Back to Journals » Journal of Pain Research » Volume 19
Effects of Adding Local Anesthesia to General Anesthesia on Postoperative Analgesia in Patients Undergoing Laparoscopic Cholecystectomy: A Retrospective Cohort Study
Authors Zhong L, Wang R, Huang L
Received 14 January 2026
Accepted for publication 24 March 2026
Published 14 April 2026 Volume 2026:19 592754
DOI https://doi.org/10.2147/JPR.S592754
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Lili Zhong,1 Rui Wang,2 Liquan Huang1
1Department of Anesthesiology, Weiyuan County People’s Hospital, Neijiang, Sichuan, 642450, People’s Republic of China; 2Department of Anesthesiology, Leshan Municipal People’s Hospital, Leshan, Sichuan, 614099, People’s Republic of China
Correspondence: Lili Zhong, Email [email protected]
Objective: Postoperative pain remains a significant concern following laparoscopic cholecystectomy (LC). This study aimed to evaluate the effects of wound infiltration and intraperitoneal instillation of local anesthetics on postoperative analgesia.
Methods: This retrospective cohort study included 202 patients undergoing elective LC under standardized balanced general anesthesia between February 2023 and July 2025. Patients were divided into three groups based on the analgesic protocols they received: control group (Group C, n=54) receiving general anesthesia with routine patient-controlled intravenous analgesia (PCIA), local infiltration group (Group L, n=73) receiving additional wound infiltration with ropivacaine, and combined group (Group CL, n=75) receiving wound infiltration plus intraperitoneal instillation. The primary outcome was Visual Analogue Scale (VAS) scores at rest and during movement. Secondary outcomes included rescue analgesia use, PCIA utilization, referred shoulder pain, time to first ambulation, postoperative hospital stay, adverse events, and patient satisfaction.
Results: Group CL demonstrated significantly lower VAS scores at rest and during movement at all time points compared with Group L and Group C (all P< 0.001). The incidence of referred shoulder pain was significantly different among the three groups (P=0.032), with Group CL showing the lowest incidence. Time to first ambulation and postoperative hospital stay were significantly reduced in Group CL (P< 0.001 and P=0.023, respectively). Patient satisfaction scores were significantly higher in Group CL (P=0.004). No significant differences in adverse events were observed among the three groups.
Conclusion: The combination of wound infiltration and intraperitoneal instillation of ropivacaine is associated with improved postoperative analgesia and facilitates early recovery in patients undergoing LC.
Keywords: cholecystectomy, laparoscopic, anesthetics, local, pain, postoperative, ropivacaine, analgesia, patient-controlled
Introduction
Laparoscopic cholecystectomy (LC) has become the gold standard surgical approach for symptomatic cholelithiasis, with millions of procedures performed annually worldwide.1 Although minimally invasive techniques have significantly reduced surgical trauma compared with open cholecystectomy, postoperative pain remains a considerable clinical challenge, particularly within the initial 24 h following surgery.2,3 Balanced general anesthesia, typically combining intravenous opioid-based induction with inhalational maintenance, remains the standard anesthetic technique for LC. However, general anesthesia alone cannot fully address the distinct pain components associated with this procedure.2 The pain experienced after LC included parietal pain from trocar insertion sites, visceral pain from gallbladder bed dissection, and referred shoulder pain caused by diaphragmatic irritation from residual carbon dioxide.4,5 Inadequate pain control can delay patient discharge and prolongs hospital stay as well as increases opioid consumption and the risk of associated adverse effects such as postoperative nausea and vomiting.6
Local anesthetic techniques, including port-site infiltration and intraperitoneal instillation, have emerged as simple, safe, and cost-effective strategies for reducing postoperative pain in patients undergoing LC.4,7 Port-site infiltration involves injecting local anesthetic agents, typically bupivacaine or ropivacaine, into the trocar insertion sites before or after skin incision.8–10 By blocking sensory nerve transmission at the surgical wound, local infiltration anesthesia can attenuate the parietal component of postoperative pain and potentially reduce the requirement for systemic analgesics. Intraperitoneal instillation delivers local anesthetics directly to the peritoneal cavity, targeting visceral pain from the gallbladder bed and referred shoulder pain caused by diaphragmatic irritation.11 The PROSPECT (PROcedure SPECific Postoperative Pain ManagemenT) Working Group has recommended port-site infiltration or intraperitoneal local anesthetic instillation as part of the analgesic regimen for LC.12 A previous meta-analysis demonstrated that local anesthetic wound infiltration reduces pain scores within the initial 24 hours, although the quality of evidence was rated as very low due to heterogeneous study designs and high risk of bias.13
Despite the abundance of randomized controlled trials examining this topic, most existing evidence was derived from controlled experimental settings with strict inclusion criteria and standardized protocols, and data reflecting routine clinical practice remain limited. Moreover, few studies have directly compared the analgesic effects of port-site infiltration alone versus its combination with intraperitoneal instillation within a single cohort. Therefore, the present study aimed to compare the effects of local infiltration anesthesia combined with general anesthesia versus general anesthesia alone on postoperative analgesia in patients undergoing elective LC.
Materials and Methods
Study Design
This retrospective cohort study was conducted at Weiyuan County People’s Hospital, Neijiang, China. Medical records of patients who underwent elective LC between February 2023 and July 2025 were reviewed. Data were extracted from electronic medical records, anesthesia records, nursing documentation, and postoperative follow-up notes. The workflow of this study is shown in Figure 1.
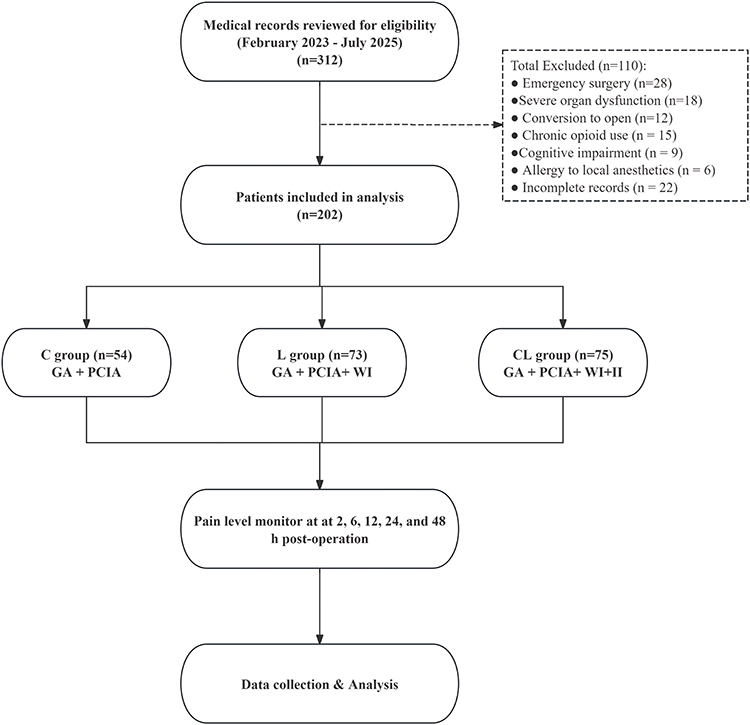 |
Figure 1 Patient flow diagram. Abbreviations: PCIA, patient-controlled intravenous analgesia; GA, General anesthesia; WI, Wound infiltration; II, Intraperitoneal instillation; Group C, control group; Group L, local infiltration group; Group CL, combined group. |
This study was approved by the Ethics Committee of Weiyuan County People’s Hospital (Approval No. 20260113). Due to the retrospective nature of this study and the use of anonymized data, the requirement for individual informed consent was waived by the ethics committee. The study was conducted in accordance with the ethical standards of the Declaration of Helsinki. All patient information was de-identified before analysis to ensure confidentiality.
Patient Selection
The inclusion criteria were as follows: (1) age between 18 and 70 years; (2) American Society of Anesthesiologists (ASA) physical status classification I or II; (3) elective LC; (4) complete medical records available for data extraction. The exclusion criteria were: (1) emergency surgery; (2) conversion to open cholecystectomy; (3) severe cardiac, pulmonary, hepatic, or renal dysfunction; (4) chronic use of analgesics or opioids; (5) known allergy to local anesthetics; (6) cognitive impairment or inability to cooperate with pain assessment.
Grouping Criteria and Methods
A total of 202 patients were enrolled and categorized into three groups according to the analgesic protocols they actually received during the perioperative period, as documented in the operative and anesthesia records: control group (Group C, n=54), local infiltration group (Group L, n=73), and combined group (Group CL, n=75).
All patients in the three groups received standardized general anesthesia. Anesthesia was induced with intravenous sufentanil 0.3–0.5 μg/kg, propofol 1.5–2.0 mg/kg, and rocuronium 0.6 mg/kg. After tracheal intubation, anesthesia was maintained with sevoflurane (1.0–1.5 MAC) in a mixture of oxygen and air, with intermittent administration of sufentanil and rocuronium as needed. All patients received intravenous ondansetron 4 mg for prevention of postoperative nausea and vomiting before the end of surgery. Upon completion of surgery, patient-controlled intravenous analgesia (PCIA) was initiated for all patients. The PCIA regimen consisted of sufentanil 100 μg and ondansetron 8 mg diluted in 100 mL of normal saline, with a background infusion rate of 2 mL/h, a bolus dose of 0.5 mL, and a lockout interval of 15 min.
Patients in Group C received only general anesthesia and postoperative PCIA as described above, without additional local anesthetic administration. In Group L, wound infiltration was performed by the surgeon immediately before skin closure. Ropivacaine 0.25% was injected into the subcutaneous tissue and muscle layers surrounding the trocar insertion sites, with approximately 5 mL administered at each of the port sites.
In Group CL, patients received both wound infiltration and intraperitoneal instillation. Wound infiltration was performed using the same protocol as in Group L. Additionally, 40 mL of 0.2% ropivacaine was instilled into the peritoneal cavity under direct laparoscopic visualization before trocar removal. The solution was distributed over the gallbladder bed, the right subdiaphragmatic space, and the hepatoduodenal ligament region, with the patient placed in Trendelenburg position to facilitate drug distribution.
Outcome Measures
Primary Outcome
The primary outcome was postoperative pain intensity assessed using the Visual Analogue Scale (VAS). The VAS is a 10-cm horizontal line, in which 0 indicates “no pain” and 10 indicates “worst pain imaginable”. Pain assessments were performed at 2, 6, 12, 24, and 48 h after surgery. At each time point, VAS scores were recorded both at rest and during movement. Resting pain was evaluated when the patient was lying quietly in bed without any physical activity. Pain during movement was assessed when the patient performed a standardized activity. As part of routine postoperative care, VAS scores were recorded by ward nurses who were not involved in the intraoperative procedures.
Secondary Outcomes
- Postoperative analgesia indicators: Rescue analgesia was defined as any additional analgesic medication administered beyond the PCIA regimen when patients reported a VAS score of 4 or higher despite PCIA use. The rescue analgesic protocol consisted of intravenous flurbiprofen axetil 50 mg. The incidence of rescue analgesia uses and the total dose of rescue analgesics within 48 h after surgery were recorded. PCIA utilization was evaluated by recording the total number of patient demands (button presses) and the number of effective deliveries within the first 48 postoperative hours. The demand-to-delivery ratio was calculated to reflect patient analgesic requirements. The incidence of referred shoulder pain was recorded, which is defined as pain localized to one or both shoulders after surgery.
- Recovery indicators: Time to first ambulation was defined as the interval from the end of surgery to the first time the patient was able to stand and walk independently with or without assistance. Postoperative length of hospital stay was calculated from the day of surgery to the day of discharge.
- Adverse Events: The incidence of postoperative nausea and vomiting (PONV) and other adverse events including dizziness, pruritus, and urinary retention were recorded during the first 48 h after surgery.
- Patient satisfaction was assessed at 48 h after surgery using the Patient Satisfaction Questionnaire Short Form (PSQ-18). This validated instrument contains 18 items evaluating seven dimensions of healthcare satisfaction: general satisfaction, technical quality, interpersonal manner, communication, financial aspects, time spent with doctor, and accessibility and convenience. Each item was rated on a 5-point Likert scale, with higher values indicating greater satisfaction.
Statistical Analysis
Statistical analysis was performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed data were expressed as mean ± standard deviation and compared among the three groups using one-way analysis of variance, followed by the Least Significant Difference test for post hoc pairwise comparisons. Non-normally distributed data were presented as median with interquartile range and analyzed using the Kruskal–Wallis H-test, with the Mann–Whitney U-test for pairwise comparisons when significant differences were detected. Categorical variables were expressed as frequencies and percentages and compared using the chi-square test or Fisher’s exact test as appropriate. Repeated measures analysis of variance was applied to compare VAS scores across multiple time points among the three groups. A two-tailed P value of less than 0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 202 patients were included in this study, with 54 patients in Group C, 73 patients in Group L, and 75 patients in Group CL. The baseline characteristics of patients in the three groups are presented in Table 1. There were no statistically significant differences among the three groups in terms of age, sex, body mass index, ASA classification, operative time, intraoperative blood loss, or comorbidities including hypertension and diabetes mellitus (all P>0.05). The three groups were comparable at baseline, indicating that subsequent comparisons of outcome measures were not confounded by differences in patient characteristics.
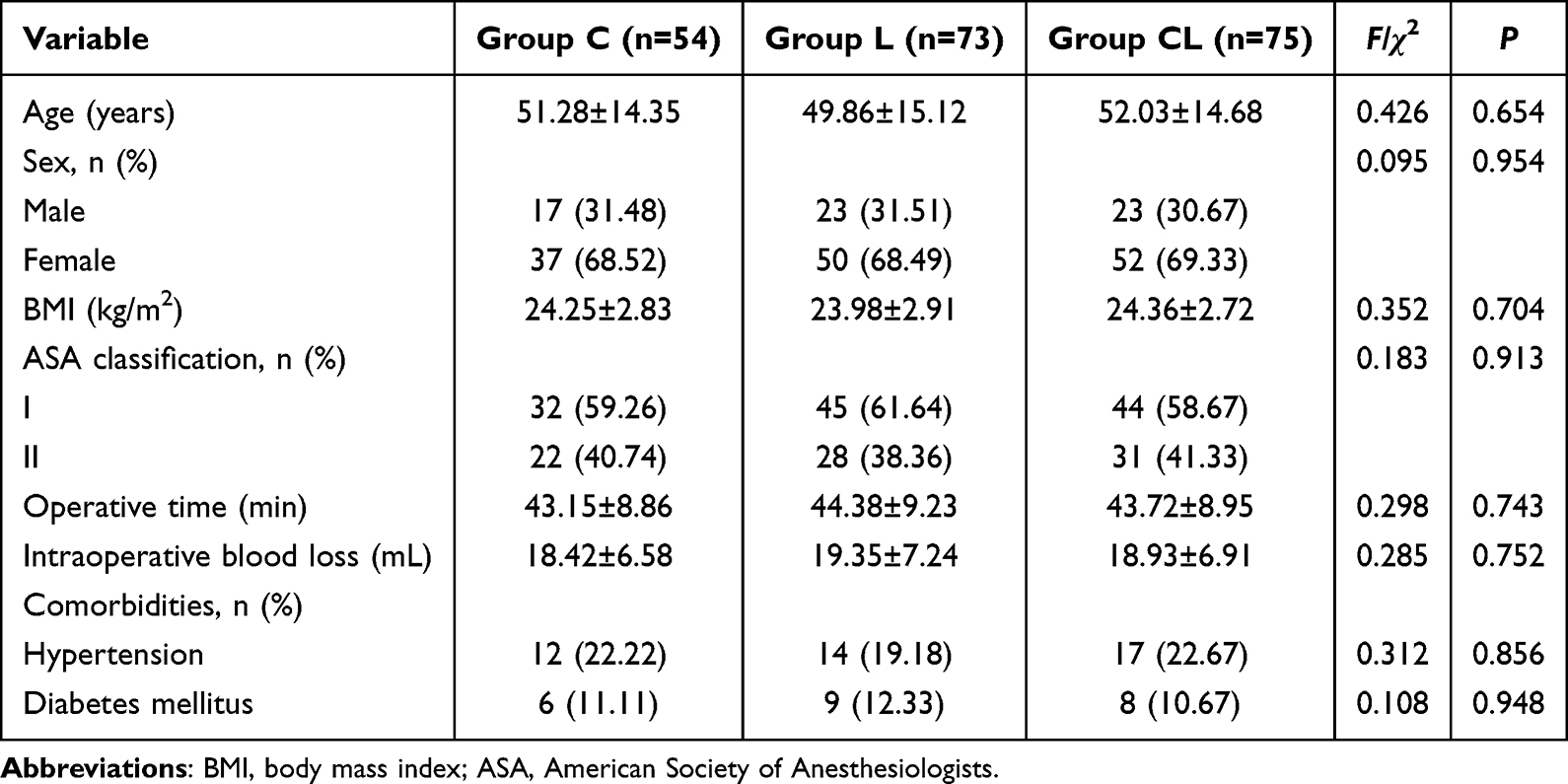 |
Table 1 Baseline Characteristics of Patients in Three Groups |
Postoperative Pain Level
The changes in VAS scores at rest and during movement over the 48-h postoperative period are illustrated in Figure 2. For resting VAS scores (Figure 2A), Group C showed a decrease from 5.83±1.24 at 2 h to 2.76±0.92 at 48 h, Group L from 4.92±1.18 to 2.28±0.84, and Group CL from 4.25±1.13 to 1.98±0.76. At each time point, Group CL demonstrated the lowest VAS scores, followed by Group L, with Group C showing the highest scores (all P<0.001). Repeated measures ANOVA revealed significant effects of time (F=312.456, P<0.001), group (F=47.832, P<0.001), and time-by-group interaction (F=3.275, P=0.008).
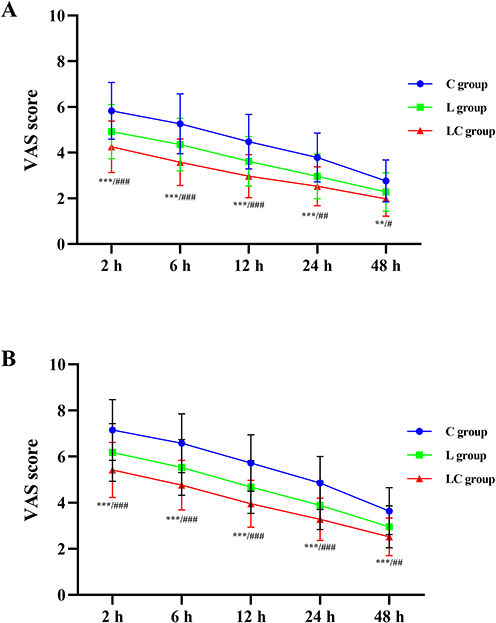 |
Figure 2 Postoperative VAS scores at different time points among the three groups. (A) VAS scores at rest. (B) VAS scores during movement. Data are presented as mean ± SD. Group C, control group; Group L, local infiltration group; Group CL, combined group. ***P<0.001, **P<0.01 vs Group C; ###P<0.001, ##P<0.01, #P<0.05 vs Group L. Abbreviation: VAS, Visual Analogue Scale. |
For VAS scores during movement (Figure 2B), Group C decreased from 7.15±1.32 at 2 h to 3.64±1.02 at 48 h, Group L from 6.18±1.25 to 2.95±0.91, and Group CL from 5.42±1.19 to 2.52±0.82. The between-group differences were statistically significant at all time points (all P<0.001). Repeated measures ANOVA demonstrated significant main effects of time (F=285.372, P<0.001) and group (F=52.146, P<0.001), as well as a significant time-by-group interaction (F=2.987, P=0.015). The greatest between-group differences were observed during the early postoperative period, with the differences gradually diminishing but remaining statistically significant at 48 h.
Postoperative Analgesia and Recovery Outcomes
The postoperative analgesia and recovery outcomes are summarized in Table 2. The incidence of rescue analgesia use showed a decreasing trend from Group C (33.33%) to Group L (21.92%) and Group CL (16.00%), although the difference did not reach statistical significance (P=0.053). Among patients who received rescue analgesia, no significant difference in rescue analgesic dose was observed among the three groups (P=0.344).
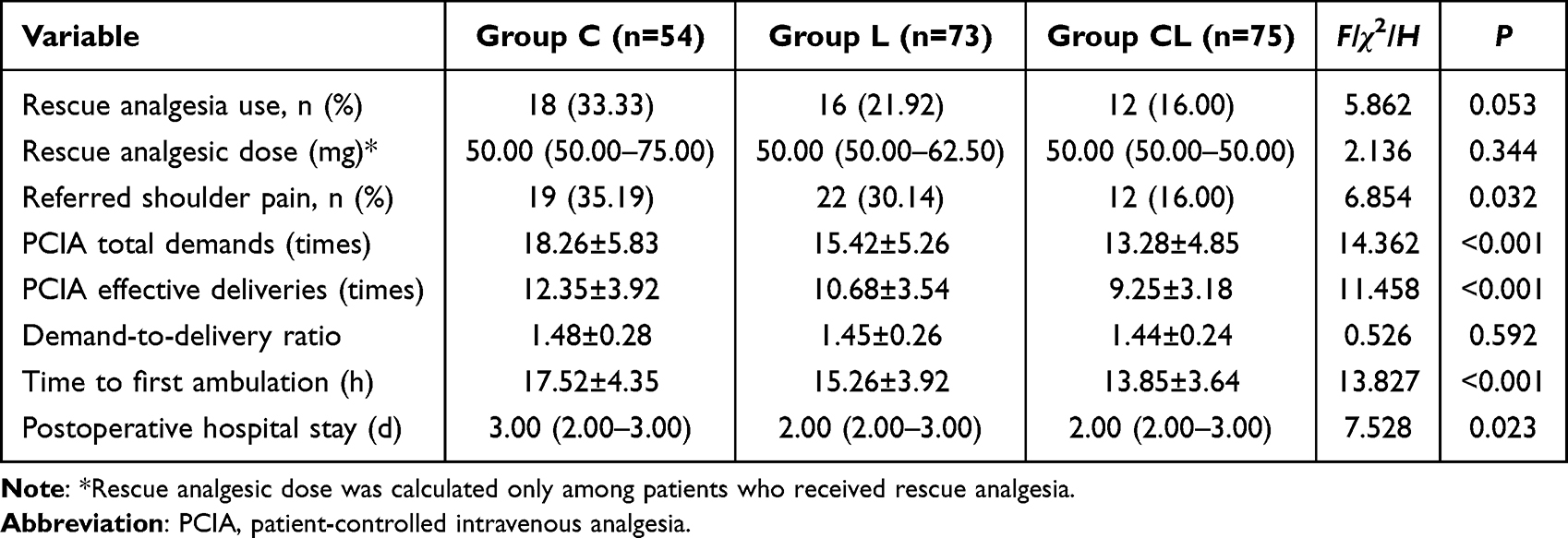 |
Table 2 Comparison of Postoperative Analgesia and Recovery Outcomes Among the Three Groups |
The incidence of referred shoulder pain was significantly lower in Group CL (16.00%) compared with Group L (30.14%) and Group C (35.19%) (P=0.032). Regarding PCIA utilization, both total demands and effective deliveries were significantly lower in Group CL compared with Group L and Group C (all P<0.001). However, the demand-to-delivery ratio was similar among the three groups (P=0.592). Time to first ambulation was significantly shorter in Group CL (13.85±3.64 h) and Group L (15.26±3.92 h) compared with Group C (17.52±4.35 h) (P<0.001). Postoperative hospital stay was also significantly reduced in Group CL and Group L compared with Group C (P=0.023).
Postoperative Adverse Events
The incidence of postoperative adverse events during the 48-hour observation period is illustrated in Table 3. PONV was the most common adverse event, occurring in 35.19% (19/54) of patients in Group C, 28.77% (21/73) in Group L, and 26.67% (20/75) in Group CL, with no significant difference among the three groups (P=0.568). The incidence of dizziness was 18.52% (10/54), 12.33% (9/73), and 9.33% (7/75) in Group C, Group L, and Group CL, respectively (P=0.290). Pruritus occurred in 12.96% (7/54) of patients in Group C, 8.22% (6/73) in Group L, and 6.67% (5/75) in Group CL (P=0.457). Urinary retention was observed in 9.26% (5/54), 5.48% (4/73), and 4.00% (3/75) of patients in Group C, Group L, and Group CL, respectively (P=0.445). Although all adverse events showed a decreasing trend from Group C to Group CL, none of these differences reached statistical significance (all P>0.05).
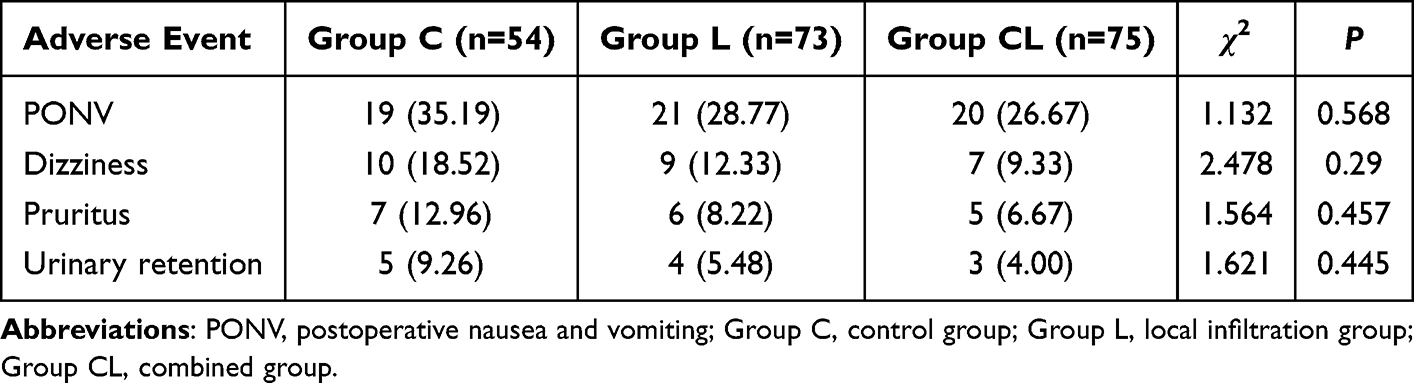 |
Table 3 Incidence of Postoperative Adverse Events Among the Three Groups |
Patient Satisfaction
The PSQ-18 scores at 48 h after surgery are presented in Table 4. The total PSQ-18 score was significantly different among the three groups (P=0.004). Significant differences among the three groups were observed in the dimensions of general satisfaction and technical quality (all P<0.001). Group CL demonstrated the highest scores in general satisfaction and technical quality, followed by Group L, with Group C showing the lowest scores. These findings indicate that patients receiving local anesthetic protocols, particularly the combined approach, reported greater overall satisfaction with their care and perceived higher quality of pain management.
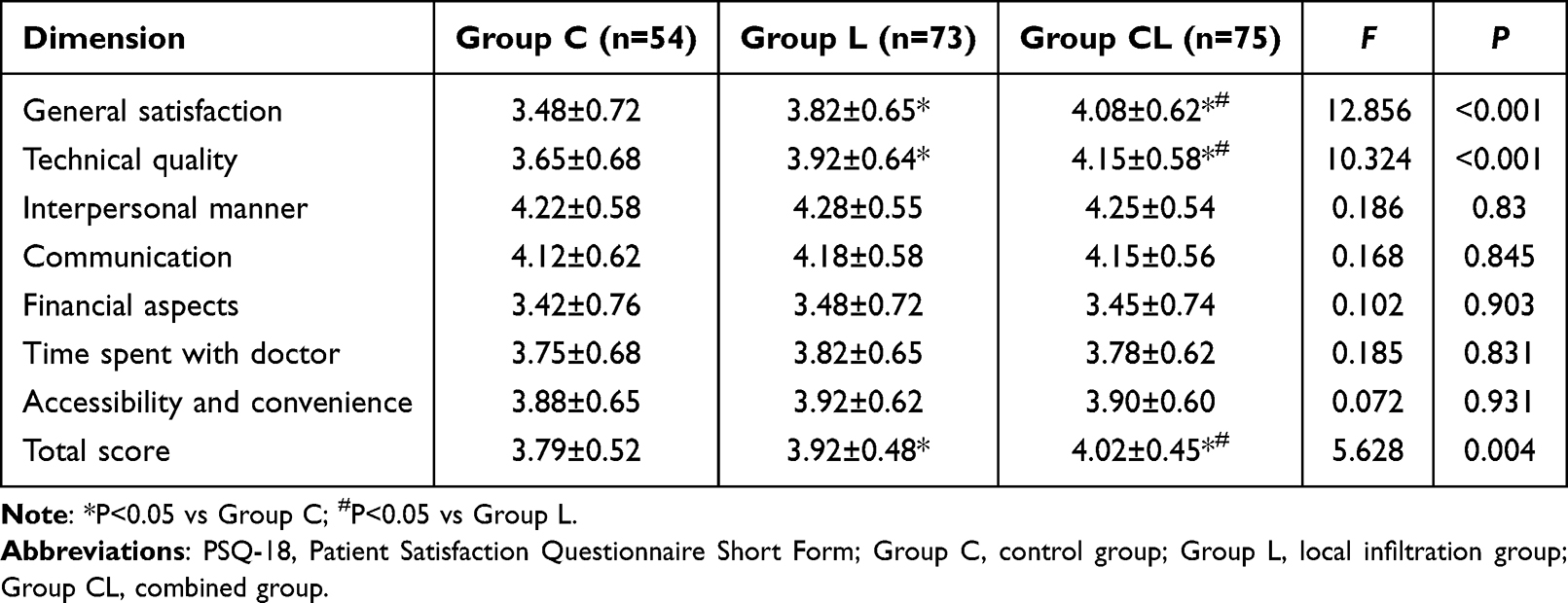 |
Table 4 Comparison of PSQ-18 Scores Among the Three Groups |
No significant differences were observed among the three groups in the dimensions of interpersonal manner, communication, financial aspects, time spent with doctor, and accessibility and convenience (all P>0.05). These results suggest that the differences in patient satisfaction were specifically related to pain management rather than other aspects of healthcare delivery.
Discussion
The present study demonstrated that combining port-site ropivacaine infiltration with intraperitoneal instillation significantly improved postoperative pain control, reduced the incidence of referred shoulder pain, and shortened the time to first ambulation and hospital stay following LC. These findings align with growing evidence supporting the additive analgesic effects of targeting different pain components through regional anesthetic techniques.
The superior analgesic efficacy observed in the CL group can be explained by the distinct origins of post-LC pain. Cha et al14 conducted a prospective randomized trial demonstrating that peritrocal infiltration primarily attenuates parietal pain arising from abdominal wall incisions, whereas intraperitoneal instillation more effectively addresses visceral and shoulder tip pain. Their four-group design revealed that combining both techniques produced additive effects on total pain scores and reduced fentanyl consumption to a greater extent than either method alone. Similarly, Das et al11 compared equipotent concentrations of bupivacaine and ropivacaine for intraperitoneal instillation, confirming that local anesthetics effectively reduce visceral pain during coughing, respiration, and mobilization. A recent meta-analysis pooled data from 24 randomized controlled trials involving 1705 patients, demonstrated that intraperitoneal ropivacaine instillation significantly decreased opioid consumption within the first 24 postoperative hours while reducing the incidence of nausea, vomiting, and shoulder pain.15 The reduction of referred shoulder pain was observed in the CL group. The pathophysiology of post-laparoscopic shoulder pain involves phrenic nerve irritation. The phrenic nerve originates from the anterior branches of C3-C5 spinal nerves, predominantly C4, while the supraclavicular nerve sharing C3-C4 roots innervates the shoulder region.16 Carbon dioxide pneumoperitoneum creates an acidic intraperitoneal environment and causes passive diaphragmatic distension, which irritates and potentially damages the phrenic nerve. Furthermore, artificial pneumoperitoneum induces peritoneal microvascular rupture, releasing inflammatory mediators that sensitize nociceptors and exacerbate pain perception.16 A randomized trial investigated pulmonary recruitment maneuvers confirmed that residual CO2 beneath the diaphragm represents a major contributor to shoulder pain, with interventions targeting gas removal demonstrating significant pain reduction.17 Intraperitoneal local anesthetic instillation interrupts this referred pain pathway through direct blockade of nociceptive transmission from the subdiaphragmatic region to the phrenic nerve. Haneef et al demonstrated that interventions reducing subdiaphragmatic irritation significantly decrease shoulder pain incidence and severity.18 When local anesthetics are instilled intraperitoneally, they spread across the peritoneal surface including the subhepatic and subdiaphragmatic spaces, blocking afferent nerve endings before pain signals can ascend through the C3-C5 pathway. Yi et al19 demonstrated that ultrasound-guided phrenic nerve block using ropivacaine significantly reduced both the incidence and severity of shoulder pain, providing evidence that interrupting phrenic nerve transmission effectively prevents this complication. Previous studies have confirmed that incision infiltration provides better control of abdominal incision pain from 30 min to 24 h postoperatively, while intraperitoneal instillation is more effective for shoulder pain control.20 In this study, the combined analgesic effect of both methods showed the best pain control effect, likely due to complementary pain relief targeting different pain components.
This study selected ropivacaine as the local anesthetic, which is a pure left-handed long-acting amide local anesthetic that inhibits nerve impulse conduction by reversibly blocking sodium ion channels.21 A previous study explained that ropivacaine prevents the increase in voltage-dependent Na+ conductance in splanchnic nerves, which contain visceral sensory afferents responsible for transmitting pain signals from the peritoneal cavity to the central nervous system.22 Compared with bupivacaine, ropivacaine exhibits lower lipophilicity, resulting in reduced cardiac toxicity while maintaining effective sensory blockade. The RELiEVE trial confirmed that intraperitoneal ropivacaine instillation during laparoscopic sleeve gastrectomy not only reduced acute postoperative pain but also enhanced respiratory effort recovery without any drug-related adverse events.23 In addition, after intraperitoneal administration, ropivacaine is absorbed through the peritoneum into the systemic circulation, producing a certain degree of systemic analgesic effect.24 These mechanisms of action may be one of the reasons for the superior efficacy of the combination therapy. The balanced general anesthesia protocol used in this study involved sequential administration of propofol and sufentanil for induction. Previous studies have confirmed that propofol-sufentanil preparations maintain physical stability within the standard clinical application window, supporting the safety and reliability of this anesthetic regimen as the baseline protocol in the present study.25
The shortened time to first ambulation and reduced hospital stay observed in this study align with enhanced recovery after surgery (ERAS) principles. In this study, the CL group achieved a mean time to first ambulation of 13.85 h, which was shorter than the 17.52 h observed in the control group. A recent meta-analysis involving 1489 LC patients demonstrated that ERAS pathways significantly reduced length of stay, time to first flatus, and pain scores compared with conventional care.26 Within ERAS protocols, local anesthetic techniques help reduce the need for opioids and avoid opioid-related adverse effects such as nausea, vomiting, ileus, and respiratory depression, thereby promoting early ambulation and gastrointestinal function recovery in patients.27 Regional anesthesia techniques for laparoscopic surgery further improve pain control, reduce readmission rates, and enhance patient experience, reinforcing their value as an integral part of perioperative care.28 The PSQ-18 results of this study showed that the between-group differences were specifically observed in the dimensions of general satisfaction and technical quality, while other dimensions remained comparable. These differences suggested that the improvement in satisfaction was potentially attributable to pain management rather than other aspects of care. Previous study has shown that the degree of pain reduction is one of the strongest predictor of patient satisfaction.29 El-Tallawy et al30 reported that patients who received local anesthetic infiltration combined with general anesthesia achieved lower pain scores and higher satisfaction compared with general anesthesia alone in a day surgery setting.
Based on the findings of this study, the combination of port-site infiltration and intraperitoneal instillation may be considered as part of the analgesic strategy for elective LC, particularly in ambulatory surgery settings. The technique requires minimal additional operative time and utilizes readily available medications, making it feasible for widespread implementation. A similar study demonstrated that the addition of intraperitoneal instillation to trocar-site infiltration provided better shoulder pain control than trocar-site infiltration alone in patients undergoing laparoscopic abdominal surgery.31 Surgeons should ensure adequate distribution of local anesthetic to both the gallbladder bed and subdiaphragmatic spaces to maximize visceral and referred pain control. For patients at higher risk of postoperative nausea and vomiting or those with contraindications to opioid analgesics, this combined approach offers particular advantages by reducing rescue opioid requirements. Integration of this technique within institutional ERAS protocols may further enhance its benefits through synergistic effects with other recovery-enhancing interventions.
This study has several limitations. The single-center design limits generalizability, as institutional practices, patient populations, and surgical techniques may differ substantially across settings. The retrospective design limits definitive causal inference and introduces potential selection bias. Furthermore, formal blinding of outcome assessors was not implemented, and group allocation could be identified through operative records, which may introduce observer bias. Although baseline characteristics were comparable across groups, unmeasured confounders cannot be excluded. Patient willingness to participate in different analgesic protocols and individual expectations regarding pain management were not assessed, potentially introducing preference-related bias that could affect reported pain scores and satisfaction outcomes. Additionally, the presence of preoperative chronic pain conditions, anxiety disorders, or catastrophizing tendencies was not documented. The fixed concentration and volume of ropivacaine used did not allow exploration of dose-response relationships. Future prospective randomized trials with larger sample sizes should evaluate different timing of administration, optimal concentrations, and cost-effectiveness of combined local anesthetic strategies.
Conclusion
In this study, under standardized balanced general anesthesia with postoperative PCIA, the addition of port-site ropivacaine infiltration and intraperitoneal instillation was associated with improved postoperative pain control, reduced incidence of referred shoulder pain, earlier ambulation, and shorter hospital stay compared with conventional analgesia or port-site infiltration alone following LC. The analgesic benefits were most pronounced during the early postoperative period and were reflected in improved patient satisfaction regarding pain management. This combined approach may serve as a feasible component of enhanced recovery protocols. However, given the retrospective nature of this study, prospective randomized trials are needed to confirm these findings and to determine optimal dosing strategies.
Ethics Approval
The study protocol was approved by the Ethics Committee of Weiyuan County People’s Hospital (Approval No. 20260113), and the requirement for informed consent was waived due to the retrospective nature of the study and the use of anonymized data. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We thank all the patients who participated in this study.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Kim SS, Donahue TR. Laparoscopic cholecystectomy. JAMA. 2018;319(17):1834. doi:10.1001/jama.2018.3438
2. Bourgeois C, Oyaert L, Van de Velde M, et al. Pain management after laparoscopic cholecystectomy: a systematic review and procedure-specific postoperative pain management (PROSPECT) recommendations. Eur J Anaesthesiol. 2024;41(11):841–10. doi:10.1097/EJA.0000000000002047
3. Jiang B, Ye S. Pharmacotherapeutic pain management in patients undergoing laparoscopic cholecystectomy: a review. Adv Clin Exp Med. 2022;31(11):1275–1288. doi:10.17219/acem/151995
4. Abuelzein MLA, Baghdadi MA, Abbdelhady WA, Khairy MM. A prospective randomized controlled study on the role of restoring liver diaphragm surface tension and pain control at port sites in optimizing pain management following laparoscopic cholecystectomy. Ann Gastroenterol Surg. 2023;7(1):131–137. doi:10.1002/ags3.12602
5. Chooklin S, Chuklin S. A hidden ally in laparoscopic cholecystectomy: quadratus lumborum block and the quest for pain-free recovery. Front Surg. 2025;12:1710676. doi:10.3389/fsurg.2025.1710676
6. Hyland SJ, Brockhaus KK, Vincent WR, et al. Perioperative pain management and opioid stewardship: a practical guide. Healthcare. 2021;9(3):333. doi:10.3390/healthcare9030333
7. Karaman Y, Kebapçı E, Görgün M, Güvenli Y, Tekgül Z. Post-laparoscopic cholecystectomy pain: effects of preincisional infiltration and intraperitoneal levobupivacaine 0.25% on pain control-a randomized prospective double-blinded placebo-controlled trial. Turk J Anaesthesiol Reanim. 2014;42(2):80–85. doi:10.5152/TJAR.2014.06025
8. Seo JW, Lee IO, Kim JC, Chung JE. The role of port site local anesthetic injection in laparoendoscopic single site surgery: a prospective randomized study. Obstet Gynecol Sci. 2020;63(3):387–394. doi:10.5468/ogs.2020.63.3.387
9. Mishra PK, Mani S, Singh RB. Evaluating the efficacy of pre-incisional infiltration and intraperitoneal instillation of a local anesthetic agent on postoperative analgesia and hemodynamics in patients undergoing laparoscopic cholecystectomy under general anesthesia. Cureus. 2022;14(3):e22977. doi:10.7759/cureus.22977
10. Protic M, Veljkovic R, Bilchik AJ, et al. Prospective randomized controlled trial comparing standard analgesia with combined intra-operative cystic plate and port-site local anesthesia for post-operative pain management in elective laparoscopic cholecystectomy. Surg Endosc. 2017;31(2):704–713. doi:10.1007/s00464-016-5024-5
11. Das NT, Deshpande C. Effects of intraperitoneal local anaesthetics bupivacaine and ropivacaine versus placebo on postoperative pain after laparoscopic cholecystectomy: a randomised double blind study. J Clin Diagn Res. 2017;11(7):Uc08–Uc12. doi:10.7860/JCDR/2017/26162.10188
12. Barazanchi AWH, MacFater WS, Rahiri JL, Tutone S, Hill AG, Joshi GP. Evidence-based management of pain after laparoscopic cholecystectomy: a PROSPECT review update. Br J Anaesth. 2018;121(4):787–803. doi:10.1016/j.bja.2018.06.023
13. Loizides S, Gurusamy KS, Nagendran M, Rossi M, Guerrini GP, Davidson BR. Wound infiltration with local anaesthetic agents for laparoscopic cholecystectomy. Cochrane Database Syst Rev. 2014;2014(3):Cd007049. doi:10.1002/14651858.CD007049.pub2
14. Cha SM, Kang H, Baek CW, et al. Peritrocal and intraperitoneal ropivacaine for laparoscopic cholecystectomy: a prospective, randomized, double-blind controlled trial. J Surg Res. 2012;175(2):251–258. doi:10.1016/j.jss.2011.04.033
15. Daghmouri MA, Chaouch MA, Deniau B, et al. Efficacy and safety of intraperitoneal ropivacaine in pain management following laparoscopic digestive surgery: a systematic review and meta-analysis of RCTs. Medicine. 2024;103(29):e38856. doi:10.1097/MD.0000000000038856
16. Zhao Y, Xin W, Luo X. Post-laparoscopic shoulder pain management: a narrative review. Curr Pain Headache Rep. 2025;29(1):18. doi:10.1007/s11916-024-01355-y
17. Temtanakitpaisan A, Temtanakitpaisan T, Pratipanawatr C, Buppasiri P, Somjit M. Additional low-pressure pulmonary recruitment for reducing post-laparoscopic shoulder pain in gynecologic laparoscopy: a randomized controlled trial. Obstet Gynecol Sci. 2024;67(2):253–260. doi:10.5468/ogs.23197
18. Haneef AK, Aljohani EA, Alzahrani RS, et al. Active gas aspiration in reducing pain after laparoscopic cholecystectomy: a systematic review and meta-analysis of randomized controlled trials. Surg Endosc. 2024;38(2):597–606. doi:10.1007/s00464-023-10651-4
19. Yi MS, Kim WJ, Kim MK, et al. Effect of ultrasound-guided phrenic nerve block on shoulder pain after laparoscopic cholecystectomy-a prospective, randomized controlled trial. Surg Endosc. 2017;31(9):3637–3645. doi:10.1007/s00464-016-5398-4
20. El-Labban GM, Hokkam EN, El-Labban MA, Morsy K, Saadl S, Heissam KS. Intraincisional vs intraperitoneal infiltration of local anaesthetic for controlling early post-laparoscopic cholecystectomy pain. J Minim Access Surg. 2011;7(3):173–177. doi:10.4103/0972-9941.83508
21. National Institute of Child Health and Human Development. Ropivacaine. In: Drugs and Lactation Database (Lactmed®). National Institute of Child Health and Human Development; 2006.
22. Benincá Albuquerque A, Carlesso de Freitas C, Corrêa Bitencourt I, Alves Pereira Chiuchetta I, Baú PC, Vontobel Padoin A. Postoperative analgesia with instillation of intraperitoneal ropivacaine in patients undergoing laparoscopic cholecystectomies. J Gastrointest Surg. 2025;29(6):102034. doi:10.1016/j.gassur.2025.102034
23. Zheng LQ, Kosai NR, Ani MFC, Maaya M. The impact of laparoscopic intraperitoneal instillation of ropivacaine in enhancing respiratory recovery and reducing acute postoperative pain in laparoscopic sleeve gastrectomy: a double-blinded randomised control; RELiEVE Trial. Obes Surg. 2023;33(10):3141–3146. doi:10.1007/s11695-023-06777-y
24. Kumar R, Nath SS, Agarwal A. Intraperitoneal nebulization versus intraperitoneal instillation of ropivacaine for postoperative pain management following laparoscopic donor nephrectomy. Korean J Anesthesiol. 2019;72(4):357–365. doi:10.4097/kja.d.18.00290
25. Husna M, Munawiroh SZ, Puji Ekawati R, Hanifah S. Systematic review of the stability and compatibility of propofol injection. Anaesthesiol Intensive Ther. 2021;53(1):79–88. doi:10.5114/ait.2021.103542
26. Nair A, Al-Aamri HHM, Borkar N, Rangaiah M, Haque PW. Application of enhanced recovery after surgery pathways in patients undergoing laparoscopic cholecystectomy with and without common bile duct exploration: a systematic review and meta-analysis. Sultan Qaboos Univ Med J. 2023;23(2):148–157. doi:10.18295/squmj.1.2023.005
27. Nechay T, Titkova S, Tyagunov A, Anurov M, Sazhin A. Modified enhanced recovery after surgery protocol in patients with acute cholecystitis: efficacy, safety and feasibility. Multicenter randomized control study. Updates Surg. 2021;73(4):1407–1417. doi:10.1007/s13304-021-01031-5
28. Macías AA, Finneran JJ. Regional anesthesia techniques for pain management for laparoscopic surgery: a review of the current literature. Curr Pain Headache Rep. 2022;26(1):33–42. doi:10.1007/s11916-022-01000-6
29. Burch T, Seipel SJ, Coyle N, Ortega KH, DeJesus O. Postoperative visual analog pain scores and overall anesthesia patient satisfaction. Crit Care Nurs Clin North Am. 2017;29(4):419–426. doi:10.1016/j.cnc.2017.08.003
30. El-Tallawy SN, Alsubaie AT, Yousef EA, et al. Identifying predictors of early postoperative pain and patient satisfaction following day surgery: insights from an observational study. Cureus. 2025;17(6):e86118. doi:10.7759/cureus.86118
31. Lysander SS, Kumar GD, Balasubramanian A, Krishnan R, Raghuraman MS, Narayanan SV. Comparison of trocar site versus trocar site plus intraperitoneal instillation of local anesthetic for shoulder pain following laparoscopic abdominal surgery. Anesth Essays Res. 2021;15(4):375–378. doi:10.4103/aer.aer_156_21
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.