")
Back to Journals » Clinical Ophthalmology » Volume 17
Effectiveness of the Use of Three-Dose Intravitreal Ziv-Aflibercept in the Management of Diabetic Macular Edema in a Real-Life Setting
Authors Munayco-Guillén F , Vazquez-Membrillo MA, Garcia-Roa MR , De La Cruz-Vargas JA , García-Perdomo HA, Pichardo-Rodriguez R
Received 22 November 2022
Accepted for publication 3 March 2023
Published 12 April 2023 Volume 2023:17 Pages 1129—1135
DOI https://doi.org/10.2147/OPTH.S398359
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fernando Munayco-Guillén,1,2 Miguel Angel Vazquez-Membrillo,1,2 Marlon Rafael Garcia-Roa,1,2 Jhony Alberto De La Cruz-Vargas,3 Herney Andrés García-Perdomo,4 Rafael Pichardo-Rodriguez3
1Department of Retina and Vitreous Surgery, Instituto Mexicano de Oftalmología (IMO), Querétaro, México; 2Universidad Nacional Autónoma de México (UNAM), México City, México; 3Instituto de Investigaciones en Ciencias Biomédicas (INICIB), Universidad Ricardo Palma, Lima, Perú; 4Division of Urology/Urooncology, Deparment of Surgery, School of Medicine, Universidad del Valle, Cali, Colombia
Correspondence: Fernando Munayco-Guillén, Fray Servando Teresa de Mier 202, Quintas del Marqués, Querétaro, México, Tel +51 985-558886, Email [email protected]
Purpose: It has been reported that intravitreal Ziv-aflibercept is a safe and effective drug for the treatment of diabetes macular edema (DME). The objective of this study was to evaluate in a real-life setting, the efficacy of intravitreal Ziv-aflibercept in the treatment of DME after the administration of three consecutive monthly doses.
Methods: A single arm, prospective cohort study. We included patients with DME who received three doses of intravitreal Ziv-aflibercept. Data such as best corrected visual acuity (BCVA) and tomographic biomarkers before treatment and a month after the third dose were collected. DME was staged using the Panozzo classification.
Results: Thirty-eight patients participated for a total of 53 eyes. The mean age was 59 ± 8.1 years. We observed significant changes after the third dose in the parameters studied (BCVA in LogMAR pre-treatment (0.6 ± 0.33) and post-treatment (0.4 ± 0.29) [p< 0.001], macular thickness pre-treatment (501 ± 167 μm) and post-treatment (324 ± 114 μm) [p< 0.001], macular volume pre-treatment 10.8 (7.5– 17.8) mm3 and post-treatment 9.3 (0– 13.6) mm3 [p< 0.005]). And 73.6% of the patients presented an advanced severe stage during their pre-treatment evaluation and after post-treatment, 64.2% of the patients no longer presented edema. No systemic or ocular adverse events occurred.
Conclusion: The use of three consecutive monthly doses of intravitreal Ziv-aflibercept in a real-life setting is effective and safe in the management of diabetic macular edema.
Keywords: antiangiogenic, diabetes mellitus, intravitreal injection, macular edema, optical coherence tomography, Ziv-aflibercept
Introduction
Diabetic macular edema (DME) is one of the main causes of vision loss that affects approximately 21 million people in the world.1 This condition presents in 12% of the patients with Type 1 diabetes mellitus (DM1) and in 28% of the patients with Type 2 diabetes mellitus (DM2).2,3 It is estimated that by the year 2030, DME will increase to 100 million cases in the entire world.3
The use of intravitreal therapy with antiangiogenics is the first line of therapy for the management of DME.4 Currently, antiangiogenics such as bevacizumab, ranibizumab and aflibercept are the most used in ophthalmology; however, a great inconvenience is its high cost when patients try to access these medications, which is why Ziv-aflibercept is used as an alternative treatment due to its lower cost, accessibility, safety and effectiveness.5,6
Ziv-aflibercept is a recombinant fusion protein that has binding domains to the vascular endothelial growth factor (VEGF) of human VEGF receptors 1 and 2 fused with the Fc domain of human immunoglobulin-G1. It is administered intravenously and has the United States FDA (Food and Drugs Administration) approval since 2012 for the treatment of metastatic colorectal carcinoma.3,7 Although it is not yet approved by the FDA for ophthalmological use, there are several studies that demonstrate that Ziv-aflibercept in doses of 1.25 mg/0.05mL or 2 mg/0.08 mL is safe for clinical use.
When comparing Ziv-aflibercept to other antiangiogenic drugs like aflibercept, Ziv-aflibercept has a molecular weight of 115 kDa equal to that of aflibercept but has a high osmolarity (1000 mOsm/kg) compared to aflibercept (300mOsm/kg). Only a small injection volume is used which is diluted in the vitreous cavity, changing the osmolarity in the vitreous cavity from 300 mOsm/kg to 312 mOsm/kg posing no risk to the retina.
So far, reported adverse events presented after the application of Ziv-aflibercept are very similar to the rest of antiangiogenics,2,9–11 therefore it can be taken into consideration as an alternative treatment for other retinal macular pathologies (diabetic macular edema, wet-age-related macular degeneration, vein occlusion macular degeneration, choroidal neovascular membranes).5,8–10 Studies carried out with Ziv-aflibercept for ophthalmological use have demonstrated to be safe for human use.2,5,6,10,12,13
Another advantage to Ziv-aflibercept is its cost, which is 60 times lower (by dose) compared to ranibizumab or aflibercept and 40 times less expensive than bevacizumab (per dose).1,4 Its adequate safety, efficacy and cost profiles are making it a good alternative as an antiangiogenic drug for diabetic macular edema.2,6
The main objective of this study was to evaluate in a real-life setting, the efficacy of intravitreal Ziv-aflibercept after administering three monthly consecutive doses for the treatment of diabetic macular edema using tomographic biomarkers to quantify anatomical changes in the macula.
Method
A single-arm prospective cohort study was done in the Mexican Ophthalmology Institute in Querétaro, México, between the months of August and November 2021. This study was evaluated and approved by the Research Ethics Committee of the Mexican Institute of Ophthalmology with authorization number: CEI/IMO-019/2021 and the approval of the Research Committee of the Mexican Institute of Ophthalmology with authorization number: CI/IMO-013-4/2021. All patients included in this study were asked to sign a consent form. The principles of the Helsinki Declaration were complied with and respected.
We included patients diagnosed with DME from the Retina and Vitreous Department of our institution and that have initiated treatment with intravitreal Ziv-aflibercept 1.25 mg/0.05 mL (Sanofi) for 3 months (1 dose per month). We excluded those with other ocular comorbidities such as patients with tractional and hemovitreous proliferative diabetic retinopathy that did not allow evaluation of the fundus or optical coherence tomography, patients treated with intravitreal antiangiogenics within the last 6 months, prior treatment with subthreshold laser, treatment with intravitreal corticoid within the last 6 months, opacity that does not allow evaluation of the posterior poke through indirect ophthalmoscopy or through optic coherence tomography (OCT), history of uveitis, post vitrectomy (<3 months), cerebrovascular and/or cardiovascular disease (<3 months).
Macular edema was confirmed by spectral-domain OCT (REVO NX 130, Optopol) using the protocol for obtaining horizontal image in the foveal center. Before the first intravitreal injection, we collected the following information for the measurement of the primary outcome: Best Corrected Visual Acuity (BCVA) (measured with a Snellen chart at 3 meters and transformed to LogMAR for statistical analysis), and secondary outcomes: tomographic biomarkers according to the classification by Panozzo et al.14
The Panozzo classification allows us to classify diabetic macular edema into: early, advanced, severe and atrophic diabetic macular edema. Unlike other classifications that only take into account macular thickness, macula morphology and the presence of cysts, this classification uses seven biomarkers (central macular thickness, intraretinal cyst size, stage of the outer limiting membrane and/or ellipsoid, presence of disorganization of inner layers, presence of hyperreflective foci, presence of subretinal fluid and vitreous/retinal ratio) that allows us to more fully assess the response to treatment with Ziv-aflibercept, which is why it was considered most suitable for our study. One month after the third dose, the same variables were quantified. General data such as sex, age, comorbidities, and duration of DM were collected at the beginning of the study. Ocular and systemic adverse events similar to other antiangiogenic drugs were taken into consideration such as intraocular inflammation, endophthalmitis, retinal detachment, vitreous hemorrhage, thromboembolic events, non-ocular hemorrhages, myocardial infarction, stroke and death.
The data obtained were collected in a database produced in Microsoft Excel 2020. Later, we evaluated the quality of the database to address the presence of lost data or inadequate typing.
Frequencies and percentages were presented for qualitative variables and summary measures for quantitative variables based on the normality test for continuous data (Kolmogorov–Smirnov). For bivariate analysis, we used McNemar’s chi squared test and paired Student’s T-test and Wilcoxon’s rank test based on the normality tests. We considered a value of p<0.05 as statistically significant. The data were processed in the JAMOVI version 2.2.5 graphic interphase in the R version 4.2 program language.
Results
A total of 53 eyes from 38 patients (20 males, 18 females) were included, average age was 59 ± 8.1 years. The left eye was most affected (52.8%; n=28). Many patients presented arterial hypertension (64,2%; n=34). There were no patients with DM1. The mean duration of diabetes was 17 ± 6.3 years. The functional and tomographic characteristics in the beginning and after the third dose of intravitreal Ziv-aflibercept ae summarized in Table 1.
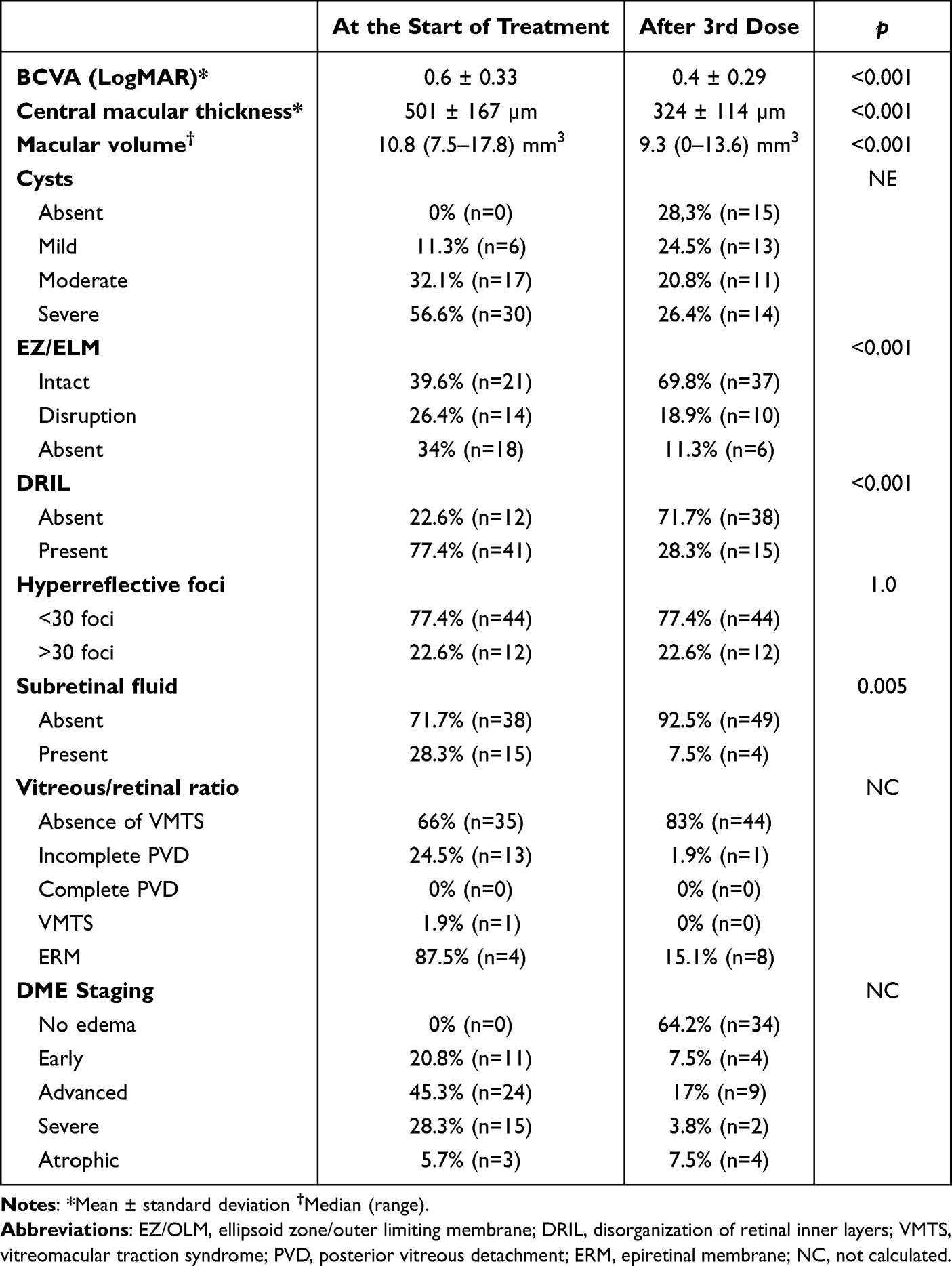 |
Table 1 Tomographic and Functional Characteristics Before and After Three Doses of Intravitreal Ziv-Aflibercept in Patients with Diabetic Macular Edema |
We evidenced improvement in BCVA after the third dose of treatment (p<0.001). Tomographic changes after treatment were seen such as a significant decrease in macular volume, improvement of macular central thickness (p<0.001) and there was a significant change in the stage of ellipsoid zone (EZ)/external limiting membrane (ELM) (p<0.001), disorganization of the inner retinal layers (DRIL) (p<0.001) and the level of subretinal fluid (p=0.005). The change of stages of DME was also statistically significant, with no edema observed in 64.2% (n=34) of eyes evaluated after the third dose of treatment. We did not observe changes in the hyperreflective foci after treatment. The bivariate analysis could not be calculated for the changes in the cysts and vitreous–retinal relationship variables.
In the beginning of the study, 79.2% (n=42) of eyes included presented an advanced, severe, atrophic stage and only 20.8% (n=11) presented an early stage; however, after treatment with intravitreal Ziv-aflibercept, 64.2% (n=34) of eyes had no macular edema, being statistically significant (Figure 1). And 35.8% (n=19) did not respond successfully to treatment and required receiving additional treatment doses.
 |
Figure 1 Changes in the stage of diabetic macular edema. (a) Before treatment, (b) 3 monthly doses of intravitreal Ziv-Aflibercept. |
No patient presented ocular or systemic adverse events.
Discussion
In our study, Ziv-aflibercept showed effectiveness for the treatment of DME. Many of the patients (79.2%) were classified pre-treatment as an advanced, severe or atrophic stage of DME according to the Panozzo et al classification,14 but after post-treatment 64.2% of the patients were classified to a no edema stage. Therefore, demonstrating a regression in the DME stages using Ziv-aflibercept. It should be noted that this DME classification allows us to view the effect of treatment through biomarkers and staging.
Within the tomographic biomarkers that the Panozzo14 classification evaluates, the decrease of mean central macular thickness was noticeable from a baseline of 501 ± 167 to 324 ± 114 µm post-treatment (p<0.05) and the mean macular cube volume from a baseline of 10.8 (7.5–17.8) mm3 to 9.3 (0–13.6) mm3 post treatment (p<0.05). BCVA improved from a mean LogMAR 0.66 ± 0.33 (Snellen 20/100) to LogMAR 0.4 ± 0.29 (Snellen 20/50) after 3 consecutive monthly doses of Ziv-aflibercept. These results are very similar to those reported by Mansour et al,12 where they used intravitreal Ziv-aflibercept 1.25 mg/0.05 mL as treatment for DME for 3 consecutive months. They obtained an initial pre-treated visual acuity LogMAR of 0.70 (20/100) and 0.42 (20/50) post-treatment and a pre-treatment macular thickness of 517.5 µm compared to 322 µm post-treatment, which indicate that there is a good and rapid response in the resolution of macular edema with 3 consecutive monthly doses.
In our study, there were no cases of ocular or systemic adverse effects reported, concordant with findings in other studies such as Mansour et al9 and De Andrade et al15 that showed that Ziv-aflibercept is safe to use for up to 2 years. The largest case series published to date where intravitreal Ziv-aflibercept is used as treatment for diverse macular pathologies (5914 patients) reported the following adverse effects: 1 case of endophthalmitis, 3 cases of intraocular inflammation, 1 case of conjunctival thinning and necrosis, and 1 case of scleral nodule, 1 case of central retinal artery obstruction.2,11,13,16 Adverse events are not much different than any other antiangiogenic drug. Prior studies and our study are indicative that Ziv-aflibercept is a safe medication for short- and long-term ophthalmic use (the largest follow-up study was up to 48 months).2,5,6,10,12,15 We suggest more studies are needed to determine the long-term safety of Ziv-aflibercept.
One of the main concerns regarding the ophthalmologic use of Ziv-aflibercept was its osmolarity (1000 mOsm/kg) which is 3 times greater than aflibercept (300 mOsm/kg) and it is hyperosmolar compared to the vitreous humor (300 mOsm).2,12 This hyperosmolarity is due to purification methods and buffer solutions (polysorbate, sodium phosphate, sodium chloride and saccharose) added during its production.10 There are many studies that have evaluated the safety of Ziv-aflibercept and resulted satisfactory for its use,2,5,6,10,12 this is because the dose used 1.25 mg/0.05 mL of Ziv-aflibercept compared to the relatively large volume of an adult vitreous (4 mL) dilutes the small volume (0.05 mL) of medication, causing the intravitreal osmolarity to increase from 300 mOsm/kg to approximately 312 mOsm/kg, very much below the 500 mOsm/kg umbral required to cause damage to the retina (retinal detachment, loss of villi from the retinal pigment epithelium, hyperosmotic cytotoxicity).5,8,13,17 Studies have also been performed using 2 mg/0.08mL and 2.5 mg/0.1mL, and no differences were found regarding safety and effectiveness compared to 1.25 mg/0.05 mL.9,10,16,18–20
Baghi et al did a similar study using three monthly consecutive doses of bevacizumab 1.25 mg/0.05 mL. They found an improvement in visual acuity of 0.4±0.3 LogMAR after 3 months, similar to what we obtained in our study with Ziv-aflibercept (0.4 ± 0.29 LogMAR). In addition, Baghi et al found a reduction in central macular thickness (313±120 μm) also very similar to results found in our study using Ziv-aflibercept (324 ± 114 μm).18
When comparing our results with another study by Lai et al, where ranibizumab 0.5 mg/0.05 mL was used, it was observed that results from our study using Ziv-aflibercept (0.4 ± 0.29 LogMAR) was superior in visual improvement after 3 monthly doses compared to ranibizumab (0.62 ± 0.38 LogMAR) but was inferior in reducing macular thickness (324 ± 114 µm vs 276±88 µm).21 Fouda et al used three consecutive monthly doses of aflibercept an demonstrated to be similar compared to Ziv-aflibercept from our study. They found an improvement of visual acuity (0.5±0.2 LogMAR vs 0.4 ± 0.29 LogMAR) and central macular thickness reduction (370±83 μm vs 324 ± 114 µm) at 3 months of treatment.22
In its molecular structure, Ziv-aflibercept is very similar to aflibercept (except in its excipients and osmolarity), with the latter having 100 times more affinity towards VEGF 165 (the most common and important isoform of VEGF-A for angiogenesis) than bevacizumab and ranibizumab. It can also join all isoforms of VEGF-B and placental growth factor (PlGF), which could explain the effectiveness of Ziv-aflibercept, not just for DME but also for other entities such as proliferative diabetic retinopathy, macular degeneration related to exudative age, choroid neovascularization, macular edema secondary to occlusive vascular events.5,19,20 The greater affinity to the receptor of the VEGF 165 isoform allows better control of vascular permeability producing a greater resolution of diabetic macular edema in short term as demonstrated by our findings.
This drug can be stored in 1-mL syringes, storage is recommended at 4 to 8 C° for up to 28 days to prevent loss of its molecular characteristics, effectiveness and sterility, which makes it a versatile drug for its storage and distribution.5,23,24
One of the main limitations of this study was the number of participants and the short post-treatment follow-up, which can explain why the change in staging after treatment was not statistically significant despite having relevant clinical results. Another limiting factor was the study design, since it was only observational, it did not allow to control the presence of potential bias (lack of randomization, control group comparison, blinding).
In conclusion, the use of three consecutive monthly doses of intravitreal Ziv-aflibercept in a real-life setting is an effective and safe for treatment of DME making Ziv-aflibercept a viable alternative.
Summary Statement
Ziv-aflibercept is an antiangiogenic drug with a chemical structure similar to aflibercept. In prior studies, it has been shown to be effective and safe for the treatment of diabetic macular edema and other macular pathologies. It constitutes an excellent alternative treatment due to its easy transportation, storage, distribution, lower cost and application techniques similar to other antiangiogenics.
Ethics Approval and Informed Consent
This research was approved by the Research Ethics Committee of the Mexican Institute of Ophthalmology with authorization number: CEI/IMO-019/2021 and the Research Committee of the Mexican Institute of Ophthalmology with authorization number: CI/IMO-013-4/2021. All patients included in this study were asked to sign a consent form.
Acknowledgments
To the directors of the Mexican Ophthalmology Institute and the Department of Retina and Vitreous Surgery personnel for the facilities granted to carry out this study.
Author Contributions
All authors meet the following authorship criteria:
- Made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas.
- Have drafted or written, or substantially revised or critically reviewed the article.
- Have agreed on the journal to which the article will be submitted.
- Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
- Agree to take responsibility and be accountable for the contents of the article.
Funding
Self-financed.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mansour AM, I Al-Ghadban S, Yunis MH, El-Sabban ME. Ziv-Aflibercept in macular disease. Br J Ophthalmol. 2015;99(8):1055–1059. doi:10.1136/bjophthalmol-2014-306319
2. Chhablani J, Narayanan R, Mathai A, et al. Short-term safety profile of intravitreal Ziv-Aflibercept. Retina. 2016;36(6):1126–1131. doi:10.1097/IAE.0000000000000913
3. De Andrade GC, De Oliveira Dias JR, Maia A, et al. Intravitreal injections of Ziv-Aflibercept for diabetic macular edema a pilot study. Retina. 2016;36(9):1640–1645. doi:10.1097/IAE.0000000000001000
4. Demirel S, Argo C, Agarwal A, et al. Updates on the clinical trials in diabetic macular edema. Middle East Afr J Ophthalmol. 2016;23(1):3–12. doi:10.4103/0974-9233.172293
5. Singh SR, Dogra A, Stewart M, et al. Intravitreal Ziv-Aflibercept: clinical effects and economic impact. Asia Pac J Ophthalmol. 2017;6(6):561–568.
6. Barmas-Alamdari D, D’Souza HS, Kapoor KG, Wagner AL. Intravitreal Ziv-Aflibercept: a comprehensive review. Semin Ophthalmol. 2019;34(6):420–435. doi:10.1080/08820538.2019.1641526
7. Hernandez-Da Mota SE, Melo-Granados EAR, Fromow-Guerra J, et al. Correlation analysis of fundus autofluorescence, spectral domain optical coherence tomography, and visual function in patients with diabetic macular oedema treated with intravitreal Ziv-Aflibercept. Eur J Ophthalmol. 2019;29(3):271–277. doi:10.1177/1120672119833267
8. Jabbarpoor Bonyadi MH, Baghi A, Ramezani A, et al. One-year results of a trial comparing 2 doses of intravitreal Ziv-Aflibercept versus bevacizumab for treatment of diabetic macular edema. Ophthalmol Retina. 2018;2(5):428–440. doi:10.1016/j.oret.2017.09.010
9. Mansour AM, Ashraf M, Charbaji A, et al. Two-year outcomes of intravitreal Ziv-Aflibercept. Br J Ophthalmol. 2018;102(10):1387–1390. doi:10.1136/bjophthalmol-2017-311591
10. Mansour AM, Stewart MW, Farah ME, et al. Ziv-Aflibercept: a cost-effective, off-label, highly potent antagonist of vascular endothelial growth factor. Acta Ophthalmol. 2020;98(5):e540–e548.
11. Singh SR, Stewart MW, Chattannavar G, et al. Safety of 5914 intravitreal ziv-aflibercept injections. Br J Ophthalmol. 2019;103(6):805–810. doi:10.1136/bjophthalmol-2018-312453
12. Mansour AM, Dedhia C, Chhablani J. Three-month outcome of intravitreal ziv-aflibercept in eyes with diabetic macular oedema. Br J Ophthalmol. 2017;101(2):166–169. doi:10.1136/bjophthalmol-2016-308679
13. Singh SR, Chattannavar G, Ayachit A, et al. Intravitreal Ziv-Aflibercept: safety analysis in eyes receiving more than ten intravitreal injections. Semin Ophthalmol. 2020;35(1):2–6. doi:10.1080/08820538.2019.1686528
14. Panozzo G, Cicinelli MV, Augustin AJ, et al. An optical coherence tomography-based grading of diabetic maculopathy proposed by an international expert panel: the European school for advanced studies in ophthalmology classification. Eur J Ophthalmol. 2020;30(1):8–18. doi:10.1177/1120672119880394
15. De Andrade GC, De Oliveira Dias JR, Maia A, et al. Intravitreal Ziv-Aflibercept for diabetic macular edema: 48-week outcomes. Ophthalmic Surg Lasers Imaging Retina. 2018;49(4):245–250. doi:10.3928/23258160-20180329-06
16. Meza-Anguiano A, Romo-García E, Gutiérrez-Ruiz GN, et al. Safety of short-term intravitreal use of ziv-aflibercept 2 mg in different retinal pathologies. Rev Mex Oftalmol. 2019;93(3):125–129.
17. Braimah IZ, Amoaku WM. Use of ziv-aflibercept in diabetic macular edema in a Ghanaian population. Eye. 2022;36(1):40–44. doi:10.1038/s41433-022-02005-6
18. Braimah IZ, Kenu E, Amissah-Arthur KN, Akafo S, Kwarteng KO, Amoaku WM. Safety of intravitreal ziv-aflibercept in choroido-retinal vascular diseases: a randomised double-blind intervention study. PLoS One. 2019;14(10):e0223944. doi:10.1371/journal.pone.0223944
19. Baghi A, Jabbarpoor Bonyadi MH, Ramezani A, et al. Two doses of intravitreal Ziv-Aflibercept versus bevacizumab in treatment of diabetic macular edema: a three-armed, double-blind randomized trial. Ophthalmol Retina. 2017;1(2):103–110. doi:10.1016/j.oret.2016.08.007
20. De Oliveira Dias JR, De Andrade GC, Novais EA, et al. Fusion proteins for treatment of retinal diseases: aflibercept, Ziv-Aflibercept, and conbercept. Int J Retina Vitr. 2016;2(1):1–9.
21. Lai IA, Hsu WC, Yang CM, Hsieh YT. Prognostic factors of short-term outcomes of intravitreal ranibizumab in diabetic macular edema. Int J Ophthalmol. 2017;10(5):765–771. doi:10.18240/ijo.2017.05.18
22. Fouda SM, Bahgat AM. Intravitreal aflibercept versus intravitreal ranibizumab for the treatment of diabetic macular edema. Clin Ophthalmol. 2017;11:567–571. doi:10.2147/OPTH.S131381
23. De Lima Farah J, Sano R, Longo Maugéri IM, et al. Evaluation of aflibercept and ziv-aflibercept binding affinity to vascular endothelial growth factor, stability and sterility after compounding. Int J Retina Vitr. 2018;4(1):1–7.
24. Hermosilla J, Pérez-Robles R, Salmerón-García A, et al. Comprehensive biophysical and functional study of Ziv-Aflibercept: characterization and forced degradation. Sci Rep. 2020;10(1):1–13. doi:10.1038/s41598-020-59465-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.