Back to Journals » Journal of Asthma and Allergy » Volume 15
Effectiveness of Switching to Benralizumab in Severe Refractory Eosinophilic Asthma
Authors Gómez-Bastero Fernández A ![]() , Medina Gallardo JF, Delgado Romero J, Romero Falcón A, Benito Bernáldez C
, Medina Gallardo JF, Delgado Romero J, Romero Falcón A, Benito Bernáldez C ![]() , Gallego Borrego J, Álvarez-Gutiérrez FJ
, Gallego Borrego J, Álvarez-Gutiérrez FJ ![]()
Received 16 January 2022
Accepted for publication 26 April 2022
Published 25 May 2022 Volume 2022:15 Pages 727—735
DOI https://doi.org/10.2147/JAA.S358705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Ana Gómez-Bastero Fernández,1 Juan Francisco Medina Gallardo,2 Julio Delgado Romero,3 Auxiliadora Romero Falcón,2 Cristina Benito Bernáldez,1 Javier Gallego Borrego,4 Francisco Javier Álvarez-Gutiérrez2
1Asthma Unit of Pneumology, Virgen Macarena University Hospital, Seville, Spain; 2Asthma Unit of Pneumology, Virgen Del Rocio University Hospital, Seville, Spain; 3Asthma Unit of Allergy, Virgen Macarena University Hospital, Seville, Spain; 4Asthma Unit of Pneumology, Valme University Hospital, Seville, Spain
Correspondence: Cristina Benito Bernáldez, Asthma Unit of Pneumology, Virgen Macarena University Hospital Avenue Doctor Fedriani, Seville, s/n. CP 41009, Spain, Tel +34 646 081 573, Fax +34 955 926 572, Email [email protected]
Purpose: Benralizumab is a monoclonal antibody that targets the α subunit of the IL-5 receptor. Clinical trials have demonstrated the efficacy of this agent with respect to lung function and symptom control in patients with refractory eosinophilic asthma. However, few studies have evaluated the efficacy of benralizumab after switching previous treatment with other monoclonal antibodies.
Patients and Methods: We performed a multicenter retrospective study under conditions of daily clinical practice. The study population comprised consecutively included patients with severe refractory eosinophilic asthma whose initial treatment with omalizumab or mepolizumab was switched to benralizumab. Patients were evaluated at 4 and 12 months after starting treatment with benralizumab. We analyzed asthma control, number of severe exacerbations, corticosteroid cycles, visits to the emergency department, and hospital admissions, as well as lung function. Similarly, we evaluated the response to treatment according to previously established criteria.
Results: We evaluated 40 patients who switched from omalizumab (n=16) or mepolizumab (n=24) to benralizumab. The reasons for switching were lack of response in 30 cases, adverse effects in 9, and patient request in 1. Switching was followed by a significant decrease in the number of exacerbations, visits to the emergency department, and corticosteroid cycles, as well as improved ACT both at 4 and 12 months. However, no significant improvement in lung function was observed. Asthma control (including complete response and control) was achieved in 55% of patients (n=22) at 12 months. Specifically, a complete response was achieved in 30% of patients at 12 months (66.7% switching from omalizumab and 33.3% from mepolizumab).
Conclusion: Patients diagnosed with severe refractory eosinophilic asthma who experience a partial response with omalizumab or mepolizumab could benefit from switching to benralizumab. This approach can reduce the number of exacerbations, visits to the emergency department, and corticosteroid cycles and improve control of asthma.
Keywords: monoclonal antibodies, severe uncontrolled asthma, daily clinical practice, treatment optimization
Introduction
The prevalence of severe refractory asthma in adults ranges from 3% to 10%.1 The recent discovery of the molecular mechanisms involved in the pathogenesis of asthma has led to the development of new biologic therapies. Omalizumab was the first biologic anti-IgE antibody approved for treatment of asthma and has proven effective in patients with allergic asthma.2 The key role of eosinophils in the inflammatory processes of asthma was subsequently clarified. These entities have also been targeted by new biologics. The first drug developed was mepolizumab, followed by reslizumab, both of which are anti-IL-5 monoclonal antibodies and, more recently, benralizumab, a monoclonal antibody targeting the α subunit of the IL-5 receptor. These treatments have proven efficacious for severe refractory eosinophilic asthma.3–7
By blocking IL-5R, benralizumab directly eliminates eosinophils and basophils via NK cells and antibody-mediated cytotoxicity.8 Several clinical trials have shown that benralizumab significantly reduces the frequency of exacerbations, increases forced expiratory volume in the first second (FEV1), and decreases the need for oral corticosteroids, with a favorable safety profile. These positive results were independent of baseline IgE levels and the presence of allergy.5–7,9
However, patients who fulfill the requirements for anti-eosinophilic treatment may not respond appropriately to benralizumab.10,11
Given the lack of direct comparisons, the initial choice of antibody is based mainly on patient and physician preference. Results from recent meta-analyses are contradictory.12–17
The response to biologic treatment in patients with severe refractory asthma should be evaluated at 4–6 months after initiation.18–20 If a good response is not achieved in terms of exacerbations, symptom control, lung function, reduced dose of oral corticosteroids, and patient satisfaction, then we can consider switching to another biologic, provided that the patient is a suitable candidate.
The efficacy of switching monoclonal antibodies was recently evaluated using the Global Evaluation of Treatment Effectiveness (GETE) score21 in patients with severe refractory asthma and an inadequate response to initial biologic therapy. Study results and real-world data on the efficacy of switching from omalizumab to mepolizumab22–26 proved satisfactory in most cases; also, recent studies show results after switching from different anti-IL-5 biologics.27–29 However, few data have been reported on the switch to benralizumab.
In the present multicenter retrospective study, we investigate whether the different mode of action of benralizumab makes it an effective treatment option for patients with severe refractory eosinophilic asthma who respond inadequately to or experience adverse effects with omalizumab or mepolizumab.
Materials and Methods
Study Population
We performed a multicenter retrospective study under conditions of daily clinical practice. We consecutively included adult patients with severe refractory eosinophilic asthma who were receiving benralizumab at the asthma units of the pulmonology and allergology departments of 3 teaching hospitals in Seville, Spain between June 2020 and June 2021. All the patients were diagnosed with severe asthma according to the European Respiratory Society/American Thoracic Society guidelines30 and were receiving treatment with high-dose inhaled corticosteroids and a long acting β2 agonist, as well as another controller medication and/or oral corticosteroids. All the patients had undergone the asthma control protocol, which consists of a review of inhaler technique and adherence (adherence is controlled by electronic prescription, where the collection of the medication by the patient in the pharmacy is verified), an evaluation of aggravating factors, and an assessment of control of comorbid conditions.
All the patients analyzed had been receiving benralizumab for at least 4 months after switching directly from another biologic (omalizumab or mepolizumab). Patients who had not previously received another biologic or had not reached 4 months of treatment with benralizumab were excluded.
The switch to benralizumab was made owing to adverse effects or absence of response according to the criteria for evaluation of monoclonal antibodies in the Consensus Document for Severe Asthma in Adults of the Spanish Society of Pulmonology and Thoracic Surgery (Sociedad Española de Neumología y Cirugía Torácica [SEPAR]).20 These criteria include the number of exacerbations, changes in the Asthma Control Test (ACT) and in the FEV1, as well as withdrawal or reduction of systemic corticosteroids (SC). Based on these criteria, we evaluated response to benralizumab treatment as complete response (no exacerbations in 12 months, ACT ≥ 20, FEV1 ≥ 80%, and SC withdrawal), control (≤ 1 exacerbation in 12 months, ACT ≥ 20, FEV1 < 80% and withdrawal of SC), partial response (reduction of exacerbations < 50% in 12 months, increase > 3 points in ACT with ACT total < 20, increase > 10% and 100 mL in FEV1 with FEV1 < 80%, and reduction > 50% of the SC dose) or no response (does not meet any of the above criteria).20
Patients attended follow-up visits 4 and 12 months after initiation of benralizumab.
The study followed ethical regulations for medical research in humans. Data confidentiality was guaranteed according to Spanish legislation on protection of personal data (Ley Orgánica de Protección de Datos de Carácter Personal [15/1999 of December 13, LOPD]). The study was approved by the Clinical Research Ethics Committee of University Hospital Virgen Macarena and University Hospital Virgen del Rocío. All the participants gave their written informed consent before inclusion in the study.
Variables
We designed a database to collect study variables based on a review of the clinical history. Data were collected prospectively and included the following: sociodemographic data (age and sex), anthropometric data (body mass index), smoking, time since onset of asthma symptoms or since diagnosis of asthma, comorbid conditions, exacerbations, therapy with oral corticosteroids, and blood work-up (IgE and eosinophil count). The blood work-up was performed during the 3 to 6 months before the patient’s baseline visit.
The presence of atopy was investigated based on at least one prick testing result or positive specific IgE for common aeroallergens, including house dust mites (Dermatophagoides pteronyssinus, Dermatophagoides farinae), moulds (Alternaria alternata, Aspergillus fumigatus, Cladosporium herbarum, and Penicillium notatum), pollens (grass mix, Parietaria judaica, Artemisia vulgaris, Oleaeuropaea, Platanus acerifolia, Cupressus arizonica), and dog and cat dander. We used the ACT to evaluate asthma control during the previous 4 weeks.31 We considered only severe exacerbations and verified cycles of oral corticosteroids, visits to the emergency department, and admissions to hospital. These data were obtained from the electronic medical records.
All the variables were recorded at baseline and 4 and 12 months after initiation of benralizumab.
Statistical Analysis
Data were analyzed using SPSS version 21.0. We performed an initial descriptive analysis, in which quantitative variables are expressed using measures of central tendency, position, and dispersion. Qualitative variables are expressed using frequencies. Changes between baseline and 4 and 12 months were assessed using the t-test for paired samples if they followed a normal distribution. Otherwise, we used the Wilcoxon test. The McNemar test was used for qualitative variables. Statistical significance was set at p<0.05.
Results
We included 40 patients who switched from omalizumab (n=16) or mepolizumab (n=24) to benralizumab. The reasons for switching treatment were lack of response in 30 cases (75%), adverse effects in 9 (22.5%), and patient request in 1 (the patient was taking mepolizumab). Patients had been receiving the original biologic for a mean of 25.9 months. Table 1 shows the general characteristics of the study population at baseline.
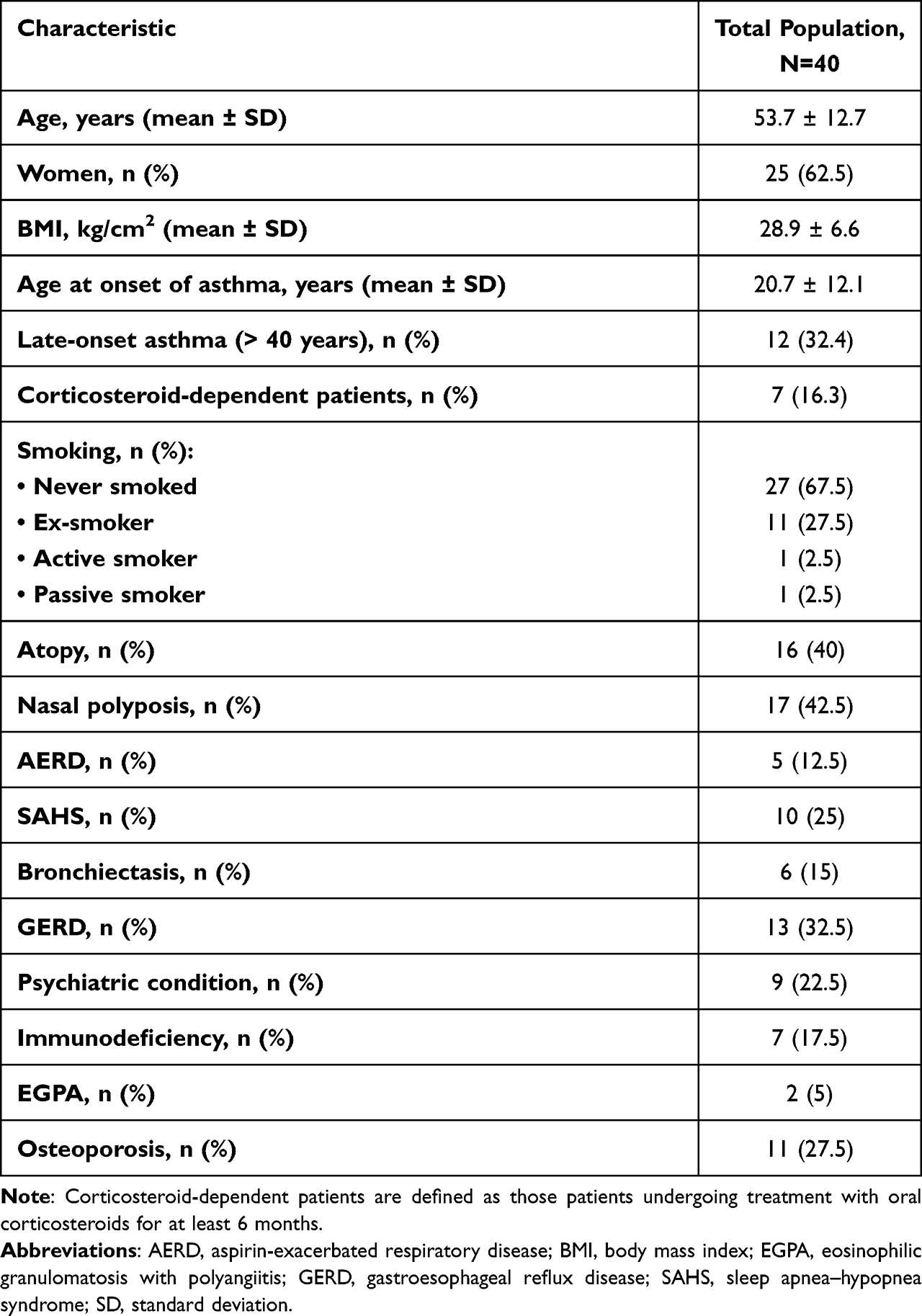 |
Table 1 General Characteristics at Baseline |
Table 2 shows asthma control parameters and laboratory and functional values at initiation of benralizumab.
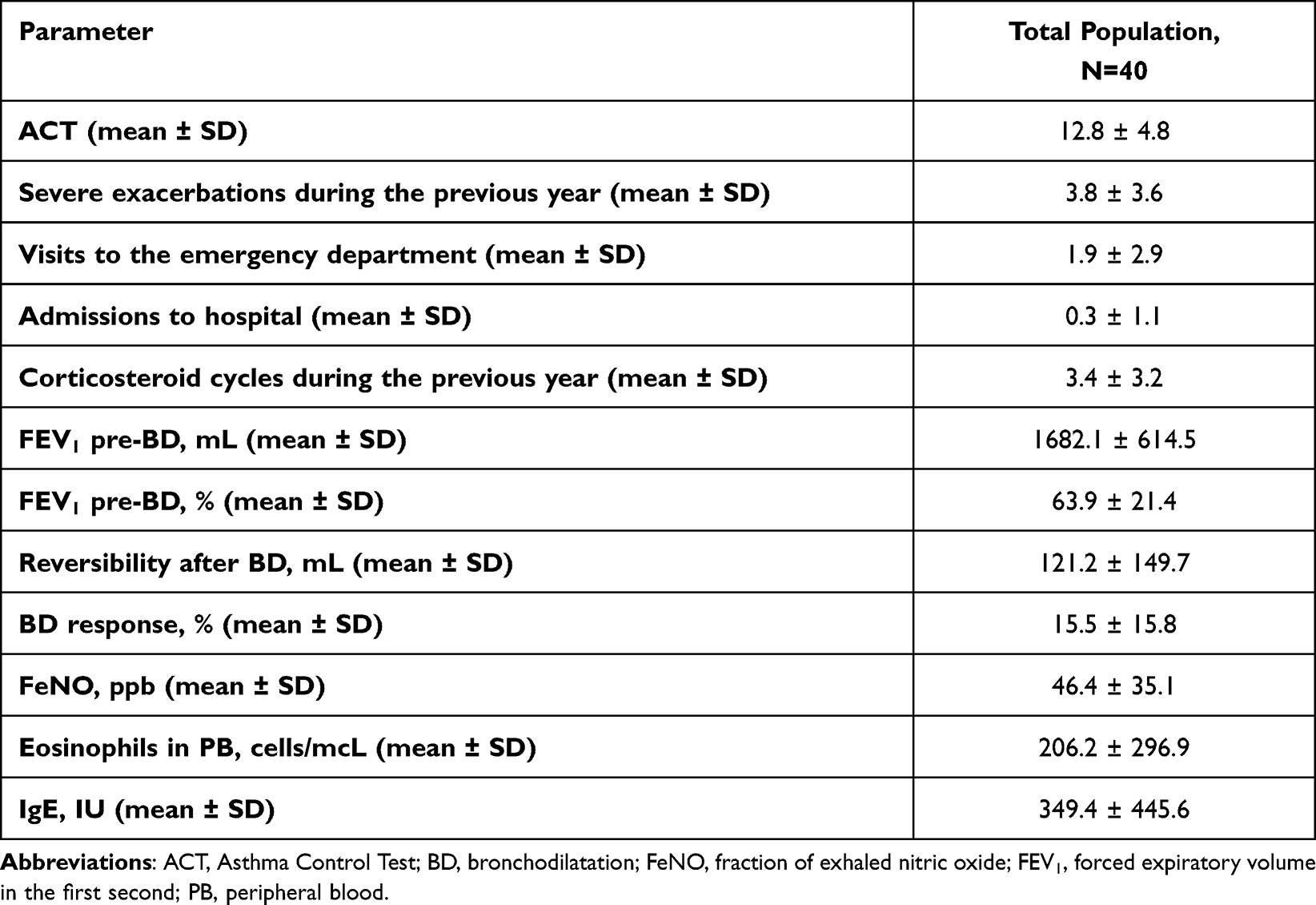 |
Table 2 Baseline Clinical, Functional, and Laboratory Parameters |
The efficacy of benralizumab was evaluated at 4 and 12 months after initiation irrespective of whether the patient had previously been taking omalizumab (Table 3) or mepolizumab (Table 4). In both cases, significant improvements were observed in the number of exacerbations, visits to the emergency department, and corticosteroid cycles, as well as in disease control (according to the ACT). The mean increase in ACT score at 12 months of benralizumab treatment was 6.8, which is numerically greater than the minimal clinically important difference (MCID) (increase of ≥ 3 units). In addition, 80.8% of patients with ACT score recorded at baseline and at 12 months from the start of treatment achieved a clinically significant response (ACT score difference ≥ 3).
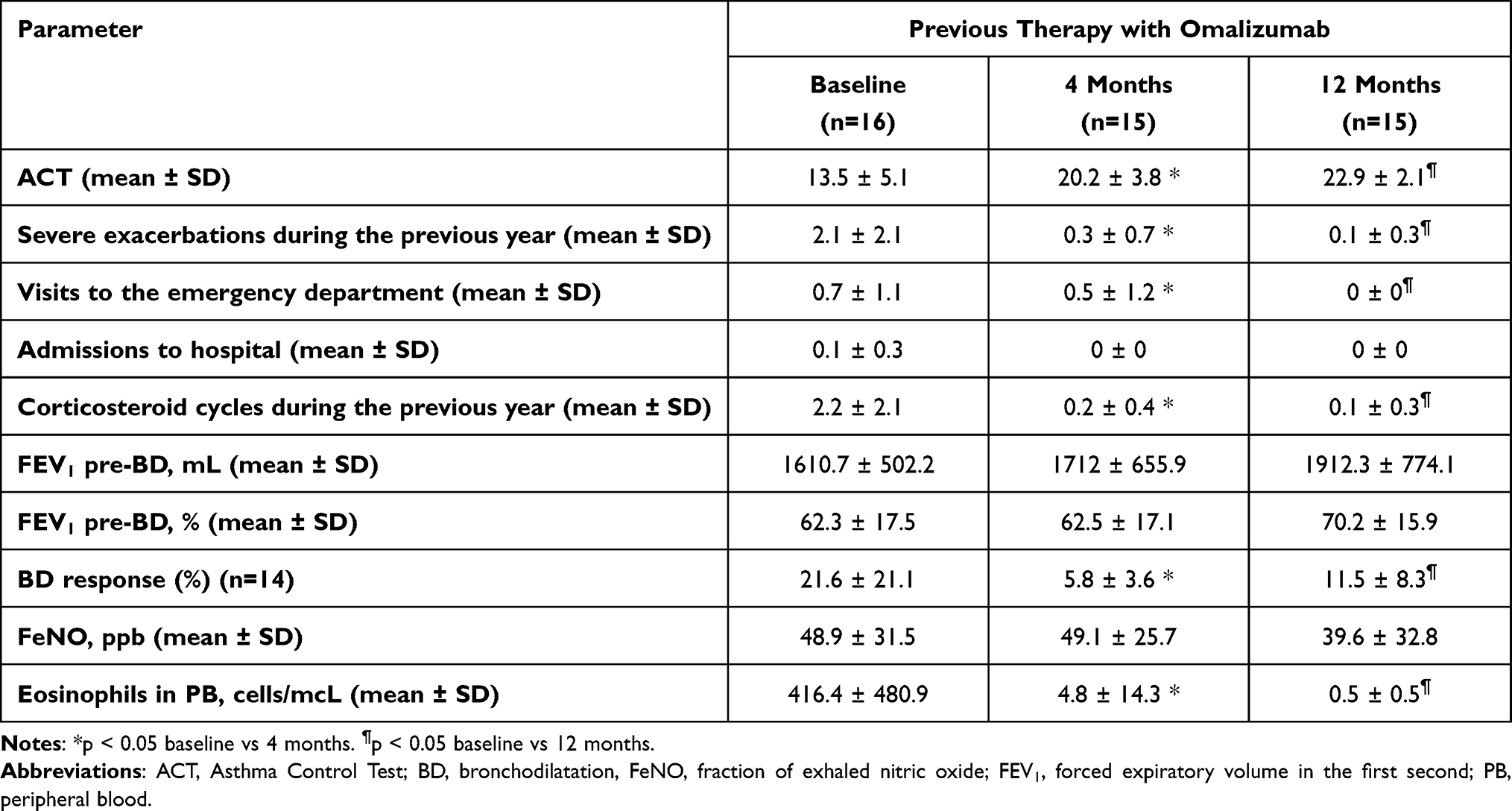 |
Table 3 Clinical, Functional, and Laboratory Parameters at Baseline and at 4 and 12 Months in Patients Who Had Previously Been Taking Omalizumab |
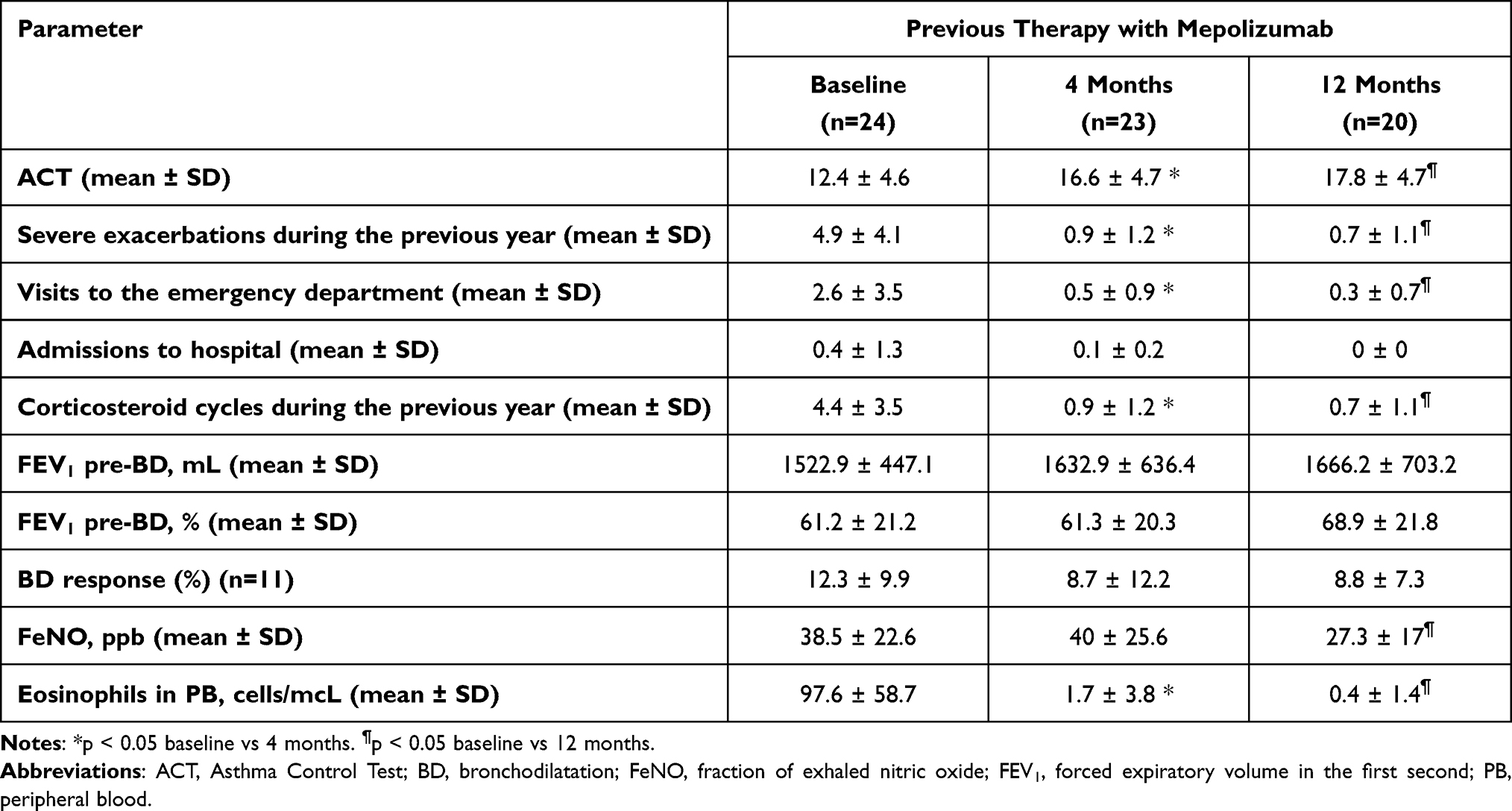 |
Table 4 Clinical, Functional, and Laboratory Parameters at Baseline and at 4 and 12 Months in Patients Who Had Previously Been Taking Mepolizumab |
Although no significant improvements in lung function were recorded, there was a clinically significant increase (+302mL in switching from omalizumab and +144mL in switching from mepolizumab).
Asthma control (including complete response and control according to the criteria mentioned above20) was achieved in 55% of patients (n=22) at 12 months after starting treatment with benralizumab. Specifically, a complete response was achieved in 30% of patients at 12 months, of whom 66.7% switched from omalizumab and 33.3% from mepolizumab; and control in 25% of patients (30% switching from omalizumab and 70% from mepolizumab). A partial response was observed in 42.5% (n=17) (23.5% patients switching from omalizumab, 76.5% patients switching from mepolizumab). No response was obtained only in the case of one patient.
Prior to the change to benralizumab, there were 17.5% of corticosteroid-dependent patients (n=7), who are defined as those patients undergoing treatment with oral corticosteroids for at least 6 months. Three patients discontinued the CS 12 months after starting treatment with benralizumab, and the remaining 4 reduced to < 50% of the dose of oral corticosteroids.
Sinonasal polyposis was recorded in 37.5% of responders and late-onset asthma (> 40 years) in 42.8%, although the responses in these groups of patients were not significantly different (sinonasal polyposis, p=0.474; late-onset asthma, p=0.102). In relation to adverse effects, 10 patients presented mild effects at 4 months after initiation treatment with benralizumab that subsequently disappeared: headache (n=4), fever (n=4), asthenia (n=1), and arthralgia (n=1).
Discussion
Various clinical trials have demonstrated the efficacy of benralizumab for treatment of severe refractory eosinophilic asthma.5–7 Benralizumab has also proven effective in real-world studies.32 However, few studies have evaluated the response of patients to benralizumab after a lack of response to previous monoclonal antibodies. We analyzed the efficacy of benralizumab at 4 and 12 months in a group of 40 patients who had responded inadequately to omalizumab or mepolizumab. After a direct switch to benralizumab, we observed an improvement not only in asthma control (as per the ACT score), but also a significant reduction in the number of severe exacerbations, corticosteroid cycles, and visits to the emergency department. This improvement was observed both in patients who had previously received omalizumab and in those who took mepolizumab, although the percentage of complete response was higher in patients who had previously received omalizumab. Our efficacy findings are consistent with those reported in clinical trials,5–7 except for the fact that the patients in our study had previously been treated with a biologic, whose mechanism of action, in the case of mepolizumab, also involves blockade of IL-5, which is similar to the action of benralizumab. We recorded a rapid response from as early as 4 months after switching, in line with findings from real-world studies;32 this was maintained at 12 months of treatment. The few published studies on switching to benralizumab from other monoclonal antibodies report similar results. Drick et al27 switched to benralizumab in 70 patients (10.5% of the total study population), of whom 60 were eventually included in the analysis. These patients received at least 4 months of treatment with benralizumab after previous treatment with reslizumab or mepolizumab. Only 10 discontinued treatment owing to an insufficient response to benralizumab after at least 4 months; the clinical condition of the remaining patients was stable with the new medication. Consistent with our findings, significant improvements were observed in the number of exacerbations, control of asthma measured using the ACT, and use of corticosteroids. Likewise with our findings, significant improvements in FEV1 (mean improvement 95 mL) were also observed. In our series, functional parameters improved after treatment with benralizumab in both groups (to a greater extent in those previously treated with omalizumab, +302mL, but also in those treated with mepolizumab, +144mL), although the differences were not statistically significant, probably due to the small sample size. Other real-life studies on the efficacy of benralizumab after switching from anti-IL5 biological treatment28,29 or omalizumab obtain efficacy data similar to those found in our series.26
The monoclonal antibody is switched in a notable percentage of patients (> 40%) with a history of nasal polyposis. In patients previously treated with mepolizumab or reslizumab, this factor has been considered a predictor of suboptimal response, together with late-onset asthma and treatment with systemic corticosteroids.10,28,33 We found no differences in the response to benralizumab in patients with sinonasal polyposis or late-onset asthma, like the results found by Kavanagh,28 where they did not find statistically significant differences in the initial characteristics between those who responded and those who did not respond clearly.
The results obtained in our series in the group previously treated with omalizumab could be due to the fact that the main underlying pathophysiological mechanism in our allergic patients with eosinophilic asthma could be due to the production of eosinophils by an IgE-independent mechanism. And with respect to the group previously treated with mepolizumab, although both biologics target IL5, benralizumab, by blocking IL-5R, may have different data because it directly eliminates eosinophils and basophils via NK cells and antibody-mediated cytotoxicity.
Our study is limited by the fact that it included only patients with severe refractory asthma previously treated with omalizumab or mepolizumab who did not respond favorably to these drugs. Therefore, the study is subject to an initial selection bias, since only patients whose previous therapy had failed were included. We were unable to make an inverse comparison, ie, evaluate the progress of patients with omalizumab or mepolizumab whose previous therapy with benralizumab had failed, since few such cases have been reported. Nevertheless, given the paucity of studies that evaluate switching from omalizumab and mepolizumab to benralizumab, we found it interesting to perform the present study. Furthermore, since ours was a multicenter, multidisciplinary study performed in the asthma units of the pulmonology and allergology departments, it may provide a more reliable picture of the course of the disease in daily clinical practice.
Conclusion
Our real-world study shows the efficacy of a direct switch to benralizumab in patients with severe refractory asthma who do not respond to long-term treatment with omalizumab or mepolizumab. The efficacy of benralizumab was demonstrated in terms of asthma control and of the reduced number of severe exacerbations, visits to the emergency department, and corticosteroid cycles. A rapid response to treatment was observed at 4 months, and this was maintained after 12 months.
Acknowledgments
The authors are grateful to María Victoria Maestre and to Vicente Merino for their support during the performance of this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
AGBF has participated in speaking activities, as a scientific advisor or as a participant in clinical studies in the last 3 years sponsored by AstraZeneca, ALK, Bial, Chiesi, GlaxoSmithKline, Mundipharma, Novartis, Orion-Pharma, Sanofi and Teva. JFMG has received honoraria as a speaker, scientific advisor or participant in clinical studies in the last 3 years sponsored by AstraZeneca, Bial, Chiesi, Gebro Pharma, GlaxoSmithKline, Novartis, Sanofi and Teva. JDR has received honoraria as a speaker, scientific advisor or participant in clinical studies in the last 3 years sponsored by AstraZeneca, Bial, Chiesi, Gebro Pharma, GlaxoSmithKline, Novartis, Sanofi and Teva. ARF declares no conflicts of interest. CBB has participated in speaking activities in the last 3 years sponsored by AstraZeneca, GlaxoSmithKline, Novartis and Sanofi. JGB has received honoraria for scientific advice sponsored by AstraZeneca. FAG participated in speaking activities and advisory boards and provided consultancy services during the period 2016–2021 sponsored by AstraZeneca, ALK, Bial, Boehringer-Ingelheim, Chiesi, GSK, Mundipharma, Novartis, Orion-Pharma and Sanofi. All authors declare not having received, directly or indirectly, funding from the tobacco industry or its affiliates. The authors report no other conflicts of interest in this work.
References
1. Hekking -P-PW, Wener RR, Amelink M, et al. The prevalence of severe refractory asthma. J Allergy Clin Immunol. 2015;135:896–902. doi:10.1016/j.jaci.2014.08.042
2. Humbert M, Beasley R, Ayres J, et al. Benefits of omalizumab as add-on therapy in patients with severe persistent asthma who are inadequately controlled despite best available therapy (GINA 2002 step 4 treatment): INNOVATE. Allergy. 2005;60(3):309–316. doi:10.1111/j.1398-9995.2004.00772.x
3. Ortega HG, Liu MC, Pavord ID, et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. 2014;371(13):1198–1207. doi:10.1056/NEJMoa1403290
4. Bel EH, Wenzel SE, Thompson PJ, et al. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N Engl J Med. 2014;371(13):1189–1197. doi:10.1056/NEJMoa1403291
5. Bleecker ER, FitzGerald JM, Chanez P, et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high dosage inhaled corticosteroids and long-acting β2-agonists (SIROCCO): a randomised, multicentre, placebo-controlled Phase 3 trial. Lancet. 2016;388(10056):2115–2127. doi:10.1016/S0140-6736(16)31324-1
6. FitzGerald JM, Bleecker ER, Nair P, et al. Benralizumab, an antiinterleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2016;388(10056):2128–2141. doi:10.1016/S0140-6736(16)31322-8
7. Nair P, Wenzel S, Rabe KF, et al. Oral glucocorticoid–sparing effect of benralizumab in severe asthma. N Engl J Med. 2017;376(25):2448–2458. doi:10.1056/NEJMoa1703501
8. Kolbeck R, Kozhich A, Koike M, et al. MEDI-563, a humanized anti-IL-5 receptor alpha mAb with enhanced antibody-dependent cell-mediated cytotoxicity function. J Allergy Clin Immunol. 2010;125(6):1344–1353.e2. doi:10.1016/j.jaci.2010.04.004
9. Chipps BE, Newbold P, Hirsch I, et al. Benralizumab efficacy by atopy status and serum immunoglobulin E for patients with severe, uncontrolled asthma. Ann Allergy Asthma Immunol. 2018;120(5):504–511. doi:10.1016/j.anai.2018.01.030
10. Mukherjee M, Forero DF, Tran S, et al. Sub-optimal treatment response to anti-IL-5 monoclonal antibodies in severe eosinophilic asthmatics with airway autoimmune phenomena. Eur Respir J. 2020;56(4):2000117. doi:10.1183/13993003.00117-2020
11. Poznanski SM, Mukherjee M, Zhao N, et al. Asthma exacerbations on benralizumab are largely non-eosinophilic. Allergy. 2020;75(5):1023–1042. doi:10.1111/all.14221
12. Bourdin A, Husereau D, Molinari N, et al. Matching-adjusted indirect comparison of benralizumab versus interleukin-5 inhibitors for the treatment of severe asthma: a systematic review. Eur Respir J. 2018;52(5):1801393. doi:10.1183/13993003.01393-2018
13. Cabon Y, Molinari N, Marin G, et al. Comparison of anti-interleukin 5 therapies in patients with severe asthma: global and indirect meta-analyses of randomized placebo-controlled trials. Clin Exp Allergy. 2017;47(1):129–138. doi:10.1111/cea.12853
14. Busse W, Chupp G, Nagase H, et al. Anti-IL-5 treatments in patients with severe asthma by blood eosinophil thresholds: indirect treatment comparison. J Allergy Clin Immunol. 2019;143(1):190–200.e20. doi:10.1016/j.jaci.2018.08.031
15. Henriksen DP, Bodtger U, Sidenius K, et al. Efficacy, adverse events, and inter-drug comparison of mepolizumab and reslizumab anti-IL-5 treatments of severe asthma - a systematic review and meta-analysis. Eur Clin Respir J. 2018;5(1):1536097. doi:10.1080/20018525.2018.1536097
16. Casale TB, Pacou M, Mesana L, et al. Reslizumab compared with benralizumab in patients with eosinophilic asthma: a systematic literature review and network meta-analysis. J Allergy Clin Immunol Pract. 2019;7(1):122–30.e1. doi:10.1016/j.jaip.2018.08.036
17. Mauger D, Apter AJ. Indirect treatment comparisons and biologics. J Allergy Clin Immunol Pract. 2019;7(1):131–133. doi:10.1016/j.jaip.2018.11.008
18. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. Fontana: Global Initiative for Asthma (GINA); 2021. Available from: http://www.ginasthma.org/.
19. GEMA 5.1. Guía Española para el Manejo del Asma [homepage on the Internet]. Madrid: GEMA 5.1; 2021. Available from: http://www.gemasma.com/.
20. Álvarez-Gutiérrez FJ, Blanco-Aparicio M, Plaza V, et al. Consensus document for severe asthma in adults. 2020 update. Open Respir Arch. 2020;2(3):158–174. doi:10.1016/j.opresp.2020.03.005
21. Numata T, Araya J, Miyagawa H, et al. Effectiveness of switching biologics for severe asthma patients in Japan: a Single-Center Retrospective Study. J Asthma Allergy. 2021;3(14):609–618. doi:10.2147/JAA.S311975
22. Carpagnano GE, Pelaia C, D’Amato M, et al. Switching from omalizumab to mepolizumab: real-life experience from Southern Italy. Ther Adv Respir Dis. 2020;14:1753466620929231. doi:10.1177/1753466620929231
23. Chapman KR, Albers FC, Chipps B, et al. The clinical benefit of mepolizumab replacing omalizumab in uncontrolled severe eosinophilic asthma. Allergy. 2019;74(9):1716–1726. doi:10.1111/all.13850
24. Liu MC, Chipps B, Munoz X, et al. Benefit of switching to mepolizumab from omalizumab in severe eosinophilic asthma based on patient characteristics. Respir Res. 2021;22(1):144. doi:10.1186/s12931-021-01733-9
25. Magnan A, Bourdin A, Prazma CM, et al. Treatment response with mepolizumab in severe eosinophilic asthma patients with previous omalizumab treatment. Allergy. 2016;71(9):1335–1344. doi:10.1111/all.12914
26. Pelaia C, Crimi C, Nolasco S, et al. Switch from omalizumab to benralizumab in allergic patients with severe eosinophilic asthma: a real-life experience from Southern Italy. Biomedicines. 2021;9(12):1822. doi:10.3390/biomedicines9121822
27. Drick N, Milger K, Seeliger B, et al. Switch from IL-5 to IL-5-receptor α antibody treatment in severe eosinophilic asthma. J Asthma Allergy. 2020;13:605–614. doi:10.2147/JAA.S270298
28. Kavanagh JE, Hearn AP, d’Ancona G, et al. Benralizumab after sub-optimal response to mepolizumab in severe eosinophilic asthma. Allergy. 2021;76(6):1890–1893. doi:10.1111/all.14693
29. Martínez-Moragón E, García-Moguel I, Nuevo J, Resler G. Real-world study in severe eosinophilic asthma patients refractory to anti-IL5 biological agents treated with benralizumab in Spain (ORBE study). BMC Pulm Med. 2021;21(1):417. doi:10.1186/s12890-021-01785-z
30. Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343–373. doi:10.1183/09031936.00202013
31. Vega JM, Badia X, Badiola C, et al. Validation of the Spanish version of the asthma control test (ACT). J Asthma. 2007;44(10):867–872. doi:10.1080/02770900701752615
32. Padilla-Galo A, Levy-Abitbol R, Olveira C, et al. Real-life experience with benralizumab during 6 months. BMC Pulm Med. 2020;20(1):184. doi:10.1186/s12890-020-01220-9
33. Harrison TW, Chanez P, Menzella F, et al. Onset of effect and impact on health-related quality of life, exacerbation rate, lung function, and nasal polyposis symptoms for patients with severe eosinophilic asthma treated with benralizumab (ANDHI): a randomised, controlled, phase 3b trial. Lancet Respir Med. 2021;9(3):260–274. doi:10.1016/S2213-2600(20)30414-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.