Back to Journals » Psychology Research and Behavior Management » Volume 15
Effects of Character Strength-Based Intervention vs Group Counseling on Post-Traumatic Growth, Well-Being, and Depression Among University Students During the COVID-19 Pandemic in Guangdong, China: A Non-Inferiority Trial
Authors Yu Y ![]() , Chotipanvithayakul R
, Chotipanvithayakul R ![]() , Wichaidit W, Cai W
, Wichaidit W, Cai W
Received 26 January 2022
Accepted for publication 9 June 2022
Published 16 June 2022 Volume 2022:15 Pages 1517—1529
DOI https://doi.org/10.2147/PRBM.S359073
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Yulan Yu,1,2 Rassamee Chotipanvithayakul,2,3 Wit Wichaidit,2 Wei Cai1
1Department of Psychology/ Research Center for Quality of Life and Applied Psychology, Guangdong Medical University, Dongguan, People’s Republic of China; 2Department of Epidemiology, Faculty of Medicine, Prince of Songkla University, Hat Yai, Thailand; 3Research Center for Child and Youth Development, Faculty of Medicine, Prince of Songkla University, Hat Yai, Thailand
Correspondence: Rassamee Chotipanvithayakul, Department of Epidemiology, Faculty of Medicine, Prince of Songkla University, Hat Yai, Thailand, Tel +66 074-451165, Email [email protected] Wei Cai, Department of Psychology/Research Center for Quality of Life and Applied Psychology, Guangdong Medical University, Dongguan, People’s Republic of China, Tel +86 0769-2289-6266, Email [email protected]
Purpose: This study assessed the effects of character strengths-based invention (CSI) vs group counseling (GC) on mental health outcomes (ie, post-traumatic growth, well-being, and depression) among university students in Guangdong Province, China.
Materials and Methods: We conducted a randomized non-inferiority trial among 124 undergraduates at a medical university during the COVID-19 pandemic. We randomly allocated students to receive either CSI (n=62) or GC (n=62). A qualified psychologist delivered both activities on campus during two consecutive weekends with a total of 7.5 hours and also gave assignments to students during weekdays. We measured the outcomes at pre-intervention, post-intervention, and 1-month follow-up. We then analyzed data using descriptive statistics and a general linear mixed model.
Results: CSI and GC groups had similar baseline characteristics. Both CSI and GC experienced an increase in post-traumatic growth and well-being. The mean±SD scores for post-traumatic growth were significantly higher in CSI compared to GC groups (87.70± 14.22 vs 78.15± 20.72, respectively), whereas well-being scores were similar between CSI and GC (82.58± 16.57 vs 83.68± 15.59, respectively). Neither CSI nor GC experienced a reduction in depression scores.
Conclusion: CSI had non-inferior effects compared to GC with regards to improvement of post-traumatic growth and well-being during the COVID-19 pandemic. However, caveats regarding lack of blinding of investigator and limited generalizability should be considered in the interpretation of the study findings.
Keywords: character strength-based intervention, post-traumatic growth, well-being, depression, university student
Introduction
Changes associated with the coronavirus disease 2019 (COVID-19) pandemic have affected public mental health worldwide.1 University students have also been affected by COVID-related prevention and control measures, which function as sources of stress in addition to academic pressure and stresses related to relationships, health, and safety.2–4 In China, university students must strictly comply to COVID-19 prevention and control regulations, with mandatory isolation for those who tested positive for the disease. The campus of the infected individual would be closed. Students and staff would subsequently be prohibited from leaving their rooms, and all in-person classes and activities would be replaced with virtual classes and activities until the government approved the campus’s re-opening. Previous studies increased anxiety (26.60–71.75%), depression (42.32–80.57%), and stress (71.26%) among university students,3,5,6 as well as a significant decrease in well-being7 during the early COVID-19 pandemic. These students may need mental health interventions such as group counseling (GC), an effective method for improving psychological growth, self-esteem, well-being, and mental health,8–13 and reducing depression.8
However, GC requires the use of high-qualified leaders, such as specialized psychologists,14 and these professionals are commonly seconded to details supporting frontline health personnel and clients undergoing isolation. GC is thus difficult to access during the COVID-19 pandemic. Moreover, GC cannot support a large number of participants in each session,15–17 making scale-up for large populations difficult.
Character strengths-based intervention (CSI) is an intervention in positive psychology that aims to identify, use, and develop character strengths,18,19 and has been shown to protect against negative adversarial outcomes.20,21 Character strengths are defined as positive, trait-like capacities for thinking, feeling, and behaving in ways that benefit oneself and others.22 Everyone possesses all 24 character-strengths (such as zest, hope, love, kindness) in different degrees, so each person has a truly unique character strengths profile. These character strengths can be classified into six broad virtue categories (wisdom and knowledge, humanity, courage, transcendence, temperance, justice) across cultures and nations.23 Roughly three-to-five character-strengths fall into one virtue. CSI may help to promote hope, engagement,24,25 self-efficacy and self-esteem,26 class cohesion27 and reduce negative emotion or behavior,28 although some studies showed no significant effect on some negative mental health outcomes.18
Unlike GC, CSI does not require trained psychologists to be conducted. It can be conducted by a teacher or a healthcare worker given a manual to follow or having received training.29,30 It can even be administered by the participants themselves via completing exercises.31 Similar effects were also found in virtual CSI24,32,33 in which participants were trained according to tasks assigned by researchers. CSI can be administered to anywhere from 10 participants34 to 577 participants33 or more. CSI may provide a viable alternative to GC with regard to both access and scalability.
However, there is limited empirical evidence on the extent that CSI is at least non-inferior to GC. Character strengths were thought to be connected with positive outcomes and against negative outcomes20,21,35 in mental health. Well-being, including happiness, subjective well-being, and psychological well-being, is the second most common positive outcome related to CSI,18 while depression is the most common negative outcome related.20 Although the early COVID-19 pandemic brought much negative outcome on individuals,3,5,6 some have post-traumatic growth36 which refers to positive changes that share a common factor of struggling with trauma, adversity, or stress.37–40 The objective of our study was to assess non-inferiority of CSI compared to GC with regard to changes in post-traumatic growth, well-being, and depression among university students during the COVID-19 pandemic. Such information can provide needed empirical data in support of the use of CSI as an alternative to GC in resource-constrained settings and situations.
Materials and Methods
Study Design and Setting
We conducted a randomized non-inferiority trial at a medical university in Dongguan City, Guangdong Province, China, during February to July 2021. There was no positive case of COVID-19 in Dongguan City during the preparation, participant recruitment, and pre-testing phases of this study. However, two students at another university in Dongguan tested positive after the pre-testing phase. The COVID-19 prevention and control policy was then reinforced throughout the city. Students and staff underwent four screening tests of COVID-19, and all classes were to be discontinued if any positive case was detected. Except the investigators of this study, all other campus psychologists and counselors were seconded to serve those living in isolation.
Sample Size Calculation
We calculated the sample size by n4Studies application41 for this non-inferiority trial based on the assumed intervention vs control marginal differences. According to a similar randomized controlled trial, −6.0 points was for post-traumatic growth mean score.42 Based on a systematic review, −8.0 points was for well-being mean score,43 and −1.9 points was for depression mean score according to previous literature.44 We also assumed a 20% loss of follow-up, and made the calculation at 95% level of confidence and 80% power. Sample size calculation yielded the requirement of 62 participants in each group, ie, 124 participants in total for the study.
Study Participants
Our study participants included first and second year undergraduate students. The students were required to live on campus. Students above second years usually have practicum or internship rotation away from the university and thus they are inaccessible during the study period. Inclusion criterion was to be over the age of 18 years. Exclusion criteria included: 1) self-reported history of psychological crisis or psychiatric illness; and 2) self-reported history of receiving any treatment for psychiatric illness or mental health problems. We invited 140 students to participate in the study, among whom 124 students were eligible.
Interventions
The contents of character strengths-based intervention (CSI) included “signature strengths (top five character-strengths)”33,45 and “growth strengths”. Growth strengths refer to five character-strengths: 1) zest; 2) hope; 3) love of learning; 4) leadership; and 5) perspective, all of which showed a strong correlation with positive growth in a previous study.36 The structure of CSI was based on a character strengths-based “aware-explore-apply” model (AEA).19 We helped participants become aware of thesignature strengths and growth strengths they might be blind to, then co-explored these positive capacities through questions, reflections, activities, and then participants apply their signature and growth strengths in a new or different way via assignments.
There were in total 7.5 hours of intervention conducted by a researcher (Y.Y.). The first 6 hours intervention included getting to know each other, boosting motivation, knowledge of character strengths, awareness and co-exploring signature strengths, and awareness and co-exploring growth strengths. All these activities happened on a Saturday in May 2021. The other 1.5 hours intervention included checking the compliance, showing and sharing your new story, encouraging to maintain using signature and growth strengths, and summarizing the workshop and lesson learned. All these activities happened on a following Saturday in May, 2021. During this week intercession period, the participants were asked to apply signature and growth strengths in a new or different way as assignments and were reminded to complete these every night, and watched a video related to post-traumatic growth.
The structure and content of group counseling (GC) was based on an existing guideline for group counseling in university students,46 with some modification to suit the COVID-19 situation. The GC included four stages: 1) initiation stage; 2) transitory stage; 3) theme stage; and 4) lock up stage. The same as CSI, there was a total 7.5 hours intervention conducted by a researcher (Y.Y.). The content of GC was included in the first 6 hours of intervention: 1) creating a community atmosphere full of trust by ice breaking; understanding and sincerity by getting to know each other activity; 2) knowledge of GC and boost motivation; 3) knowing oneself further by looking for one’s advantages to build confidence; 4) emotional management; 5) coping with stress and frustration; and 6) contemplating one’s future. All these activities happened on a Sunday in May 2021. Another 1.5 hours intervention happened in a similar way to CSI, that is checking the compliance, showing and sharing stories according to the requirements of the GC group, encouraging them to continue using what they learned in the first 6 hours intervention, and summarizing the workshop and lesson learnt. All these activities happened on a following Sunday in May 2021. During this week intercession period, the participants were asked to contemplate their future and draw a self-portrayal and self-portrait (a new me) and watched a video related to improving mental health; they were also reminded to complete assignments.
Both groups received a total time of 7.5 hours intervention conducted by Y.Y., a researcher. The first 6 hours of intervention happened in a weekend (Saturday for CSI and Sunday for GC), and the other 1.5 hours happened the following weekend (Saturday for CSI and Sunday for GC). Both groups had to finish some assignments during the intercession period. The adherence was defined by completion of more than 80% of the assignments and assessed at the end of intervention. We gave students a small gift after the study’s completion.
Study Instrument
Our study instrument was a self-administered questionnaire that included general characteristics of the study participants (ie, gender, grade, self-reported academic achievement, family income per month, having siblings) as well as questions to measure the three main study outcomes: post-traumatic growth, well-being, and depression.
Measurement of Post-Traumatic Growth
We used the Posttraumatic Growth Inventory (PTGI)39 questions to measure post-traumatic growth. The PTGI consisted of 21 questions that assessed post-traumatic growth with a 6-point Likert scale in five domains: 1) New Possibilities; 2) Relating to Others; 3) Personal Strength; 4) Spiritual Change, and; 5) Appreciation of Life. For this study, we used the Chinese version of the PTGI with Cronbach’s α coefficient being 0.83 and the re-test coefficient after 2 weeks was 0.71.47
Measurement of Well-Being
We used the China version48 of the Well-being Index (WHO-5) instrument (1998 version)43 to measure participants’ well-being. The WHO-5 consisted of five self-reported questions with a sensitivity of 0.86 and specificity of 0.81. The raw score ranges from 0 to 25, with 0 representing worst possible and 25 representing best possible quality of life. We multiplied the raw score by 4 to obtain a standardized percentage score ranging from 0 to 100. A 10% change in standardized score between periods indicates a significant change.43
Measurement of Depression
We used the Centre for Epidemiologic Studies Depression Scale-Short Form (CES-D-SF) instrument to screen for depression. The instrument consisted of nine self-reported depression-related questions with 4-point Likert scales.49 We used the Chinese version of the CES-D-SF with internal consistency reliability ranging from 0.85 to 0.88.50
Study Procedures and Data Collection
After determining eligibility, giving information, and obtaining written informed consent of participants, we randomly allocated eligible students to receive either character strength-based intervention (CSI) or group counseling (GS) using computer generated numbers. The students were not aware of which intervention they were to receive. We then used the study instrument to measure the participants’ characteristics and study outcomes before the intervention was given (“Point 1”, ie, baseline), after the intervention was completed (“Point 2”, ie, post-intervention), and at 1 month follow-up (“Point 3”). We sent reminders to participants to complete their assignment in a timely manner each day during the intercession period and checked for their compliance at post-intervention.
Statistical Analysis
We used percentage to describe the baseline characteristics of participants in two groups. We then used general linear mixed model analyses to compare changes in all three outcomes (post-traumatic growth, well-being, and depression) between groups, with the baseline level of each outcome as a covariate. We described and assessed the significance of changes in the mean scores (95% CI) within each group comparing the baseline and the mean difference in these changes (95% CI) between groups at post-intervention and at 1 month follow-up using a linear mixed-effect model with participants as a random effect to allow for within-subject correlation of repeated measures over time. Fixed effects included the main effects and interactions with time (post-intervention and 1 month follow-up test). All analyses were based on an intention-to-treat (ITT) analysis approach.
Ethical Considerations
Investigators received ethical approval from the Human Research Ethics Committee, Faculty of Medicine, Prince of Songkla University, Hat Yai, Thailand (REC: 63-382-18-1). Investigators also received ethical approval from the Medical Ethics Committee, Affiliated Hospital of Guangdong Medical University (Approval number: PJ2020-097). This trial is registered on the Chinese Clinical Trial Registry (http://www.chictr.org.cn), Registration number ChiCTR2100045609. Our study complies with the Declaration of Helsinki.
Results
We recruited 140 students, and excluded 16 students due to a history of psychiatric illness (2 students) and history of psychiatric treatment (14 students), and 124 students remained as study participants (n=124 students), and we randomly allocated 62 students to each group. However, three participants left before intervention after allocation because of emergency, and two and three participants became lost to follow-up after 1 month intervention test, respectively. The flow diagram of the study is shown in Figure 1. Due to only 6.5% (8/124) loss of follow-up rate, findings based on the intention-to-treat (ITT) analyses were similar to the per protocol analyses. We present here only the results of ITT analyses. Fifty-one out of 57 students (89.47%) in the CSI group and 52 out of 59 (88.14%) in the GC group completed more than 80% of the assignments. The common reasons for incompletion were lack of time, being physically unwell, and not knowing how to finish the assignments.
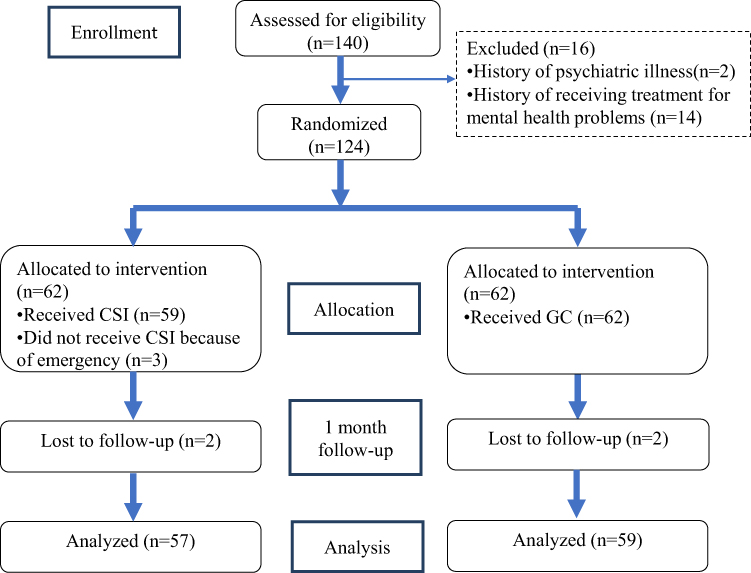 |
Figure 1 Flow diagram of the study. |
Both CSI and GC groups had similar demographic and socio-demographic characteristics (Table 1). There were almost twice as many females as males, and almost twice as many freshmen as sophomores. Over 70% of participants in both groups had one or more siblings.
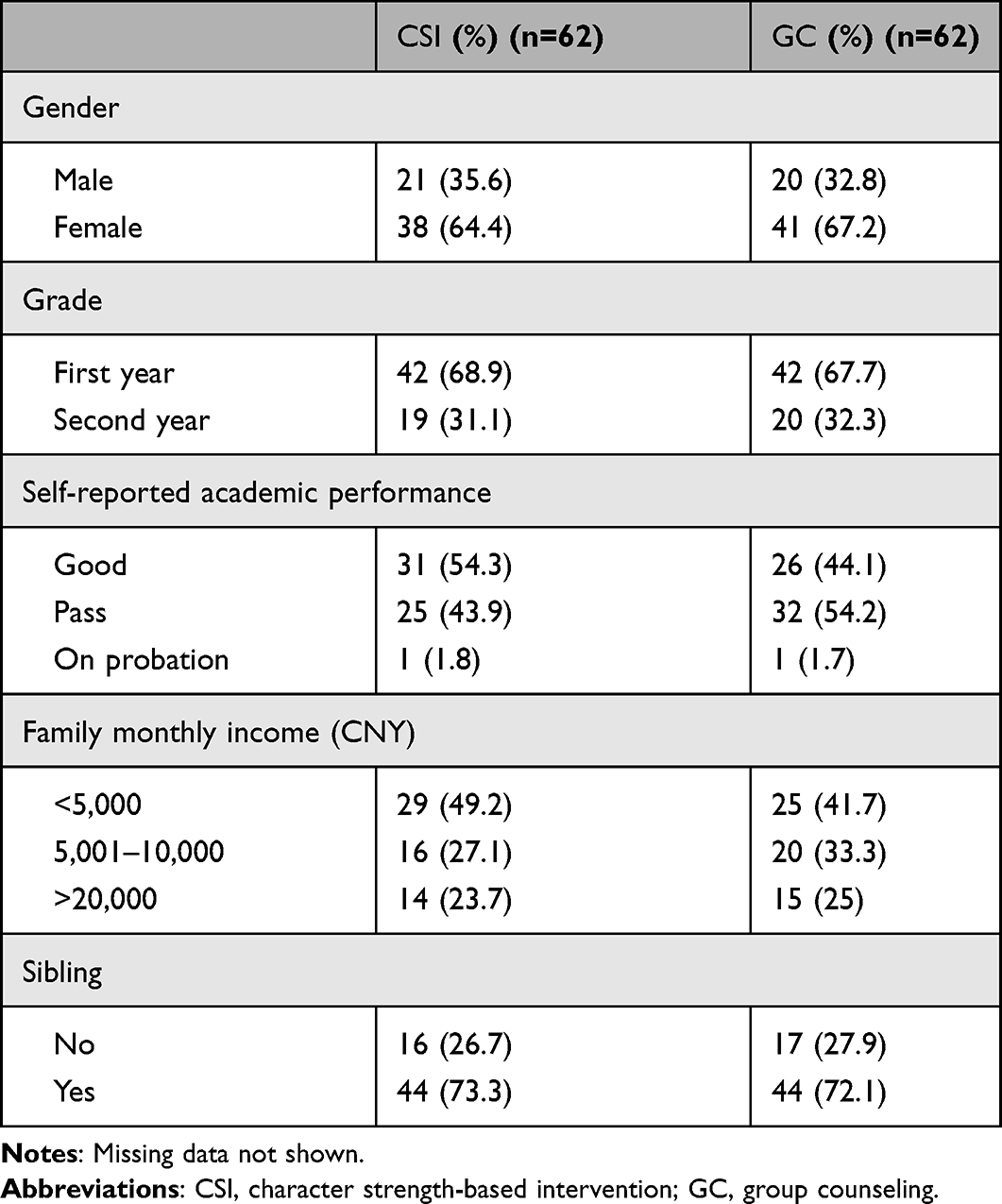 |
Table 1 Baseline Demographic and Socio-Economic Characteristics of the Study Participants Included in the Analysis |
Participants had relatively low score of post-traumatic growth (Figure 2) and well-being (Figure 3) at baseline and there was significant increasing after intervention which was maintained after 1 month follow-up. There was a significant difference between the CSI and GC group on post-traumatic growth at the post-intervention point (p<0.01), but no significant difference at 1 month follow-up (Figure 2). There were no significant differences between the two groups on well-being at both post-intervention and 1 month follow-up. The mean values depression score in both groups were close to the cut-off for depression (≥10 points) (Figure 4). This accounted for a 29.3% depressive tendency and 13.0% of high-risk depression. The average scores of the two groups were similar and did not significantly change over time.
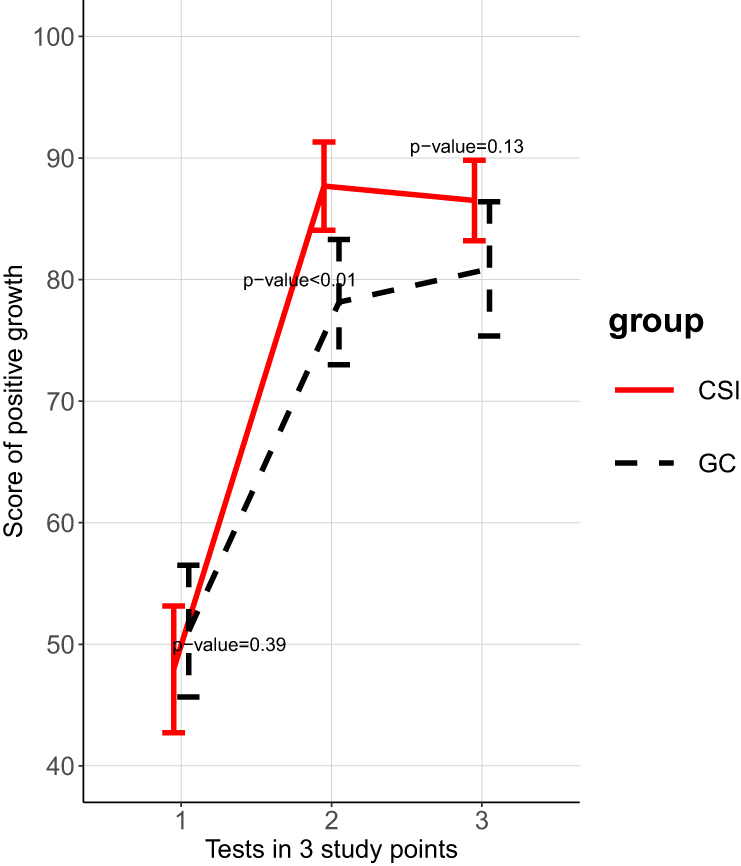 |
Figure 2 Mean and 95% CI of positive growth score between two groups. |
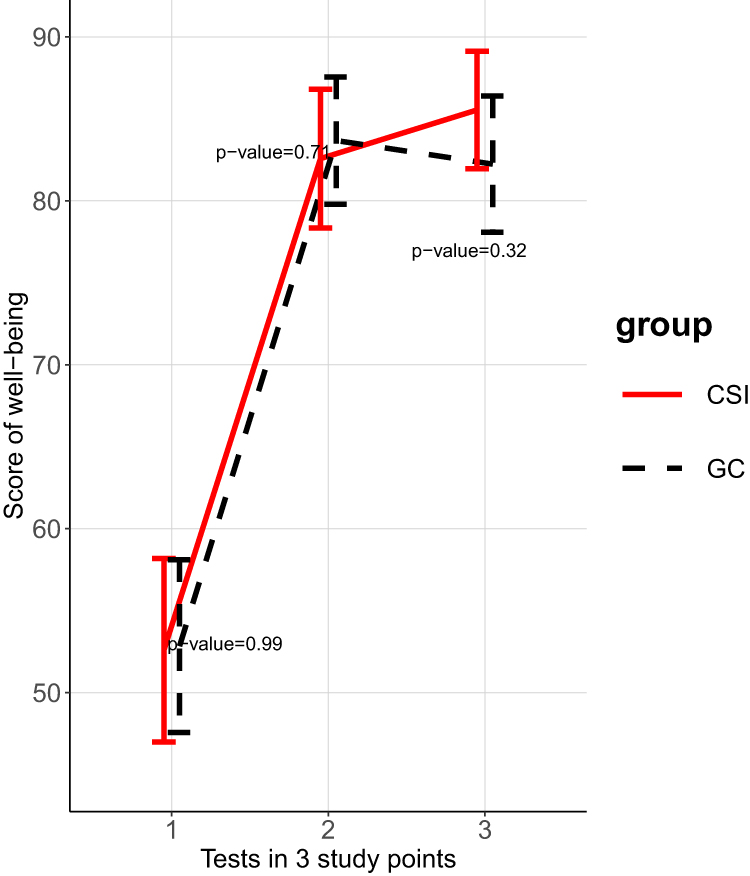 |
Figure 3 Mean and 95% CI of well-being score between two groups. |
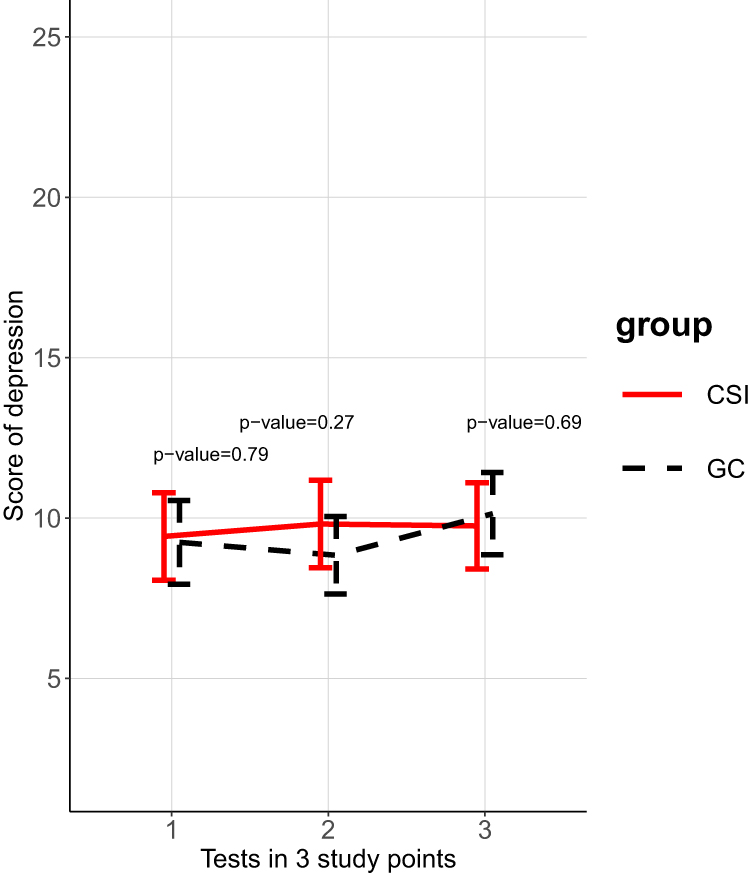 |
Figure 4 Mean and 95% CI of depression score between two groups. |
The linear mixed effect model (Table 2) showed significant improvements in post-traumatic growth and well-being over time. However, this effect was not observed for depression. The effect of CSI was not inferior to GC for well-being. Students who received CSI had significantly greater change in post-traumatic growth than students who received GC at post-intervention (p<0.001) and at 1-month follow-up (p=0.021) (Table 2). Neither CSI nor GC had significant effects on depression at post-intervention and at 1 month follow-up.
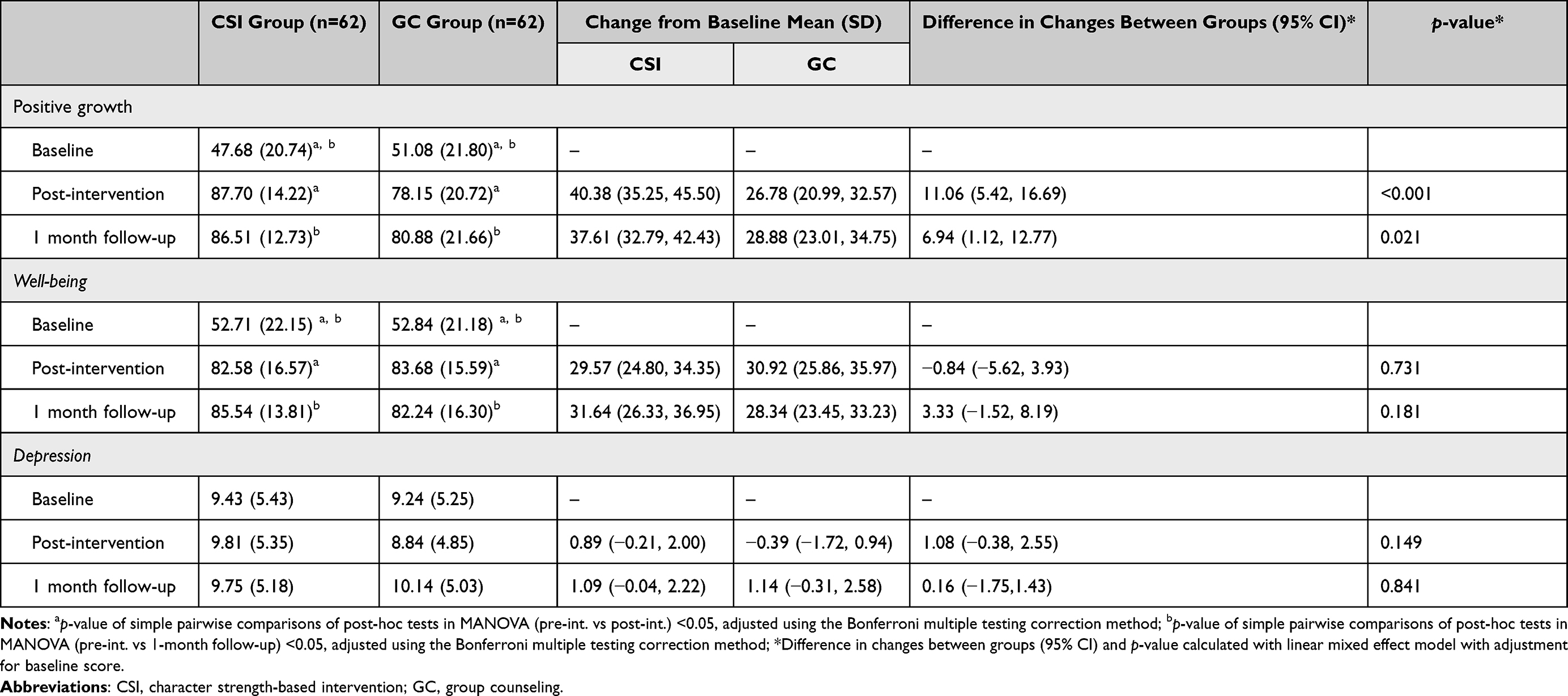 |
Table 2 Outcomes Scores at Three Study Points, Mean Changes in Each Group Comparing to Baseline and Adjust Difference in Changes Between Groups |
Discussion
In this non-inferiority trial conducted during the COVID-19 pandemic, participants who received character strength-based intervention (CSI) had the same level of improvement in post-traumatic growth and well-being as participants who received conventional group counseling (GC). However, neither group had any significant reduction in depression scores. Improvement in post-traumatic growth in the CSI group was significantly greater than that in the GC group and remained high at 1 month follow-up. Well-being scores were moderately low at baseline and were significantly improved at post-intervention and at 1-month follow-up.
Post-traumatic growth is one of the important factors for thriving in adversity.51 A previous longitudinal study during the COVID-19 pandemic showed overall character strengths, especially virtue of humanity, were significantly associated with post-traumatic growth and virtue of transcendence was related to mental health among the adult population.52 Moreover, character strengths could help people cope with the threat from COVID-19.53 This RCT showed that character strength-based intervention could timely promote post-traumatic growth among university students. In addition to humanity and transcendence virtues,52 our previous study36 showed that wisdom and knowledge virtue (love of learning, perspective), courage (zest), as well as justice virtue (leadership) plays an important role for post-traumatic growth cultivation during the COVID-19 pandemic.
Well-being has been shown to be associated with quality-of-life and longevity.54,55 During the early COVID-19 pandemic, however well-being was lower.7 A number of studies showed signature strength intervention enhanced well-being among the general population.33,45,56 Our study added that CSI was still effective to promote well-being during the pandemic. This positive effect was maintained for at least 1 month. Character strength-based intervention (CSI) habituating and exerting one’s character strengths allows individuals to experience a sense of fulfillment or a feeling of self with vigor and authenticity, and results in positive functioning and well-being.57
However, our RCT did not show an effect on depression during the COVID-19 pandemic. A meta-analysis showed that signature strengths had a significant decreasing effect on depression with a weighted Hedges’ g=0.21.20 In most interventions on depression, the participants were asked to use signature strengths in a new or different way each day during 1 week and they had a significant decrease.20 Our CSI asked the participants to use signature strengths and growth strengths in a new or different way each day within a week as assignments. The differentiation is growth strengths added in the present study and then signature strengths may have less chance to be used, or growth strengths are interfering factors on decreasing depression. The CSI program may be further developed and tested for depression. We have to be aware that group counseling also had no effect on depression in the present study, although conventionally group counseling is a useful intervention to decrease depression for university students.8 Depression among university students in our study (43%) and others (42.3–80.5%)58,59 were obviously high during the COVID-19 pandemic compared to the normal situation (21.2%),50 which may be one of the possible reasons leading to no decrease in depression in the present study. This suggested a screening and an appropriate intervention for this high-risk group.
Strengths and Limitations
The randomized trial design of our study with complete randomization allowed us to attribute the difference (or lack thereof) to the intervention rather than confounding. The relatively low loss-to-follow-up helped to reduce the presence of selection bias in our study findings. However, a number of limitations should be considered in the interpretation of our study findings. Firstly, there was only one qualified psychologist available during the study period, YY. The psychologist administered both CSI and GC and was not blinded to group allocation. However, the psychologist administered CSI and GC according to guidelines, and measured outcomes using self-reported instruments, which might have helped in reducing potential information bias in the study. Secondly, this study was conducted during the COVID-19 pandemic period in a city in southern China where strict, stress-inducing prevention and control measures were being implemented. These unique contexts may have limited the generalizability of the study findings.
Conclusion
A character strengths-based intervention, awareness, explore and apply of signature and growth strengths, showed short-term improvement and maintenance in post-traumatic growth and well-being, but no significant changes in depression among university students during the COVID-19 pandemic. The effects of character strengths-based intervention (CSI) on mental health outcomes among university students were non-inferior to those of group counseling (GC). The findings of this study provided useful information for relevant stakeholders. However, caveats regarding lack of blinding of investigator and limited generalizability should be considered in the interpretation of the study findings.
Data Sharing Statement
The data that support the findings of this study are available from now on in the following link: https://figshare.com/s/c6a2440c5849ca943aff as well as the introduction of the data.
Funding
This work was supported by the foundation of the 13th Five-Year Plan of Education Science of Guangdong Province (Moral Education Special Project), Grant No. 2020JKDY030.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Waters L, Algoe SB, Dutton J, et al. Positive psychology in a pandemic: buffering, bolstering, and building mental health. J Posit Psychol. 2021;17(3):1–21. doi:10.1080/17439760.2021.1940251
2. Husky MM, Kovess-Masfety V, Swendsen JD. Stress and anxiety among university students in France during Covid-19 mandatory confinement. Compr Psychiatry. 2020;102:152191. doi:10.1016/j.comppsych.2020.152191
3. Wang X, Hegde S, Son C, Keller B, Smith A, Sasangohar F. Investigating mental health of US college students during the COVID-19 pandemic: cross-sectional survey study. J Med Internet Res. 2020;22(9):e22817. doi:10.2196/22817
4. Yang C, Chen A, Chen Y. College students’ stress and health in the COVID-19 pandemic: the role of academic workload, separation from school, and fears of contagion. PLoS One. 2021;16(2):e0246676. doi:10.1371/journal.pone.0246676
5. Lyons Z, Wilcox H, Leung L, Dearsley O. COVID-19 and the mental well-being of Australian medical students: impact, concerns and coping strategies used. Australas Psychiatry. 2020;28(6):649–652. doi:10.1177/1039856220947945
6. Stein MB. COVID‐19 and anxiety and depression in 2020. Depress Anxiety. 2020;37(4):302. doi:10.1002/da.23014
7. Boateng GO, Doku DT, Enyan NIE, et al. Prevalence and changes in boredom, anxiety and well-being among Ghanaians during the COVID-19 pandemic: a population-based study. BMC Public Health. 2021;21:985. doi:10.1186/s12889-021-10998-0
8. Hu R, Chen J, Wang Y, Chen Z. Effectiveness of group training on depressive mood among college students: a meta-analysis. Chin J School Health. 2017;38(5):676–682.
9. Perusse R, Goodnough GE, Lee VV. Group counseling in the schools - Pérusse - 2009 - Psychology in the Schools - Wiley Online Library [Internet]. Psychol Sch. 2009;46(3):225–231. doi:10.1002/pits.20369
10. Shao J, Fan F. Status and trends of group counseling researches from 1996 to 2013 in China. Chin Ment Health J. 2015;29(4):258–263.
11. Wang Y, Tang X, Zhao Y, et al. Effectiveness of group counseling on well-being among college students: a Meta-analysis. Chin J School Health. 2016;37(7):1031–1036.
12. Zhang W, Yan T, Du Y, Liu X. Brief report: effects of solution-focused brief therapy group-work on promoting post-traumatic growth of mothers who have a child with ASD. J Autism Dev Disord. 2014;44(8):2052–2056. doi:10.1007/s10803-014-2051-8
13. Zhang X, Shi X, Xu S, Qiu J, Turel O, He Q. The effect of solution-focused group counseling intervention on college students’ internet addiction: a pilot study. Int J Environ Res Public Health. 2020;17(7):2519. doi:10.3390/ijerph17072519
14. Rybak C, Sathaye D, Deuskar M. Group counseling and satsang: learning from Indian group practices. J Spec Group Work. 2015;40(2):147–162. doi:10.1080/01933922.2015.1017064
15. Kim EK, Baek S, Woo JS, et al. Group counseling for medical students with drop-out experiences. Korean J Med Educ. 2013;25(1):23–28. doi:10.3946/kjme.2013.25.1.23
16. Kissen M. On becoming a group member: personal growth and effectiveness in group counseling. Int J Group Psychother. 2011;61(2):330–332. doi:10.1521/ijgp.2011.61.2.330
17. Li C, Ma C, Li P, Liang Z. The effect of model-based group counseling on the resiliency of disadvantaged adolescents from poor areas of china: a single-blind randomized controlled study. School Ment Health. 2021. doi:10.1007/s12310-021-09479-x
18. Kumar PA, Mohideen F. Strengths-based positive schooling interventions: a scoping review. Contemp School Psychol. 2021;25(1):86–98. doi:10.1007/s40688-019-00260-1
19. Niemiec RM. Character strengths interventions: a field guide for practitioners. Library of Congress Cataloging in Publication; 2017.
20. Schutte NS, Malouff JM. The impact of signature character strengths interventions: a meta‑analysis. J Happiness Stud. 2018;20(4):1179–1196.
21. Park N, Peterson C. Positive psychology and character strengths: application to strengths-based school counseling. Prof School Couns. 2008;12(2):2156759X0801200. doi:10.1177/2156759X0801200214
22. Peterson C, Seligman MEP. Character Strengths and Virtues: A Handbook and Classification. American Psychological Association; 2004:815.
23. Park N, Peterson C, Seligman MEP. Strengths of character and well-being. J Soc Clin Psychol. 2004;23(5):603–619. doi:10.1521/jscp.23.5.603.50748
24. Harzer C, Ruch W. Your strengths are calling: preliminary results of a web-based strengths intervention to increase calling. J Happiness Stud. 2016;17(6):2237–2256. doi:10.1007/s10902-015-9692-y
25. Madden W, Green S, Grant A. A pilot study evaluating strengths-based coaching for primary school students: enhancing engagement and hope. Int Coach Psychol Rev. 2010;Jan(6):71–83.
26. Toback RL, Graham-Bermann SA, Patel PD. Outcomes of a character strengths–based intervention on self-esteem and self-efficacy of psychiatrically hospitalized youths. Psychiatr Serv. 2016;67(5):574–577. doi:10.1176/appi.ps.201500021
27. Quinlan D, Vella-Brodrick DA, Gray A, Swain N. Teachers matter: student outcomes following a strengths intervention are mediated by teacher strengths spotting. J Happiness Stud. 2019;20(8):2507–2523. doi:10.1007/s10902-018-0051-7
28. Kim HR, Kim SM, Hong JS, et al. Character strengths as protective factors against depression and suicidality among male and female employees. BMC Public Health. 2018;18(1):1084. doi:10.1186/s12889-018-5997-1
29. Khanna P, Singh K, Proctor C. Exploring the impact of a character strengths intervention on well-being in Indian classrooms. School Ment Health. 2021;13(4):819–831. doi:10.1007/s12310-021-09450-w
30. Yan T, Chan CWH, Chow KM, Zheng W, Sun M. A systematic review of the effects of character strengths-based intervention on the psychological well-being of patients suffering from chronic illnesses. J Adv Nurs. 2020;76(7):1567–1580. doi:10.1111/jan.14356
31. Kloos N, Drossaert CHC, Bohlmeijer ET, Westerhof GJ. Online positive psychology intervention for nursing home staff: a cluster-randomized controlled feasibility trial of effectiveness and acceptability. Int J Nurs Stud. 2019;98:48–56. doi:10.1016/j.ijnurstu.2019.06.004
32. Proyer RT, Ruch W, Buschor C. Testing strengths-based interventions: a preliminary study on the effectiveness of a program targeting curiosity, gratitude, hope, humor, and zest for enhancing life satisfaction. J Happiness Stud. 2013;14(1):275–292. doi:10.1007/s10902-012-9331-9
33. Seligman MEP, Peterson C. Positive psychology progress: empirical validation of interventions. Am Psychol. 2005;60(5):410–421. doi:10.1037/0003-066X.60.5.410
34. Andrewes HE, Walker V, O’Neill B. Exploring the use of positive psychology interventions in brain injury survivors with challenging behaviour. Brain Injury. 2014;28(7):965–971. doi:10.3109/02699052.2014.888764
35. Niemiec RM. Six functions of character strengths for thriving at times of adversity and opportunity: a theoretical perspective. Appl Res Qual Life. 2020;15(2):551–572. doi:10.1007/s11482-018-9692-2
36. Yu Y, Chotipanvithayakul R, Kuang H, Wichaidit W, Wan C. Associations between mental health outcomes and adverse childhood experiences and character strengths among university students in southern China; 2022.
37. Linley PA, Joseph S. Positive change following trauma and adversity: a review. J Traum Stress. 2004;17(1):11–21. doi:10.1023/B:JOTS.0000014671.27856.7e
38. Russo-Netzer P, Moran G. Positive growth from adversity and beyond: insights gained from cross-examination of clinical and nonclinical samples. Am J Orthopsychiatry. 2018;88(1):59–68. doi:10.1037/ort0000224
39. Tedeschi RG, Calhoun LG. The posttraumatic growth inventory: measuring the positive legacy of trauma. J Traum Stress. 1996;9(3):455–471. doi:10.1002/jts.2490090305
40. Fortune D, Richards H, Griffiths C, Main C. Adversarial growth in patients undergoing treatment for psoriasis: a prospective study of the ability of patients to construe benefits from negative events. Psychol Health Med. 2005;10(1):44–56. doi:10.1080/13548500512331315352
41. Ngamjarus C, Chongsuvivatwong V, Mcneil E. n4Studies: sample size calculation for an epidemiological study on a smart device. Siriraj Med J. 2016;68:160–170.
42. van der Spek N, Vos J, van Uden-Kraan CF, et al. Efficacy of meaning-centered group psychotherapy for cancer survivors: a randomized controlled trial. Psychol Med. 2017;47(11):1990–2001. doi:10.1017/S0033291717000447
43. Topp CW, Østergaard SD, Søndergaard S, The BP. WHO-5 well-being index: a systematic review of the literature. PPS. 2015;84(3):167–176.
44. Ming Z, Chen Z, Liu Y, Chen G. Status and influencing factors of mental health among veterans in China. Chin J Public Health. 2022;38(2):167–171.
45. Proyer RT, Gander F, Wellenzohn S, Ruch W. Strengths-based positive psychology interventions: a randomized placebo-controlled online trial on long-term effects for a signature strengths- vs. a lesser strengths-intervention. Front Psychol. 2015;06. doi:10.3389/fpsyg.2015.00456
46. Fan F, He J. Group psychological counseling. Shanghai: East China Normal University Press; 2010.
47. Geng Y, Xu Q, Liu H, Xu X. Reliability and validity analysis of The Chinese version of the post-traumatic growth inventory in multiple trauma survivors. Chin J Nurs. 2011;46(10):1003–1005.
48. Fung S, Kong CYW, Liu Y, et al. Validity and psychometric evaluation of the Chinese Version of the 5-Item WHO well-being index. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.872436
49. Martens MP, Parker JC, Smarr KL, et al. Development of a shortened center for epidemiological studies depression scale for assessment of depression in rheumatoid arthritis. Rehabilitat Psychol. 2006;51(2):135–139. doi:10.1037/0090-5550.51.2.135
50. He J, Chen Z, Guo F, Zhang J, Yang Y, Wang Q. Short form of Chinese version of Center for epidemiologic studies depression scale. Chin J Behav Med Brain Sci. 2013;22(12):1133–1136.
51. Baños RM, Garcés JJ, Miragall M, Herrero R, Vara MD, Soria-Olivas E. Exploring the heterogeneity and trajectories of positive functioning variables, emotional distress, and post-traumatic growth during strict confinement due to COVID-19. J Happiness Stud. 2021;2:1–26.
52. Casali N, Feraco T, Meneghetti C. Character strengths sustain mental health and post-traumatic growth during the COVID-19 pandemic. A longitudinal analysis. Psychol Health. 2021;21:1–17. doi:10.1080/08870446.2021.1952587
53. Subhashini P. Character strengths for post COVID-19 growth. JCGR. 2020;37(1):3–18.
54. Diaz Hernandez L, Giezendanner S, Fischer R, Zeller A. The effect of COVID-19 on mental well-being in Switzerland: a cross-sectional survey of the adult Swiss general population. BMC Fam Pract. 2021;22(1):181. doi:10.1186/s12875-021-01532-7
55. Liu Z, Li L, Huang J, et al. Association between subjective well-being and exceptional longevity in a longevity town in China: a population-based study. Age. 2014;36(3):9632. doi:10.1007/s11357-014-9632-5
56. Proyer RT, Gander F, Wellenzohn S, Ruch W. Positive psychology interventions in people aged 50–79 years: long-term effects of placebo-controlled online interventions on well-being and depression. Aging Ment Health. 2014;18(8):997–1005. doi:10.1080/13607863.2014.899978
57. Proctor C, Maltby J, Linley PA. Strengths use as a predictor of well-being and health-related quality of life. J Happiness Stud. 2011;12(1):153–169. doi:10.1007/s10902-009-9181-2
58. Chang J, Yuan Y, Wang D. [Mental health status and its influencing factors among college students during the epidemic of COVID-19]. Nan Fang Yi Ke Da Xue Xue Bao. 2020;40(2):171–176. Chinese. doi:10.12122/j.issn.1673-4254.2020.02.06
59. Wathelet M, Duhem S, Vaiva G, et al. Factors associated with mental health disorders among university students in France confined during the COVID-19 pandemic. JAMA Netw Open. 2020;3(10):e2025591. doi:10.1001/jamanetworkopen.2020.25591
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.