Back to Journals » Advances in Medical Education and Practice » Volume 7
Effects of adding a new PCMH block rotation and resident team to existing longitudinal training within a certified PCMH: primary care residents’ attitudes, knowledge, and experience
Authors Anandarajah G, Furey C, Chandran R, Goldberg A, El Rayess F, Ashley D, Goldman R
Received 9 April 2016
Accepted for publication 5 May 2016
Published 4 August 2016 Volume 2016:7 Pages 457—466
DOI https://doi.org/10.2147/AMEP.S110215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Gowri Anandarajah,1,2 Christopher Furey,1 Rabin Chandran,1 Arnold Goldberg,3,4 Fadya El Rayess,1 David Ashley,1 Roberta E Goldman,1,5
1Department of Family Medicine, 2Department of Medical Science, Warren Alpert Medical School of Brown University, Providence, RI, 3Department of Family Medicine, University of South Florida Morsani College of Medicine, Tampa, FL, 4Department of Family Medicine, Leigh Valley Family Health Network, Allentown, PA, 5Department of Social and Behavioral Sciences, Harvard T.H. Chan School of Public Health, Boston, MA, USA
Background: Although the patient-centered medical home (PCMH) model is considered important for the future of primary care in the USA, it remains unclear how best to prepare trainees for PCMH practice and leadership. Following a baseline study, the authors added a new required PCMH block rotation and resident team to an existing longitudinal PCMH immersion and didactic curriculum within a Level 3-certified PCMH, aiming for “enhanced situated learning”. All 39 residents enrolled in a USA family medicine residency program during the first year of curricular implementation completed this new 4-week rotation. This study examines the effects of this rotation after 1 year.
Methods: A total of 39 intervention and 13 comparison residents were eligible participants. This multimethod study included: 1) individual interviews of postgraduate year (PGY) 3 intervention vs PGY3 comparison residents, assessing residents’ PCMH attitudes, knowledge, and clinical experience, and 2) routine rotation evaluations. Interviews were audiorecorded, transcribed, and analyzed using immersion/crystallization. Rotation evaluations were analyzed using descriptive statistics and qualitative analysis of free text responses.
Results: Authors analyzed 23 interviews (88%) and 26 rotation evaluations (67%). Intervention PGY3s’ interviews revealed more nuanced understanding of PCMH concepts and more experience with system-level PCMH tasks than those of comparison PGY3s. More intervention PGY3s rated themselves “extremely prepared” to implement PCMH than comparison PGY3s; however, most self-rated “somewhat prepared”. Their reflections demonstrated deeper understanding of PCMH implementation and challenges than comparison PGY3s but inadequate experience to directly see the results of successful solutions. Rotation evaluations from PGY1, PGY2, and PGY3s revealed strengths and several areas for improvement.
Conclusion: Adding one 4-week block rotation to existing longitudinal training appears to improve residents’ PCMH knowledge, skills, and experience from “basic” to “intermediate”. However, this training level appears inadequate for PCMH leadership or for teaching junior learners. Further study is needed to determine the optimum training for different settings.
Keywords: primary care, new models of healthcare, curriculum, family medicine, population health, residency education
Introduction
The health care landscape in the USA continues to change at a remarkable pace. New models of health care delivery, including the patient-centered medical home (PCMH) model, and population health management are increasingly considered critical for the future of medicine, especially for primary care.1–3 However, it remains unclear how to best prepare primary care residents for practice in this changing environment. While many residency programs describe PCMH practice transformation efforts4–7 or focused aspects of PCMH implementation,8–11 few describe formal curricula preparing residents for practice within these new health care delivery models12 and even fewer report curriculum evaluations.13,14 Most published residency curricula rely on immersion in a transforming PCMH practice as the primary educational method. Some supplement this with didactics, quality improvement projects, and chronic disease management training.12–14
While the larger health care system is undergoing fundamental transformation, residency programs struggle to meet existing accreditation requirements, while attempting to provide innovative training suited to the health care system of tomorrow. Radical changes in primary care residency education may be needed. However, currently only incremental changes may be possible. Additionally, it remains unclear what the appropriate “dose” of PCMH/population health training is needed for different clinical specialties.
The Brown University Family Medicine Residency Program’s faculty-resident teaching practice is located in an urban, underserved setting in Rhode Island, USA, and provides care for patients with a heavy burden of complex medical and psychosocial needs. An early adopter of the PCMH model, this practice was recognized by the National Committee for Quality Assurance as a Level 3 PCMH in 2010. Level 3 is the highest level of PCMH accreditation available in the USA. Despite experiencing this high level of PCMH practice transformation and exposure to a PCMH didactic curriculum, our previous qualitative interview study of all graduating postgraduate year (PGY) 3 residents in June 2011 showed that residents’ knowledge of PCMH-related concepts was vague and limited to a few specific elements, and their readiness to incorporate PCMH skills into their practices was limited.15 Although these senior family medicine residents had considerable experience practicing within a Level 3 PCMH (eg, >1,650 patient visits each; Figure 1) and had received PCMH training comparable to that described by other programs,12,14 residents appeared to remain peripheral to the system-level aspects of the PCMH, only passively participating in population health, chronic disease management, and quality improvement activities that are central to the PCMH model.15
 | Figure 1 Comparison of PCMH training received by PGY3 comparison residents vs PGY3 intervention residents. Abbreviations: GMV, group medical visit; PCMH, patient-centered medical home; PDSA, Plan Do Study Act; PGY, postgraduate year; NH, nursing home; HB, homebound. |
In reflecting on these findings, we reasoned that a simple situated learning model16–18 (ie, longitudinal immersion in a PCMH practice with supporting didactics) was not adequate to ensure that residents gain the new skills necessary for practice and leadership in our rapidly changing health care environment. This may be because the “community of practice” (including most faculty and staff), which supports situated learning, was itself attempting to acquire new knowledge and skills. This left teaching about new models of practice to a handful of PCMH faculty “champions”. We hypothesized that in order to effectively teach PCMH and population health skills, an “enhanced” situated learning model is needed. This would entail purposefully shifting residents from the periphery to the center of PCMH activities and having them take on increasing levels of responsibility as they progress from junior to senior residents. Thus, as they develop from novice to expert in PCMH-related skills, they become integral to the community of practice supporting future learners.
With this enhanced situated learning model in mind, in July 2011, the Brown Family Medicine Residency underwent a significant curricular redesign in order to implement a new required 4-week PCMH block rotation for PGY1, PGY2, and PGY3 residents, forming a new three-member outpatient PCMH resident leadership team, modeled after the structure of inpatient resident teams.19 We added this new block rotation to our existing longitudinal immersion and didactic PCMH curriculum, studied previously.15 This redesign followed a critical review of our overall residency curriculum and specialty-specific Accreditation Council for Graduate Medical Education requirements. Redesign required making challenging choices regarding training priorities and negotiating with multiple stakeholders.19 The goal of this new PCMH block rotation and resident leadership team is to improve residents’ knowledge, attitudes, and skills regarding PCMH and population health competencies. We derived content from the National Committee for Quality Assurance PCMH standards20 and recommendations of family medicine thought leaders.21,22 Content is consistent with recent recommendations for family medicine residents23 and a consensus report of PCMH entrustable professional activities (EPAs) for internal medicine residents.24 A description of curriculum development within the Rhode Island context has been previously published.19 Table 1 summarizes key curriculum content and teaching methods.
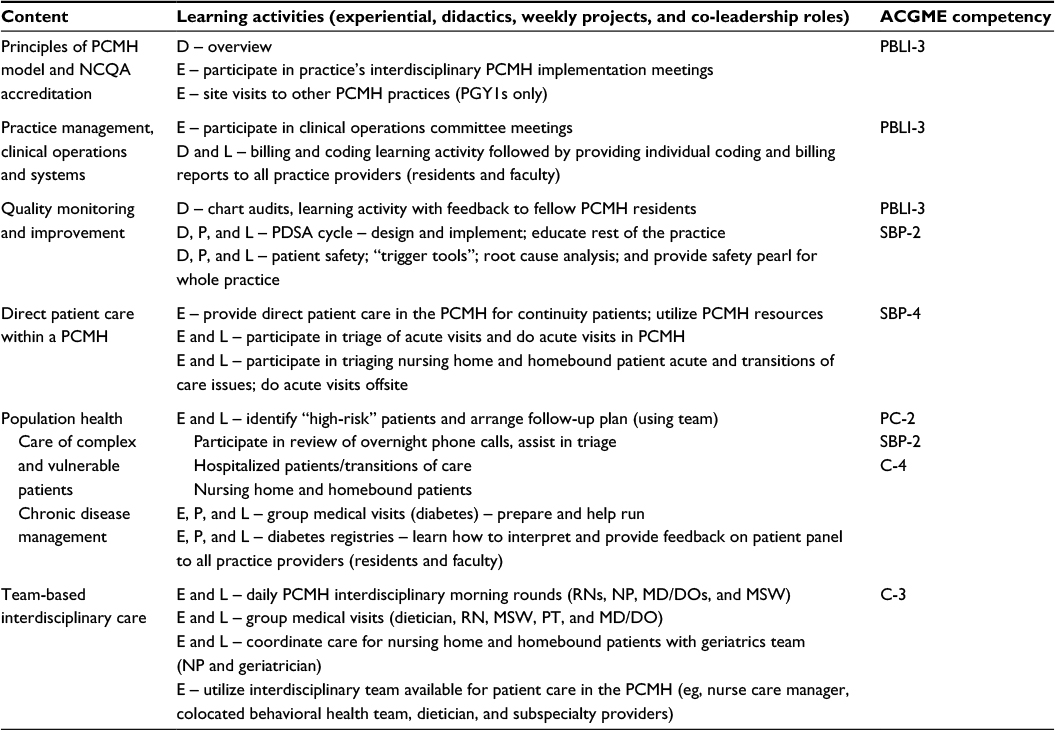 | Table 1 Curriculum content and teaching methods Abbreviations: ACGME, Accreditation Council for Graduate Medical Education; D, didactic; E, experiential; P, project; L, leadership or co-leadership (taught and coached by faculty); NCQA, National Committee for Quality Assurance; PDSA, Plan Do Study Act; PCMH, patient-centered medical home; PGY, postgraduate year; RNs, registered nurses; NP, nurse practitioner; MD, medical doctor; DO, doctor of osteopathic medicine; MSW, master of social work; PT, physical therapist; PBLI-3, improves systems in which physician provides care; SBP-4, coordinates team-based care; SBP-2, emphasizes patient safety; PC-2, cares for patient with chronic conditions; C-4, utilizes technology to optimize communication; C-3, develops relationships and effectively communicates with physicians, other health professionals, and health care teams. |
The purpose of this study is to critically explore the effects of this new curriculum 1 year after implementation, at which time all residents had participated in one, 4-week long, PCMH block rotation. Given the multiple completing training demands that residencies face and the varying needs of different clinical specialties, we felt it critical to determine whether a 4-week rotation, added to an existing longitudinal PCMH practice immersion and didactic curriculum, is adequate to impart PCMH leadership training or whether the planned full 3-year longitudinal block rotation series (4 wk/y ×3 years) is needed.
Methods
Study design
We used a multimethod approach to assess the effects of this new required rotation after the first year of implementation. To explore the meaning and context that residents brought to their experience, knowledge, and attitudes regarding their PCMH training, we chose as our primary method qualitative individual interviews comparing PGY3 intervention residents with PGY3 comparison residents. We supplemented this with analysis of routine rotation evaluations submitted through our electronic evaluation system (E*Value) from all intervention residents. We received Institutional Review Board approval for this study.
Participants and setting
We invited all 39 residents present at Brown University’s 13–13–13 family medicine residency program during academic year 2011–2012 (intervention residents) and 13 comparison residents (Brown Family Medicine residency class of 2011) to participate in the study.
Intervention participants
All Brown Family Medicine residents participated in this new required block rotation during academic year 2011–2012. These 39 intervention residents included 13 PGY1s, 13 PGY2s, and 13 PGY3s.
Interview study participants
The 13 PGY3 intervention residents (class of 2012; who received baseline PCMH training15 plus one PCMH block rotation) and 13 comparison PGY3 residents (class of 2011; who received baseline PCMH training only15) were eligible to participate in the qualitative interview study. Figure 1 illustrates the differences in curriculum received by these two groups.
Rotation evaluation participants
All 39 intervention residents were asked to complete routine rotation evaluations through the E*Value system.
Data collection
A nonteaching, nonsupervisory staff person conducted semistructured individual in-person interviews, using a largely open-ended interview guide, with the 13 PGY3 intervention and the 13 PGY3 comparison residents just prior to graduation. Questions topics included PCMH attitudes and knowledge as well as residents’ self-assessment of preparedness for PCMH practice and self-report of the number of selected PCMH-related activities they had performed during residency. Interviews were audiorecorded and transcribed verbatim with identifiers removed. Participants signed written informed consent forms.
We extracted all PCMH rotation evaluations from all 39 residents present during academic year 2011–2012 from the E*Value system. These deidentified evaluations included both numerical ratings and free text responses.
Data analysis
We conducted a thematic analysis of the content of the individual interviews using the immersion/crystallization method.25 This entailed two researchers (GA and RG) first individually reading transcripts and making notes regarding emerging themes. This was followed by analysis meetings to discuss data and interpretation of content until we reached consensus regarding major themes and subthemes. Three researchers (CF, RC, and GA) extracted numerical data from the interviews and analyzed the findings using descriptive methods. Three researchers (GA, RC, and FE) analyzed E*Value rotation evaluations, using descriptive statistics of numerical ratings and qualitative analysis of free text responses.
Ethical approval
This study was reviewed and approved by the Memorial Hospital of Rhode Island’s Institutional Review Board. Memorial Hospital of Rhode Island is the home institution for the Brown University Family Medicine Residency Program.
Results
Participants
Eleven PGY3 intervention (85%) and 12 PGY3 comparison residents (92%) participated in the individual interview study. Twenty-six residents (66.7%) completed rotation evaluations.
Qualitative interviews: intervention vs comparison PGY3s
Our analysis of interview data from intervention and comparison residents yielded four major differences between the groups (Tables 2 and 3).
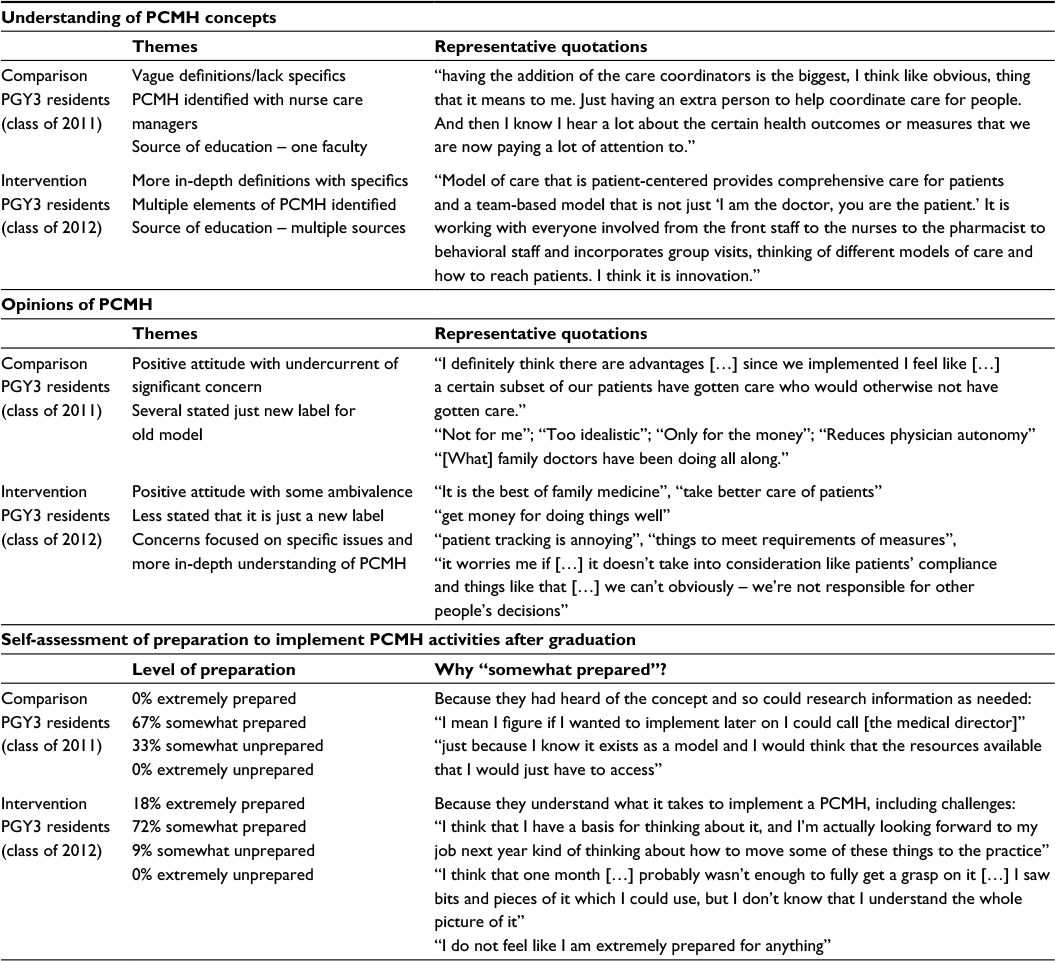 | Table 2 Comparison vs intervention residents’ PCMH knowledge, attitudes, and preparedness (qualitative interviews) Abbreviations: PCMH, patient-centered medical home; PGY, postgraduate year. |
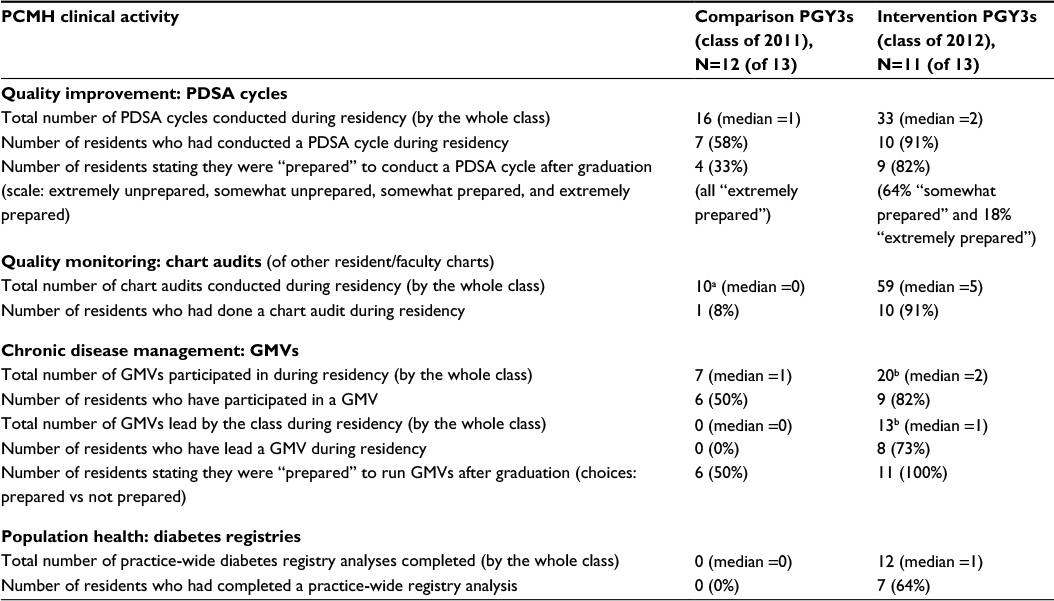 | Table 3 Intervention vs comparison residents’ experience with PCMH clinical activities (from qualitative interviews) Notes: Data extracted from closed ended questions in qualitative interviews; therefore, only raw numbers, percentages, and medians are provided. aAll done by one resident – prenatal chart reviews (elective project). bOne resident did additional group medical visits (elective project). Abbreviations: GMVs, Group Medical Visits; PCMH, patient-centered medical home; PDSA, Plan Do Study Act; PGY, postgraduate year. |
Attitudes toward the PCMH model
Both sets of residents expressed generally positive attitudes toward the PCMH model. However, comparison residents displayed an undercurrent of significant, often vague, concerns such as the model is “too challenging to fully implement” or “only for large practices”. For intervention residents, after addition of only one 4-week rotation, expressed concerns were less pointed and focused on specific issues, reflecting a more in-depth understanding of the PCMH model. For example, one intervention resident reflecting on poor diabetes measures in patients with complex psychosocial issues wondered “would you be penalized for that or should you be commended for taking on more complicated patients?”
In comparison group interviews, there was a sharp contrast in attitudes between the few PCMH resident champions in the class and the majority of the class. This contrast was much less apparent in the intervention group. In both groups, several residents believed that PCMH-related competencies would be unnecessary in their future practice, although this attitude was much less prominent in intervention residents.
Knowledge of PCMH concepts
Comparison residents’ definitions of the PCMH model were vague and imprecise, with most residents equating PCMH with a recently hired nurse care manager who had been of tremendous help to them. Almost all reported that their PCMH education came solely from a single faculty member, the medical director. In contrast, intervention residents provided more nuanced definitions of PCMH, were able to articulate multiple elements of the PCMH model, and referenced multiple sources of education regarding PCMH-related competencies.
Preparedness to implement PCMH
There was a difference in self-reported preparedness to implement PCMH principles after graduation between comparison and intervention residents, with none of the comparison residents vs 18% of intervention residents feeling “extremely prepared” (Table 2). In both groups, the majority felt “somewhat prepared”. However, the reasons they felt somewhat prepared differed significantly. Many comparison residents believed that because they had heard of PCMH, they would be able to find more information if needed. In contrast, intervention residents provided more in-depth explanations reflecting a detailed understanding of the challenges involved with implementing a PCMH.
Specific learning activities
As a proxy measure for PCMH and population health skills gained through the rotation, we asked residents about their experience with specific learning activities (Table 3). The intervention class reported having participated in higher numbers of diabetes group medical visits (GMVs) (median 2 vs 1), Plan Do Study Act quality improvement cycles (median 2 vs 1), chart audits (median 5 vs 0), and practice-wide chronic disease registry analysis (median 1 vs 0). The quality of the involvement in these activities also differed considerably, with comparison residents reporting observer or participant status, whereas intervention residents reported having had some mentored leadership roles. For example, more intervention residents had co-led a GMV. Residents in both groups who expressed low interest in future practice leadership roles appeared less interested in learning about quality improvement.
Educational strengths and challenges with the PCMH rotation
Intervention residents were asked to reflect on what they learned and what needed improvement (Table 4). Residents felt that they learned many things including “big picture” aspects of PCMH and their practice, that change was possible and how change happens, how to work with interdisciplinary teams on a system level, and some specific skills. However, they struggled with resolving the gap between the ideal of a PCMH and the realities of practicing within their faculty-resident practice, which had limited resources and a high burden of underserved and vulnerable patients. Several residents voiced frustration with certain rotation components, including tracking hospital transitions of care for PCMH patients, which was arduous due to the outdated community hospital’s information technology system (and not, they felt, a physician role), and doing acute nursing home visits (which they felt did not “fit” with PCMH). Many, however, expressed understanding of the link between population health and both of these activities. Finally, many commented that 4 weeks was inadequate time to see the positive results of their efforts: “it’s just really not long enough to have anything really change. And I think that’s part of the things that are disheartening”.
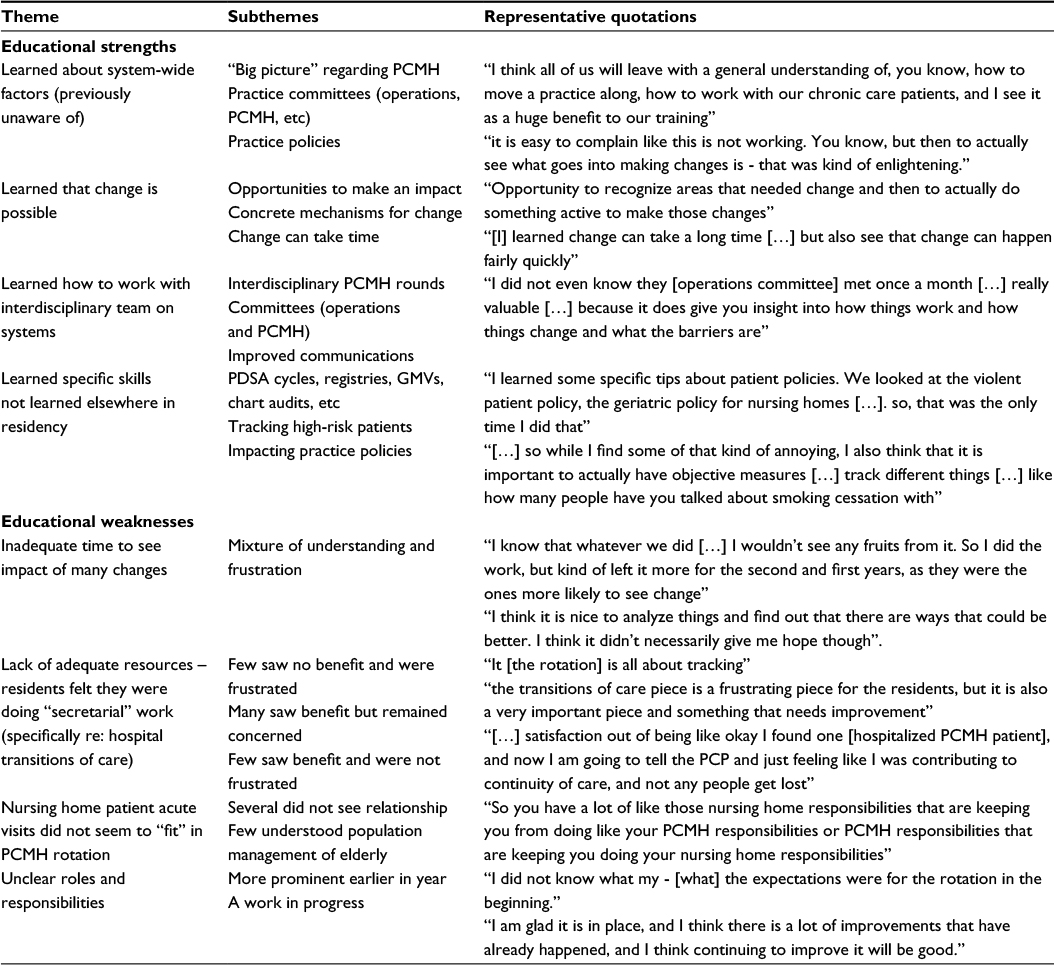 | Table 4 Interventions residents’ opinions of rotation’s educational strengths and weaknesses (qualitative interviews) Abbreviations: GMV, group medical visit; PCMH, patient-centered medical home; PDSA, Plan Do Study Act; PCP, primary care physician. |
E*Value surveys: implementation and process evaluation
Monthly E*Value rotation evaluations and verbal feedback from residents and faculty informed rotation improvements throughout the year. Table 5 provides details of E*Value numerical ratings (1–4 scale) from residents. While residents rated the quality of teaching between “very good” and “excellent” (mean 3.35), they rated overall educational value only “adequate” to “very good” (mean 2.58). We did not calculate P-values due to small sample size. However, there appeared to be a trend in median ratings of overall educational value from highest in PGY1s (3= very good) and lowest in PGY3s (2= adequate). PGY3s rated the quality of teaching higher than other groups.
 | Table 5 First year implementation feedback: rotation evaluation numerical ratings from residents (E*Value) Note: Rating scale of 1–4 (1, inadequate; 2, adequate; 3, very good; 4, excellent). Abbreviation: PGY, postgraduate year. |
Free text responses revealed that residents considered the “most valuable” components to be review of overnight phone calls during PCMH morning rounds, GMVs, acute visits, and didactic sessions. Additionally, many PGY1 residents reported seeing acute nursing home patients with their senior resident (PGY3) as among the most valuable learning experiences. The most commonly reported “least valuable” activity was tracking the practice’s hospitalized patients to ensure appropriate transition of care. The most common resident requests for improvement encompassed logistics of rotation orientation, clarification of roles and expectations, and improvement of the hospital’s information technology (IT) system.
Discussion
We instituted a major curriculum redesign that added a new annual PCMH block rotation and resident leadership team19 to our existing longitudinal PCMH immersion and didactic curriculum.15 Residents’ rotation evaluations revealed strengths (eg, quality of teaching) and several areas requiring improvement (eg, clarification of residents’ roles). Residents especially expressed frustration at their hospital’s lack of adequate IT capabilities to enable efficient tracking of the practice’s hospitalized patients.
Despite these implementation challenges and after only 1 year of implementation, our qualitative interview data showed interesting differences between intervention and comparison PGY3s. Intervention residents expressed fewer concerns about the PCMH model, with remaining concerns focused on specific issues rather than general impressions, reflecting a more nuanced conceptual understanding of the model. Although the majority in both groups rated themselves as only somewhat prepared to implement PCMH principles after graduation, intervention residents’ reasons for this self-rating reflected a more sophisticated understanding of the challenges involved with PCMH implementation. Proxy measures for PCMH-related skills (eg, Plan Do Study Act cycles) demonstrated a greater number done and more active resident leadership roles in the intervention group. Finally, despite addition of this 4-week block rotation, several intervention PGY3s were still not convinced that PCMH would touch their work lives and PGY3s tended to rate the overall educational value of the rotation lower than PGY1s and PGY2s.
Although literature review reveals many articles discussing PCMH training in residency education, most focus on the challenges of PCMH practice transformation in residency settings.3,4,26,27 Some describe implementation of specific PCMH training based on a simple situated learning model,12–14 similar to that of our baseline PCMH curriculum prior to 2011,15 with few reporting curricular evaluation.13,14 Studies of effects on residents have been limited to quantitative evaluations of resident self-reported knowledge, attitudes, and skills, with either small sample sizes14 or pooled results of multiple programs with multiple different curricular interventions.13 In contrast, our intervention was created in response to our qualitative interview study that revealed that longitudinal immersion in a PCMH practice with supporting curricula, similar to those implemented by others in early stages of PCMH transformation,12–14 was not adequate to impart PCMH leadership skills to family medicine residents. We reasoned that while residents were experiencing active situated learning related to direct patient care within a PCMH, they were experiencing only passive situated learning related to population health and PCMH systems. Therefore, our educational intervention is an attempt to move beyond “PCMH basic training” toward “PCMH leadership training”, which many experts have described as essential for the future of primary care.22,23,28,29 By actively creating a meaningful role for resident leadership within the PCMH, we attempted to transform passive situated learning to active situated learning.
Our qualitative interviews reveal what might not be easily measured by quantitative questionnaires, namely a subtle, yet significant difference between intervention and comparison of PGY3 residents’ PCMH knowledge and attitudes, and their experience conducting PCMH-related tasks. However, after experiencing just 4 weeks of this new PCMH block rotation, the PGY3 residents in this study appear not to have had adequate experience to become leaders in the PCMH community of practice necessary to support junior learners in the situated learning model. A PCMH curriculum dose of our baseline longitudinal immersion and didactic curriculum15 plus one 4-week block rotation likely provides adequate opportunity to appreciate the system-level challenges involved with such things as population health and quality improvement, but inadequate experience to tackle complexities and see results of interventions, leading to some frustration. Thus, this higher level of training might be considered “PCMH intermediate training” but does not reach our goal of PCMH leadership training.
There are several limitations to this study. This is an intervention at a single family medicine residency, which has been a Level 3 PCMH since 2010, so this intervention many not be well suited to programs in earlier stages of PCMH transformation or to residencies for which primary care is not a central concern. In addition, our study was conducted after only 1 year of program implementation; therefore, the long-term effects of the rotation have not been assessed. Finally, although a family medicine residency size of 39 residents (13 in each class) is considered a large residency program in the USA, a qualitative study of only 13 participants in each group (total 26) may limit the generalizability of these findings.
Next steps
Given the promising results of this study and the need for family medicine residencies to prepare future leaders in primary care innovation,21–23,28 we are continuing with our plan for a robust 3-year longitudinal curriculum toward PCMH leadership training. We have developed and are implementing new educational elements and progressive leadership roles for residents returning for Year 2 and Year 3 of this block rotation. Clarification of resident roles and expectations improved through this first year but need ongoing attention. While residents’ frustration with institutional barriers to improve patient care systems (eg, transitions of care) reflects a new understanding of real-world system challenges, explicit education regarding institutional change process may be needed. Faculty development regarding PCMH transformation is being implemented as residents progress from novice to proficient or even expert in PCMH-related competencies. Finally, we plan to rigorously assess the PCMH learning trajectory as residents progress through this longitudinal curriculum.
Conclusion
The primary care practice landscape in the USA is changing rapidly making it necessary for primary care residencies to prepare graduates to be knowledgeable and versatile leaders in this changing environment. While PCMH practice transformation with PCMH basic training is a necessary first step in this process, PCMH intermediate training, utilizing an enhanced situated learning model, such as studied in this article, may be a necessary next step in the journey toward PCMH leadership training for primary care residents. Further study is needed to assess the effectiveness and sustainability of this educational intervention.
Acknowledgments
The authors thank Judith Walker, Helen Bryan, and Scott Hewitt for their administrative support in curricula implementation and data gathering. We thank Nicola Polleti for assistance in literature search. This project was supported by HRSA Primary Care Residency Training grant # D58HP20805.
Disclosure
The authors report no conflicts of interest in this work.
References
Rosenthal TC. The medical home: growing evidence to support a new approach to primary care. J Am Board Fam Med. 2008;21(5):427–440. | ||
Martin JC, Avant RF, Bowman MA; Future of Family Medicine Project Leadership Committee. The Future of Family Medicine: a collaborative project of the family medicine community. Ann Fam Med. 2004;2(1):s3–s32. | ||
Angelotti M, Bliss K, Schiffman D, et al. Transforming the primary care training clinic: New York State’s hospital medical home demonstration pilot. J Grad Med Educ. 2015;7(2):247–252. | ||
Brown CM, Cronholm PF, Wright J, Warning WJ 2nd, Radosh L, Gabbay R. A collaborative approach to achieving NCQA PCMH recognition within family medicine residency practices. Fam Med. 2014;46(1):19–27. | ||
Reid A, Baxley E, Stanek M, Newton W. Practice transformation in teaching settings: lessons from the I3 PCMH Collaborative. Fam Med. 2011;43(7):487–494. | ||
Carney PA, Eiff MP, Saultz JW, et al. Assessing the impact of innovative family medicine training for the patient centered medical home. J Grad Med Educ. 2012;4(1):16–22. | ||
Hochman ME, Asch S, Jibilian A, et al. Patient-centered medical home intervention at an internal medicine resident safety-net clinic. JAMA Intern Med. 2013;173(18):1694–1701. | ||
Evans L, Whitham JA, Trotter DR, Filtz KR. An evaluation of family medicine residents’ attitudes before and after a PCMH innovation for patients with chronic pain. Fam Med. 2011;43(10):702–711. | ||
Saffel-Shrier S, Gunning K, Van Hala S, et al. An RC-FM variance to establish a patient-centered medical home in an assisted living facility. Fam Med. 2012;44(2):128–131. | ||
Barr WB, Aslam S, Levin M. Evaluation of a group prenatal care-based curriculum in a family medicine residency. Fam Med. 2011;43(10):712. | ||
Markova T, Mateo M, Roth LM. Implementing teams in a patient-centered medical home residency practice: lessons learned. J Am Board Fam Med. 2012;25(2):224–231. | ||
Doolittle BR, Tobin D, Genao I, Ellman M, Ruser C, Brienza R. Implementing the patient-centered medical home in residency education. Educ Health (Abingdon). 2015;28(1):74–78. | ||
Jortberg BT, Fernald DH, Dickinson LM, et al. Curriculum redesign for teaching the PCMH in Colorado family medicine residency programs. Fam Med. 2014;46(1):11–18. | ||
Thomas-Hemak L, Palamaner Subash Shantha G, Gollamudi LR, et al. Nurturing 21st century physician knowledge, skills and attitudes with medical home innovations: the wright center for graduate medical education teaching health center curriculum experience. PeerJ. 2015;3:e766. | ||
El Rayess F, Goldman R, Furey C, Chandran R, Goldberg AR, Anandarajah G. Patient-centered medical home knowledge and attitudes of residents and faculty: certification is just the first step. J Grad Med Educ. 2015;7(4):580–588. | ||
Mann K. Theoretical perspectives in medical education: past experiences and future possibilities. Med Educ. 2011;45(1):60–68. | ||
Morris C, Blaney D. Work-based learning. In: Swanwick T, editor. Understanding Medical Education. Oxford: Wiley Blackwell; 2014:97–109. | ||
Harden RM, Laidlaw JM. Essential Skills for a Medical Teacher. London: Elsevier, Churchill, Livingston; 2012:99–103. | ||
Chandran R, Furey C, Goldberg A, Ashley D, Anandarajah G. Training family medicine residents to build and remodel a patient centered medical home in rhode island: a team based approach to PCMH education. R I Med J (2013). 2014;98(4):35–41. | ||
National Committee for Quality Assurance [webpage on the Internet]. Patient Centered Medical Home Recognition. Available from: http://www.ncqa.org/Programs/Recognition/Practices/PatientCenteredMedicalHomePCMH.aspx. Accessed January 10, 2016. | ||
Scherger J. Preparing the personal physician for practice (P4): essential skills for new family physicians and how residencies may provide them. J Am Board Fam Med. 2007;20(4):348–354. | ||
Rogers J, Heaton C. STFM focuses activities on the patient-centered medical home. Ann Fam Med. 2009;7(1):89–90. | ||
Kruse J. The patient-centered medical home: a brief educational agenda for teachers of family medicine. Fam Med. 2013;45(2):132–136. | ||
Chang A, Bowen J, Buranosky R, et al. Transforming primary care training – patient-centered medical home entrustable professional activities for internal medicine residents. J Gen Intern Med. 2013;28(6):801–809. | ||
Borkan J. Immersion/crystallization. In: Crabtree BF, Miller WL, editors. Doing Qualitative Research. 2nd ed. Thousand Oaks, CA: Sage Publications; 1999:179–194. | ||
Lindbloom EJ, Ringdahl E. Resident duty hour changes: impact in the patient-centered medical home. Fam Med. 2014;46(6):463–466. | ||
Fernald DH, Deaner N, O’Neill C, Jortberg BT, degruy FV 3rd, Dickinson WP. Overcoming early barriers to PCMH practice improvement in family medicine residencies. Fam Med. 2011;43(7):503–509. | ||
Scherger JE. The unfinished story of family medicine transformation. Fam Med. 2014;46(1):5–6. | ||
Scherger JE. Preparing the personal physician for practice (P4): essential skills for new family physicians and how residency programs may provide them. J Am Board Fam Med. 2007;20(4):348–355. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.