial Hospital from November 2017 to December 2019. Patients diagnosed with CAD who were at least 18 years of age and underwent percutaneous coronary intervention services were included in the analysis. Patients who had lived in Fuzhou City for less than 1 month before admission were excluded. The coronary angiography was performed for all included CAD patients, and the degree of coronary artery stenosis was quantitatively analyzed using a Digital Subtraction Angiography (DSA) image processing system. This study was approved by the Institutional Review Board of Fujian Provincial Hospital (approval number: K2021-01-035), and all participants provided informed consent. All study procedures were conducted in accordance with the guidelines of the Declaration of Helsinki.
Patient data collection included age, sex, and diagnosis information (Supplement Table 1). Temperature data were collected from the Fujian Provincial Meteorological Bureau (http://fj.cma.gov.cn/). Air pollution data were derived from 5-fixed site air quality monitoring stations of the Real-time Air Quality Index Visual Map (http://aqicn.org/map).
Outcome and Definition
The outcome of this study was the daily CAD hospital admissions. The relationship between daily mean temperature and daily CAD hospital admissions was analyzed in all included patients and stratified by severity of CAD. The severity of CAD was indicated by the Gensini score and severity of lesions,18 respectively. The process of assessing CAD severity using the Gensini score is as follows. The degree of stenosis was scored as follows: narrowing ≤ 25% (1 score), 26–50% (2 scores), 51–75% (4 scores), 76–90% (8 scores), 91–99% (16 scores), and total occlusion (32 scores). The position importance coefficient of the lesion in the coronary circulation was: the left main coronary artery (5.0), the proximal segment of the left anterior descending coronary artery (2.5), the proximal segment of the circumflex artery (2.5), the mid-segment of the left anterior descending coronary artery (1.5), the distal segment of the left anterior descending coronary artery (1.0), the posterolateral artery (1.0), the obtuse marginal artery (1.0), the right coronary artery (1.0), and other segments (0.5). The Gensini score is the sum of the product of the stenosis degree score of each branch and the importance coefficient of the lesion site, and the higher the score, the more serious it was.19,20 In this study, the Gensini score was divided into three parts based on tri-sectional quantile: tertile 1, ≤39; tertile 2, 39–67; and tertile 3, ≥ 67. In addition, the severity of lesions was categorized into single-branch lesions and multiple-branch lesions.
Statistical Analysis
The association between temperature and cardiovascular diseases has been reported to be non-linear and delayed by many previous studies.10,17 To explore the association between daily mean temperature and daily CAD hospital admissions, the distributed lag non-linear model (DLNM) was used.21 Since the daily CAD hospital admissions fit the Poisson distribution, the time-stratified case-crossover with a DLNM analysis based on a quasi-Poisson generalized additive regression model (GAM) was utilized to analyze the lagged effects of daily mean temperature on the daily CAD hospital admissions. The model is formulated as follows: (1)

where t, the day of the observation; Yt, the hospitalizations for CAD on day t; α, the intercept; Tt,l, the cross-basis of daily mean temperature in DLNM; l, lag days; β, coefficient for Tt,l; AQIt, the air quality index (AQI) on day t; ns (…, 3), the natural cubic spline, three degrees of freedom (df) were used to smooth relative AQI; Strata is a categorical variable of the year and calendar moth used to control for season and trends, and λ is the vector of coefficient; Dowt, the t day of the week; η, coefficient for DOWt.
In the descriptive analysis, the mean and standard deviation (mean ± SD), minimum, 25th percentile, 50th percentile, 75th percentile, and maximum to describe daily mean temperature and daily CAD hospital admissions. Using the mean temperature of 20 °C (Fuzhou) as a reference temperature, the relationship between daily mean temperature (extreme cold, moderate cold, moderate heat, and extreme heat)22 and daily CAD hospital admissions at different lag days (lag 0, 0–5, 0–15, 0–20, and 0–25 days) was analyzed. Extreme cold is defined as the daily mean temperature at or below the 1th temperature percentile and the daily mean temperature at or above the 99th temperature percentile as extreme heat. The range between the 1th and 5th temperature percentile is moderate cold, and the range between the 95th and 99th temperature percentile is moderate heat. In this study, extreme cold was 8°C, moderate cold was 10°C, moderate heat was 30°C, and extreme heat was 32°C. Then, stratified analyses of the association between daily mean temperature and daily CAD hospital admissions were conducted based on Gensini score (tertile 1, ≤39; tertile 2, 39–67; and tertile 3, ≥ 67) and severity of lesions (single-branch lesions, multiple-branch lesions). The relative risk (RR) with a 95% confidence interval (CI) was used to assess the relationship. All statistical analyses were performed using the R software (version 4.1.2). The DLNM was conducted using the “dlnm” package (Gasparrini and Leone, 2014). P-value < 0.05 was considered statistically significant.
Results
Descriptive Statistics
A total of 1883 CAD patients who underwent percutaneous coronary intervention were included in this study. Demographic data of patients showed that the mean age was 64.61 ± 10.74 years and 1483 (78.76%) patients were male (Supplement Table 1). The mean Gensini score of patients was 52.00 (32.00, 78.00), 687 (36.48%) patients had single-branch lesions, and 1196 (63.52%) patients had multiple-branch lesions. Table 1 presents the descriptive statistics of daily mean temperature and daily CAD hospital admissions. The daily mean temperature ranged from 9.74 to 29.79 °C and the mean was 20.52 ± 6.03 °C. The mean number of daily CAD hospital admissions was 2.37 ± 2.01, with a range of 0 to 12.
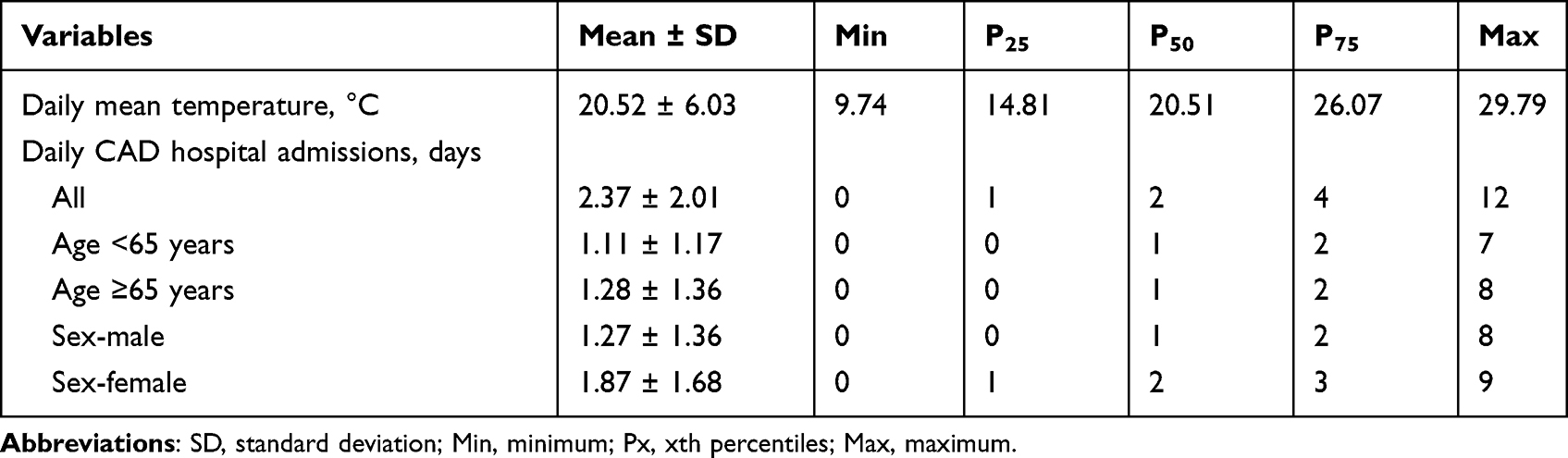 |
Table 1 Descriptive Statistics of Daily Mean Temperature and Daily Coronary Artery Disease (CAD) Hospital Admissions |
Lag Effects of Daily Mean Temperature on the Daily CAD Hospital Admissions
The effects of daily mean temperature on the daily CAD hospital admissions were presented in Table 2. Extreme cold daily mean temperature with a lag of 0–20 days (RR=0.49, 95% CI: 0.25–0.99) and a lag of 0–25 days (RR=0.59, 95% CI: 0.37–0.95) were related to a lower risk of daily CAD hospital admissions. Similarly, moderate cold daily mean temperature with a lag of 0–20 days (RR=0.56, 95% CI: 0.31–0.99) and a lag of 0–25 days (RR=0.65, 95% CI: 0.44–0.95) were linked to a lower risk of daily CAD hospital admissions. For hot temperature, moderate heat daily mean temperature with a lag of 0–20 days (RR=1.80, 95% CI: 1.01–3.20) and a lag of 0–25 days (RR=1.54, 95% CI: 1.05–2.27) were associated with a higher risk of daily CAD hospital admissions. Similarly, extreme heat daily mean temperature with a lag of 0–20 days (RR=2.02, 95% CI: 1.01–4.04) and a lag of 0–25 days (RR=1.68, 95% CI: 1.06–2.67) were related to a higher risk of daily CAD hospital admissions. Figure 1 illustrates the three-dimensional plots of the lag RR on daily CAD hospital admission, with daily mean temperature referenced at 20 °C. A nonlinear relationship between daily mean temperature and daily CAD hospital admission was found. Figure 2 shows the lagged effects of daily mean temperature on the daily CAD hospital admissions. The lagged effects showed an “S” shape relationship between daily mean temperature (extreme cold, moderate cold, moderate heat, and extreme heat) and daily CAD hospital admissions. However, statistical significance was found only for the daily mean temperature with a lag of 0–20 days and a lag of 0–25 days.
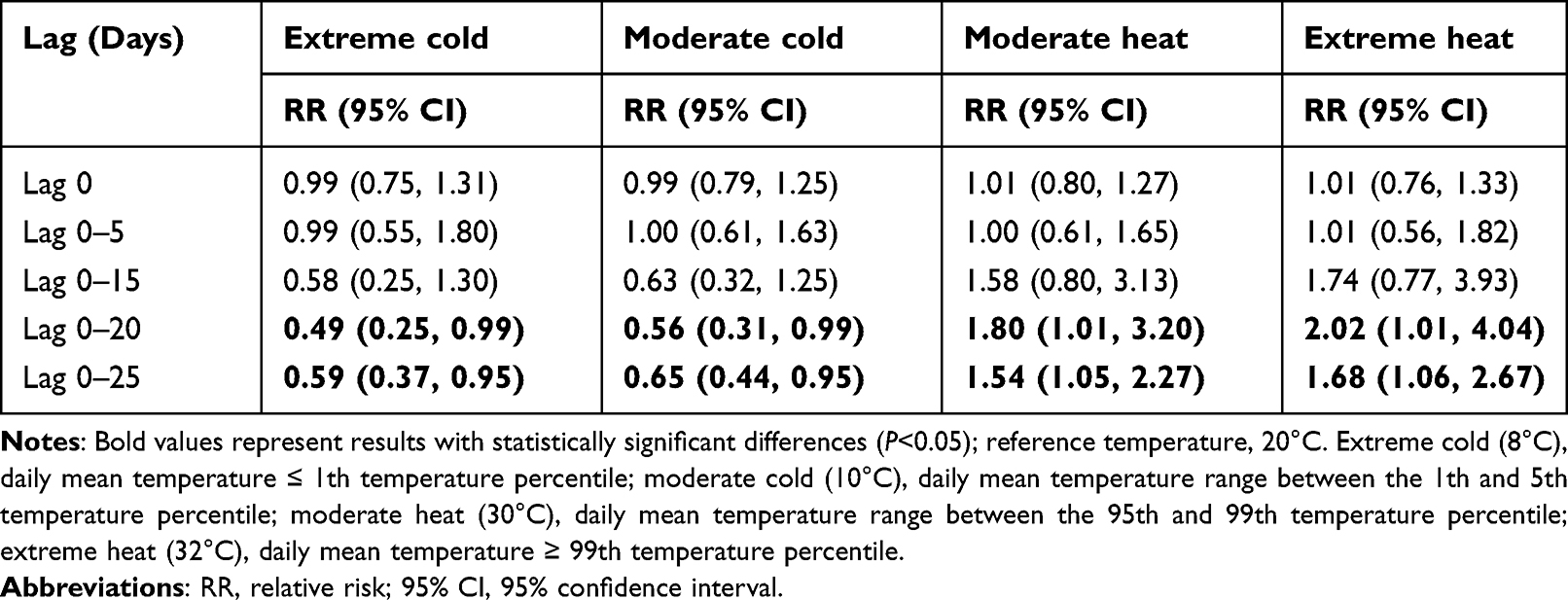 |
Table 2 The Cumulative Effect of Daily Mean Temperature on Daily Coronary Artery Disease (CAD) Hospital Admissions |
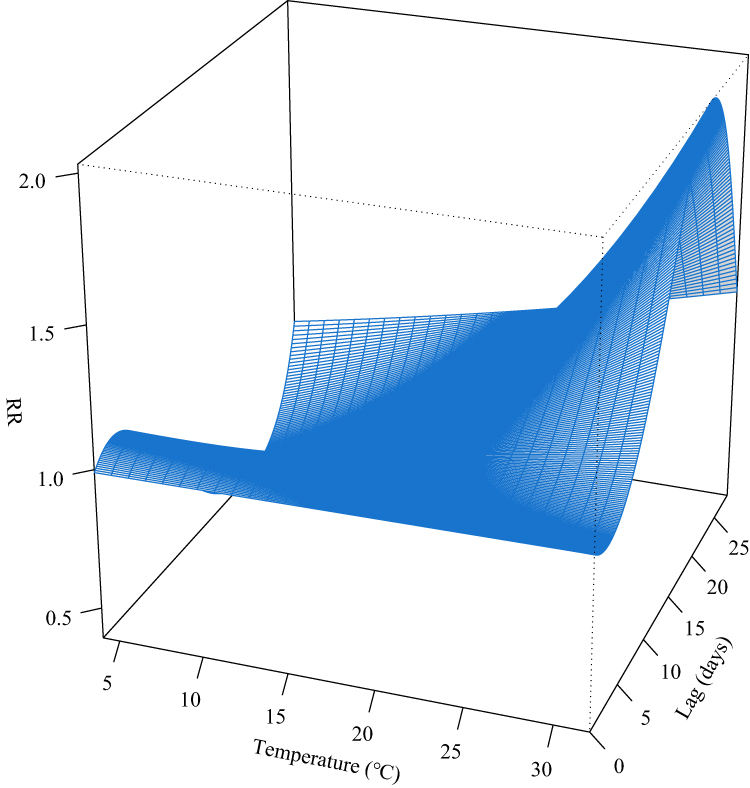 |
Figure 1 Three-dimensional plots of the lag relative risk (RR) on daily coronary artery disease (CAD) hospital admission compared with that of a reference value of 20 °C. |
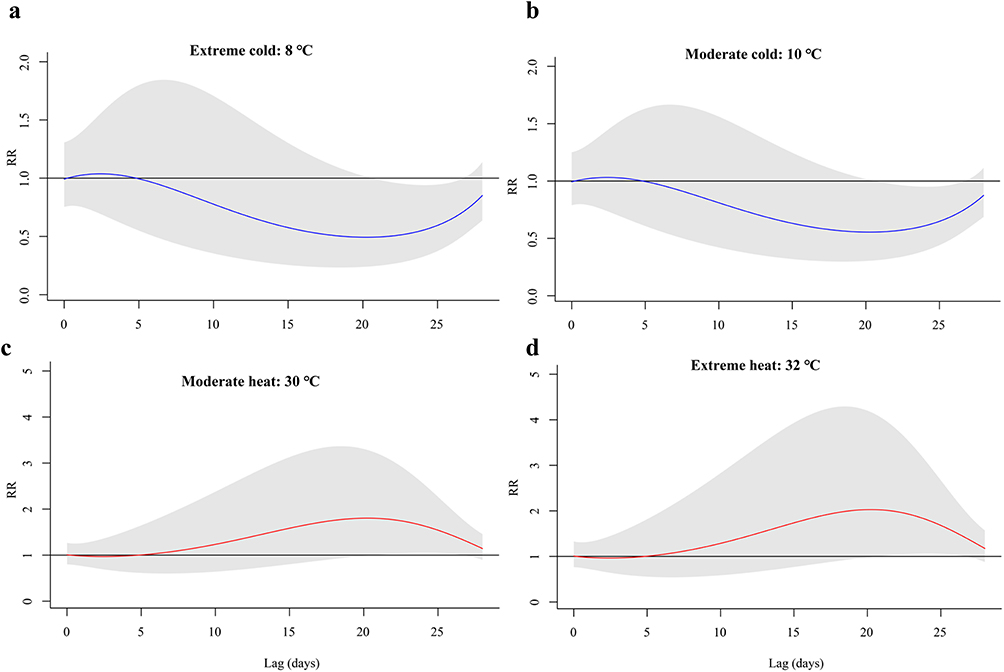 |
Figure 2 The lagged effects of daily mean temperature on the daily coronary artery disease (CAD) hospital admissions. (a) extreme cold (8°C); (b) moderate cold (10°C); (c) moderate heat (30°C); (d) extreme heat (32°C). Reference temperature, 20°C; extreme cold (8°C), daily mean temperature ≤ 1th temperature percentile; moderate cold (10°C), daily mean temperature range between the 1th and 5th temperature percentile; moderate heat (30°C), daily mean temperature range between the 95th and 99th temperature percentile; extreme heat (32°C), daily mean temperature ≥ 99th temperature percentile. |
Stratified Analyses Based on Gensini Score and Severity of Lesions
The stratified analyses of the lagged effect of daily mean temperature on the daily CAD hospital admissions were shown in Table 3. For patients with different Gensini scores, the lagged effect of daily mean temperature on the daily CAD hospital admissions was observed only in patients with Gensini scores ≤39 (tertile 1). Specifically, extreme cold and moderate cold daily mean temperature with a lag of 0, 0–5, 0–15, 0–20, and 0–25 days were linked to a lower risk of daily CAD hospital admissions, whereas moderate heat and extreme heat daily mean temperature with a lag of 0, 0–5, 0–15, 0–20, and 0–25 days were associated with a higher risk of daily CAD hospital admissions. For cold temperature, the lowest RR values were found for extreme cold (RR=0.00, 95% CI: 0.00–0.41) and moderate cold (RR=0.01, 95% CI: 0.00–0.48) daily mean temperatures with a lag of 0–15 days. For hot temperature, the highest RR values were observed for moderate heat (RR=90.02, 95% CI: 2.10–3854.68) and extreme heat (RR=221.42, 95% CI: 2.44–20,099.56) daily mean temperatures with a lag of 0–15 days, but their 95% CI intervals were unusually large.
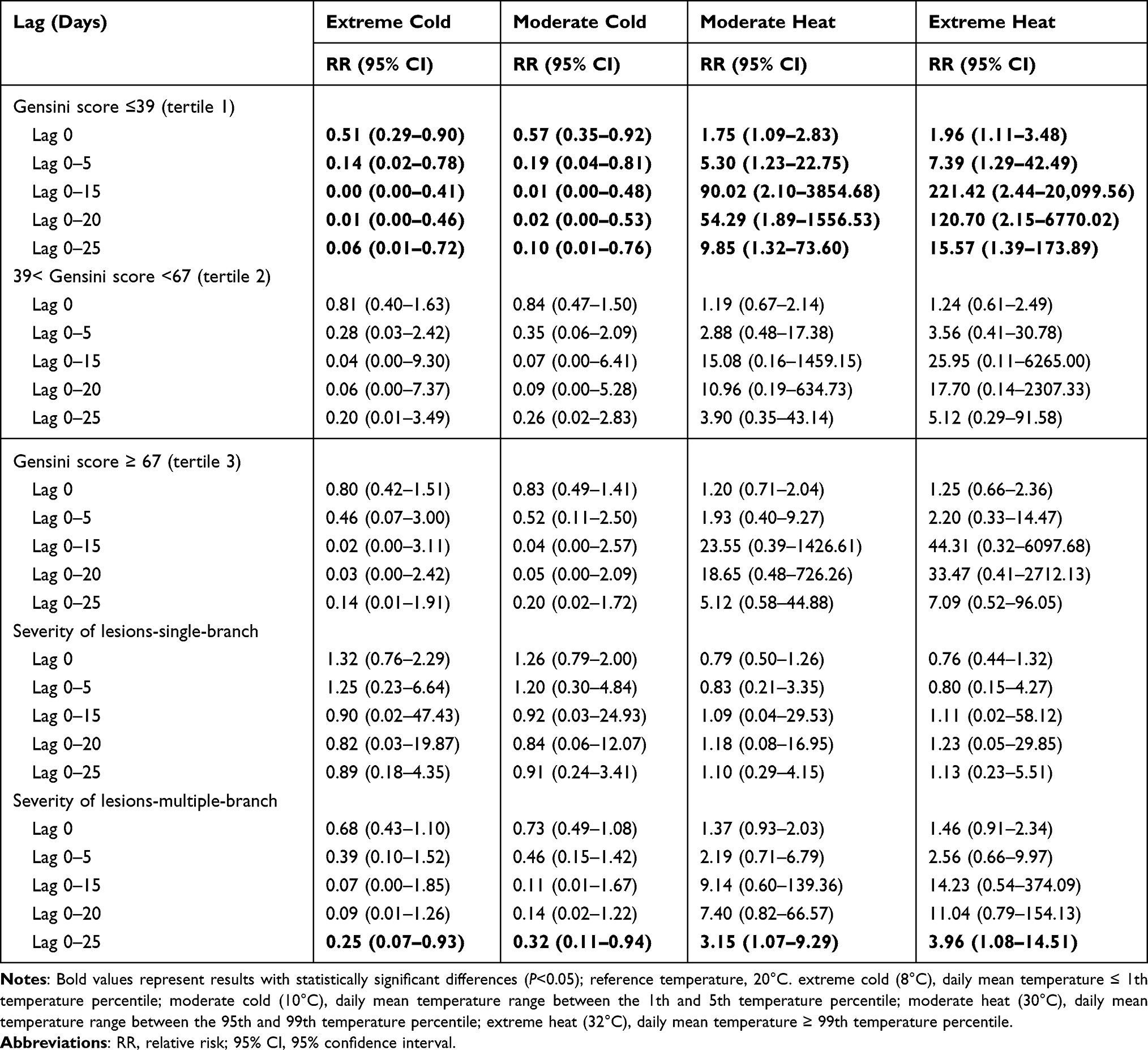 |
Table 3 Stratified Analysis of the Lagged Effect of Daily Mean Temperature on the Daily Coronary Artery Disease (CAD) Hospital Admissions |
For patients with different severity of lesions, extreme cold (RR=0.25, 95% CI: 0.07–0.93) and moderate cold (RR=0.32, 95% CI: 0.11–0.94) daily mean temperatures with a lag of 0–25 days were associated with a lower risk of daily CAD hospital admissions only in patients with multiple-branch lesions, whereas moderate heat (RR=3.15, 95% CI: 1.07–9.29) and extreme heat (RR=3.96, 95% CI: 1.08–14.51) daily mean temperatures with a lag of 0–25 days were related to a higher risk of daily CAD hospital admissions.
Discussion
This study explored the effect of daily mean temperature on the daily CAD hospital admissions in the southeast coast of China. Extreme cold (8°C) and moderate cold (10°C) daily mean temperatures with a lag of 0–20 and 0–25 days were correlated with a lower risk of daily CAD hospital admissions, whereas moderate heat (30°C) and extreme heat (32°C) daily mean temperatures with a lag of 0–20 and 0–25 days were correlated with a higher risk of daily CAD hospital admissions. Further analysis demonstrated the relationship between daily mean temperature and daily CAD hospital admissions was only significant in patients with Gensini score ≤ tertile 1 (39 scores) or multiple-branch lesions.
The cumulative and delayed effects of temperature on cardiovascular diseases have been found in many studies.15,23,24 Wang et al found a “J” shaped relationship between temperature and hospitalization risk of cardiovascular diseases in western China, with both low and high temperatures increasing the hospitalization risk.24 Mohammad et al demonstrated that a 7.4 °C increase in temperature was correlated with a 2.8% reduction in the risk of myocardial infarction in Sweden.23 In China, previous studies on temperature and cardiovascular disease were mainly in the northwest and inland areas.15–17 Chen et al reported climate differences in the risk and burden of death from main cardiopulmonary diseases.14 Therefore, the current study explored the effect of daily mean temperature on daily CAD hospital admissions in the southeast coast of China. Our results found cold daily mean temperatures with a lag of 0–20 and 0–25 days were correlated with a lower risk of daily CAD hospital admissions, whereas hot daily mean temperatures were linked to a higher risk of daily CAD hospital admissions. The effect of cold daily mean temperature on cardiovascular disease in our results is inconsistent with previous studies,24 probably because the extreme cold and moderate cold temperatures in our study are 8 °C and 10 °C, respectively, whereas the extreme cold temperature in previous studies may reach −15 °C. This suggests that the adverse effects of hot temperature lag on CAD should be prevented in the southeast coast of China. The possible mechanisms of temperature on cardiovascular diseases have been guessed in previous studies. Hot temperature initiates cardiovascular responses to passive heat stress and exogenous heat gain, which are overlapping and complex, with potential systemic effects.25 When heat gain exceeds the body’s ability to dissipate heat, a series of pathological events may lead to cardiovascular damage.26,27 Sweating and increased skin blood flow can lead to water loss and dehydration, with a corresponding decrease in plasma volume, increased concentrations of red blood cells and other blood components, increased blood viscosity, and elevated cholesterol concentrations, which may cause thromboembolism.28 The effects of cold temperature on the cardiovascular system are usually associated with potential complications of increased cardiovascular risk that involve changes in the autonomic nervous system, blood pressure, thermogenesis, inflammatory response, and oxidative stress.14,29,30
We further analyzed the effect of daily mean temperature on the daily CAD hospital admissions based on the severity of CAD. The results demonstrated that the relationship between daily mean temperature and daily CAD hospital admissions was only significant in patients with a Gensini score ≤ tertile 1 (39 scores). The effect of daily mean temperature on the daily CAD hospital admissions was more significant in patients with mild disease, possibly because the burden of the disease itself made the effect of temperature on admission in patients with less pronounced in patients with severe disease. In addition, seasons and air pollution have been reported to affect cardiovascular disease. The study by Bhatnagar reported that seasonal changes alter sunlight exposure, physical activity, and food intake behavior and that these changes may affect cardiovascular function and disease by altering physiological responses and metabolism.5 Several studies have found a possible combined effect of air pollutants and climatic factors on cardiovascular diseases.31,32 Therefore, our study used “Strata” and “AQI” to consider the effects of season and air pollution, respectively. In addition, the 95% CIs of some results were abnormally large in the subgroup analyses, which may be caused by the small sample size of the subgroups. Thus, prospective large-sample studies may be needed in subsequent studies.
This study analyzed the effect of daily mean temperature on daily CAD hospital admissions in Fuzhou City, which may fill a gap in the effect of temperature on cardiovascular disease in the southeastern coastal region of China. However, this study has some limitations. First, although we considered the impact of air pollutants through AQI, we did not assess the effect of specific air pollutants such as PM2.5, SO2, CO, and NO2. However, previous studies have found that air pollutants may have little impact on the main results in China.33,34 Second, we included hospitalized patients with CAD who underwent percutaneous coronary intervention, which may affect the inference of the results to all CAD patients. Third, we did not explore the effect of mean air temperature on different subtypes of CAD, which may require studies.
Conclusions
In this study, we explored the effect of daily mean temperature on daily CAD hospital admissions in the southeast coast of China (Fuzhou). The results showed that cold daily mean temperatures with a lag of 0–20 and 0–25 days were associated with a lower risk of daily CAD hospital admissions in Fuzhou, while hot daily mean temperatures with a lag of 0–20 and 0–25 days were related to a higher risk of daily CAD hospital admissions. In addition, the effect of daily mean temperature on the daily CAD hospital admissions may be more significant in patients with mild CAD.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board of Fujian Provincial Hospital (approval number: K2021-01-035), and all participants provided informed consent. All study procedures were conducted in accordance with the guidelines of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: executive Summary: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(3):e4–e17. doi:10.1161/CIR.0000000000001039
2. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart Disease and Stroke Statistics-2023 Update: a Report From the American Heart Association. Circulation. 2023;147(8):e93–e621. doi:10.1161/CIR.0000000000001123
3. Malakar AK, Choudhury D, Halder B, Paul P, Uddin A, Chakraborty S. A review on coronary artery disease, its risk factors, and therapeutics. J Cell Physiol. 2019;234(10):16812–16823. doi:10.1002/jcp.28350
4. Patel JV, Vyas A, Cruickshank JK, et al. Impact of migration on coronary heart disease risk factors: comparison of Gujaratis in Britain and their contemporaries in villages of origin in India. Atherosclerosis. 2006;185(2):297–306. doi:10.1016/j.atherosclerosis.2005.06.005
5. Bhatnagar A. Environmental Determinants of Cardiovascular Disease. Circ Res. 2017;121(2):162–180. doi:10.1161/CIRCRESAHA.117.306458
6. Hedlund E, Kaprio J, Lange A, et al. Migration and coronary heart disease: a study of Finnish twins living in Sweden and their co-twins residing in Finland. Scand J Public Health. 2007;35(5):468–474. doi:10.1080/14034940701256875
7. Feigin VL, Roth GA, Naghavi M, et al. Global burden of stroke and risk factors in 188 countries, during 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016;15(9):913–924. doi:10.1016/S1474-4422(16)30073-4
8. Giorgini P, Di Giosia P, Petrarca M, Lattanzio F, Stamerra CA, Ferri C. Climate Changes and Human Health: a Review of the Effect of Environmental Stressors on Cardiovascular Diseases Across Epidemiology and Biological Mechanisms. Curr Pharm Des. 2017;23(22):3247–3261. doi:10.2174/1381612823666170317143248
9. Biondi-Zoccai G, Frati G, Gaspardone A, et al. Impact of environmental pollution and weather changes on the incidence of ST-elevation myocardial infarction. Eur J Prev Cardiol. 2021;28(13):1501–1507. doi:10.1177/2047487320928450
10. Aklilu D, Wang T, Amsalu E, et al. Short-term effects of extreme temperatures on cause specific cardiovascular admissions in Beijing, China. Environ Res. 2020;186:109455. doi:10.1016/j.envres.2020.109455
11. Alahmad B, Khraishah H, Royé D, et al. Associations Between Extreme Temperatures and Cardiovascular Cause-Specific Mortality: results From 27 Countries. Circulation. 2023;147(1):35–46. doi:10.1161/CIRCULATIONAHA.122.061832
12. Redfors B, Simonato M, Chen S, et al. Ambient temperature and infarct size, microvascular obstruction, left ventricular function and clinical outcomes after ST-segment elevation myocardial infarction. Coron Artery Dis. 2022;33(2):81–90. doi:10.1097/MCA.0000000000001099
13. Hensel M, Stuhr M, Geppert D, Kersten JF, Lorenz J, Kerner T. Relationship between ambient temperature and frequency and severity of cardiovascular emergencies: a prospective observational study based on out-of-hospital care data. Int J Cardiol. 2017;228:553–557. doi:10.1016/j.ijcard.2016.11.155
14. Chen R, Yin P, Wang L, et al. Association between ambient temperature and mortality risk and burden: time series study in 272 main Chinese cities. BMJ. 2018;363:k4306. doi:10.1136/bmj.k4306
15. Cui L, Geng X, Ding T, Tang J, Xu J, Zhai J. Impact of ambient temperature on hospital admissions for cardiovascular disease in Hefei City, China. Int J Biometeorol. 2019;63(6):723–734. doi:10.1007/s00484-019-01687-0
16. Mokoena KK, Ethan CJ, Yu Y, Quachie AT. Interaction Effects of Air Pollution and Climatic Factors on Circulatory and Respiratory Mortality in Xi’an, China between 2014 and 2016. Int J Environ Res Public Health. 2020;17(23):9027. doi:10.3390/ijerph17239027
17. Zha Q, Chai G, Zhang ZG, Sha Y, Su Y. Effects of diurnal temperature range on cardiovascular disease hospital admissions in farmers in China’s Western suburbs. Environ Sci Pollut Res Int. 2021;28(45):64693–64705. doi:10.1007/s11356-021-15459-0
18. Su J, Li Z, Huang M, et al. Triglyceride glucose index for the detection of the severity of coronary artery disease in different glucose metabolic states in patients with coronary heart disease: a RCSCD-TCM study in China. Cardiovasc Diabetol. 2022;21(1):96. doi:10.1186/s12933-022-01523-7
19. Gensini GG. A more meaningful scoring system for determining the severity of coronary heart disease. Am J Cardiol. 1983;51(3):606. doi:10.1016/S0002-9149(83)80105-2
20. Wang KY, Zheng YY, Wu TT, Ma YT, Xie X. Predictive Value of Gensini Score in the Long-Term Outcomes of Patients With Coronary Artery Disease Who Underwent PCI. Front Cardiovasc Med. 2021;8:778615. doi:10.3389/fcvm.2021.778615
21. Gasparrini A, Armstrong B, Kenward MG. Distributed lag non-linear models. Stat Med. 2010;29(21):2224–2234. doi:10.1002/sim.3940
22. Hurtado-Díaz M, Cruz JC, Texcalac-Sangrador JL, et al. Short-term effects of ambient temperature on non-external and cardiovascular mortality among older adults of metropolitan areas of Mexico. Int J Biometeorol. 2019;63(12):1641–1650. doi:10.1007/s00484-019-01778-y
23. Mohammad MA, Koul S, Rylance R, et al. Association of Weather With Day-to-Day Incidence of Myocardial Infarction: a SWEDEHEART Nationwide Observational Study. JAMA Cardiol. 2018;3(11):1081–1089. doi:10.1001/jamacardio.2018.3466
24. Wang B, Chai G, Sha Y, Zha Q, Su Y, Gao Y. Impact of ambient temperature on cardiovascular disease hospital admissions in farmers in China’s Western suburbs. Sci Total Environ. 2021;761:143254. doi:10.1016/j.scitotenv.2020.143254
25. Liu J, Varghese BM, Hansen A, et al. Heat exposure and cardiovascular health outcomes: a systematic review and meta-analysis. Lancet Planet Health. 2022;6(6):e484–e495. doi:10.1016/S2542-5196(22)00117-6
26. Guo Y, Li S, Zhang Y, et al. Extremely cold and hot temperatures increase the risk of ischaemic heart disease mortality: epidemiological evidence from China. Heart. 2013;99(3):195–203. doi:10.1136/heartjnl-2012-302518
27. De Blois J, Kjellstrom T, Agewall S, Ezekowitz JA, Armstrong PW, Atar D. The Effects of Climate Change on Cardiac Health. Cardiology. 2015;131(4):209–217. doi:10.1159/000398787
28. Liu C, Yavar Z, Sun Q. Cardiovascular response to thermoregulatory challenges. Am J Physiol Heart Circ Physiol. 2015;309(11):H1793–H1812. doi:10.1152/ajpheart.00199.2015
29. Hintsala H, Kenttä TV, Tulppo M, et al. Cardiac repolarization and autonomic regulation during short-term cold exposure in hypertensive men: an experimental study. PLoS One. 2014;9(7):e99973. doi:10.1371/journal.pone.0099973
30. Cai J, Meng X, Wang C, et al. The cold effects on circulatory inflammation, thrombosis and vasoconstriction in type 2 diabetic patients. Sci Total Environ. 2016;568:271–277. doi:10.1016/j.scitotenv.2016.06.030
31. Huang CH, Lin HC, Tsai CD, Huang HK, Lian IB, Chang CC. The Interaction Effects of Meteorological Factors and Air Pollution on the Development of Acute Coronary Syndrome. Sci Rep. 2017;7:44004. doi:10.1038/srep44004
32. Tobaldini E, Iodice S, Bonora R, et al. Out-of-hospital cardiac arrests in a large metropolitan area: synergistic effect of exposure to air particulates and high temperature. Eur J Prev Cardiol. 2020;27(5):513–519. doi:10.1177/2047487319862063
33. Yang J, Ou CQ, Ding Y, Zhou YX, Chen PY. Daily temperature and mortality: a study of distributed lag non-linear effect and effect modification in Guangzhou. Environ Health. 2012;11:63. doi:10.1186/1476-069X-11-63
34. Zhao Q, Zhang Y, Zhang W, et al. Ambient temperature and emergency department visits: time-series analysis in 12 Chinese cities. Environ Pollut. 2017;224:310–316. doi:10.1016/j.envpol.2017.02.010
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.